

Abstract
BACKGROUND AND PURPOSE: Incidental positron-emission tomography (PET) uptake in the thyroid bed represents a diagnostic dilemma. Currently, there is no consensus regarding the significance of this finding or the most appropriate approach to management. The purpose of this study was to determine the significance of incidental fluorodeoxyglucose (FDG) uptake in the thyroid gland on [18F]FDG–positron-emission tomography (FDG-PET/CT) in patients being initially staged for lymphomas and/or cancers other than of thyroid origin.
MATERIALS AND METHODS: A retrospective review was conducted on patients who were incidentally found to have focal FDG uptake in the thyroid bed on initial staging for cancer. Patient records were assessed for age, sex, clinical presentation, standard uptake values (SUVmax), on FDG-PET/CT, and CT findings in those patients undergoing FDG-PET/CT, fine-needle aspiration (FNA) cytology, and surgical pathologic examination.
RESULTS: Thirty patients were identified with incidental FDG-PET uptake in the thyroid bed from 630 studies performed for evaluation of cancer between March 2004 and June 2006. Complete records were available for 18 patients (6 men, 12 women). Five (27.8%) of 18 patients with incidental focal FDG-PET/CT uptake in the thyroid gland demonstrated papillary thyroid carcinoma on final pathologic findings. The mean and SD of SUVmax was 3.0 ± 1.8 (range, 1.1–7.4) overall, 2.9 ± 1.6 (range, 1.1–6.8) in the patients without malignant growth, and 3.4 ± 2.6 (range, 1.1–7.4) in the 5 patients with papillary thyroid carcinoma. No statistical difference in SUVmax was noted between patients with papillary thyroid carcinoma and patients with benign pathologic findings (P = .63).
CONCLUSIONS: Incidental FDG-PET uptake in the thyroid gland in patients with cancer of nonthyroidal origin is associated with a 27.8% risk for well-differentiated thyroid carcinoma; however, there seems to be no correlation between intensity of FDG uptake and the risk for a malignant process.
The use of functional imaging such as [18F]fluorodeoxyglucose–positron-emission tomography (FDG-PET) has resulted in an increase in the detection of incidentally found thyroid lesions. In a recent retrospective study, Choi et al1 found the prevalence of incidentally found focal thyroid lesions on FDG-PET/CT to be 4.0% and the risk for thyroid malignant tumor associated with these lesions to be 36.7%. Several other retrospective studies have reported the incidence of incidentally identified thyroid lesions on FDG-PET to be 1.1% to 4.3%, with a risk for a malignant process ranging from 14% to 50%.2–7 Although the incidence of these lesions is increasing, determining the most appropriate management represents a challenge for endocrinologists and head and neck surgeons. To date, no specific guidelines exist to define which lesions necessitate surgical management. Although diffuse thyroid uptake in FDG-PET is believed to be either a normal variant, chronic thyroiditis, or Graves disease, focal thyroid lesions have been associated with a high risk for malignant tumors.1–10 Unfortunately, no definitive studies have identified specific characteristics that increase the likelihood of a malignant tumor. Although standard uptake values (SUVmax) has been introduced to predict malignant potential, investigators are still divided regarding this issue. Choi et al and others1–5 reported a correlation between an elevated SUVmax value and a thyroid malignant tumor. However, Kim et al6 did not find any significant difference in the maximal SUVmax value between benign and malignant thyroid nodules on FDG-PET and suggested mandatory cytologic diagnosis regardless of the SUVmax.
The purpose of this study was to determine the clinical significance of incidental FDG-PET/CT uptake in the thyroid in patients with lymphomas and/or cancers of nonthyroidal origin and develop a management algorithm on the basis of the available data.
Materials and Methods
Subjects
Between March 2004 and June 2006, a total of 630 patients were evaluated at our institution with FDG-PET. The studies were done for a variety of diagnoses including metastatic work-up for lymphoma, head and neck cancer, and other nonthyroidal malignant nodules. None of the studies were performed for suspicion of thyroid disease. Thirty patients were identified with incidental focal uptake in the thyroid bed. The complete records were available for retrospective review in 18 patients. None of the patients included in the study had any history of thyroid-related disorder, including cancer. Of these 18 patients, 11 had undergone FDG-PET for evaluation of suspected lymphoma, 3 patients had the FDG-PET study performed as part of metastatic work-up for a known nonthyroidal malignant process, and the remaining 4 patients were being evaluated for a variety of conditions including previous gastrointestinal tract malignant tumor, lung mass, and fatigue. The 18 patients were included in this analysis.
FDG-PET Method
The FDG-PET/CT images were obtained on a Discovery LS integrated PET/CT system (GE Healthcare, Milwaukee, Wis). The patients had fasted for at least 4 hours before fluorodeoxyglucose was administered. Blood glucose levels were checked before the injection, and if these levels were lower than 200 mg/dL, the patients received an intravenous injection of 10 to 15 mCi/370–555 MBq of [18F]fluorodeoxyglucose. PET imaging was obtained 60 minutes after [18F]fluorodeoxyglucose administration.
A thyroid “incidentaloma” was defined as focal thyroid uptake identified incidentally on FDG-PET or FDG-PET/CT study performed to evaluate nonthyroidal disease. FDG uptake in the entire thyroid gland was defined as a diffuse pattern, whereas uptake in less than 1 lobe was considered a focal thyroid lesion. All PET images were qualitatively examined by an expert nuclear radiologist. SUVmax was calculated according to routine clinical fashion. We performed statistical analysis using a 2-tailed t test, and significance was set at P < .05.
Results
All of the 18 patients (6 men, 12 women) entered in this study had focal uptake in 1 thyroid lobe (Table). The mean age of the patients was 42.3 years (age range, 24–67 years). Patients were evaluated with either sonography-guided fine-needle aspiration (FNA) biopsy followed by thyroidectomy (6 patients [33.3%]), or thyroidectomy (12 patients [66.7%]). The decision to perform an FNA or proceed with a thyroidectomy was determined after a discussion with the patient regarding the options of observation with serial evaluation, FNA, and thyroidectomy. Sonography-guided FNA biopsy revealed atypical cytologic features in 4 (66.7%) of 6 patients. After thyroidectomy, 1 patient with atypical cytologic findings had papillary thyroid carcinoma. Patients who underwent thyroidectomy without FNA biopsy had benign disease in 8 (66.7%) of 12 cases, and papillary thyroid carcinoma occurred in 4 of 12 cases (Fig 1). Therefore, 5 (27.8%) of 18 patients with incidental FDG-PET uptake in the thyroid gland demonstrated papillary thyroid carcinoma on final pathologic examination. The mean and SD of SUVmax was 3.0 ± 1.8 (range, 1.1–7.4) overall, 2.9 ± 1.6 (range, 1.1–6.8) in the patients without malignant tumor, and 3.4 ± 2.6 (range, 1.1–7.4) in the 5 patients with papillary thyroid carcinoma. Although the mean SUVmax was slightly higher in the group with papillary thyroid carcinoma vs the patients with benign pathologic findings, there was no statistically significant difference (P = .63).
Patient data
| Patient | Uptake | SUVmax | Intervention | US-Guided FNA | Final Pathologic Findings |
|---|---|---|---|---|---|
| 1 | Right | 2.1 | FNA/thyroidectomy | Atypical | Benign* |
| 2 | Right | 2.5 | FNA/thyroidectomy | Benign* | Benign |
| 3 | Right | 7.4 | FNA/thyroidectomy | Atypical | PTC |
| 4 | Left | 6.8 | FNA/thyroidectomy | Atypical | Benign* |
| 5 | Left | 5.3 | FNA/thyroidectomy | Benign* | Benign* |
| 6 | Right | 2.2 | FNA/thyroidectomy | Atypical | Benign* |
| 7 | Right | 1.9 | Thyroidectomy | Not performed | PTC |
| 8 | Left | 1.3 | Thyroidectomy | Not performed | Benign* |
| 9 | Left | 4.6 | Thyroidectomy | Not Performed | PTC |
| 10 | Left | 3 | Thyroidectomy | Not performed | Benign* |
| 11 | Left | 1.1 | Thyroidectomy | Not performed | Benign* |
| 12 | Right | 3.6 | Thyroidectomy | Not performed | Benign* |
| 13 | Right | 1.1 | Thyroidectomy | Not performed | PTC |
| 14 | Left | 2 | Thyroidectomy | Not performed | Benign* |
| 15 | Right | 3.1 | Thyroidectomy | Not performed | Benign* |
| 16 | Left | 3 | Thyroidectomy | Not performed | Benign* |
| 17 | Right | 2 | Thyroidectomy | Not performed | PTC |
| 18 | Right | 1.9 | Thyroidectomy | Not performed | Benign* |
Note:—SUVmax indicates standard uptake values; US-guided FNA, ultrasound-guided fine-needle aspiration biopsy; PTC, papillary thyroid carcinoma.
Benign indicates that all pathologic findings were adenomas.
Fig 1.
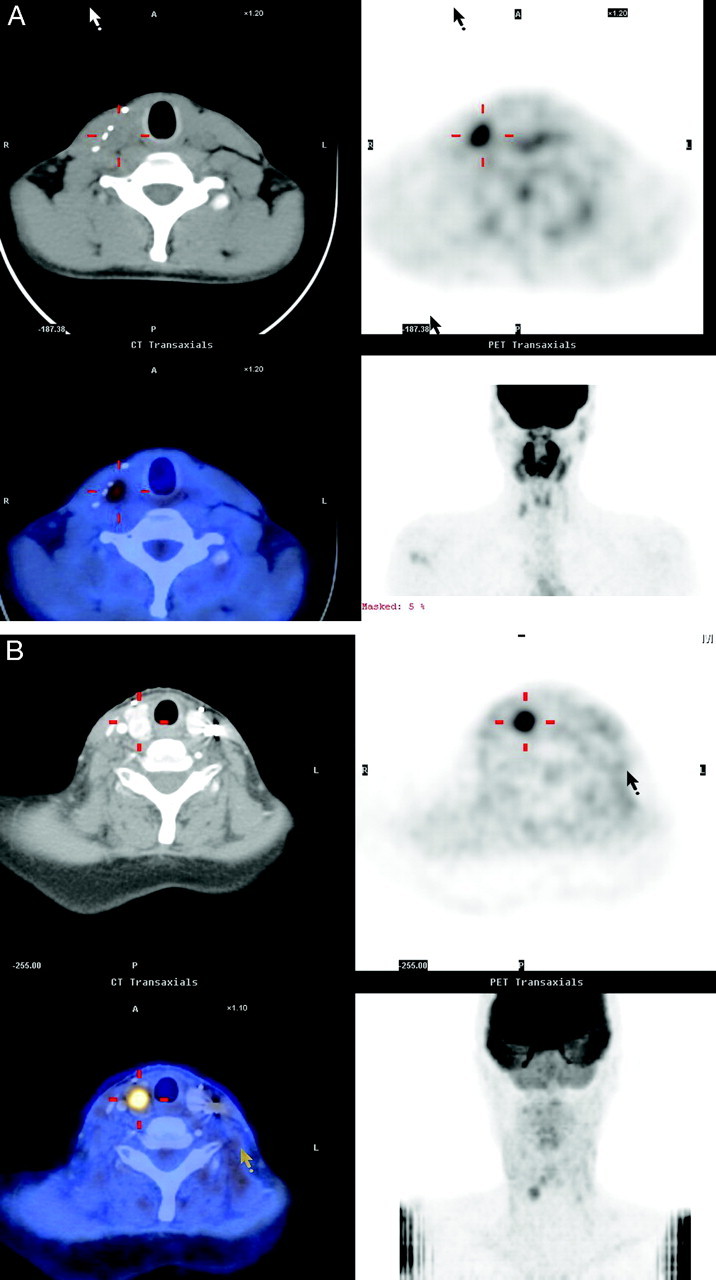
Axial FDG-PET/CT fusion (A) of a patient with a right thyroid adenoma (SUVmax = 6.8). FDG-PET/CT fusion (B) in a patient with a right papillary thyroid cancer (SUVmax = 7.4).
Discussion
The current widespread usage of whole-body FDG-PET and FDG-PET/CT studies as a screening tool for evaluation of malignant tumors has resulted in an increase in the detection of incidentally found thyroid lesions.11 In fact, as this technology becomes more available, the incidence of thyroid “incidentalomas” will likely continue to increase. This strengthens the need to identify which of these lesions are at high risk for a malignant process. Because there is a risk for malignant growth associated with these lesions, appropriate management guidelines and protocols need to be designed to adequately treat patients with focal “incidentalomas” to prevent undertreatment or unnecessary thyroidectomy.
In our study, incidental focal thyroid lesions were identified in 30 of 630 patients, corresponding to a prevalence of 4.8%. This finding is comparable with what was previously reported in the literature.1–7 Similar to previous reports,1,2,6,7 we found a high (27.8%) risk for malignant tumors in patients with incidentally identified focal FDG-PET uptake in the thyroid gland.
Although differences in SUVmax have been suggested to distinguish benign from malignant disease, many experts do not rely on these values because of significant overlap between benign and malignant lesions.1–6 In our patients, the mean SUVmax was 2.9 for the benign lesions and 3.4 for the malignant lesions, without a statistical difference between these groups (P > .05). This finding is similar to that of a previous report by Kim et al.6
The risk for malignant disease in any thyroid nodule is in the range of 4% to 5%,12,13 and nodules found incidentally on carotid Doppler studies, MR imaging studies, and CT scans carry a similar risk for malignant disease.14 Thus, as in other studies, in our study lesions incidentally found on FDG-PET had at least a 5 times greater risk for malignant tumor than other nodules.
Because there is no defined consensus on the management for such “incidentalomas” in the literature, a multidisciplinary treatment algorithm is proposed in our study (Fig 2). If incidental thyroid uptake is found on FDG-PET, the first diagnostic step should be testing thyroid-stimulating hormone (TSH) levels followed by ultrasonography. The presence of a nodule should lead to a sonography-guided FNA. Malignant cells found on FNA should ultimately lead to a total thyroidectomy, whereas the treatment of “benign” or “atypical” cells leads to a more nebulous course. Although some studies have demonstrated very high accuracy rates of FNA in the diagnosis of thyroid lesions,15 others have shown substantial false-negative rates.16,17 All of the malignant lesions detected in our study were papillary cancer, which generally has a low risk for distant metastasis. However, aggressive tumors do occur, and tumors positive for FDG-PET uptake are often the high-grade type of differentiated thyroid cancer because glucose metabolism is generally increased in poorly differentiated cancer.18 Given the high risk for malignant disease in FDG-PET–positive thyroid lesions, the possibility of false-negative FNA, and the possibility of a high-grade lesion, we recommend either serial thyroid ultrasound examination with FNA biopsy or surgery for patients with FDG-PET–positive thyroid nodules. If surgery is ultimately decided in cases of “benign” or “atypical” cells on FNA, hemithyroidectomy followed by intraoperative frozen section with completion thyroidectomy in cases of malignant findings should be offered. Previous studies demonstrating the accuracy of FNA would suggest that FNA is an appropriate initial step in all patients presenting with suspicious thyroid nodules; however, given this small sample size, a larger study is necessary to elucidate the role for FNA in this unique patient population presenting with incidental focal thyroid FDG-PET uptake.
Fig 2.

Algorithm for the treatment of patients with incidental focal 18F-FDG-PET uptake in the thyroid gland.
Conclusions
We found a 27.8% rate of malignant disease associated with focal incidental thyroid lesions identified on FDG-PET or FDG-PET/CT in patients being worked up for a malignant nodule. There was no correlation between SUVmax intensity and the risk for a malignant lesion. We recommend that patients with incidentally detected FDG-PET–positive thyroid nodules be evaluated with TSH and sonography-guided FNA biopsy per usual protocol, but because of the high rate of malignant findings in these lesions, most patients should undergo surgery.
Footnotes
Paper previously presented at: Annual Meeting of the American Thyroid Association, October 12, 2006; Phoenix, Ariz.
References
- 1.Choi JY, Lee KS, Kim HJ, et al. Focal thyroid lesions incidentally identified by integrated 18F-FDG PET/CT: clinical significance and improved characterization. J Nucl Med 2006;47:609–15 [PubMed] [Google Scholar]
- 2.Cohen MS, Arslan N, Dehdashti F, et al. Risk of malignancy in thyroid incidentalomas identified by fluorodeoxyglucose-positron emission tomography. Surgery 2001;130:941–46 [DOI] [PubMed] [Google Scholar]
- 3.Kang KW, Kim SK, Kang HS, et al. Prevalence and risk of cancer of focal thyroid incidentaloma identified by 18F-fluorodeoxyglucose positron emission tomography for metastasis evaluation and cancer screening in healthy subjects. J Clin Endocrinol Metab 2003;88:4100–04 [DOI] [PubMed] [Google Scholar]
- 4.Chen YK, Ding HJ, Chen KT, et al. Prevalence and risk of cancer of focal thyroid incidentaloma identified by 18F-fluorodeoxyglucose positron emission tomography for cancer screening in healthy subjects. Anticancer Res 2005;25:1421–26 [PubMed] [Google Scholar]
- 5.Yi JG, Marom EM, Munden RF, et al. Focal uptake of fluorodeoxyglucose by the thyroid in patients undergoing initial disease staging with combined PET/CT for non-small cell lung cancer. Radiology 2005;236:271–75 [DOI] [PubMed] [Google Scholar]
- 6.Kim TY, Kim WB, Ryu JS, et al. 18F-fluorodeoxyglucose uptake in thyroid from positron emission tomogram (PET) for evaluation in cancer patients: high prevalence of malignancy in thyroid PET incidentaloma. Laryngoscope 2005;115:1074–78 [DOI] [PubMed] [Google Scholar]
- 7.Chu Q, Connor MS, Lilien DL, et al. Positron emission tomography (PET) positive thyroid incidentaloma: the risk of malignancy observed in a tertiary referral center. Am J Surg 2006;72:272–75 [PubMed] [Google Scholar]
- 8.Yasuda S, Shohtsu A, Ide M, et al. Chronic thyroiditis: diffuse uptake of FDG at PET. Radiology 1998;207:775–78 [DOI] [PubMed] [Google Scholar]
- 9.Macapinlac HA. FDG-PET in head and neck, and thyroid cancer. Chang Gung Med J 2005;28:284–95 [PubMed] [Google Scholar]
- 10.Ramos CD, Chisin R, Yeung HW, et al. Incidental focal thyroid uptake on FDG positron emission tomographic scans may represent a second primary tumor. Clin Nucl Med 2001;26:193–97 [DOI] [PubMed] [Google Scholar]
- 11.Van den Bruel A, Maes A, De Potter T, et al. Clinical relevance of thyroid fluorodeoxyglucose-whole body positron emission tomography incidentaloma. J Clin Endocrinol Metab 2002. :87:1517–20 [DOI] [PubMed] [Google Scholar]
- 12.Lin JD, Chao TC, Huang BY, et al. Thyroid cancer in the thyroid nodules evaluated by ultrasonography and fine-needle aspiration cytology. Thyroid 2005;15:708–17 [DOI] [PubMed] [Google Scholar]
- 13.Rojeski MT, Gharib H. Nodular thyroid disease: evaluation and management. N Engl J Med 1985;313:428–36 [DOI] [PubMed] [Google Scholar]
- 14.Liebeskind A, Sikora AG, Komisar A, et al. Rates of malignancy in incidentally discovered thyroid nodules evaluated with sonography and fine-needle aspiration. J Ultrasound Med 2005;34:629–34 [DOI] [PubMed] [Google Scholar]
- 15.Mandell DL, Genden EM, Mechanick JI, et al. Diagnostic accuracy of fine-needle aspiration and frozen section in nodular thyroid disease. Otolaryngol Head Neck Surg 2001;124:531–36 [DOI] [PubMed] [Google Scholar]
- 16.Flanagan MB, Ohori P, Carty SE, et al. Repeat thyroid nodule fine-needle aspiration in patients with initial benign cytologic results. Am J Clin Path 2006;125:698–702 [DOI] [PubMed] [Google Scholar]
- 17.Sidawy MK, Del Vecchio DM, Knoll SM. Fine-needle aspiration of thyroid nodules: correlation between cytology and histology and evaluation of discrepant cases. Cancer 1997;81:253–59 [DOI] [PubMed] [Google Scholar]
- 18.Shiga T, Tsukamoto E, Nakada K, et al. Comparison of 18F-FDG, 131I-Na, and 201Tl in diagnosis of recurrent or metastatic thyroid carcinoma. J Nucl Med 2001;42:414–19 [PubMed] [Google Scholar]