

Abstract
Aims and Objectives:
The aims of the study were to comprehensively assess the perception of altered dentofacial aesthetics between dental students and laypersons and to identify the threshold where different variables such gender and clinical training impair dentofacial attractiveness.
Materials and Methods:
Ten photographs were digitally manipulated involving three facial, two smile, four dental, and one gingival components. Fifty images were randomized and rated according to attractiveness by two groups dental students which subdivided into preclinical students and clinical students, and laypersons. The participants evaluated the original and manipulated images using a visual analog scale. The responses were then analyzed using Mann–Whitney U test.
Results:
The results showed threshold levels of noticeable differences between varying levels of discrepancy. The overall perception of aesthetics was high among dental clinical students with the highest perception toward facial profile and the lowest toward gingival margin height. Of the respondents, no differences were found in the perception between male and female participants. Dental students perceived aesthetic components more accurately than laypersons.
Conclusion:
Dental students group had a better perception of dentofacial aesthetics than included laypersons. Unlike gender, clinical training has a substantial positive effect on the assessment of beauty. Dental students sub divided into dental preclinical students and dental clinical students (clinical training is a variable of all subgroups).
Keywords: Aesthetics, dental students, dentofacial, laypersons, perception
Introduction
People pay more attention to their beauty and they are more concerned about their appearance than their health.[1] The face is reported to be a determinant factor for the perception of aesthetics, especially the mouth and eyes, which are the most important areas the people focus on during social interactions.[2,3] With the advent of time, it has been noticed that the definition of beauty keeps changing constantly. Additionally, dental and facial beauty is influenced by geographic, ethnic, cultural, and demographic factors. Perception of smile depends not only on concerns associated with teeth but also on the nearby soft tissues, which include gingival display, buccal corridors, smile arc, diastema, midline position, and facial symmetrical alterations.[4]
Dentofacial aesthetics is more objective when perceived by dental specialists, orthodontists more specifically. Perception of beauty by dental students, on the contrary, may reflect varying degrees of fluctuation owing to the level of their dental education gained from different aspects of dentistry. Perception of dentofacial aesthetics by laypersons depends on their society’s beliefs and norms, which differ among societies for dental and orthodontic treatment decisions, it is essential to understand the threshold of what community considers acceptable in terms of abnormal dentofacial aesthetic features.[5]
To the best of our knowledge, no study has been conducted so far that compare how different dental students and laypersons perceive dentofacial aesthetics. Therefore, the aims of this study were to assess the perception of dentists, dental students, dental technicians, and laypersons on 10 dentofacial aesthetic components, and whether such a perception is affected by gender or clinical training.
Materials and Methods
This is a prospective cross-sectional observational study conducted at the College of Dentistry, Thamar University, Thamar, Yemen, from December 2018 to March 2019. Two groups of university students were included in this study: Dental students whose subdivided into: preclinical students and clinical students, and laypersons
-
Dental students group (group 1: n = 533, 309 males and 224 females), which are further divided into the following two subgroups:
-
a.
Clinical subgroup: n = 202, 129 males and 73 females
-
b.
Preclinical subgroup: n = 331, 179 males and 149 females
-
a.
Laypersons group (group 2: n = 213, 131 males and 82 females)
When we deal with subgroups as a one group when compared the dental students with laypersons, however, we compare both subgroups to show the main group of dental students
Photo manipulation
Three standard photographs of facial aesthetics and seven standard photographs of posed smile of young man were digitally modified using Adobe Photoshop (version CS 3, Adobe Systems, San Jose, California). Each standard photograph along with four modified analogues represented one group for specific esthetic trait (facial or smile, [Figures 1–10]).
Figure 1:

Chin manipulation of male with a pleasant face: (A) The midsagittal plane coincident with soft tissue pogonion point of the chin, (B) 2 mm shift of soft tissue pogonion to the left, (C) 4 mm shift of soft tissue pogonion to the left, (D) 6 mm shift of soft tissue pogonion to the left, (E) 8 mm shift of soft tissue pogonion to the left
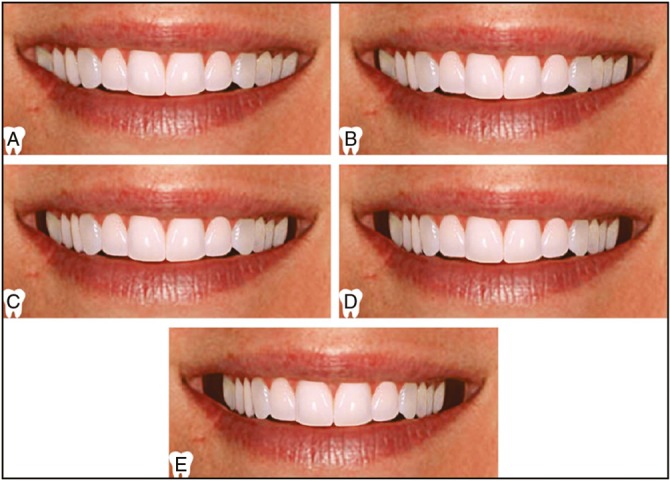
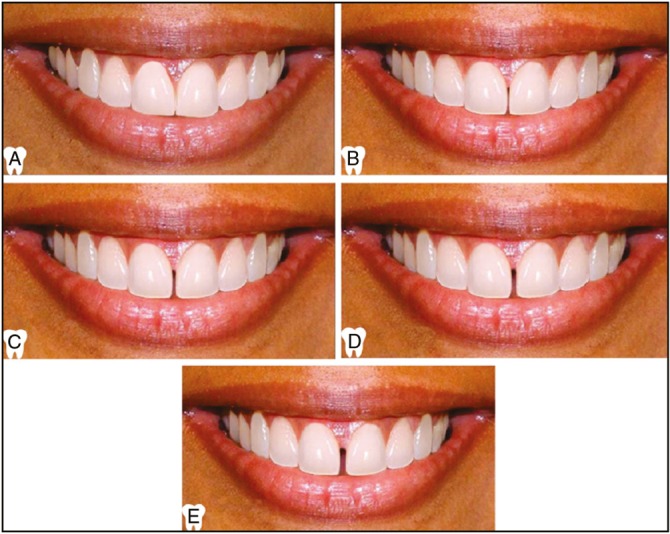
Figure 10:
Manipulation of crown height by manipulation of gingival margin height of maxillary right central incisor: (A) 0 mm gingival margin height, (B) 0.5 mm increase in gingival margin height, (C) 1 mm increase in gingival margin height, (D) 1.5 mm increase in gingival margin height, (E) 2 mm increase in gingival margin height
A total of 35 photographs displayed anterior teeth and 15 photographs displayed the facial aesthetics. The colored photographs of dental aesthetics did not display the nose, chin, and cheeks in an attempt to avoid their confounding influence on the smile. The photographs were grouped into 10 sets. Every set included five images, one with ideal aesthetics and the others obtained by gradual alterations of the original photograph for each variable. A visual analog scale was set from 1 to 5 to score these images, where 5 was the most pleasant and 1 was the least pleasant one. An overall aesthetic score was calculated by adding the individual component scores together and multiplying it by two to be presented of 100 [Table 1]. The photographs within each group were arranged randomly and differently in different groups. The manipulation involved three facial components (facial symmetry [Figure 1], facial soft tissue profile [Figure 2], and facial vertical proportion [Figure 3]), two smile components (smile line [Figure 4] and buccal corridor [Figure 5]), four dental (maxillary midline deviation [Figure 6], maxillary midline diastema [Figure 7], clinical crown width [Figure 8], and occlusal plane canting [Figure 9]), and one gingival component (clinical crown height [Figure 10]).
Table 1:
Scoring system of the perception of overall, facial, smile, dental, and gingival components
| Variable | Score | |
|---|---|---|
| Overall | 100 | |
| Facial components | ||
| Q1 | No facial asymmetry | 5 |
| 2 mm facial asymmetry | 4 | |
| 4 mm facial asymmetry | 3 | |
| 6 mm facial asymmetry | 2 | |
| 8 mm facial asymmetry | 1 | |
| Q2 | Straight soft tissue profile | 5 |
| Slightly convex soft tissue profile | 4 | |
| Moderately convex soft tissue profile | 3 | |
| Severely convex soft tissue profile | 2 | |
| Concave soft tissue profile | 1 | |
| Q3 | Average facial vertical proportions | 5 |
| Slightly reduced anterior lower facial height | 4 | |
| Short face | 2 | |
| Slightly increased anterior lower facial height | 3 | |
| Long face | 1 | |
| Smile components | ||
| Q4 | Normal gingival display | 5 |
| 1 mm increased gingival display | 4 | |
| 2 mm increased gingival display | 3 | |
| 3 mm increased gingival display | 2 | |
| 4 mm increased gingival display | 1 | |
| Q5 | Narrow buccal corridor (10%) | 4 |
| Normal buccal corridor (15%) | 5 | |
| Wide buccal corridor (22%) | 3 | |
| Obliterated buccal corridor (2%) | 2 | |
| Very wide buccal corridor (28%) | 1 | |
| Dental components | ||
| Q6 | No maxillary midline deviation | 5 |
| 1 mm maxillary midline deviation | 4 | |
| 2 mm maxillary midline deviation | 3 | |
| 3 mm maxillary midline deviation | 2 | |
| 4 mm maxillary midline deviation | 1 | |
| Q7 | No maxillary midline diastema | 5 |
| 0.5 mm maxillary midline diastema | 4 | |
| 1 mm maxillary midline diastema | 3 | |
| 1.5 mm maxillary midline diastema | 2 | |
| 2 mm maxillary midline diastema | 1 | |
| Q8 | Normal clinical crown width | 5 |
| 1 mm reduction of clinical crown width | 4 | |
| 2 mm reduction of clinical crown width | 3 | |
| 3 mm reduction of clinical crown width | 2 | |
| 4 mm reduction of clinical crown width | 1 | |
| Q9 | No frontal occlusal canting | 5 |
| 1 mm frontal occlusal canting | 4 | |
| 2 mm frontal occlusal canting | 3 | |
| 3 mm frontal occlusal canting | 2 | |
| 4 mm frontal occlusal canting | 1 | |
| Gingival components | ||
| Q10 | Symmetric gingival margin height | 5 |
| 0.5 mm asymmetric gingival margin height | 4 | |
| 1 mm asymmetric gingival margin height | 3 | |
| 1.5 mm asymmetric gingival margin height | 2 | |
| 2 mm asymmetric gingival margin height | 1 | |
Figure 2:
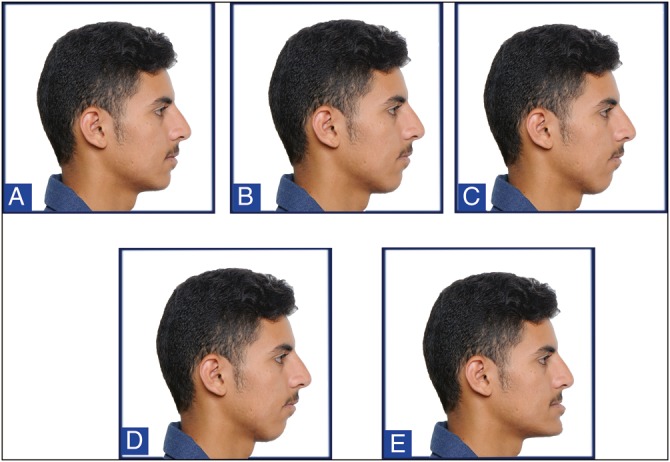
Manipulation of facial soft tissue profile: (A) Straight facial profile (Class I), (B) slightly convex facial soft tissue profile (mild Class II), (C) moderately convex facial soft tissue profile (moderate Class II), (D) severely convex facial soft tissue profile (severe Class II), (E) concave facial soft tissue profile (Class III)
Figure 3:
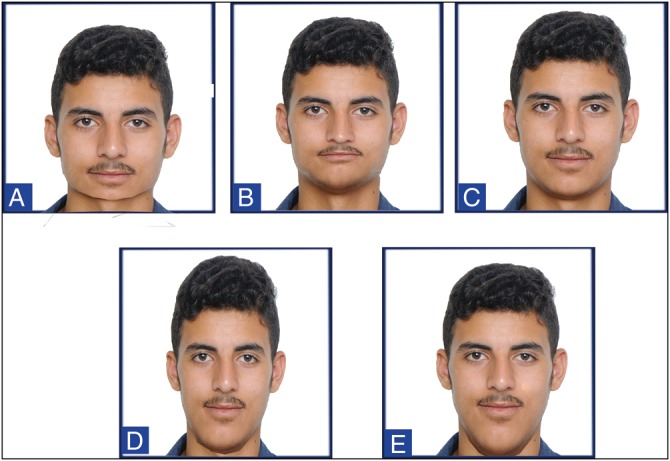
Manipulation of facial vertical proportions: (A) Severely reduced lower anterior facial height (short face), (B) slightly reduced lower anterior facial height, (C) average vertical facial proportions, (D) slightly increased lower anterior facial height, (E) severely increased lower anterior facial height (long face)
Figure 4:

Manipulation of a women photograph with pleasant smile: (A) Normal smile line, (B) 1 mm higher upper lip positions, (C) 2 mm higher upper lip position, (D) 3 mm higher upper lip position, (E) 4 mm higher upper lip position
Figure 5:
Manipulation of buccal corridor: (A) Obliterated buccal corridor (2%), (B) narrow buccal corridor (10%), (C) normal buccal corridor (15%), (D) wide buccal corridor (22%), (E) very wide buccal corridor (28%)
Figure 6:

Manipulation of maxillary dental midline: (A) No midline deviation, (B) 1 mm midline deviation, (C) 2 mm midline deviation, (D) 3 mm midline deviation, (E) 4 mm midline deviation
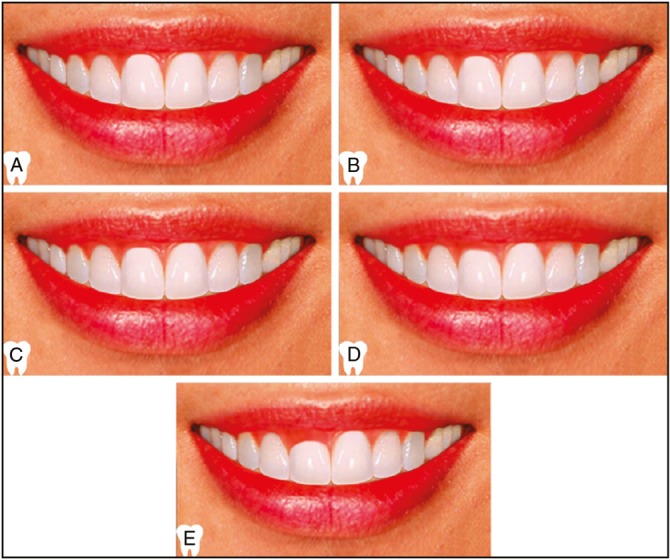
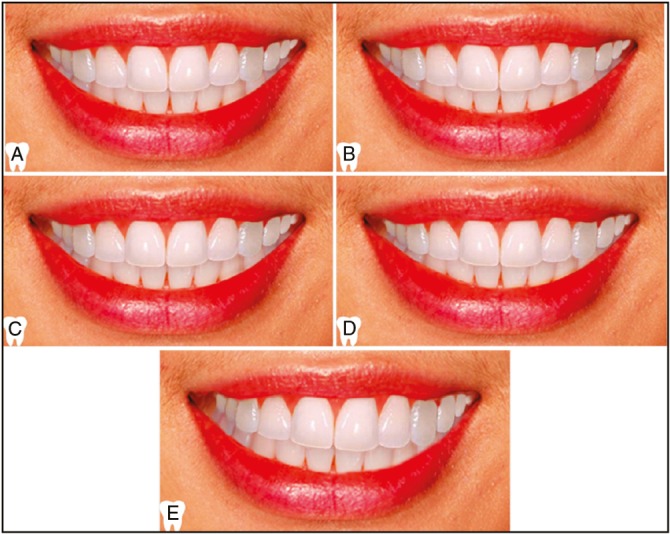
Figure 7:
Manipulation of maxillary midline diastema: (A) No maxillary midline diastema, (B) 0.5 mm maxillary midline diastema, (C) 1 mm maxillary midline diastema, (D) 1.5 mm maxillary midline diastema, (E) 2 mm maxillary midline diastema
Figure 8:

Manipulation of clinical crown width of maxillary right lateral incisor: (A) Normal clinical crown width, (B) 1 mm mesiodistal reduction of clinical crown width, (C) 2 mm mesiodistal reduction of clinical crown width, (D) 3 mm mesiodistal reduction of clinical crown width, (E) 4 mm mesiodistal reduction of clinical crown width
Figure 9:
Manipulation of occlusal plane canting of maxillary arch: (A) No occlusal plane canting, (B) 1 mm occlusal plane canting, (C) 2 mm occlusal plane canting, (D) 3 mm occlusal plane canting, (E) 4 mm occlusal plane canting
Data collection
The manipulated photos were presented in the form of Power Point software version 16.0.4266.1003 (USA, NY, Microsoft Corporation, Microsoft Office 2016). There were 10 slides, each slide represented a group of five numbered photographs for a given aesthetic component as aforementioned [Figures 1–10]. The following question was asked as a heading for each of these slides: “Which of the following images is the most beautiful from your point of view?” The participants answered in a predesigned answer sheet that included inquiry about participant’s gender, participant’s profession, and level of study.
Ethical considerations
A consent form was signed by the participant in the study, those who refused to participate were not included, and the ethical approval was given by the ethics committee of the College of Dentistry, Thamar University, Yemen.
Statistical analysis
Data were handled and analyzed using the standard package for social sciences, the Statistical Package for the Social Sciences (SPSS) software, version 21 (IBM, Armonk, New York). Qualitative variables were statistically described using frequencies and proportions, and by mean values with interquartile range (IQR) for quantitative variables. Individual (of 5) and overall (of 100) aesthetic scores were checked for normal distribution using Kolmogorov–Smirnov test. Between group comparisons, based on gender and, clinical training, were done using Mann-Whitney U test.
Stepwise multiple linear regression analysis for the significant independent determinants of perception of individual overall aesthetics was conducted where gender and clinical training were entered into the equation as independent variables. A P value of 0.05 was considered as significant.
Results
The total number of participants was 746; of the respondents, 534 (58.4%) were males and 381 (41.6%) were females. The total response rate of the participants was 95.11%, 331 (36.2%) were students at preclinical level in dentistry, 202 (22.1%) were students at clinical level in dentistry, and 213 (23.2%) were Laypersons group (art, financial banking, and trading) as shown in Table 2.
Table 2:
Descriptive data of the participants in the present study
| Group | Male | Female | Total |
|---|---|---|---|
| Preclinical | 180 (19.7%) | 151 (16.5%) | 331 (36.2%) |
| Clinical | 129 (14.1%) | 73 (8%) | 202 (22.1%) |
| Layperson | 132 (17.69%) | 81 (10.85%) | 213 (28.55%) |
| Total | 441 (59.11%) | 305 (40.88%) | 746 (100%) |
The overall perception of aesthetics was high among dental students, especially students at clinical levels. (30.16 ± 3.66) with the highest perception found toward facial profile (3.62 ± 1.07) followed by gingival display and midline deviation (3.61 ± 1.64 and 3.61 ± 0.93, respectively), and The gingival height of clinical crown. Facial asymmetry was perceived as aesthetically acceptable by more than 35% of dental students (median [IQR] = 3 [3–4]). Gingival display and clinical crown height were perceived by more than half of the sample [Table 3].
Table 3:
Mean and median scores of the participants’ perception of different aesthetic components for the whole sample and by gender
| Aesthetic components | All sample (n = 746) |
Males (n = 441) |
Females (n = 305) |
P value | |||
|---|---|---|---|---|---|---|---|
| Mean (SD) | Median(IQR) | Mean (SD) | Median (IQR) | Mean (SD) | Median (IQR) | ||
| Overall | 30.69 (4.13) | 31 (28 – 33) | 30.65 (4.29) | 31 (28 – 33) | 30.75 (3.88) | 31 (28 – 33) | 0.759 |
| Facial components | |||||||
| Q1 (Facial symmetry) | 3.35 (1.04) | 3 (3 – 4) | 3.29 (1.04) | 3 (3–4) | 3.44 (1.02) | 3 (3 – 4) | 0.057 |
| Q2 (Facial profile) | 3.64 (1.05) | 4 (3 – 4) | 3.61 (1.06) | 4 (3–4) | 3.69 (1.04) | 4 (3 – 4) | 0.304 |
| Q3 (Facial height) | 3.54 (0.91) | 4 (3 – 4) | 3.66 (0.95) | 4 (3–4) | 3.37 (0.82) | 3 (3 – 4) | <0.001* |
| Smile components | |||||||
| Q4 (Gingival display) | 3.58 (1.61) | 4 (2 – 5) | 3.45 (1.63) | 4 (2–5) | 3.77 (1.55) | 5 (2 – 5) | 0.009* |
| Q5 (Buccal corridors) | 2.47 (1.47) | 3 (1 – 4) | 2.80 (1.46) | 3 (1–4) | 2.65 (1.45) | 2 (1 – 4) | 0.161 |
| Dental components | |||||||
| Q6 (Midline deviation) | 3.62 (1.71) | 4 (3 – 4) | 3.63 (2.08) | 4 (3–4) | 3.62 (0.95) | 4 (3 – 4) | 0.961 |
| Q7 (Midline diastema) | 2.38 (0.91) | 2 (2 – 2) | 2.36 (0.91) | 2 (2–2) | 2.42 (0.92) | 2 (2 – 2) | 0.350 |
| Q8 (Clinical crown width) | 3.24 (1.33) | 4 (2 – 4) | 3.18 (1.30) | 4 (2–4) | 3.31 (1.37) | 3 (2 – 4) | 0.186 |
| Q9 (Occlusal canting) | 3.09 (1.42) | 3 (2 – 4) | 3.15 (1.45) | 3 (2–5) | 3.01 (1.36) | 3 (2 – 4) | 0.182 |
| Gingival components | |||||||
| Q10 (Gingival marginal height) | 1.51 (0.94) | 1 (1 – 2) | 1.53 (0.97) | 1 (1–2) | 1.48 (0.88) | 1 (1 – 2) | 0.448 |
SD = standard deviation. *Significance at 5%
Table 4 showed that less than one-third of the dental students perceived gingival height (median [IQR] = 1 [1–1]). Overall, dental students perceived aesthetic components more accurately than laypersons (P < 0.05 and P < 0.01, respectively) [Tables 4 and 5]. No difference was found in aesthetic perception between males and females, P > 0.05 [Table 2]. However, males significantly perceived facial height, buccal corridor, midline deviation, and gingival marginal height more accurately than females; whereas females perceived vertical facial proportion, frontal occlusal canting, maxillary midline shift, gingival display, midline diastema, and facial symmetry more accurately than males [Table 3]. The effect of dental students participants’ clinical training on the dentofacial esthetic perception was presented [Table 4]. Students in clinical levels generally perceived aesthetic components (30.92 ± 4.64) more accurately than those in preclinical levels (30.46 ± 92). Those significant differences include facial symmetry, soft tissue facial profile, gingival display, maxillary midline deviation, and gingival marginal height of clinical crown.
Table 4:
Mean and median scores of dental students’ perception of different aesthetic components by clinical training
| Aesthetic components | Preclinical students (n = 331) |
Clinical students (n = 202) |
P value | ||
|---|---|---|---|---|---|
| Mean (SD) | Median (IQR) | Mean (SD) | Median (IQR) | ||
| Overall | 30.16 (3.66) | 30 (28–33) | 30.92 (4.64) | 31 (28–34) | 0.048* |
| Facial components | |||||
| Q1 (Facial symmetry) | 3.33 (1.00) | 3 (3–4) | 3.26 (0.93) | 3 (3–3) | 0.413 |
| Q2 (Facial profile) | 3.62 (1.07) | 4 (3–4) | 3.73 (0.84) | 4 (3–4) | 0.188 |
| Q3 (Facial height) | 3.48 (0.84) | 4 (3–4) | 3.47 (0.84) | 3 (3–4) | 0.894 |
| Smile components | |||||
| Q4 (Gingival display) | 3.61 (1.64) | 4 (2–5) | 3.78 (1.70) | 5 (2–5) | 0.257 |
| Q5 (Buccal corridors) | 2.68 (1.89) | 3 (1–4) | 2.63 (1.52) | 2 (1–4) | 0.737 |
| Dental components | |||||
| Q6 (Midline deviation) | 3.61 (0.93) | 4 (3–4) | 3.92 (2.74) | 4 (4–4) | 0.121 |
| Q7 (Midline diastema) | 2.30 (0.79) | 2 (2–2) | 2.28 (0.95) | 2 (2–2) | 0.802 |
| Q8 (Clinical crown width) | 3.19 (1.32) | 4 (2–4) | 3.39 (1.29) | 4 (3–4) | 0.086 |
| Q9 (Occlusal canting) | 3.04 (1.41) | 3 (2–4) | 3.11 (1.52) | 3 (2–5) | 0.596 |
| Gingival components | |||||
| Q10 (Gingival marginal height) | 1.31 (0.72) | 1 (1–1) | 1.36 (0.82) | 1 (1–1) | 0.475 |
SD = standard deviation. *Significance at 5%
Table 5:
Mean and median scores of dental students’ perception and laypersons’ perception of different aesthetic components
| Aesthetic components | Dental (preclinical) students (n = 331) |
Layperson students (n = 213) |
P value | ||
|---|---|---|---|---|---|
| Mean (SD) | Median (IQR) | Mean (SD) | Median (IQR) | ||
| Overall | 30.16 (3.66) | 30 (28–33) | 31.30 (4.21) | 31 (29–34) | 0.001* |
| Facial components | |||||
| Q1 (Facial symmetry) | 3.33 (1.00) | 3 (3–4) | 3.47 (1.16) | 3 (3–5) | 0.148 |
| Q2 (Facial profile) | 3.62 (1.07) | 4 (3–4) | 3.59 (1.20) | 4 (3–4) | 0.767 |
| Q3 (Facial height) | 3.48 (0.84) | 4 (3–4) | 3.70 (1.06) | 4 (3–5) | 0.011* |
| Smile components | |||||
| Q4 (gingival display) | 3.61 (1.64) | 4 (2–5) | 3.36 (1.43) | 3 (2–4) | 0.061 |
| Q5 (Buccal corridors) | 2.68 (1.89) | 3 (1–4) | 2.92 (1.49) | 3 (2–4) | 0.100 |
| Dental components | |||||
| Q6 (Midline deviation) | 3.61 (0.93) | 4 (3–4) | 3.37 (1.29) | 4 (2–4) | 0.019* |
| Q7 (Midline diastema) | 2.30 (0.79) | 2 (2–2) | 2.61 (1.01) | 2 (2–3) | <0.001* |
| Q8 (Clinical crown width) | 3.19 (1.32) | 4 (2–4) | 3.17 (1.38) | 4 (2–4) | 0.867 |
| Q9 (Occlusal canting) | 3.04 (1.41) | 3 (2–4) | 3.15 (1.34) | 3 (2–4) | 0.360 |
| Gingival components | |||||
| Q10 (Gingival marginal height) | 1.31 (0.72) | 1 (1–1) | 1.95 (1.61) | 2 (1–2) | <0.001* |
SD = standard deviation. *Significance at 5%
Multiple linear regression confirmed the bivariate analysis, clinical training and gender were the independent determinants of aesthetic perception by dental students; however, the fractions by which these two variables contributed to the explanation of the variability of aesthetic perception were minimal ranging from 1.9% (facial height) to 77% (overall aesthetics) as shown in Table 6.
Table 6:
Independent determinants of perception of dental students, dentists, dental technicians, and laypersons of different aesthetic components and overall aesthetics as shown by stepwise multiple linear regression analyses
| Determinants | Independents* | B | 95% CI of B | Adjusted R2 | P value |
|---|---|---|---|---|---|
| Overall | No variables were entered into the equation | ||||
| Facial components | |||||
| Q1 (Facial symmetry) | No variables were entered into the equation. | ||||
| Q2 (Facial profile) | College | –0.105 | (–0.175, –0.036) | 0.009 | 0.003* |
| Q3 (Facial height) | Gender | –0.263 | (–0.384, –0.143) | 0.019 | <0.001* |
| Smile components | |||||
| Q4 (gingival display) | No variables were entered into the equation. | ||||
| Q5 (Buccal corridors) | Gender | –0.195 | (–0.385, –0.006) | 0.003 | 0.044* |
| Dental components | |||||
| Q6 (Midline deviation) | No variables were entered into the equation. | ||||
| Q7 (Midline diastema) | No variables were entered into the equation. | ||||
| Q8 (Clinical crown width) | College | –0.088 | (–0.175, 0) | 0.003 | 0.049* |
| Q9 (Occlusal canting) | No variables were entered into the equation. | ||||
| Gingival components | |||||
| Q10 (Gingival marginal height) | College | 0.283 | (0.220, 0.346) | 0.077 | <0.001* |
*Independent variables: Gender and college. *Significance at 5%
Discussion
Aesthetics has become more important factor than health and function nowadays. Perception of dentofacial aesthetics varies between the people depending on their age, gender, socioeconomic status, level of education, and occupation; therefore, trying to screen the dentofacial aesthetic perception is a challenge for a given group of population, and the result comparison rarely presents similarities.
To achieve reliability of the presentation; PowerPoint was presented properly to all participants, it was presented by the same operates to every group in class rooms, all the classrooms that present study was conducted checked for light and data show performance to guarantee that the proper presentation of PowerPoint slides were achieved for all participants. PowerPoint was presented to every group in their classrooms. And it was not presented to the whole participants at once. These classrooms were large enough to accommodate 50-60 students who have clear vision onto the screen irrespective of their locations in the classroom. In addition, the screen was large enough, which could be seen clearly from different angles in the classrooms.
The 10 sets of images had been subjected to digital manipulation including slight modifications to investigate the effects of dental education level of clinical training The original and manipulated images were organized in five different sequences to avoid systematic errors or biases that could to lead an observer to take the first image as a model and compare to the manipulated one. No instructions were given to the raters to avoid focusing their attention at any specific area, such as smile, midline, teeth, or any other dental parameters, as they were asked about facial expression beauty. To assess the internal consistency reliability, 50 randomly selected participants were invited to fill a second copy of the questionnaire two weeks later; Cronbach’s alpha results for both were 0.95, which indicated a perfect agreement. This was the first study that provided published information about 10 aesthetic components assessed in general and among dental students and laypersons in particular; a previous study conducted in Saudi Arabia indicated those 10 measures between dental students.[5] The use of the image rating method had been reliable and validated and applicable for recent study.[6] The respondents (a response rate of 95.11%) who participated in this study were distributed by gender, studying sector, and clinical training of only dental students, and were sufficient for proper statistical analysis to provide valid results. The overall perception of aesthetics was high among dental students (30.45 ± 4.07). Students in clinical levels generally perceived aesthetic components (30.92 ± 4.64) more accurately than those in preclinical levels (30.46 ± 92). This was less than that found by Al-Saleh et al.[7] and Omar and Tai.[8] The highest perception was toward facial profile, gingival display, and maxillary midline deviation as more than 33% of dental students perceived the standards of these three components.
Perception of facial asymmetry is important to clinicians in assessment and treatment and to patient themselves as a part of normal required aesthetics. More than two-third of the dental students perceived 2 mm or 4 mm facial asymmetry, McAvinchey et al.[22] found that dental students considered 5.13+2.06 mm of facial asymmetry as normal. This study found no sex difference in the precision of facial asymmetry, this is similar to the findings of a study by McAvinchey et al.[22] Facial profile is essential and is the fundamental standardized soft tissue parameter used in orthodontic practice.[11] Assessment of soft tissue facial profile revealed that approximately 74.48% of the participating dental students consider slightly convex and straight profiles as aesthetically normal, with no sex differences. This is in line with a previous study that found that the preferred soft tissue profile was slight convex and straight facial profile.[12] Furthermore, Yin et al.[12] and Macías et al.[11] found that females preferred slight convex facial profile, whereas males preferred slight concave facial profile.[11,12]
Gingival display is a sensitive factor in smile perception by dental students and dentists but less critical with laypersons, nonetheless all consider gummy smile as unpleasant.[13] Literature showed the tolerable appearance of gingival display while smiling was 1–2 mm.[8,14] May et al.[15] found 3 mm was appealing. Wang et al.[16] found that laypersons preferred average or low smile line over high smile line “gummy smile,” which confirms what we found in this study, that is, the least favored smile by laypersons (14.55%) was 4-mm gingival display [Table 6]. Furthermore, in this study regarding perception of gingival display, a significant difference was observed between both dental students and dentists; preclinical dental students considered gummy smile as attractive unlike clinical students, dentists, and laypersons. In this study, maxillary midline deviation was not significantly different among gender; however, it was significantly different between dental students and laypersons. More than 44% of the participating laypersons accepted the appearance of maxillary midline shift of 2 mm or more. This supports what Chang et al.[17] found, that is, laypersons tolerate smile with more than 2 mm midline shift. In addition, orthodontists and laypersons had the same perception of midline deviations.[18] This is contradictory to this study that revealed significant difference between laypersons and dental students. However, dental students and laypersons considered a 4-mm discrepancy between the dental and facial midlines as unattractive facial feature.
Regarding perception of vertical changes, this study revealed that significant difference was found between dental students and laypersons; dental students were more aware of vertical changes, which was in agreement with the findings of a study by Romani et al.[19] The facial vertical changes were less decisive to laypersons but were critical to dental students. In addition, statistical difference regarding gender was found in a recent study, males (38.38%) preferred slightly increased lower facial height, this is in disagreement with, Johnston et al.[20] who found that slight decrease in lower facial height third was more appealing third was more appealing. However, we found that slightly reduced, slightly increased, or average lower facial height were considered as pleasant faces. This is similar to the findings of a study by Abu Arqoub and Al-Khateeb[21] on a group of non-dental students and laypersons.
According to literature, whether the person was attractive or not, facial symmetry increases the beauty perception.[6,10,17,24] More than two-third of the dental students in this study perceived a facial symmetry of 2 mm as normal; Alhammadi et al.[5] found that dental students considered 4.21 ± 1.13 mm of facial asymmetry as normal. We found that there was no gender difference in the perception of facial asymmetry; this is similar to the findings of a study by Alhammadi et al.[5] and McAvinchey et al.[22] However, there was a significant difference between dental students, especially preclinical level students, and dentists with dental technicians, as dental students perceived 6 mm and more asymmetry as aesthetically unpleasant.
The clinical crown width of lateral incisor was modified while keeping the gingival level to be consistent with resulting change. Change in length and width decreases the perception of aesthetic smile.[6,16,25,26] Dentists and laypersons considered a decrease in length and width will automatically decrease the attractiveness of smile.[23,24] No significance in gender was found in this study. This is similar with the findings of a study by Daou et al.[25] and Kim and Kim,[14] which showed that gender was not a significant factor. However, a significant difference was found among dental students as clinical dental students were more sensitive to height/width ratio change.
Frontal occlusal canting was difficult to determine for all groups; all groups had high perception threshold. This is in agreement with the findings of a study by Alhammadi et al.,[5] where highest perception threshold was noticed in the determination of frontal occlusal canting between clinical and preclinical dental students. This is contradictory to the findings of a study by Padwa et al.[26] who found that the perception of frontal occlusal canting depends on the degree of inclination rather than the observers’ levels of experience. This study showed no significant difference between dental students and laypersons.
All groups had high perception threshold toward buccal corridor in this study The difficulty to perceive buccal corridor was reported in several studies.[5,17,23,26] Pithon et al.[27] found that females were sensitive to the buccal corridor change; wider buccal corridor was more pleasant. This is consistent with our study findings, which revealed significant difference among gender. However, narrow and obliterated buccal corridor was found to be more pleasant by females. Laypersons and dentists perceived buccal corridor similarly.[23] Agree with our study that found buccal corridor was no significant difference between dental students and laypersons.
Midline diastema appearance was not pleased by different geographical population.[5,7,28,29] Midline diastema of 0.5 mm was considered the threshold for dental students, dentists, and laypersons. This is less than the findings of a study by Kokich et al.[29] who reported that 2 mm maxillary midline diastema was considered as the threshold for general dentists and laypersons. Pinho[28] reported that increase in midline diastema increases unpleasantness. Midline diastema was not significant among gender, this is similar to the findings of a study by Pinho.[28] However, a significant difference was found between dental students and laypersons. Midline diastema perception are differ between several studies. In this study, the lowest perception was toward gingival marginal height, as less than 25% of the dental students perceived the standards of these elements. Which was in agreement with a study that excepted by dental and pharmacy students.[8] No significant difference among gender was found. In agreement with previous studies.[7,17] A significant difference was found between dental students and dentists with technicians and dental students with laypersons. Pinho[28] reported a significant difference between orthodontists and laypersons, as orthodontists were sensitive to gingival position and crown length.
Stepwise linear regression analyses were used to strengthen the role in the explanation between study variables in aesthetic perception by study sample. This study included studying sector, and clinical training of only dental students, and were sufficient for proper statistical analysis to provide valid results. However, their roles were very little as revealed by the stepwise linear regression analyses; these variables explained just up to 8.9% of the variability of the overall perception of aesthetics. This means that up to 91% of the variability was explained by other factors not included in our study. This emphasizes the role of other factors, such as cultural norms and ethnicity, in determining the aesthetics. Hence, large-scale studies are highly recommended where the role of other factors must be considered.”
Conclusion
The overall perception of dentofacial aesthetics was high among dental students, with the highest perception observed toward facial profile and the lowest toward gingival marginal height. Clinical dental students level in generally perceived aesthetic components more accurately than did this by clinical training with no differences in overall aesthetic perception between males and females.
Ethical considerations
All the procedures have been performed as per the ethical guidelines laid down by the Declaration of Helsinki and have been approved by the review board of ethics committee of the College of Dentistry, Thamar University, Thamar, Yemen (approval number: EA-12, dated: November 7, 2018).
Data availability
The data set used in this study is available on request from the corresponding author (e-mail: drdurai2008@gmail.com) at the Orthodontic Department, College of Dentistry, Thamar University, Thamar, Yemen.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
We would like to thank the officials and other staff members at the University of Science and Technology for their help during the period of this project work.
References
- 1.Dudea D, Lasserre JF, Alb C, Culic B, Pop Ciutrila IS, Colosi H. Patients’ perspective on dental aesthetics in a south-eastern European community. J Dent. 2012;40:e72–81. doi: 10.1016/j.jdent.2012.01.016. [DOI] [PubMed] [Google Scholar]
- 2.Peck S, Peck L. Selected aspects of the art and science of facial esthetics. In Seminars in orthodontics. 1995;1:105–26. doi: 10.1016/s1073-8746(95)80097-2. [DOI] [PubMed] [Google Scholar]
- 3.Miller AG. Role of physical attractiveness in impression formation. Psych Sci. 1970;19:241–3. [Google Scholar]
- 4.Ioi H, Kang S, Shimomura T, Kim SS, Park SB, Son WS, et al. Effects of vertical positions of anterior teeth on smile aesthetics in Japanese and Korean. J Esthet Restor Dent. 2013;25:274–82. doi: 10.1111/jerd.12032. [DOI] [PubMed] [Google Scholar]
- 5.Alhammadi MS, Halboub E, Al-Mashraqi AA, Al-Homoud M, Wafi S, Zakari A, et al. Perception of facial, dental, and smile esthetics by dental students. J Esthet Restor Dent. 2018;30:415–26. doi: 10.1111/jerd.12405. [DOI] [PubMed] [Google Scholar]
- 6.Howells DJ, Shaw WC. The validity and reliability of ratings of dental and facial attractiveness for epidemiologic use. Am J Orthod. 1985;88:402–8. doi: 10.1016/0002-9416(85)90067-3. [DOI] [PubMed] [Google Scholar]
- 7.Al-Saleh S, Abu-Raisi S, Almajed N, Bukhary F. Esthetic self-perception of smiles among a group of dental students. Int J Esthet Dent. 2018;13:220–30. [PubMed] [Google Scholar]
- 8.Omar H, Tai Y. Perception of smile esthetics among dental and nondental students. J Educ Ethics Dent. 2014;4:54–60. [Google Scholar]
- 9.Almurtadha RH, Alhammadi MS, Fayed MMS, Abou-El-Ezz A, Halboub E. Changes in soft tissue profile after orthodontic treatment with and without extraction: A systematic review and meta-analysis. J Evid Based Dent Pract. 2018;18:193–202. doi: 10.1016/j.jebdp.2017.09.002. [DOI] [PubMed] [Google Scholar]
- 10.Yin L, Jiang M, Chen W, Smales RJ, Wang Q, Tang L. Differences in facial profile and dental esthetic perceptions between young adults and orthodontists. Am J Orthod Dentofacial Orthop. 2014;145:750–6. doi: 10.1016/j.ajodo.2014.01.021. [DOI] [PubMed] [Google Scholar]
- 11.Macías Gago AB, Romero Maroto M, Crego A. The perception of facial aesthetics in a young Spanish population. Eur J Orthod. 2012;34:335–9. doi: 10.1093/ejo/cjr014. [DOI] [PubMed] [Google Scholar]
- 12.Khosravanifard B, Rakhshan V, Raeesi E. Factors influencing attractiveness of soft tissue profile. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;115:29–37. doi: 10.1016/j.oooo.2012.03.021. [DOI] [PubMed] [Google Scholar]
- 13.Pinzan-Vercelino CRM, Costa ACS, Ferreira MC, Bramante FS, Fialho MPN, de Araújo Gurgel J. Comparison of gingival display in smile attractiveness among restorative dentists, orthodontists, prosthodontists, periodontists, and laypeople. J Prosthet Dent. 2019 doi: 10.1016/j.prosdent.2019.03.023. [DOI] [PubMed] [Google Scholar]
- 14.Kim S-K, Kim O-S. Analysis of esthetic factors and evaluation of esthetic perception for maxillary anteriors of dental students. J Korean Acad Prosthodontics. 2019;57:118–26. [Google Scholar]
- 15.May J, Bussen PV, Steinbacher DM. Smile Aesthetics. Aesthetic Orthognathic Surgery and Rhinoplasty. 2019. pp. 253–87.
- 16.Wang C, Hu WJ, Liang LZ, Zhang YL, Chung KH. Esthetics and smile-related characteristics assessed by laypersons. J Esthet Restor Dent. 2018;30:136–45. doi: 10.1111/jerd.12356. [DOI] [PubMed] [Google Scholar]
- 17.Chang CA, Fields HW, Jr., Beck FM, Springer NC, Firestone AR, Rosenstiel S, et al. Smile esthetics from patients’ perspectives for faces of varying attractiveness. Am J Orthod Dentofacial Orthop. 2011;140:e171–80. doi: 10.1016/j.ajodo.2011.03.022. [DOI] [PubMed] [Google Scholar]
- 18.Sadrhaghighi H, Zarghami A, Sadrhaghighi S, Eskandarinezhad M. Esthetic perception of smile components by orthodontists, general dentists, dental students, artists, and laypersons. J Investig Clin Dent. 2017;8:e12235. doi: 10.1111/jicd.12235. [DOI] [PubMed] [Google Scholar]
- 19.Romani KL, Agahi F, Nanda R, Zernik JH. Evaluation of horizontal and vertical differences in facial profiles by orthodontists and lay people. Angle Orthod. 1993;63:175–82. doi: 10.1043/0003-3219(1993)063<0175:EOHAVD>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 20.Johnston DJ, Hunt O, Johnston CD, Burden DJ, Stevenson M, Hepper P. The influence of lower face vertical proportion on facial attractiveness. Eur J Orthod. 2005;27:349–54. doi: 10.1093/ejo/cji023. [DOI] [PubMed] [Google Scholar]
- 21.Abu Arqoub SH, Al-Khateeb SN. Perception of facial profile attractiveness of different antero-posterior and vertical proportions. Eur J Orthod. 2011;33:103–11. doi: 10.1093/ejo/cjq028. [DOI] [PubMed] [Google Scholar]
- 22.McAvinchey G, Maxim F, Nix B, Djordjevic J, Linklater R, Landini G. The perception of facial asymmetry using 3-dimensional simulated images. Angle Orthod. 2014;84:957–65. doi: 10.2319/120213-888.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Baudouin JY, Tiberghien G. Symmetry, averageness, and feature size in the facial attractiveness of women. Acta Psychol (Amst) 2004;117:313–32. doi: 10.1016/j.actpsy.2004.07.002. [DOI] [PubMed] [Google Scholar]
- 24.Almanea R, Modimigh A, Almogren F, Alhazzani E. Perception of smile attractiveness among orthodontists, restorative dentists, and laypersons in Saudi Arabia. J Conserv Dent. 2019;22:69–75. doi: 10.4103/JCD.JCD_429_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Daou R, Akl R, Ghoubril J, Khoury E. Influence of the vertical position of maxillary lateral incisors on the perception of smile esthetics among dentists, orthodontists and laypersons: A computerized simulated photographic assessment. Int Arab J Dent. 2019;10:p19–24 6p.. [Google Scholar]
- 26.Padwa BL, Kaiser MO, Kaban LB. Occlusal cant in the frontal plane as a reflection of facial asymmetry. J Oral Maxillofac Surg. 1997;55:811–6. doi: 10.1016/s0278-2391(97)90338-4. [DOI] [PubMed] [Google Scholar]
- 27.Pithon MM, Mata KR, Rocha KS, Costa BdoN, Neves F, Barbosa GC, et al. Perceptions of brachyfacial, mesofacial and dolichofacial individuals with regard to the buccal corridor in different facial types. J Appl Oral Sci. 2014;22:382–9. doi: 10.1590/1678-775720140003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Pinho T. Assessment of the perception of smile esthetics by laypersons, dental students and dental practitioners. Int Orthod. 2013;11:432–44. doi: 10.1016/j.ortho.2013.09.007. [DOI] [PubMed] [Google Scholar]
- 29.Kokich VO, Kokich VG, Kiyak HA. Perceptions of dental professionals and laypersons to altered dental esthetics: Asymmetric and symmetric situations. Am J Orthod Dentofacial Orthop. 2006;130:141–51. doi: 10.1016/j.ajodo.2006.04.017. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data set used in this study is available on request from the corresponding author (e-mail: drdurai2008@gmail.com) at the Orthodontic Department, College of Dentistry, Thamar University, Thamar, Yemen.