

SUMMARY:
Pain referred to the ear is a well-documented phenomenon, which can be due to a multitude of disease processes. With the recent and rapid progression of CT and MR imaging technology, radiologists have played an increasing role in solving this potentially difficult diagnostic dilemma. Essentially any pathology residing within the sensory net of cranial nerves V, VII, IX, and X and the upper cervical nerves C2 and C3 can potentially cause referred otalgia. This article will attempt to outline the various sensorineural pathways that dually innervate the ear and other sites within the head and neck, as well as discuss various disease processes that are known to result in referred otalgia.
Ear pain (otalgia) can be divided into 2 main categories: primary and secondary.1 Primary ear pain is an entity whereby the origin of the pain arises from the ear itself. Common disease processes resulting in primary otalgia include otomastoiditis, cholesteatoma, and foreign bodies lodged within the ear canal. In close to 50% of cases, however, the source of the pain does not reside within the ear but, rather, originates from sources distant from the ear—so called “referred otalgia” (Fig 1).1,2 The focus of our topic is the radiology of referred otalgia.
Fig 1.

Otalgia arising from head and neck sources. Essentially any pathology residing within the sensory net of cranial nerves V, VII, IX, and X and upper cervical nerves C2 and C3 can potentially cause pain referred to the ear. Reprinted with permission from the American Journal of Clinical Oncology (2003;26:e157–62).
Significance
Many cases of referred otalgia are secondary to benign processes.2 However, referred otalgia may be an early harbinger of serious underlying pathology; each case must be carefully and individually evaluated.3 Otalgia may be the earliest and only symptom of cancer lurking somewhere within the head and neck. The severity of the symptoms do not correlate with the gravity of disease: Dental caries have the capacity to produce constant boring pain ear pain, whereas laryngeal cancer may result in a much less intense earache.1,4
Diagnostic Work-Up for Referred Otalgia
In the setting of otalgia with completely negative findings on ear examination (including an unremarkable otoscopic examination and dedicated CT of the temporal bone), it is imperative that distant sources within the head and neck be evaluated. To clinicians, this may include palpating within the patient's oral cavity or performing an indirect mirror examination or fiberoptic examination of the hypopharynx and larynx.5 If the source of the patient's pain is found, no further work-up may be necessary. However, in the cases of negative findings on physical examination, CT or MR imaging may be an excellent tool to investigate further regions of the head and neck that are not easily evaluated by physical examination.5 It is, therefore, important that radiologists are cognizant of the types and locations of relevant disease processes so that they are best equipped to aid their colleagues and patients.
Mechanism of Referred Otalgia
Although the mechanism of referred otalgia is slightly controversial, the most accepted theory is the convergence-projection theory, which states that multiple nerves converge onto a single shared neural pathway, with the central nervous system (CNS) unable to differentiate the origin of stimulation.6 In referred otalgia, there is a convergence of common sensory pathways between the complex sensory innervation supplying both the ear and cranial nerves innervating the head and neck, with the CNS unable to correctly pinpoint the location of pathology.7 This sensory “error” is analogous to a patient's having pain in the medial left arm when experiencing an acute coronary syndrome or patient's feeling pain in the shoulder when, in actuality, a lesion is irritating the patient's diaphragm.7
Sensory Innervation of the Ear
The innervation to the ear is one of the most complex in the body, and a brief introduction to the neural pathways in the ear is necessary to appreciate the concept of referred otalgia. There are 4 cranial nerves and 2 upper cervical nerves that contribute to sensory innervation of the ear: cranial nerves V, VII, IX, and X and upper cervical nerves C2 and C3.8,9 Although the sensory innervation to the ear may appear fairly well defined, there is considerable overlap and ambiguity in the sensory distribution of these nerves.10
V3 supplies the tragus, helical crus, anterosuperior wall of the external canal, adjacent tympanic membrane, and temporomandibular joint.9,11 The facial nerve (VII) supplies the posterior-inferior portion of the external ear canal and adjacent tympanic membrane.9 The glossopharyngeal nerve (IX) supplies the inner ear and inner tympanic membrane, whereas the vagus nerve (X) supplies a similar distribution to IX but also innervates the concha.8,9 The upper cervical nerves (C2 and C3) innervate the skin in front of and behind the ear and also of the medial and lateral aspect of the auricle and lobule.8,9,11,12
Sources of Referred Otalgia, Grouped According to Cranial and Cervical Nerves
Cranial Nerve V3
The trigeminal nerve is cited as the most common sensorineural pathway leading to referred otalgia because of the wide sensory “net” that it covers and the type of pathology that occurs within this region.2,13 V3 innervates the ear via the auriculotemporal branch but also has sensory nerve fibers via the lingual, buccal, and inferior alveolar nerves, which serve to innervate the oral cavity and floor of mouth, lower teeth, palate, mandible including the temporomandibular joint (TMJ), and the 3 major salivary glands (Fig 2).1,7,10,12,14 Any irritative focus such as tumor, infection, or inflammation of structures within the oral cavity (specifically including the floor of mouth, cheek, anterior tongue, hard palate, and sublingual and submandibular glands), lower teeth, mandible including the TMJ, and parotid glands can all be sites of distant pathology resulting in referred otalgia.1,10
Fig 2.

Primary and referred otalgia pathways of the mandibular nerve (V3). Cranial nerve V is the most frequent pathway for referred otalgia via the auriculotemporal branch of the trigeminal nerve. Reprinted with permission from the American Journal of Clinical Oncology (2003;26:e157–62).
Within the subset of processes affecting V3, dental diseases account for most pathology causing referred otalgia.3 Plain film bite wing radiographs are still the workhorse for dental evaluation because of their superior resolution and low cost compared with conventional CT,15,16 but CT can still accurately detect periodontal disease, periapical abscesses, and condensing osteitis if dental radiographs have not been acquired by the referring physician. Periodontal disease refers to infection around the tooth, which begins at the gum line and burrows down the margin of the tooth to widen the periodontal ligament.15,16 If progressive enough, it may result in a visible radiolucency on CT surrounding the margins of the tooth. Periapical abscesses, on the other hand, develop when bacteria burrow through the substance of the tooth by eroding through the enamel, dentin, and neurovascular pulp/root canal to exit the apical foramen.15 Condensing osteitis is the result of an osseous stress response indicated by an area of increased sclerosis surrounding an infected tooth,16 which itself does not result in referred otalgia but is an indicator of periodontal or periapical infection that can produce referred otalgia. Unerupted wisdom teeth, erupting teeth, and malocclusion can likewise cause referred otalgia.14
Otalgia is listed as a chief complaint by 70%–78% of patients with TMJ disorders (Fig 3).17,18 TMJ disorders have a 2–9 times higher prevalence in women than in men and occur in both sexes between 40 and 70 years of age.19,20 It is unclear whether this is a true reflex referred ear pain secondary to direct impingement of the auriculotemporal nerve,21,22 related to masseteric muscle spasm, or secondary to a direct ligamentous connection between the TMJ and middle ear, but 1 or all of these theories may potentially explain TMJ pathology resulting in otalgia.20 Clark et al19 performed a study at the Mayo Clinic during a 9-year period and found that 164 of 222 patients with bony crepitus had signs of degenerative changes of the condyle, glenoid fossa, and/or articular eminence on plain film. However, the degree of plain film TMJ degenerative changes has little bearing on clinical symptoms.23
Fig 3.

TMJ. Coronal reformatted CT scan demonstrates severe erosion and irregularity involving the head of the left condylar process. TMJ disease has been well documented to be associated with referred otalgia via the auriculotemporal and masseteric branches of V3.
Major salivary gland pathology, particularly the parotid gland, is known to cause otalgia.2 Infectious parotitis, typically from mumps, sialolithiasis, and occasionally neoplastic processes involving the parotid gland can cause otalgia (Fig 4).1,2,4,14 If a stone is suspected within the parotid (Stensen) or submandibular (Wharton) duct, noncontrast CT, sonography, or, more recently, thin-section T2-weighted MR imaging may detect calculi.24 Contrast-enhanced scans may be useful in the detection of infectious or inflammatory processes not related to stone disease.24
Fig 4.
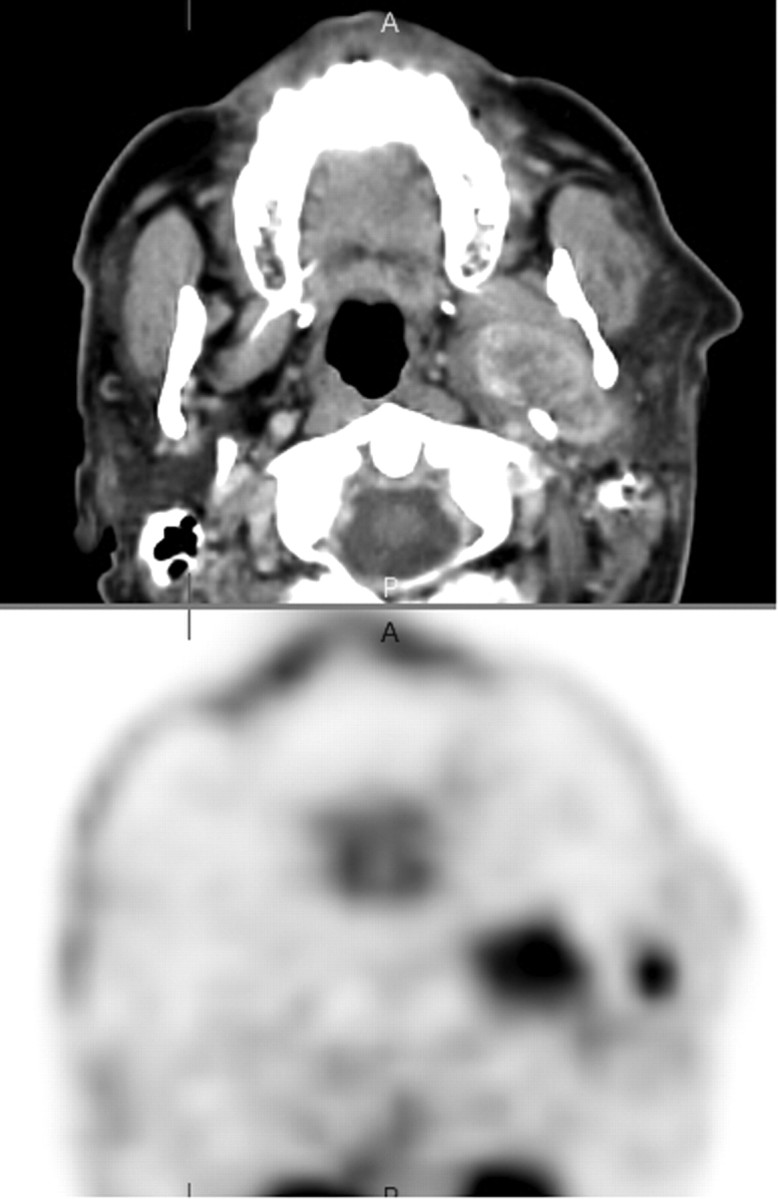
Parotid malignancy. Positron-emission tomography image demonstrates abnormal hypermetabolic activity involving the left prestyloid parapharyngeal region. The corresponding anatomic images demonstrate a calcified mass within the deep lobe of the parotid gland. The parotid branches of the auriculotemporal nerve mediate referred otalgia.
Cancer or ulceration of the anterior tongue, from a process such as aphthous ulcers, can likewise cause otalgia. These entities will typically be diagnosed by physical examination.1 Cross-sectional imaging becomes very useful in determining the local and distant spread of neoplastic disease. Important staging parameters include depth of tongue invasion, spread across the midline lingual septum, and nodal disease.25
Cranial Nerve VII
The sensory distribution of the facial nerve is variable, with an overlapping sensory distribution with the trigeminal nerve. A branch of the seventh cranial nerve, the posterior auricular nerve, serves to innervate the ear directly, whereas the greater superficial petrosal nerve and the vidian nerve serve to supply the nasal mucosa, posterior ethmoid, and sphenoid sinuses (Fig 5).12,14 Mucosal inflammation of the sphenoid and posterior ethmoid sinuses and septal spurs impinging on the nasal mucosa can cause referred otalgia, though this is probably not a common pathway (Figs 6 and 7).13,14
Fig 5.

Primary and referred otalgia pathways of the facial nerve (VII). Cranial nerve VII produces referred otalgia via the auricular branch of the facial nerve. Bell palsy can present as ear pain, antecedent to facial paralysis. Reprinted with permission from the American Journal of Clinical Oncology (2003;26:e157–62).
Fig 6.

Sphenoid sinusitis. T2-weighted image demonstrates mucosal thickening in the left sphenoid sinus. The greater superficial petrosal nerve supplies afferents to this region.
Fig 7.

Nasal spur. Coronal CT with bone algorithm demonstrates a nasal spur that touches the adjacent concha. Referred otalgia may be eliminated during the ENT examination via placement of a cocaine solution over the spur.
Cranial Nerve IX
Head and neck radiologists are most familiar with the areas innervated by the glossopharyngeal nerve. The tympanic nerve (Jacobson nerve, a branch of cranial nerve IX) directly innervates the ear but also has pharyngeal, lingual, and tonsillar branches to supply the posterior one-third portion of the tongue, tonsillar fossa/pillars, pharynx, eustachian tube,10 and parapharyngeal and retropharyngeal spaces (Fig 8).1 Any pathologic process involving the aforementioned areas can result in referred otalgia.
Fig 8.

Primary and referred otalgia pathways of the glossopharyngeal nerve (IX). Cranial nerve IX mediates otalgia via the tympanic nerve of Jacobson. Reprinted with permission from the American Journal of Clinical Oncology (2003;26:e157–62).
Oropharyngeal cancer, most being squamous cell cancer, is one of the most worrisome entities producing pain referred to the ear. Otalgia may be the only presenting complaint but is usually accompanied by soreness or discomfort in the throat.26 Risk factors include alcohol consumption and cigarette smoking, and patients are generally older than 45 years of age. Sectional imaging is best for evaluating deep-tissue involvement, whereas superficial spread of disease is generally best assessed via physical examination.26
Pathology involving the tongue base and palatine tonsil can cause referred otalgia. Because it is generally asymptomatic until late in the disease and the tongue base has a rich lymphatic supply, tongue base cancer is typically advanced, and 60% will have cervical nodal involvement at the time of presentation.26 Palatine tonsillar cancer is more common than tongue base cancer, representing 75%–80% of all squamous cell cancers of the oropharynx.26 Like tongue base cancer, it is a late presenter and will commonly have cervical node metastases at the time of examination. Sixty to eighty percent of patients will initially complain of odynophagia and dysphagia requiring them to seek medical attention. Otalgia and a foreign body sensation in the back of the throat are other early symptoms, whereas trismus is a late sign of disease, with invasion of the muscles of mastication.26
Otalgia is an infrequent symptom of nasopharyngeal cancer, but some sources describe its presence in as many as 14% of patients.8 The usual presentation is a neck mass from metastatic adenopathy, conductive hearing loss, and bloody nasal discharge.25 Cross-sectional imaging will reveal a mass in the lateral pharyngeal recess, often accompanied by metastatic cervical lymphadenopathy (Fig 9).25
Fig 9.

Squamous cell carcinoma of the nasopharynx. Axial CT scan with contrast demonstrates an abnormal soft-tissue mass with relatively uniform contrast enhancement filling the left lateral fossa of Rosenmueller, affecting the pharyngeal plexus of cranial nerve IX.
Non-neoplastic processes involving the palatine tonsil, peritonsillar space, and retropharyngeal spaces may also produce otalgia (Figs 10 and 11).1 Acute tonsillitis should be diagnosed by visualization of enlarged and tender tonsils. Throat culture is the most sensitive test and may be performed in case the highly specific and rapid antigen-detection test findings are negative.27 Contrast-enhanced CT should be performed if there is concurrent trismus, indicating spread of disease into the deep peritonsillar spaces.25 Although not commonly imaged, cases of postadenoidectomy otalgia have also been reported.7
Fig 10.

Peritonsillar abscess. Axial CT scan with contrast demonstrates a right inferior peritonsillar abscess in association with edematous change in the adjacent right parapharyngeal space irritating the pharyngeal plexus (cranial nerve IX).
Fig 11.

Retropharyngeal adenitis. Axial CT scan demonstrates suppurative adenitis involving the right retropharyngeal space, which can affect the pharyngeal plexus and produce referred otalgia.
Eagle syndrome occurs when an elongated styloid process or calcified stylohyoid ligament serves to irritate the tonsillar bed, classically resulting in cervicofacial pain, dysphagia, tinnitus, and otalgia precipitated by talking, yawning, or swallowing (Fig 12).4 The styloid process is usually approximately 1 inch (2.54 cm) in length, but calcification of the stylohyoid ligament can elongate this complex much further. In practice, the elongated styloid process/calcified stylohyoid ligament complex occurs in approximately 4% of patients, but only 4% of this subset of patients are actually symptomatic and require treatment.7 Reproduction of symptoms with transoral palpation of the tonsillar fossae is said to be diagnostic of this entity. If conservative measures such as nonsteroidal anti-inflammatory drugs and local steroid injections fail to work, surgical removal of the elongated process from an intraoral or external approach may be necessary.28
Fig 12.

Eagle syndrome. A 30-year-old man with otalgia. Plain film demonstrates a thickened and elongated styloid process, which can irritate the tonsillar bed via the tonsillar branch of cranial nerve IX. Patients classically have reproduction of pain on transoral palpation of the tonsils.
Cranial Nerve X
The vagus nerve supplies the valleculae, lingual, and laryngeal surfaces of the epiglottis, supraglottic larynx, pyriform sinuses, thyroid gland, and more distant sites within the thorax, including the tracheobronchial tree and esophagus (Fig 13).12,14 The Arnold nerve directly innervates the ear, whereas the internal branch of the superior laryngeal nerve and pharyngeal branch of the vagus nerve innervate the larynx and lower pharynx respectively.12,13 The recurrent laryngeal nerve innervates the cervical esophagus and trachea, and the bronchial branch of the vagus nerve innervates the lungs and bronchi.
Fig 13.

Primary and referred otalgia pathways of the vagus nerve (X). Cranial nerve X is involved with otalgia via the auricular nerve of Arnold. Reprinted with permission from the American Journal of Clinical Oncology (2003;26:e157–62)
CT or MR imaging evidence for abnormal thickening or mass lesion within the lower pharynx, larynx, and trachea should be carefully scrutinized in a patient with ear pain because neoplasms or inflammation of these regions can be the only presenting sign of cancer. In most cases, though, an additional history of hoarseness, shortness of breath, or weight loss can be elicited.29
Laryngeal cancer is the second most common place for neoplasm in the upper aerodigestive tract, with squamous cell cancer accounting for 95% of these cancers (Fig 14). Diagnosis rests with a combination of history, physical examination, and endoscopy. Sectional imaging is typically used to stage a clinically detected malignancy. Like other cancers in the upper aerodigestive tract, there is usually a gradual history of sore throat, hoarseness, dysphagia, and odynophagia. Painful swallowing typically indicates involvement of the hypopharynx or base of tongue, whereas hoarseness indicates involvement of the glottis. Referred otalgia is a less common presenting symptom.30
Fig 14.
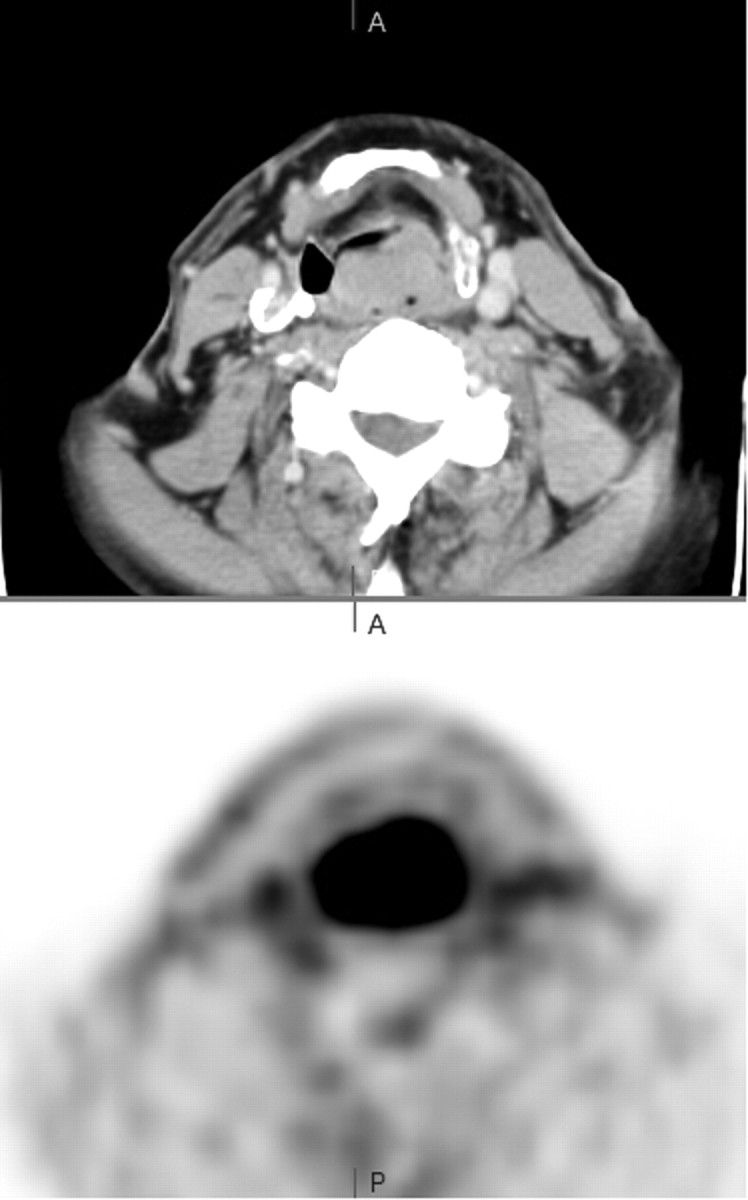
Supraglottic squamous cell carcinoma. Positron-emission tomography/CT scan demonstrates an enhancing exophytic supraglottic mass arising from the posterior wall of the larynx. This area is innervated by the internal branch of the superior laryngeal nerve and can result in otalgia when irritated.
Several case reports have documented otalgia as being the presenting symptom of lung carcinoma. Some authors have even recommended performing a chest x-ray in every patient with a long history of smoking and having atypical facial pain.31 A thorough review of the lung apices, trachea, and mediastinum is warranted on every sectional imaging study for referred otalgia.
Non-neoplastic processes of the larynx may rarely cause referred otalgia. The cricoarytenoid joint, like any joint, can be affected by systemic disorders, direct trauma, and infection.32 When this joint is inflamed, otalgia may result.4 Because the cricoarytenoid joint has a synovial lining, it may be affected by rheumatoid arthritis.32,33 Ankylosing spondylitis, lupus, and gout are other systemic disorders that may affect this joint. Clinical symptoms range from local pain and hoarseness all the way to acute airway compromise.33,34
On rare occasions, esophageal pathology, including hiatal hernias and gastroesophageal reflux, have been reported to cause referred otalgia.35 “Paparella” describes a case of advanced carcinoma of the esophagus presenting solely as ear pain.4 Thyroiditis and thyroid neoplasms are occasional causes of referred otalgia (Fig 15).36
Fig 15.

Papillary thyroid cancer. Axial CT scan demonstrates a hypoattenuated mass centered in the thyroid isthmus. Although most thyroid cancers are subclinical, some may present with pain or dysphagia. Because the sensory innervation to the thyroid gland is via the superior and recurrent laryngeal nerves, there have been documented cases of thyroid pathology manifesting as ear pain.
Cervical Nerves (C2 and C3)
The upper cervical nerves (C2 and C3) innervate a significant portion of the external ear, including the auricle, lobule, and the skin in front of and behind the external ear via the great auricular nerve and lesser occipital nerves.12 Additionally, C2 and C3 serve to innervate other areas within the head and neck, particularly the muscles and facet joints of the cervical spine, including the atlantoaxial joint and facet joints of C2 and C3.37 The mechanism of how cervical spine disease is referred to the ear is controversial. One possible mechanism is via an interconnection between the cervical afferents with the spinal tract of the trigeminal nerve, which is thought to descend as far down as C4.38–40 Sensory information from the upper cervical roots is subsequently relayed to the trigeminal dermatomes (namely CN V3), which in turn can be referred to the ear.38–41
Neuralgia as the Source of Otalgia
Several neuralgias have been implicated in causing otalgia. The neuralgias are a group of diseases causing lancinating pain in the distribution of the affected nerve without producing a neurologic deficit.40,42 Once an objective neurologic deficit is encountered, the term “neuralgia” should be exchanged for “neuropathy.”40 Most sources group neuralgia into primary and secondary categories, with primary causes being idiopathic and physiologic in disturbance and secondary neuralgia arising from a distinct anatomic abnormality, such as a compressive tumor or vessel. Idiopathic neuralgia should only be considered when no organic cause for the patient's clinical symptoms can be found, at the expense of failing to treat something much more serious. Radiologists play a pivotal role in the diagnosis of neuralgia by determining whether there is an anatomic basis for the patient's symptoms. In other words, we can help determine whether the neuralgia is primary or secondary.
Trigeminal (V) neuralgia, tic douloureux, is the most common cranial neuralgia but has only been loosely linked to referred otalgia.5,42 Typically, the diagnosis is not difficult if the classic clinical history is present. Patients are usually in their second half of life and present with unilateral lancinating pain in the distribution of the second or third portion of the trigeminal nerve. Chewing, talking, or eating can reproduce the pain, as can certain trigger points on physical examination.43
Geniculate (VII), glossopharyngeal (IX), vagal (X), sphenopalatine, and occipital neuralgias are much less common than trigeminal neuralgia, but all are widely documented as causing pain in the ear.42 Geniculate neuralgia occurs in middle-aged women, who have pain deep in the ear simulating TMJ pathology.29 It can be either idiopathic or secondary to herpetic involvement (Ramsay Hunt syndrome) and can result in facial nerve enhancement.14,44 Glossopharyngeal neuralgia is another rare cause of otalgia, which results in brief yet sharp lancinating pain within the throat, brought about by swallowing, chewing, or yawning.29 Vagal neuralgia causes pain in the distribution of the larynx and hypopharynx. Sphenopalatine neuralgia, also known as Sluder neuralgia, presents with lancinating pain in the eye and nose with radiation to the ear.5 Occipital neuralgia results in scalp tenderness and a piercing or throbbing occipital/suboccipital headache with radiation to the ear.38,41 MR imaging will help to determine whether structural abnormalities such as cervical disk disease, cervical spondylosis, or tumors of the upper cervical spine are the cause of the patient's occipital neuralgia.7
In the case of negative examination findings and neuralgia, treatment may initially be attempted with medications such as carbamazepine or phenytoin.1 Isolated rhizotomies can be performed if a classic presentation of an isolated neuralgia is present, but oftentimes the clinical presentation is muddled, and sectioning the nervus intermedius, geniculate ganglion, ninth nerve, and portions of the 10th nerve must be performed to cure essential otalgia.42
Conclusions
Since the early 1900s, referred otalgia has been a well-documented phenomenon in the ear, nose, and throat (ENT) and neurosurgical literature. However, it is only in the past few decades with the recent and rapid progression of CT and MR imaging technology that head and neck radiologists have been capable of being an integral part in the team of physicians helping to solve the dilemma of referred otalgia. Essentially any pathology residing within the sensory net of cranial nerves V, VII, IX, and X and upper cervical nerves C2 and C3 can potentially cause referred otalgia. A thorough understanding of the various sensorineural pathways that dually innervate the ear and other sites in the head and neck, alongside a constant and ongoing dialogue with our clinical colleagues, will ensure that patients with referred otalgia will receive the best care possible.
References
- 1. Yanagisawa K, Kyeton JF. Referred otalgia. Am J Otolaryngol 1992;13:323–27 [DOI] [PubMed] [Google Scholar]
- 2. Thaller SR, De Silva A. Otalgia with a normal ear. Am Fam Physician 1987;36:129–36 [PubMed] [Google Scholar]
- 3. Tremble G. Referred pain in the ear: causes and probable nerve pathways. Arch Otolaryngol 1965;81:57–63 [DOI] [PubMed] [Google Scholar]
- 4. Paparella MM. Otalgia. In: Paparella MM, Shumrick DA. eds. Otolaryngology. 2nd ed. Philadelphia: WB Saunders; 1980:1354–57 [Google Scholar]
- 5. Rareshide EH, Amedee RG. Referred otalgia. J La State Med Soc 1990;142:7–10 [PubMed] [Google Scholar]
- 6. Wright EF. Referred craniofacial pain patterns in patients with temporomandibular disorder. J Am Dent Assoc 2000;131:1307–05 [DOI] [PubMed] [Google Scholar]
- 7. Powers WH, Britton BH. Nonotogenic otalgia: diagnosis and treatment. Am J Otolaryngol 1980;2:97–104 [PubMed] [Google Scholar]
- 8. Scarbrough TJ, Day TA, Williams TE. Referred otalgia in head and neck cancer: a unifying schema. Am J Clin Oncol 2003;26:157–62 [DOI] [PubMed] [Google Scholar]
- 9. Levine HL. Otorhinolaryngologic causes of headache. Med Clin N Am 1991;75:677–92 [DOI] [PubMed] [Google Scholar]
- 10. Kern EB. Referred pain to the ear. Minn Med 1972;55:896–98 [PubMed] [Google Scholar]
- 11. Papay FA, Levine HL, Schiavone WA. Facial fuzz and funny findings: facial hair causing otalgia and oropharyngeal pain. Cleve Clin J Med 1989;56:273–76 [DOI] [PubMed] [Google Scholar]
- 12. Netter FH. Atlas of Human Anatomy. 2nd ed. East Hanover, NJ: Novartis; 1997 [Google Scholar]
- 13. Watson-Williams E. Earache with special reference to referred pain. Med Press 1941;205:269–71 [Google Scholar]
- 14. Weissman JL. A pain in the ear: the radiology of otalgia. AJNR Am J Neuroradiology 1997;18:1641–51 [PMC free article] [PubMed] [Google Scholar]
- 15. Abrahams JJ, Berger SB. Inflammatory disease of the jaw: appearance on reformatted CT scans. AJR Am J Roentgenol 1998;170:1085–91 [DOI] [PubMed] [Google Scholar]
- 16. Stafne EC, Gibilisco JA. Oral Roentgenographic Diagnosis. 4th ed. Philadelphia: WB Saunders Co; 1975 [Google Scholar]
- 17. Uthman AA, Sheth BJ, Gale EN. Prevalence of otologic symptoms in a clinical setting. J Dent Res 1986;65(Special Issue A):335 [Google Scholar]
- 18. Okeson JP. Management of Temporomandibular Disorders and Occlusion. 4th ed. St. Louis: Mosby; 1998:149–77 [Google Scholar]
- 19. Clark JL, Mayne JG, Gibilisco JA. The roentgenographically abnormal temporomandibular joint. Oral surg Oral Med Oral Pathol 1972;33:836–40 [DOI] [PubMed] [Google Scholar]
- 20. Ramirez LM, Sandoval GP, Ballasteros LE. Temporomandibular joint disorders: referred cranio-cervico-facial clinic. Med Oral Patol Oral Cir Bucal 2005;10(suppl):E18–26 [PubMed] [Google Scholar]
- 21. Costen JB. Diagnosis of mandibular joint neuralgia and its place in general head pain. Ann Otol Rhinol Laryngol 1944;53:655 [Google Scholar]
- 22. Johansson H, Sojka P. Pathophysiological mechanism involved in genesis and spread of muscular tension in occupational muscle pain and in chronic musculoskeletal pain syndromes: a hypothesis. Med Hypotheses 1991;35:196–203 [DOI] [PubMed] [Google Scholar]
- 23. Kreisberg MK, Turner J. Dental causes of referred otalgia. Ear Nose Throat J 1987;66:30–48 [PubMed] [Google Scholar]
- 24. Yousem DM, Kraut MA, Chalian AA. Major salivary gland imaging. Radiology 2000;216:19–29 [DOI] [PubMed] [Google Scholar]
- 25. Harnsberger RH, Wiggins RH, Hudgins PA, et al. Diagnostic Imaging: Head and Neck. Altona, Manitoba, Canada: Amirsys; 2006 [Google Scholar]
- 26. Civantos FJ, Goodwin WJ. Cancer of the oropharynx. In: Myers EN, Suen JY. eds. Cancer of the Head and Neck. 3rd ed. Philadelphia: WB Saunders; 1996:361–78 [Google Scholar]
- 27. Johansson L, Mansson NO. Rapid test, throat culture and clinical assessment in the diagnosis of tonsillitis. Fam Pract 2003;20:108–11 [DOI] [PubMed] [Google Scholar]
- 28. Subramaniam S, Majid MD. Eagle's syndrome. Med J Malaysia 2003;58:139–41 [PubMed] [Google Scholar]
- 29. Harvey H. Diagnosing referred otalgia: the ten Ts. Cranio 1992;10:333–34 [DOI] [PubMed] [Google Scholar]
- 30. Sinard RJ, Netterville JL, Garrett CG, et al. Cancer of the larynx. In: Myers EN, Suen JY. eds. Cancer of the Head and Neck. 3rd ed. Philadelphia: WB Saunders Co, 1996:381–422 [Google Scholar]
- 31. Bindoff LA, Heseltine D. Unilateral facial pain in patients with lung cancer: a referred pain via the vagus? Lancet 1988;9:812–15 [DOI] [PubMed] [Google Scholar]
- 32. Curtin HD. The larynx. In: Som PM, Curtin HD. eds. Head and Neck Imaging. 4th ed. St. Louis: Mosby; 2003:1595–699 [Google Scholar]
- 33. Chen JJ, Branstetter BF, Myers EN. Cricoarytenoid rheumatoid arthritis: an important consideration in aggressive lesions of the larynx. AJNR Am J Neuroradiol 2005;26:970–72 [PMC free article] [PubMed] [Google Scholar]
- 34. Kolman J, Morris I. Cricoarytenoid arthritis: a cause of acute upper airway obstruction in rheumatoid arthritis. Can J Anest 2002;49:729–32 [DOI] [PubMed] [Google Scholar]
- 35. Blau JN. Ear pain referred by the vagus. BMJ 1989;299:1569–70 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Stevenson J. Acute bacterial thyroiditis presenting as otalgia. J Laryngol Otol 1991;105:788–89 [DOI] [PubMed] [Google Scholar]
- 37. Halderman S. Principles and Practice of Chiropractic Medicine. 3rd ed. New York: McGraw-Hill; 2004:241 [Google Scholar]
- 38. Edmeads J. Headaches and head pains associated with diseases of the cervical spine. Med Clin North Am 1978;62:533–44 [DOI] [PubMed] [Google Scholar]
- 39. Denny-Brown D, Yanagisawa N. The descending trigeminal tract as a mechanism for intersegmental sensory facilitation. Trans Am Neurol Assoc 1970;95:129–33 [PubMed] [Google Scholar]
- 40. List CF. Cranial neuralgia: introduction, definitions, anatomic and pathologic aspects. In: Vinken PJ, Bruyn GW. eds. Handbook of Clinical Neurology: Headaches and Cranial Neuralgia. Vol 5. Amsterdam, the Netherlands: North Holland Pub Co; 1968:270–78 [Google Scholar]
- 41. Dugan MC, Locke S, Gallagher JR. Occipital neuralgia in adolescents. N Engl J Med 1962;67:1166–72 [Google Scholar]
- 42. Rupa V, Saunders RL, Weider DJ. Geniculate neuralgia: the surgical management of primary otalgia. J Neurosurg 1991;75:505–11 [DOI] [PubMed] [Google Scholar]
- 43. Blozis GG. Evaluation of patients with maxillofacial pain. Dent Clin North Am 1973;17:379–89 [PubMed] [Google Scholar]
- 44. Anderson RE, Laskoff JM. Ramsay Hunt syndrome mimicking intracanalicular acoustic neuroma on contrast-enhanced MR. AJNR Am J Neuroradiol 1990;11:409. [PMC free article] [PubMed] [Google Scholar]