

Abstract
Objective:
Little attention has been paid to understanding how engaging in cancer-related interpersonal exchanges via varying modes of communication influences psychological well-being among young adults with cancer. This study explored the moderating role of communication mode on the relationship of relational processes of disclosure and responsiveness with psychological well-being.
Methods:
61 young adults with cancer (Mage=34.59, SD=4.82) completed a questionnaire about their most recent cancer-related conversation. Participants reported on communication mode (i.e., face-to-face, text message, phone call) and relational processes of self- and support member- disclosure of thoughts, information, and feelings and how accepted, cared for, and understood they felt within the cancer-related conversation. Cancer adjustment measures included functional well-being and depressive symptoms.
Results:
There were no main effects of communication mode or relational processes. However, communication mode did moderate the relationship between relational processes and cancer adjustment. Greater relational processes of disclosure and responsiveness were associated with better functional well-being and lower depressive symptoms only among those who engaged in their most recent cancer-related conversation through technology-related communication and not for those engaged in face-to-face communication.
Conclusion:
Relational processes that are likely to benefit psychological adjustment after cancer appear to be particularly advantageous over technology-based communication. Young adults commonly report feelings of social isolation and psychological distress after cancer. These findings suggest that technology-related communication holds promise as a way to strengthen support-related communication and protect against distress.
Keywords: cancer, depressive symptoms, functional well-being, oncology, relational processes, technology-related communication, young adults
Background
Despite decades of studies reporting positive associations of social support with cancer-related quality of life, our current approaches to understanding effective support communication might not meet the needs of young adult cancer survivors. While face-to-face communication (e.g., talking about one’s feelings in person with a caring other) has been held as the gold standard of communication,1 with many cancer-related behavioral interventions grounded in face-to-face support, technological advances have provided new avenues and norms to maintaining social interaction and eliciting social support. In fact, most social support and cancer communication studies among young adults have focused almost exclusively on face-to-face communication, ignoring communication that is technology-driven.
Relatively few studies or interventions2 are designed to understand, facilitate, or enhance social support for young adult survivors across different communication modalities, even though young adults prefer interventions that are convenient (e.g., increase participants control and flexibility) and provide social support.3,4 Further, studies have primarily focused on perceptions of social support (e.g., emotional, instrumental), ignoring the impact of relational processes within cancer-related communication (e.g., self-disclosure, perceived disclosure, perceived responsiveness) that are known to underlie the facilitation of support provision and psychological adjustment.5 Indeed, the social cognitive processing theory suggests that adjustment to cancer depends on the extent to which one perceives their social network to be open and responsive to emotional disclosure.6 For young adults with cancer one’s social network serves as a key resource in managing cancer-related concerns (e.g., fertility, recurrence, treatment-related) and promotes psychological adjustment7–9 whereas socially constraining interactions (e.g., changing the topic of conversation) have been associated with increased psychological distress among young adults with cancer.10,11
More importantly, young adults with cancer are increasingly turning to interactive technology platforms (e.g., texting, social media applications) as a form of soliciting and eliciting cancer support, as well as support in general.12,13 These types of platforms allow young adults to interact with their peers and support network as well as with other cancer patients about their diagnosis and its impact on their lives without needing to be in the same physical space.14 Indeed studies have started to analyze narrative content and structure of online young adult cancer social support groups.15–17 One study comparing across an online social support group and a face-to-face communication group found that content expressed online contains greater expression of anger and sadness and more references to friends and sexual topics compared to face-to-face communication whereby more positive emotion was expressed.17 However, research examining the effectiveness of eliciting social support through technology-related communication is limited and results are mixed; majority of this work has focused on the impact of text messaging suggesting that texting specifically is associated with a greater sense of connection and satisfaction in close relationships.18–22
To our knowledge, no studies have examined the impact of mode of communication when an individual with cancer is communicating with their close support network. Thus, examining mode of communication when engaged in cancer-related interpersonal exchange with known social support network members is a novel approach to understanding cancer-related communication among young adults. Further, examining relational processes between face-to-face and technology-related communication (i.e., communication over technology devices: text message, phone call) across young adults with cancer would afford greater insight into how these processes are related to aspects of psychological adjustment across different communication patterns providing an assessment of communication modalities that might foster or hinder cancer-related adjustment. In the absence of rigid intervention studies comparing across modes of communication and contrasting communication-based theories directional hypotheses where not made. Instead, the current study aimed to explore the moderating role of mode of communication on the relationship between relational processes and psychological well-being.
Method
Participants and procedures
Young adults with cancer were identified by the Pennsylvania State Cancer Registry or recruited through social media and/or blog posts on various young adult cancer organizations (Army of Women, GRYT Health, Lacuna Loft, and Young Survival Coalition) to participate in a study on “technology-related communication among young adults with cancer”. These specific cancer organizations were chosen because they either focus specifically on providing support to young adult cancer survivors or have been identified as organizations that support young adult cancer research. Eligibility criteria included: (a) diagnosed with cancer (excluding nonmelanoma skin cancer) and current age between 18–45 and (b) ability to read and understand English. Participants completed questionnaires online through Qualtrics between December 2017 and March of 2019, with majority of participants recruited through social media between January and March 2019. After the conclusion of the study four participants were randomly selected to receive a $25 gift card. Informed consent was obtained from all individual participants included in the study and procedures were approved by the appropriate Institutional Review Board (approval number: 2017–0807).
Demographic and medical characteristics of the sample are displayed in Table 1. Participants included 62 young adults with cancer who ranged in age from 24–42 years (M=34.59, SD=4.82) with a cancer diagnosed between the ages of 19–42. One participant was excluded in the present study due to missing data on outcomes of interest resulting in a final sample size of 61 participants. Participants were predominantly White (93.4%), female (95.1%), and married/partnered (70.5%). The majority were diagnosed with breast cancer (72.1%) and treated with surgery (91.8%) and/or chemotherapy (75.4%). Over 80% of the sample were diagnosed with early stage disease (88.1%) and had completed treatment at the time of enrollment (88.5%). The average time since diagnosis was 2.5 years (M=28.76 months, SD=30.68).
Table 1.
Demographic and Medical Characteristics
| Variable | N (%) | Range |
|---|---|---|
| Age [Mean (SD)] | 34.59 (4.82) | 24–42 |
| Female | 58 (95.1%) | |
| Race/ethnicity | ||
| White | 57 (93.4%) | |
| Asian | 2 (3.4%) | |
| Black/African American | 1 (1.6%) | |
| Hispanic/Latino | 1 (1.6%) | |
| Education | ||
| High school degree | 2 (3.4%) | |
| Some college, Trade/Business school | 9 (14.6%) | |
| 4-year college degree | 25 (41%) | |
| Graduate degree | 25 (41%) | |
| Employment status | ||
| Employed | 44 (72.2%) | |
| Student | 3 (4.8%) | |
| Medical leave/disability/unemployed | 14 (23.0%) | |
| Relationship status | ||
| Single, never married | 14 (23.0%) | |
| Married/Partnered | 43 (70.4%) | |
| Divorced/Widowed | 4 (6.6%) | |
| Cancer type | ||
| Breast | 44 (72.1%) | |
| Othera | 17 (27.9%) | |
| Cancer stage | ||
| Early Stage (0-III) | 52 (88.1%) | |
| Stage IV | 2 (3.4%) | |
| Not staged (e.g., brain cancer) | 5 (8.5%) | |
| Treatmentb | ||
| Surgery | 56 (91.8%) | |
| Chemotherapy | 46 (75.4%) | |
| Hormone | 37 (60.7%) | |
| Radiation | 30 (49.2%) | |
| Treatment status | ||
| Completed main treatmentc | 54 (88.5%) | |
| Months since diagnosis [Mean (SD)] | 28.76 (30.68) | |
| Mode of Communication | ||
| Face-to-Face | 39 (69.3%) | |
| Technology-related: Text | 14 (23.0%) | |
| Technology-related: Phone | 8 (13.1%) |
Brain/Hodgkin’s/Cervical/Leukemia/Colon/Ovarian/Thyroid/Salivary gland/Testicular
>1 treatment could be selected
includes hormonal therapy
Measures
Mode of Communication.
Participants were asked five open-ended questions in relation to the prompt, “Think about the most recent cancer-related conversation you had with someone from your social support network.” These open-ended questions asked about, (1) who they were communicating with (e.g., close friend, mother, partner), (2) when the conversation took place (3) what the cancer-related conversation was about, (4) who initiated the conversation, and (5) how (i.e., mode) the conversation took place. Mode of communication was coded as face-to-face vs. technology-related (e.g., text message, phone call). Conversational topics were coded by the first author and a research assistant by independently reading open-ended responses to identify cancer-related concern domain areas (inter-rater reliability >80%).
Relational Processes.
Ratings were adapted from Laurenceau et al. (1998).23 Relational processes measured included: self-disclosure, perceived support member disclosure, and perceived support member responsiveness.
Self-disclosure.
Participants rated the degree to which they disclosed thoughts, information, and feelings to their social support member within their most recent cancer-related conversation with three questions on a 7-point Likert scale ranging from (1) not at all to (7) very much. A sample item includes, “How much did you disclose information to your social support member?” A total score for self-disclosure was calculated by summing across the three questions with higher scores indicating higher levels of self-disclosure. Cronbach’s alpha was 0.75.
Perceived Support Member Disclosure.
Participants rated the degree to which they perceived their social support network member to disclose their own thoughts and feelings (positive emotion) within their most recent cancer-related conversation with two questions on a 7-point Likert scale ranging from (1) not at all to (7) very much. A sample item included, “How much positive emotion did your social support member disclose?” A total score for perceived disclosure was calculated by summing across the two questions. Cronbach’s alpha of 0.78.
Perceived Support Member Responsiveness.
Participants rated the degree to which they felt accepted, cared for, and understood by their support member within their most recent cancer-related conversation with three questions on a 7-point Likert scale ranging from (1) not at all to (7) very much. Sample items included, “To what degree did you feel accepted by your social support member”, “To what degree did you feel understood by your social support member.” A total score for perceived responsiveness was calculated by summing across the three questions. Cronbach’s alpha was 0.88.
Functional Well-Being.
Functional well-being in the past week was assessed using the Functional Well-being subscale of the Functional Assessment for Cancer Therapy, General Version (FACT-G).24 Participants rated their agreement with items of a 5-point scale ranging from (0) not at all to (4) very much. Sample items included, “I am able to work (including work at home)”, “I am enjoying the things I usually go for fun”. Items are reverse scored so that higher scores indicate better functional well-being. Cronbach’s alpha was 0.84.
Depressive Symptoms.
Depressive symptoms during the past week was measured by the 10-item Center for Epidemiological Studies Depression Scale (CESD-10).25 Participants rated their agreement with items on a 4-point scale ranging from (0) rarely or none of the time to (3) all of the time. Scores were summed to a total score where higher scores reflected more depressive symptoms. Sample items included, “I felt depressed” and “I felt happy” (reverse scored). A total score of 10 is typically used as a cut off for identifying individuals at risk for clinical depression. Cronbach’s alpha was 0.81.
Data Analytic Plan
Descriptive statistics and zero-order correlations were conducted for key study variables. Associations between demographic and medical variables were examined as possible covariates. Multiple linear regression was used to test expected relationships between relational processes, mode of communication, and well-being. In each model, relevant covariates were entered into the first block, relational process variables (self-disclosure, perceived support member disclosure, perceived support member responsiveness; entered in separate models) and mode of communication in the second block, and the interaction term (relational process variable x mode of communication). Separate regression models were tested for each relational process variable and associated interaction term. To avoid multicollinearity variables were centered around the mean and interaction terms were analyzed in accordance with methods outlined by Aiken & West (1991).26 To interpret significant interactions, simple slopes analyses were conducted at one standard deviation above and below the mean using PROCESS.27
Results
Descriptive statistics and identification of covariates
Descriptive statistics and correlations of key study variables were examined (see Table 2). Average levels of functional well-being (M=17.84, SD=5.41) were consistent with prior reports by young adults.28,29 Half of the sample (n=33; 55.1%) met the CESD-10 cutoff of ≥ 10 (M=11.20, SD=5.62). For relational process variables almost half of young adults (49.2%) indicated that they self-disclosed above a moderate amount of their thoughts, information, and feelings (M=15.14, SD=4.62) to their support member during their most recent cancer-related conversation. For perceived support member disclosure, over half (63.6%) of young adults reported that they perceived their support member to disclose their thoughts and engage with positive emotion to a great extent (M=9.56, SD=3.27). Majority of young adults (77.5%) reported that they felt their support member accepted, understood, and cared for them to a great extent (M=16.11, SD=4.72) during that same cancer-related conversation.
Table 2.
Descriptives of the Study Sample
| Variable | Mean | SD | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|---|---|
| 1. Communication Mode | - | −.22 | −.04 | −.08 | .17 | −.08 | ||
| 2. Self-Disclosure | 15.14 | 4.62 | - | .69** | .50** | −.24 | .17 | |
| 3. Perceived Disclosure | 9.56 | 3.27 | - | .68** | −.28* | .28* | ||
| 4. Perceived Responsiveness | 16.11 | 4.72 | - | −.23 | −.24 | |||
| 5. Depressive Symptoms | 11.20 | 5.62 | - | −.71** | ||||
| 6. Functional Well-Being | 17.84 | 5.41 | - |
p<.05
p<.01
Close to two-thirds of the sample (63.9%) engaged in their most recent cancer-related conversation face-to-face with their identified social support member while 36.1% engaged in their most recent cancer-related conversation over technology-related communication (text message: 23.0%, phone call: 13.1%). Majority of young adults reported having their most recent cancer-related conversation with a friend (41.0%) or family member (37.7%), with conversations with partners/spouses less commonly reported (21.3%). Two-thirds of the sample (65.6%) reported initiating the conversation, with conversation topics including recurrence and treatment (36.1%), survivorship and health follow-up (29.5%), emotional concerns and body image (18.0%), fertility and sexual functioning (8.2%), cancer-related concerns due to the support member having cancer in their family (4.9%), and financial concerns (3.3%).
Bivariate correlations were conducted to test for associations between demographic, medical, and dependent variables. Significant associations were controlled for in the respective models. Age, employment status, history of depression, and person communicated with during their most recent cancer-related conversation were controlled for in analyses predicting functional well-being. History of depression, marital status, and employment status were controlled for in analyses predicting depressive symptoms.
Hypotheses testing
Results are presented by outcome variable.
Functional Well-Being.
There were no significant main effects of relational process variables and mode of communication for functional well-being. However, there were significant relational process variable x mode of communication interactions across all relational processes. The self-disclosure x mode of communication interaction [F(7,52)=5.99, p<.001, adjusted R2=0.37; β=0.38, p<.05] was significant, explaining an additional 6% of the variance. The perceived support member disclosure x mode of communication interaction [F(7,53)=6.40, p<.001, adjusted R2=0.39; β=0.28, p<.05] was significant, explaining an additional 5% of the variance. The perceived support member responsiveness x mode of communication interaction was significant [F(7,53)=9.40, p<.001, adjusted R2=.50; β=0.54, p<.001), explaining an additional 14% of the variance.
Simple slopes analyses revealed the same slope directions for each relational process variable. For each interaction there was a significant increasing slope only for those who engaged in their most recent cancer-related conversation through technology-based communication. This increasing slope suggests that functional well-being is increasing as self-disclosure, perceived support member disclosure, and perceived support member responsiveness increases over technology-related communication. The slope for face-to-face interaction was not significant (see Figure 1).
Figure 1.
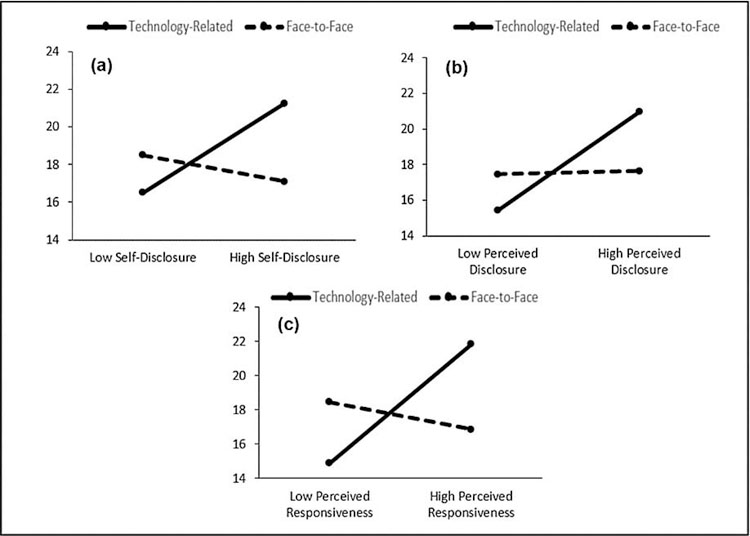
The three graphs in figure 1 represent the interaction of relational processes (a) self-disclosure, (b) perceived support member disclosure, (c) perceived support member responsiveness and mode of communication on functional well-being. The dashed line represents non-significant simple slopes.
Depressive Symptoms.
There were no significant main effects of relational process variables and mode of communication for depressive symptoms. However, there were significant relational process variable x mode of communication interactions across all relational processes. The self-disclosure x mode of communication interaction was significant [F(6,52)=4.17, p<.01, adjusted R2=0.25; β=−0.38, p<.05], explaining an additional 6% of the variance. The perceived support member disclosure x mode of communication interaction was significant [F(6,53)=4.69, p<.01, adjusted R2=0.27; β=−0.31, p<.05], explaining an additional 5% of the variance. The perceived support member responsiveness x mode of communication interaction was significant [F(6,53)=5.55, p<.001,adjusted R2=0.32; β=−0.42, p<.01), explaining an additional 9% of the variance.
Simple slopes analyses revealed the same slope directions for each relational process variable. For each interaction there was a significant decreasing slope only for those who engaged in their most recent cancer-related conversation through technology-based communication. This decreasing slope suggests that depressive symptoms are decreasing as self-disclosure, perceived support member disclosure, and perceived support member responsiveness increases over technology-related communication. The slope for face-to-face interaction was not significant (see Figure 2).
Figure 2.
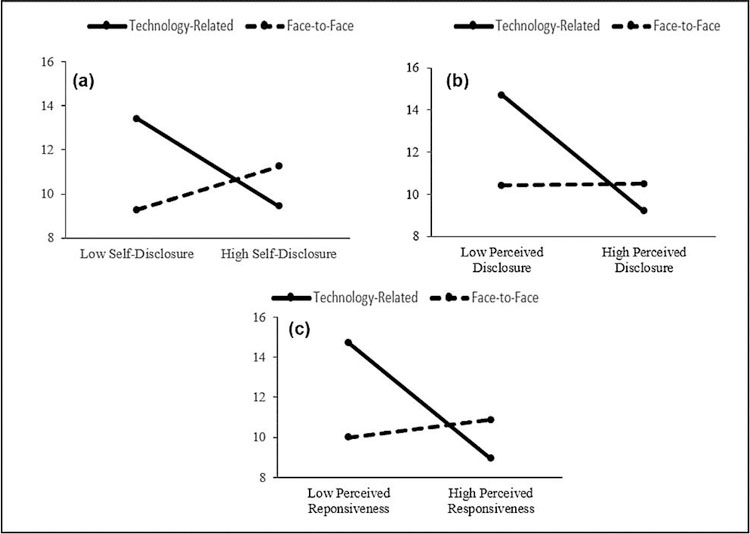
The three graphs in figure 2 represent the interaction of relational processes (a) self-disclosure, (b) perceived support member disclosure, (c) perceived support member responsiveness and mode of communication on depressive symptoms. The dashed line represents non-significant simple slopes.
Discussion
The present study examined the moderating role of mode of communication on the relationship between relational processes and psychological well-being among young adults with cancer. Overall, results suggested that, among young adults who engaged in their most recent cancer-related conversation via technology-related communication, those reporting higher relational processes had greater functional well-being and lower depressive symptoms compared to young adults who engaged in their most recent cancer-related conversation via face-to-face conversation. This pattern of interaction was significant across all analyses potentially suggesting that the relational processes of disclosure: self-disclosure, perceived support member disclosure, and perceived support member responsiveness appear to be particularly advantageous in cancer-related interpersonal exchanges via technology-based communication among young adult survivors.
At the same time, relational processes had no relationship with adjustment for face-to-face communication. It might be that the physical presence of another individual, as in face-to-face communication, regardless of amount of disclosure and felt responsiveness, is protective. Indeed, decades of several decades of social support research has found that the presence of a supportive other has a protective effect on both psychological and physiological well-being among individuals with cancer.30–33 Communication theories that take an evolutionary perspective34,35 have suggested that the human brain has evolved primarily for the purpose of face-to-face communication and is generally less skilled at processing communication that lacks a face-to-face component, potentially due to the decrease of nonverbal cues (e.g., eye contact, light touch).
In large, technology-related communication has an absence of nonverbal cues. Given this absence of nonverbal cues, Social Information Processing theory suggests that there will be greater reliance on message content when inferring meaning rather than body language or other nonverbal cues typical of face-to-face communication.36 With minimal disclosure or responsiveness (e.g., phone silence, brevity of text message response), heavy reliance on the content of messages might lead one to interpret uncertain or hostile interpersonal behaviors37 thus decreasing psychological well-being. Therefore, the extent that one can self-disclose thoughts, feelings, and information and perceive reciprocal disclosure and responsiveness from their supportive other via technology-related channels, the less ambiguity in inferring content meaning and the greater the benefit to psychological and functional well-being.
However, there is growing body of literature focused on the non-written elements of technology-mediated communication (e.g., emoji usage, GIFs, memes). These types of non-written communication can be seen as a humanized tool for expressing emotion, replacing the cues that are naturally present in face-to-face communication which then provides additional context to the technology-based interaction and enhances comprehension of messages.38 Future technology-based research should focus on understanding how this non-written usage unfolds and impacts relational processes and well-being within the dynamics of a technology-based interaction.
Future research should also examine the potential for active decision-making processes associated with initiation of cancer-related conversations. Mode of communication might be influenced, for example, by an active decision to engage in a conversation about fear of cancer recurrence over technology-related communication or face-to-face communication, thus communication mode might vary depending on several decision making factors (e.g., person communicating with, topic of conversation).
Study Limitations
This study is not without limitations. First, young adults were asked to retrospectively consider their most recent-cancer related conversation and rate the degree of relational disclosure and closeness, which may be vulnerable to recall bias. Second, data are cross-sectional. Although directionality was theory-driven, causal interpretations cannot be established. Future studies should explore the potential for a dynamic relationship of cancer-related discussions over varying communication methods that unfolds over time and across the care continuum. Further, technology-related communication was defined as any communication form that happens over a mobile or computer device, therefore text messaging and phone calls were considered technology-based for the present study. Future studies should test various types of mediated communication separately in order to understand the potential influence of one form of communication over another.
In addition, all demographic and clinical data (including diagnosis) were self-reported. Finally, the demographic and clinical representativeness of this sample limits generalizability. While recruitment aimed to focus on social media platforms that had a broad young adult cancer following this resulted in a sample was mostly comprised of an ‘older’ young adult population that was almost exclusively female, predominantly white, married, and with a breast cancer diagnosis. It is possible that recruitment across additional cancer-related organizations would have resulted in different demographics. Further, there are known gender differences in technology-based communication suggesting that women might be more emotionally expressive than men,39 thus future studies should attempt to oversample young male survivors and minorities in order to achieve a more heterogenous sample.
Clinical Implications
These findings have clinical applications. Support from family and friends contributes to resilience and is a vital means of coping for young adults with cancer.40 Reinforcing the benefits of talking to members of one’s social support network and the importance of voicing and disclosing thoughts, information, and feelings is vital. However, this may be difficult for some young adults with cancer and thus reinforcing discussion over technology-related methods might be one way of reducing social isolation and facilitating well-being. Health-care providers and social support members should be aware of the multiple technology-based approaches to supporting young adults with cancer.
Conclusions
This study challenges the foundations of the medium in which communication must take place in order to fulfill support needs. Support-related communication theories are grounded in face-to-face interactions; however, these findings suggest that perhaps technology-related communication is beneficial but there needs to be greater relational processing on both sides of the dyad for that communication to have protective effects. Reinforcing disclosure and responsiveness across technology-related communication might be one key to increased psychological well-being as young adults are increasingly using these outlets. In fact, in the present sample, when asked about how these young adults are typically communicating with other family members and/or friends about a cancer-related concern, majority of the sample (76.7%) reported engaging in technology-related communication (e.g., text message, social media, phone call) as their go-to mode of communication for cancer-related concerns in general.
Technology-related communication is transforming the way in which young adults with cancer are interacting with their social support network by providing a platform in which personal cancer-related concerns can be shared and support can be received without the physical presence of another individual. However, there remains a large gap in the supportive literature addressing the changing social landscape. A critical need is the development of theory-based, age-appropriate communication studies that include technology-related communication and apply current evidence derived from young adults with cancer. Challenging the notion of traditional face-to-face support as a prerequisite for health and intimacy can substantially improve the lives of young adults with cancer.
Acknowledgements:
Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under Award Number F99CA222727 (PI: Darabos). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. This research was additionally supported by funds from the American Psychological Foundation, and the Graduate Center Doctoral Student Research Grant. Part of these data were supplied by the Bureau of Health Statistics & Registries, Pennsylvania Department of Health, Harrisburg, Pennsylvania. The Pennsylvania Department of Health specifically disclaims responsibility for any analyses, interpretations or conclusions. The authors would like to thank the Army of Women, GRYT Health, Lacuna Loft, and the Young Survival Coalition for their assistance in recruitment.
Footnotes
Conflict of Interest: The authors declare that they have conflicts of interest.
Data Availability Statement: The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
- 1.Hinds PJ, Kiesler S. Distributed work: New research on working across distance using technology. Cambridge, MA: MIT Press; 2002. [Google Scholar]
- 2.Iannarino NT, Scott AM, Shaunfield SL. Normative social support in young adult cancer survivors. Qual Health Res 2017. January;27(2):271–84. 10.1177/1049732315627645 [DOI] [PubMed] [Google Scholar]
- 3.Benedict C, Victorson D, Love B, Fuehrer D, Lazard A, Saffer AJ, Linscott T, Zachary M. The audacity of engagement: Hearing directly from young adults with cancer on their attitudes and perceptions of cancer survivorship and cancer survivorship research. J Adolesc Young Adult Oncol 2018. February 1;7(1):103–11. 10.1089/jayao.2017.0038 [DOI] [PubMed] [Google Scholar]
- 4.Rabin C, Simpson N, Morrow K, Pinto B. Intervention format and delivery preferences among young adult cancer survivors. Int J Behav Med 2013. June 1;20(2):304–10. 10.1007/s12529-012-9227-4 [DOI] [PubMed] [Google Scholar]
- 5.Reis HT, Shaver P. Intimacy as an interpersonal process In: Duck S, editor. Handbook of personal relationships. Chichester, England: Wiley; 1988; pp. 367–389. [Google Scholar]
- 6.Lepore SJ, Revenson TA. Social constraints on disclosure and adjustment to cancer. Soc Personal Psychol Compass 2007. November;1(1):313–33. 10.1111/j.1751-9004.2007.00013.x [DOI] [Google Scholar]
- 7.Bloom JR, Stewart SL, Johnston M, Banks P, Fobair P. Sources of support and the physical and mental well-being of young women with breast cancer. Soc Sci Med 2001. December 1;53(11):1513–24. 10.1016/S0277-9536(00)00440-8 [DOI] [PubMed] [Google Scholar]
- 8.Boinon D, Sultan S, Charles C, Stulz A, Guillemeau C, Delaloge S, Dauchy S. Changes in psychological adjustment over the course of treatment for breast cancer: the predictive role of social sharing and social support. Psychooncology. 2014. March;23(3):291–8. 10.1002/pon.3420 [DOI] [PubMed] [Google Scholar]
- 9.Cohee AA, Stump T, Adams RN, Johns SA, Von Ah D, Zoppi K, et al. Factors associated with depressive symptoms in young long-term breast cancer survivors. Qual Life Res 2016. August 1;25(8):1991–7. 10.1007/s11136-016-1241-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cohee AA, Adams RN, Johns SA, Von Ah D, Zoppi K, Fife B, et al. Long-term fear of recurrence in young breast cancer survivors and partners. Psychooncology. 2017. January;26(1):22–28. https://doi: 10.1002/pon.4008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Darabos K, Hoyt MA. Cancer-related worry and physical well-being in the context of perceived stress in young adults with testicular cancer. J Adolesc Young Adult Oncol 2017. June;6(2):363–366. https://doi: 10.1089/jayao.2016.0069 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Fox S, Purcell K. Social media and health. 2010. http://www.pewinternet.org/2010/03/24/social-media-and-health/. Accessed on 24 Jun 2019.
- 13.Perales MA, Drake EK, Pemmaraju N, Wood WA. Social media and the adolescent and young adult (AYA) patient with cancer. Curr Hematol Malig Rep 2016. December 1;11(6):449–55. 10.1007/s11899-016-0313-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Abrol E, Groszmann M, Pitman A, Hough R, Taylor RM, Aref-Adib G. Exploring the digital technology preferences of teenagers and young adults (TYA) with cancer and survivors: a cross-sectional service evaluation questionnaire. J Cancer Survivorship. 2017. December 1;11(6):670–82. 10.1007/s11764-017-0618-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Crook B, Love B. Examining the light and dark of an online young adult cancer support community. Qual Health Res 2016. October:27(6):938–948. 10.1177/1049732316672638 [DOI] [PubMed] [Google Scholar]
- 16.Love B, Crook B, Thompson C, et al. Exploring psychosocial support online: A content analysis of messages in an adolescent and young adult cancer community. Cyberpsychol Behav 2012. October:15(10):555–559. 10.1089/cyber.2012.0138 [DOI] [PubMed] [Google Scholar]
- 17.Thompson CM, Crook B, Love B, Macpherson CF, Johnson R. Understanding how adolescnts and young adults talk about needs in online and face-to-face support groups. J Health Psychol 2016. November:21(11):2636–2646. 10.1177/1359105315581515 [DOI] [PubMed] [Google Scholar]
- 18.Angster A, Frank M, Lester D. An exploratory study of students’ use of cell phones, texting, and social networking sites. Psychol Rep 2010. October;107(2):402–4. 10.2466/17.PR0.107.5.402-404. [DOI] [PubMed] [Google Scholar]
- 19.Coyne SM, Stockdale L, Busby D, Iverson B, Grant DM. “I luv u:)!”: A descriptive study of the media use of individuals in romantic relationships. Fam Rel 2011. April;60(2):150–62. 10.1111/j.1741-3729.2010.00639.x. [DOI] [Google Scholar]
- 20.Murdock KK. Texting while stressed: Implications for students’ burnout, sleep, and well-being. Psychol Pop Media Cult 2013. October;2(4):207 10.1037/ppm0000012 [DOI] [Google Scholar]
- 21.Pettigrew J Text messaging and connectedness within close interpersonal relationships. J Marriage Fam 2009. August 1;45(6–8):697–716. 10.1080/01494920903224269 [DOI] [Google Scholar]
- 22.Saad L Nearly half of smartphone users can’t imagine life without it. 2015. http://www.gallup.com/poll/184085/nearly-half-smartphone-users-imaginelife-without.aspx. Accessed 24 Jun 2019
- 23.Laurenceau JP, Barrett LF, Pietromonaco PR. Intimacy as an interpersonal process: The importance of self-disclosure, partner disclosure, and perceived partner responsiveness in interpersonal exchanges. J Pers Soc Psychol 1998. May;74(5):1238 10.1037/0022-3514.74.5.1238 [DOI] [PubMed] [Google Scholar]
- 24.Cella DF, Tulsky DS, Gray G, Sarafian B, Linn E, Bonomi A, et al. The Functional Assessment of Cancer Therapy scale: development and validation of the general measure. J Clin Oncol 1993. March 1;11(3):570–9. 10.1200/JCO.1993.11.3.570 [DOI] [PubMed] [Google Scholar]
- 25.Andresen EM, Malmgren JA, Carter WB, Patrick DL. Screening for depression in well older adults: Evaluation of a short form of the CES-D. Am J Prev Med 1994. March 1;10(2):77–84. [PubMed] [Google Scholar]
- 26.Aiken LS, West SG. Multiple regression: Testing and interpreting interactions. Newbury Park: Sage; 1991. [Google Scholar]
- 27.Hayes AF. Introduction to mediation, moderation, and conditional process analysis. 2nd edition. Guilford Press; 2018. [Google Scholar]
- 28.Hoyt MA, Gamarel KE, Saigal CS, Stanton AL. Goal navigation, approach-oriented coping, and adjustment in young men with testicular cancer. Ann Behav Med 2016. March 2;50(4):572–81. 10.1007/s12160-016-9785-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Valle CG, Tate DF, Mayer DK, Allicock M, Cai J. A randomized trial of a Facebook-based physical activity intervention for young adult cancer survivors. J Cancer Survivorship. 2013. September 1;7(3):355–68. 10.1007/s11764-013-0279-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Zebrack B, Isaacson S. Psychosocial care of adolescent and young adult patients with cancer and survivors. J Clin Oncol 2012. March 12;30(11):1221–6. 10.1200/JCO.2011.39.54677 [DOI] [PubMed] [Google Scholar]
- 31.Cassel J The contribution of the social environment to host resistance. Am J Epidemiol 1976. August;104(2):107–23. 10.1093/oxfordjournals.aje.a112281 [DOI] [PubMed] [Google Scholar]
- 32.Cobb S Social support as a moderator of life stress. Psychosom Med 1976. Sep-Oct;38(5):300–14 [DOI] [PubMed] [Google Scholar]
- 33.Kyngäs H, Mikkonen R, Nousiainen EM, Rytilahti M, Seppänen P, Vaattovaara R, Jämsä T. Coping with the onset of cancer: coping strategies and resources of young people with cancer. Eur J Cancer Care. 2001. March;10(1):6–11. 10.1046/j.1365-2354.2001.00243.x [DOI] [PubMed] [Google Scholar]
- 34.Knock N Media naturalness theory: human evolution and behaviour towards electronic communication technologies Roberts SC, editor. Applied evolutionary psychology. Oxford University Press; 2011, pp. 381–398. [Google Scholar]
- 35.Hantula DA, Kock N, D’Arcy JP, DeRosa DM. Media compensation theory: A Darwinian perspective on adaptation to electronic communication and collaboration Saad G, editor. Evolutionary psychology in the business sciences. Berlin: Springer; 2011, pp. 339–363. [Google Scholar]
- 36.Walther JB, Parks MR. Cues filtered out, cues filtered in: Computers-mediated communications add relationships Knapp ML, & Daly JA, editors. Handbook of interpersonal communication. Thousand Oaks, CA: SAGE; 2002, pp. 529–563. [Google Scholar]
- 37.Baxter LA, Braithwaite DO. Relational dialectics theory, applied. New directions in interpersonal communication research. 2010. January 1:48–66. [Google Scholar]
- 38.Aldunate N, Gonzalez-Ibanez R. An integrated review of emoticons in computer-mediated communication. Front Psychol 2017. January:7:2061 10.3389/fpsyg.2016.02061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Gooden RJ, Winefield HR. Breast and prostate cancer online discussion boards: A thematic analysis of gender differences and similarities. J Health Psychol 2007. January:12(1):103–114. 10.1177/1359105307071744 [DOI] [PubMed] [Google Scholar]
- 40.Soliman H, Agresta SV. Current issues in adolescent and young adult cancer survivorship. Cancer Control. 2008. January;15(1):55–62. 10.1177/107327480801500107 [DOI] [PubMed] [Google Scholar]