

Abstract
Summary: Multichannel fenestration of the internal carotid artery (ICA) is a rare, previously unreported developmental anomaly with unknown clinical significance. Although previously thought to have distinct embryologic origins, the presence of multiple channels in a short-segment fenestration favors a common developmental pathway for the origin of duplications and fenestrations: the persistence of a plexiform vascular network from the 4-mm to 5-mm embryologic stage of development.
Reported cases of duplication and fenestration of the internal carotid artery (ICA) are rare. Duplications have been defined as long-segment involvement of the ICA, whereas the term “fenestration” has been used to describe short-segment duplications. The presence of greater than two channels in a short segment of the ICA has not been previously described. Our case describes an example of a multichannel short-segment fenestration of the ICA revealed by digital subtraction angiography.
Case Report
A 73-year-old man suffering from atypical Parkinson's disease presented with diminished mental status, vertigo, and dizziness when his head was actively placed in a highly flexed position. These symptoms were alleviated when the head was extended. The patient underwent noninvasive Doppler sonographic examination of his neck vessels, which suggested minimal flow in the right vertebral artery. Digital subtraction angiography of both common carotid and vertebral arteries was subsequently performed. The vertebral artery injections were repeated with the head flexed in an attempt to reproduce the patient's clinical symptoms. The right vertebral artery was slightly smaller in diameter than the left vertebral artery; however both vertebral arteries were free of stenosis in the neutral and flexed positions. The right ICA demonstrated a short-segment division of the petrous segment into four channels (Fig 1). The fenestration was approximately 1-cm long. The ICA was equal in diameter above and below the fenestration. No additional abnormality of the cervical or intracranial vessels was identified.
fig 1.

Selective injection of the right common carotid artery reveals a fenestration of the petrous segment of the ICA into four discrete channels
Discussion
Numerous reports of duplications and fenestrations of the intracranial internal carotid, anterior cerebral, middle cerebral, vertebral and basilar arteries exist (1–5). These have been associated with an increased occurrence of aneurysms, both at the proximal site of fenestration, and in unrelated vessels (1, 3, 4). Reported cases of extracranial duplication and fenestration are rarer, but have also had additional vascular abnormalities including aneurysms, persistent stapedial artery, and lateral course of the external carotid artery (6–10). One reported case attributed a transient ischemic attack to the embolization of a thrombus suspected to have been present within a fenestration (11). Our patient's symptoms suggested a posterior circulation abnormality, and a relation to the fenestration of the ICA. Intracranial angiographic examination of our patient yielded normal findings, but sonographic evaluation should be performed in all patients with fenestrations and duplications associated with the higher incidence of associated vascular abnormalities.
The normal embryologic development of the ICA involves modifications and regressions of the ventral and dorsal aorta and its arches. The different segments of the ICA correspond to persistence of embryologic structures as follows: the cervical segment (third aortic arch); the ascending intrapetrous segment (dorsal aorta between the second and third aortic arches); the horizontal intrapetrous segment (dorsal aorta between primitive maxillary artery and first aortic arch); the horizontal segment of the carotid siphon (dorsal aorta between the inferolateral trunk and the primitive maxillary artery); and the supraclinoid segment (dorsal aorta between the inferolateral trunk and its terminal branches) (Fig 2).
fig 2.
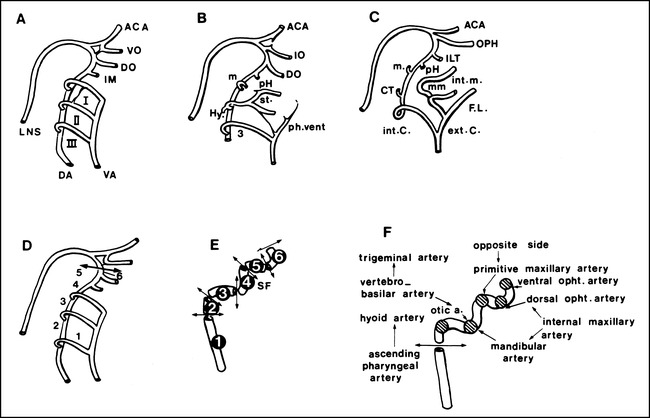
An illustration of the embryonic development of the aortic arches in the craniocephalic region is depicted. Successive stages of development are shown (A, B, and C), while the specific development of the internal carotid artery (D), its different segments (E) and the embryonic vessels and their origins (F) are highlighted.
A, Aortic arches (I—III) are numbered in the craniocaudal direction: the anterior cerebral artery (ACA); ventral ophthalmic artery (VO); dorsal ophthalmic artery (DO); primitive maxillary artery (IM); longitudinal neural system (LNS); dorsal aorta (DA), and ventral aorta (VA) are shown.
B, The primitive ophthalmic (IO), stapedial (st), hyoid (Hy), and ventral pharyngeal artery (vent. Ph.) arteries are illustrated.
C, The definitive ophthalmic artery (OPH), intracavernous collateral of the internal carotid artery (ILT) middle meningeal arteries (mm), caroticotympanic artery (CT), internal maxillary artery (int. m.), faciolingual system (FL), internal carotid (int. C) and external carotid artery (ext. C) are highlighted.
D, The third aortic arch (1), dorsal aorta between the second and third aortic arches (2), dorsal aorta between the first and second aortic arches (3), dorsal aorta between the first aortic arch and the primitive maxillary artery (4), dorsal aorta between the primitive maxillary artery and the inferolateral trunk (5), and dorsal aorta between the inferolateral trunk and its terminal branches (6) are shown.
E, The cervical segment (1), initial ascending intrapetrous segment (2), distal horizontal intrapetrous segment (3), segment ascending in the sphenoid fissure (SF) and through the cavernous sinus (4), horizontal segment of the carotid siphon (5), and clinoid segment (6) are shown.
F, Embryonic vessels and their origin are illustrated.
Several theories on the embryologic development of fenestration and duplication have been proposed. At the early stage of embryonic development (4–5-mm stage), the third aortic arch (or primitive cervical segment) appears in plexiform arterial channels (12, 13). It has been proposed that if two channels persist, a duplication of the cervical ICA will result rather than the usual single channel (14). Fenestrations, however, are proposed to result from an anomalous connection of the third aortic arch with the dorsal aorta, or from persistence of the cranial portion of the carotid duct (the segment of the dorsal aorta between the third and fourth arches) (7, 16). This suggests alternative theories for the development of fenestrations and duplications. Our case of a short-segment of plexiform arterial channels within the ICA, however, seems to favor the former theory of persistence of multiple channels at the 4–5-mm embryologic stage. This would favor the theory of a single embryologic developmental pathway for both entities. The alternative hypothesis of multiple anomalous connections between the third aortic arch and the dorsal aorta proposes persistence of multiple channels within the distal segment of the carotid duct. This latter theory remains possible, suggesting a plexiform network within the carotid duct and other segments of the dorsal aorta at a similar stage of embryologic development.
Conclusion
Short-segment multichannel fenestration of the ICA is a rare, previously unreported finding that at present has unknown clinical significance. Although previously thought to have distinct embryologic origins, our case appears to favor a common developmental pathway for fenestrations and duplications of the ICA.
Footnotes
Address reprint requests to George P. Teitelbaum, M.D., USC University Hospital, 1500 San Pablo St, Los Angeles, CA 90033.
*Reprinted with permission from Surgical Neuroangiography, Volume I: Functional Anatomy of Craniofacial Arteries, Springer-Verlag, New York, NY.
References
- 1.Banach MJ, Flamm ES. Supraclinoid internal carotid artery fenestration with an associated aneurysm. Case report. J Neurosurg 1993;79:438-441 [DOI] [PubMed] [Google Scholar]
- 2.Fujimukra M, Seki H, Suguwara T, Tomich N, Oku T, Higuchi H. Anomalous internal carotid artery-anterior cerebral artery anastomosis associated with fenestration and cerebral aneurysm. Neuro Med Chir 1996;36:229-233 [DOI] [PubMed] [Google Scholar]
- 3.Lazar ML, Bland JE, North RR, Bringewald PF. Middle cerebral artery fenestration. Neurosurgery 1980;6:297-300 [PubMed] [Google Scholar]
- 4.Osborne RE, Kirk G. Cerebral artery fenestration. Comput Radiol 1987;11:141-145 [DOI] [PubMed] [Google Scholar]
- 5.Uchiyarna S, Yoshinaga T, Shima T. A case of basilar artery fenestration with recurrent attacks of vertebrobasilar insufficiency. No To Shinkei 1987;39:1163-1169 [PubMed] [Google Scholar]
- 6.Chess MA, Barsotti JB, Chang JK, Ketonen LM. Duplication of the extracranial internal carotid artery. AJNR Am J Neuroradiol 1995;16:1545-1547 [PMC free article] [PubMed] [Google Scholar]
- 7.Tanaka M, Matsumoto S. Fenestration of the internal carotid artery. Neurol Med Chir 1982;22:391-395 [DOI] [PubMed] [Google Scholar]
- 8.Schmieder K, Hardenack M, Harders A. Proximal long fenestration associated with an internal carotid artery aneurysm. Case illustration. . J Neurosurg 1997;86:733. [DOI] [PubMed] [Google Scholar]
- 9.Schmieder K, Hardenack M, Harders A. Proximal long fenestration associated with an internal carotid artery aneurysm. Case illustration. J Neurosurg 1997;86:733. [DOI] [PubMed] [Google Scholar]
- 10.Koenigsberg RA, Zito JL, Patel M, Swartz JD, Goldofsky E, Zahtz G. Fenestration of the internal carotid artery: a rare mass of the hypotympanum associated with persistence of the stapedial artery. AJNR AM J Neuroradiol 1995;16:908-910 [PMC free article] [PubMed] [Google Scholar]
- 11.Nakamura H, Yamada H, Nagao T, Fujita K, Tamaki N. Fenestration of the internal carotid artery associated with an ischemic attack. Case report. Neurol Med Chir 1993;33:306-308 [DOI] [PubMed] [Google Scholar]
- 12.Congdon ED. Transformation of the aortic arch system during the development of the human embryo. Contrib Embryol 1922;47-110
- 13.Padget DH. The development of the cranial arteries in the human embryo. Contrib Embryol 1948;31:205-262 [Google Scholar]
- 14.Killien FC, Wyler AR, Cromwell LD. Duplication of the internal carotid artery. Neuroradiology 1980;19:101-102 [DOI] [PubMed] [Google Scholar]
- 15.Yamada T, Inagawa T, Takedo T. Ruptured aneurysm of the anterior cerebral artery fenestration. Case report. J Neurosurg 1982;57:826-828 [DOI] [PubMed] [Google Scholar]