

Abstract
Background:
Medical error reporting is fundamental for improving patient safety. We surveyed healthcare professionals to evaluate their experience of adverse events witness and reporting, knowledge about adverse events, attitude toward own and colleagues' errors, and perceived barriers in reporting errors.
Methods:
This cross-sectional study was conducted on healthcare professionals from May to October 2017 at Chamran hospital, which is the largest referral orthopedic center in southern Iran. The self-administered questionnaire comprised 32 items covering five domains: (1) demographic and professional characteristics, (2) medical error witness and reporting, (3) actual and perceived knowledge regarding type of events and the status of completed training courses, (4) attitude toward reporting one's own and colleagues' errors, and (5) perceived barriers in error reporting. Questionnaire validity and reliability was proven in our previous study.
Results:
From a total of 210 participants, 164 returned completed questionnaires (response rate = 78.1%); 87 (53%) were physicians and 77 (47%) were nurses. Underreporting was common, particularly among physicians. Out of physicians and nurses, 57.1% and 49.4% had poor knowledge, respectively. Participants reported their own or colleagues' errors alike, but physicians tended to only provide verbal warning to their colleagues (36.8%), and nurses stated they would report the colleagues' errors, if it was serious (32.4%). Fear of blame and punishment and fear of legal ramification were the most important perceived barriers.
Conclusions:
Improvements in current medical error registry system, implementing effective educational courses, and modifying the curricula for students seem to be necessary to resolve the problem of underreporting and poor knowledge level.
Keywords: Barriers, education, health personnel, knowledge, medical errors, patient safety, quality of healthcare
Introduction
Patient safety is a fundamental constitute of medical practice, which was valued since ancient times as embedded in the Hippocratic Oath under “Do no harm”.[1] Over the decades, medicine has overcome great challenges; nonetheless, it still fails to deliver optimal care, as a considerable number of patients are subject to preventable medical errors committed by health personnel. While some errors might not be harmful, some can result in irreversible consequences leading to morbidity and mortality, as well as additional financial burden.[2,3]
Even the most skilled experts are not principally immune to unintended adverse events; however, negligence is not justifiable. Disclosure of medical errors to patients and to systems is an essential component of professional practice, which reflects upon ethical and legal accountability.[4] Error reporting systems have been developed to document the frequency, causes and the resultant harms of medical errors, which can differ in each setting.[5] By this means, detrimental and highly recurrent errors can be recognized. Notifying peers of such events helps to prevent similar incidences in the future; hence it improves the quality of care and patient safety.[6]
A major pitfall of error reporting systems is the reliance on self-reports.[7,8] Despite tremendous efforts to encourage open communication, underreporting, particularly with regards to the high-impact errors, remains a focal concern.[9] Transparency is hindered by a range of individual, organizational, and cultural obstacles. Developing a reporting culture calls for the introduction of a persuasive approach, which targets and eliminates such barriers. Thus, identifying the motivational and discouraging factors can be the first step to facilitate the collaboration of healthcare workers.[10,11]
Reports from Iranian hospitals are sporadic and diverse; however, they are an indication for the absence of a satisfactory status. In particular, barriers and preventive measures are less understood.[12] We designed the present study with the aim to evaluate key aspects of medical errors for healthcare providers including their experience of adverse events witness and reporting, knowledge about adverse events and opinion on educational needs, attitude toward own and colleagues' errors, and perceived barriers in reporting errors.
Methods
Study design and participants
This cross-sectional study was conducted on healthcare professionals from May to October 2017 at Chamran hospital (affiliated with Shiraz University of Medical Sciences, Shiraz, Iran), which is the largest referral orthopedic center in southern Iran with 13 wards, 245 inpatient beds. Paper-based medical error reporting system has been implemented in this hospital since 2010. Considering the growing web-based systems and the limitations and drawbacks of the traditional method (7), electronic reporting system was launched in 2016 besides the previous one. Both structures are in accordance to standard national and international error reporting definitions.
After obtaining a permit to visit the wards, two trained supervisors; a nurse and a physician, personally distributed and collected a self-administered questionnaire on medical error reporting. The supervisors were trained about the eligibility criteria of the participants as well as the content of the questionnaire. In order to increase the response rate, they were requested to express the goal of study and assure the participants that the result of this study would not be included in their formal annual evaluations. For this purpose, the project was presented to them as an educational needs/system assessment.
Ethical considerations
The study protocol was in accordance with the Helsinki Declaration and approved by the institutional review board. Verbal consent was obtained, and complete anonymity and data confidentiality was guaranteed.
Questionnaire
The utilized questionnaire was developed by the second author (MA) based on the reviewed relevant literatures[13,14,15] as well as an expert panel [Supplementary Table 1]. Detailed information about its validity and reliability (Cronbach's α: 0.81) has been published in our previous study (unpublished data). The tool is available in full length in the Appendix.
Supplementary Table 1.
Main questionnaire
| Part 1: Demographic and professional characteristics | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Profession: physician nurse | ||||||||||
| 2 | Duration of work experience : ….…….month | ||||||||||
| 3 | Gender: Men women | ||||||||||
| 4 | Employment status: official contract | ||||||||||
| Part 2: Experience with medical error reporting | |||||||||||
| 1 | Have you witnessed medical error within the past year? | Yes 1-2 times No | |||||||||
| 2 | Have you informally reported any medical error to your colleagues? | 3-10 times | |||||||||
| 3 | Have your colleagues informally reported any medical error to you? | >10 times | |||||||||
| 4 | Have you formally reported any medical error? | Yes No | |||||||||
| 5 | If yes, by what means? | Paper-based | |||||||||
| 6 | Which of these methods do you prefer? | Verbal/telephone Messenger Registry system |
|||||||||
| Part 3: Actual and perceived knowledge and the status of completed training courses | |||||||||||
| 1 | How much do you know about medical error? | No idea at all Scientific definition Scientific definition and classification Scientific definition and classification and identification |
|||||||||
| 2 | Non-occurrence of a potentially harmful event owing to good fortune or activation of a back-up care system. | Sentinel event Non-sentinel event |
|||||||||
| 3 | Unpredicted incident involving death or serious physical/psychological damage, or risk of a serious outcome | Harmful No harm | |||||||||
| 4 | Occurrence of an event that harmed a patient. | Near miss | |||||||||
| 5 | Occurrence of an event that did not result in patient harm, but risk of potential harm remains till the end of process. | ||||||||||
| 6 | Have you completed any educational course on definition, classification and identification of medical errors? | Yes Yes, but not enough |
|||||||||
| 7 | Have you completed any educational course on how to formally report medical errors? | No | |||||||||
| Part 4: Attitude toward one’s own and colleagues’ medical error | |||||||||||
| 1 | What would you do, if your colleague commits a medical error? | I report. I report, only if it is significant. I notify themselves, but don’t report formally. I report to other colleagues, but not formally. I don’t do anything. |
|||||||||
| 2 | Whose error are you more likely to report? | My own My colleagues’ No difference | |||||||||
| Part 5: Perceived barriers in reporting (rating from 1-10 based on significance) | |||||||||||
| 1 | I don’t know exactly what I should report. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 2 | I don’t know how to report. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 3 | Concerned about one’s lack of anonymity | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 4 | Concerned about colleagues’ lack of anonymity | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 5 | Time-consumption | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 6 | Fear of legal confrontation | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 7 | Fear of professional insecurity or punishment | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 8 | Being scolded by supervising peers | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 9 | I don’t notice any major medical errors to report. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 10 | Lack of feedback and proper future improvement | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 11 | Lack of interest in engaging in such tasks | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 12 | I don’t normally think about medical error reporting. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 13 | Medical error is inevitable; thus, it is not necessary to be reported | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
The questionnaire comprised 32 items covering five domains: (1) demographic and professional characteristics (4 items), (2) medical error witness and reporting (6 items), (3) actual and perceived knowledge regarding type of events and the status of completed training courses (7 items), (4) attitude toward reporting one's own and colleagues' errors (2 items), and (5) perceived barriers in error reporting (13 items). Barrier items consisted of individual and organizational categories. Lack of knowledge (q1, q2, q9), fear of blame (q7, q8), and cultural reasons (q11, q12, q13) were aspects related to individual barriers assessed. Lack of anonymity (q3, q4), time consumption (q5), satisfactory feedback (q10), and fear of legal ramification (q6) were aspects related to organizational barriers. Also, participants could provide an e-mail address if they wished to receive the correct answers to knowledge questions and the project results.
Herein, we clarify the scoring for knowledge and perceived barriers domains. Actual knowledge questions were scored using a two-point scale (1 = correct; 0 = incorrect). Therefore, considering that four items evaluated the actual knowledge, the sum score ranged from 0 to 4. It was classified as good, moderate, and poor based on the Bloom's cut-off point.[16,17] For perceived barriers domain, each question was rated on a scale of 1 (not important) to 10 (highly important). To evaluate the scores for each category and aspect, the average score of the related items were calculated.
Statistical analysis
Analysis was performed using SPSS 15 (SPSS, Chicago, IL, USA). Data are represented as mean ± standard deviation (SD) or proportions (%), as applicable. Chi-square test was used for inter-group comparison of quantitative variables. Multinomial logistic regression analyses were performed to identify predictive factors for participants' actual knowledge level. Correlation between actual and perceived knowledge levels was evaluated by the Kendall rank correlation coefficient. The Spearman's rank correlation coefficient was used to determine the correlation between actual knowledge level and the status of completed training courses. The scores of perceived barrier items were compared within each group using analysis of variance (ANOVA), while Tukey post hoc test was applied for pairwise comparisons. A P value <0.05 was considered as statistically significant.
Results
From a total of 210 physicians and nurses, who participated in this study, 46 were excluded as they did not return the form or submitted incomplete answers (response rate = 78.1%). Among the remaining 164 participants (61.6% female), 87 (53%) were physicians and 77 (47%) were nurses. The majority had less than 3 years' work experience (60.4%). The common area of practice was inpatient care (80.5%). Since most of the physicians were medical students and residents, employment status was not applicable for them; 37.7% of the nurses had permanent contracts, and the rest (62.3%) had temporary employment status.
Medical error witness and reporting
The reported frequency of medical error witness was significantly higher among nurses compared to physicians (P = 0.03). However, informal giving and receiving warnings were not of any significant difference (P > 0.05). Formal reporting was less usual among physicians. Moreover, while paper-based or verbal/telephone reporting was the common ways of formal reporting by the physicians, nurses tended to report via the registry system (P < 0.001). In addition, the preferred formal reporting methods showed a similar pattern in both groups (P < 0.001) [Table 1].
Table 1.
Experience of participants with medical error witness and reporting
| Items | Physicians (n=87) | Nurses (n=77) | P |
|---|---|---|---|
| Error witness | |||
| Never | 21 (24.1%) | 6 (7.8%) | 0.03 |
| 1-2 times | 32 (36.8%) | 37 (48.1%) | |
| 3-10 times | 28 (32.2%) | 26 (33.8%) | |
| >10 times | 6 (6.9%) | 8 (10.4%) | |
| Informal reporting | |||
| Never | 43 (49.4%) | 27 (35.1%) | 0.21 |
| 1-2 times | 29 (33.3%) | 28 (36.4%) | |
| 3-10 times | 11 (12.65) | 17 (22.1%) | |
| >10 times | 4 (4.6%) | 5 (6.5%) | |
| Receiving informal reports | |||
| Never | 27 (31.0%) | 23 (29.9%) | 0.84 |
| 1-2 times | 36 (4.6%) | 29 (37.7%) | |
| 3-10 times | 20 (23.0%) | 18 (23.4%) | |
| >10 times | 4 (4.6%) | 6 (7.8%) | |
| Formal reporting method | |||
| Never | 74 (87.1%) | 31 (40.8%) | <0.001 |
| Paper-based | 5 (5.9%) | 3 (3.9%) | |
| Verbal/telephone | 4 (4.7%) | 7 (9.2%) | |
| Voice messenger | 1 (1.2%) | 1 (1.3%) | |
| Registry system | 1 (1.2%) | 32 (42.1%) | |
| Preferred method | |||
| Paper-based | 27 (32.5%) | 6 (8.1%) | <0.001 |
| Verbal/telephone | 28 (33.7%) | 12 (16.2%) | |
| Voice messenger | 17 (20.5%) | 2 (2.7%) | |
| Registry system | 11 (13.3%) | 54 (73.0%) | |
Actual and perceived knowledge and completion of training courses
A single question assessed the self-perceived knowledge about familiarity with the definition, classification, and identification of medical errors with four choices as follows: (1) No idea at all, (2) know scientific definition, (3) know scientific definition and classification, and (4) know scientific definition, classification and identification. Most commonly, physicians selected choice 1 (44.7%), followed by choice 2 (30.6%), 3 (21.2%), and finally 4 (3.5%). On the other hand, nurses selected choice 3 (32.9%), 2 (26.1%), 4 (26.0%), and 1 (15.1%), respectively. The differences were statistically significant between the two groups (P < 0.001). Participants' actual knowledge regarding adverse events was classified based on the Bloom's cut-off point. Only 13.8% of physicians and 10.8% of nurses had good knowledge level. There were no statistically significant differences (P = 0.23) [Table 2].
Table 2.
Participants’ actual and perceived knowledge and completion of training courses
| Items | Physicians | Nurses | P |
|---|---|---|---|
| Perceived knowledge level | |||
| No idea at all | 38 (44.7%) | 11 (15.1%) | <0.001 |
| Definition | 26 (30.6%) | 16 (26.1%) | |
| Definition and classification | 18 (21.2%) | 24 (32.9%) | |
| Definition, classification, and identification | 3 (3.5%) | 19 (26.0%) | |
| Actual knowledge level | |||
| Good | 12 (13.8%) | 8 (10.4%) | 0.23 |
| Moderate | 26 (29.9%) | 14 (18.2%) | |
| Poor | 43 (49.4%) | 44 (57.1%) | |
| Completion of training course on medical errors | |||
| Yes | 15 (17.2%) | 42 (54.5%) | 0.001 |
| Yes, but unsatisfactory | 21 (24.1%) | 23 (29.9%) | |
| No | 51 (58.6%) | 10 (13.0%) | |
| Completion of training course on reporting methods | |||
| Yes | 9 (10.3%) | 48 (62.3%) | 0.001 |
| Yes, but unsatisfactory | 14 (16.1%) | 19 (24.7%) | |
| No | 64 (73.6%) | 8 (10.4%) | |
The correlation between self-perceived and actual knowledge levels of participants were statistically non-significant (physicians: correlation coefficient = -0.04, P = 0.65; nurses: correlation coefficient = -0.13, P = 0.24). The Spearman rank correlation coefficient between completion of training courses and participants' actual knowledge within each group were weak and not statistically significant (physicians: correlation coefficient = 0.15, P = 0.17; nurses: correlation coefficient = 0.20, P = 0.11). Furthermore, the relation between participants' knowledge with demographic and professional characteristics was only statistically significant for nurses' work experience (P < 0.001). It was also the only significant predictor of nurses' knowledge after adjusting for other variables in multinomial logistic regression model.
Attitude toward reporting one's own and colleagues' errors
Participants' attitude toward reporting colleagues' medical errors was assessed by the question “What would you do if your colleague commits a medical error?” Physicians were more likely to only give verbal warning to their colleague (36.8%), or report in case of remarkably important errors (32.2%). Reporting in any situation (18.4%), reporting only to the department manager (6.9%), and taking no actions at all (5.7%) were less common. In contrast, reporting was more popular among nurses as they stated they would respectively report the colleagues' errors only in case of remarkably important incidents (32.4%), report in any situation (31.1%), only give verbal warning to their colleague (23.0%), only report to the department manager (10.8%), and finally take no actions at all (2.7%).
Regarding the question “If you were to report an error, would you report your own error or your colleague's?” around half of both physicians (49.4%) and nurses (55.3%) claimed that they would report without discrimination. However, physicians showed greater tendency to report colleague's error (30.6%) versus their own (20.0%), in contrast to the nurses (38.2% for own error vs. 6.6% for colleague's error), (P < 0.001).
Perceived barriers in error reporting
Organizational barriers were shown to be of higher influence as compared with the individual barriers (physicians: 5.3 ± 2.2 vs. 4.7 ± 1.6; nurses: 4.4 ± 2.2 vs. 3.6 ± 1.7). Figure 1 demonstrates the findings. Fear of blame and punishment, lack of feedback, and fear of legal ramification were the most important aspects from the physicians' perspective. The average values of these aspects were significantly higher than cultural aspect (P < 0.05). Fear of legal ramification, fear of blame and punishment, and lack of anonymity were the most important aspect to nurses. The average values of these aspects were significantly higher than lack of knowledge and cultural aspects (P < 0.05).
Figure 1.
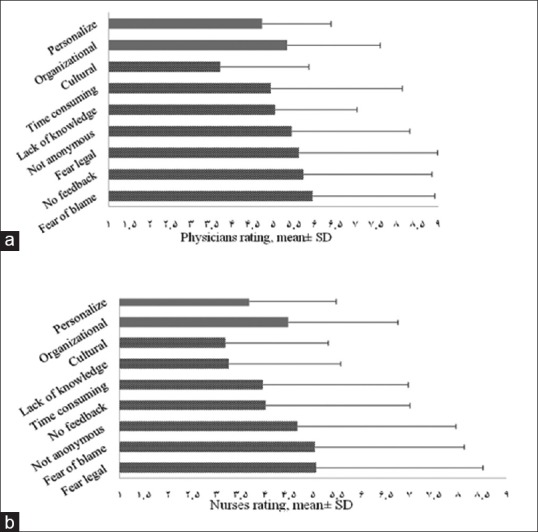
(a and b). Rating to medical error reporting barriers by physicians and nurses, Organizational perceived barrier includes no feedback (q10), legal fear (q6), no anonymous (q3, q4) and, time consuming (q5); Personalize perceived barrier includes fear of blame (q7, q8), lack of knowledge (q1, q2, q9) and cultural (q11, q12, q13)
Discussion
Despite widespread preventive measurements, medical errors continue to burden patients by prolonged hospital stay, disability, or even premature mortality.[7] The purpose of this study was to explore the experience of healthcare professionals with witness and reporting of medical errors, assess their knowledge and attitude toward adverse events, and investigate existing barriers in reporting.
We found that the majority of participants had witnessed medical errors or received informal error reports from their colleagues. Nonetheless, the frequency of formal reports to respective authorities was far less than the frequency of both witness and informal reports to peers, particularly among physicians. In fact, this finding is in line with previous reports. Jeanmonod et al. stated that from a total of 263 annual error reports in their center, 51% were registered by nurses, 27% by medical technicians, 19% by other personnel, 2% by mid-level providers, and 1% by physicians.[8] Another study by Bayazidi et al. showed that the true rate of medication errors by nurses was much higher than the rate of their reports.[18] In a study on pediatricians by Garbutt et al., it was shown that the majority of participants had been involved in an error, more often minor or near-miss ones, but they were more likely to report serious ones.[19] These results mean that despite widespread recognition of reporting barriers in different studies, the problem of under-reporting is in place.
Another interesting finding in our study was the preference of nurses for registry system as opposed to physicians, who favored paper-based and verbal/telephone methods for formal reporting. This result was in concordance with claim of our nurses regarding completion of training courses on reporting methods. Other possible reasons could be better compliance with organizational guidelines and more free time among nurses compared to physicians.
Even though a great proportion of participants claimed they had acceptable knowledge about the definition and classification of medical errors, physician and nurse knowledge scores were in poor level. Moreover, the correlation coefficient between the status of completed training courses and participants' actual knowledge was weak and non-significant. As a result, curricula modification and improving the efficacy of training methods seem to be necessary. We did not find any similar investigations about knowledge level and its correlates.
Although we found that half of the participants would report their own or colleagues' errors alike, physicians tended to only give verbal warning to their colleagues, and nurses stated that they would report the colleagues' errors, only if it was serious. Most respondents in a study by Kaldjian et al. believed that error reporting improves the quality of care (84.3%), hence, would willingly report hypothetical errors resulting in minor (73%) or major (92%) harm to a patient.[20] This supports the possibility that underreporting among our participants might be due to not knowing how and which errors to report.
In our survey, organizational barriers outweighed the individual ones. Fear of blame and punishment, lack of feedback, and fear of legal ramification were the most important barriers from physicians' perspective. On the other hand, fear of legal ramification, fear of blame and punishment, and lack of anonymity concerned nurses more than other items. This is supported to some extent by several studies. Soydemir et al. suggested that fear, the attitude of administration, system-related difficulties, and the error perceptions were the major barriers.[21] Fear was also the key barrier in a study by Chiang et al.[22] Tobaiqy et al. identified lack of awareness about the reporting policy, time constraints, and poor access to the reporting form as chief barriers.[23] Samsiah et al. mentioned that even though healthcare practitioners in primary care clinics recognized the importance of error reporting for patient safety, their decision to do so was primarily influenced by the severity of error consequences. They would eagerly report errors, if they were familiar with the system and forms, indicated errors, and timing of reporting.[24] Another study showed that nurses' perceived barriers were blaming individuals instead of the system, consequences of reporting errors, and fear of reprimand and punishment.[18] According to Flotta et al., physicians were reluctant to report due to system failures, workload, stress, or fatigue.[25] Lack of familiarity with and accessibility to reporting systems was the main reason for underreporting medication errors in a study by Abdel-Latif.[26]
Such extensive efforts attempting to shed light on barriers to medical error reporting designates that this issue has unique characteristics in each healthcare center or in each culture. Moreover, awareness of barriers does not guarantee the feasibility of their elimination, thus strict plans are required to resolve the issue.
To the best of our knowledge, this is the first study that has evaluated main aspects of medical errors in our region; healthcare professionals' knowledge, status of training courses, and top barriers. In addition, we ensured participants that the results would not influence their career to increase their participation rate. The main limitation of our study was about generalizability of the results. Second, our findings about error witness or reporting were based on self-report and we did not have access to hospital registry system for data checking or comparison.
Conclusions
Our results revealed underreporting and poor knowledge level regarding adverse events among our healthcare professionals. We recommend improving the current medical errors registry system along with employing persuasive mechanisms to utilize it, implementing effective educational courses, and modifying the curricula for students. These steps could be effective in proper knowledge translation to positive attitude and perfect practice.
Financial support and sponsorship
This research was funded by the Shiraz University of Medical Sciences, Shiraz, Iran (code: 95-01-56-13424).
Conflicts of interest
There are no conflicts of interest.
Contributions
All authors have contributed equally to this work and have approved the final article. All authors fulfill the criteria of authorship.
Acknowledgments
We would like to show our gratitude to the hospital administrators for providing the essential logistic supports and all the staff at Chamran Hospital, especially Ms. Zare.
References
- 1.Edelstein L. The Hippocratic oath, text, translation and interpretation. 1943 [Google Scholar]
- 2.Jha AK, Larizgoitia I, Audera-Lopez C, Prasopa-Plaizier N, Waters H, Bates DW. The global burden of unsafe medical care: Analytic modelling of observational studies. BMJ Qual Saf. 2013 doi: 10.1136/bmjqs-2012-001748. doi: 101136/bmjqs-2012-001748. [DOI] [PubMed] [Google Scholar]
- 3.Makary MA, Daniel M. Medical error-the third leading cause of death in the US. BMJ. 2016:353. doi: 10.1136/bmj.i2139. [DOI] [PubMed] [Google Scholar]
- 4.Kalra J, Kalra N, Baniak N. Medical error, disclosure and patient safety: A global view of quality care. Clin Biochem. 2013;46:1161–9. doi: 10.1016/j.clinbiochem.2013.03.025. [DOI] [PubMed] [Google Scholar]
- 5.Holden RJ, Karsh B-T. A review of medical error reporting system design considerations and a proposed cross-level systems research framework. Hum Factors. 2007;49:257–76. doi: 10.1518/001872007X312487. [DOI] [PubMed] [Google Scholar]
- 6.Donaldson MS, Corrigan JM, Kohn LT. To err is Human: Building a Safer Health System. National Academies Press; 2000. [PubMed] [Google Scholar]
- 7.Askarian M, Ghoreishi M, Haghighinejad HA, Palenik CJ, Ghodsi M. Evaluation of a web-based error reporting surveillance system in a large Iranian hospital. Arch Iran Med. 2017;20:511–7. [PubMed] [Google Scholar]
- 8.Jeanmonod R, Katz B. Error reporting in the emergency department: Do we do what we say we do? World J Emerg Med. 2012;3:261–4. doi: 10.5847/wjem.j.issn.1920-8642.2012.04.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Noble DJ, Pronovost PJ. Underreporting of patient safety incidents reduces health care's ability to quantify and accurately measure harm reduction. J Patient Saf. 2010;6:247–50. doi: 10.1097/pts.0b013e3181fd1697. [DOI] [PubMed] [Google Scholar]
- 10.Perez B, Knych SA, Weaver SJ, Liberman A, Abel EM, Oetjen D, et al. Understanding the barriers to physician error reporting and disclosure: A systemic approach to a systemic problem. J Patient Safe. 2014;10:45–51. doi: 10.1097/PTS.0b013e31829e4b68. [DOI] [PubMed] [Google Scholar]
- 11.Vrbnjak D, Denieffe S, O'Gorman C, Pajnkihar M. Barriers to reporting medication errors and near misses among nurses: A systematic review. Int J Nurs Stud. 2016;63:162–78. doi: 10.1016/j.ijnurstu.2016.08.019. [DOI] [PubMed] [Google Scholar]
- 12.Mansouri A, Ahmadvand A, Hadjibabaie M, Kargar M, Javadi M, Gholami K. Types and severity of medication errors in Iran; a review of the current literature. DARU. 2013;21:49. doi: 10.1186/2008-2231-21-49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Evans SM, Berry J, Smith B, Esterman A, Selim P, O'shaughnessy J, et al. Attitudes and barriers to incident reporting: A collaborative hospital study. Qual Saf Health Care. 2006;15:39–43. doi: 10.1136/qshc.2004.012559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Waring JJ. Beyond blame: Cultural barriers to medical incident reporting. Soc Sci Med. 2005;60:1927–35. doi: 10.1016/j.socscimed.2004.08.055. [DOI] [PubMed] [Google Scholar]
- 15.Wilson B, Bekker H, Fylan F. Reporting of clinical adverse events scale: A measure of doctor and nurse attitudes to adverse event reporting. Qual Saf Health Care. 2008;17:364–7. doi: 10.1136/qshc.2006.021691. [DOI] [PubMed] [Google Scholar]
- 16.Hwaid AH. Knowledge and awareness of papillomavirus and cervical cancer among college students and health care workers women in Diyala, Iraq. Am J Public Health Res. 2013;1:221–5. [Google Scholar]
- 17.Mahdaviazad H, Keshtkar V, Emami MJ. Osteoporosis guideline awareness among Iranian family physicians: Results of a knowledge, attitudes, and practices survey. Prim Health Care Res Dev. 2018:19;485–91. doi: 10.1017/S1463423618000014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bayazidi S, Zarezadeh Y, Zamanzadeh V, Parvan K. Medication error reporting rate and its barriers and facilitators among nurses. J Caring Sci. 2012;1:231–6. doi: 10.5681/jcs.2012.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Garbutt J, Brownstein DR, Klein EJ, Waterman A, Krauss MJ, Marcuse EK, et al. Reporting and disclosing medical errors: Pediatricians' attitudes and behaviors. Arch Pediatr Adolesc Med. 2007;161:179–85. doi: 10.1001/archpedi.161.2.179. [DOI] [PubMed] [Google Scholar]
- 20.Kaldjian LC, Jones EW, Wu BJ, Forman-Hoffman VL, Levi BH, Rosenthal GE. Reporting medical errors to improve patient safety: A survey of physicians in teaching hospitals. Arch Intern Med. 2008;168:40–6. doi: 10.1001/archinternmed.2007.12. [DOI] [PubMed] [Google Scholar]
- 21.Soydemir D, Seren Intepeler S, Mert H. Barriers to medical error reporting for physicians and nurses. West J Nurs Res. 2017;39:1348–63. doi: 10.1177/0193945916671934. [DOI] [PubMed] [Google Scholar]
- 22.Chiang HY, Pepper GA. Barriers to nurses' reporting of medication administration errors in Taiwan. J Nurs Scholarsh. 2006;38:392–9. doi: 10.1111/j.1547-5069.2006.00133.x. [DOI] [PubMed] [Google Scholar]
- 23.Tobaiqy M, Stewart D. Exploring health professionals' experiences of medication errors in Saudi Arabia. Int J Clin Pharm. 2013;35:542–5. doi: 10.1007/s11096-013-9781-0. [DOI] [PubMed] [Google Scholar]
- 24.Samsiah A, Othman N, Jamshed S, Hassali MA. Perceptions and attitudes towards medication error reporting in primary care clinics: A qualitative study in Malaysia. PloS One. 2016;11:e0166114. doi: 10.1371/journal.pone.0166114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Flotta D, Rizza P, Bianco A, Pileggi C, Pavia M. Patient safety and medical errors: Knowledge, attitudes and behavior among Italian hospital physicians. Int J Qual Health Care. 2012;24:258–65. doi: 10.1093/intqhc/mzs014. [DOI] [PubMed] [Google Scholar]
- 26.Abdel-Latif MM. Knowledge of healthcare professionals about medication errors in hospitals. J Basic Clin Pharm. 2016;7:87–92. doi: 10.4103/0976-0105.183264. [DOI] [PMC free article] [PubMed] [Google Scholar]