

Abstract
Background
Recent meta-analyses have demonstrated a higher adenoma detection rate using the water exchange method (WE), compared to water immersion (WI) and air/CO2 insufflation (ACI). Proximal adenomas have a high miss rate owing to their location and appearance. We performed a systematic review and meta-analysis of studies comparing the WE and WI methods to the ACI method, with a primary focus on proximal adenoma detection rate.
Methods
The following databases were searched for our systematic review: Medline, Embase, Cochrane Library, CINAHL, and Web of Sciences. We included both randomized controlled trials and cohort studies. The primary outcome was proximal adenoma detection rate, and secondary outcomes were right adenoma detection rate and cecal intubation rate.
Results
A total of 12 studies (17 arms) with 5660 patients (2260 ACI, 2281 WE, and 1119 WI) were included. A higher proximal adenoma detection rate (risk ratio [RR] 1.30, 95% confidence interval [CI] 1.11-1.53; P=0.001) and right adenoma detection rate (RR 1.43, 95%CI 1.19-1.71; P≤0.001; I2=0%) were noted for the WE group compared to the ACI group. The WI group did not demonstrate a better detection rate of proximal or right adenomas.
Conclusions
The water exchange method for colonoscopy holds promise and should be encouraged in the clinical setting to increase proximal and right adenoma detection rates. This will in turn decrease the incidence of colorectal cancer.
Keywords: Colonoscopy, proximal adenoma detection rate, right adenoma detection rate, water exchange, water immersion
Introduction
Recent years have seen the development of 2 water-aided methods, water exchange (WE) and water immersion (WI), for performing colonoscopy [1,2]. Cadoni et al defined the WE method as “a standardized technique that, through infusion and nearly simultaneous suction of water, entails substituting all colon content with a layer of clear water allowing gasless instrument progression to the cecum, minimizing distention, and maximizing cleanliness during insertion” [3]. These authors also defined the WI method as a “technique in which water is infused to facilitate cecal intubation, with limited use of insufflation when necessary. Opaque water is removed as needed to aid progression without maximizing cleanliness. Residual air pockets are used to bypass dirty content” [3]. The infused water is removed during the insertion phase in the WE method and during the withdrawal phase in the WI method [1-3]. Gas insufflation is used for the withdrawal phase in both water-aided methods [3].
Advantages of water-aided methods during colonoscopy potentially include less abdominal distension, improved mucosal visualization, and a higher rate of achieving cecal intubation, all of which should increase patient comfort and allow a thorough endoscopic examination. Rex et al also described a need for lower sedation medication dosages with the use of water-based methods [4]. Potential disadvantages of water-based methods include the increased overall procedural time, as highlighted by Cadoni et al [5]. On the other hand, the air/CO2 insufflation (ACI) method is the most prevalent and has been associated with lower rates of perforation and post-procedural pain. The ACI method is also considered essential for procedures such as endoscopic mucosal dissection, wide-field endoscopic mucosal resection, and colorectal stent placement. The biggest challenge with this method is filling a gravity-dependent colon with gas, usually carbon dioxide [4].
Adenoma detection rate (ADR) is an important quality indicator during colonoscopy [6]. An increase in ADR has been strongly linked to a decrease in the incidence of colorectal cancer (CRC) and subsequent mortality [7]. Fuccio et al compared the WE, WI and ACI methods in a comparative meta-analysis and demonstrated the superiority of the WE method over both WI and ACI in terms of overall adenoma detection rate and right colon adenoma detection rate (RADR) [8]. Another network meta-analysis by Facciorusso et al supported the use of water techniques for improving overall ADR [9]. Critically, the authors of this study did not perform an analysis of the proximal adenoma detection rate (PADR).
Proximal colon adenomas, owing to their location and nature, have higher rates of being missed during colonoscopy [10-14]. Efforts are being made to increase PADR in order to decrease the overall interval incidence of CRC [15-17]. We performed a systematic review and meta-analysis of the available literature to compare the WE, WI and ACI techniques with a focus on the PADR obtained when each of these approaches were used.
Patients and methods
Study definitions
PADR is defined as the proportion of patients with at least 1 adenoma detected proximal to the splenic flexure. RADR is defined as the proportion of patients with at least 1 adenoma detected in the cecum and/or ascending colon. The ACI method is defined as insufflation of the colon using either air or CO2, without the use of water.
Search strategy
We searched the following databases from inception through July 31st, 2019, to generate a comprehensive and up-to-date list of articles for the purposes of this systematic review: PubMed/MEDLINE, Embase, Cochrane Register of Controlled Trials, Web of Science Core Collection, and CINAHL. Controlled subject terms and keyword synonyms for the concepts of colonoscopy, adenoma/polyp detection rate, and water/underwater method were developed for PubMed and translated to the vocabularies and syntax of the other databases. The search strategy was created and performed by (WL-S) and cross checked by another reviewer (MA). Pertinent articles were finalized by 2 reviewers (MA and SS). We adhered to the PRISMA guidelines for this systematic review. The detailed search strategy for PubMed is highlighted in Supplementary Table 1 (1.1MB, tif) .
Inclusion and exclusion criteria
We restricted our systematic review to include only randomized controlled trials (RCT) and cohort studies. All other studies, including editorials, case reports, case series, and single-arm studies were excluded. Abstracts were also included in this review if they adhered to study design, i.e. RCT or cohort. Our search was not restricted to language or dates. If studies were found to contain duplicate data, the most recent available study was included.
Data collection
Baseline demographic data (age, sex), colonoscopy indication (screening/surveillance vs. diagnostic), and outcomes (PADR, RADR, and CIR) were extracted where applicable. Data extraction was performed by 2 individual reviewers (MA and SS) and cross-checked for any discrepancies.
Primary and secondary outcomes
The primary outcome of our analysis was PADR; secondary outcomes included RADR and CIR. We performed a comparative head-to-head meta-analysis of each technique for the WE, WI and ACI groups, where applicable. In addition, subgroup analysis was performed based on full articles and study design.
Statistical analysis
Data were extracted using Microsoft Excel (Microsoft, Redmond, Washington, United States). Risk ratio (RR) with 95% confidence interval (CI) were calculated for all pooled proportional outcomes. The DerSimonian-Laird method and a random-effects model were used as computing techniques and Open Meta Analyst (CEBM, University of Oxford, Oxford, United Kingdom) was used as the computing software for generating all outcomes. The fixed-effect model was used as a sensitivity tool. Heterogeneity was evaluated using the I2 statistic between the studies, defined by Cochrane handbook for systematic reviews. Percentages of 25% (I2=25), 50% (I2=50), and 75% (I2=75) were considered to represent low, moderate and high degrees of heterogeneity, respectively [18,19]. A P-value <0.05 was considered statistically significant for all outcomes between the 2 groups.
Bias assessment
Study quality was assessed using Cochrane risk-of-bias tools for RCTs and the Newcastle Ottawa score for cohort studies [20,21]. Publication bias was assessed using Egger’s regression analysis, and was displayed using funnel plots generated using Review Manager V5.3 (The Cochrane Collaboration, Oxford, United Kingdom), where applicable.
Evidence rating
We used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to rate the overall quality of evidence (high, moderate, low, very low) and provided summary of funding (SoF) Tables. We utilized GRADEpro GDT software (Evidence Prime Inc., Hamilton, Ontario, Canada) to generate the SoF Tables [22].
Results
A total of 12 studies with 17 arms were included in the final analysis for this systematic review and meta-analysis (Fig. 1) [23-34]. Of these, all were RCTs except one cohort study [32]. Nine of these studies were published as full manuscripts and 2 were published as abstracts. Two studies by Cadoni et al included data from the same RCT and hence we only included data once while comparing outcomes [26,27].
Figure 1.
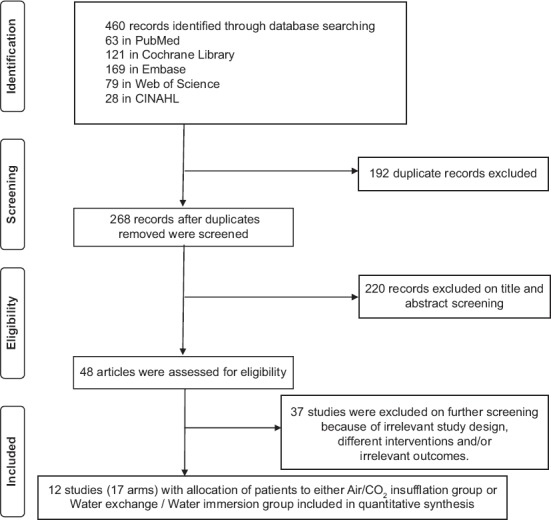
Flow diagram representing the selection of studies
The risk-of-bias assessment is shown in Supplementary Table 2 (1.4MB, tif) . All RCTs had high performance bias, as it was impossible to blind the endoscopist performing the procedure. We were unable to perform the bias assessment on the cohort study as it was an abstract. No significant publication bias was observed based on the funnel plot obtained (Supplementary Fig. 1 (566KB, tif) ) or Egger’s regression test (P=0.34).
Study details and demographics of patients are summarized in Supplementary Table 3 (1.7MB, tif) and Table 1. Of all the studies included, 11 directly compared ACI to WE [23-34] and 4 directly compared ACI to WI [26,28,30,34]. The total number of patients included in these 11 studies was 5660 (2260 ACI, 2281 WE, 1119 WI). No statistically significant difference was observed in terms of age range (54.8-63.6, 55.7-63.1, and 54.3-61) or the proportion male sex (65.3%, 64.9%, and 55.3%) across the 3 groups for ACI, WE and WI, respectively. The primary and secondary outcomes for individual studies are summarized in Table 2.
Table 1.
Demographics and characteristics of patients included in the study
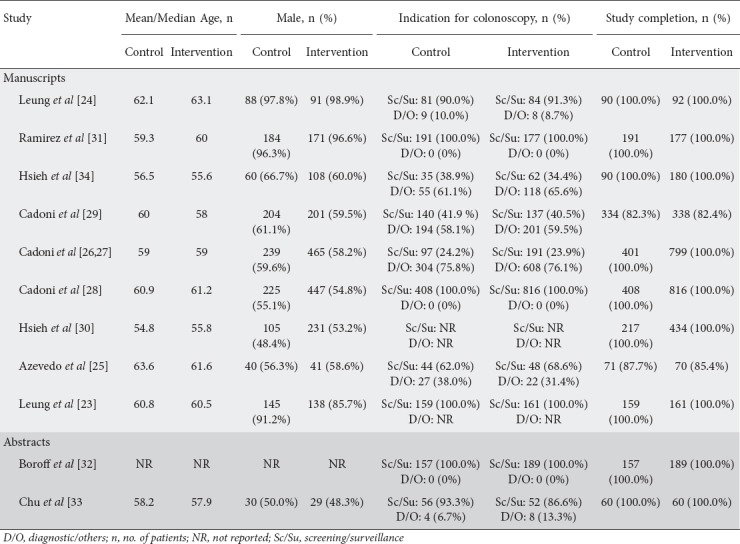
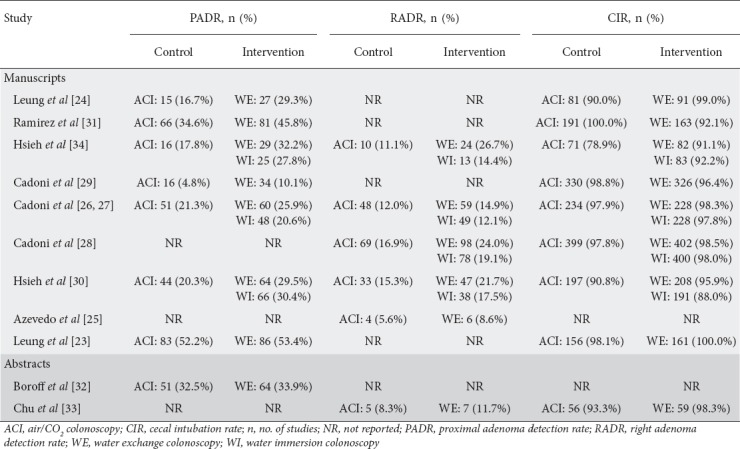
Table 2.
Primary and secondary outcomes for all studies
PADR
Overall, 8 studies reported PADR [23,24,27,29-32,34]. The 8 arms comparing WE to ACI revealed a higher PADR for the WE group (WE: 29.7%, 95%CI 21.8-41.9% vs. ACI: 23.2%, 95%CI 14.1-33.8%; RR 1.30, 95%CI 1.11-1.53; P=0.001; I2=43.5%) (Fig. 2A). Only 3 arms compared WI to ACI and found no difference in PADR between them (WI: 26.0%, 95%CI 19.4-33.3% vs. ACI: 20.3%, 95%CI 17.2-23.9%; RR 1.28, 95%CI 0.93-1.76; P=0.13; I2=48.1%) (Fig. 2B).
Figure 2.
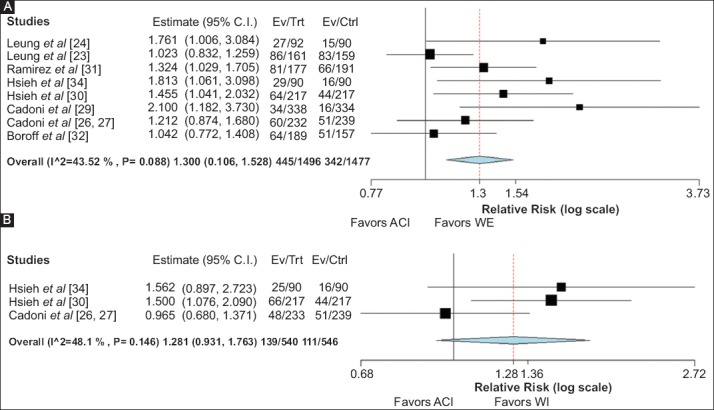
Forest plot comparing PADR in (A) WE versus ACI group (B) WI versus ACI group C.I., confidence interval; ACI, air/CO2 insufflation colonoscopy; Trt, WE group; Ctrl, ACI group; PADR, proximal adenoma detection rate; WE, water exchange colonoscopy; WI, water immersion colonoscopy
RADR
Overall 5 studies reported RADR [25,28,30,31,34]. RADR was significantly greater in the WE group compared to the ACI group, with a direct comparison in 5 arms (WE: 19.8%, 95%CI 14.6-25.4% vs. ACI: 13.8%, 95%CI 10.4-16.9%; RR 1.43, 95%CI 1.19-1.71; P≤0.001; I2=0%) (Fig. 3A). Four arms compared the WI to the ACI group and found no difference in RADR (WI: 15.9%, 95%CI 12.4-19.9% vs. ACI: 14.3%, 95%CI 11.7-17.3%; RR 1.11, 95%CI 0.91-1.35; P=0.29; I2=0%) (Fig. 3B).
Figure 3.
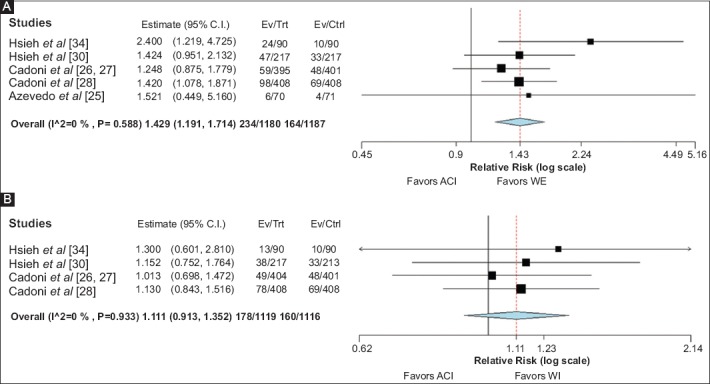
Forest plot comparing RADR in (A) WE vs. ACI group (B) WI vs. ACI group C.I., confidence interval; ACI, air/CO2 insufflation colonoscopy; Trt, WE group; Ctrl, ACI group; RADR, right adenoma detection rate; WE, water exchange colonoscopy; WI, water immersion colonoscopy
CIR
No significant difference was observed in CIR for either comparison: i.e. WE vs. ACI (97.0% vs. 95.3%, RR 1.02, 95%CI 0.99-1.05; P=0.18; I2=77.7%) (Fig. 4A) and WI vs. ACI (92.2% vs. 93.8%, RR 0.99, 95%CI 0.94-1.05; P=0.76; I2=83.3%) (Fig. 4B).
Figure 4.
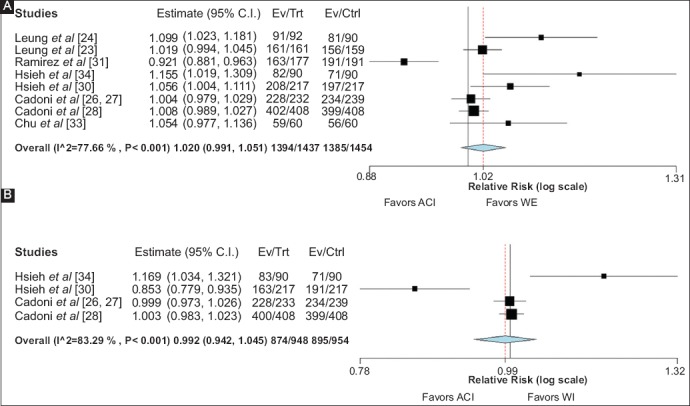
Forest plot comparing CIR in (A) WE vs. ACI group (B) WI vs. ACI group C.I., confidence interval; ACI, Air/CO2 insufflation colonoscopy; Trt, WE group; Ctrl, ACI group; CIR, cecal intubation rate; WI, water exchange colonoscopy
Subgroup analysis
A subgroup analysis of only published RCTs showed higher PADR (28.8% vs. 22.8%, RR 1.30, 95%CI 1.05-1.62; P=0.02; I2=51.5%) and RADR (19.8% vs. 13.8%, RR 1.43, 95%CI 1.19-1.71; P≤0.001; I2=0%) in the WE group compared to the ACI group. PADR for screening colonoscopies was available in 3 studies and a higher detection rate was found for the WE group; however, the results were not statistically significant (41.9% vs. 33.5 %, RR 1.31, 95%CI 0.93-1.85; P=0.13; I2=70.9%).
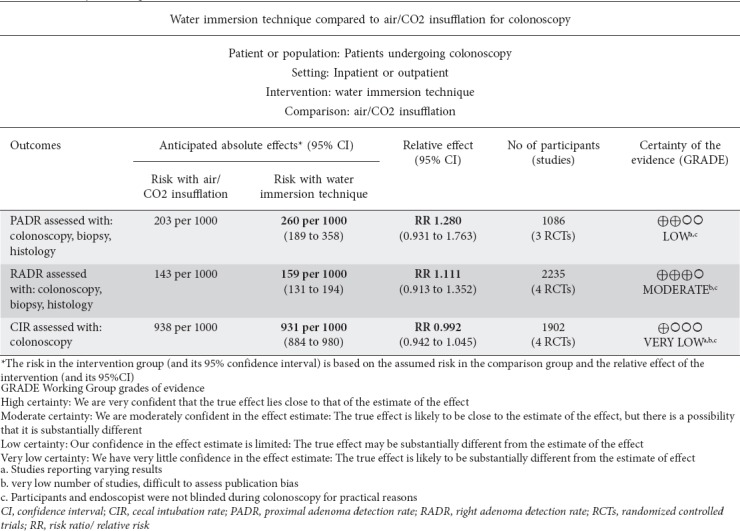
Evidence rating
Using the GRADE approach, the certainty of evidence was moderate for PADR and RADR assessed for WE vs. ACI colonoscopy (Table 3). The certainty of evidence was low and moderate for PADR and RADR, respectively, when the WI and ACI techniques were compared (Table 4).
Table 3.
Summary of findings
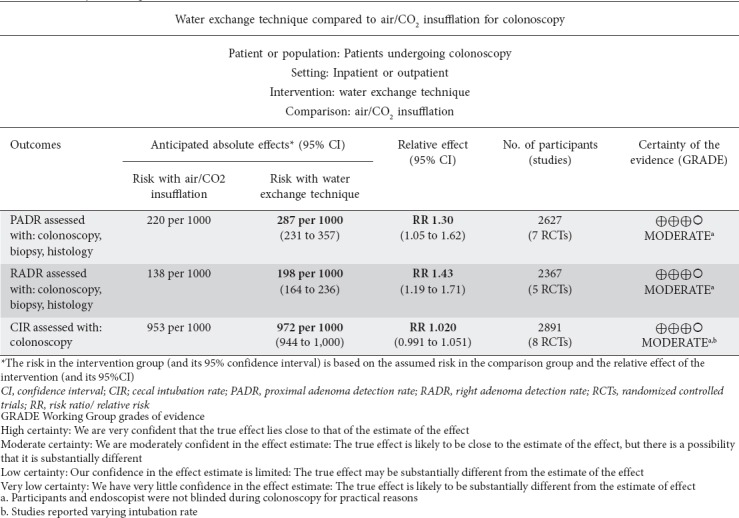
Table 4.
Summary of findings
Discussion
The results of our systematic review and meta-analysis demonstrate a greater PADR and RADR for the WE compared to the ACI method. This was also consistent with our subgroup analysis of RCTs. No difference in detection rates was observed when the WI group was compared with the ACI group.
The exact mechanism through which WE improves colonoscopy outcome metrics, such as ADR, RADR and PADR, is not fully understood. One possible theory points to the greater cleanliness throughout the colon achieved through simultaneous water infusion and suction in the WE method, as shown by Fuccio et al [8]. Another possible mechanism is the magnifying effect of water itself on the endoscope optics during the insertion phase, leading to higher detection rates [34]. Lastly, a thorough examination is possible, as the WE technique eliminates the need for constant washing and suctioning and hence reduces the incidence of luminal collapse [35]. A combination of the aforementioned factors may increase the yield of colonoscopy outcome metrics and decrease the incidence of interval CRC.
Proximal lesions can be challenging to detect, because of their location and subtle appearance. Sessile serrated adenomas/polyps (SSA/Ps), a subset of these lesions, are particularly important, as they may account for ~20% of all CRC cases [36]. Yang et al previously showed that 61.2% of SSA/Ps were found in the proximal colon [37]. This further necessitates the improvement of techniques to increase detection of these proximal lesions. Only one study directly evaluated SSA/Ps, showing a significantly greater detection rate of these lesions using the WE method compared to the ACI method (23.6% vs. 11.3%, P<0.01) [23]. Our meta-analysis is important, as we pooled data from all available studies regarding proximal adenomas and our results demonstrate the superiority of the WE method in detecting these lesions; this, in turn, should increase the detection rate for SSA/Ps.
The current meta-analysis has some limitations. Not all studies reported both PADR and RADR for each technique; however, a sufficient number of patients were analyzed to generate a pooled outcome for each metric. Our results for PADR showed some degree of heterogeneity and hence the results should be interpreted with caution. The heterogeneity can be explained by a combination of endoscopist skill, the inclusion of cohort study design, the indications for colonoscopy, procedural technicalities such as method of sedation, use of adjunctive modalities such as distal attachments or chromoendoscopy, etc. To compensate for this, we tried to limit our search criteria to exclude studies that used additional adjunctive modalities. The subgroup analysis for only RCTs also showed consistent results for both PADR and RADR using the WE method compared to the ACI method. The studies included were reported from limited institutions with expert endoscopists and the results may not be generalizable to a general population. Lastly, the impracticality of blinding the endoscopist and patient during a study does bring performance and detection bias into play. The limitations are partly attenuated by the combined statistical power of large number of studies with diverse study populations. All studies except one were RCTs and we used strict inclusion and exclusion criteria for screening studies.
In conclusion, the use of WE during colonoscopy showed significantly better PADR and RADR compared to the ACI method. Given the importance of SSA/Ps, future studies should be conducted to directly assess the use of the WE method to evaluate the detection rate of these lesions.
Summary Box.
What is already known:
The water exchange technique has been found to have significantly better detection rates for polyps and adenomas
Previous meta-analyses have demonstrated the efficacy of water exchange techniques in improving overall adenoma detection rate (ADR), right ADR (RADR), and polyp detection rate
What the new findings are:
Our meta-analysis evaluated proximal adenoma detection rate (PADR), which is another outcome metric
The water exchange technique showed significantly better PADR and RADR compared to standard (air/CO2) insufflation colonoscopy
Given the efficacy of water exchange techniques, clinicians should be encouraged to utilize them to further improve their colonoscopy outcome metrics
PubMed search strategy
Risk of bias in the included randomized controlled trials (RCTs)
Study details
Funnel plot demonstrating no visible asymmetry (signifying no publication bias), based on cecal intubation rate RR, risk ratio; SE, standard error
Biography
University of Toledo Medical Center, Ohio; University of Toledo Libraries, Ohio; University of Utah, Salt Lake City, USA
Footnotes
Conflict of Interest: None
References
- 1.Leung FW, Harker JO, Jackson G, et al. A proof-of-principle, prospective, randomized, controlled trial demonstrating improved outcomes in scheduled unsedated colonoscopy by the water method. Gastrointest Endosc. 2010;72:693–700. doi: 10.1016/j.gie.2010.05.020. [DOI] [PubMed] [Google Scholar]
- 2.Leung CW, Kaltenbach T, Soetikno R, Wu KK, Leung FW, Friedland S. Water immersion versus standard colonoscopy insertion technique:randomized trial shows promise for minimal sedation. Endoscopy. 2010;42:557–563. doi: 10.1055/s-0029-1244231. [DOI] [PubMed] [Google Scholar]
- 3.Cadoni S, Ishaq S. How to perform water-aided colonoscopy, with differences between water immersion and water exchange:a teaching video demonstration. VideoGIE. 2018;3:169–170. doi: 10.1016/j.vgie.2018.02.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rex DK. Water filling and carbon dioxide insufflation:tools for every colonoscopist. Clin Gastroenterol Hepatol. 2015;13:1981–1983. doi: 10.1016/j.cgh.2015.07.046. [DOI] [PubMed] [Google Scholar]
- 5.Cadoni S, Hassan C, Frazzoni L, Ishaq S, Leung FW. Impact of water exchange colonoscopy on endoscopy room efficiency:a systematic review and meta-analysis. Gastrointest Endosc. 2019;89:159–167. doi: 10.1016/j.gie.2018.07.020. [DOI] [PubMed] [Google Scholar]
- 6.Rex DK, Schoenfeld PS, Cohen J, et al. Quality indicators for colonoscopy. Gastrointest Endosc. 2015;81:31–53. doi: 10.1016/j.gie.2014.07.058. [DOI] [PubMed] [Google Scholar]
- 7.Kaminski MF, Wieszczy P, Rupinski M, et al. Increased rate of adenoma detection associates with reduced risk of colorectal cancer and death. Gastroenterology. 2017;153:98–105. doi: 10.1053/j.gastro.2017.04.006. [DOI] [PubMed] [Google Scholar]
- 8.Fuccio L, Frazzoni L, Hassan C, et al. Water exchange colonoscopy increases adenoma detection rate:a systematic review with network meta-analysis of randomized controlled studies. Gastrointest Endosc. 2018;88:589–597. doi: 10.1016/j.gie.2018.06.028. [DOI] [PubMed] [Google Scholar]
- 9.Facciorusso A, Triantafyllou K, Murad MH, et al. Compared abilities of endoscopic techniques to increase colon adenoma detection rates:a network meta-analysis. Clin Gastroenterol Hepatol. 2019;17:2439–2454. doi: 10.1016/j.cgh.2018.11.058. [DOI] [PubMed] [Google Scholar]
- 10.Zhao S, Wang S, Pan P, et al. Magnitude, risk factors, and factors associated with adenoma miss rate of tandem colonoscopy:a systematic review and meta-analysis. Gastroenterology. 2019;156:1661–1674. doi: 10.1053/j.gastro.2019.01.260. [DOI] [PubMed] [Google Scholar]
- 11.Lee J, Park SW, Kim YS, et al. Risk factors of missed colorectal lesions after colonoscopy. Medicine (Baltimore) 2017;96:e7468. doi: 10.1097/MD.0000000000007468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zimmermann-Fraedrich K, Sehner S, Rex DK, et al. Right-sided location not associated with missed colorectal adenomas in an individual-level reanalysis of tandem colonoscopy studies. Gastroenterology. 2019;157:660–671. doi: 10.1053/j.gastro.2019.05.011. [DOI] [PubMed] [Google Scholar]
- 13.Chokshi RV, Hovis CE, Hollander T, Early DS, Wang JS. Prevalence of missed adenomas in patients with inadequate bowel preparation on screening colonoscopy. Gastrointest Endosc. 2012;75:1197–1203. doi: 10.1016/j.gie.2012.01.005. [DOI] [PubMed] [Google Scholar]
- 14.Ahn SB, Han DS, Bae JH, Byun TJ, Kim JP, Eun CS. The miss rate for colorectal adenoma determined by quality-adjusted, back-to-back colonoscopies. Gut Liver. 2012;6:64–70. doi: 10.5009/gnl.2012.6.1.64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Klare P, Phlipsen H, Haller B, et al. Longer observation time increases adenoma detection in the proximal colon - a prospective study. Endosc Int Open. 2017;5:E1289–E1298. doi: 10.1055/s-0043-121072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Desai M, Sanchez-Yague A, Choudhary A, et al. Impact of cap-assisted colonoscopy on detection of proximal colon adenomas:systematic review and meta-analysis. Gastrointest Endosc. 2017;86:274–281. doi: 10.1016/j.gie.2017.03.1524. [DOI] [PubMed] [Google Scholar]
- 17.Aziz M, Desai M, Hassan S, et al. Improving serrated adenoma detection rate in the colon by electronic chromoendoscopy and distal attachment:systematic review and meta-analysis. Gastrointest Endosc. 2019;90:721–731. doi: 10.1016/j.gie.2019.06.041. [DOI] [PubMed] [Google Scholar]
- 18.Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Shuster J. Higgins JPT, Green S, editors. Review:Cochrane handbook for systematic reviews for interventions, Version 5.1.0, published 3/2011. Res Synth Methods. 2011;2:126–130. [Google Scholar]
- 20.Higgins JP, Altman DG, Gøtzsche PC, et al. Cochrane Statistical Methods Group. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi: 10.1136/bmj.d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Deeks JJ, Dinnes J, D'Amico R, et al. European Carotid Surgery Trial Collaborative Group. Evaluating non-randomised intervention studies. Health Technol Assess. 2003;7:iii–x. doi: 10.3310/hta7270. [DOI] [PubMed] [Google Scholar]
- 22.Zhang Y, Akl EA, Schünemann HJ. Using systematic reviews in guideline development:the GRADE approach. Res Synth Methods. 2019;10:312–329. doi: 10.1002/jrsm.1313. [DOI] [PubMed] [Google Scholar]
- 23.Leung JW, Yen AW, Jia H, et al. A prospective RCT comparing combined chromoendoscopy with water exchange (CWE) vs water exchange (WE) vs air insufflation (AI) in adenoma detection in screening colonoscopy. United European Gastroenterol J. 2019;7:477–487. doi: 10.1177/2050640619832196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Leung FW, Leung JW, Siao-Salera RM, Mann SK. The water method significantly enhances proximal diminutive adenoma detection rate in unsedated patients. J Interv Gastroenterol. 2011;1:8–13. doi: 10.4161/jig.1.1.14587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Azevedo R, Leitão C, Pinto J, et al. Can Water Exchange Improve Patient Tolerance in Unsedated Colonoscopy A Prospective Comparative Study. GE Port J Gastroenterol. 2018;25:166–174. doi: 10.1159/000484093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Cadoni S, Falt P, Sanna S, et al. Impact of colonoscopy insertion techniques on adenoma detection. Dig Dis Sci. 2016;61:2068–2075. doi: 10.1007/s10620-016-4053-1. [DOI] [PubMed] [Google Scholar]
- 27.Cadoni S, Falt P, Sanna S, et al. Insertion water exchange increases right colon adenoma and hyperplastic polyp detection rates during withdrawal. Dig Liver Dis. 2016;48:638–643. doi: 10.1016/j.dld.2016.03.004. [DOI] [PubMed] [Google Scholar]
- 28.Cadoni S, Falt P, Rondonotti E, et al. Water exchange for screening colonoscopy increases adenoma detection rate:a multicenter, double-blinded, randomized controlled trial. Endoscopy. 2017;49:456–467. doi: 10.1055/s-0043-101229. [DOI] [PubMed] [Google Scholar]
- 29.Cadoni S, Gallittu P, Sanna S, et al. A two-center randomized controlled trial of water-aided colonoscopy versus air insufflation colonoscopy. Endoscopy. 2014;46:212–218. doi: 10.1055/s-0033-1353604. [DOI] [PubMed] [Google Scholar]
- 30.Hsieh YH, Tseng CW, Hu CT, Koo M, Leung FW. Prospective multicenter randomized controlled trial comparing adenoma detection rate in colonoscopy using water exchange, water immersion, and air insufflation. Gastrointest Endosc. 2017;86:192–201. doi: 10.1016/j.gie.2016.12.005. [DOI] [PubMed] [Google Scholar]
- 31.Ramirez FC, Leung FW. A head-to-head comparison of the water vs. air method in patients undergoing screening colonoscopy. J Interv Gastroenterol. 2011;1:130–135. doi: 10.4161/jig.1.3.18512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Boroff E, Ruff KC, Ramirez FC. Sa1430:Outcomes of the water exchange technique during screening colonoscopy at an academic medical center. Gastrointest Endosc. 2015;81:AB212. [Google Scholar]
- 33.Chu VW, Li EH, Cheung ML, et al. Sa1439:Water exchange colonoscopy reduced sedation requirement without compromising success of cecal intubation in patients accepting the option of on demand sedation in Chinese patients in Hong Kong. Gastrointest Endosc. 2015;81:AB216. [Google Scholar]
- 34.Hsieh YH, Koo M, Leung FW. A patient-blinded randomized, controlled trial comparing air insufflation, water immersion, and water exchange during minimally sedated colonoscopy. Am J Gastroenterol. 2014;109:1390–1400. doi: 10.1038/ajg.2014.126. [DOI] [PubMed] [Google Scholar]
- 35.Yen AW. Insertion water exchange minimizes endoscopist multitasking during withdrawal inspection-a plausible explanation for enhanced polyp detection in the right colon. J Interv Gastroenterol. 2015;5:3. [Google Scholar]
- 36.Leggett B, Whitehall V. Role of the serrated pathway in colorectal cancer pathogenesis. Gastroenterology. 2010;138:2088–2100. doi: 10.1053/j.gastro.2009.12.066. [DOI] [PubMed] [Google Scholar]
- 37.Yang JF, Tang SJ, Lash RH, Wu R, Yang Q. Anatomic distribution of sessile serrated adenoma/polyp with and without cytologic dysplasia. Arch Pathol Lab Med. 2015;139:388–393. doi: 10.5858/arpa.2013-0523-OA. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
PubMed search strategy
Risk of bias in the included randomized controlled trials (RCTs)
Study details
Funnel plot demonstrating no visible asymmetry (signifying no publication bias), based on cecal intubation rate RR, risk ratio; SE, standard error