

Abstract
Self-Discrepancy Theory (Higgins, 1987) predicts that the difference between the ideal and the actual self will be associated with impaired-control-over-drinking (IC; dysregulated drinking beyond one’s own limits) as well as alcohol-related-problems. According to Slaney et al. (2001) perfectionism is a multi-faceted personality trait which represents both adaptive (e.g. high-standards) and maladaptive (e.g. discrepancy) aspects. In particular, discrepancy has been associated with poorer coping approaches, which may suggest a Self-Medication route to IC. Yet, to date, no one has examined whether drinking-motives (e.g., social, enhancement, coping and conformity) mediate the relations between discrepancy and high standards and alcohol-outcomes such as IC. We used a structural equation model to test indirect associations of discrepancy and high-standards to both heavy-episodic-drinking and alcohol-related-problems through the mediating mechanisms of drinking-motives and IC. Results supported the distinction between discrepancy and high-standards consistent with the Self-Medication Hypothesis (Hersh & Hussong, 2009). Discrepancy was associated with poorer alcohol-outcomes through greater coping-motives, conformity-motives and IC. In contrast, higher-standards were associated with fewer alcohol-outcomes through less coping-motives, conformity-motives, and IC. This study illustrates the importance of personality factors such as discrepancy in the development of problematic alcohol-use suggesting that it might be a good target for intervention.
Keywords: Alcohol Use, Perfectionism, Drinking-Motives, Impaired Control, Heavy-Episodic-Drinking, Alcohol Problems
1. Introduction
Perfectionism constitutes setting unreasonably high-standards, striving for a perfect performance, and being overly critical of one’s mistakes (Stoeber, 2018). Self-Discrepancy Theory (Higgins, 1987) involves disparities between the different types of the self: the ideal (i.e. what one aspires to be) versus the actual (i.e. what one actually is). Related to alcohol use, one’s ideal self might wish to sip one or two drinks to socialize at a party, but one’s actual self, will gulp drinks until throwing up or blacking out. According to Slaney et al.’s (2001) conceptualization, perfectionism is a multi-faceted personality trait including both adaptive (e.g. high-standards, order) and maladaptive (e.g. discrepancy) aspects. Discrepancy involves the inconsistency between the ideal and the actual self; it is a transdiagnostic factor for stress, anxiety, and depression (Egan, Wade & Shafran, 2011) which are all strongly comorbid with alcohol use disorders (AUDs; Ebbert et al. 2018; King et al., 2011). Individuals higher in maladaptive-perfectionism have greater difficulty controlling their drinking behavior when experiencing negative affect (Bardone-Cone et al., 2012). Further, self-control mediates the relationship between dimensions of perfectionism and perceived stress (Achtziger & Bayer, 2013). This literature suggests the unique dimensions of perfectionism may be associated with impaired-control-over-drinking (IC).
IC involves difficulty limiting drinking behavior despite intentions to do so (Heather, et al., 1993). It is a self-regulation failure specific to the drinking context (Patock-Peckham and colleagues 2001; 2006; 2011). IC has traditionally been studied in relation to behavioral control constructs (Patock-Peckham and colleagues 2001; 2006; 2011; Vaughan et al., 2019), and has only recently been linked to internalizing pathways to alcohol-consequences (i.e. anxiety-sensitivity, Ebbert et al., 2018; depression, Patock-Peckham & Corbin, 2019). IC has prospectively predicted problem-drinking (Leeman, et al., 2009) and develops early in the progression of AUD (Heather, 1995). While the Self-Medication-Hypothesis posits individuals drink to alleviate negative-affect (Hersh & Hussong, 2009), very few studies have explored the relationship of adaptive/maladaptive perfectionism to dysregulated drinking (i.e. IC; Heather et al., 1993) and alcohol-related-problems, especially through motives for drinking (Rice & Van Arsdale, 2010).
Dimensions of Perfectionism
Models of perfectionism typically outline both adaptive and maladaptive characteristics, which may be useful for understanding AUDs (Stairs et al., 2012; Stoeber, 2012). Adaptive aspects of perfectionism include having high-standards for oneself (i.e., I try to do the best at everything I do) plus orderliness (e.g., neatness; Slaney & Johnson, 1992). Adaptive perfectionism has been associated with less avoidant coping and positively associated with active-coping (Stoeber & Rennert, 2008), trait conscientiousness (Stoeber & Janssen, 2011), and fewer alcohol-related-problems (Rice & Van Arsdale, 2010).
Maladaptive perfectionism involves the magnitude of discrepancy between one’s ideal self and one’s actual flawed self. In prior studies, Discrepancy has been associated with fewer problem-focused coping-strategies, more emotion-focused coping-strategies, and more alcohol-related-problems (Bahramnejad et al., 2015; Kaviani, Mohammadi, & Zarei, 2014; Rice & Van Arsdale, 2010). Yet, no one to date has examined whether drinking-motives and IC mediate relations between discrepancy and alcohol-use and related-problems.
Motives to Drink
One’s motive(s) for consuming alcohol, such as not living up to one’s ideal version of oneself, may play a role in under-controlled drinking (i.e., IC). Cooper (1994) conceptualized drinking as a behavior motivated by desires to achieve certain outcomes; including coping, conformity, enhancement, and social motives. Coping-motives are internal, and reflect negative-reinforcement (i.e., removal of an adverse state) reasons-for-drinking in order to alleviate negative emotions. They have been consistently linked to heavy alcohol-use for self-medication purposes (Sher & Walitzer, 1986; Corbin, et. al., 2013). In one study, drinking-to-cope was the strongest predictor of alcohol-problems, accounting for a larger proportion of variance than expectancies and social-norms (Neighbors et al., 2007). Even though all four motives were linked to alcohol use, only coping-motives have been associated with alcohol-related-problems over and above alcohol-use (Carey & Correia, 1997; Cooper, 1994). As discrepancy has been previously associated with other problematic coping approaches such as self-blame and non-acceptance (Stoeber & Janssen, 2011), we hypothesized discrepancy would also be associated with increased coping-motives. In contrast, we hypothesized high-standards would be associated with fewer coping-motives.
Conformity-motives involve drinking to avoid social rejection (i.e. external, negative-reinforcing motive; Cooper, 1994). Higher conformity-motives have been related to less alcohol-use quantity/frequency, and less heavy-episodic-drinking, yet were associated with more trait impulsivity (Loxton et al., 2015) as well as more alcohol-related-problems (Grant, et al., 2007). Thus, we expected discrepancy to be positively associated with more conformity-motives, while we anticipated high-standards would be associated with fewer conformity-motives.
Enhancement-motives are internal positive-reinforcement motives involving drinking to enhance positive mood and have been associated with less conscientiousness (Kuntsche, von Fischer, & Gmel, 2008) as well as more heavy-episodic-drinking (Cooper, 1994; Kuntsche, Knibbe, Gmel, & Engels, 2005). Further, higher enhancement-motives during the first year of college mediated associations between perceived norms in the first year and alcohol-use in sophomore year longitudinally (Read, et al., 2003). Therefore, we expected high-standards to be associated with fewer enhancement-motives.
Social-motives (i.e. external, positive-reinforcing-motive; Cooper, 1994) involve drinking to obtain positive social interactions. As drinking is part of the social milieu of college life, presumably social-motives play an important role in student drinking behavior (LaBrie, Hummer, & Pederson, 2007). Although high-standards for success in school can protect against drinking, studies have shown motivation for success in college is also positively associated with alcohol-use (Wormington, Anderson, & Corpus, 2011). As individuals who typically attend college tend to have higher-standards for themselves, we expected those with higher-standards to have higher social-motives for alcohol use and therefore consume more alcohol.
Perfectionism and Motives for Drinking
Rice and Van Arsdale (2010) found maladaptive-perfectionists are significantly more likely to drink-to-cope than adaptive-perfectionists and non-perfectionists. Since Rice and Van Arsdale’s seminal work, few have explored associations between both dimensions of perfectionism (i.e., adaptive and maladaptive), drinking-motives, and alcohol-outcomes. Thus far, research has focused largely on discrepancy and coping with stress among both college and substance using populations (Kaviani et al., 2014; Bahramnejad et al., 2015). Thus, the present study will investigate how discrepancy as well as high standards relate to motives for drinking and, in turn, IC along the alcohol-related-problems pathway.
1.1. Hypotheses.
Based on Self-Discrepancy-Theory, this investigation seeks to explore whether or not levels of discrepancy are indirectly linked to alcohol-related-problems through the mediating mechanisms of drinking motives and IC. Consistent with previous literature, we hypothesized individuals higher on discrepancy will also be higher on all drinking-motives thereby increasing IC, and in turn, indirectly present a risk for more heavy-episodic-drinking as well as more alcohol-related-problems. Conversely, individuals with high-standards are expected to have fewer coping-motives and therefore lower levels of IC, heavy-episodic-drinking, and alcohol-related-problems. Further, we posit higher-standards will be positively related to social-motives and will be indirectly linked to less IC, heavy-episodic-drinking and alcohol-related-problems. We eliminated the order dimension from our proposed model to enhance parsimony. Previous literature does not support specific hypotheses for orderliness.
2. Material and Methods
2.1. Participants
Participants were 941 individuals (50.3% male) from a large university who reported drinking alcoholic beverages at least once per month and provided written consent. The Internal Review Board approved our studies’ procedures. The sample had a mean age of 19.88 (SD = 2.79). Participants were 54.1% Caucasian, 15.3% Hispanic, 21.8% Asian, 4.7% African American, 1.3% Native American, and 2.8% “other” race.
2.2. Measures
2.2.1. Perfectionism.
The Revised Almost Perfect Scale (Slaney et al., 2001) contains three factors: Discrepancy, High-Standards, and Orderliness. This scale is a 23-item scale containing 12 Discrepancy items, 7 High-Standard items, and 4 Orderliness items. A sample Discrepancy item included: “My performance rarely measures up to my standards.” A sample High-Standards item included: “I set very high standards for myself.” We excluded Orderliness from the current study. The alpha reliabilities for this sample were Discrepancy (.96) and High-Standards (.94).
2.2.2. Drinking-motives.
Cooper’s 1994 four-factor model of drinking-motives included: Social, Enhancement, Coping, and Conformity. This is a 20-item scale with 5-items reflecting each motive. Responses ranged from 1 = almost never/never to 5 = almost always/always. A sample Social-Motive item included: “To be sociable.” A sample Enhancement-Motive item included: “Because you like the feeling”. A sample Coping-Motive item included: “To forget your worries”. A sample Conformity-Motive item included: “To fit in with a group you like”. The α reliabilities in this sample were Social (.92), Enhancement (.89), Coping (.83), and Conformity (.84).
2.2.3. Impaired-control-over-drinking (IC).
This scale reflects 10-items from the Impaired-Control Scale Part 3 (Heather et al., 1993). Higher scores reflect a lack of perceived control over drinking (i.e., an inability to stop drinking). Two sample items included: “Even if I intended having only one or two drinks, I would end up having many more” and reverse scored “I could cut down my drinking (i.e. drink less) if I wanted to”. Responses range from 1 = strongly disagree to 5 = strongly agree. The α reliability for this sample was (.82).
2.2.4. Heavy-episodic-drinking.
This a single item measure of the frequency of heavy-episodic-drinking (Wood et al., 1992). “How many times in the past year (or when you were drinking) did you drink 5 or more bottles (4 for women) or cans of beer, glasses of wine, or drinks of distilled spirits on a single occasion?” Responses ranged from 0 = never to 7 = daily or nearly daily.
2.2.5. Alcohol-Related-Problems.
We used the Young Adult Alcohol Problems Screening Test (YAAPST; Hurlbut & Sher, 1992) to assess common consequences from drinking young adults’ experience. Sample items included “Have you ever driven a car when you knew you had too much to drink and drive safely?” and “Have you ever gotten into physical fights when drinking?” The α reliability for this sample was (.88).
2.3. Analyses
Using Mplus 7.4 (Muthén & Muthén, 1998–2016), we evaluated a path-model with chi-square statistics, RMSEA (Browne & Cudeck, 1993; Hu & Bentler, 1998), and CFI (Bentler, 1990). Both discrepancy and high-standards were tested as predictors of the four drinking-motives and, in turn, IC, with heavy-episodic-drinking and alcohol-related-problems as the outcomes. See Figure 1 for the full conceptual model. We utilized gender as a covariate for all outcomes.
Figure 1. Conceptual Model.
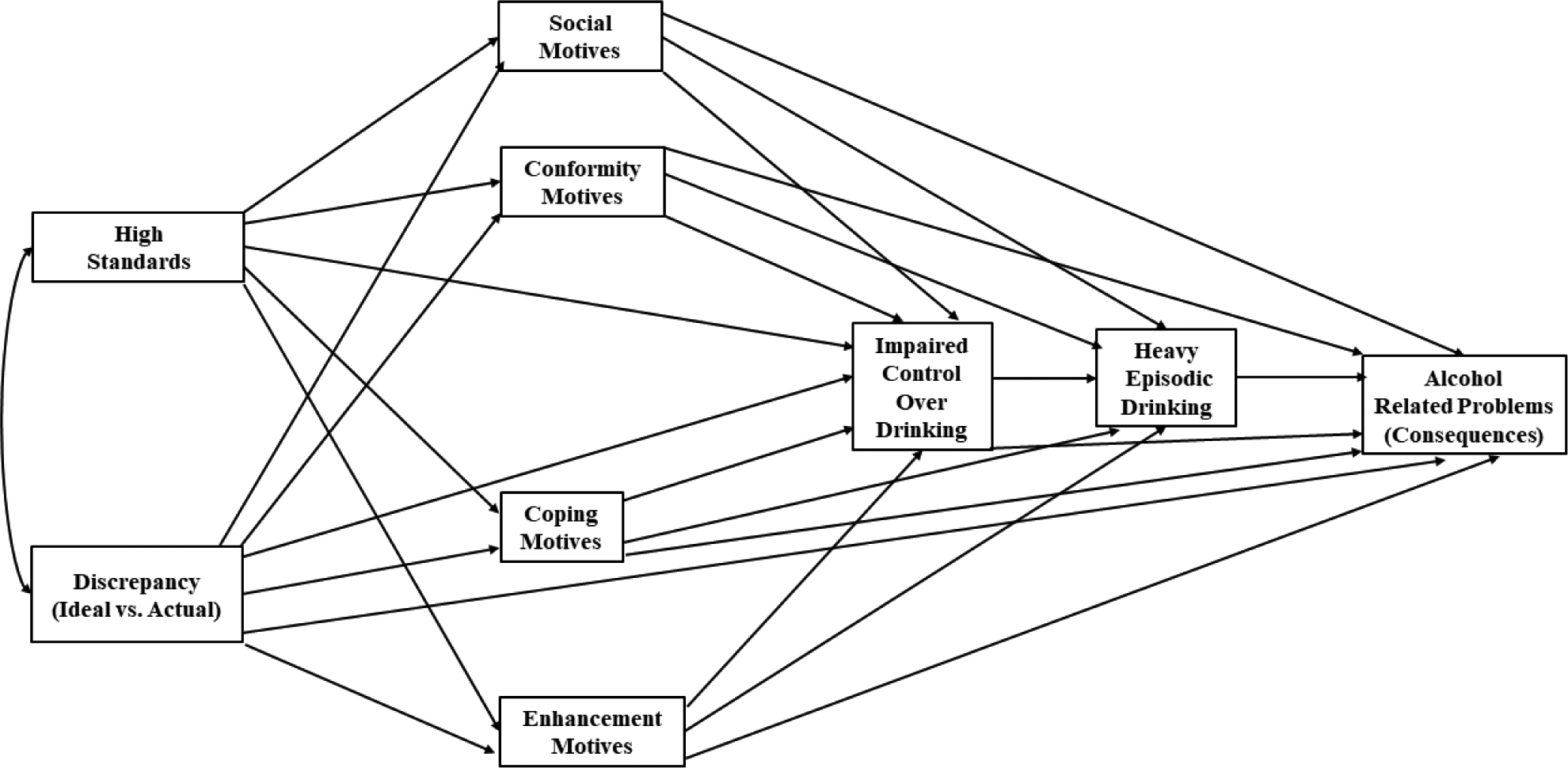
Conceptual structural equation model with all hypothesized direct effects. Gender was used as a covariate for all outcomes and is excluded for parsimony.
Two, three and four-path indirect effects were tested by examining whether the parametric bootstrapped (K = 20,000) 99% asymmetric confidence interval around the estimates of the indirect-effects included zero or not (Hancock & Liu, 2012; MacKinnon, 2008; Taylor et al., 2007). Significant mediated effects do not include zero in the interval. We used this much more stringent 99% C.I. rather than the normative 95% C.I. level in an effort to control for type one errors.
3. Results
All hypothesized paths are included in the conceptual model (Figure 1) and significant standardized direct-paths are included in the fit model (Figure 2). Gender was a covariate for all outcomes in the model. Table 1 displays all correlations, means and standard deviations for all variables.
Figure 2.
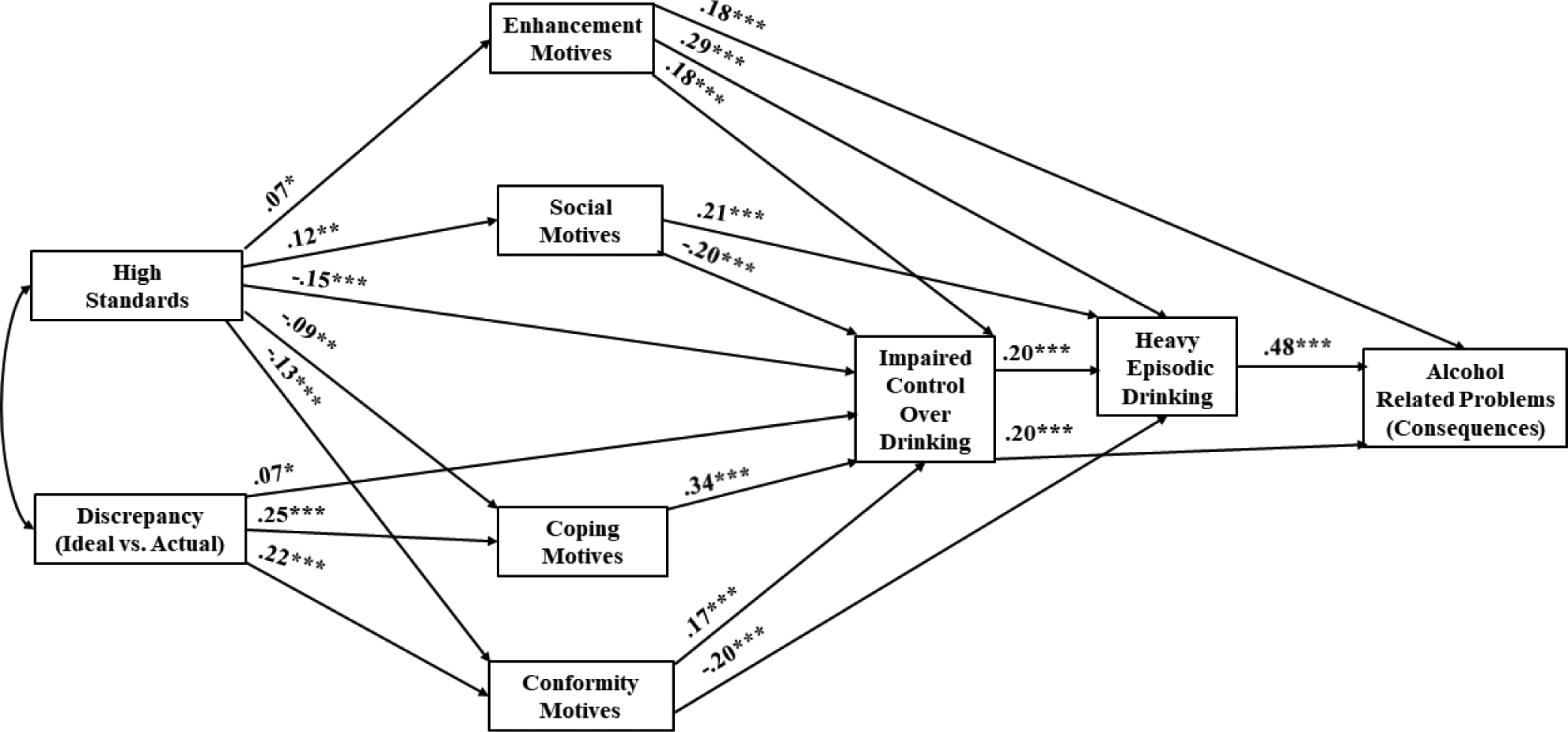
Final fit model with significant direct paths. Gender was used as a covariate for all outcomes and is excluded for clarity. * p < .05; ** p < .01; *** p < .001
Table 1.
Means, standard deviations, and correlations among all variables
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. High-standards | 5.55 | 1.26 | - | ||||||||
| 2. Discrepancy | 3.44 | 1.66 | 0.00 | - | |||||||
| 3. Enhancement-motives | 3.03 | 1.17 | 0.06 | −0.01 | - | ||||||
| 4. Conformity-motives | 1.79 | 0.86 | −0.14 | 0.22 | 0.24 | - | |||||
| 5. Social-motives | 3.49 | 1.14 | 0.11 | 0.03 | 0.74 | 0.33 | - | ||||
| 6. Coping-motives | 2.20 | 0.98 | −0.09 | 0.25 | 0.47 | 0.46 | 0.48 | - | |||
| 7. Impaired-control | 1.87 | 0.74 | −0.22 | 0.19 | 0.23 | 0.35 | 0.14 | 0.44 | - | ||
| 8. Heavy-episodic-drinking | 2.02 | 1.84 | −0.03 | −0.04 | 0.49 | 0.06 | 0.44 | 0.29 | 0.27 | - | |
| 9. Alcohol-related-problems | 0.60 | 0.55 | −0.05 | 0.06 | 0.49 | 0.20 | 0.42 | 0.37 | 0.40 | 0.63 | - |
n = 941
The base model yielded a χ2 (3 df) = 4.173, p = .2433; RMSEA = 0.02, 90% CI [0.00, 0.062]; CFI = 1.00. Due to the complexity of our proposed model, which included a large number of potential mediated pathways, we only discuss 4-path mediated effects at 99% C.I. in the text of the paper. Further, Table 2 displays significant indirect effects at the 99% confidence interval only due to the large number of significant mediated effects.
Table 2.
Mediated indirect pathways
| Pathway Effects | Indirect Effect | Z-Score | P-Value | 99% CI |
|---|---|---|---|---|
| Impaired Control (IC) | ||||
| High-Standards→Social-Motives→IC | −0.014 | −2.571 | 0.010 | (−0.031, −0.003) |
| High-Standards→Conformity-Motives→IC | −0.012 | −2.738 | 0.006 | (−0.026, −0.003) |
| High-Standards→Coping-Motives→IC | −0.017 | −2.652 | 0.008 | (−0.036, −0.002) |
| Discrepancy→Conformity-Motives→IC | 0.017 | 3.666 | 0.001 | (0.007, 0.030) |
| Discrepancy→Coping-Motives→IC | 0.039 | 5.172 | 0.001 | (0.022, 0.060) |
| Heavy Episodic Drinking (HED) | ||||
| High-Standards→Social-Motives→HED | 0.036 | 2.802 | 0.005 | (0.008, 0.075) |
| High-Standards→Conformity-Motives→HED | 0.036 | 3.007 | 0.003 | (0.009, 0.072) |
| High-Standards→IC→HED | −0.044 | −3.376 | 0.001 | (−0.081, −0.015) |
| Discrepancy→Conformity-Motives→HED | −0.049 | −4.140 | 0.001 | (−0.083, −0.023) |
| Social-Motives→IC→HED | −0.065 | −3.383 | 0.001 | (−0.123, −0.022) |
| Enhancement-Motives→IC→HED | 0.057 | 3.150 | 0.002 | (0.017, 0.112) |
| Conformity-Motives→IC→HED | 0.073 | 3.443 | 0.001 | (0.027, 0.134) |
| Coping-Motives→IC→HED | 0.128 | 4.602 | 0.001 | (0.063, 0.209) |
| Discrepancy→Conformity-Motives→IC→HED | 0.008 | 3.002 | 0.003 | (0.003, 0.017) |
| Discrepancy→Coping-Motives→IC→HED | 0.020 | 3.800 | 0.001 | (0.008, 0.036) |
| Alcohol-Related Consequences (ARC) | ||||
| IC→HED→ARC | 0.076 | 5.184 | 0.001 | (0.041, 0.117) |
| Conformity-Motives→IC→ARC | 0.023 | 3.365 | 0.001 | (0.009, 0.044) |
| Social-Motives→IC→ARC | −0.021 | −3.602 | 0.001 | (−0.038, −0.008) |
| Enhancement-Motives→IC→ARC | 0.018 | 3.254 | 0.001 | (0.006, 0.034) |
| Coping-Motives→IC→ARC | 0.040 | 4.782 | 0.001 | (0.021, 0.064) |
| High-Standards→IC→ARC | −0.014 | −3.632 | 0.001 | (−0.024, −0.005) |
| Conformity-Motives→IC→HED→ARC | 0.011 | 3.276 | 0.001 | (0.004, 0.021) |
| Social-Motives→IC→HED→ARC | −0.010 | −3.249 | 0.001 | (−0.019, −0.003) |
| Enhancement-Motives→IC→HED→ARC | 0.009 | 3.003 | 0.002 | (0.003, 0.018) |
| Coping-Motives→IC→HED→ARC | 0.019 | 4.292 | 0.001 | (0.009, 0.033) |
| High-Standards→Social-Motives→HED→ARC | 0.005 | 2.740 | 0.006 | (0.001, 0.012) |
| High-Standards→Conformity-Motives→HED→ARC | 0.005 | 3.010 | 0.003 | (0.001, 0.011) |
| Discrepancy→Conformity-Motives→HED→ARC | −0.007 | −3.999 | 0.001 | (−0.013, −0.003) |
| High-Standards→IC→HED→ARC | −0.007 | −3.280 | 0.008 | (−0.013, −0.002) |
| Discrepancy→Coping-Motives→IC→HED→ARC | 0.003 | 3.611 | 0.001 | (0.001, 0.006) |
Significant indirect mediated effects between all variables as well as Z-scores, P-values, and CI listed. Variables were shorted within the table; IC=Impaired-control, HED=Heavy-episodic-drinking, ARC= Alcohol-related-consequences
We presented standardized beta coefficients for significant effects with the gender covariate. Being male was significantly related to more social-motives (β = .129; s.e. = .032; Z = 3.974; p <.001), conformity-motives (β = .144; s.e. =.032; Z = 4.489, p < .001), as well as more heavy-episodic-drinking (β = .192; s.e. = .028; Z = 6.799; p < .001).
3.1. Four-path-mediated-effects presented at 99% C.I.
3.1.1. Alcohol-Related-Problems.
Higher levels of discrepancy were indirectly linked to greater alcohol-related-problems through higher coping-motives, greater IC, and more heavy-episodic-drinking (indirect-effect = 0.003; Z = 3.611; p = 0.001; 99% CI [0.001, 0.006]). No four-path mediated effects from high-standards to alcohol-related problems were significant at the 99% confidence interval.
4. Discussion
Self-Discrepancy-Theory (Higgins, 1987) posits differences between the ideal and the actual self may result in psychological discomfort, often leading to negative emotional states. We applied this theory to Hersh and Hussong’s (2009) Self-Medication theory of alcohol use to reduce negative emotional states. Specifically, this study explored how the high standards and discrepancy dimensions of Slaney et al.’s (2001) conceptualization of perfectionism were indirectly related to alcohol-use through drinking-motives and impaired control over drinking (IC). We hypothesized there would be a distinction between high-standards and discrepancy, which is consistent with adaptive and maladaptive perfectionism, respectively. Consistent with Self-Discrepancy-Theory, our findings demonstrated how discrepancy was related to greater impaired-control-over-drinking while high-standards alone was protective of IC. These findings expand on previous literature by demonstrating the connection between discrepancy and IC was accounted for by both internal and external negative-reinforcing motives (i.e., coping and conformity, respectively), and was in turn, associated with greater alcohol-use and alcohol-related-problems. This suggests those higher in discrepancy may experience IC because they are drinking to alleviate negative emotional states produced by the discomfort of not living up to one’s ideal self. Further, the distinction between negative-reinforcing and positive-reinforcing motives for drinking (e.g., social and enhancement) in relation to discrepancy demonstrates support for the Self-Medication-Hypothesis (Hersh & Hussong, 2009). Reducing perfectionistic discrepant cognitions (specifically negative self-evaluations) may be a possible therapeutic target for some individuals with AUDs.
Our study replicates and extends findings regarding maladaptive perfectionism and coping-motives. While coping-motives were known to be associated with discrepancy (Rice & Van Arsdale, 2010), we demonstrated that conformity-motives are also important in explaining the relation between discrepancy and alcohol-outcomes. In social contexts, those with higher levels of discrepancy appear more likely to use alcohol to try to fit in socially with others than those with lesser degrees of discrepancy. Conformity-motives are externally-driven, negative-reinforcing motives, and perfectionism discrepancy is often linked to performance-based concerns and social-anxiety (Egan et al., 2011). Conceivably, maladaptive perfectionists may use alcohol to alleviate their own negative affect as well as to avoid uncomfortable social interactions.
Our findings are consistent with Slaney et al.’s (2001) conceptualization that high-standards are required for discrepancy to occur, yet, attainable high-standards are overall adaptive (Slaney et al., 2011). For instance, we found high-standards were negatively linked to more coping and conformity-motives, and in turn, less IC, alcohol-use, and alcohol-related-problems. Nevertheless, high-standards were also directly and positively linked to more social and enhancement-motives. This suggests high-standards are positively associated with positive-reinforcement-motives (i.e. social and enhancement) and negatively associated with negative-reinforcement-motives (i.e. coping and conformity). Hence, our a priori hypotheses were only partially supported. It is important to note high-standards were also indirectly related to both less alcohol-use and fewer alcohol-related-problems through less IC. This suggests holding oneself to higher standards may be a protective factor against some symptoms of AUDs, such as IC. This finding is novel to the literature at large.
While these findings are novel, as one of the first studies to evaluate Slaney et al.’s (2001) multi-dimensional perfectionism in the prediction of all four drinking-motives and alcohol outcomes, this study is not without limitations. Sironic and Reeve (2015) suggest there are a number of measures of perfectionism worth investigating and our results here are limited to just Slaney et al.’s (2001) concept of perfectionism facets using the Revised Almost Perfect Scale (APS-R). This scale contains three factors: Perfectionism-Discrepancy, High-Standards, and Orderliness. A limitation of the APS-R include one discrepancy item which lacks specificity in the degree of one’s ideal standards (e.g., my performance rarely measures up to my standards). Additionally, the APS-R does not measure socially-prescribed perfectionism which is a dimension of the Multidemensional Perfectionism Scale (MPS; Hewitt & Flett, 1991). Socially-prescribed perfectionism measures one’s beliefs regarding other people’s expectations of him/her. Bieling and colleagues explained this subscale of the MPS is often interpreted as a “perception that other people expect one to be perfect and that others are harsh, punitive judges” (Bieling, Israeli, & Antony, 2004). Socially-prescribed perfectionism has been found to be associated with the depression facet of neuroticism (Hill et al., 1997), giving it a strong tie to negative consequences of alcohol use. Nevertheless, Suddarth and Slaney (2001) found the Perfectionism-Discrepancy subscale and Hewitt and Flett’s (1991) Socially Prescribed Perfectionism subscale were significantly correlated, and both subscales loaded into the same factor model. However, it does seem prudent to replicate our exploratory findings here utilizing multiple comprehensive measures of perfectionism which include socially prescribed perfectionism.
While our results were largely consistent with hypotheses, further research is necessary to confirm these findings due to the exploratory nature of this study. Further, with cross-sectional data, this study only explored associations and multiple-wave studies are necessary to understand if discrepancy is prospectively predictive of drinking-motives or IC. It is unknown whether or not discrepancy is prospectively related to the onset of alcohol-use and the development of AUDs across the lifespan. Mixed results related to high-standards suggests they should be investigated further. Finally, this study did not investigate the potential underlying mechanisms in the relationship between perfectionism and drinking-motives. Motives and drinking behavior are influenced by many predictors, including one’s context, beliefs about alcohol, and other personality traits (Hultgren, Canning & Larimer, 2018). Therefore, further work is necessary to fully understand how discrepancy contributes to one’s risk for heavy alcohol-use and alcohol-related-problems.
Still, this study provides clarification on how multi-dimensional perfectionism is related to alcohol-use. This study presents novel findings about differences among drinking-motives and alcohol-outcomes for both adaptive and maladaptive perfectionism. This is one of the first studies to explore discrepancy and high standards with several types of motives. Adaptive perfectionists (i.e., those with high standards) appear to drink primarily for positive-reinforcement while maladaptive perfectionists (i.e., those high in discrepancy) may drink mainly for negative-reinforcement (i.e., self-medication reasons). This study expands on our knowledge of how personality traits are related to risk factors for AUDs such as IC. Additionally, this study may contribute to further advances in prevention and interventions for alcohol-use, such as helping to suggest which aspects of perfectionism (i.e. discrepancy) might be promising targets for intervention to ameliorate AUDs. Treatments for discrepancy typically involve CBT-focused treatment (LaSota, Ross & Kearney, 2017) or functional analysis of behavior (Rice, Neimeyer & Taylor, 2011), which could be incorporated into future intervention programs for alcohol-use within the same theoretical model. Future research would benefit from the continued exploration of how discrepancy and high standards are related to alcohol use through IC and drinking-motives.
Highlights.
Discrepancy was directly linked to more coping and conformity-motives.
Coping, enhancement, & conformity-motives were linked to more impaired-control.
Social-motives were linked to less impaired-control.
High-standards were linked to more social-motives and thus, less impaired-control.
Coping-motives and impaired-control mediated discrepancy on alcohol-outcomes.
Funding
This work was supported by NIH/NIAAA award number F31 AA027471 to Jessica R. Canning, NIH/NIAAA award number K01 AA024160-01A1 and Burton Family Foundation award number FP11815 to Julie A. Patock-Peckham, NIH/NIAAA award numbers R21 AA026918 and UH3 AA02614, the Mary F. Lane Endowed Professorship, and moonshot initiative pilot funding from the University of Florida Center for Research to Investigate Substance use & Pain (UF-CRISP) to Robert F. Leeman.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Achtziger A, & Bayer UC (2013). Self-control mediates the link between perfectionism and stress. Motiv. Emot, 37(3), 413–423. [Google Scholar]
- Bahramnejad A, Rabani-Bavojdan M, Rabani-Bavojdan M, & Kaviani N (2015). The value of perfectionism in predicting coping strategies in drug-user women. Addict. Health, 7(3–4), 157. [PMC free article] [PubMed] [Google Scholar]
- Bardone-Cone AM, Brownstone LM, Higgins MK, Harney MB, & Fitzsimmons-Craft EE (2012). Predicting Difficulties Controlling Overeating and Drinking When Experiencing Negative Affect in Undergraduate Women. J. Soc. Clin. Psychol, 31(10), 1051–1073. [Google Scholar]
- Bentler PM (1990). Comparative fit indexes in structural models. Psychol. Bull, 107(2), 238–246. [DOI] [PubMed] [Google Scholar]
- Bieling PJ, Israeli AL, & Antony MM (2004). Is perfectionism good, bad, or both? Examining models of the perfectionism construct. Pers. Individ. Differ, 36(6), 1373–1385. [Google Scholar]
- Browne MW, Cudeck R (1993). Alternative ways of assessing model fit In Bollen, Lond JS (eds.) Test. Struct. Equ. Model Newbury Park, CA: Sage. [Google Scholar]
- Carey KB, & Correia CJ (1997). Drinking motives predict alcohol-related problems in college students. J. Stud. Alcohol, 58(1), 100–105. [DOI] [PubMed] [Google Scholar]
- Cooper ML (1994). Motivations for alcohol use among adolescents: Development and validation of a four-factor model. Psychol. Assess, 6(2), 117–128. [Google Scholar]
- Corbin WR, Farmer NM, & Nolen-Hoekesma S (2013). Relations among stress, coping strategies, coping motives, alcohol consumption and related problems: A mediated moderation model. Addict. Behav, 38(4), 1912–1919. [DOI] [PubMed] [Google Scholar]
- Ebbert AM, Patock-Peckham JA, Luk JW, Voorhies KR, Warner O, & Leeman RF (2018). The mediating role of anxiety sensitivity in uncontrolled drinking: A look at gender specific parental influences. Alcohol: Clin. Exp. Res, 42(5), 914–925. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Egan SJ, Wade TD, & Shafran R (2011). Perfectionism as a transdiagnostic process: A clinical review. Clin. Psychol. Rev, 31(2), 203–212. [DOI] [PubMed] [Google Scholar]
- Grant VV, Stewart SH, O’Connor RM, Blackwell E, & Conrod PJ (2007). Psychometric evaluation of the five-factor Modified Drinking Motives Questionnaire—Revised in undergraduates. Addict. Behav, 32(11), 2611–2632. [DOI] [PubMed] [Google Scholar]
- Hancock GR, Liu M (2012). Bootstrapping standard errors and data-model fit statistics in structural equation modeling In Hoyle RH (ed.) Handbook of structural equation modeling. New York: The Gilford Press. [Google Scholar]
- Heather N, Tebbutt JS, Mattick RP, & Zamir R (1993). Development of a scale for measuring impaired control over alcohol consumption: a preliminary report. J. Stud. Alcohol, 54(6), 700–709. [DOI] [PubMed] [Google Scholar]
- Hersh MA, & Hussong AM (2009). The association between observed parental emotion socialization and adolescent self-medication. J. Abnorm. Child Psychol, 37(4), 493–506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hewitt PL, & Flett GL (1991). Perfectionism in the self and social contexts: conceptualization, assessment, and association with psychopathology. J. Pers. Soc. Psychol, 60(3), 456. [DOI] [PubMed] [Google Scholar]
- Higgins ET (1987). Self-discrepancy: A theory relating self and affect. Psychol. Rev, 94(3), 319–340. [PubMed] [Google Scholar]
- Hill RW, McIntire K, & Bacharach VR (1997). Perfectionism and the big five factors. J. Soc. Behav. Pers, 12(1), 257. [Google Scholar]
- Hu L, & Bentler PM (1998). Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychol. Method, 3(4), 424–453. [Google Scholar]
- Hultgren B, Canning JR, & Larimer ME (2018). The Prevalence of High-Risk Drinking Among College Students In Cimini D & Rivero E (Eds). Promoting Behavioral Health and Reducing Risk among College Students: A Comprehensive Approach. New York: Routledge. [Google Scholar]
- Hurlbut SC, & Sher KJ (1992). Assessing alcohol problems in college students. J. Am. Coll. Health, 41(2), 49–58. [DOI] [PubMed] [Google Scholar]
- Kaviani N, Mohammadi K, & Zarei E (2014). The relationship between perfectionism and coping strategies in drug-dependent men. Addict. Health, 6(1–2), 9. [PMC free article] [PubMed] [Google Scholar]
- Kuntsche E, Knibbe R, Gmel G, & Engels R (2005). Why do young people drink? A review of drinking motives. Clin. Psychol. Rev, 25(7), 841–861. [DOI] [PubMed] [Google Scholar]
- Kuntsche E, von Fischer M, & Gmel G (2008). Personality factors and alcohol use: A mediator analysis of drinking motives. Personal. Individ. Differ, 45(8), 796–800. [Google Scholar]
- LaBrie JW, Hummer JF, & Pedersen ER (2007). Reasons for drinking in the college student context: The differential role and risk of the social motivator. J. Stud. Alcohol Drugs, 68(3), 393–398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- LaSota MT, Ross EH, & Kearney CA (2017). A cognitive-behavioral-based workshop intervention for maladaptive perfectionism. J. Ration.-Emot. Cogn.-Behav. Ther, 35(3), 314–328. [Google Scholar]
- Leeman RF, Toll BA, Taylor LA, & Volpicelli JR (2009). Alcohol-induced disinhibition expectancies and impaired control as prospective predictors of problem drinking in undergraduates. Psychol. Addict. Behav, 23(4), 553–563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Loxton NJ, Bunker RJ, Dingle GA, & Wong V (2015). Drinking not thinking: A prospective study of personality traits and drinking motives on alcohol consumption across the first year of university. Personal. Individ. Differ, 79, 134–139. [Google Scholar]
- MacKinnon DP (2008). Introduction to Statistical Mediation Analysis. New York, NY: Taylor & Francis Group/Lawrence Erlbaum Associates. [Google Scholar]
- Muthén LK, & Muthén B (2016). Mplus. The comprehensive modelling program for applied researchers: user’s guide, 5. [Google Scholar]
- Neighbors C, Lee CM, Lewis MA, Fossos N, & Larimer ME (2007). Are social norms the best predictor of outcomes among heavy-drinking college students?. J. Stud. Alcohol Drugs, 68(4), 556–565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patock-Peckham JA, Cheong J, Balhorn ME, & Nagoshi CT (2001). A social learning perspective: A model of parenting styles, self-regulation, perceived drinking control, and alcohol use and problems. Alcohol: Clin. Exp. Res, 25(9), 1284–1292. [PubMed] [Google Scholar]
- Patock-Peckham JA, & Corbin WR (2019). Perfectionism and self-medication as mediators of the links between parenting styles and drinking outcomes. Addict. Behav. Report, December; 10.1016/jabrep.2019.100218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patock-Peckham JA, King KM, Morgan-Lopez AA, Ulloa EC, & Filson Moses JM (2011). Gender-specific mediational links between parenting styles, parental monitoring, impulsiveness, drinking control, and alcohol-related problems. J. Stud. Alcohol Drugs, 72(2), 247–258. [DOI] [PubMed] [Google Scholar]
- Patock-Peckham JA, & Morgan-Lopez AA (2006). College drinking behaviors: Mediational links between parenting styles, impulse control, and alcohol-related outcomes. Psychol. Addict. Behav, 20(2), 117–125. [DOI] [PubMed] [Google Scholar]
- Read JP, Wood MD, Kahler CW, Maddock JE, & Palfai TP (2003). Examining the role of drinking motives in college student alcohol use and problems. Psychol. Addict. Behav, 17(1), 13–23. [DOI] [PubMed] [Google Scholar]
- Rice KG, & Van Arsdale AC (2010). Perfectionism, perceived stress, drinking to cope, and alcohol-related problems among college students. J. Couns. Psychol, 57(4), 439–450. [Google Scholar]
- Rice KG, Neimeyer GJ, & Taylor JM (2011). Efficacy of coherence therapy in the treatment of procrastination and perfectionism. Couns. Outcome Res. Eval, 2(2), 126–136. [Google Scholar]
- Sher KJ, & Walitzer KS (1986). Individual differences in the stress-response-dampening effect of alcohol: A dose-response study. J. Abnorm. Psychol, 95(2), 159–167. [DOI] [PubMed] [Google Scholar]
- Sironic A, & Reeve RA (2015). A combined analysis of the Frost Multidimensional Perfectionism Scale (FMPS), Child and Adolescent Perfectionism Scale (CAPS), and Almost Perfect Scale—Revised (APS-R): Different perfectionist profiles in adolescent high school students. Psychol. Assess, 27(4), 1471–1483. [DOI] [PubMed] [Google Scholar]
- Slaney RB, & Johnson DG (1992). The almost perfect scale. Unpublished manuscript, Pennsylvania State University. [Google Scholar]
- Slaney RB, Rice KG, Mobley M, Trippi J, & Ashby JS (2001). The revised almost perfect scale. Meas. Eval. Couns. Dev, 34(3), 130–146. [Google Scholar]
- Stairs AM, Smith GT, Zapolski TC, Combs JL, & Settles RE (2012). Clarifying the construct of perfectionism. Assess., 19(2), 146–166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stoeber J (2018). The psychology of perfectionism: An introduction In Stoeber J (Ed.), The psychology of perfectionism: Theory, research, applications (pp. 3–16). London: Routledge. [Google Scholar]
- Stoeber J (2012). Perfectionism and Performance. Oxford University Press. [Google Scholar]
- Stoeber J, & Janssen DP (2011). Perfectionism and coping with daily failures: Positive reframing helps achieve satisfaction at the end of the day. Anxiety Stress Copin, 24(5), 477–497. [DOI] [PubMed] [Google Scholar]
- Stoeber J, & Rennert D (2008). Perfectionism in school teachers: Relations with stress appraisals, coping styles, and burnout. Anxiety Stress Copin, 21(1), 37–53. [DOI] [PubMed] [Google Scholar]
- Suddarth BH, & Slaney RB (2001). An investigation of the dimensions of perfectionism in college students. Meas. Eval. Couns. Dev, 34(3), 157–165. [Google Scholar]
- Taylor AB, MacKinnon DP, & Tein JY (2008). Tests of the three-path mediated effect. Organ. Res. Method, 11(2), 241–269. [Google Scholar]
- Vaughan CL, Stangl BL, Schwandt ML, Corey KM, Hendershot CS, & Ramchandani VA (2019). The relationship between impaired control, impulsivity, and alcohol self-administration in nondependent drinkers. Exper. Clin. Psychopharm., 27(3), 236–246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wood MD, Nagoshi CT, & Dennis DA (1992). Alcohol norms and expectations as predictors of alcohol use and problems in a college student sample. Am. J. Drug Alcohol Abus, 18(4), 461–476. [DOI] [PubMed] [Google Scholar]
- Wormington SV, Anderson KG, & Corpus JH (2011). The role of academic motivation in high school students’ current and lifetime alcohol consumption: Adopting a self-determination theory perspective. J. Stud. Alcohol Drugs, 72(6), 965–974. [DOI] [PMC free article] [PubMed] [Google Scholar]