

Abstract
Background
Tuberculosis (TB) is the leading cause of death from a single infectious agent, with around 1.5 million deaths reported in 2018, and is a major contributor to suffering worldwide, with an estimated 10 million new cases every year. In the context of the World Health Organization’s End TB strategy and the quest for digital innovations, there is a need to understand what is happening around the world regarding research into the use of digital technology for better TB care and control.
Objective
The purpose of this scoping review was to summarize the state of research on the use of digital technology to enhance TB care and control. This study provides an overview of publications covering this subject and answers 3 main questions: (1) to what extent has the issue been addressed in the scientific literature between January 2016 and March 2019, (2) which countries have been investing in research in this field, and (3) what digital technologies were used?
Methods
A Web-based search was conducted on PubMed and Web of Science. Studies that describe the use of digital technology with specific reference to keywords such as TB, digital health, eHealth, and mHealth were included. Data from selected studies were synthesized into 4 functions using narrative and graphical methods. Such digital health interventions were categorized based on 2 classifications, one by function and the other by targeted user.
Results
A total of 145 relevant studies were identified out of the 1005 published between January 2016 and March 2019. Overall, 72.4% (105/145) of the research focused on patient care and 20.7% (30/145) on surveillance and monitoring. Other programmatic functions 4.8% (7/145) and electronic learning 2.1% (3/145) were less frequently studied. Most digital health technologies used for patient care included primarily diagnostic 59.4% (63/106) and treatment adherence tools 40.6% (43/106). On the basis of the second type of classification, 107 studies targeted health care providers (107/145, 73.8%), 20 studies targeted clients (20/145, 13.8%), 17 dealt with data services (17/145, 11.7%), and 1 study was on the health system or resource management. The first authors’ affiliations were mainly from 3 countries: the United States (30/145 studies, 20.7%), China (20/145 studies, 13.8%), and India (17/145 studies, 11.7%). The researchers from the United States conducted their research both domestically and abroad, whereas researchers from China and India conducted all studies domestically.
Conclusions
The majority of research conducted between January 2016 and March 2019 on digital interventions for TB focused on diagnostic tools and treatment adherence technologies, such as video-observed therapy and SMS. Only a few studies addressed interventions for data services and health system or resource management.
Keywords: tuberculosis, mHealth, eHealth, medical informatics
Introduction
Background
Tuberculosis (TB) is among the top 10 causes of death worldwide, the leading cause from a single infectious agent, above HIV or AIDS, and the leading killer of people with HIV [1]. The most vulnerable people are the poorest, with 95% of cases and 98% of deaths occurring in low- and middle-income countries [2]. Although most TB deaths are preventable if detected and treated at an early stage, TB still caused an estimated 1.5 million deaths in 2018 [1].
In September 2015, the Global TB Program of the World Health Organization (WHO) developed an agenda for action on digital health exploring what contributions can be offered by this technology to the care and control of TB. This agenda highlighted opportunities and the latest information available on the use of digital health technology to combat TB [3]. Its use was categorized into 4 types of function. First, patient care and electronic directly observed therapy (eDOT), mainly refer to TB screening, TB diagnosis, and treatment adherence. As part of the latter, eDOT concerns the general recommendation of supervising and supporting patients when they take their TB drugs, thus ensuring the regular intake of medicines at home and the avoidance of daily or frequent visits to clinics. Second, surveillance and monitoring covering health information system management, measurement of the burden of TB disease and death, and the monitoring of drug resistance. Third, program management includes items such as drug stock management systems, the development of norms, and training. Fourth, electronic learning (e-learning) is the function by which electronic media and devices are used as tools for improving access to training, communication, and interaction [4].
Previously, directly observed therapy was the standard of care to ensure treatment adherence by patients throughout their long treatment duration and monitoring for adverse drug effects [5]. However, ensuring patients’ adherence to the full course of medications has traditionally been a critical challenge in TB treatment as patients needed to be observed by a health provider in a health facility, or the health provider, including community workers, had to visit the patients daily. After the introduction of digital health technology, eDOT became a significant part of digital health interventions (DHIs). Many studies were conducted around video-observed therapy (VOT), SMS, and mobile apps. In 2010, the GeneXpert Mycobacterium tuberculosis (MTB)/rifampicin (RIF) assay was introduced, after which an increasing number of studies assessed digital health technology in the identification of active TB cases. Most high-income countries use digital diagnostic tools to reduce diagnostic delays and prevent further transmission in the community [6].
In 2018, the WHO released a general classification on DHIs that are applicable to all conditions [7]. This classification is organized by the targeted primary user: clients, health care providers, health systems or resource managers, and data services. First, clients are the potential or current users of health services. Second, health care providers are members of the health workforce who deliver health services. Third, health system managers and resource managers are involved in administrative or surveillance works, including supply chain management, health financing, and human resource management. Finally, data services consist of supporting a wide range of activities related to data collection, management, use, and exchange.
Objective
To achieve the End TB Strategy milestones for 2020 and 2025—TB incidence needs to be falling by 10% per year by 2025, and the proportion of people with TB who die from the disease needs to fall to 6.5% by 2025—as well as the 2030 to 2035 global targets, digital health is considered critical [3]. In other words, the existing approaches to patient care, surveillance and monitoring, program management, and e-learning could be strengthened by the utilization of digital health technologies, including mobile phones, big data, genetic algorithms, and artificial intelligence.
The goal of this scoping review was to provide an overview of the publications covering this subject. The results of this study could ultimately be applied to enhance the use of digital technology in TB control more sustainably and effectively. This study answers 3 main questions. First, to what extent has the subject been covered in the scientific literature between January 2016 and March 2019? Second, which countries were investing in research in this field? Finally, what digital technologies were used? The study compares results based on 2 types of classifications: one by function and the other by targeted user.
Methods
Scoping Review
A scoping review documents the entire process in sufficient detail, which could be replicated by other scholars (Textbox 1). It assigns a more precise meaning to ambiguous terms and includes them in search criteria, which makes this review evidence based. In addition, a scoping review excludes the quality of papers from the selection criteria, meaning that it is less biased in the inclusion criteria [8].
Five processes of scoping review.
Identify the research question with a broad approach.
Identify relevant studies.
Study selection.
Chart the data by synthesizing and interpreting the qualitative data.
Collate, summarize, and report the results.
Following the framework of a standard scoping review, this work first identified research questions that were as wide as possible to include all of the relevant studies on the use of digital health technology for TB care and control. Afterwards, relevant studies were collected from 2 major databases pertinent to global health, followed by the process of study selection. Finally, the findings were categorized into 4 types of interventions following logic derived from 2 WHO-recommended approaches. One by function, including patient care, surveillance and monitoring, program management, and e-learning [4], and the other by the primary targeted user, such as clients, health care providers, health system or resource managers, and data services [5].
Search Strategy
To identify all relevant studies, a comprehensive search strategy was developed to include, but not be confined to, (tuberculosis OR tuberculosis infection OR TB OR tuberculosis disease OR mycobacterium tuberculosis) AND (digital OR ehealth OR mhealth OR technology OR telemedicine OR mobile OR big data OR artificial intelligence OR real-time OR video). These search terms were used to identify relevant literature in 2 primary databases, PubMed and Web of Science.
Study Selection
The scoping review included articles covering both quantitative and qualitative research, systematic reviews, editorials and viewpoints, and correspondence indexed in the PubMed or Web of Science databases. The publication dates ranged from January 2016 to March 2019. This date range was selected to cover the period after the WHO recommended date for worldwide adoption of the new End TB Strategy in 2016. On the basis of the inclusion and exclusion criteria, the articles collected were screened for relevance. The first selection was made by reviewing the titles and abstracts of the articles. English, Chinese, and French languages were considered for selection, whereas Russian was excluded. A final selection was made after reviewing the full texts.
Of the original 1005 articles, 333 were excluded as duplicate studies, and 449 did not meet the inclusion criteria based on the title and abstract. As a result, 223 articles were assessed in full. Articles were eligible for inclusion if they focused on the use of digital health technologies in TB patient care, surveillance, programmatic function, or e-learning. Articles on bovine TB, TB drug development, epidemiology of TB, or evaluation on the quality of technology were excluded. After full reading of the 223 articles, 62 were excluded, and 1 article (in Russian) without English or Chinese summary was also excluded. A total of 15 articles, which were not available in full text, but for which only the conference abstracts or summary existed, were excluded. Of the original 1005, 527 studies did not meet the inclusion criteria (511 were not relevant, 15 were not available with full-text, and 1 was in Russian). Therefore, a total of 145 studies, including 140 in English and 5 in Chinese, were finally identified as relevant (see Multimedia Appendix 1 [3,6,9-150]). Figure 1 summarizes the flow of literature search and screening.
Figure 1.
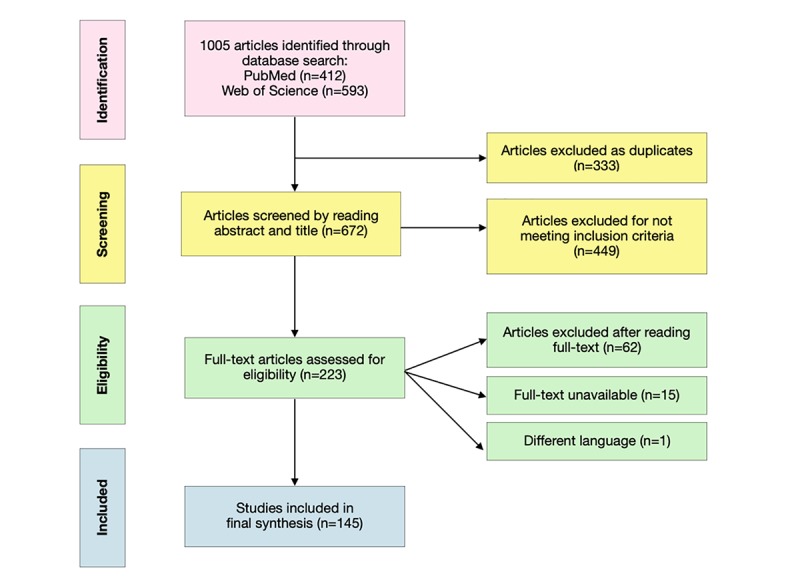
Flowchart of literature search and screening.
Data Synthesis
In the analysis, a descriptive numerical summary is provided to present the following information: author/s, publication year, study type, geographic region of the study, the first author’s affiliation country, digital health technology domain, interventions of digital technology, and the main results. The geographic origin of the papers was categorized according to the World Bank regional grouping, which includes East Asia and Pacific, Latin America and Caribbean, North America, Sub-Saharan Africa, Europe and Central Asia, Middle East and North Africa, and South Asia [151]. Papers that did not focus on a specific region or country or studies on more than one region were classified as global. The extracted data were extrapolated into a data charting form in a Microsoft Excel file.
Results
Main Results
In the assessment by function, 105 studies identified the primary use of digital technology as TB patient care. This included TB diagnosis, treatment, and care support (Table 1). A total of 30 studies used digital technology in surveillance and monitoring, including electronic medical records and information systems; 7 focused on program management, and 3 focused on e-learning.
Table 1.
Four types of interventions.
| Intervention type and digital health technology | References | ||
| Patient care |
|
||
|
|
GeneXpert | [1-11] | |
|
|
Chest x-ray | [12-22] | |
|
|
Polymerase chain reaction | [23-31] | |
|
|
Video directly observed therapy | [32-49] | |
|
|
text messages | [50-60] | |
|
|
Mobile phone apps | [61-70] | |
|
|
Artificial intelligence | [71-73] | |
|
|
Novel technologies | [74-102] | |
| Surveillance and monitoring |
|
||
|
|
Health information system webpages (eg, OUT-TB, e-TB, ETR.Net, TB portals, and TB Genova network) | [103-133] | |
|
|
Program management | [134-140] | |
| Electronic learning |
|
||
|
|
Digital platform for chest x-ray training | [141] | |
|
|
Educational video | [142] | |
|
|
Mobile app | [143] | |
Using the other WHO classification of the use of digital technology in health by targeted user, of the 145 studies, 107 (73.8%) studies focused on health care providers, 20 (13.8%) studies targeted clients, 17 (11.7%) studies data services, and 1 (0.7%) study the health system or resource managers. The vast majority of scientific literature targeted health care providers compared with patients or general health system managers.
Using the other WHO classification of the use of digital technology in health by targeted user, of the 145 studies, 107 (73.8%) studies focused on health care providers, 20 (13.8%) studies targeted clients, 17 (11.7%) studies data services, and 1 (0.7%) study the health system or resource managers. The vast majority of scientific literature targeted health care providers compared with patients or general health system managers.
First Authors’ Affiliation
In this study, the first author’s affiliation is defined by the country of the author’s academic institution rather than the nationality of the author. The first author’s affiliation included both high- and low-income countries. In terms of frequency of publications, the following countries were identified: the United States, China, India, the United Kingdom), Canada, South Africa, Switzerland, South Korea, and Italy. Figure 2 shows that the United States was the country with the highest number of publications on this topic. Out of the 30 studies published in the United States, 11 had a geographic focus on regions outside of North America, including Sub-Saharan Africa, Latin America, and Caribbean regions. China and India were the second and third countries in terms of the number of publications when the first author’s affiliation was used as a criterion. Considering the burden of disease, it is not unusual to see the growing interests of China and India in the use of digital health technology in TB.
Figure 2.
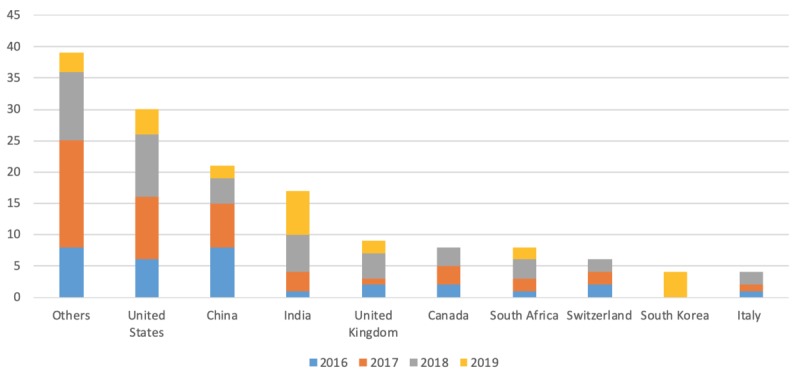
Number of publications by first author’s affiliation.
Types of Digital Technology
Of the 105 studies on patient care, 62 analyzed the use of digital technology in diagnosis and 43 its use in treatment adherence. Among the 62 studies on digital technology for diagnosis, 16 were on GeneXpert MTB/RIF, which is today considered the test of choice for early and rapid diagnosis of TB [10,11]. The other studies were on digital chest x-ray (CXR) with the computer-aided detection of TB (n=14), digital real-time polymerase chain reaction technologies (n=11), artificial intelligence (n=3), deep learning or machine learning (n=2), a dot-blot system (n=1), computational modeling (n=1), and mobile 3D-printed induration (n=1), among others (n=13).
A total of 39 studies undertook a mobile health (mHealth) approach to analyze the use of mobile phones in TB treatment adherence. This approach included VOT (n=19), SMS (n=9), mobile apps (n=6), voice calls (n=2), mobile phone 3D-printed induration (n=1), and framework studies on mHealth for TB treatment (n=2). In the 19 studies on VOT, a cost and impact analysis on VOT showed that VOT could save up to 58% of costs, in addition to alleviating inconvenience and cost when visiting the treatment center [12,13]. VOT demonstrated a promising adherence rate, which is practical and enables patients in remote areas to have easy access to treatment. The challenges of VOT lie in patient confidentiality, the management of adverse drug reactions, and technical issues [14]. Patients may be unable to read SMS messages, especially women, because of the high prevalence of illiteracy [15].
A total of 30 studies on surveillance and monitoring revealed the absence of standardized health information systems to collect data on the care and control of TB [16,17]. Digital records demonstrated fewer data quality issues than paper-based records [18] and improved patient management [19]. However, newly recruited health care workers had low confidence to use digital health technologies. To enhance national or global TB surveillance and monitoring systems, some studies (n=14/30) tested Web-based platforms, the connectivity of diagnostic technologies, and standardized health information systems. Existing systems include OUT-TB Web, e-TB Manager, ETR.Net, TB Portals, and TB Genova network. In addition, artificial neural networks, big data analysis, Web-based surveys, and mathematical modeling (10/30) were used to predict the flow of TB patients. The remaining 2 studies examined TB drug susceptibility testing based on next-generation sequencing and whole-genome sequencing.
A total of 7 studies addressed the intervention of digital technology in program management. Three studies looked into the e-learning aspect of digital technology, with 1 examining a mobile phone app [20], another a Web-based training course on CXR [21], and the third a multilingual educational video on latent TB [22]. In conclusion, Figure 3 summarizes the major types of digital technology for TB that are discussed in this scoping review.
Figure 3.
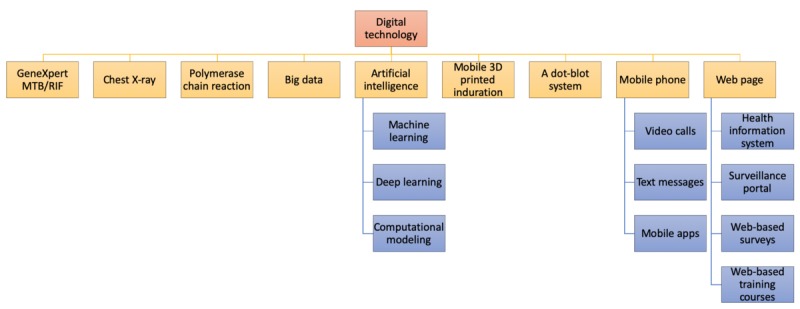
Types of digital technology. MTB: mycobacterium tuberculosis; RIF: rifampicin.
Discussion
The findings of this scoping review suggest that the overall research efforts on the use of digital health technologies in TB care and control between January 2016 and March 2019 were focused disproportionately on patient care (105/145, 72.4%) and surveillance (30/145, 20.7%), and were aimed essentially at benefiting health care providers (107/145, 73.8% of all studies).
Only 1 study called for increased patient support focus after reviewing 24 TB-related apps in use [9]. This study argued that apps for TB patient care had minimal functionality, primarily targeted frontline health care workers, and focused on data collection. Few apps were developed for use by patients, and none were designed to support TB patients’ involvement in and management of their care. A total of 3 studies out of 145 integrated perspectives of both health care providers and patients into their analysis. These findings show a clear trend in the present literature on digital health technology for TB. It centers on feedback by health professionals, rather than TB patients, in utilizing digital health technology.
Using the TB-specific categorization by function, despite recognition of its importance, only 7 studies were devoted to program management and only 3 to e-learning. One of the 7 studies on program management developed a general framework on all priority products and concepts of digital health technologies in TB [23]. Some policy reports suggested scaling up investment in digital health to enhance TB control [152]. In the assessment of the frequency of research based on the TB-specific categorization of themes, 1 reason for the scarcity of studies on programmatic challenges could be the inclusion of TB drug management in studies outside of the TB field. This scoping review did not count studies without any keywords referring to TB; therefore, other studies, which may have referred to TB program management but without the keyword TB could have been overlooked. Similarly, the inclusion of gray literature, such as project reports of executive groups, could have increased the percentage of studies targeting health system managers and data services. However, this was outside the aims of this scoping review.
Another reason could be the nature of academic research papers. Standard study design in health science journals prefers interventions that are comparatively discrete and well standardized. This is the reason why most researchers prefer to focus on straightforward outcomes of interventions and on strict methodological approaches. In fact, specific diagnostic tools and VOT were the subject of a substantial number of studies, and tools such as GeneXpert MTB/RIF, VOT, and SMS were more frequently assessed under randomized controlled trial (RCT) conditions. Complex interventions such as Web-based platforms, mobile apps, e-learning, or health information systems, which go beyond testing of an individual tool, are less likely to be studied through RCTs and therefore, to be the preferred theme for a researcher.
Regarding the categorization of digital health research efforts through the lens of targeted users, a disproportionate 73.8% of studies (107/145) focused on health care providers. Some other areas, for instance health systems or resource managers, are currently not well covered by research efforts. More importantly, very few studies have focused on clients revealing the need to further explore the use of digital technology in TB care from a different and more person-centered perspective to truly identify the benefits that these tools can bring to clients.
Multifunctionality of Digital Technology
The main results categorized the existing literature by 2 types of taxonomy. Each DHI was classified into 1 of only 4 options for the sake of simplifying the analysis. However, the possibility of overlap in technological function must be considered. In other words, some digital technologies no longer have a single function or are targeting a single user but instead have multifunctionality and can target different types of users.
For instance, for the purpose of analysis, GeneXpert MTB/RIF was considered under the category of patient care. However, at the same time, it could serve as a tool for the surveillance of drug resistance. In the past, it was impossible to connect microscopy to a database. Since 2010, however, GeneXpert has enabled the synchronization of all data into the database once the test results are available. Therefore, both health professionals and data services can obtain benefits from the use of a rapid diagnostic technology. Similarly, TB surveillance tools can be used to manage the health system. OUT-TB Web provides surveillance services such as customizable heat maps for visualizing TB and drug-resistance cases. In addition, it serves program management functions such as the allocation of financial, technical, and human resources [24]. Furthermore, reports from the ETR.Net surveillance platform were used to inform and guide resource allocation at the facilities [25].
Another good example of double targets is that of VOT. In this study, VOT was categorized depending on the primary function of the technology. It was considered an intervention for health care providers if the primary purpose was consultations between remote clients and health care providers (WHO category 2.4.1). If VOT was to ensure treatment adherence by transmitting targeted alerts and reminders, then it was considered to be a tool targeting clients (WHO category 1.1.3). The difference in the targeted user clearly shows various perspectives in understanding the functions of a single technology.
Limitations and Direction for Further Research
This review has some limitations. One is related to the first author’s affiliation. To capture which countries invested the most in research in this field, we simplified the analysis by equating the first author’s affiliation with a country. However, the first author’s affiliation represents neither the nationality of the author nor the affiliation of the other authors if there are more. Another limitation relates to the search strategy that could be further refined. The literature search only included 2 major databases. Some articles and gray literature presented exclusively in other databases or websites could have been missed, although we suspect that they may not have had a significant impact on the findings.
Future research should fill the gaps that we unveiled, particularly in the areas of data services, health system management, and client focus. Potential research topics that have not been well investigated to date include sustainable financing of digital health technologies used for TB, surveillance of TB diagnosis equipment stocks, TB drug forecasting, and reporting on counterfeit or substandard drugs (WHO classification 3.2) [5]. In addition, it seems worth exploring the role of other e-learning tools such as the application of game techniques to education, augmented reality, and 3D learning environments.
Furthermore, not all findings in a high- or a low-resource country may apply to another country in a different situation in terms of epidemiological trends and patient populations. Thus, it is necessary to focus further on high-burden countries where digital technology has not yet been studied properly; these may include WHO-identified high-burden countries such as Angola, Bangladesh, DR Congo, Ethiopia, Kenya, Myanmar, Nigeria, and Vietnam.
Added Value of This Study
The strengths of this review consist of the high number of studies included and the breadth of the analysis based on 2 different taxonomies of functions and targets. It summarizes the range of research activity on the use of digital technology to enhance TB control between January 2016 and March 2019. The findings highlight a need to expand knowledge and research in health system management and data services, with a view on targeting clients rather than mainly health care workers. A discussion on the multifunctionality of digital technology also provides added value in regard to different perspectives to examine various functions of a single technology.
Conclusions
Our findings suggest that the major hubs of research on digital health for TB include the United States, as well as China and India. It is presumably because of available resources and high disease prevalence, respectively. An interesting observation derived from the study is the multifunctionality of digital technology. Unlike single-function tools in the past, an increasing number of digital health technologies carry multiple functions. Out of 145 studies, 105 (72.4%) addressed patient care as the main focus of digital health technology, and 30 (20.7%) targeted surveillance. Program management and e-learning were 2 underrepresented topics of research. Looking at the findings from a target perspective, compared with studies targeting health care providers, studies on health system managers and data services were limited as were, of particular concern, those addressing clients. Therefore, more research and development are necessary to arrive at a broader understanding of the full potential of digital technology in the TB field. We suggest that future research should focus on program management, e-learning, and surveillance, with enhanced focus on the clients, the ultimate beneficiaries, to enhance the effectiveness of care, prevention, and control of TB and contribute to its elimination.
Acknowledgments
The study was conducted as part of YL’s Master’s thesis in Global Health at the University of Geneva.
Abbreviations
- CXR
chest x-ray
- DHI
digital health intervention
- eDOT
electronic directly observed therapy
- e-learning
electronic learning
- mHealth
mobile health
- MTB
mycobacterium tuberculosis
- RCT
randomized controlled trial
- RIF
rifampicin
- TB
tuberculosis
- VOT
video-observed therapy
- WHO
World Health Organization
Appendix
Search strategy syntax for databases PubMed and Web of Science.
Footnotes
Authors' Contributions: MR contributed to analysis, review, and editing throughout the writing process, and AF provided guidance and approval of the manuscript for publication.
Conflicts of Interest: None declared.
References
- 1.World Health Organization . Global Tuberculosis Report 2019. Geneva: World Health Organization; 2019. [Google Scholar]
- 2.Benatar SR, Upshur R. Tuberculosis and poverty: what could (and should) be done? Int J Tuberc Lung Dis. 2010 Oct;14(10):1215–21. [PubMed] [Google Scholar]
- 3.World Health Organization. 2015. [2019-12-16]. Digital Health for the End TB Strategy - An Agenda for Action https://www.who.int/tb/publications/digitalhealth-TB-agenda/en/
- 4.World Health Organization. 2015. [2019-12-16]. Digital Health in the TB Response https://www.who.int/tb/publications/ehealth_TB.pdf?ua=1.
- 5.Essential components of a tuberculosis prevention and control program. Recommendations of the Advisory Council for the Elimination of Tuberculosis. MMWR Recomm Rep. 1995 Sep 8;44(RR-11):1–16. http://www.cdc.gov/mmwr/preview/mmwrhtml/00038823.htm. [PubMed] [Google Scholar]
- 6.Gliddon HD, Shorten RJ, Hayward AC, Story A. A sputum sample processing method for community and mobile tuberculosis diagnosis using the Xpert MTB/RIF assay. ERJ Open Res. 2019 Feb;5(1):pii: 00165-2018. doi: 10.1183/23120541.00165-2018. http://europepmc.org/abstract/MED/30723725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.World Health Organization. 2018. [2019-12-16]. Classification of Digital Health Interventions v1.0 https://apps.who.int/iris/bitstream/handle/10665/260480/WHO-RHR-18.06-eng.pdf?sequence=1.
- 8.Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi: 10.1080/1364557032000119616. [DOI] [Google Scholar]
- 9.Iribarren S, Schnall R. Call for increased patient support focus: review and evaluation of mobile apps for tuberculosis prevention and treatment. Stud Health Technol Inform. 2016;225:936–7. [PMC free article] [PubMed] [Google Scholar]
- 10.Calligaro GL, Zijenah LS, Peter JG, Theron G, Buser V, McNerney R, Bara W, Bandason T, Govender U, Tomasicchio M, Smith L, Mayosi BM, Dheda K. Effect of new tuberculosis diagnostic technologies on community-based intensified case finding: a multicentre randomised controlled trial. Lancet Infect Dis. 2017 Apr;17(4):441–50. doi: 10.1016/S1473-3099(16)30384-X. [DOI] [PubMed] [Google Scholar]
- 11.Mazzola E, Arosio M, Nava A, Fanti D, Gesu G, Farina C. Performance of real-time PCR Xpert MTB/RIF in diagnosing extrapulmonary tuberculosis. Infez Med. 2016 Dec 1;24(4):304–9. https://www.infezmed.it/index.php/article?Anno=2016&numero=4&ArticoloDaVisualizzare=Vol_24_4_2016_304. [PubMed] [Google Scholar]
- 12.Nsengiyumva NP, Mappin-Kasirer B, Oxlade O, Bastos M, Trajman A, Falzon D, Schwartzman K. Evaluating the potential costs and impact of digital health technologies for tuberculosis treatment support. Eur Respir J. 2018 Nov;52(5):pii: 1801363. doi: 10.1183/13993003.01363-2018. http://erj.ersjournals.com:4040/cgi/pmidlookup?view=long&pmid=30166325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Story A, Garfein RS, Hayward A, Rusovich V, Dadu A, Soltan V, Oprunenco A, Collins K, Sarin R, Quraishi S, Sharma M, Migliori GB, Varadarajan M, Falzon D. Monitoring therapy compliance of tuberculosis patients by using video-enabled electronic devices. Emerg Infect Dis. 2016 Mar;22(3):538–40. doi: 10.3201/eid2203.151620. doi: 10.3201/eid2203.151620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chuck C, Robinson E, Macaraig M, Alexander M, Burzynski J. Enhancing management of tuberculosis treatment with video directly observed therapy in New York City. Int J Tuberc Lung Dis. 2016 May;20(5):588–93. doi: 10.5588/ijtld.15.0738. [DOI] [PubMed] [Google Scholar]
- 15.Basu S. mHealth to enhance TB referrals: challenge in scaling up. Public Health Action. 2018 Mar 21;8(1):29. doi: 10.5588/pha.17.0108. http://europepmc.org/abstract/MED/29581942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mukasa E, Kimaro H, Kiwanuka A, Igira F. Challenges and strategies for standardizing information systems for integrated TB/HIV services in Tanzania: a case study of Kinondoni municipality. Electron J Inf Syst Dev Ctries. 2017;79(1):1–11. doi: 10.1002/j.1681-4835.2017.tb00581.x. [DOI] [Google Scholar]
- 17.Yassi A, Adu PA, Nophale L, Zungu M. Learning from a cluster randomized controlled trial to improve healthcare workers' access to prevention and care for tuberculosis and HIV in Free State, South Africa: the pivotal role of information systems. Glob Health Action. 2016;9:30528. doi: 10.3402/gha.v9.30528. http://europepmc.org/abstract/MED/27341793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ali S, Naureen F, Noor A, Boulos MK, Aamir J, Ishaq M, Anjum N, Ainsworth J, Rashid A, Majidulla A, Fatima I. Data quality: a negotiator between paper-based and digital records in Pakistan’s TB control program. Data. 2018 Jul 19;3(3):27–73. doi: 10.3390/data3030027. [DOI] [Google Scholar]
- 19.Tweya H, Feldacker C, Gadabu OJ, Ng'ambi W, Mumba SL, Phiri D, Kamvazina L, Mwakilama S, Kanyerere H, Keiser O, Mwafilaso J, Kamba C, Egger M, Jahn A, Simwaka B, Phiri S. Developing a point-of-care electronic medical record system for TB/HIV co-infected patients: experiences from Lighthouse Trust, Lilongwe, Malawi. BMC Res Notes. 2016 Mar 5;9:146. doi: 10.1186/s13104-016-1943-4. https://bmcresnotes.biomedcentral.com/articles/10.1186/s13104-016-1943-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Pande T, Cohen C, Pai M, Ahmad Khan F. Computer-aided detection of pulmonary tuberculosis on digital chest radiographs: a systematic review. Int J Tuberc Lung Dis. 2016 Sep;20(9):1226–30. doi: 10.5588/ijtld.15.0926. [DOI] [PubMed] [Google Scholar]
- 21.Semakula-Katende NS, Andronikou S, Lucas S. Digital platform for improving non-radiologists' and radiologists' interpretation of chest radiographs for suspected tuberculosis - a method for supporting task-shifting in developing countries. Pediatr Radiol. 2016 Sep;46(10):1384–91. doi: 10.1007/s00247-016-3630-y. [DOI] [PubMed] [Google Scholar]
- 22.Gao J, Cook VJ, Mayhew M. Preventing tuberculosis in a low incidence setting: evaluation of a multi-lingual, online, educational video on latent tuberculosis. J Immigr Minor Health. 2018 Jun;20(3):687–96. doi: 10.1007/s10903-017-0601-9. [DOI] [PubMed] [Google Scholar]
- 23.Falzon D, Raviglione M. The Internet of Things to come: digital technologies and the End TB Strategy. BMJ Glob Health. 2016;1(2):e000038. doi: 10.1136/bmjgh-2016-000038. http://europepmc.org/abstract/MED/28588935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Guthrie JL, Alexander DC, Marchand-Austin A, Lam K, Whelan M, Lee B, Furness C, Rea E, Stuart R, Lechner J, Varia M, McLean J, Jamieson FB. Technology and tuberculosis control: the OUT-TB Web experience. J Am Med Inform Assoc. 2017 Apr 1;24(e1):e136–42. doi: 10.1093/jamia/ocw130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Mlotshwa M, Smit S, Williams S, Reddy C, Medina-Marino A. Evaluating the electronic tuberculosis register surveillance system in Eden District, Western Cape, South Africa, 2015. Glob Health Action. 2017;10(1):1360560. doi: 10.1080/16549716.2017.1360560. http://europepmc.org/abstract/MED/28849725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bassett IV, Forman LS, Govere S, Thulare H, Frank SC, Mhlongo B, Losina E. Test and Treat TB: a pilot trial of GeneXpert MTB/RIF screening on a mobile HIV testing unit in South Africa. BMC Infect Dis. 2019 Feb 4;19(1):110. doi: 10.1186/s12879-019-3738-4. https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-019-3738-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Zhang A, Li F, Liu X, Xia L, Lu S. [Application of Gene Xpert Mycobacterium tuberculosis DNA and resistance to rifampicin assay in the rapid detection of tuberculosis in children] Zhonghua Er Ke Za Zhi. 2016 May;54(5):370–4. doi: 10.3760/cma.j.issn.0578-1310.2016.05.012. [DOI] [PubMed] [Google Scholar]
- 28.Jin Y, Shi S, Zheng Q, Shen J, Ying X, Wang Y. [Application value of Xpert MTB/RIF in diagnosis of spinal tuberculosis and detection of rifampin resistance] Zhongguo Gu Shang. 2017 Sep 25;30(9):787–91. doi: 10.3969/j.issn.1003-0034.2017.09.002. [DOI] [PubMed] [Google Scholar]
- 29.Stevens W, Scott L, Noble L, Gous N, Dheda K. Impact of the GeneXpert MTB/RIF Technology on Tuberculosis Control. Microbiol Spectr. 2017 Jan;5(1) doi: 10.1128/microbiolspec.TBTB2-0040-2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Rendell N, Bekhbat S, Ganbaatar G, Dorjravdan M, Pai M, Dobler C. Implementation of the Xpert MTB/RIF assay for tuberculosis in Mongolia: a qualitative exploration of barriers and enablers. PeerJ. 2017;5:e3567. doi: 10.7717/peerj.3567. doi: 10.7717/peerj.3567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Wattal C, Raveendran R. Newer diagnostic tests and their application in pediatric TB. Indian J Pediatr. 2019 May;86(5):441–7. doi: 10.1007/s12098-018-2811-0. [DOI] [PubMed] [Google Scholar]
- 32.Khumsri J, Hiransuthikul N, Hanvoravongchai P, Chuchottaworn C. Effectiveness of tuberculosis screening technology in the initiation of correct diagnosis of pulmonary tuberculosis at a tertiary care hospital in Thailand: comparative analysis of Xpert MTB/RIF versus sputum AFB smear. Asia Pac J Public Health. 2018 Sep;30(6):542–50. doi: 10.1177/1010539518800336. [DOI] [PubMed] [Google Scholar]
- 33.Morishita F, Garfin AM, Lew W, Oh KH, Yadav R, Reston JC, Infante LL, Acala MR, Palanca DL, Kim HJ, Nishikiori N. Bringing state-of-the-art diagnostics to vulnerable populations: the use of a mobile screening unit in active case finding for tuberculosis in Palawan, the Philippines. PLoS One. 2017;12(2):e0171310. doi: 10.1371/journal.pone.0171310. http://dx.plos.org/10.1371/journal.pone.0171310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Datta B, Hazarika A, Shewade HD, Ayyagari K, Kumar AM. Digital chest X-ray through a mobile van: public private partnership to detect sputum negative pulmonary TB. BMC Res Notes. 2017 Feb 14;10(1):96. doi: 10.1186/s13104-017-2420-4. https://bmcresnotes.biomedcentral.com/articles/10.1186/s13104-017-2420-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Muyoyeta M, Kasese NC, Milimo D, Mushanga I, Ndhlovu M, Kapata N, Moyo-Chilufya M, Ayles H. Digital CXR with computer aided diagnosis versus symptom screen to define presumptive tuberculosis among household contacts and impact on tuberculosis diagnosis. BMC Infect Dis. 2017 Apr 24;17(1):301. doi: 10.1186/s12879-017-2388-7. https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-017-2388-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Datta B, Prakash AK, Ford D, Tanwar PK, Goyal P, Chatterjee P, Vipin S, Jaiswal A, Trehan N, Ayyagiri K. Comparison of clinical and cost-effectiveness of two strategies using mobile digital x-ray to detect pulmonary tuberculosis in rural India. BMC Public Health. 2019 Jan 22;19(1):99. doi: 10.1186/s12889-019-6421-1. https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-019-6421-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Melendez J, Sánchez CI, Philipsen RH, Maduskar P, Dawson R, Theron G, Dheda K, van Ginneken B. An automated tuberculosis screening strategy combining X-ray-based computer-aided detection and clinical information. Sci Rep. 2016 Apr 29;6:25265. doi: 10.1038/srep25265. doi: 10.1038/srep25265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Khan FA, Pande T, Tessema B, Song R, Benedetti A, Pai M, Lönnroth K, Denkinger CM. Computer-aided reading of tuberculosis chest radiography: moving the research agenda forward to inform policy. Eur Respir J. 2017 Jul;50(1):pii: 1700953. doi: 10.1183/13993003.00953-2017. http://erj.ersjournals.com/cgi/pmidlookup?view=long&pmid=28705949. [DOI] [PubMed] [Google Scholar]
- 39.Zaidi SM, Habib SS, van Ginneken B, Ferrand RA, Creswell J, Khowaja S, Khan A. Evaluation of the diagnostic accuracy of Computer-Aided Detection of tuberculosis on Chest radiography among private sector patients in Pakistan. Sci Rep. 2018 Aug 17;8(1):12339. doi: 10.1038/s41598-018-30810-1. doi: 10.1038/s41598-018-30810-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Koesoemadinata RC, Kranzer K, Livia R, Susilawati N, Annisa J, Soetedjo NN, Ruslami R, Philipsen R, van Ginneken B, Soetikno RD, van Crevel R, Alisjahbana B, Hill PC. Computer-assisted chest radiography reading for tuberculosis screening in people living with diabetes mellitus. Int J Tuberc Lung Dis. 2018 Sep 1;22(9):1088–94. doi: 10.5588/ijtld.17.0827. [DOI] [PubMed] [Google Scholar]
- 41.Hooda R, Mittal A, Sofat S. Tuberculosis detection from chest radiographs: a comprehensive survey on computer-aided diagnosis techniques. Curr Med Imaging Rev. 2018;14(4):506–20. doi: 10.2174/1573405613666171115154119. [DOI] [Google Scholar]
- 42.Becker AS, Blüthgen C, Phi VD, Sekaggya-Wiltshire C, Castelnuovo B, Kambugu A, Fehr J, Frauenfelder T. Detection of tuberculosis patterns in digital photographs of chest X-ray images using Deep Learning: feasibility study. Int J Tuberc Lung Dis. 2018 Mar 1;22(3):328–35. doi: 10.5588/ijtld.17.0520. [DOI] [PubMed] [Google Scholar]
- 43.Sweetlin JD, Nehemiah HK, Kannan A. Computer aided diagnosis of drug sensitive pulmonary tuberculosis with cavities, consolidations and nodular manifestations on lung CT images. Int J Bioinspired Comput. 2019;13(2):71–85. doi: 10.1504/ijbic.2019.098405. [DOI] [Google Scholar]
- 44.Yang J, Han X, Liu A, Bai X, Xu C, Bao F, Feng S, Tao L, Ma M, Peng Y. Use of digital droplet PCR to detect DNA in whole blood-derived DNA samples from patients with pulmonary and extrapulmonary tuberculosis. Front Cell Infect Microbiol. 2017;7:369. doi: 10.3389/fcimb.2017.00369. doi: 10.3389/fcimb.2017.00369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Devonshire AS, O'Sullivan DM, Honeyborne I, Jones G, Karczmarczyk M, Pavšič J, Gutteridge A, Milavec M, Mendoza P, Schimmel H, van Heuverswyn F, Gorton R, Cirillo DM, Borroni E, Harris K, Barnard M, Heydenrych A, Ndusilo N, Wallis CL, Pillay K, Barry T, Reddington K, Richter E, Mozioğlu E, Akyürek S, Yalçınkaya B, Akgoz M, Žel J, Foy CA, McHugh TD, Huggett JF. The use of digital PCR to improve the application of quantitative molecular diagnostic methods for tuberculosis. BMC Infect Dis. 2016 Aug 3;16:366. doi: 10.1186/s12879-016-1696-7. https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-016-1696-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Luo J, Luo M, Li J, Yu J, Yang H, Yi X, Chen Y, Wei H. Rapid direct drug susceptibility testing of Mycobacterium tuberculosis based on culture droplet digital polymerase chain reaction. Int J Tuberc Lung Dis. 2019 Feb 1;23(2):219–25. doi: 10.5588/ijtld.18.0182. [DOI] [PubMed] [Google Scholar]
- 47.Ushio R, Yamamoto M, Nakashima K, Watanabe H, Nagai K, Shibata Y, Tashiro K, Tsukahara T, Nagakura H, Horita N, Sato T, Shinkai M, Kudo M, Ueda A, Kaneko T. Digital PCR assay detection of circulating Mycobacterium tuberculosis DNA in pulmonary tuberculosis patient plasma. Tuberculosis (Edinb) 2016 Jul;99:47–53. doi: 10.1016/j.tube.2016.04.004. [DOI] [PubMed] [Google Scholar]
- 48.Sadr S, Darban-Sarokhalil D, Irajian GR, Fooladi AA, Moradi J, Feizabadi MM. An evaluation study on phenotypical methods and real-time PCR for detection of Mycobacterium tuberculosis in sputa of two health centers in Iran. Iran J Microbiol. 2017 Feb;9(1):38–42. http://europepmc.org/abstract/MED/28775822. [PMC free article] [PubMed] [Google Scholar]
- 49.Meng Q, Liu ZW. [The development and application of digital PCR used in Mycobacterium tuberculosis detection] Zhonghua Jie He He Hu Xi Za Zhi. 2017 Dec 12;40(12):946–7. doi: 10.3760/cma.j.issn.1001-0939.2017.12.017. [DOI] [PubMed] [Google Scholar]
- 50.Raveendran R, Wattal C. Utility of multiplex real-time PCR in the diagnosis of extrapulmonary tuberculosis. Braz J Infect Dis. 2016;20(3):235–41. doi: 10.1016/j.bjid.2016.01.006. https://linkinghub.elsevier.com/retrieve/pii/S1413-8670(16)30039-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Negi SS, Singh P, Chandrakar S, Gaikwad U, Das P, Bhargava A. Diagnostic evaluation of multiplex real time PCR, GeneXpert MTB/RIF assay and conventional methods in extrapulmonary tuberculosis. J Clin Diagn Res. 2019 Jan;13(1):12–16. doi: 10.7860/JCDR/2019/37569.12485. https://www.jcdr.net/articles/PDF/12485/37569_CE[Ra1]_F(SL)_PF1(AGAK)_PFA(AK)_PB(AG_SHU)_PN(SL).pdf. [DOI] [Google Scholar]
- 52.Gallo JF, Pinhata JM, Chimara E, Gonçalves MG, Fukasawa LO, Oliveira RS. Performance of an in-house real-time polymerase chain reaction for identification of Mycobacterium tuberculosis isolates in laboratory routine diagnosis from a high burden setting. Mem Inst Oswaldo Cruz. 2016 Sep;111(9):545–50. doi: 10.1590/0074-02760160048. http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0074-02762016005018101&lng=en&nrm=iso&tlng=en. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Babafemi EO, Cherian BP, Banting L, Mills GA, Ngianga K. Effectiveness of real-time polymerase chain reaction assay for the detection of Mycobacterium tuberculosis in pathological samples: a systematic review and meta-analysis. Syst Rev. 2017 Oct 25;6(1):215. doi: 10.1186/s13643-017-0608-2. https://systematicreviewsjournal.biomedcentral.com/articles/10.1186/s13643-017-0608-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Lv Z, Zhang M, Zhang H, Lu X. Utility of real-time quantitative polymerase chain reaction in detecting Mycobacterium tuberculosis. Biomed Res Int. 2017;2017:1058579. doi: 10.1155/2017/1058579. doi: 10.1155/2017/1058579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Olano-Soler H, Thomas D, Joglar O, Rios K, Torres-Rodríguez M, Duran-Guzman G, Chorba T. Notes from the field: use of asynchronous video directly observed therapy for treatment of tuberculosis and latent tuberculosis infection in a long-term-care facility - Puerto Rico, 2016-2017. MMWR Morb Mortal Wkly Rep. 2017 Dec 22;66(50):1386–7. doi: 10.15585/mmwr.mm6650a5. doi: 10.15585/mmwr.mm6650a5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Holzschuh EL, Province S, Johnson K, Walls C, Shemwell C, Martin G, Showalter A, Dunlay J, Conyers A, Griffin P, Tausz N. Use of video directly observed therapy for treatment of latent tuberculosis infection - Johnson County, Kansas, 2015. MMWR Morb Mortal Wkly Rep. 2017 Apr 14;66(14):387–9. doi: 10.15585/mmwr.mm6614a3. doi: 10.15585/mmwr.mm6614a3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Nguyen TA, Pham MT, Nguyen TL, Nguyen VN, Pham DC, Nguyen BH, Fox GJ. Video directly observed therapy to support adherence with treatment for tuberculosis in Vietnam: a prospective cohort study. Int J Infect Dis. 2017 Dec;65:85–9. doi: 10.1016/j.ijid.2017.09.029. https://linkinghub.elsevier.com/retrieve/pii/S1201-9712(17)30256-4. [DOI] [PubMed] [Google Scholar]
- 58.Sinkou H, Hurevich H, Rusovich V, Zhylevich L, Falzon D, de Colombani P, Dadu A, Dara M, Story A, Skrahina A. Video-observed treatment for tuberculosis patients in Belarus: findings from the first programmatic experience. Eur Respir J. 2017 Mar;49(3):pii: 1602049. doi: 10.1183/13993003.02049-2016. http://erj.ersjournals.com/cgi/pmidlookup?view=long&pmid=28331042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Holzman SB, Zenilman A, Shah M. Advancing patient-centered care in tuberculosis management: a mixed-methods appraisal of video directly observed therapy. Open Forum Infect Dis. 2018 Apr;5(4):ofy046. doi: 10.1093/ofid/ofy046. http://europepmc.org/abstract/MED/29732378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Garfein RS, Liu L, Cuevas-Mota J, Collins K, Muñoz F, Catanzaro DG, Moser K, Higashi J, Al-Samarrai T, Kriner P, Vaishampayan J, Cepeda J, Bulterys MA, Martin NK, Rios P, Raab F. Tuberculosis treatment monitoring by video directly observed therapy in 5 health districts, California, USA. Emerg Infect Dis. 2018 Oct;24(10):1806–15. doi: 10.3201/eid2410.180459. doi: 10.3201/eid2410.180459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Lam CK, McGinnis Pilote K, Haque A, Burzynski J, Chuck C, Macaraig M. Using video technology to increase treatment completion for patients with latent tuberculosis infection on 3-month isoniazid and rifapentine: an implementation study. J Med Internet Res. 2018 Nov 20;20(11):e287. doi: 10.2196/jmir.9825. https://www.jmir.org/2018/11/e287/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Ingram D. Video directly observed therapy: enhancing care for patients with active tuberculosis. Nursing. 2018 May;48(5):64–6. doi: 10.1097/01.NURSE.0000531912.91585.85. [DOI] [PubMed] [Google Scholar]
- 63.Kumar AA, de Costa A, Das A, Srinivasa G, D'Souza G, Rodrigues R. Mobile health for tuberculosis management in South India: is video-based directly observed treatment an acceptable alternative? JMIR Mhealth Uhealth. 2019 Apr 3;7(4):e11687. doi: 10.2196/11687. https://mhealth.jmir.org/2019/4/e11687/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Story A, Aldridge RW, Smith CM, Garber E, Hall J, Ferenando G, Possas L, Hemming S, Wurie F, Luchenski S, Abubakar I, McHugh TD, White PJ, Watson JM, Lipman M, Garfein R, Hayward AC. Smartphone-enabled video-observed versus directly observed treatment for tuberculosis: a multicentre, analyst-blinded, randomised, controlled superiority trial. Lancet. 2019;393(10177):1216–24. doi: 10.1016/s0140-6736(18)32993-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Fraser H, Keshavjee S. Video-observed therapy for tuberculosis: strengthening care. Lancet. 2019 Mar 23;393(10177):1180–1. doi: 10.1016/S0140-6736(19)30293-4. https://linkinghub.elsevier.com/retrieve/pii/S0140-6736(19)30293-4. [DOI] [PubMed] [Google Scholar]
- 66.Thakkar D, Piparva KG, Lakkad SG. A pilot project: 99DOTS information communication technology-based approach for tuberculosis treatment in Rajkot district. Lung India. 2019;36(2):108–11. doi: 10.4103/lungindia.lungindia_86_18. http://www.lungindia.com/article.asp?issn=0970-2113;year=2019;volume=36;issue=2;spage=108;epage=111;aulast=Thakkar. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Macaraig M, Lobato MN, McGinnis Pilote K, Wegener D. A national survey on the use of electronic directly observed therapy for treatment of tuberculosis. J Public Health Manag Pract. 2018;24(6):567–70. doi: 10.1097/PHH.0000000000000627. [DOI] [PubMed] [Google Scholar]
- 68.Buchman T, Cabello C. A new method to directly observe tuberculosis treatment: Skype observed therapy, a patient-centered approach. J Public Health Manag Pract. 2017;23(2):175–7. doi: 10.1097/PHH.0000000000000339. [DOI] [PubMed] [Google Scholar]
- 69.Tseng Y, Chang J, Liu Y, Cheng L, Chen Y, Wu M, Lu C, Yen Y. The role of video-assisted thoracoscopic therapeutic resection for medically failed pulmonary tuberculosis. Medicine (Baltimore) 2016 May;95(18):e3511. doi: 10.1097/MD.0000000000003511. doi: 10.1097/MD.0000000000003511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Hirsch-Moverman Y, Daftary A, Yuengling KA, Saito S, Ntoane M, Frederix K, Maama LB, Howard AA. Using mHealth for HIV/TB treatment support in Lesotho: enhancing Patient-Provider Communication in the START study. J Acquir Immune Defic Syndr. 2017 Jan 1;74(Suppl 1):S37–43. doi: 10.1097/QAI.0000000000001202. http://europepmc.org/abstract/MED/27930610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Babirye D, Farr K, Shete P, Davis JL, Joloba M, Moore D. Feasibility of utilizing short messaging service (SMS) technology to deliver tuberculosis testing results in Uganda. Am J Respir Crit Care Med. 2017;195:A1174. https://www.atsjournals.org/doi/pdf/10.1164/ajrccm-conference.2017.195.1_MeetingAbstracts.A1174. [Google Scholar]
- 72.Hermans S, Elbireer S, Tibakabikoba H, Hoefman B, Manabe Y. Text messaging to decrease tuberculosis treatment attrition in TB-HIV coinfection in Uganda. Patient Prefer Adherence. 2017;11:1479–87. doi: 10.2147/PPA.S135540. doi: 10.2147/PPA.S135540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Meyer AJ, Babirye D, Armstrong-Hough M, Mark D, Ayakaka I, Katamba A, Haberer JE, Davis JL. Text messages sent to household tuberculosis contacts in Kampala, Uganda: process evaluation. JMIR Mhealth Uhealth. 2018 Nov 20;6(11):e10239. doi: 10.2196/10239. https://mhealth.jmir.org/2018/11/e10239/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Johnston JC, van der Kop ML, Smillie K, Ogilvie G, Marra F, Sadatsafavi M, Romanowski K, Budd MA, Hajek J, Cook V, Lester RT. The effect of text messaging on latent tuberculosis treatment adherence: a randomised controlled trial. Eur Respir J. 2018 Feb;51(2):pii: 1701488. doi: 10.1183/13993003.01488-2017. http://erj.ersjournals.com/cgi/pmidlookup?view=long&pmid=29437940. [DOI] [PubMed] [Google Scholar]
- 75.Nhavoto JA, Grönlund Å, Klein GO. Mobile health treatment support intervention for HIV and tuberculosis in Mozambique: Perspectives of patients and healthcare workers. PLoS One. 2017;12(4):e0176051. doi: 10.1371/journal.pone.0176051. http://dx.plos.org/10.1371/journal.pone.0176051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Oren E, Bell ML, Garcia F, Perez-Velez C, Gerald LB. Promoting adherence to treatment for latent TB infection through mobile phone text messaging: study protocol for a pilot randomized controlled trial. Pilot Feasibility Stud. 2017;3:15. doi: 10.1186/s40814-017-0128-9. https://pilotfeasibilitystudies.biomedcentral.com/articles/10.1186/s40814-017-0128-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Boer IM, van den Boogaard J, Ngowi KM, Semvua HH, Kiwango KW, Aarnoutse RE, Nieuwkerk PT, Kibiki GS. Feasibility of real time medication monitoring among HIV infected and TB patients in a resource-limited setting. AIDS Behav. 2016 May;20(5):1097–107. doi: 10.1007/s10461-015-1254-0. [DOI] [PubMed] [Google Scholar]
- 78.Ngwatu BK, Nsengiyumva NP, Oxlade O, Mappin-Kasirer B, Nguyen NL, Jaramillo E, Falzon D, Schwartzman K, Collaborative group on the impact of digital technologies on TB The impact of digital health technologies on tuberculosis treatment: a systematic review. Eur Respir J. 2018 Jan;51(1):pii: 1701596. doi: 10.1183/13993003.01596-2017. http://erj.ersjournals.com/cgi/pmidlookup?view=long&pmid=29326332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Saunders MJ, Wingfield T, Tovar MA, Herlihy N, Rocha C, Zevallos K, Montoya R, Ramos E, Datta S, Evans CA. Mobile phone interventions for tuberculosis should ensure access to mobile phones to enhance equity - a prospective, observational cohort study in Peruvian shantytowns. Trop Med Int Health. 2018 Aug;23(8):850–9. doi: 10.1111/tmi.13087. doi: 10.1111/tmi.13087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Choun K, Achanta S, Naik B, Tripathy JP, Thai S, Lorent N, Khun KE, van Griensven J, Kumar AM, Zachariah R. Using mobile phones to ensure that referred tuberculosis patients reach their treatment facilities: a call that makes a difference. BMC Health Serv Res. 2017 Aug 22;17(1):575. doi: 10.1186/s12913-017-2511-x. https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-017-2511-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Chadha S, Trivedi A, Nagaraja SB, Sagili K. Using mHealth to enhance TB referrals in a tribal district of India. Public Health Action. 2017 Jun 21;7(2):123–6. doi: 10.5588/pha.16.0080. http://europepmc.org/abstract/MED/28695085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Bhargava A, Bhargava M, Pande T, Rao R, Parmar M. N-TB: a mobile-based application to simplify nutritional assessment, counseling and care of patients with tuberculosis in India. Indian J Tuberc. 2019 Jan;66(1):193–6. doi: 10.1016/j.ijtb.2018.10.005. [DOI] [PubMed] [Google Scholar]
- 83.Do D, Garfein RS, Cuevas-Mota J, Collins K, Liu L. Change in patient comfort using mobile phones following the use of an app to monitor tuberculosis treatment adherence: longitudinal study. JMIR Mhealth Uhealth. 2019 Feb 1;7(2):e11638. doi: 10.2196/11638. https://mhealth.jmir.org/2019/2/e11638/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Iribarren SJ, Schnall R, Stone PW, Carballo-Diéguez A. Smartphone applications to support tuberculosis prevention and treatment: review and evaluation. JMIR Mhealth Uhealth. 2016 May 13;4(2):e25. doi: 10.2196/mhealth.5022. https://mhealth.jmir.org/2016/2/e25/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Iribarren S, Demiris G, Lober B, Chirico C. What do patients and experts want in a smartphone-based application to support tuberculosis treatment completion? Stud Health Technol Inform. 2018;250:32. [PubMed] [Google Scholar]
- 86.DiStefano MJ, Schmidt H. mHealth for tuberculosis treatment adherence: a framework to guide ethical planning, implementation, and evaluation. Glob Health Sci Pract. 2016 Jun 20;4(2):211–21. doi: 10.9745/GHSP-D-16-00018. http://www.ghspjournal.org/cgi/pmidlookup?view=long&pmid=27353615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Lee S, Lee Y, Lee S, Islam S, Kim SY. Toward developing a standardized core set of outcome measures in mobile health interventions for tuberculosis management: systematic review. JMIR Mhealth Uhealth. 2019 Feb 19;7(2):e12385. doi: 10.2196/12385. https://mhealth.jmir.org/2019/2/e12385/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Li L, Liu Z, Zhang H, Yue W, Li C, Yi C. A point-of-need enzyme linked aptamer assay for Mycobacterium tuberculosis detection using a smartphone. Sens Actuators B Chem. 2018;254:337–46. doi: 10.1016/j.snb.2017.07.074. [DOI] [Google Scholar]
- 89.Dande P, Samant P. Acquaintance to Artificial Neural Networks and use of artificial intelligence as a diagnostic tool for tuberculosis: A review. Tuberculosis (Edinb) 2018 Jan;108:1–9. doi: 10.1016/j.tube.2017.09.006. [DOI] [PubMed] [Google Scholar]
- 90.Xiong Y, Ba X, Hou A, Zhang K, Chen L, Li T. Automatic detection of mycobacterium tuberculosis using artificial intelligence. J Thorac Dis. 2018 Mar;10(3):1936–40. doi: 10.21037/jtd.2018.01.91. doi: 10.21037/jtd.2018.01.91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Deshpande D, Pasipanodya J, Mpagama S, Bendet P, Srivastava S, Koeuth T, Lee PS, Bhavnani SM, Ambrose PG, Thwaites G, Heysell SK, Gumbo T. Levofloxacin pharmacokinetics/pharmacodynamics, dosing, susceptibility breakpoints, and artificial intelligence in the treatment of multidrug-resistant tuberculosis. Clin Infect Dis. 2018 Nov 28;67(suppl_3):S293–302. doi: 10.1093/cid/ciy611. http://europepmc.org/abstract/MED/30496461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Igarashi Y, Chikamatsu K, Aono A, Yi L, Yamada H, Takaki A, Mitarai S. Laboratory evaluation of the Anyplex II MTB/MDR and MTB/XDR tests based on multiplex real-time PCR and melting-temperature analysis to identify Mycobacterium tuberculosis and drug resistance. Diagn Microbiol Infect Dis. 2017 Dec;89(4):276–81. doi: 10.1016/j.diagmicrobio.2017.08.016. [DOI] [PubMed] [Google Scholar]
- 93.Heo SJ, Kim Y, Yun S, Lim S, Kim J, Nam CM, Park E, Jung I, Yoon J. Deep learning algorithms with demographic information help to detect tuberculosis in chest radiographs in annual workers' health examination data. Int J Environ Res Public Health. 2019 Jan 16;16(2):pii: E250. doi: 10.3390/ijerph16020250. http://www.mdpi.com/resolver?pii=ijerph16020250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Jiao D, Yang H, Yang D, Tian W, Wang H, Ji H. Application of digital tomosynthesis in diagnosing spinal tuberculosis. Clin Imaging. 2016;40(3):461–4. doi: 10.1016/j.clinimag.2015.11.003. [DOI] [PubMed] [Google Scholar]
- 95.Bionghi N, Daftary A, Maharaj B, Msibi Z, Amico KR, Friedland G, Orrell C, Padayatchi N, O'Donnell MR. Pilot evaluation of a second-generation electronic pill box for adherence to Bedaquiline and antiretroviral therapy in drug-resistant TB/HIV co-infected patients in KwaZulu-Natal, South Africa. BMC Infect Dis. 2018 Apr 11;18(1):171. doi: 10.1186/s12879-018-3080-2. https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-018-3080-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Teixeira RC, Rodríguez M, de Romero NJ, Bruins M, Gómez R, Yntema JB, Abente GC, Gerritsen JW, Wiegerinck W, Bejerano DP, Magis-Escurra C. The potential of a portable, point-of-care electronic nose to diagnose tuberculosis. J Infect. 2017 Nov;75(5):441–7. doi: 10.1016/j.jinf.2017.08.003. [DOI] [PubMed] [Google Scholar]
- 97.Hu X, Liao S, Bai H, Wu L, Wang M, Wu Q, Zhou J, Jiao L, Chen X, Zhou Y, Lu X, Ying B, Zhang Z, Li W. Integrating exosomal microRNAs and electronic health data improved tuberculosis diagnosis. EBioMedicine. 2019 Feb;40:564–73. doi: 10.1016/j.ebiom.2019.01.023. https://linkinghub.elsevier.com/retrieve/pii/S2352-3964(19)30028-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Vaccaro F, Signorelli C, Odone A. Information and communication technology to enhance TB control in migrant populations. Eur J Public Health. 2018;28(4) doi: 10.1093/eurpub/cky218.196. https://www.researchgate.net/publication/329112048_Information_and_communication_technology_to_enhance_TB_control_in_migrant_populations. [DOI] [Google Scholar]
- 99.Suwanpimolkul G, Kawkitinarong K, Manosuthi W, Sophonphan J, Gatechompol S, Ohata PJ, Ubolyam S, Iampornsin T, Katerattanakul P, Avihingsanon A, Ruxrungtham K. Utility of urine lipoarabinomannan (LAM) in diagnosing tuberculosis and predicting mortality with and without HIV: prospective TB cohort from the Thailand Big City TB Research Network. Int J Infect Dis. 2017 Jun;59:96–102. doi: 10.1016/j.ijid.2017.04.017. https://linkinghub.elsevier.com/retrieve/pii/S1201-9712(17)30129-7. [DOI] [PubMed] [Google Scholar]
- 100.Mueller-Using S, Feldt T, Sarfo FS, Eberhardt KA. Factors associated with performing tuberculosis screening of HIV-positive patients in Ghana: LASSO-based predictor selection in a large public health data set. BMC Public Health. 2016 Jul 13;16:563. doi: 10.1186/s12889-016-3239-y. https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-016-3239-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Kim HJ, Jang C. Liquid crystal-based aptasensor for the detection of interferon-γ and its application in the diagnosis of tuberculosis using human blood. Sens Actuators B Chem. 2019 Mar;282:574–9. doi: 10.1016/j.snb.2018.11.104. [DOI] [Google Scholar]
- 102.Shabut AM, Tania MH, Lwin KT, Evans BA, Yusof NA, Abu-Hassan KJ, Hossain M. An intelligent mobile-enabled expert system for tuberculosis disease diagnosis in real time. Expert Syst Appl. 2018;114:65–77. doi: 10.1016/j.eswa.2018.07.014. [DOI] [Google Scholar]
- 103.Tang X, Wu S, Xie Y, Song N, Guan Q, Yuan C, Zhou X, Zhang X. Generation and application of ssDNA aptamers against glycolipid antigen ManLAM of Mycobacterium tuberculosis for TB diagnosis. J Infect. 2016 May;72(5):573–86. doi: 10.1016/j.jinf.2016.01.014. [DOI] [PubMed] [Google Scholar]
- 104.Melendez J, van Ginneken B, Maduskar P, Philipsen RH, Ayles H, Sanchez CI. On combining multiple-instance learning and active learning for computer-aided detection of tuberculosis. IEEE Trans Med Imaging. 2016 Apr;35(4):1013–24. doi: 10.1109/TMI.2015.2505672. [DOI] [PubMed] [Google Scholar]
- 105.Varghese S, Anil A, Scaria S, Abraham E. Nanoparticulate technology in the treatment of tuberculosis: a review. Int J Pharm Sci Res. 2018;9(10):4109–16. doi: 10.13040/IJPSR.0975-8232. [DOI] [Google Scholar]
- 106.Ramirez-Priego P, Martens D, Elamin AA, Soetaert P, van Roy W, Vos R, Anton B, Bockstaele R, Becker H, Singh M, Bienstman P, Lechuga LM. Label-free and real-time detection of tuberculosis in human urine samples using a nanophotonic point-of-care platform. ACS Sens. 2018 Oct 26;3(10):2079–86. doi: 10.1021/acssensors.8b00393. [DOI] [PubMed] [Google Scholar]
- 107.Heller T, Mtemang'ombe EA, Huson MA, Heuvelings CC, Bélard S, Janssen S, Phiri S, Grobusch MP. Ultrasound for patients in a high HIV/tuberculosis prevalence setting: a needs assessment and review of focused applications for Sub-Saharan Africa. Int J Infect Dis. 2017 Mar;56:229–36. doi: 10.1016/j.ijid.2016.11.001. https://linkinghub.elsevier.com/retrieve/pii/S1201-9712(16)31216-4. [DOI] [PubMed] [Google Scholar]
- 108.Liu W, Zou D, He X, Ao D, Su Y, Yang Z, Huang S, Zhao Q, Tang Y, Ma W, Lu Y, Wang J, Wang X, Huang L. Development and application of a rapid Mycobacterium tuberculosis detection technique using polymerase spiral reaction. Sci Rep. 2018 Feb 14;8(1):3003. doi: 10.1038/s41598-018-21376-z. doi: 10.1038/s41598-018-21376-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Ou X, Wang S, Dong H, Pang Y, Li Q, Xia H, Qu Y, Zhang Z, Li J, Zhang J, Huan S, Chin DP, Zhao Y. Multicenter evaluation of a real-time loop-mediated isothermal amplification (RealAmp) test for rapid diagnosis of Mycobacterium tuberculosis. J Microbiol Methods. 2016 Oct;129:39–43. doi: 10.1016/j.mimet.2016.07.008. [DOI] [PubMed] [Google Scholar]
- 110.Law I, Loo J, Kwok H, Yeung H, Leung C, Hui M, Wu S, Chan H, Kwan Y, Ho H, Kong S. Automated real-time detection of drug-resistant Mycobacterium tuberculosis on a lab-on-a-disc by Recombinase Polymerase Amplification. Anal Biochem. 2018 Mar 1;544:98–107. doi: 10.1016/j.ab.2017.12.031. [DOI] [PubMed] [Google Scholar]
- 111.Liu Q, Lim BK, Lim SY, Tang WY, Gu Z, Chung J, Park MK, Barkham T. Label-free, real-time and multiplex detection of Mycobacterium tuberculosis based on silicon photonic microring sensors and asymmetric isothermal amplification technique (SPMS-AIA) Sens Actuators B Chem. 2018;255:1595–603. doi: 10.1016/j.snb.2017.08.181. [DOI] [Google Scholar]
- 112.Trzaskowski M, Napiórkowska A, Augustynowicz-Kopeć E, Ciach T. Detection of tuberculosis in patients with the use of portable SPR device. Sens Actuators B Chem. 2018;260:786–92. doi: 10.1016/j.snb.2017.12.183. [DOI] [Google Scholar]
- 113.Zhu F, Ou Q, Zheng J. Application Values of T-SPOT.TB in Clinical Rapid Diagnosis of Tuberculosis. Iran J Public Health. 2018 Jan;47(1):18–23. http://europepmc.org/abstract/MED/29318113. [PMC free article] [PubMed] [Google Scholar]
- 114.Nabeta P, Havumaki J, Ha DT, Caceres T, Hang PT, Collantes J, Lan NT, Gotuzzo E, Denkinger CM. Feasibility of the TBDx automated digital microscopy system for the diagnosis of pulmonary tuberculosis. PLoS One. 2017;12(3):e0173092. doi: 10.1371/journal.pone.0173092. http://dx.plos.org/10.1371/journal.pone.0173092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Bedard BA, Younge M, Pettit PA, Mendoza M. Using telemedicine for tuberculosis care management: A three county inter-municipal approach. J Med Syst. 2017 Nov 27;42(1):12. doi: 10.1007/s10916-017-0872-7. [DOI] [PubMed] [Google Scholar]
- 116.Naraghi S, Mutsvangwa T, Goliath R, Rangaka MX, Douglas TS. Mobile phone-based evaluation of latent tuberculosis infection: proof of concept for an integrated image capture and analysis system. Comput Biol Med. 2018 Jul 1;98:76–84. doi: 10.1016/j.compbiomed.2018.05.009. [DOI] [PubMed] [Google Scholar]
- 117.Mulder C, Mgode G, Reid SE. Tuberculosis diagnostic technology: an African solution … think rats. Afr J Lab Med. 2017;6(2):420. doi: 10.4102/ajlm.v6i2.420. http://europepmc.org/abstract/MED/28879158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Ho U, Chen C, Lin C, Hsu Y, Chi F, Chou C, Chen T, Wang C, Lou P, Ko J, Hsiao T, Yang T. Application of ultrasound-guided core biopsy to minimize the non-diagnostic results and the requirement of diagnostic surgery in extrapulmonary tuberculosis of the head and neck. Eur Radiol. 2016 Sep;26(9):2999–3005. doi: 10.1007/s00330-015-4159-4. [DOI] [PubMed] [Google Scholar]
- 119.Su M, Chen J, Bai B, Huang Y, Wei L, Liu M, Chen T. [Establishment and preliminary application of detection of Mycobacterium tuberculosis in sputum based on variable number tandem repeat] Zhejiang Da Xue Xue Bao Yi Xue Ban. 2016 Jan;45(1):61–7. doi: 10.3785/j.issn.1008-9292.2016.01.10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Oommen S, Banaji N. Laboratory diagnosis of tuberculosis: advances in technology and drug susceptibility testing. Indian J Med Microbiol. 2017;35(3):323–31. doi: 10.4103/ijmm.IJMM_16_204. http://www.ijmm.org/article.asp?issn=0255-0857;year=2017;volume=35;issue=3;spage=323;epage=331;aulast=Oommen. [DOI] [PubMed] [Google Scholar]
- 121.Chaintarli K, Jackson S, Cotter S, O'Donnell J. Evaluation and comparison of the National Tuberculosis (TB) Surveillance System in Ireland before and after the introduction of the Computerised Electronic Reporting System (CIDR) Epidemiol Infect. 2018 Oct;146(14):1756–62. doi: 10.1017/S0950268818001796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Medeiros ER, Silva SY, Ataide CA, Pinto ES, Silva MD, Villa TC. Clinical information systems for the management of tuberculosis in primary health care. Rev Lat Am Enfermagem. 2017 Dec 11;25:e2964. doi: 10.1590/1518-8345.2238.2964. http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-11692017000100401&lng=en&nrm=iso&tlng=en. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Tweed C, Nunn A. Data in TB have to be both big and good. Int J Tuberc Lung Dis. 2018 May 1;22(5):476. doi: 10.5588/ijtld.18.0200. [DOI] [PubMed] [Google Scholar]
- 124.Sanchini A, Andrés M, Fiebig L, Albrecht S, Hauer B, Haas W. Assessment of the use and need for an integrated molecular surveillance of tuberculosis: an online survey in Germany. BMC Public Health. 2019 Mar 18;19(1):321. doi: 10.1186/s12889-019-6631-6. https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-019-6631-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Manana PN, Kuonza L, Musekiwa A, Koornhof H, Nanoo A, Ismail N. Feasibility of using postal and web-based surveys to estimate the prevalence of tuberculosis among health care workers in South Africa. PLoS One. 2018;13(5):e0197022. doi: 10.1371/journal.pone.0197022. http://dx.plos.org/10.1371/journal.pone.0197022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Ha YP, Tesfalul MA, Littman-Quinn R, Antwi C, Green RS, Mapila TO, Bellamy SL, Ncube RT, Mugisha K, Ho-Foster AR, Luberti AA, Holmes JH, Steenhoff AP, Kovarik CL. Evaluation of a mobile health approach to tuberculosis contact tracing in Botswana. J Health Commun. 2016 Oct;21(10):1115–21. doi: 10.1080/10810730.2016.1222035. http://europepmc.org/abstract/MED/27668973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Rosenthal A, Gabrielian A, Engle E, Hurt DE, Alexandru S, Crudu V, Sergueev E, Kirichenko V, Lapitskii V, Snezhko E, Kovalev V, Astrovko A, Skrahina A, Taaffe J, Harris M, Long A, Wollenberg K, Akhundova I, Ismayilova S, Skrahin A, Mammadbayov E, Gadirova H, Abuzarov R, Seyfaddinova M, Avaliani Z, Strambu I, Zaharia D, Muntean A, Ghita E, Bogdan M, Mindru R, Spinu V, Sora A, Ene C, Vashakidze S, Shubladze N, Nanava U, Tuzikov A, Tartakovsky M. The TB Portals: an open-access, Web-based platform for global drug-resistant-tuberculosis data sharing and analysis. J Clin Microbiol. 2017 Nov;55(11):3267–82. doi: 10.1128/JCM.01013-17. http://jcm.asm.org/cgi/pmidlookup?view=long&pmid=28904183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Giannini B, Riccardi N, di Biagio A, Cenderello G, Giacomini M. A web based tool to enhance monitoring and retention in care for tuberculosis affected patients. Stud Health Technol Inform. 2017;237:204–8. [PubMed] [Google Scholar]
- 129.Davidson J, Anderson L, Adebisi V, de Jongh L, Burkitt A, Lalor M. Creating a web-based electronic tool to aid tuberculosis (TB) cluster investigation: data integration in TB surveillance activities in the United Kingdom, 2013 to 2016. Euro Surveill. 2018 Nov;23(44) doi: 10.2807/1560-7917.ES.2018.23.44.1700794. http://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2018.23.44.1700794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Crepaldi NY, de Lima IB, Vicentine FB, Rodrigues LM, Sanches TL, Ruffino-Netto A, Alves D, Rijo RP. Towards a clinical trial protocol to evaluate health information systems: evaluation of a computerized system for monitoring tuberculosis from a patient perspective in Brazil. J Med Syst. 2018 May 8;42(6):113. doi: 10.1007/s10916-018-0968-8. [DOI] [PubMed] [Google Scholar]
- 131.Shi Q, Ma J. [Big data analysis of flow of tuberculosis cases in China, 2014] Zhonghua Liu Xing Bing Xue Za Zhi. 2016 May;37(5):668–72. doi: 10.3760/cma.j.issn.0254-6450.2016.05.016. [DOI] [PubMed] [Google Scholar]
- 132.Khan MT, Kaushik AC, Ji L, Malik SI, Ali S, Wei D. Artificial neural networks for prediction of tuberculosis disease. Front Microbiol. 2019;10:395. doi: 10.3389/fmicb.2019.00395. doi: 10.3389/fmicb.2019.00395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Lopez-Garnier S, Sheen P, Zimic M. Automatic diagnostics of tuberculosis using convolutional neural networks analysis of MODS digital images. PLoS One. 2019;14(2):e0212094. doi: 10.1371/journal.pone.0212094. http://dx.plos.org/10.1371/journal.pone.0212094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Chithra R, Jagatheeswari P. Fractional crow search-based support vector neural network for patient classification and severity analysis of tuberculosis. IET Image Process. 2018;13(1):108. doi: 10.1049/iet-ipr.2018.5825. [DOI] [Google Scholar]
- 135.Ko DH, Lee EJ, Lee S, Kim H, Shin SY, Hyun J, Kim J, Song W, Kim HS. Application of next-generation sequencing to detect variants of drug-resistant Mycobacterium tuberculosis: genotype-phenotype correlation. Ann Clin Microbiol Antimicrob. 2019 Jan 3;18(1):2. doi: 10.1186/s12941-018-0300-y. https://ann-clinmicrob.biomedcentral.com/articles/10.1186/s12941-018-0300-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Dheda K, Lenders L, Srivastava S, Magombedze G, Wainwright H, Raj P, Bush SJ, Pollara G, Steyn R, Davids M, Pooran A, Pennel T, Linegar A, McNerney R, Moodley L, Pasipanodya JG, Turner CT, Noursadeghi M, Warren RM, Wakeland E, Gumbo T. Spatial network mapping of pulmonary multidrug-resistant tuberculosis cavities using RNA sequencing. Am J Respir Crit Care Med. 2019 Aug 1;200(3):370–80. doi: 10.1164/rccm.201807-1361OC. http://europepmc.org/abstract/MED/30694692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Hippner P, Sumner T, Houben RM, Cardenas V, Vassall A, Bozzani F, Mudzengi D, Mvusi L, Churchyard G, White RG. Application of provincial data in mathematical modelling to inform sub-national tuberculosis program decision-making in South Africa. PLoS One. 2019;14(1):e0209320. doi: 10.1371/journal.pone.0209320. http://dx.plos.org/10.1371/journal.pone.0209320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138.Seethamraju R, Diatha KS, Garg S. Intention to use a mobile-based information technology solution for tuberculosis treatment monitoring – applying a UTAUT model. Inf Syst Front. 2018;20(1):163–81. doi: 10.1007/s10796-017-9801-z. [DOI] [Google Scholar]
- 139.van Beek J, Haanperä M, Smit P, Mentula S, Soini H. Evaluation of whole genome sequencing and software tools for drug susceptibility testing of Mycobacterium tuberculosis. Clin Microbiol Infect. 2019 Jan;25(1):82–6. doi: 10.1016/j.cmi.2018.03.041. [DOI] [PubMed] [Google Scholar]
- 140.White EB, Meyer AJ, Ggita JM, Babirye D, Mark D, Ayakaka I, Haberer JE, Katamba A, Armstrong-Hough M, Davis JL. Feasibility, acceptability, and adoption of digital fingerprinting during contact investigation for tuberculosis in Kampala, Uganda: a parallel-convergent mixed-methods analysis. J Med Internet Res. 2018 Nov 15;20(11):e11541. doi: 10.2196/11541. https://www.jmir.org/2018/11/e11541/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Maraba N, Hoffmann CJ, Chihota VN, Chang LW, Ismail N, Candy S, Madibogo E, Katzwinkel M, Churchyard GJ, McCarthy K. Using mHealth to improve tuberculosis case identification and treatment initiation in South Africa: Results from a pilot study. PLoS One. 2018;13(7):e0199687. doi: 10.1371/journal.pone.0199687. http://dx.plos.org/10.1371/journal.pone.0199687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Khaparde SD, Gupta D, Ramachandran R, Rade K, Mathew ME, Jaju J. Enhancing TB surveillance with mobile technology: opportunities and challenges. Indian J Tuberc. 2018 Jul;65(3):185–6. doi: 10.1016/j.ijtb.2018.06.002. [DOI] [PubMed] [Google Scholar]
- 143.Andre E, Isaacs C, Affolabi D, Alagna R, Brockmann D, de Jong BC, Cambau E, Churchyard G, Cohen T, Delmee M, Delvenne J, Farhat M, Habib A, Holme P, Keshavjee S, Khan A, Lightfoot P, Moore D, Moreno Y, Mundade Y, Pai M, Patel S, Nyaruhirira AU, Rocha LE, Takle J, Trébucq A, Creswell J, Boehme C. Connectivity of diagnostic technologies: improving surveillance and accelerating tuberculosis elimination. Int J Tuberc Lung Dis. 2016 Aug;20(8):999–1003. doi: 10.5588/ijtld.16.0015. http://europepmc.org/abstract/MED/27393530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Ng KC, Meehan CJ, Torrea G, Goeminne L, Diels M, Rigouts L, de Jong BC, André E. Potential application of digitally linked tuberculosis diagnostics for real-time surveillance of drug-resistant tuberculosis transmission: validation and analysis of test results. JMIR Med Inform. 2018 Feb 27;6(1):e12. doi: 10.2196/medinform.9309. https://medinform.jmir.org/2018/1/e12/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Riccardi N, Giannini B, Borghesi ML, Taramasso L, Cattaneo E, Cenderello G, Toscanini F, Giacomini M, Pontali E, Cassola G, Viscoli C, di Biagio A. Time to change the single-centre approach to management of patients with tuberculosis: a novel network platform with automatic data import and data sharing. ERJ Open Res. 2018 Jan;4(1):pii: 00108–2017. doi: 10.1183/23120541.00108-2017. http://europepmc.org/abstract/MED/29410957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Falzon D, Migliori GB, Jaramillo E, Weyer K, Joos G, Raviglione M, Global Task Force on digital health for TB Digital health to end tuberculosis in the Sustainable Development Goals era: achievements, evidence and future perspectives. Eur Respir J. 2017 Nov;50(5):pii: 1701632. doi: 10.1183/13993003.01632-2017. http://erj.ersjournals.com/cgi/pmidlookup?view=long&pmid=29122920. [DOI] [PubMed] [Google Scholar]
- 147.Doshi R, Falzon D, Thomas BV, Temesgen Z, Sadasivan L, Migliori GB, Raviglione M. Tuberculosis control, and the where and why of artificial intelligence. ERJ Open Res. 2017 Apr;3(2):pii: 00056–2017. doi: 10.1183/23120541.00056-2017. http://europepmc.org/abstract/MED/28656130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148.Konduri N, Bastos LG, Sawyer K, Reciolino LFA. User experience analysis of an eHealth system for tuberculosis in resource-constrained settings: a nine-country comparison. Int J Med Inform. 2017 Jun;102:118–29. doi: 10.1016/j.ijmedinf.2017.03.017. https://linkinghub.elsevier.com/retrieve/pii/S1386-5056(17)30078-3. [DOI] [PubMed] [Google Scholar]
- 149.Konduri N, Sawyer K, Nizova N. User experience analysis of e-TB Manager, a nationwide electronic tuberculosis recording and reporting system in Ukraine. ERJ Open Res. 2017 Apr;3(2):pii: 00002–2017. doi: 10.1183/23120541.00002-2017. http://europepmc.org/abstract/MED/28512634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Pande T, Saravu K, Temesgen Z, Seyoum A, Rai S, Rao R, Mahadev D, Pai M, Gagnon M. Evaluating clinicians' user experience and acceptability of LearnTB, a smartphone application for tuberculosis in India. Mhealth. 2017;3:30. doi: 10.21037/mhealth.2017.07.01. doi: 10.21037/mhealth.2017.07.01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.The World Bank. [2019-08-03]. Where We Work https://www.worldbank.org/en/where-we-work.
- 152.Falzon D, Timimi H, Kurosinski P, Migliori GB, van Gemert W, Denkinger C, Isaacs C, Story A, Garfein RS, Bastos LG, Yassin MA, Rusovich V, Skrahina A, van Hoi Le, Broger T, Abubakar I, Hayward A, Thomas BV, Temesgen Z, Quraishi S, von Delft D, Jaramillo E, Weyer K, Raviglione MC. Digital health for the End TB Strategy: developing priority products and making them work. Eur Respir J. 2016 Jul;48(1):29–45. doi: 10.1183/13993003.00424-2016. http://erj.ersjournals.com/cgi/pmidlookup?view=long&pmid=27230443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.To KW, Kam KM, Lee SS, Chan KP, Yip T, Lo R, Ngai J, Ng S. Clinical application of Genexpert on BAL samples in management of TB in intermediate burden area. Chest. 2017;152(4):A194. doi: 10.1016/j.chest.2017.08.225. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Search strategy syntax for databases PubMed and Web of Science.