

Abstract
CT is a readily available imaging modality for cross-sectional characterization of acute musculoskeletal injuries in trauma. Dual-energy CT provides several additional benefits over conventional CT, namely assessment for bone marrow edema, metal artifact reduction, and enhanced assessment of ligamentous injuries. Winter sports such as skiing, snowboarding, and skating can result in high speed and high energy injury mechanisms; dual-energyCT is well suited for the characterization of those injuries.
Introduction
Canadian winters can be long, giving plenty of time for participation in winter sports. The low coefficient of friction between skis, snowboards and skates with snow and ice can result in spectacular falls and injuries at high speeds. Resultant injuries range from minor to life threatening. CT is fast and readily available in most emergency departments, and often serves as the first line cross-sectional imaging assessment in the setting of acute sports trauma.
Dual-energy CT (DECT) is a technique gaining popularity in the characterization of acute musculoskeletal injuries. Scans are acquired at two energy levels, facilitating material decomposition and generation of virtual monoenergetic images. The physics and technical details have been well summarized by several authors.1–3 The resultant scan data allow for mapping of specific materials such as monosodium urate and iodine, creation of virtual noncalcium images and bone marrow edema maps, collagen and tendon maps, and metal artifact reduction, without an increased radiation dose.4–6
This pictorial review illustrates DECT findings of winter sports injuries evaluated at Vancouver General Hospital, Canada. Images were acquired on a Siemens Flash (80 and 140 kEV energies) or Force (80 and 150 kEV energies) Scanner (Siemens Healthineers, Forcheim, Germany) and processed on SyngoVia software, v. 5.1. At our institution, bone marrow edema maps are automatically generated and sent to PACS. Manual adjustments are made directly in Syngovia when the automated maps fail to normalize to background marrow—normal marrow should be assigned purple or blue. This adjustment is a simple slider adjustment in Syngovia, and when necessary, generally takes only a few minutes to perform. Tendon maps are generated manually; the software is not set up for automating these maps.
Clinical examples
There are approximately 275 Canadian ski areas with over 19 million visits per season. Skicanada estimates that there are 2.5 million skiers and snowboarders in Canada.7 Injuries at alpine resorts are common, occurring approximately 4–8 per 1000 skier/snowboarder-days, with extremity injuries accounting for approximately one-third of all injuries.8 Hemorrhage and edema are detectable at fractures sites on DECT, increasing the conspicuity of subtle fractures (Figure 1). Extensive marrow edema often accompanies displaced and comminuted fractures (Figure 2). In those cases, the marrow maps may not alter the diagnosis, but does offer the opportunity or identify other associated or ancillary fractures, reducing satisfaction of search errors. Small cortical avulsions will typically show limited marrow edema; the absence of marrow edema does not obviate the need for scrutiny of the standard images (Figure 3).
Figure 1. .

A 25-year-old male injured his left hip skiing. Unenhanced DECT image of the hip (1a) showing a non-displaced fracture of the femoral neck (arrow). The 3D bone marrow map (1b) and coronal bone marrow overlay (1c) show corresponding marrow edema (arrowheads), increasing the conspicuity of the fracture. Marrow edema is encoded as green, with normal background marrow blue/purple. The fracture was managed with operative fixation (1d). 3D, three-dimensional; DECT, dual-energy CT.
Figure 2. .
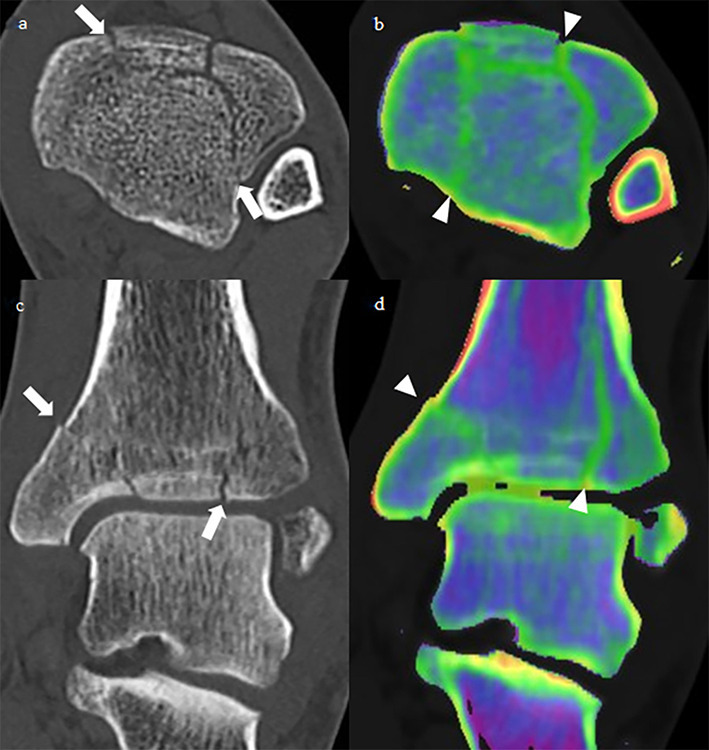
A 55-year-old male injured his ankle snowboarding. Unenhanced axial and coronal DECT image of the ankle showing a comminuted, non-displaced intra-articular fracture (arrows) of the tibial plafond (2a, 2c). The dual-energy bone marrow overlay shows marrow edema (arrowheads) corresponding with the fractures (2b, 2d). The fracture was managed non-operatively with casting. DECT, dual-energy CT.
Figure 3. .
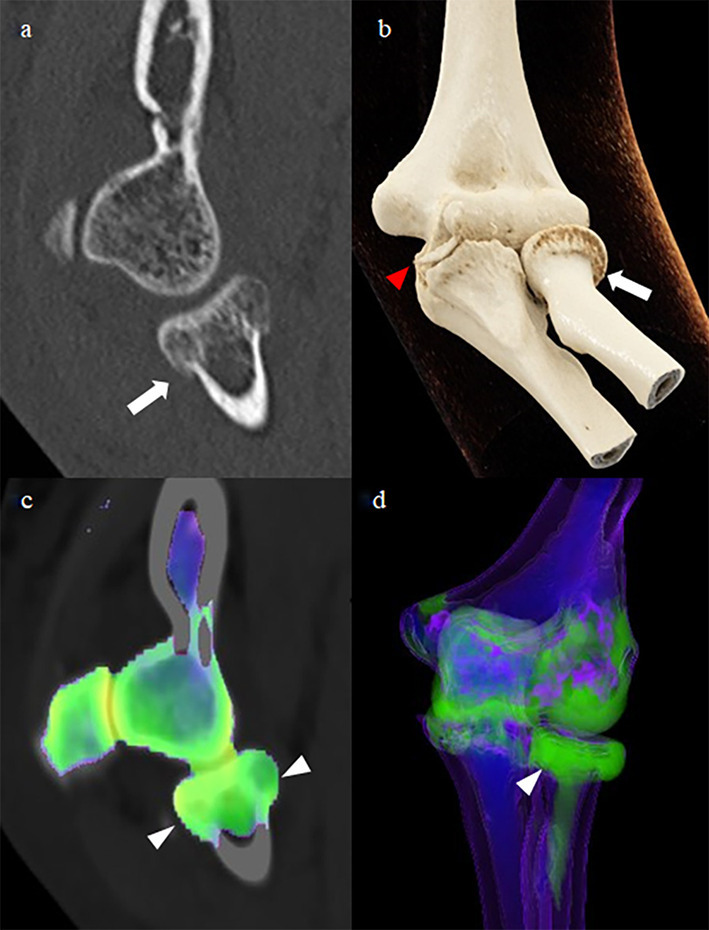
A 53-year-old female injured her elbow skiing. A non-enhanced DECT and 3D cinematic rendering show a radial neck (arrow) and coronoid process (red arrowhead) fractures (3a, 3b). The dual energy marrow overlay and 3D bone marrow map show marrow edema (arrowheads) in the radial head and neck (3c, 3d). There is no apparent edema associated with the coronoid process fracture. Small cortical avulsions often do not show detectable associated edema. 3D, three-dimensional; DECT, dual-energy CT.
Snowboarders ride with their lower extremities fixed to their boards; falls tend to result in injuries to the outstretched upper extremities. Scaphoid fractures remain radiographically occult in up to 25% of cases, with sensitivity of conventional CT of approximately 83%, and MRI of 96%.9 Dareez et al showed that marrow edema is visible in the scaphoid in non-displaced fractures, similar to decreased T1 weighted and high T2 weighted signal on MRI10 (Figure 4). Although there are no prospective studies at present to quantify the added sensitivity of DECT over conventional CT in wrist fractures, the accuracy of DECT for detecting bone marrow edema in the lower extremities and spine have has been investigated by a number of researchers, with sensitivities of 71–95% when compared to MRI.5 The relatively high sensitivity for detection of bone marrow edema provides reassurance to the reporting radiologist that significant osseous injuries are excluded when absent. Furthermore, identification of marrow contusions can provide an explanation for patient pain and may preclude the need for further imaging investigations.
Figure 4. .

A 28-year-old female injured left wrist snowboarding. The radiograph of the wrist was reported as normal (4a). A DECT was subsequently performed, showing subtle buckling (arrow) of the posterior radial metaphyseal cortex (4c). The bone marrow edema map shows increased water in the radial metaphysis (arrowheads), corresponding with edema in a microtrabecular fracture (4b, 4d). The fracture was managed non-operatively with casting. DECT, dual-energy CT.
A review by Wijdicks et al showed a trend towards lower extremity injuries in elite vs recreational level snowboarders, a trend likely related to landing from high amplitude jumps and higher velocity crashes.11 Knee injuries in elite snowboarders follow a similar trend to those in of skiers, with knee injuries accounting for one-third of skier injuries. Anterior cruciate ligament (ACL) tears and knee sprains account for the most common knee injuries for both elite snowboarders and skiers.12,13
DECT is particularly well suited to the assessment of traumatic knee injuries. There is less beam hardening artifact in the knees when compared to the shoulders or pelvis, and the marrow spaces are large when compared to the smaller peripheral bones; marrow edema maps often closely resemble the corresponding pattern of edema on T2 weighted or inversion recover images on MRI. Microtrabecular fractures and marrow contusions are detectable by DECT which would otherwise be missed on conventional radiographs or CT6 (Figure 5).
Figure 5. .
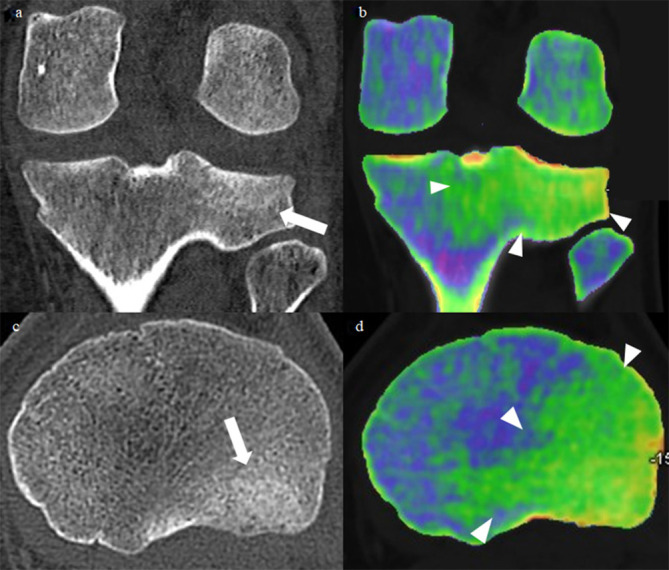
A 23-year-old male injured his knee snowboarding. Unenhanced DECT images of the knee show a subtle fracture (arrows) of the posterolateral tibial plateau (5a, 5c). The bone marrow overlay shows extensive marrow edema (arrowheads) in the posterolateral tibial plateau (5b, 5d). DECT, dual-energy CT.
While a typical pattern of contusions in the knee can assist the radiologist in determining the integrity of the cruciate ligaments, ligament assessment is enhanced by DECT mapping of the collagen in the ligaments. In a porcine model directly comparing MRI to DECT for the evaluation of the ACL, DECT had a high sensitivity and specificity for complete ACL tears, but was not as accurate as MRI (sensitivity 75 vs 100%; specificity 68 vs 75%).14 Visualization of the collateral ligaments and menisci is also enhanced using DECT collagen mapping techniques, which leads to a more complete assessment of the extent of internal derangement of the knee over conventional CT (Figures 6 and 7). The higher specificity and sensitivity of MRI will require that many patients continue to undergo MRI evaluation, but for patients who are not MRI candidates due to implants, pacemakers, claustrophobia or obesity, the additional information provided by DECT increases the diagnostic yield. Collagen mapping is also applicable in other joints, including the wrists and ankles. This is particularly useful in the assessment of displaced fractures where tendon entrapment will alter orthopedic surgical management.
Figure 6.

A 36-year-old male felt a “pop” in his knee while ice skating. He presented to the emergency department the next day with a locked, painful knee. Axial unenhanced DECT of the knee at the level of the plateau (6a) shows the medial meniscus flipped into the joint. DECT collagen overlay map (6b) enhances the conspicuity of the flipped meniscus. Axial T2FS MRI image (6c) from the same day confirms the flipped meniscus. Findings were confirmed intra operatively. DECT, dual-energy CT.
Figure 7. .

A 24-year-old female injured her knee skiing. Unenhanced coronal DECT (7a) shows medial cruciate ligament (MCL) thickening with periligamentous edema. The tendon mapping application which highlights tightly bundled collagen shows a defect in the proximal MCL (7b, red arrowhead), and indistinctness of the ACL (7f, arrow). The marrow edema overlay (7c) shows focal edema in the lateral femoral condyle (white arrowhead). Coronal T2FS (7d) and sagittal Timages (7g) of the knee show a partial thickness tear of the proximal MCL (red arrowhead), a medial femoral condyle marrow contusion (white arrowhead), and a tear of the ACL (arrow). The patient went on to have an ACL repair.
A final relevant application of DECT is metal artifact reduction. The use of metal braces to stabilize fractures can result in metallic artifact obscuring injuries. Virtual monoenergetic images, usually at energies greater than 120 kV, can be generated form a dual-energy dataset to significantly reduce the amount of metal artifact (Figure 8). This is also a useful technique in assessment of traumatic injuries in patients with joint prostheses, and for post-operative assessment of fracture fixation, although higher energy monoenergetic reconstructions tend to come at the expense of decreased soft tissue contrast.1 Similar to the bone marrow edema maps, virtual monoenergetic images can be automatically generated and sent to PACS from the DECT data set, limiting the impact on radiologist reporting time.
Figure 8. .
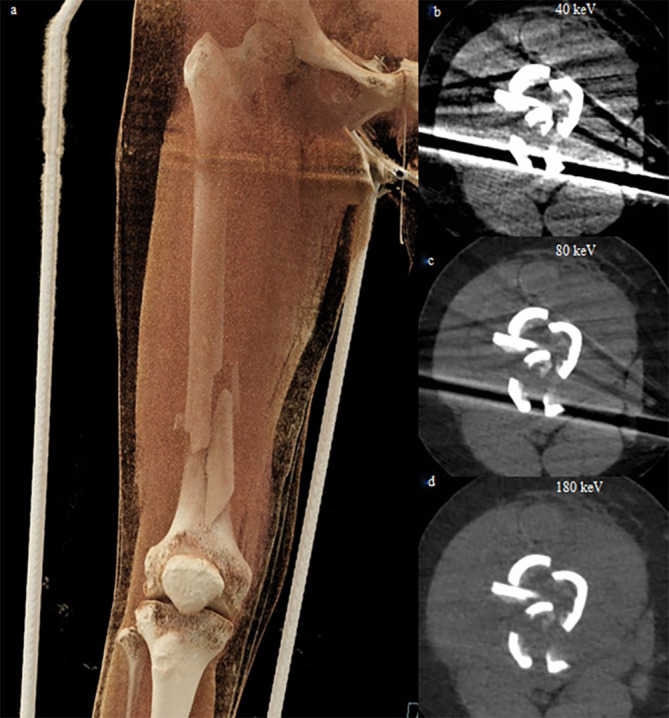
A 53-year-old female injured her right leg snowmobiling. A cinematic rendering of the right femur (8a) shows a comminuted diaphyseal fracture held in an external metal brace. 40, 80 and 180 keV virtual monoenergetic images (8a, b, c) show decreasing beam hardening artifact from the external metallic brace but decreasing soft tissue contrast as the energy level is increased. Her fracture was managed with an intramedullary rod.
Conclusion
Bone marrow edema and collagen mapping provide additional diagnostic information, potentially obviating the need for MRI in some cases, leading to faster diagnosis and patient care, without a significant radiation dose penalty. Virtual monoenergetic images can be used to reduce metal artifact when a metallic brace or prosthesis is present. These added benefits facilitate a more thorough evaluation of traumatic musculoskeletal injuries; DECT is well suited to the evaluation of winter sports and other traumatic injuries.
Contributor Information
Jonathan Hickle, Email: jonathan.hickle@gmail.com.
Frances Walstra, Email: fewalstra@gmail.com.
Peter Duggan, Email: peter.duggan2@vch.ca.
Hugue Ouellette, Email: hugue.ouellette@vch.ca.
Peter Munk, Email: peter.munk@vch.ca.
Paul Mallinson, Email: paul.mallinson@vch.ca.
REFERENCES
- 1.Mallinson PI, Coupal TM, McLaughlin PD, Nicolaou S, Munk PL, Ouellette HA. Dual-Energy CT for the musculoskeletal system. Radiology 2016; 281: 690–707. doi: 10.1148/radiol.2016151109 [DOI] [PubMed] [Google Scholar]
- 2.Omoumi P, Becce F, Racine D, Ott JG, Andreisek G, Verdun FR. Dual-Energy CT: basic principles, technical approaches, and applications in musculoskeletal imaging (Part 1. Semin Musculoskelet Radiol 2015; 19: 431–7. doi: 10.1055/s-0035-1569253 [DOI] [PubMed] [Google Scholar]
- 3.Millner MR, McDavid WD, Waggener RG, Dennis MJ, Payne WH, Sank VJ. Extraction of information from CT scans at different energies. Med Phys 1979; 6: 70–1. doi: 10.1118/1.594555 [DOI] [PubMed] [Google Scholar]
- 4.Nicolaou S, Liang T, Murphy DT, Korzan JR, Ouellette H, Munk P. Dual-Energy CT: a promising new technique for assessment of the musculoskeletal system. AJR Am J Roentgenol 2012; 199(5_supplement): S78–S86. doi: 10.2214/AJR.12.9117 [DOI] [PubMed] [Google Scholar]
- 5.Wong WD, Shah S, Murray N, Walstra F, Khosa F, Nicolaou S. Advanced musculoskeletal applications of dual-energy computed tomography. Radiol Clin North Am 2018; 56: 587–600. doi: 10.1016/j.rcl.2018.03.003 [DOI] [PubMed] [Google Scholar]
- 6.Suh CH, Yun SJ, Jin W, Lee SH, Park SY, Ryu C-W. Diagnostic performance of dual-energy CT for the detection of bone marrow oedema: a systematic review and meta-analysis. Eur Radiol 2018; 28: 4182–94. doi: 10.1007/s00330-018-5411-5 [DOI] [PubMed] [Google Scholar]
- 7.Quick Facts [Internet].. Available from: SkiCanada.org. [cited 2019 Jun 7].https://www.skicanada.org/about-us/quick-facts/.
- 8.McBeth PB, Ball CG, Mulloy RH, Kirkpatrick AW. Alpine Ski and snowboarding traumatic injuries: incidence, injury patterns, and risk factors for 10 years. Am J Surg 2009; 197: 560–4. doi: 10.1016/j.amjsurg.2008.12.016 [DOI] [PubMed] [Google Scholar]
- 9.Carpenter CR, Pines JM, Schuur JD, Muir M, Calfee RP, Raja AS. Adult scaphoid fracture. Acad Emerg Med 2014; 21: 101–21. doi: 10.1111/acem.12317 [DOI] [PubMed] [Google Scholar]
- 10.Dareez NM, Dahlslett KH, Engesland E, Lindland ES. Scaphoid fracture: bone marrow edema detected with dual-energy CT virtual non-calcium images and confirmed with MRI. Skeletal Radiol 2017; 46: 1753–6. doi: 10.1007/s00256-017-2730-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wijdicks CA, Rosenbach BS, Flanagan TR, Bower GE, Newman KE, Clanton TO, et al. Injuries in elite and recreational snowboarders. Br J Sports Med 2014; 48: 11–17. doi: 10.1136/bjsports-2013-093019 [DOI] [PubMed] [Google Scholar]
- 12.Rust DA, Gilmore CJ, Treme G. Injury patterns at a large Western United States Ski resort with and without snowboarders: the Taos experience. Am J Sports Med 2013; 41: 652–6. doi: 10.1177/0363546512472045 [DOI] [PubMed] [Google Scholar]
- 13.Hagel BE, Goulet C, Platt RW, Pless IB. Injuries among skiers and snowboarders in Quebec. Epidemiology 2004; 15: 279–86. doi: 10.1097/01.ede.0000120044.62029.b4 [DOI] [PubMed] [Google Scholar]
- 14.Fickert S, Niks M, Dinter DJ, Hammer M, Weckbach S, Schoenberg SO, et al. Assessment of the diagnostic value of dual-energy CT and MRI in the detection of iatrogenically induced injuries of anterior cruciate ligament in a porcine model. Skeletal Radiol 2013; 42: 411–7. doi: 10.1007/s00256-012-1500-8 [DOI] [PubMed] [Google Scholar]