

Abstract
Individual differences in eating behaviors have been associated with obesity among young children. Food responsiveness tends to be positively associated with childhood obesity, satiety responsiveness tends to show a negative association, and the results for emotional overeating are mixed. Previous studies in this area, however, have generally employed cross-sectional designs. The purpose of the present study was to examine, in a sample of Hispanic children from families with low-income levels, the degree to which individual differences in child eating behaviors in the preschool years predicted changes in child weight into the early elementary school years. Parent/child dyads (n = 113) were seen on three separate occasions starting when the children were 4-years-old and ending when they were 8-years-old. Separate cross-lag panel analyses were conducted for food responsiveness, satiety responsiveness, and emotional overeating in examining the relationships between child eating behavior and child weight status over time. Consistent with previous cross-sectional studies, at all three time points, food responsiveness was positively associated with concurrent child weight status and satiety responsiveness showed a negative relationship. No concurrent relationship with child weight status was found for emotional overeating until the third time point when children were eight-years-old. Only two cross-lag associations between child eating behavior and child weight status were significant: emotional overeating and child weight status showed a bidirectional relationship between the second and third time points. Future longitudinal studies should examine these relationships in other populations.
Keywords: Hispanic preschoolers, child eating self-regulation, child weight status, child eating behaviors
1.1. Introduction
It is well-documented that individual differences in children’s eating behavior are associated with childhood obesity. As described in several review papers (e.g., French, Epstein, Jeffery, Blundell, & Wardle, 2012; Russell & Russell, in press), children with obesity show greater enjoyment of food (as assessed by measures of food liking and the relative reinforcement value of food) and poorer eating self-regulation (as assessed by eating disinhibition and eating in the absence of hunger). These same reviews show that eating behaviors negatively associated with childhood obesity include food avoidance/fussiness and eating self-regulation (as assessed by satiety responsiveness and caloric compensation). However, despite considerable research in this area, most studies examining children’s eating behavior and childhood obesity have been cross-sectional and have not examined eating behaviors as predictors of changes in children’s weight status over time (French et al., 2012).
To address the research gap, this research evaluated the extent to which individual differences in children’s eating behaviors in the preschool years predicted changes in children’s weight status into the early elementary school years in a sample of Hispanic children from low-income families. We chose to study this population because children from low-income families show the highest rates of childhood obesity (Yeaton, Shah, & Moss, 2018), and Hispanic children show higher rates of obesity than other ethnic groups (Ogden et al., 2018; Yeaton et al., 2018). We focused on the preschool years because this is an important period for the development of children’s eating behaviors—particularly the development of food preferences, mealtime routines, and the self-regulation of caloric intake (Birch & Fisher, 1998).
Because we were interested in the self-regulation of eating, we focused on three eating dimensions related to the self-regulation of eating assessed using the Children’s Eating Behavior Questionnaire (CEBQ) (Wardle, Guthrie, Sanderson, & Rapoport, 2001): food responsiveness, satiety responsiveness, and emotional overeating. Children who are high in food responsiveness tend to eat in response to the sight and smell of food and often eat in the absence of hunger. Numerous cross-sectional studies of young children show that children with obesity typically show higher levels of food responsiveness compared to healthy weight children (French et al., 2012). Children who are high on satiety responsiveness, in contrast, tend to stop eating in response to internal cues of fullness and often will not finish a meal if they have eaten something just beforehand. As one might expect, satiety responsiveness is typically negatively associated with children’s weight status in early childhood (French et al., 2012). Finally, emotional overeating is the tendency to eat more when experiencing boredom or negative emotions. Cross-sectional research on emotional eating during early childhood is mixed, with some studies finding a positive association with childhood obesity (Leung et al., 2016; Mallan, Daniels, & Nicholson, 2017; Spence, Carson, Casey, & Boule, 2011), some studies finding no significant relationship (Derks et al., 2018; Jansen et al., 2012; Quah et al., 2017), one study finding a positive relationship only for boys (Lipowska, Lipowski, Jurek, Jankowska, & Pawlicka, 2018), and one study finding a positive relationship only in the presence of an uninvolved parental feeding style (Hankey, Williams, & Dev, 2016).
Fewer studies have examined the degree to which eating behaviors assessed by the CEBQ in the preschool years predict changes in children’s weight status over time. In the literature review conducted for this paper, we found one longitudinal study that examined fussy eating (assessed by the CEBQ) as a predictor of subsequent child weight status (de Barse et al., 2015), and four longitudinal studies examining one or more of the three CEBQ scales considered here: satiety responsiveness, food responsiveness, and emotional overeating (Derks et al., 2018; Gregory, Paxton, & Brozovic, 2010; Leung et al., 2016; Mallan, Nambiar, Magarey, & Daniels, 2014). All four studies examined the degree to which food responsiveness predicted changes in child weight status over time and none found a significant relationship. Three of these studies examined satiety responsiveness as a predictor and only one (a small sample study of toddlers, n = 37) found that satiety responsiveness negatively was associated with child weight status over time (Mallan et al., 2014). The other two studies with much larger samples of four-year-olds (Dreks et al., 2018, n = 331; Lueng et al., 2016, n = 379) found that satiety responsiveness did not predict changes in child weight status over time. Finally, only two studies examined emotional overeating: one found significant prediction of child weight status (a positive relationship) between the ages of 4 and 10 (Derks et al., 2018) and the other found no significant relationship (Lueng et al., 2016).
Although most studies have focused on examining the degree to which child eating behavior predicts child weight status over time, one study examined the bidirectional relationships between child eating behavior and child weight status over time. Derks and colleagues (2018), in a longitudinal study of children from 4 to 10 years, found that for all three of the constructs of interest here (emotional overeating, food responsiveness, and satiety responsiveness), age and sex adjusted child BMI SD scores predicted later child eating behavior (positive relationships for emotional overeating and food responsiveness and a negative relationship for satiety responsiveness), but as mentioned above, only emotional overeating significantly predicted changes in child weight status over time. They argued that the bidirectional relationship between emotional overeating and child weight status may reflect the impact of biological mechanisms contributing to the impact of BMI on food consumption (e.g., increased energy balance set point and decreased leptin sensitivity) as well as learned responses that result in overeating in response to negative emotions. They argue that such processes can set up a “vicious cycle” between weight and eating practices that could contribute to and exacerbate the problem of childhood obesity. Although not mentioned by these authors, an additional factor that might contribute to this vicious cycle are negative emotions resulting from the negative stigma associated with higher child weight.
Given the limited number of longitudinal studies in this area, and the fact that no study has examined the bidirectional relationships between child eating behavior and child weight status in a sample of Hispanic children from families with low-incomes (a population at high risk for childhood obesity), the purpose of this study was to examine, using cross-lagged panel analyses, the associations between children’s eating behavior and children’s weight status as children transition from the preschool to the early elementary school years. Similar to the approach of Derks and colleagues (2018), the use of cross-lag panel analyses allowed us to examine both the degree to which child eating behavior predicted changes in children’s weight status over time, as well as examine the degree to which children’s weight status predicted changes in child eating behavior over time. Such work is needed to determine whether child eating behaviors play a causal role in the development of childhood obesity or simply reflect the behavior of children with obesity. Based on the results of the Derks et al. (2018) study, we predicted that child weight status would be associated positively with food responsiveness and emotional overeating over time, and that child weight status would be negatively associated with satiety responsiveness over time. Also, consistent with Derks et al. (2018), we predicted that of the three feeding patterns studied here, only emotional overeating would predict changes in child weight status over time.
1.2. Methods
1.2.1. Participants
A total of 113 Hispanic parent-child dyads participated. These participants were part of a larger longitudinal study of maternal feeding, children’s self-regulation, and child weight status (Hughes, Power, O’Connor, & Fisher, 2015; Hughes, Power, O’Connor, Fisher, & Chen, 2016). Parents for the larger study were recruited through Head Start centers and flyers sent home with the children. The person primarily responsible for feeding when the child was not at Head Start was targeted along with their Head Start preschooler. Caregivers were screened for eligibility on the phone and invited to the project laboratory. To be eligible, caregivers had to be of Hispanic origin and have a child in the study age range (4 to 5 years) attending Head Start. Children with extensive dietary restrictions such as those on special diets due to diabetes or major food allergies were excluded from the study because tasks in the larger study involved consumption of common foods. To further ensure that children were protected, a second screener was completed by the parent prior to involvement in the food tasks. Consent forms were offered in English and Spanish, explained to caregivers in their language of choice, and signed prior to participating in the study. Seventy-seven percent of the caregivers consented in Spanish. All caregivers recruited for this study were mothers except for two grandmothers (hereafter referred to as mothers). Mothers received $90 for participating in the two day study at time one ($25 for day one; $65 for day two), $185 for participating at time two ($45 for day one; $140 for day 2), and $35 for participating at the third time point. The study was reviewed and approved by the Institutional Review Board at Baylor College of Medicine.
1.2.2. Procedures
As part of the larger study, mothers completed the CEBQ and their children’s height and weight were assessed at three time points. The first two time points were 18 months apart, with data collected on mothers and children in a laboratory setting. As described in more detail in the results section, there was considerable variability in the timing of the third time point—this interval ranged from one to three years following time point 2. Data at the third time point were collected during home or Head Start visits.
1.2.3. Measures
1.2.3.1. Children’s Eating Behavior Questionnaire (CEBQ).
The three subscales of the CEBQ related to child eating self-regulation were used for this study: satiety responsiveness, food responsiveness, and emotional overeating (Wardle et al., 2001). Responses were scored on a 1 to 5 point scale (never to always). Example items for these subscales are: satiety responsiveness (“My child cannot eat a meal if s/he has had a snack just before,” “My child gets full before his/her meal is finished”), food responsiveness (“Even if my child is full up s/he finds room to eat his/her favorite food,” “If given the chance, my child would always have food in his/her mouth”), emotional overeating (“My child eats more when worried,” “My child eats more when annoyed”). The factor structure, test-retest reliability, and internal consistency of the CEBQ was established in a sample of predominately white families in the United Kingdom (Wardle et al., 2001). These subscales have been used successfully in a low-income sample of African-American and Hispanic mothers of preschoolers (Morrison, Power, Nicklas, & Hughes, 2013).
Mothers completed the CEBQ in English (23%) or Spanish (77%) depending upon their language preference. The Spanish version of the CEBQ used in this study was the same as the one used across multiple separate studies (Morrison et al., 2013; Frankel et al., 2014; Hughes et al., 2015; Power, Johnson, Beck, Martinez, & Hughes, 2019). The Spanish version of the CEBQ was translated and back-translated following common practices (see Hughes et al., 2006 for a review of translation methods). Coefficient alphas were adequate in the current sample (0.68 for satiety responsiveness, 0.80 for food responsiveness, and 0.70 for emotional overeating). Higher scores on satiety responsiveness reflected higher child eating self-regulation; higher scores on food responsiveness and emotional overeating reflected lower child eating self-regulation.
1.2.3.2. Anthropometries.
Child and mother height and weight measurements were taken by trained staff following procedures described by Lohman, Roche, and Martorell (1988). The same procedures were used for the lab and the home visits. Research assistants collecting data in the home were trained following the same protocols as staff collecting data in the lab. The same electronic weight scale (Health-o-Meter model 752KL) and stadiometer (Seca model 214) used in the lab visits were used in the home visits. Children and mothers were dressed in light clothing and asked to remove their shoes. Height and weight were measured in duplicate to assure accuracy; the two scores were averaged. For children, scores were converted to age- and sex-specific BMI z-scores and percentiles using the revised 2000 growth charts from the Centers for Disease Control and Prevention (Kuczmarski, Ogden, & Guo, 2002). Children were assigned to three weight status categories based on their age- and sex specific percentiles: with healthy weight (< 85th percentile), with overweight (85th to < 95th percentile), and with obesity (≥ 95th percentile). Mothers were assigned to weight status categories using the CDC guidelines (Centers for Disease control and Prevention, 2017): with healthy weight: BMI < 25; with overweight: BMI ≥ 25 and < 30; with obesity: BMI ≥ 30.
1.2.4. Statistical Analyses
Statistics were run using the Statistical Package for the Social Sciences (SPSS, Version 20.0, Chicago, IL). Descriptive statistics were generated for all variables and examined to evaluate distributions. Bivariate correlations between the study variables were examined as well. To identify covariates, the demographic variables in Table 1 were correlated with child BMI z-scores at the three time points. To identify changes in the three CEBQ subscales over time, a repeated measures, multivariate analysis of variance was run with the three CEBQ subscales serving as the dependent variable. The independent variable was time (three levels). Follow-up univariate analyses of variance and paired t-tests were run to follow up any significant multivariate effects.
Table 1.
Characteristics of Study Sample at Time 1
| n = 113 | |
|---|---|
| Parent sex - female | 100.0% |
| Child sex - female | 47.6% |
| Mother age, mean in years (SD) | 31.48 (6.49) |
| Child age, mean in months (SD) | 57.4 (5.2) |
| Education of parent | |
| High school diploma or less | 64.7% |
| Some college or more | 35.3% |
| Employment status, currently employed | 23.5% |
| Marital status | |
| Married | 59.3% |
| Never Married | 14.4% |
| Widowed, separated, divorced | 26.3% |
| Immigrant status of Mother | |
| Born in the U.S. | 21.4% |
| Born in Mexico | 60.4% |
| Born in Central America | 16.6% |
| Born in another country | 1.6% |
| Mother BMI categories | |
| With Healthy Weight (< 25) | 16.1% |
| With Overweight (≥ 25 and < 30) | 30.1% |
| With Obesity (≥ 30) | 53.8% |
| Child BMI categories | |
| With Healthy Weight (<85th percentile) | 52.9% |
| With Overweight (85th to <95th percentile) | 20.9% |
| With Obesity (≥95th percentile) | 26.2% |
The main study questions were tested through three cross-lag panel analyses (Martens & Haase, 2006): separate analyses for the three CEBQ subscales (satiety responsiveness, food responsiveness, and emotional eating). The models involved examining all adjacent paths between the three time points (1, 2, and 3). Covariates identified in the correlational analyses were included in the models. Structural equation analyses were conducted using AMOS (version 24). Parameters were estimated using maximum likelihood methods. As is standard practice in cross-lagged panel models, the errors of the constructs at the second and third time points were allowed to correlate (Martens & Haase, 2006). Model fit was determined by examining the chi square (n.s.), ratio of the chi square to the degrees of freedom (< 3.0), the CFI (≥ .95), and the RMSEA (≤ .08) (Hooper, Couglan, & Mullen, 2008; MacCallum, Browne, & Sugawara, 1996).
1.3. Results
The study was originally designed to have two time points eighteen months apart, with mothers visiting the research center two times at each time point. However, since this was a relatively mobile, hard-to-track, low-income population, often with significant transportation obstacles, many appointments had to be postponed or rescheduled, resulting in variability in the timing of the second visit. Eighty seven percent of the mothers were seen between 17 and 20 months after the first visit, 11% were seen at 21 to 23 months, and 1% seen at 24 or 25 months. The decision to add a third time point was made after most of the data from the first two time points had been collected. We made this decision because we did not see as much change in children’s weight status between the first two time points as expected. Although the original plan was to conduct this visit 18 months after the second visit, this was not possible for about half of the mothers because the 18 month interval had already passed. Moreover, because our funding was ending, we needed to collect some time point 3 data early. Therefore, the distribution of timing for the third visit was bimodal, with about half of the visits occurring between 16 and 22 months after the second visit and about one quarter between 31 and 33 months. The length of time between the two visits ranged from 11 to 37 months, with a mean of 23.60 months (SD = 6.52). Given this variability in the timing of the data collection, we refer to the three time points below with regard to their number (first, second, or third) or in reference to the mean child age at each visit: visit 1, mean = 4.74 years, SD = 0.43; visit 2, mean = 6.34 years, SD = 0.50 years; visit 3, mean = 8.30 years, SD = 0.43.
Of the 187 mothers and their preschool child who participated in two laboratory visits at the first time point, 147 mothers returned for two laboratory visits at time two, and 130 completed anthropomorphic and questionnaire assessments at time 3. Mother-child dyads used in this paper were those 113 dyads who had data on child BMI and maternal ratings of child eating behavior (CEBQ) at all three time points. Characteristics of the 113 dyads at the first time point are presented in Table 1. Comparison of dyads who had data at all three time points to those who did not revealed only one significant difference on the demographic variables listed in Table 1 at the first time point: mothers who had data at all three time points were more likely to be born outside of the U.S. (85%) than mothers who did not (69%), X2(1) = 6.84, p < .01.
1.3.1. Bivariate Correlations
Preliminary analyses showed that three of the demographic variables in Table 1 were correlated with child BMI z-scores at one or more time points: mother BMI (r = .35, p < .01, to r = 43, p < .01), maternal marital status (mother married versus other, r = −.10, n.s., to r = .−.22, p < .01), and maternal age (r = .11, n.s., to r = .12, p < .09). The negative correlation for marital status indicates that children of married mothers had lower BMI z-scores than children of other mothers. To allow for a more sensitive test of the hypotheses, these three variables were included as covariates in the cross-lag panel analyses. Finally, because the time interval between the second and third time point varied so widely, we reran these analyses adding time interval as a covariate as well. The time interval covariate was not a significant predicator of time 3 BMI z-scores in any of these analyses, nor did the addition of this control variable change the pattern of results. Therefore, we did not include time interval as a covariate in the final models.
As described in Table 2, all three child eating subscales showed moderately high levels of stability over time. Over adjacent time points, the mean correlations across time were satiety responsiveness (mean r = .56), food responsiveness (mean r = .60), and emotional overeating (mean r = .48). As expected, across non-adjacent time points (i.e., time 1 to time 3), these values were slightly lower, r’s = .44, .36, and .29 respectively. Within time points, the correlations between food responsiveness and emotional overeating were moderately high (mean r = .57). Satiety responsiveness, in contrast, showed lower within-time point correlations with food responsiveness (r’s ranged from −.10 to −.29) and was not significantly correlated with emotional overeating (r’s ranged from .00 to.15).
Table 2.
Intercorrelations of Child Eating Behavior Subscales and Child BMI z Scores across All Three Time Points
| Time 1 | Time 2 | Time 3 | Time 1 | Time 2 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| SR | FR | EOE | SR | FR | EOE | SR | FR | EOE | Child BMIz | ||
| Time 1 | |||||||||||
| FR | − 29** | ||||||||||
| EOE | .00 | .58** | |||||||||
| Time 2 | |||||||||||
| SR | .61** | −.13 | −.01 | ||||||||
| FR | −.14 | .52** | .42** | −.20* | |||||||
| EOE | .07 | .42** | .47** | .15 | .48** | ||||||
| Time 3 | |||||||||||
| SR | .44** | .03 | −.02 | .51** | −.06 | .13 | |||||
| FR | .00 | .36** | .24** | −.12 | .67** | .40** | −.10 | ||||
| EOE | .08 | .18* | .29** | −.01 | .37** | .50** | .01 | .66** | |||
| Time 1 | −.22** | .18* | .06 | −.21* | .12 | .08 | .13 | .11 | .22* | ||
| Child BMIz | |||||||||||
| Time 2 | −.17* | .13 | .08 | −.24** | .23** | .12 | .23* | .28** | .32** | .93** | |
| Child BMIz | |||||||||||
| Time 3 | −.13 | .12 | .11 | −.23* | .26** | .20* | .20* | .25** | .36** | .83** | .94** |
| Child BMIz | |||||||||||
SR = Satiety Responsiveness, FR = Food Responsiveness, EOE = Emotional Overeating,
p < .05
p < .01
Correlations of child eating behavior and child BMI z were significant within the three time points (4, 6, and 8 years) for satiety responsiveness (mean r = −.22) and food responsiveness (mean r = .22). Emotional overeating was not significantly correlated with child BMI z-scores at the first two time points (r’s = .06 and .12 respectively). However, it was positively correlated with child BMI z-scores at the third time point (r = .36, p < .01). Finally, BMI z-scores showed very high levels of stability over time (correlations between adjacent time points of .93 and .94 and a correlation between the first and third time point of .83).
1.3.2. Mean Differences in Child Eating Behavior Over Time
The multivariate effect of time was significant, F(6, 108) = 5.78, p < .001, eta2 = .24. As shown in Table 3, all three univariate ANOVAs were significant. Follow-up paired t-tests showed that satiety responsiveness decreased between times 1 and 2, and that both food responsiveness and emotional overeating increased between times 2 and 3 (see Table 3 and Figure 1).
Table 3.
Mean Differences in Child Eating Behavior Over Time
| CEBQ Subscale | Univariate ANOVAs F(2,226) | Eta2 | Time 1 Mean (SD) | Time 2 Mean (SD) | Time 3 Mean (SD) |
|---|---|---|---|---|---|
| Satiety Responsiveness | 10.97** | .09 | 2.88a (0.67) | 2.69b (0.64) | 2.61b (0.63) |
| Food Responsiveness | 5.40** | .05 | 2.24b (0.82) | 2.20b (0.77) | 2.43a (0.83) |
| Emotional Overeating | 3.52* | .03 | 1.74b (0.64) | 1.77b (0.58) | 1.90a (0.71) |
Note: Means with different subscripts were significantly different from one another (p < .05)
Figure 1.
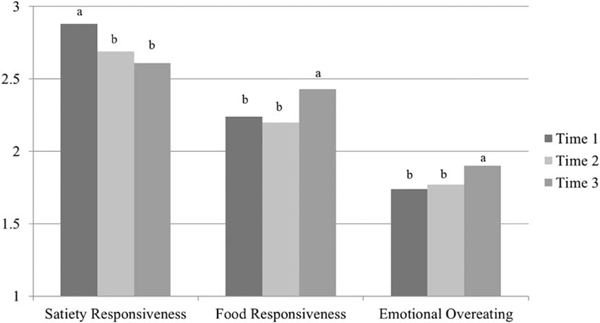
Child Eating Behaviors Over Time
Note: Means with different subscripts were significantly different from one another (p < .05)
In the cross-lagged panel analyses, the models for all three CEBQ subscales showed acceptable fit: satiety responsiveness, X2(10) = 15.85, p = .10, X2/df = 1.58, CFI = .99, RMSEA = .072; food responsiveness, X2(10) = 17.75, p = .06, X2/df = 1.78, CFI = .99, RMSEA = .082; emotional overeating, X2(10) = 14.00, p = .17, X2/df = 1.40, CFI = .99, RMSEA = .059. As shown in Figure 2, for emotional overeating, all of the autoregressive paths and both of the cross-lag paths from time 2 to time 3 were significant, indicating a bidirectional relationship between emotional overeating and child BMI z over time. Examination of the path coefficients for both satiety responsiveness and food responsiveness showed that only the autoregressive paths were significant—i.e., the paths between the adjacent time points for the CEBQ subscales and the paths between the adjacent time points for child BMI z-scores. No cross-lag paths (i.e., CEBQ subscales to child BMI z-scores or vice versa) were significant for these two variables.
Figure 2.
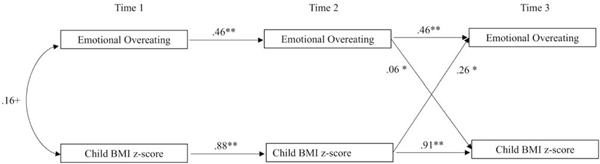
Cross-Lag Panel Analysis: Emotional Overeating and Child BMI z-scores
+p < .10, *p < .05, **p < .01
Note: Analysis controlled for effects of mother BMI, mother marital status, and mother age on eating behavior and child BMI z (not shown). The time two and time three errors were allowed to correlate (also not shown—see text). The path coefficients in the figure are standardized estimates.
1.4. Discussion
The current findings replicate and extend the results of Derks and associates’ (2018) study of middle-class Dutch children by demonstrating, in a population at high risk for obesity in the U.S. (i.e., Hispanic children from families with low incomes), that emotional overeating in early childhood was the only early eating dimension that significantly predicted obesity in the elementary school years. As also demonstrated by Derks et al. (2018), the longitudinal relationship between emotional overeating and child weight status in the current study was bidirectional, with early child weight status also predicting changes in emotional overeating over time. Finally, in both the current study and in research by others (Derks et al., 2018; Jansen et al., 2012; Quah et al., 2017), there was no concurrent relationship between emotional overeating and child weight status in the preschool years. This contrasts with the positive relationship typically reported in the elementary school years, a finding replicated in the current study (e.g., Demir & Bektas, 2017; dos Passos, Gigante, Maciel & Matijasevich, 2015; Sanlier, Arslan, Buyukgenc, & Toka, 2018; Santos et al., 2011; Viana, Sinde, & Saxton, 2008; Webber, Hill, Saxton, Van Jaarsveld, & Wardle, 2009).
Emotional overeating might not play a role in the development of childhood obesity until later ages because young children’s natural response to stress is undereating rather than overeating (van Strien & Ouwens, 2007) and it might take some time before the learned response to eat in times of stress develops in some children. This is supported by the results of a twin study that found that individual differences in emotional over- and under-eating were accounted for primarily by environmental factors (Herle, Fildes, Steinsbekk, Rijsdijk, & Llewellyn, 2017), and by several studies showing that food as a reward and emotional feeding practices predict the development of emotional eating in young children (Farrow, Haycraft, & Blissett, 2015; Powell, Frankel, & Hernandez, 2017; Steinsbekk, Barker, Llewellyn, Fildes, & Wichstrøm, 2018).
The bidirectional relationship between child weight status and emotional overeating likely reflect the operation of both biological and environmental processes. Emotional overeating likely influences child weight status through increased caloric consumption due to stress. The factors accounting for the prediction of later emotional eating from earlier child weight status are less clear. These could be the result of biological changes due to increased child weight status (e.g. energy balance set-point and leptin sensitivity) leading to greater consumption as argued by Derks et al. (2018). They could also be due to environmental factors not considered here, such as the possibility that calorie dense snack foods are more available or accessible in homes of children with obesity, that children with obesity experience greater levels of stress in the home, or that parental perceptions of emotional eating are influenced by child weight status and might lead to parental feeding practices (such as using food as a reward or emotional feeding practices) that subsequently contribute to children’s emotional eating (Farrow et al., 2015; Powell et al., 2017; Steinsbekk et al., 2018).
The current study also replicates the bidirectional relationship between emotional overeating and children’s weight status in low-income, Latino sample. Children and adolescents in this population often show emotional distress in response to the stresses they face—e.g., acculturative stress, discrimination, and stresses associated with low-income status (Aber, Bennett, & Conley, 1997; Park, Wang, Williams, & Alegria, 2018; Suarez-Morales, Dillon, & Szapocznik, 2007). Therefore, one possible factor that might contribute to the higher childhood obesity rates in this population (Ogden et al., 2018) may be higher levels of emotional overeating in response to these stresses.
The current results replicate the findings of the three previous longitudinal studies of preschool children that showed that, despite concurrent relationships with weight status, neither food responsiveness nor satiety responsiveness predicted changes in young children’s weight over time (Derks et al., 2018; Gregory et al., 2010; Leung et al., 2016). The current results, however, did not replicate Derks and colleagues’ (2018) finding that child weight status at age four predicted changes in food responsiveness and satiety responsiveness over time. Several differences between the two studies might account for these results: Derks et al. (2018) employed a much larger sample (n = 331), studied a different population (middle class Dutch children versus low-income Hispanic children), and followed children up at a later age (10 versus 8 years).
The changes in eating behavior over time replicate and extend the literature as well. First, consistent with both questionnaire (e.g., Ascroft, Semmler, Carnell, van Jaarsveld, & Wardle, 2008) and behavioral task (e.g., Fisher & Birch, 2002; Johnson & Taylor-Holloway, 2006) studies, with increasing age, children showed less self-regulation of eating. Specifically, satiety responsiveness decreased between the first two time points and both food responsiveness and emotional overeating increased between the second and third time points. These developmental changes indicate that obesity prevention programs that focus on the self-regulation of children’s eating might best be implemented for children in the infancy or the early childhood years (Spill et al., 2019).
The results of this study should be considered in light of its limitations. The current study focused on Latina mothers with low incomes and their children; therefore, the findings cannot be generalized to other ethnic and income groups. The use of a convenience sample also limited our ability to generalize to a larger population of mothers. Moreover, the relatively low coefficient alpha for the satiety responsiveness subscale of the CEBQ (.68) might have worked against finding significant effects in some of the analyses involving this variable. Finally, individual differences in child eating behavior were only assessed through maternal reports—future studies would benefit from using multiple methods and measures to assess children’s eating behavior. Despite these limitations, the study also has multiple strengths, including the study of a sample at high risk for childhood obesity; the use of a well-known, and well-validated questionnaire to assess children’s eating behavior (i.e., the CEBQ); the longitudinal design; and the use of cross-lagged panel analyses.
In conclusion, the current study replicates the findings of longitudinal studies of the CEBQ and child weight status in a sample of children from Hispanic families with low incomes. It confirms the findings of Derks and associates (2018) who demonstrated the important role of emotional eating in predicting later childhood weight status, despite the lack of a concurrent relationship in the preschool years. Future longitudinal studies should examine these relationships in other populations, with larger samples, and using multiple measures and methods to assess emotional eating (e.g., questionnaires, laboratory assessments). Such studies should also examine how environmental factors interact with individual differences in early eating behavior in contributing to the development of childhood obesity in the elementary school years. Such knowledge could help inform obesity prevention efforts in this population. Given the findings of the present study concerning emotional eating, one component of effective prevention programs might be to provide children with alternative strategies for coping with minor and major life stresses in order to reduce the level of emotional eating and thereby reduce their obesity risk.
Highlights.
Cross-lag analyses to examine child eating behaviors and weight longitudinally.
Food responsiveness positively associated with concurrent child weight.
Satiety responsiveness negatively associated with concurrent child weight.
Emotional overeating showed no concurrent association with child weight.
Emotional overeating and child weight showed a later bidirectional relationship.
Acknowledgments
Role of the Funding Sources
This research was supported by funds from the National Institute of Child Health and Human Development (Grant R01 HD062567). This work is also a publication of the US Department of Agriculture (USDA/ARS) Children’s Nutrition Research Center, Department of Pediatrics, Baylor College of Medicine (Houston, TX) funded in part by the USDA/ARS (Cooperative Agreement 58-3092-5-001). The contents of this publication do not necessarily reflect the views or policies of the USDA, nor does mention of trade names, commercial products, or organizations imply endorsement from the US government. The funding source had not involvement in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Footnotes
Author Disclosures
Conflict of Interest
The authors declare no conflicts of interest.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Aber JL, Bennett NG, Conley DC, & Li J (1997). The effects of poverty on child health and development. Annual Reviews of Public Health, 18, 463–483. [DOI] [PubMed] [Google Scholar]
- Ascroft J, Semmler C, Carnell S, van Jaarsveld CHM, & Wardle J (2008). Continuity and stability of eating behaviour traits in children. European Journal of Clinical Nutrition, 62, 985–990. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (2017). Defining Adult Overweight and Obesity. Retrieved from https://www.cdc.gov/obesity/adult/defining.html
- de Barse LM, Tiemeier H, Leermakers ETM, Voortman T, Jaddoe VWV, Edelson LR, Franco OH, & Jansen PW (2015). Longitudinal association between preschool fussy eating and body composition at 6 years of age: The Generation R Study. International Journal of Behavioral Nutrition and Physical Activity, 12, 153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Birch LL, & Fisher JO (1998). Development of eating behaviors among children and adolescents. Pediatrics, 101, 539–549. [PubMed] [Google Scholar]
- Demir D, & Bektas M (2017). Effects of children’s eating behaviors and children’s eating style on childhood obesity. Eating Behaviors, 26, 137–142. [DOI] [PubMed] [Google Scholar]
- Derks IPM, Sijbrands EJG, Wake M, Qureshi F, van der Ende J, Hillegers MHJ, Jaddoe VWV, Tiemeier H, & Jansen PW (2018). Eating behavior and body composition across childhood: A prospective cohort study. International Journal of Behavioral Nutrition and Physical Activity, 15, 96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- dos Passos DR, Gigante DP, Maciel FV, & Matijasevich A (2015). Children’s eating behavior: Comparison between normal and overweight children from a school in Pelotas, Rio Grande do Sul, Brazil. Revista Paulista de Pediatria, 33, 42–49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farrow CV, Haycraft E, & Blissett JM (2015). Teaching our children when to eat: How parental feeding practices inform the development of emotional eating—a longitudinal experimental design. American Journal of Clinical Nutrition, 101, 908–913. [DOI] [PubMed] [Google Scholar]
- Fisher JO, & Birch LL (2002). Eating in the absence of hunger and overweight in girls from 5 to 7 y of age. The American Journal of Clinical Nutrition, 76, 226–231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frankel LA, O’Connor TM, Chen TA, Nicklas T, Power TG, & Hughes SO (2014). Parents’ perceptions of preschool children’s ability to regulate eating. Feeding style differences. Appetite, 76, 166–174. [DOI] [PubMed] [Google Scholar]
- French SA, Epstein LH, Jeffery RW, Blundell JE, & Wardle J (2012). Eating behavior dimensions: Associations with energy intake and body weight. A review. Appetite, 59, 541–549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gregory JE, Paxton SJ, & Brozovic AM (2010). Maternal feeding practices, child eating behavior and body mass index in preschool-aged children: A prospective analysis. International Journal of Behavioral Nutrition and Physical Activity, 7, 55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hankey M, Williams NA, & Dev D (2016). Uninvolved maternal feeding style moderates the association of emotional overeating to preschoolers’ body mass index z-scores. Journal of Nutrition Education and Behavior, 48, 530–537. [DOI] [PubMed] [Google Scholar]
- Herle M, Fildes A, Steinsbekk S, Rijsdijk F, & Llewellyn CH (2017). Emotional over-and under-eating in early childhood are learned not inherited. Scientific Reports, 7, article number 9092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hooper D, Coughlan J, & Mullen MR (2008). Structural equation modeling: Guidelines for determining model fit. The Electronic Journal of Business Research Methods, 6, 53–60. [Google Scholar]
- Hughes SO, Anderson CB, Power TG, Micheli N, Jaramillo S, Nicklas TA (2006). Measuring feeding in low-income African-American and Hispanic parents. Appetite, 46, 215–223. [DOI] [PubMed] [Google Scholar]
- Hughes SO, Power TG, O’Connor TM, & Fisher JO (2015). Executive functioning, emotion regulation, eating self-regulation, and weight status in low-income preschool children: How do they relate? Appetite, 89, 1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hughes SO, Power TG, O’Connor TM, Fisher JO, & Chen T (2016). Maternal feeding styles and food parenting practices as predictors of longitudinal changes in weight status in Hispanic preschoolers from low-income families. Journal of Obesity, Article ID 7201082, 9 pages. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jansen PW, Roza SJ, Jaddoe VWV, Mackenbach JD, Raat H, Hofman A, Verhulst FC, & Tiemeier H (2012). Children’s eating behavior, feeding practices of parents and weight problems in early childhood: Results from the population-based Generation R study. International Journal of Behavioral Nutrition and Physical Activity, 9, 130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson SL, & Taylor-Holloway LA (2006). Non-Hispanic white and Hispanic elementary school children’s self-regulation of energy intake. The American Journal of Clinical Nutrition, 83, 1276–1282. [DOI] [PubMed] [Google Scholar]
- Kuczmarski R, Ogden C, & Guo S (2002). CDC growth charts for the United States:Methods and development. Vital Health Statistics, 11, 1–190. [PubMed] [Google Scholar]
- Leung CYY, Miller AL, Kaciroti NA, Chen YP, Rosenblum K, & Lumeng JC (2016). Low-income preschoolers with higher temperamental surgency enjoy and respond more to food, mediating the path to higher body mass index. Pediatric Obesity, 11, 181–186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lipowska M, Lipowski M, Jurek P, Jankowska AM, & Pawlicka P (2018). Gender and body-fat status as predictors of parental feeding styles and children’s nutritional knowledge, eating habits, and behaviours. International Journal of Environmental Research and Public Health, 15, 852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lohman TG, Roche AF, & Martorell M (1988). Anthropometric standardization reference manual. Champaign, IL: Human Kinetics [Google Scholar]
- MacCallum RC, Browne MW, & Sugawara HM (1996). Power analysis and determination of sample size for covariance structure modeling. Psychological Methods, 1, 130–149. [Google Scholar]
- Mallan KM, Daniels LA, & Nicholson JM (2017). Obesogenic eating behaviors mediate the relationships between psychological problems and BMI in children. Obesity, 25, 928–934 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mallan KM, Nambiar S, Magarey AM, & Daniels LA (2014). Satiety responsiveness in toddlerhood predicts energy intake and weight status at four years of age. Appetite, 74, 79–85. [DOI] [PubMed] [Google Scholar]
- Martens MP, & Haase RF (2006). Advanced applications of structural equation modeling in counseling psychology research. The Counseling Psychologist, 34, 878–911. [Google Scholar]
- Morrison H, Power TG, Nicklas T, & Hughes SO (2013). Exploring the effects of maternal eating patterns on maternal feeding and child eating. Appetite, 63, 77–83. [DOI] [PubMed] [Google Scholar]
- Ogden CL, Fryar CD, Hales CM, Carroll MD, Aoki Y, & Freedman DS (2018). Differences in obesity prevalence by demographics and urbanization in US children and adolescents, 2013–2016. Journal of the American Medical Association, 319, 2410–2418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Park IJK, Wang L, Williams DR, & Alegria M (2018). Coping with racism: Moderators of the discrimination-adjustment link among Mexican-origin adolescents. Child Development, 89, 293–310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Powell EM, Frankel LA,& Hernandez DC (2017). The mediating role of child self-regulation of eating in the relationship between parental use of food as a reward and child emotional overeating. Appetite, 113, 78–83. [DOI] [PubMed] [Google Scholar]
- Power TG, Johnson SL, Beck AD, Martinez AD, & Hughes SO (2019). The Food Parenting Inventory: Factor structure, reliability, and validity in a low-income, Latina sample. Appetite, 134, 111–119. [DOI] [PubMed] [Google Scholar]
- Quah PL, Cheung YB, Pang WW, Toh JY, Saw S, Godfrey KM, Yap F, Chong Y, & Mary CF (2017). Validation of the Children’s Eating Behavior Questionnaire in 3 year old children of a multi-ethnic Asian population: The GUSTO cohort study. Appetite, 113, 100–105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Russell A, & Russell CG (2019). A biopsychosocial approach to processes and pathways in the development of overweight and obesity in childhood: Insights from developmental theory and research. Obesity Reviews, 20, 725–749. [DOI] [PubMed] [Google Scholar]
- Sanlier N, Arslan S, Buyukgenc N, & Toka O.(2018). Are eating behaviors related with by body mass index, gender and age? Ecology of Food and Nutrition, 57, 372–387. [DOI] [PubMed] [Google Scholar]
- Santos JL, Ho-Urriola JA, González A, Smalley SV, Domínguez-Vásquez P, Cataldo R, Obregón AM, Amador P, Weisstaub G, & Hodgson MI (2011). Association between eating behavior scores and obesity in Chilean children. Nutrition Journal, 10, 108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spence JC, Carson V, Casey L, & Boule N (2011). Examining behavioural susceptibility to obesity among Canadian pre-school children: The role of eating behaviours. International Journal of Pediatric Obesity, 6, e501–e507. [DOI] [PubMed] [Google Scholar]
- Spill MK, Callahan EH, Shapiro MJ, Spahn JM, Wong YP, Benjamin-Neelon SE, ... Casavale KO (2019). Caregiver feeding practices and child weight outcomes: A systematic review. The American Journal of Clinical Nutrition, 109, 990S–1002S. [DOI] [PubMed] [Google Scholar]
- Steinsbekk S, Barker ED, Llewellyn C, Fildes A, & Wichstrøm L (2018). Emotional feeding and emotional eating: Reciprocal processes and influence of negative affectivity. Child Development, 89, 1234–1246. [DOI] [PubMed] [Google Scholar]
- Suarez-Morales L, Dillon FR, & Szapocznik J (2007). Validation of the acculturative stress inventory for children. Cultural Diversity and Ethnic Minority Psychology, 13, 216–224. [DOI] [PubMed] [Google Scholar]
- Van Strien T, & Ouwens MA (2007). Effects of distress, alexithymia and impulsivity on eating. Eating Behaviors, 8, 251–257. [DOI] [PubMed] [Google Scholar]
- Viana V, Sinde S, & Saxton JC (2008). Children’s eating behaviour questionnaire: Associations with BMI in Portuguese children. British Journal of Nutrition, 100, 445–450. [DOI] [PubMed] [Google Scholar]
- Wardle J, Guthrie CA, Sanderson S, & Rapoport L (2001). Development of the Children’s Eating Behaviour Questionnaire. Journal of Child Psychology and Psychiatry, 42, 963–970. [DOI] [PubMed] [Google Scholar]
- Webber L, Hill C, Saxton J, Van Jaarsveld CHM, & Wardle J (2009). Eating behaviour and weight in children. International Journal of Obesity, 33, 21–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yeaton WH, Shah MK, & Moss BG (2018). Evaluating coincident relationships between obesity incidence and normal weight incidence from birth through kindergarten for US children. American Journal of Health Promotion, 32, 177–187. [DOI] [PubMed] [Google Scholar]