

Abstract
Streptococcus intermedius is a Gram-positive cocci, normally found in the oral cavity and gastrointestinal tract. It has been associated with deep-seated purulent abscesses commonly in the brain or liver in immunocompromised patients. Here, we discuss the case of a 21-year-old immunocompetent patient that presented with septic shock in the setting of multiple pyogenic liver abscesses with positive blood cultures for S. intermedius. The patient had a dental cleaning 3 months prior to admission. The abscesses resolved with ultrasound guided drainage and antibiotic therapy.
Keywords: infections, infection (gastroenterology), hepatitis and other GI infections
Background
Streptococcus intermedius, a Gram-positive, non-motile catalase negative bacterium, is a member of the Streptococcus anginosus group, also referred to as the ‘Streptococcus milleri’ group.1–4 The S. anginosus group is part of the oral cavity and GI tract normal flora.1–3 S. intermedius is a cause of abscesses in the liver and brain and rarely in the spleen.4 5 The majority of patients with liver abscesses in the setting of S. intermedius bacteremia have an immunocompromised state such as underlying diabetes, HIV, or are parenteral drug users.3 4
Pyogenic liver abscesses following dental extractions as part of the treatment for pyogenic dental infections in otherwise healthy individuals have been reported but are rare.1 We hereby report the case of an otherwise healthy 21-year-old man who developed S. intermedius bacteremia after a routine dental cleaning 3 months prior. This case raises the concerns that routine dental cleanings are not necessarily always benign and highlights that even immunocompetent individuals are not immune to developing S. intermedius sepsis.
Case presentation
A 21-year-old man without significant medical history and no history of drug abuse was admitted to the hospital with a 3-week history of intermittent fever up to 400C, fatigue and right upper quadrant (RUQ) abdominal pain. Two days prior to admission, the patient experienced stabbing RUQ pain, which prompted him to seek evaluation. He also had a routine dental cleaning 3 months prior, with no teeth extractions.
On admission, his blood pressure was 88/53 mm Hg with heart rate of 142/min, temperature of 38.7°C and oxygen saturation 90% on 2 L of O2/min by nasal cannula. RUQ tenderness and hepatomegaly were noted on physical examination without rebound tenderness, guarding or rigidity. The rest of his physical examination was unremarkable.
Investigations
At the time of presentation, the patient had a leukocytosis of 16×109/L (normal 3.3–10.7×109/L), haemoglobin of 123 g/L (normal 121–150 g/L) and a platelet count of 62×109/L (normal 150 –400×109/L). His serum creatinine was elevated to 2.66 mg/dL (normal 0.5–1.10 mg/dL). His sodium was 127 mEq/L (normal 135–145 mEq/L). His liver enzymes were remarkable for an elevation of alkaline phosphatase (ALP) of 573 U/L (normal 33–120 U/L), aspartate aminotransferase (AST) of 102 U/L (normal 0–34 U/L), alanine aminotransferase (ALT) of 65 U/L (normal 9–47 U/L) and total bilirubin of 1.8 mg/dL (normal 0.3–1.2 mg/dL). Serum lipase was 71 U/L (normal 7–60 U/L). Serum pro-calcitonin was >200 ng/mL. Ferritin was 1747 ng/mL (normal 12.0–207.0). Lactic acid was elevated at 4.9 mmol/L (normal 0.5–2.2 mmol/L). Hepatitis A, B and C serologies were negative. Non-contrast enhanced CT of the abdomen and pelvis showed one versus two foci measuring 10.7×6.1 cm, an additional hepatic foci measuring 3.8 cm and splenomegaly up to 18.8 cm (figure 1). An ultrasound of the abdomen showed three complex hepatic masses, measuring 7.3×6.0×7.2 cm, 5.0 cm and 4.1 cm, respectively (figure 2). Vancomycin, piperacillin/tazobactam and intravenous fluids were started. Two sets of blood cultures returned positive for Gram-positive cocci in chains identified later as S. intermedius.
Figure 1.
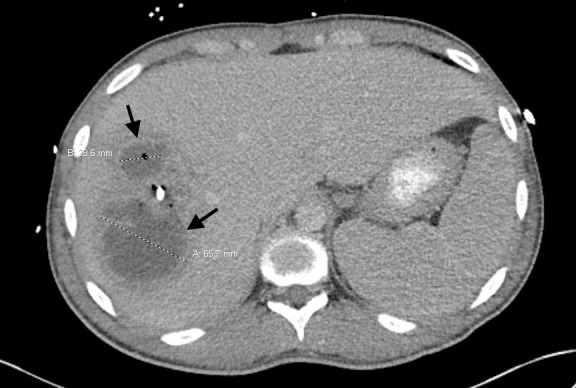
CT of the abdomen/pelvis at initial presentation with arrows pointing at a low attenuation focus versus two adjacent foci measuring 10.7×6.1 cm and an additional hepatic low attenuation focus measuring 3.8 cm, and splenomegaly up to 18.8 cm.
Figure 2.
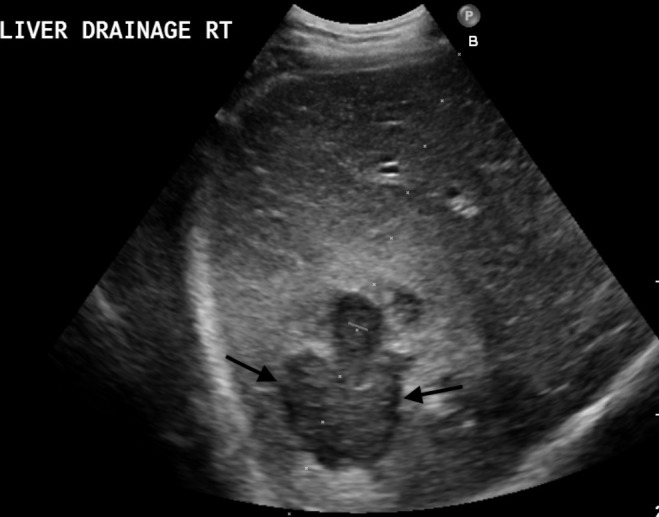
Ultrasound of the abdomen at initial presentation with arrows pointing towards the largest hepatic mass, measuring 7.3×6.0×7.2 cm.
Treatment
Ultrasound-guided aspiration was performed for the 7.3 cm abscess and pigtail catheter was also placed for continuous drainage. Antibiotic regimen was changed to ampicillin–sulbactam 3 g every 6 hours during the remainder of his hospitalisation and he was discharged with a 6-week course of ertapenem 1 g every 24 hours.
Outcome and follow-up
Six weeks after initial admission, follow-up CT scan showed a decrease in hepatic abscess size from 7.3 to 4.6 cm (figure 3); at this time, his antibiotic regimen was changed from ertapenem to amoxicillin/clavulanic acid 875–125 mg one tablet every 12 hours for an additional 2 months. Follow-up CT scans at 3 and 4 months showed further decreases in abscess size: 3.5 and 3.0 cm, respectively. He was taken off of antibiotics after 4 months from initial admission and was observed clinically. A final CT scan at 5 months after admission showed an abscess size of 1.9 cm. Patient fully recovered with no known complications.
Figure 3.

CT of the abdomen/pelvis at 2 months after initial presentation, with arrows showing interval decrease in size of largest hepatic abscess to 4.6×4.4 cm.
Discussion
The case reported was particularly interesting as it occurred in an immunocompetent young man in the setting of routine dental cleaning 3 months prior. While other case studies have reported liver abscesses from S. intermedius after dental cleaning, typical latency is 1 month from the dental cleaning while much longer latency is noted in the reported case.1 3 This suggests that it may take quite some time for micro-abscesses to form from S. intermedius bacteremia. Knowing the possible prolonged length of latency for abscess formation in addition to common presenting symptoms should assist in making an early diagnosis. As shown in table 1, common presenting symptoms are variable and may include fevers, abdominal pain, nausea, vomiting or diarrhoea.
Table 1.
Case reports of pyogenic liver abscesses associated with S t reptococcus intermedius bacteremia for the past 10 years on PubMed, including age and gender, chief complaint, number of liver abscesses, size of liver abscesses, antibiotic regimen and length of treatment1 3 8 9
| Author and date | Age and gender | Presenting chief complaint | Number and size of liver abscesses | Treatment | Total treatment length | Outcome | |
| 1 | Neumayr et al 1 | 18-year-old man | RUQ abdominal pain and remittent fevers | 3 (largest measuring 9.8×9.5×9.8 cm) | Initial: Intravenous imipenem and penicillin G (dosing not reported) Final: Oral levofloxacin and metronidazole |
7 weeks | Ultrasound of abdomen 35 days later showing minimal residual of one abscess, all others resolved |
| 2 | Livingston and Perez-Colon3 | 65-year-old man | RUQ abdominal pain, diarrhoea, nausea and poor appetite | 1 (10.2×7.4×9.4 cm) | Initial: Intravenous iprofloxacin 400 mg every 12 hours and intravenous metronidazole 500 mg every 8 hours Final: Intravenous ceftriaxone 2 g daily |
4 weeks | No follow-up imaging; significant clinical improvement |
| 3 | Tran et al 8 | 24-year-old man | Fevers, chills, myalgias and abdominal pain | Multiple-exact number and size unspecified | Initial: Intravenous ceftriaxone 2 g daily and azithromycin 500 mg daily Final: Penicillin 24 million units daily and low dose gentamicin |
6 months | No follow-up imaging; significant clinical improvement |
| 4 | Tran et al 8 | 53-year-old woman | Nausea, vomiting, diarrhoea and weight loss | Multiple-exact number unspecified (largest measuring 10×9.9 cm) | Initial: Imipenem 500 mg every 8 hours Final: Ceftriaxone 2 g daily |
6 months | CT abdomen/pelvis 6 months later showing resolution of liver abscesses |
| 5 | Reddy et al 9 | 50-year-old man | Generalised abdominal pain, nausea, vomiting, diarrhoea and fever | 4, size unspecified | Initial: Intravenous levofloxacin and intravenous metronidazole (dosing not reported) Final: Intravenous meropenem |
6 weeks | CT abdomen/pelvis 9 months later showing complete resolution of hepatic abscesses |
RUQ, right upper quadrant.
An important point from this case is that patients who are otherwise healthy yet presenting with sepsis should undergo a thorough history that includes inquiring about any recent dental work. Although considered to be safe in the vast majority of cases, any dental work, even a routine cleaning, may predispose an individual to suppurative infection. Livingston and Perez-Colon report a similar case in which a 65-year-old immunocompetent man underwent a dental cleaning 1.5 months prior to presenting to the hospital with RUQ pain. He was found to have a 10.2×7.4×9.4 cm cystic lesion demonstrating multiple internal thickened septations within the right hepatic lobe on ultrasound of the abdomen.3 He had no other risk factors for developing a hepatic abscess. Both blood and fluid cultures grew S. intermedius.
Furthermore, in any patient presenting with S. intermedius bacteremia, regardless of immune state, there should be a high index of suspicion for pyogenic abscesses in the liver and/or brain. It is also important to note that even if a patient is found to have an abscess in the liver, this does not automatically rule out the possibility of abscesses elsewhere in the body.4 5 A thorough review of systems in these patients is critical to identifying all areas of bacterial seeding.
Once diagnosis of pyogenic liver abscess is confirmed, it is imperative that the patient receive appropriate antimicrobial therapy as well as percutaneous aspiration if indicated. Generally, hepatic abscesses less than 3–5 cm can be treated with antibiotics alone and do not require percutaneous drainage.6 Until a specific organism can be identified, broad-spectrum antibiotic therapy is indicated, as a pyogenic liver abscess left untreated can become fatal. The vast majority of S. milleri group bacteria are susceptible to penicillins; there is no standard therapy; however, intravenous ampicillin with sulbactam and oral amoxicillin with clavulanate are common therapy choices.7 Currently, there is no set standard length of antibiotic therapy for S. intermedius associated pyogenic liver abscesses; however, it is reasonable to use clinical symptoms to help guide duration. In the patient discussed above, his liver abscess persisted despite greater than 3 months of antibiotic therapy; however, antibiotics were ultimately discontinued as he continued to improve with no symptoms. On reviewing other cases in the literature, it may be reasonable to administer antibiotics for 4–6 weeks and monitor off of therapy after this time duration, even with evidence of persistent abscess. As evidenced by table 1, there are several cases in which a variety of both antibiotic therapies and shorter length of treatment resulted in clinical resolution.
Learning points.
S treptococcus intermedius, although commonly known to cause suppurative infection in immunocompromised patients, can still affect patients with immunocompetency.
Any trauma to the oral cavity, even something as benign as a routine dental cleaning, can predispose patients to developing subsequent bacteremia.
It is imperative that abscesses as potential sites of infection do not get missed, as results can be fatal.
There are currently no standard antibiotic regimens or durations of therapy that are appropriate to treat S. intermedius associated abscesses, and this may be researched in the future.
Footnotes
Twitter: @bhavinddalal
Contributors: AH and FO assisted in writing the article and assisted in the literature search. ZI and BD assisted in writing and revising the article critically.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Patient consent for publication: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Neumayr A, Kubitz R, Bode JG, et al. Multiple liver abscesses with isolation of Streptococcus intermedius related to a pyogenic dental infection in an immuno-competent patient. Eur J Med Res 2010;15:319–22. 10.1186/2047-783X-15-7-319 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Whiley RA, Beighton D, Winstanley TG, et al. Streptococcus intermedius, streptococcus constellatus, and streptococcus anginosus (the streptococcus milleri group): association with different body sites and clinical infections. J Clin Microbiol 1992;30:243–4. 10.1128/JCM.30.1.243-244.1992 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Livingston LV, Perez-Colon E. Streptococcus intermedius bacteremia and liver abscess following a routine dental cleaning. Case Rep Infect Dis 2014;2014:1–4. 10.1155/2014/954046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Sánchez-Porto A, Torres-Tortosa M, Canueto J, et al. [Bacteremias due to the Streptococcus milleri group. An analysis of 18 episodes]. Rev Clin Esp 1997;197:393–7. [PubMed] [Google Scholar]
- 5. Maliyil J, Caire W, Nair R, et al. Splenic abscess and multiple brain abscesses caused by Streptococcus intermedius in a young healthy man. Proc 2011;24:195–9. 10.1080/08998280.2011.11928714 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Lardière-Deguelte S, Ragot E, Amroun K, et al. Hepatic abscess: diagnosis and management. J Visc Surg 2015;152:231–43. 10.1016/j.jviscsurg.2015.01.013 [DOI] [PubMed] [Google Scholar]
- 7. Han JK, Kerschner JE. Streptococcus milleri: an organism for head and neck infections and abscess. Arch Otolaryngol Head Neck Surg 2001;127:650–4. 10.1001/archotol.127.6.650 [DOI] [PubMed] [Google Scholar]
- 8. Tran MP, Caldwell-McMillan M, Khalife W, et al. Streptococcus intermedius causing infective endocarditis and abscesses: a report of three cases and review of the literature. BMC Infect Dis 2008;8:154 10.1186/1471-2334-8-154 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Reddy S, Singh K, Hughes S. Liver abscesses caused by Streptococcus intermedius in an immunocompromised patient. Cureus 2018;10 10.7759/cureus.2107 [DOI] [PMC free article] [PubMed] [Google Scholar]