

Abstract
Background
Many women experience leg cramps in pregnancy. They become more common as pregnancy progresses and are especially troublesome at night.
Objectives
The objective of this review was to assess methods of preventing and treating leg cramps in pregnancy.
Search methods
We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (October 2001). We updated this search on 4 July 2011 and added the results to the awaiting classification section.
Selection criteria
Randomised trials of treatments for leg cramps in pregnancy.
Data collection and analysis
Trial quality was assessed and data were extracted independently by two reviewers.
Main results
Five trials involving 352 women were included. The trials were of moderate quality. The only placebo‐controlled trial of calcium treatment showed no evidence of benefit. Trials comparing sodium chloride with placebo (odds ratio 0.54, 95% confidence interval 0.23 to 1.29) and calcium with sodium chloride (odds ratio 1.23, 95% confidence intervals 0.47 to 3.27 ) showed no evidence of benefit. Placebo controlled trials of multivitamin with mineral supplements (odds ratio 0.23, 95% confidence intervals 0.05 to 1.01) and magnesium (odds ratio 0.18, 95% confidence intervals 0.05 to 0.60) provided some suggestion of benefit.
Authors' conclusions
The evidence that calcium reduces cramp is weak and seems to depend on placebo effect. The evidence for sodium chloride is stronger but the results of the sodium chloride trial may no longer be relevant because of dietary changes which include an increased sodium intake in the general population. It is not possible to recommend multivitamins with mineral supplementation, as it is not clear which ingredient, if any, is helping. If a woman finds cramp troublesome in pregnancy, the best evidence is for magnesium lactate or citrate taken as 5mmol in the morning and 10mmol in the evening.
[Note: The five citations in the awaiting classification section of the review may alter the conclusions of the review once assessed.]
Plain language summary
Interventions for leg cramps in pregnancy
Sodium supplements may decrease the number of cramp attacks experienced by women in pregnancy but the effect is slight. Calcium is of no benefit. The evidence of benefit for magnesium is stronger. Multivitamin and mineral supplements also seem to help but the relevance of this is unclear as the preparation used contained twelve separate constituents and it is not possible to discover which of these was effective, or indeed if there was synergy between constituents. There is a theoretical risk that sodium supplementation could raise blood pressure. It is unlikely that magnesium supplementation would be harmful at the suggested doses.
Background
Leg cramps are a common problem in the second half of pregnancy, experienced by up to half of pregnant women (Salvatore 1961). They can be particularly troublesome at night. The mechanism is unclear but leg cramps occur in fit and healthy people such as athletes. Nor is it clear why they should occur more commonly in pregnancy, becoming more so as pregnancy progresses. Possible mechanisms which have been suggested are: slowed venous return resulting from raised intra abdominal pressure with progesterone decreasing the tone in the venous musculature and nutritional deficiencies brought about by the demands of the growing fetus. The pain seems to be caused by a build up of lactic and pyruvic acids leading to involuntary contraction of the affected muscles, usually in the legs. Though cramp causes no lasting damage to muscle, it can be very painful and, unfortunately is very much more common at night in bed. It is a common experience that getting out of bed, walking around, stretching and massaging the affected muscle(s) seems to be helpful, possibly by dispersing the build up of acids.
Objectives
To assess the effects of different treatments for leg cramps in pregnancy.
Methods
Criteria for considering studies for this review
Types of studies
All trials comparing treatments for cramp with placebo or no treatment, or comparisons between different treatments. Trials are only included which assess symptomatic relief.
Types of participants
Pregnant women who have developed or might develop leg cramps.
Types of interventions
Oral calcium versus no treatment (Hammar 1981). Oral calcium versus placebo (Vitamin C) (Hammar 1987). Sodium chloride versus three different control interventions namely placebo, saccharin and calcium lactate (Robinson 1947). Multivitamin and mineral supplements versus placebo (Thauvin 1992). Magnesium versus placebo (sorbitol/fructose/dextrose) (Dahle 1995).
Types of outcome measures
Persistence or recurrence of leg cramps.
Search methods for identification of studies
We searched the Cochrane Pregnancy and Childbirth Group’s Trials Register by contacting the Trials Search Co‐ordinator (October 2001). We updated this search on 4 July 2011 and added the results to Studies awaiting classification.
The Cochrane Pregnancy and Childbirth Group’s Trials Register is maintained by the Trials Search Co‐ordinator and contains trials identified from:
quarterly searches of the Cochrane Central Register of Controlled Trials (CENTRAL);
weekly searches of MEDLINE;
weekly searches of EMBASE;
handsearches of 30 journals and the proceedings of major conferences;
weekly current awareness alerts for a further 44 journals plus monthly BioMed Central email alerts.
Details of the search strategies for CENTRAL, MEDLINE and EMBASE, the list of handsearched journals and conference proceedings, and the list of journals reviewed via the current awareness service can be found in the ‘Specialized Register’ section within the editorial information about the Cochrane Pregnancy and Childbirth Group.
Trials identified through the searching activities described above are each assigned to a review topic (or topics). The Trials Search Co‐ordinator searches the register for each review using the topic list rather than keywords.
We did not apply any language restrictions.
Data collection and analysis
Trials under consideration were evaluated for methodological quality and appropriateness for inclusion, without consideration of their results. Included trial data were processed as described in Clarke 2001.
Results
Description of studies
Risk of bias in included studies
The methodological quality of these trials is only moderate. In the Hammar 1981 paper, calcium treatment was compared with no treatment, rather than with placebo. Given this is the only one of the three trials using calcium which showed a positive result, it is likely that this result is due to a placebo effect. Hammar 1987 used vitamin C as placebo. Both of these were small studies with totals of 42 and 60 patients respectively. In neither study is the method of randomization described. In neither is there any discussion of adverse effects. Robinson 1947 used an elaborate methodology to compare calcium and sodium chloride with placebo and saccharin. Allocation of the 198 participants was by alternation; problems with the taste of sodium chloride led the investigator to change the formulation in the course of the study. The dose of sodium chloride began as 60g of powder but the taste was obvious and later three 15g tablets were used. The author states that sodium chloride "has no ill effects ". There is no further discussion of any possible adverse effects except to record that the taste of the powder was unacceptable hence the switch to tablets. Thauvin 1992 seemed mainly interested in studying the effects of mineral supplements on zinc and copper levels through pregnancy. The information on cramp occupies only seven lines in the study. Only 27 women out of the 60 who began in the trial were assessed for cramp at the end of their pregnancies. Twelve ingredients (see table of included studies), something of a witch's brew, made up the tablets and it is not possible to know which, if any, of these helped. The method of randomization is not described. Adverse effects are not mentioned. The magnesium versus placebo trial (Dahle 1995) is the best study in this review though the method of randomization is again not described. Seventy three women began the study and only four dropped out. The study assessed the women after three weeks of treatment. There was no further follow‐up. Side effects are described as infrequent, mainly slight nausea. One woman taking the placebo gave up because of severe nausea.
Effects of interventions
Five trials involving 352 women were included. The trials were of moderate quality. (Five reports from an updated search in October 2009 have been added to Studies awaiting classification.) Calcium (mainly as calcium lactate) stopped leg cramps in all but 21 of 99 women compared with 39 of 108 women given either no treatment or placebo (odds ratio 0.45, 95% confidence interval 0.24 to 0.83). However, there was significant heterogeneity between these results and if the trial of 42 women comparing calcium with no treatment is excluded (Hammar 1981) i.e. where the benefit may have been a placebo effect, calcium was effective in stopping cramp in all but 19 of 78 women, compared with 19 of 87 given placebo, i.e. there is clear evidence of no benefit. One trial of 150 women comparing sodium chloride with placebo (Robinson 1947) showed a possible reduction in leg cramps: 13 of 57 women given placebo were unchanged or their cramps recurred, compared with 13 of 93 women given sodium chloride, (odds ratio 0.54, 95% confidence interval 0.23 to 1.29). If recurrences of cramp after treatment ended are excluded, sodium chloride does seem to be effective as only one woman in 93 given sodium chloride did not benefit, compared with 13 of 57 given placebo or no treatment. The same trial, this time involving 141 women (Robinson 1947), showed no difference between calcium and sodium chloride (odds ratio 1.23, 95% confidence intervals 0.47 to 3.27). Multivitamin and mineral supplements may have an effect (Thauvin 1992), two of 11 women given supplements still had cramp at term compared with 10 of 18 given placebo (odds ratio 0.23, 95% confidence intervals 0.05 to 1.01) but it is not clear which of twelve ingredients, if any, was the active one. For magnesium, the evidence that it can reduce cramp is stronger (Dahle 1995). Twenty three women of 34 given magnesium still had some cramp compared with 33 of 35 given placebo (odds ratio 0.18, 95% confidence intervals 0.05 to 0.60 ). The trial only assessed symptoms after three weeks of treatment.
Discussion
Given the frequency of leg cramps in pregnancy it is surprising how little research has been done. Only two studies of acceptable quality have been published in the past 20 years. The causes of cramp are not understood, nor why it becomes so much more common through pregnancy. This does not help the rational search for prevention and treatment. Salt loss in heat was implicated in cramp in miners and salt was added to beer, anecdotally, as treatment. Robinson 1947 gave salt supplements to pregnant women who had cramps. The dose (45 to 60g) seems today very large. There was evidence of benefit but if recurrence of cramp on stopping treatment is taken into consideration (which it was not in previous versions of this review) then the benefit appears much less. The average intake of salt is higher today than it was in UK in 1946 when Robinson carried out her trial. Given that sodium chloride can raise blood pressure it does not seem right to recommend sodium chloride as a treatment for cramp in pregnancy except perhaps in countries where the daily intake is low. Given the marked differences in the effect of calcium when compared with no treatment (Hammar 1981) and calcium when compared with placebo (Hammar 1987), it is more likely that calcium has no effect other than that of placebo and cannot therefore be recommended. Multivitamins with minerals (Thauvin 1992) may help cramp but the effect was small as was the trial and, as the product contained 12 separate ingredients, no particular constituent can be recommended.
The magnesium lactate/citrate study ( Dahle 1995) is important because it was well carried out. It shows a clear though modest benefit with extra magnesium. It also shows that there is a marked placebo effect on the frequency of leg cramps which should make anyone wary of trials which are not placebo controlled or are not properly blinded e.g. Mauss 1970.
Authors' conclusions
Implications for practice.
There is evidence that calcium supplementation is not effective in the treatment of pregnant women who suffer cramp in pregnancy. Sodium chloride when given in high doses in 1945‐1946 was found to be helpful by most women but there was a high relapse rate on stopping treatment, and there may be an adverse effect on blood pressure from taking such high doses (45‐60g daily). It is possible that one or more of the ingredients in the multivitamin/mineral tablet helps cramp but the evidence is not strong enough to recommend its use. Only with magnesium is there clear evidence of benefit: 5mmol of magnesium as a mixture of lactate and citrate in the morning and 10mmol in the evening will stop some women having cramp, and will reduce the frequency of attacks in some other women.
Implications for research.
No further research is needed on calcium supplementation. It does not work for cramp in pregnancy. More research on sodium chloride would be helpful as there is only one paper published on this treatment, in 1947. It would be helpful to know what is the minimum effective dose, and, whether this has any impact on maternal blood pressure and, if it does, whether that matters. The possible benefit of the multivitamin/mineral treatment may have been due to magnesium. If further research is carried out on dietary supplements it should be on one constituent at a time initially so it can be seen if any particular supplement is helpful on its own before any possible synergy between supplements is looked for. Venostasin (see Mauss 1970) may merit further research but this will need to be properly randomized and fully blinded given the likelihood of a large placebo effect in the treatment of this condition.
[Note: The five citations in the awaiting classification section of the review may alter the conclusions of the review once assessed.]
Feedback
Herxheimer, September 1998
Summary
Abstract: The conclusion does not follow from the review.
Background: Discussion of current hypotheses about the causes of leg cramps in pregnancy would be helpful, as would a description of the natural history of the cramps. The second sentence should begin "They" or Cramps".
Objectives: Treatments would be a better term than preparations, and consistent with the abstract.
Characteristics of included studies: More information about the study design would be helpful, and if this is not available information about the comparability of the groups should be presented. Details of how calcium and sodium was given should be included. The dose of 45g sodium chloride is very high, is it correct? Information about any adverse effects, how cramps were reported and any losses to follow up would be helpful.
Implications for practice: The comments on massage and stretching would be more appropriate in the background, and references would be helpful.
Implications for research: How would the data in the review influence the design of the suggested sodium chloride trial?
Reply
These comments have been responded to in the review update.
(Summary of response from Gavin Young, November 2001)
Contributors
Summary of comments from Andrew Herxheimer, September 1998.
Herzheimer, August 2002
Summary
In the magnesium trial did the stage of pregnancy have any relation to the effectiveness of magnesium?
It would be interesting to give more background about magnesium. Why was it tried? How might it work? Now we know that magnesium sulphate helps prevent eclampsia, has anyone ever suggested a connection between cramp and pre‐eclampsia?
Since the trials of calcium were clearly heterogeneous, as is noted under Results, a meta‐analysis is misleading and unjustified. The diamond giving a combined result should be deleted.
Reply
A response will be published when the review is updated.
Contributors
Summary of comments received from Andrew Herxheimer, August 2002.
What's new
| Date | Event | Description |
|---|---|---|
| 7 October 2015 | Amended | This review will not be updated by the currrent review team and has now been superseded by a new review on this topic (see Zhou 2015). |
History
Protocol first published: Issue 2, 1996 Review first published: Issue 2, 1996
| Date | Event | Description |
|---|---|---|
| 30 January 2013 | Amended | Contact details updated. |
| 4 July 2011 | Amended | Search updated. Five reports added to Studies awaiting classification (Griffith 1998; Kohama 2006; Nygaard 2008; Shahraki 2006; Sohrabvand 2006). |
| 3 November 2008 | Amended | Converted to new review format. |
| 31 October 2001 | New search has been performed | Two further studies have been included. One (Dahle 1995) compares magnesium supplements with placebo. The other (Thauvin 1992) compares multivitamin and mineral supplements with placebo. More detailed analysis of the three original studies has shown calcium to be ineffective and sodium to be less effective than previously thought. The background section has been enlarged. |
Notes
This review will not be updated by the currrent review team. A new review team have now prepared a new review on this topic (see Zhou 2015).
Acknowledgements
The updating of this review in 2001 was made possible because of a grant to Gavin Young from the Scientific Foundation Board of the Royal College of General Practitioners.
Data and analyses
Comparison 1. Calcium versus placebo or no treatment.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Women with persisting leg cramps | 3 | 207 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.45 [0.24, 0.83] |
1.1. Analysis.
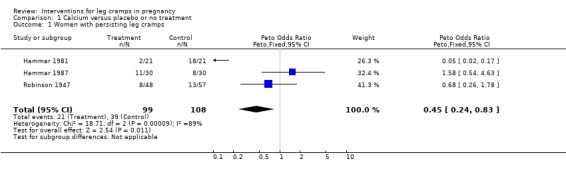
Comparison 1 Calcium versus placebo or no treatment, Outcome 1 Women with persisting leg cramps.
Comparison 2. Sodium chloride versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Women with persisting or recurring leg cramps | 1 | 150 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.54 [0.23, 1.29] |
2.1. Analysis.
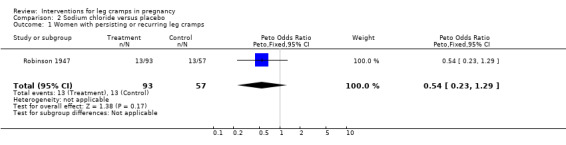
Comparison 2 Sodium chloride versus placebo, Outcome 1 Women with persisting or recurring leg cramps.
Comparison 3. Calcium versus sodium chloride.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Women with persisting leg cramps | 1 | 141 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.23 [0.47, 3.27] |
3.1. Analysis.
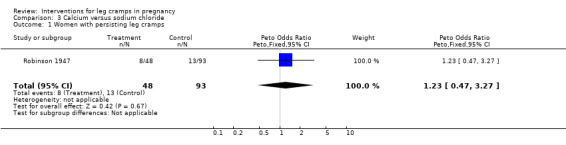
Comparison 3 Calcium versus sodium chloride, Outcome 1 Women with persisting leg cramps.
Comparison 4. Multivitamin and mineral supplements versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 women with persisting leg cramps | 1 | 29 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.23 [0.05, 1.01] |
4.1. Analysis.
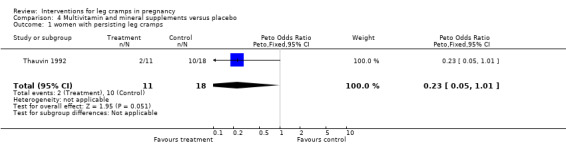
Comparison 4 Multivitamin and mineral supplements versus placebo, Outcome 1 women with persisting leg cramps.
Comparison 5. Magnesium versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 women with persisting leg cramps | 1 | 69 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.18 [0.05, 0.60] |
5.1. Analysis.
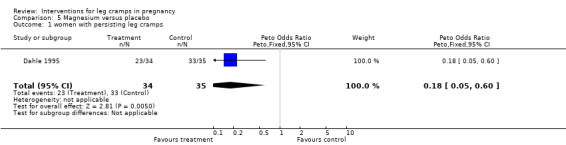
Comparison 5 Magnesium versus placebo, Outcome 1 women with persisting leg cramps.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Dahle 1995.
| Methods | Method of randomization not stated. | |
| Participants | 73 women with leg cramps at 22‐36 weeks gestation (mean = 29 ) at two separate centres in Sweden. | |
| Interventions | Magnesium lactate and citrate chewable tablets containing 5mmol Mg per tablet taken as one tablet in the morning and two in the evening for 3 weeks versus a similar regime of chewable tablets containing sorbitol/fructose/dextrose. | |
| Outcomes | Women's evaluation of whether they felt better worse or unchanged. Cramp frequency before and after treatment was also measured though not used in this review. | |
| Notes | This study is important as it shows the importance of the placebo effect. Outcome measures are provided for 69 of the 73 women who began in the study. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Hammar 1981.
| Methods | Method of allocation not stated. | |
| Participants | Women at 21‐38 weeks' gestation, with cramps at least twice weekly for a fortnight. | |
| Interventions | Oral calcium in a dose of 1gm twice daily for two weeks, versus nothing. | |
| Outcomes | Persistence of leg cramps and serum calcium. | |
| Notes | No placebo used. It is likely that the beneficial of effect shown in this study was due to the placebo effect rather than calcium itself‐see the same author's placebo controlled 1987 study. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | High risk | C ‐ Inadequate |
Hammar 1987.
| Methods | Method of allocation not stated. | |
| Participants | Women aged 18‐40, with leg cramps for more than two weeks. | |
| Interventions | Oral calcium 1gm twice daily for three weeks, versus oral vitamin C, 1gm twice daily. | |
| Outcomes | Persistence of leg cramps. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | High risk | C ‐ Inadequate |
Robinson 1947.
| Methods | By alternation. | |
| Participants | Women at antenatal clinic complaining of cramp. | |
| Interventions | Sodium chloride initially as 60g powder, later as 45g daily (3 x 15g tablets), versus three groups of control, given placebo, saccharin or calcium lactate. | |
| Outcomes | No change or no improvement in symptoms of cramp. | |
| Notes | Complex trial, with four groups. One 'control' group was given calcium lactate, which was used as treatment in other trials covered in this review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | High risk | C ‐ Inadequate |
Thauvin 1992.
| Methods | This study is not specifically described as randomized but is described as double blind and both reviewers infer that it was randomized. Attempts to contact the authors have been unsuccessful. | |
| Participants | 62 women attending an obstetric clinic at 3 months gestation in Grenoble, whether suffering cramps or not. | |
| Interventions | Supplements containing: copper gluconate 2mg, zinc gluconate 30mg, Iron gluconate 50mg, chromium chloride 50mcg, magnesium lactate 200mg, ascorbic acid (vitamin C) 50mg, thiamine nitrate (vitamin B1) 2mg, riboflavine (vitamin B2) 2mg, pyridoxyl chlorhydrate (vitamin B6) 4mg, folic acid 1mg, cyanocobalamin 2.5mcg, alpha tocopherol acetate (vitamin E ) 15mg versus placebo (no details). | |
| Outcomes | Multiple serum levels measured, not used in this review and number of women suffering cramps at term. | |
| Notes | Though 62 women began the trial, only 29 had assessment for cramp at term. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Mauss 1970 | This was a cross‐over trial (not in itself a reason for exclusion from this review) examining the effect of Venostasin (horse chestnut extract), but the study was only single‐blinded. The reasons given for the single blinding seem inadequate (that women would have failed to take the tablets properly if unsupervised). There is a strong suspicion that the lack of blinding influenced the results: no placebo effect was noted, a very unlikely result in this subject. |
| Mukherjee 1997 | This study of calcium supplementation is only published as a 17 line abstract. Attempts to contact the authors for further details have failed. The studied was only quasi‐randomized, by alternate allocation. |
| Odendaal 1974 | Another study of calcium supplementation. The methodology is complex, women being offered calcium or placebo and further courses being offered if treatment was considered effective. The data could not be used in this review as it was not possible to work out how many women were entered in the trial. |
Contributions of authors
All the studies were read and analyzed by both reviewers. Gavin Young entered the data and wrote the text.
Sources of support
Internal sources
No sources of support supplied
External sources
Royal College of General Practitioners, UK.
Declarations of interest
None known.
Edited (no change to conclusions)
References
References to studies included in this review
Dahle 1995 {published data only}
- Dahle LO, Berg G, Hammar M, Hurtig M, Larsson L. The effect or oral magnesium substitution on pregnancy‐induced leg cramps. American Journal of Obstetrics and Gynecology 1995;173:175‐80. [DOI] [PubMed] [Google Scholar]
Hammar 1981 {published data only}
- Hammar M, Larsson L, Tegler L. Calcium treatment of leg cramps in pregnancy. Acta Obstetricia et Gynecologica Scandinavica 1981;60:345‐7. [DOI] [PubMed] [Google Scholar]
Hammar 1987 {published data only}
- Hammar M, Berg G, Solheim F, Larsson L. Calcium and magnesium status in pregnant women. A comparison between treatment with calcium and vitamin C in pregnant women with leg cramps. International Journal for Vitamin and Nutrition Research 1987;57:179‐83. [PubMed] [Google Scholar]
Robinson 1947 {published data only}
- Robinson M. Cramps in pregnancy. Journal of Obstetrics and Gynaecology for the British Commonwealth 1947;54:826‐929. [DOI] [PubMed] [Google Scholar]
Thauvin 1992 {published data only}
- Thauvin E, Fusselier M, Arnaud J, Faure H, Favier M, Coudray C, et al. Effects of multivitamin mineral supplement on zinc and copper status during pregnancy. Biological Trace Element Research 1992;32:405‐14. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Mauss 1970 {published data only}
- Mauss HJ. Muscular cramp in the calf caused by pregnancy. Therapy in a blind study (translation). Medizinische Welt 1970;36:1570‐1. [PubMed] [Google Scholar]
Mukherjee 1997 {published data only}
- Mukherjee J, Jong A, Wu MY, Tsim YL. Leg cramps in pregnancy and calcium supplementation. Acta Obstetricia et Gynecologica Scandinavica 1997;76:89. [Google Scholar]
Odendaal 1974 {published data only}
- Odendaal HJ. Kalsium vir die Behandeling van Beenkrampe tydens Swangerskap. South African Medical Journal 1974;48:780‐1. [PubMed] [Google Scholar]
References to studies awaiting assessment
Griffith 1998 {published data only}
- Griffith EC, Crowther CA, Hiller JE, Wilson KJ, ACT Study Group. Leg cramps in pregnancy: ineffectiveness of calcium supplementation. 2nd Annual Congress of the Perinatal Society of Australia & New Zealand; 1998 March 30‐April 4; Alice Springs, Australia. 1998:99.
Kohama 2006 {published data only}
- Kohama T, Inoue M. Pycnogenol alleviates pain associated with pregnancy. Phytotherapy Research 2006;20(3):232‐4. [DOI] [PubMed] [Google Scholar]
Nygaard 2008 {published data only}
- Nygaard IH, Valbo A, Pethick SV, Bohmer T. Does oral magnesium substitution relieve pregnancy‐induced leg cramps?. European Journal of Obstetrics & Gynecology and Reproductive Biology 2008;141(1):23‐6. [DOI] [PubMed] [Google Scholar]
Shahraki 2006 {published data only}
- Shahraki AD. Effects of vitamin E, calcium carbonate and milk of magnesium on muscular cramps in pregnant women. Journal of Medical Sciences 2006;6(6):979‐83. [Google Scholar]
Sohrabvand 2006 {published data only}
- Sohrabvand F, Shariat M, Haghollahi F. Vitamin B supplementation for leg cramps during pregnancy. International Journal of Gynecology & Obstetrics 2006;95(1):48‐9. [DOI] [PubMed] [Google Scholar]
Additional references
Clarke 2001
- Clarke M, Oxman AD (editors). Cochrane Reviewers' Handbook 4.1 [updated July 2000]. In: Review Manager (RevMan) [Computer program]. Version 4.1 Oxford, England: The Cochrane Collaboration, 2000. Oxford: Oxford University Press.
Salvatore 1961
- Salvatore C.A. Leg cramp syndrome in pregnancy. Obstetrics and Gynecology 1961;17(5):634‐9. [PubMed] [Google Scholar]
Zhou 2015
- Zhou K, West HM, Zhang J, Xu L, Li W. Interventions for leg cramps in pregnancy. Cochrane Database of Systematic Reviews 2015, Issue 8. [DOI: 10.1002/14651858.CD010655.pub2] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Young 2001
- Young GL, Jewell D. Interventions for leg cramps in pregnancy. Cochrane Database of Systematic Reviews 2002, Issue 1. [DOI: 10.1002/14651858.CD000121] [DOI] [PubMed] [Google Scholar]