

Abstract
Summary: We present the case of a 57-year-old patient who was admitted to the hospital for preoperative cerebral angiography because of an intraspinal mass at the level of C1 and C2. Angiographic examination revealed an abnormal origin of the right vertebral artery, which normally originates from the right subclavian artery. Thus, the right vertebral artery was the last branch of the supraaortic vessels. We also review herein the incidence of the various anomalous origins of the right vertebral artery in the literature and discuss their potential embryologic development and clinical significance.
In angiographic or anatomic postmortem examinations, abnormal vertebral artery origins are only incidental findings because, for most cases, they are clinically asymptomatic. Nonetheless, these abnormalities are of diagnostic importance either prior to vascular surgery in the neck region or in cases of intravascular diseases such as arteriovenous malformations or cerebral aneurysms. On the basis of this case report and descriptions in the literature, this article aims to depict the different variants of anomalous right vertebral artery origins, their rate of occurrence, and their potential embryologic development.
Case Report
A 57-year-old man was admitted to the hospital because of an increasing paresthesia in his left arm and leg that began 2 months before. In addition, he was suffering from an isolated neck pain, which increased with motion, and began during the previous 4 weeks. Conventional radiographic images showed markedly degenerative changes in the cervical vertebrae associated with spondylophytic growth. MR imaging of the cervical spine revealed a contrast-enhancing intraspinal extramedullar mass at the level of the C1 and C2 consisting of a large extraspinal portion and a myelin compression, whereas the CT examination exhibited a bony destruction of the first vertebral bow. Overall, the clinical and neuroradiologic findings revealed the need for tumor resection.
In order to assess tumor vascularisation, a preoperative digital subtraction angiography was performed. During this procedure, the origin of the right vertebral artery from the brachiocephalic artery was lacking and a hypoplasia or aplasia of this artery was assumed. Nonetheless, during selective injection of contrast medium into the left vertebral artery, a retrograde filling of the distal right vertebral artery could be seen. After further attempts to find other possible origins, this artery ultimately could be depicted ascending directly from the aortic arch, distally to the left subclavian artery (Fig 1, 2). The anatomic relation of all supraaortic arteries was confirmed at the end of the procedure by global injections into the aortic arch (Fig 3).
fig 1.
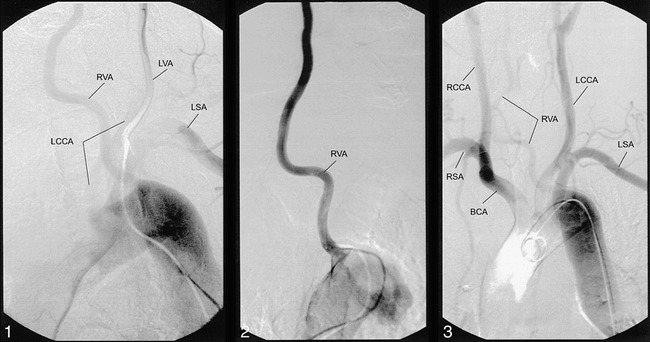
During the selective contrast medium injection into the left vertebral artery, the catheter was pulled back to the aortic arch. A filling of the left common carotid artery and the anomalous right vertebral artery origin is shown.
Note.—RVA, right vertebral artery; LVA, left vertebral artery; LSA, left subclavian artery; LCCA, left common carotid artery.
fig 2. The selective position of the catheter within the right vertebral artery shows the direct origin of this artery from aortic arch.
fig 3. Angiography of the aortic arch confirms the anomalous origin and connection to other supraaortic arteries.
Note.—RCCA, right common carotid artery; RSA, right subclavian artery; BCA, brachiocephalic artery.
In subsequent surgery, intra- and extraspinal tumor masses (histologically confirmed neurinoma) could be removed after laminectomy of C1. Several days thereafter, the patient improved symptomatically.
Discussion
Anomalous origin of the vertebral arteries is not very common. In fact, most types have been published in a few case reports. Only two variants have a higher frequency. In a large autopsy series, the origin of the left vertebral artery directly from the aortic arch between the left common carotid artery and left subclavian artery was seen in 2.4% to 5.8% of cases (1, 2); angiographic findings were described in 15 case reports. The origin of the right vertebral artery from the right common carotid artery, in combination with a right subclavian artery originating distal to the left subclavian artery (artery lusoria), was documented in 10 case reports.
The anomalous origins of the right vertebral artery were divided into three categories: those originating directly from the aorta (n=9), those originating from the carotid arteries (minus those mentioned above combined with artery lusoria) or from the brachiocephalic artery (n=10), and those of duplicated origin (n=13). A detailed overview of these findings is given in Figure 4. The variant of a right vertebral artery originating distal from the left subclavian artery as the last branch of the aortic arch, as described in this paper (Fig 5), has been published previously in seven cases (five in English-language and two in Japanese-language journals). To the best of our knowledge, only one original-research radiologic paper on this variant has been published (3). Further anomalous origins arising directly from the aortic arch can be located between the common carotid artery and the subclavian artery (n=l) and in combination with a missing brachiocephalic artery between the right subclavian artery and the common carotid artery (n=1). The anomalous origins of the left vertebral artery are those previously mentioned from the aortic arch, as well as those originating from the carotid region (n=7) and duplicated origins (n=13).
fig 4.
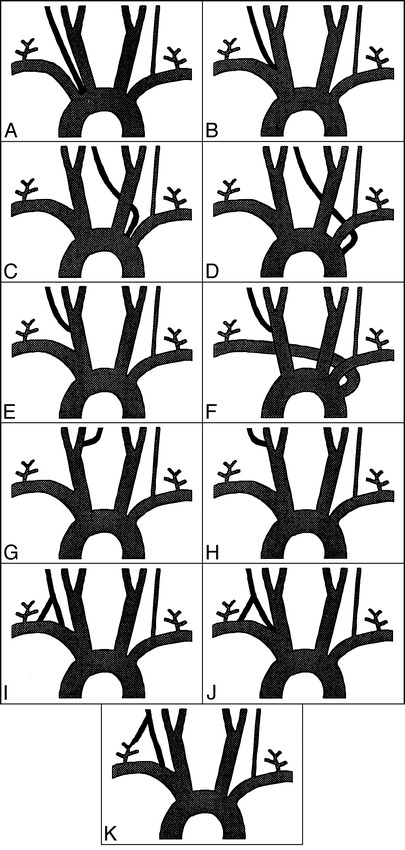
Overview of the different origin variants of the right vertebral artery.
A, Right vertebral artery from the aorta between the right subclavian and common carotid artery in cases of missing brachiocephalic arteries. One case has been described in the literature (Lippert H [1985]).
B, Right vertebral artery from the aorta on the left between the left common carotid artery and left subclavian artery. One case has been described in the literature (Wasserman BA [1992]).
C, Right vertebral artery from the aorta on the left, distal to the left subclavian artery. Seven cases have been described in the literature (Lie TA [1968], Newton TH [1974], Argenson C [1980], Sakamoto H [1980], Schwarzacher SW [1989], Takagi T [1992]), and in one case this was combined with coactation (Stoesslein F [1982]).
D, Right vertebral artery directly from the brachiocephalic artery. Three cases have been described in the literature (Daseler EH [1959], Argenson C [1980], Lippert H [1985]).
E, Right vertebral artery from the right common carotid artery without A. lusoria. Six cases have been reported in the literature (Daseler EH [1959], Koo K [1966], Lippert H [1985]).
F, Right vertebral artery from the right common carotid artery with A. lusoria. Ten cases have been reported in the literature (Iyer AA [1927], Windel WF [1928] Newton TH [1974], Bernard L [1975], Palmer FJ [1977] Tan WS [1979] Wackenheim A [1979]).
G. Right vertebral artery from the right internal carotid artery via the hypoglossal artery. One case has been reported in the literature (Keller HL [1973]).
H, Right vertebral artery from the right external carotid artery. There have been no known cases of this vertebral artery origin.
I, Right vertebral artery with double origin from the right subclavian artery. Eleven cases have been reported (Lie TA [1968], Babin E [1974], Argenson C [1980], Rath G [1984], Harada J [1987], Hashimoto [1987], Nishijima M [1989], Cavdar S [1989], Nogueira TE [1997], Takasato Y [1992]).
J, Right vertebral artery with double origin from the right subclavian artery and the brachiocephalic artery. One case has been reported in the literature (Kiss J [1968]).
K, Right vertebral artery with double origin from the right subclavian artery and the right thyreocervical trunk. One case has been reported in the literature (Lippert H [1985]).
fig 5.
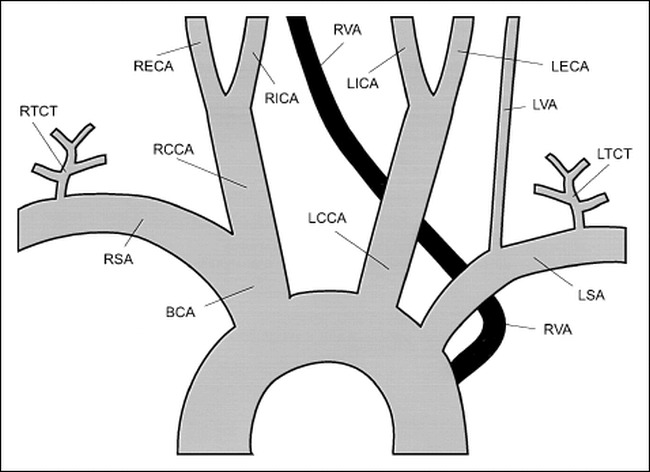
Drawing of the case presented herein
To understand the hypothetical development of anomalous origin of vertebral arteries, knowledge of the embryologic development of the aortic arch and the brachiocephalic vessels is necessary (4). Embryologically, the right subclavian artery develops partially from the right primitive dorsal aorta. During this process, the caudal part of the dorsal aorta is obliterated just before the confluence with the left dorsal aorta, and the C7 intercostal artery continues into the subclavian artery (4, 5). The vertebral artery arises from the postcostal longitudinal anastomosis between the C1 and C7 intercostal arteries and the cervical intercostal obliteration zone (Fig 6A). If the obliteration zone is proximal to the origin of the C7 intercostal artery, the origin of the left subclavian artery is moved to the left. Therefore, it originates left, distal to the left subclavian artery (A. lusoria) (5). The right vertebral artery originates from the normal position from the right subclavian artery (Fig 6B). A separation of the right vertebral artery origin from the subclavian artery can be explained by migration of the vertebral artery onto the dorsal aorta (5) or with a separate development of the vertebral artery from the C6 or C8 intercostal artery (5, 6) instead of the C7 intercostal artery. If the right vertebral artery arises from the C6 intercostal artery, with obliteration of the longitudinal anastomosis between the C6 and C7 intercostal artery, and the obliteration of the right dorsal aorta occurs proximal to the C7 intercostal artery origin, the origin of the right subclavian artery is moved to the left (A. lusoria). The right vertebral artery, however, originates from the right common carotid artery (Fig 6C). If the vertebral artery arises from the C8 intercostal artery and the physiologic obliteration of the right dorsal aorta is distal from the C7 intercostal artery, only the origin of the right vertebral artery is moved to the left (6). In this process, corresponding to the case presented herein, the right subclavian artery originates from the right side of the aorta and the right vertebral artery originates from the left distally to left subclavian artery (Fig 6D). The origin variants of the vertebral artery from the carotid arteries frequently display persisting embryonal vessel and hypoplasia or aplasia of the proximal vertebral artery (7).
fig 6.
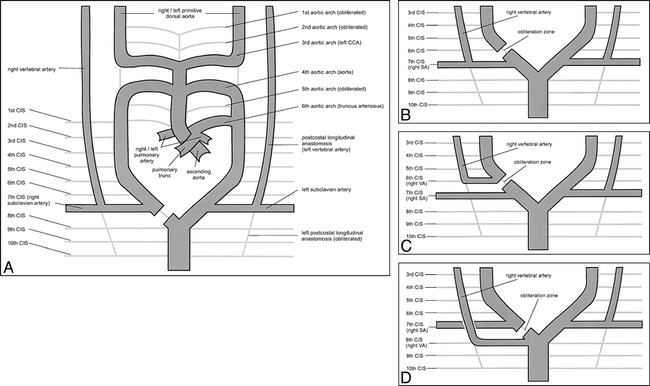
Drawing of the embryologic development of the aorta and brachiocephalic vessels (14-mm embryonic stage).
A, Normal development.
B, Development of lusorian artery; origin of right vertebral artery also moves to the left.
C, Development of lusorian artery, origin of right vertebral artery remains on the right (common carotid artery).
D, Development of the right vertebral artery originating from the left and right subclavian artery arising from the right.
In most cases described in the literature, anomalous vertebral artery origins did not result in clinical symptoms (5). In rare cases, patients complained of dizziness, which was thought to have no connection to the anomalous origin of the vertebral artery (8). There is no conclusive evidence that these variants lead to a predisposition to cerebrovascular disorders (5). Nevertheless, some authors hypothesize that anomalous origins and the distribution of the large aortic arch vessels can cause changes in cerebral hemodynamics that may lead to cerebral abnormalities (9).
The true value of detecting anomalous origins is the diagnostic gain prior to the surgery of supraaortic arteries. For cases in which the vertebral artery originates from the carotid artery or its branches, the ligation of the common carotid artery may cause a compromise of the posterior fossa blood supply (10). Detailed knowledge of an anomalous origin of supraaortic arteries is also of importance for patients who have to undergo four-vessel angiography in an emergency to rule out, for example, the possibility of intracranial aneurysm after subarachnoid hemorrhage. If the detection of a vertebral artery in the normal position is not possible, the presence of such a variant must be taken into consideration.
In summary, although anomalous origins of the vertebral artery are only anatomic variants, detailed information of these is crucial for vascular surgery in the head and neck region or in cases of four-vessel angiography.
Footnotes
Address reprint requests to Dr. med. Arne-Jörn Lemke, Universitätsklinikum Charité, Medizinische Fakultät der Humboldt-Universität zu Berlin, Campus Virchow-Klinikum Strahlenklinik und Poliklinik, Augustenburger Platz 1, 13353 Berlin, Germany.
References
- 1.Adachi B. Das Arteriensystem der Japaner. Kyoto: Kenkyu-Sha; 1928
- 2.Newton TH, Mani RL. The vertebral artery. . In: Newton TH, Potts DG, eds. Radiology of the Skull and Brain. St. Louis: Mosby; 1974;1659-1672
- 3.Stoesslein F, Porstmann W, Schueler F, Schoepke W. Aberrant vertebral artery originating from the descending aorta: a new congenital steal syndrome in coarctation. . Eur J Radiol 1982;2:157-159 [PubMed] [Google Scholar]
- 4.Moore KL. The Developing Human. . 3rd ed. Philadelphia: Saunders; 1982
- 5.Wasserman BA, Mikulis DJ, Manzione JV. Origin of the right vertebral artery from the left side of the aortic arch proximal to the origin of the left subclavian artery. . AJNR Am J Neuroradiol 1992;13:355-358 [PMC free article] [PubMed] [Google Scholar]
- 6.Schwarzacher SW, Krammer EB. Complex anomalies of the human aortic arch system: unique case with both vertebral arteries as additional branches of the aortic arch. . Anat Rec 1989;225:246-250 [DOI] [PubMed] [Google Scholar]
- 7.Keller HL, Weiss D. Origin of an artery supplying the vertebral region, descendingfrom the cervical sector of the right internal carotid artery. . Fortschr Geb Rontgenstr Nuklearmed 1973;118:473-474 [PubMed] [Google Scholar]
- 8.Nishijima M, Harada J, Nogami K, Endo S, Takaku A. Operative correction of kinking and coiling at the origin of vertebral artery and stellate ganglionectomy in patients with severe vertigo and dizziness. . No Shinkei Geka 1989;17:255-261 [PubMed] [Google Scholar]
- 9.Bernardi L, Dettori P. Angiographic study of a rare anomalous origin of the vertebral artery. . Neuroradiology 1975;9:43-47 [Google Scholar]
- 10.Flynn RE. External carotid origin of the dominant vertebral artery. Case report. . J Neurosurg 1968;29:300-301 [DOI] [PubMed] [Google Scholar]