

Abstract
Background:
Decision-making in patients suspected of having acute appendicitis has remained a diagnostic challenge worldwide despite the advances in imaging and appendiceal surgery. There have been efforts to improve the diagnosis of appendicitis using clinical scoring systems.
Aim:
We evaluated and compared the diagnostic accuracy and role of Alvarado score (AS) and two of its modification (Kalan and Al-Fallouji) in the preoperative diagnosis of acute appendicitis.
Materials and Methods:
This was a prospective study conducted at the Usmanu Danfodiyo University Teaching Hospital, Sokoto, of all adult patients operated for acute appendicitis from July 2014 to June 2017. The results were analyzed on computer using Statistical Package for the Social Science version 15.
Results:
One hundred and eleven patients were studied. Sixty-six (59.5%) patients were males and 45 (40.5%) were females. The male-to-female ratio was 1.5:1. The mean age was 23.89 ± 4.93 years. The AS sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of 90.3%, 83.3%, 96.6%, 62.2%, and 89.2%, respectively, were similar to the findings of Kalan score (90.3%, 83.3%, 96.6%, 62.5%, and 89.2%, respectively) and Al-Fallouji score (96.8%, 66.7%, 93.8%, 80%, and 91.9%, respectively). The receiver operating curve and area under the curve show that Alvarado, Kalan, and Al-Fallouji are accurate scores in the preoperative diagnosis of acute appendicitis with an area under the curve of 0.88, 0.86, and 0.85, respectively.
Conclusion:
Kalan and Al-Fallouji scores have comparably good diagnostic accuracy as the AS among our patients. Any of these scores can be used as an adjunct in the preoperative diagnosis of acute appendicitis.
KEYWORDS: Acute appendicitis, Al-Fallouji score, Alvarado score, appendicectomy, diagnostic accuracy, Kalan score, modified Alvarado score, Nigeria, sensitivity, specificity
INTRODUCTION
Appendicitis continues to remain a diagnostic challenge after over a 120 years since its first description.[1] This common surgical disease can surprise the best of clinicians, especially in the extremes of age and among females.[2] Delay in diagnosis definitely increases the morbidity, mortality, and cost of treatment.[2] Surgeons may be inclined to operate when the diagnosis is probable rather than certain. This clinical decision may lead to removal of a normal appendix in 20%–40% of cases.[3] Removing normal appendix is an economic burden both on patients and health resources.[4]
The diagnostic accuracy varies from 25% to 90%, optimal accuracy rate is 80%, and diagnostic error rate is 25% and twice as common in female as in males.[5] Difficulty in diagnosis arises more in very young patients, elderly patients, and females of reproductive age because they usually have atypical presentation in the first two, while many other conditions also mimic appendicitis in females of reproductive age group. Literature shows that 3%–7% of all adults on exploration for acute appendicitis have diseases other than appendicitis.[6]
A drive, therefore, has been to improve the diagnosis of appendicitis using clinical scoring systems. These systems have been based on symptoms, signs, and laboratory findings. In some instances, they have been part of a computer-aided diagnostic algorithm.[7] The most widely cited score in the diagnosis of adults with acute appendicitis is the Alvarado score (AS).[7]
The AS was developed by Alfredo Alvarado in 1986 as an aid to the diagnosis of appendicitis. The score was based on a retrospective study conducted on 305 patients hospitalized at the Nazareth Hospital in Philadelphia, Pennsylvania, USA, with abdominal pain suggestive of acute appendicitis.[8] Signs, symptoms, and laboratory findings were analyzed for specificity, sensitivity, predictive value, and joint probability.[9] The total joint probability, the sum of a true positive and a true negative result, was chosen as diagnostic weight indicative of the accuracy of the test.[8] Eight predictive factors were found to be useful in making the diagnosis of acute appendicitis.[8] AS has shown encouraging results among African patients.[10] Kanumba et al.[10] in their study among Tanzanian patients showed that the use of modified AS (MAS) in patients suspected to have acute appendicitis provided a high degree of diagnostic accuracy and can reduce negative apppendicectomy and complication rates.
There has been modification of the original AS mainly due to unavailability of routine reporting of shift to the left of neutrophils maturation by laboratories in some medical facilities where the AS has been evaluated.[11,12]
The unavailability of routine reporting of shift to the left of neutrophils outside normal working hours made these modifications of Alvarado relevant in our setting. Despite this, there is a dearth of studies comparing Alvarado and its modifications among African patients. We, therefore, compared the diagnostic accuracy of AS and two of its modification, Kalan and Al-Fallouji.
MATERIALS AND METHODS
Design
This was a prospective study conducted at the Usmanu Danfodiyo University Teaching Hospital (UDUTH), Sokoto, over a 3-year period (July 2014 to June 2017). UDUTH is a 572-bed tertiary referral hospital in Northwestern Nigeria with a predominant Hausa-Fulani population.
Inclusion criteria
All consenting consecutive patients during the study period operated with an initial clinical diagnosis of acute appendicitis
Patients who are 16 years or older.
Exclusion criteria
Patients who withhold or are unable to give consent
Patients <16 years
Patients not operated
Patients with demonstrable extra appendicular cause (radiologic or intraoperative) of pain in the right iliac fossa.
Method
The demographic characteristics of the patients; history; physical examination findings including cough, psoas, and obturator signs; concomitant diseases; blood parameters; abdominal ultrasound findings; surgical findings; and histopathological findings were recorded on a pro forma.
All the individual parameters required to score both the Alvarado and MASs – the Kalan and Al-Fallouji were recorded individually and scattered in different areas of the pro forma to make spot calculation difficult. The total score was not calculated until after the appendicectomy.
The decision to perform appendicectomy was made solely on the clinical features of the patient and not influenced by the score. To guarantee this, the actual summation of the scores from the various parameters of the AS and MAS (Kalan and Al-Fallouji) was not done until after the surgery.
After the appendicectomy, the AS was calculated. The patients were assigned to the following four groups based on the score.
Unlikely - AS 1–4
Compatible - AS 5–6
Probable - AS 7–8
Definite - AS 9–10.
The MAS was calculated as described by Kalan et al.[11] Bengezi (Al-Fallouji)[12] was also calculated postoperatively. Classification of patients is similar to the AS.
Data analysis
The results were analyzed on a computer using the Statistical Package for the Social Sciences (SPSS) version 15 (SPSS) Inc. Chicago, IL, USA.
ASs and MASs were correlated with histopathological findings. Negative appendicectomy rate (NAR), positive and negative predictive value (NPV), sensitivity, specificity, and accuracy were calculated.
Multivariate analysis was done to determine the effect of age, sex, and duration of symptoms on the accuracy of Alvarado.
The level of statistical significance was set at P ≥ 0.05.
Ethical clearance
Ethical clearance was obtained from the Ethics Committee of the UDUTH, Sokoto. The ethical clearance approval number is UDUTH/HREC/2014/No. 278.
RESULTS
A total of 111 patients who met the inclusion criteria were studied among which 66 (59.5%) were males and 45 (40.5%) were females, giving a male: female ratio of 1.5:1. The age range was between 16 and 38 years. The mean age was 23.89 ± 4.93 years [Figure 1].
Figure 1.
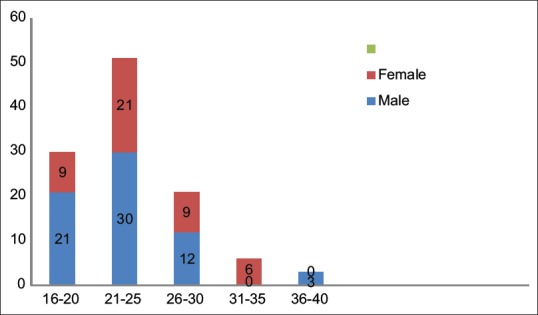
Age/sex distribution of patients with appendicitis
Majority (72 [64.9%]) of the patients were students among which 69 (62.4%) patients had a tertiary education. They were predominantly of the Hausa/Fulani tribe (78.4%).
All the patients presented with an abdominal pain and abdominal tenderness in the right iliac fossa. Other common presentation included anorexia and nausea/vomiting which constituted 87 (78.4%) patients and 99 patients (89.2%), respectively. Rebound tenderness was present in 108 (97.3%), cough sign in 96 (86.5%) patients, psoas sign in 66 (59.5%) patients, obturator sign in 30 (27%) patients, and Rovsing's sign in 51 (45.9%) patients. Table 1 shows the clinical findings among the patients.
Table 1.
Clinical Findings among the patients
| Symptoms/sign | Frequency (n=111), n (%) |
|---|---|
| Abdominal pain | 111 (100) |
| Lower abdominal pain | 108 (97.3) |
| Migratory RIF pain | 87 (78.4) |
| Anorexia | 87 (78.4) |
| Nausea/vomiting | 99 (89.2) |
| Fever | 57 (51.4) |
| History of similar symptoms | 36 (32.4) |
| Urinary symptoms | 18 (16.2) |
| Abdominal tenderness | 111 (100) |
| Rebound tenderness | 108 (97.3) |
| Pyrexia | 54 (48.6) |
| Psoas sign | 66 (59.5) |
| Obturator sign | 30 (27) |
| Rovsing’s sign | 51 (45.9) |
| Cough sign | 96 (86.5) |
| Rectal tenderness | 6 (5.4) |
RIF: Right iliac fossa
Majority of the patients (24 [72.7%] of the 33 patients) who had perforation presented after 24 h (P = 0.02). All the patients who had a perforated appendicitis had an Alvarado, Kalan, or Al-Fallouji score of >6.
Majority of the patients (105 [94.6%]) patients had a leukocyte count of 4000–11,000 cells/ml and only 42 (37.8%) patients had a shift to the left.
The mean scores of Alvarado, Kalan, and Al-Fallouji modification of Alvarado were 8.05 ± 1.68, 7.7 ± 1.49, and 8.6 ± 1.54, respectively. The sensitivities, specificities, positive and NPVs, and diagnostic accuracies of the various scores are shown in Table 2.
Table 2.
Accuracy of Alvarado and modified Alvarado scores (Kalan and Al-Fallouji)
| Score | Sensitivity | Specificity | PPV | NPV | Accuracy | P |
|---|---|---|---|---|---|---|
| Alvarado | 90.3 | 83.3 | 96.6 | 62.5 | 89.2 | 0.001 |
| Kelan | 90.3 | 83.3 | 96.6 | 62.5 | 89.2 | 0.001 |
| Al-Fallouji | 96.8 | 66.7 | 93.8 | 80 | 91.9 | 0.001 |
Histological analysis was used as gold standard for diagnosis, Accuracy: True positive + true negative/total number of patients. PPV: Positive predictive value, NPV: Negative Predictive value
NAR was 16.2%. A cutoff of 7 was used as a criterion for surgery, using derivative statistical calculations; the NAR so calculated was 3.45% (P < 0.001) on the Alvarado or Kalan scoring systems. However, the calculated NAR was 6.25% if in a similar vein a presumptive cutoff of 7 was used on the Al-Fallouji scoring system.
Receiver operating characteristic curve (ROC) is a plot of the true-positive rate against the false-positive rate for the different possible cutoff points of a diagnostic test. The closer the curve follows the left hand border and then the top border of the ROC space, the more accurate the test. The area under the curve (AUC) is a measure of test accuracy whose score of 0.8 and above depicts an accurate test, whereas 0.5 a worthless test.
The ROC and AUC show that Alvarodo, Kelan, and Al-Falluoji are accurate scores in the preoperative diagnosis of acute appendicitis with an AUC of 0.88, 0.86, and 0.85, respectively [Figure 2].
Figure 2.
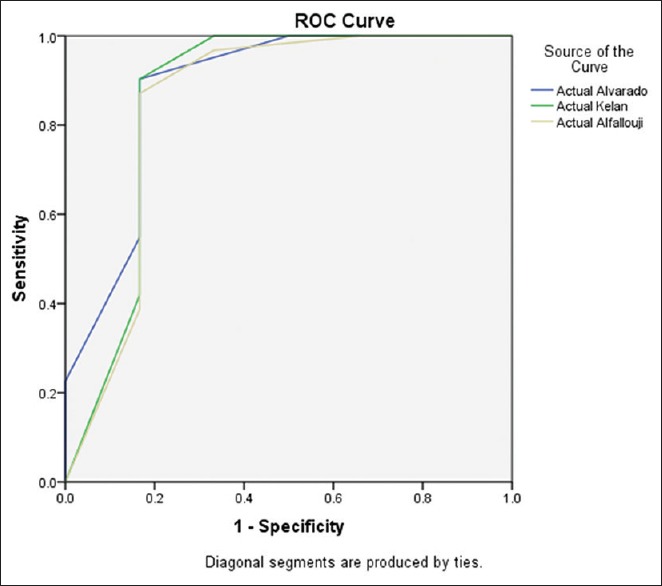
Receiver operating characteristic curve for Alvarado, Kalan, and Al-Fallouji scores
A multivariate analysis of the patients’ age, sex, and duration of symptoms before presentation showed no significant association between these variables and AS [Table 3].
Table 3.
Association between some patient variables and Alvarado score
| Alvarado score | P | ||||
|---|---|---|---|---|---|
| <4 | 5-6 | 7-8 | 9-10 | ||
| Age (years) | |||||
| 16-20 | 3 | 9 | 9 | 9 | 0.140 |
| 21-30 | 3 | 9 | 21 | 39 | |
| 30-40 | 0 | 0 | 3 | 6 | |
| Sex | |||||
| Male | 3 | 12 | 21 | 30 | 0.941 |
| Female | 3 | 6 | 12 | 24 | |
| Duration of symptoms in days | |||||
| <1 | 3 | 15 | 15 | 27 | 0.638 |
| 1-2 | 3 | 0 | 12 | 18 | |
| 3-7 | 0 | 3 | 6 | 3 | |
| >7 | 0 | 0 | 0 | 6 | |
DISCUSSION
Vermiform appendix, though described anatomically to be vestigial, is one of the most important surgical organs in the human body. There are many disease conditions involving this organ among which acute appendicitis is the most common. Appendicitis is an inflammatory condition of the vermiform appendix affecting mainly adolescents and young adults.[13]
The incidence among Africans and Asians has consistently been reported to be low. Reports from Africa put the prevalence around 1%.[14] The finding of this study of yearly hospital-based presentation of 37 patients with a male-to-female ratio of 1.5:1 and a peak age incidence of 20–24 years mirrors what has been reported in a previous hospital-based study from Nigeria.[15,16,17] The age and sex distribution is in agreement with the reported epidemiology of the disease in the United states where the highest incidence of positive appendectomy (appendicitis) is found in persons aged 10–29 years. Males had higher rates of appendicitis than females for all age groups, with an overall rate ratio of 1.4:1.[18]
AS is reported by some workers as the best performing of the clinical scoring systems for acute appendicitis in use and is therefore the most widely used.[4] Kalan et al. modified the original AS by excluding shift to the left of neutrophil maturation.[11] They found that a high MAS was an easy and a satisfactory aid to early diagnosis.[11] Several studies have evaluated and validated the Kalan modification of AS in adult surgical practice.[10,19] Bengezi and Al-Fallouji in their prospective study of 345 consecutive patients admitted with a diagnosis of acute appendicitis introduced another modification of AS; they also omitted the shift to the left of neutrophil maturation but introduced an extra sign (cough test, Rovsing's sign, and rectal tenderness).[12] They concluded that their MAS was simpler, was easier to read and interpret, and was more practical and reliable than the original AS.[12] This modification has been validated in surgical practice.[20,21,22]
In this study using a cutoff of 7 for the AS s, sensitivity, specificity, positive predictive value, NPV, and diagnostic accuracy of 90.3%, 83.3%, 96.6%, 62.2%, and 89.2%, respectively, were similar to the findings for Kalan scores (90.3%, 83.3%, 96.6%, 62.5%, and 89.2%, respectively) and Al-Fallouji scores (96.8%, 66.7%, 93.8%, 80%, and 91.9%, respectively). However, Al-Fallouji showed a slightly higher sensitivity and diagnostic accuracy than the other two scores.
Similar finding was also demonstrated in a Thai study by Phrophrom and Trivej[23] in their comparative study using Bengezi's MAS and the original AS, which showed that the accuracy of the Bengezi MAS was slightly greater than the original Alvarado in the diagnosis of acute appendicitis. Fente and Echem[22] in a similar prospective study evaluated the Bengezi and Al-Fallouji modification of the AS among acute appendicitis patients presenting to a tertiary hospital in South-South Nigeria and also found a high sensitivity of 92.93% and a specificity of 92.93%. Similar findings were reported by studies from other parts of the world.[24]
Kalan et al. in a similar prospective study of 49 patients who were sick enough to warrant surgery for suspected appendicitis found that a high MAS was an easy and a satisfactory aid to the early diagnosis of appendicitis in children and men with sensitivity of 93% and 100%, respectively, but the results were disappointing in women where sensitivity was only 67%.[11] Unlike what was reported by Kalan et al., there was no statistically significant difference in accuracy of this score between female and male patients (P < 0.941) in our study. This could be explained by the fact that we excluded any demonstrable extra appendicular cause of right iliac fossa pain in our study population. It could therefore be postulated that these extra appendicular causes of right iliac fossa pain (demonstrated in this study mainly by abdominal ultrasound) are responsible for poor diagnostic accuracy of AS among females. A well-designed randomized study is needed to confirm this. Kanumba et al.[10] in their study among Tanzanian patients showed that the use of MAS (Kalan) in patients suspected to have acute appendicitis provided a high degree of diagnostic accuracy and can reduce negative appendicectomy rate and complication rates, however they concluded that additional investigations may be required to confirm the diagnosis in the case of atypical diagnosis.
A slightly higher diagnostic accuracy of Al-Fallouji MAS than the AS (91.9% for Al-Fallouji as against 89.2% Alvarado) may be partly explained by the relatively low white blood cell (WBC) count among Africans as compared to Caucasians, which was also demonstrated in this study and therefore the low diagnostic weight of leukocytosis and shift to the left as compared to the high diagnostic weight demonstrated by Alvarado.[8] The lower WBC and neutrophil among African descents has been referred to as ethnic neutropenia.[25] The reason for the difference between Africans and White patients is largely unclear, with many researchers accepting the genetic hypothesis.[25] Mechanisms postulated for the low counts include low release of mature granulocytes, altered bone marrow reserve, and Duffy null polymorphism.[25,26]
The ROC curve for the three scores showed an AUC of 0.88, 0.086, and 0.85 for Alvarado, Kalan, and Al-Fallouji, respectively. This further confirms the diagnostic accuracy of all these scores. This is similar to what was reported by previous workers.[27,28] This is similar to the findings of an Iranian study by Nasiri et al. who studied 75 patients who had appendicectomy over a 9-month period and also found an AUC of 0.837.[27]
Histological analysis showed a NAR of 16.2%, which is similar to a previous report from our hospital by Mungadi et al.[16] Using an AS cutoff of 7 as a criterion for appendicectomy, the NAR will reduce to 3.45% (P < 0.001). The reduction in NAR is same if the same cutoff is applied to Kelan and 6.25% for Al-Fallouji. This is desirable to prevent unnecessary surgeries and sequel of morbidities and economic burden on our patients. This will also help reduce the burden on the already-weak health-care delivery system. Similar reduction in NAR was also demonstrated by Fente and Echem in their study among patients presenting to a tertiary hospital in South-South Nigeria.[22]
The rate of perforation in our study was 29.7%, which is comparable to previous studies carried out in Northern Nigeria.[17,29] A finding in this study of a significant statistical relationship between perforated appendix and all the three scores (P = 0.0001, P = 0.002, and P = 0.0001) for Alvarado, Kalan, and Al-Fallouji, respectively (with no patient with perforated appendix having a score of <7 regardless of the scoring system), further confirms the usefulness of all the three scores in the preoperative diagnosis in our setting.
CONCLUSION
MASs (Kalan and Al-Fallouji) have comparably high sensitivity, specificity, and good diagnostic accuracy as the AS among our patients. These modifications can, therefore, be used to circumvent the difficulty of obtaining the result of shift to the left in neutrophils. Any of the three scores is useful as an adjunct in the preoperative diagnosis of acute appendicitis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Fitz RH. Perforating inflammation of the vermiform appendix with special reference to it's early diagnosis and to treatment. Am J Med Sci. 1886;92:32–46. [Google Scholar]
- 2.Liu CD, McFadden DW. Acute abdomen and appendix. In: Greenfield LJ, Mulholland MW, editors. Surgery: Scientific principles and practice. 2nd. Philadelphia: Lippincott-Raven; 1997. pp. 1246–61. [Google Scholar]
- 3.Poole GV. Appendicitis. The diagnostic challenge continues. Am Surg. 1988;54:609–12. [PubMed] [Google Scholar]
- 4.Ohmann C, Yang Q, Franke C. Diagnostic scores for acute appendicitis. Abdominal Pain Study Group. Eur J Surg. 1995;161:273–81. [PubMed] [Google Scholar]
- 5.Horman J, Rasmussen OO. Aids in the diagnosis of acute appendicitis. Br J Surg. 1989;46:774–90. doi: 10.1002/bjs.1800760803. [DOI] [PubMed] [Google Scholar]
- 6.Gilmore OJ, Jones D, Bang Q. Appendicitis and mimicking conditions. Lancet. 1975;11:421–4. doi: 10.1016/s0140-6736(75)90841-7. [DOI] [PubMed] [Google Scholar]
- 7.Humes DJ, Simpson J. Acute appendicitis. BMJ. 2006;333:530–4. doi: 10.1136/bmj.38940.664363.AE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Alvarado A. A practical score for the early diagnosis of acute appendicitis. Ann Emerg Med. 1986;15:557–64. doi: 10.1016/s0196-0644(86)80993-3. [DOI] [PubMed] [Google Scholar]
- 9.Fenyö G, Lindberg G, Blind P, Enochsson L, Oberg A. Diagnostic decision support in suspected acute appendicitis: Validation of a simplified scoring system. Eur J Surg. 1997;163:831–8. [PubMed] [Google Scholar]
- 10.Kanumba ES, Mabula JB, Rambau P, Chalya PL. Modified Alvarado scoring system as a diagnostic tool for acute appendicitis at Bugando Medical Centre, Mwanza, Tanzania. BMC Surg. 2011;11:4. doi: 10.1186/1471-2482-11-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kalan M, Talbot D, Cunliffe WJ, Rich AJ. Evaluation of the modified Alvarado score in the diagnosis of acute appendicitis: a prospective study. Ann R Coll Surg Engl. 1994;76:418–9. [PMC free article] [PubMed] [Google Scholar]
- 12.Macklin CP, Radcliffe GS, Merei JM, Stringer MD. A prospective evaluation of the modified Alvarado score for acute appendicitis in children. Ann R Coll Surg Engl. 1997;79:203–5. [PMC free article] [PubMed] [Google Scholar]
- 13.Marcovitch H. Dictionary. In: Marcovitch H, editor. Black Medical Dictionary. 41st. A and C Publishers; 2005. [Google Scholar]
- 14.Madiba TE, Haffejee AA, Mbete DL, Chaithram H, John J. Appendicitis among African patients at King Edward VIII Hospital, Durban, South Africa: A review. East Afr Med J. 1998;75:81–4. [PubMed] [Google Scholar]
- 15.Oguntola AS, Adeoti ML, Oyemolade TA. Appendicitis: Trends in incidence, age, sex, and seasonal variations in South-Western Nigeria. Ann Afr Med. 2010;9:213–7. doi: 10.4103/1596-3519.70956. [DOI] [PubMed] [Google Scholar]
- 16.Mungadi IA, Jabo BA, Agwu NP. A review of appendicectomy in Sokoto, North-western Nigeria. Niger J Med. 2004;13:240–3. [PubMed] [Google Scholar]
- 17.Regan FW. Diagnosing ruptured appendicitis pre operatively in paediatric patients. J Am Coll Surg. 2009;208:819–25. doi: 10.1016/j.jamcollsurg.2009.01.029. [DOI] [PubMed] [Google Scholar]
- 18.Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990;132:910–25. doi: 10.1093/oxfordjournals.aje.a115734. [DOI] [PubMed] [Google Scholar]
- 19.Shah J, Pukar M, Mishra V, Mewada SG. Modified Alvarado score in management of acute appendicitis. Int J Res Health Sci. 2014;2:570–6. [Google Scholar]
- 20.Malik KA, Sheikh MR. Role of modified Alvarado score in acute appendicitis. Pak J Surg. 2007;23:251–4. [Google Scholar]
- 21.Talukder DM, Siddiq AK. Modified Alvarado scoring system in the diagnosis of acute appendicitis. JAFMC Bangladesh. 2009;5:18–20. [Google Scholar]
- 22.Fente BG, Echem RC. Prospective evaluation of the Bengezi and Al-Fallouji modified Alvarado score for presumptive accurate diagnosis of acute appendicitis in University of Port Harcourt Teaching Hospital, Port Harcourt. Niger J Med. 2009;18:398–401. doi: 10.4314/njm.v18i4.51251. [DOI] [PubMed] [Google Scholar]
- 23.Phrophrom J, Trivej T. The modified Alvarado score versus the Alvarado score for the diagnosis of acute appendicitis. Thai J Surg. 2005;26:69–72. [Google Scholar]
- 24.Rithin PS, Agarwal A, Budigi B. Evaluation of modified Alvarado scoring system in acute appendicitis at Vydehi Institute of Medical Sciences and Research Centre, Bangalore, Karnataka, India. Int Surg J. 2017;4:218–22. [Google Scholar]
- 25.Hershman D, Weinberg M, Rosner Z, Alexis K, Tiersten A, Grann VR, et al. Ethnic neutropenia and treatment delay in African American women undergoing chemotherapy for early-stage breast cancer. J Natl Cancer Inst. 2003;95:1545–8. doi: 10.1093/jnci/djg073. [DOI] [PubMed] [Google Scholar]
- 26.Reich D, Nalls MA, Kao WHL, Akylbekova EL, Tandon A. Reduced neutrophil count in people of African descent is due to a regulatory variant in the Duffy antigen receptor for Chemokines gene. PLOS Genet. 2009;5:e1000360. doi: 10.1371/journal.pgen.1000360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Nasiri S, Mohebbi F, Sodagari N, Hedayat A. Diagnostic values of ultrasound and the Modified Alvarado Scoring System in acute appendicitis. Int J Emerg Med. 2012;5:26. doi: 10.1186/1865-1380-5-26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Sun JS, Noh HW, Min YG, Lee JH, Kim JK, Park KJ, et al. Receiver operating characteristic analysis of the diagnostic performance of a computed tomographic examination and the Alvarado score for diagnosing acute appendicitis: emphasis on age and sex of the patients. J Comput Assist Tomogr. 2008;32:386–91. doi: 10.1097/RCT.0b013e31812e4b54. [DOI] [PubMed] [Google Scholar]
- 29.Patnalk VV, Singla, Rajan K, Bansal VK. Surgical incisions- Their anatomical basis. Anat Soc India. 2001;50:170–8. [Google Scholar]