

Abstract
INTRODUCTION:
Hepatic involvement in hereditary hemorrhagic telangiectasia (HHT) is common and can be associated with severe clinical consequences, including portal hypertension, cardiac failure, and encephalopathy. However, there are no reliable clinical predictors of hepatic involvement and its associated complications, limiting appropriate identification of these patients. In this work, we define the utility of serum ammonia and liver biochemical tests (LFTs) in predicting hepatic HHT involvement and its complications.
METHODS:
We performed a retrospective study examining a well-characterized cohort of patients with HHT. Clinical characteristics, laboratory tests, liver imaging, transthoracic echocardiography assessment of right ventricular systolic pressure (RVSP), and history of other HHT-related outcomes were assessed. Patients were followed for the development of encephalopathy.
RESULTS:
Of 45 patients with definite HHT, 18 (40%) had elevated ammonia levels. An elevated ammonia associated with the presence of hepatic arteriovenous malformations (AVMs) on imaging (P < 0.03) and when combined with elevated liver tests increased the sensitivity for hepatic AVMs by 18% (55% for LFTs vs 73% for LFTs plus ammonia). Furthermore, an elevated serum ammonia in patients with HHT associated with an elevated RVSP (>35 mm Hg), providing an 80% sensitivity and 71% specificity for predicting the presence of pulmonary hypertension. In contrast, there was no association with an elevated serum ammonia and encephalopathy over a total of 859 months of follow-up.
DISCUSSION:
Elevated ammonia in a cohort of patients with HHT was associated with the presence of hepatic AVMs and elevated RVSP, but no other complications of HHT, including encephalopathy.
INTRODUCTION
Hereditary hemorrhagic telangiectasia (HHT) is an autosomal dominant multisystem disorder characterized by vascular dysregulation, leading to telangiectasias and arteriovenous malformations (AVMs) of the skin, lung, gastrointestinal tract, liver, and brain. Although HHT is rare with a prevalence of approximately 1 in 5,000 people, hepatic involvement in the disease is common (1). The existing literature suggests that 32%–78% of patients with HHT have hepatic involvement, with AVMs affecting the destination of portal venous and hepatic arterial blood flow (1–3). The clinical consequences of hepatic AVMs include high-output cardiac failure, portal hypertension, ischemic biliary disease, hepatic encephalopathy, and abdominal angina (4). According to the largest longitudinal cohort study to date, approximately 25% of patients with hepatic HHT involvement eventually experience one of these complications (5).
Despite the dire potential consequences of hepatic involvement in HHT, there are limited data regarding appropriate hepatic screening, resulting in ambiguous expert recommendations. In 2018, the European Reference Networks for Rare Vascular Diseases (VASCERN) published recommended clinical practices for patients with HHT, but did not explicitly address screening for hepatic involvement (6). A consensus statement from the 2005 HHT International Scientific Conference stated that liver involvement in HHT can be investigated by way of liver tests and imaging in all patients at risk of HHT, but cited poor level evidence to support the recommendation (7). Updated recommendations from the 2019 International HHT Guidelines expert panel are awaited. Other groups have recommended echocardiography and Doppler ultrasound of the liver for those with abnormal liver function tests, but offer no clear guidance as to when liver function tests are warranted (1,3,8). Therapies exist for the high-output cardiac failure and hepatic complications of hepatic AVMs in HHT; accordingly, there is a great need for screening strategies to diagnose hepatic involvement, which may in turn improve patient outcomes (3,7,9–11).
Ammonia is a product of intestinal microbial metabolism, transported via the portal vein to the liver where it is detoxified. In the presence of portosystemic shunts, ammonia can bypass the liver and enter the systemic circulation. Given the vascular malformations inherent to HHT, elevated venous ammonia in a patient with HHT may be a valuable marker of portosystemic shunting via AVMs. This portosystemic shunting may contribute to the development of hepatic encephalopathy or high-output cardiac failure. To our knowledge, no study has reported the efficacy of venous ammonia or other liver tests to predict the presence of hepatic AVMs and their associated complications.
We hypothesized that some patients with HHT would have an elevated venous ammonia, and furthermore, that elevated venous ammonia would be associated with hepatic involvement of HHT and the development of heart failure and hepatic encephalopathy.
METHODS
This study was approved by the Institutional Review Board of the Massachusetts General Hospital. We performed a single-center retrospective study of patients in our HHT clinic from September 2012 through February 2019.
Patient selection
The Massachusetts General Hospital has an HHT Center of Excellence, composed of subspecialists in pulmonary hypertension, gastroenterology, hepatology, neurology, hematology, otolaryngology, and interventional radiology. After anecdotal recognition that several patients with HHT had elevated venous ammonia levels, in September 2012, providers began to routinely test venous ammonia in many patients with HHT. Patients who had undergone venous ammonia testing by members of the HHT center were identified via manual chart review of an HHT patient list in the electronic medical record. We only included patients who met the criteria for “definite” HHT, defined as at least 3 of the 4 Curaçao criteria: epistaxis, mucocutaneous telangiectasias, visceral AVMs, and family disease history (3,6). We excluded individuals meeting fewer than 3 of these criteria.
Data collection
The following data were collected from each patient's medical record: age, sex, Curaçao diagnostic criteria for HHT, HHT genetic mutation data, other known liver disease, venous ammonia, liver biochemical tests, and assessments of HHT-related clinical outcomes.
Ammonia testing was performed in the outpatient setting with the commercial Sekure ammonia assay (Sekisui Diagnostics LLC, Maidstone, United Kingdom). Each patient's first ammonia test result was recorded and categorized as elevated if above our laboratory's reference range (12–48 μmol/L). Baseline alanine transaminase, aspartate transaminase (AST), total bilirubin, and alkaline phosphatase levels were also collected.
An abdominal radiologist blinded to diagnosis, ammonia level, and clinical outcome evaluated all the patients' abdominal imaging studies to assess for evidence of hepatic HHT involvement. Liver involvement was confirmed by the presence of AVMs on ultrasound, computed tomography, magnetic resonance imaging (MRI), or angiography (12). The study radiologist interpretation was discordant with the original radiologist in 2 of the 31 studies; our reported results use the study radiologist interpretation.
Transthoracic echocardiography (TTE) was interrogated for assessment of right ventricular systolic pressure (RVSP), which can be elevated in pulmonary artery hypertension and right heart overload states. RVSP > 35 was specifically selected as an important outcome, given previous literature finding sensitivity of 86% and negative predictive value of 80% for pulmonary hypertension with that cutoff (13). The most recent RVSP assessment was used and could be no more than 3 years before baseline ammonia testing. Transthoracic contrast echocardiography was also interrogated for the presence and grade of microbubbles in the left ventricle within 3–8 cycles, consistent with intrapulmonary shunt. In accordance with convention, grade 0 signified no bubbles, grade 1 signified 1–30 bubbles, grade 2 signified 30–100 bubbles, and grade 3 signified >100 bubbles in the left ventricle (14–16).
A gastroenterologist (J.L.) and gastroenterology fellow (P.P.B.) reviewed the medical records and assessed for a diagnosis of cholangitis or overt hepatic encephalopathy. Two pulmonary hypertension specialists (J.R.-L. and A.S.W.) assessed for high-output cardiac failure. The remaining outcomes were obtained from thorough documentation of multiple subspecialty providers in the HHT Clinic, including the presence of and intervention on gastrointestinal AVMs, epistaxis, pulmonary AVMs, and central nervous system AVMs. Any concomitant liver disease was recorded.
Statistical analysis
We used a parametric t test or Fisher exact test to compare clinical characteristics of patients with HHT with high baseline ammonia levels and those with normal ammonia levels. Descriptive statistics were summarized using a mean and SD (continuously measured) or presented as proportions (categorical). An ANOVA was used to assess the ammonia level between 3 categories: no liver imaging, hepatic AVMs on imaging, and no hepatic AVMs on imaging. We used a parametric t test or Fisher exact test to compare the presence of HHT complications between those with high and normal baseline ammonia levels. Analyses were not adjusted for multiple comparisons because a small number of nonoverlapping clinical events were evaluated. All data were analyzed with SAS version 9.4 (Cary, NC).
RESULTS
Forty-five patients in our HHT clinic met the criteria for definite HHT and underwent ammonia testing from September 2012 through February 2019. The mean age of the cohort was 52.7 years (SD 15.4, range 24–84 years). Nine patients (20.0%) never underwent genetic testing, 28 patients (62.2%) were tested, and the genetics of 8 patients (17.8%) were inferred based on family testing. When comparing patients with elevated ammonia to normal ammonia, there were more visceral AVMs in any organ in the elevated ammonia group (88.9% vs 59.3%, P < 0.05; Table 1). Twenty-seven patients (60%) had a normal ammonia levels, whereas 18 patients (40%) had ammonia levels elevated above the upper limit of the reference range (mean ammonia 71.9 vs 28.1, P < 0.0001). The elevated ammonia group had higher alkaline phosphatase (97.3 vs 76.1, P = 0.06) and AST (34.2 vs 23.9, P = 0.06) compared with the normal ammonia group. Otherwise, there were no significant differences between the normal and elevated ammonia groups, including in alanine transaminase, total bilirubin, hemoglobin, ferritin, and rates of recent overt gastrointestinal bleeding.
Table 1.
Clinical characteristics of patients with HHT at the time of ammonia testinga

Association of liver tests with the presence of hepatic AVMs
Twenty-five patients (56%) underwent dedicated liver imaging to evaluate for hepatic AVMs, 12 with ultrasound, 11 with MRI, and 8 with computed tomography; several patients underwent more than 1 hepatic imaging study. Of the patients who underwent dedicated liver imaging, 11 patients (44%) had evidence of hepatic AVMs on imaging, and 14 (56%) did not. Patients who underwent liver imaging did not differ from those who did not undergo liver imaging on any measured variable (see Supplementary Table 1, Supplementary Digital Content 1, http://links.lww.com/CTG/A165).
Of patients with HHT with an elevated ammonia level, 7/13 (54%) had hepatic AVMs on imaging. Of patients with HHT with a normal ammonia level, 4/12 (33%) had hepatic AVMs on imaging. In an ANOVA analysis, the ammonia level in those who did not undergo dedicated liver imaging was 36.6 compared with 45.6 in those with no hepatic AVMs on imaging and 62.1 in those with hepatic AVMs on imaging (P < 0.03; Figure 1). Patients without hepatic imaging were included, as they may represent a unique group in whom there was no suspicion of hepatic HHT involvement. AST or total bilirubin above the upper limit of normal had 100% specificity for hepatic AVMs on imaging, whereas ammonia had the highest sensitivity for a single test to predict hepatic AVMs at 64% (Table 2). The sensitivity of any abnormal liver test or ammonia for hepatic AVMs was 73%.
Figure 1.
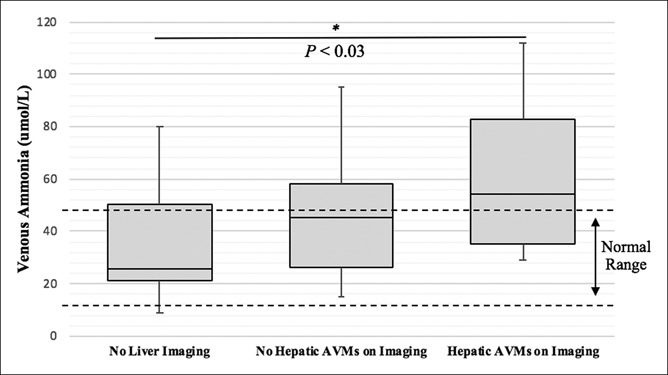
*The P value is derived from an ANOVA test comparing all 3 groups. AVM, arteriovenous malformation.
Table 2.
Ability of liver tests to predict the presence of hepatic AVMs on imaginga

Association of ammonia with hepatic encephalopathy and cholangitis
The cumulative duration of follow-up was 435 months in the elevated ammonia group and 424 months in the normal ammonia group. Over this follow-up duration, only 1 patient with HHT in the cohort developed hepatic encephalopathy, and none developed cholangitis after ammonia testing. The single patient who developed hepatic encephalopathy had an elevated baseline ammonia level, hepatic AVMs on MRI, and no other liver disease on imaging, laboratory testing, or gastroenterologist assessment. Because of only a single patient developing hepatic encephalopathy, there was insufficient statistical power to perform comparisons between those who did and did not develop encephalopathy.
Association of liver tests with cardiopulmonary outcomes
All 45 patients underwent TTE assessment of RVSP, and 43 patients underwent transthoracic contrast echocardiography to assess for pulmonary AVMs. Ammonia was higher in patients with HHT with an RVSP > 35 mm Hg than those with RVSP ≤ 35 mm Hg (62.1 vs 40.9, P = 0.02). Elevated ammonia had an 80% sensitivity and 71% specificity for predicting RVSP > 35 mm Hg (Table 3). The sensitivity of any abnormal liver test or ammonia for RVSP > 35 mm Hg was 90%. Elevated ammonia was not associated with a greater prevalence of grade 2–3 bubbles on transthoracic contrast echocardiography or a diagnosis of pulmonary AVMs (Table 4). Elevated ammonia was also not associated with other complications of HHT.
Table 3.
Ability of liver tests to predict the presence of elevated RVSP on transthoracic echocardiographya

Table 4.
Clinical outcomes of patients with hereditary hemorrhagic telangiectasia by ammonia levela

DISCUSSION
In a cohort of patients with hereditary HHT and baseline venous ammonia testing, 40% had elevated ammonia levels. Elevated ammonia was associated with the presence of hepatic AVMs and elevated RVSP, but no other complications of HHT, including hepatic encephalopathy.
Consensus guidelines and expert recommendations have previously recommended performing liver imaging to evaluate for HHT involvement in patients with elevated liver tests (1,3,8). Our study affirms these recommendations by showing that an elevated ammonia test was associated with hepatic HHT involvement on imaging. We found that the presence of any elevated liver test, including ammonia, is 73% sensitive for hepatic HHT involvement. Furthermore, we found that patients with HHT with an RVSP > 35 mm Hg had higher venous ammonia than those with lower RVSP and that elevated venous ammonia had an 80% sensitivity and 71% specificity for predicting RVSP > 35 mm Hg. Elevated RVSP is a marker of elevated right heart pressures, which can be found in pulmonary hypertension and high-output cardiac failure. As such, venous ammonia was not only associated with the presence of hepatic HHT involvement but also with the early stages of one of its most common and feared complications: high-output cardiac failure.
There is a plausible biological explanation for why venous ammonia is associated with hepatic HHT and predicts elevated right heart pressures. Ammonia is transported from the intestinal lumen to the liver via the portal vein and can enter the systemic circulation via shunts or collaterals. Therefore, elevated systemic venous ammonia in a patient with HHT may be a marker of portosystemic shunting via AVMs. Portosystemic shunting can increase preload delivery to the heart and increase right heart pressures. Venous ammonia can also be elevated in the setting of gastrointestinal bleeding, but there was no difference in hemoglobin or gastrointestinal bleeding between elevated and normal ammonia patients.
Portosystemic shunting has both chemical and mechanical consequences. Chemically, portosystemic shunting of ammonia and other intestinal products can lead to hepatic encephalopathy, which we only observed in our cohort once after a total 435 months of follow-up in the elevated ammonia group and 424 months of follow-up in the normal ammonia group. The mechanical consequences of shunting, however, lead ultimately to high-output cardiac failure. Although only 2 (4.4%) of our patients developed clinically apparent high-output cardiac failure, 10 (22.2%) had elevated right heart pressures on TTE, an earlier and more easily assessable outcome.
Most complications of HHT do not involve portosystemic shunting, such as the consequences of pulmonary, brain, and gastrointestinal AVMs. Not surprisingly, venous ammonia did not correlate with the presence of these AVMs or the need to intervene on them.
Our results must be interpreted within the context of study design. First, we do not know whether ammonia was obtained while fasting, which can impact test results. Second, our sensitivity and specificity analyses were not based on the gold standard of angiography, rather the hepatic imaging available for clinical use. However, Doppler ultrasound has been recommended as the ideal first-line assessment tool for hepatic HHT, and ultrasound was the most common modality in our study (17). Given the retrospective design and heterogeneous imaging modalities used, we could not comprehensively evaluate for every type of AVM for each patient, nor could we evaluate for minimal hepatic encephalopathy. In addition, most patients with elevated RVSP did not undergo right heart catheterization to confirm the presence or absence of high cardiac output. Like many other HHT studies, we were limited in our number of patients and the duration of follow-up, although the total number of patients included is respectable, given that we are evaluating a complication of a rare disease. A greater sample size and duration of follow-up is needed to understand the value of ammonia and other liver tests to predict high-output cardiac failure, a complication that can take years to manifest. Finally, hepatic imaging was not performed on every patient in this cohort, thus introducing potential bias. Future work should perform ammonia, hepatic panel, and hepatic imaging in an entire cohort of patients with HHT.
Given that it is an inexpensive and widely available assay, future longitudinal studies of HHT should consider inclusion of baseline ammonia and liver test assessment to better understand their prognostic value. The value of accurate screening tests will only improve with more widespread use of novel antiangiogenic agents to treat hepatic involvement and gastrointestinal bleeding in HHT (11,18–21). In the setting of a highly morbid disease, an inexpensive, sensitive screening test is particularly useful.
In conclusion, ammonia and liver biochemical testing may be useful to identify patients with HHT with hepatic AVMs and elevated right heart pressures. These tests may be valuable in determining which patients require dedicated liver imaging and echocardiography. Additional prospective studies with ammonia levels drawn under controlled conditions will be necessary to confirm our findings.
CONFLICTS OF INTEREST
Guarantor of the article: Jay Luther, MD.
Specific author contributions: P.P.B.: study concept and design, acquisition of data, analysis and interpretation of data, and drafting of the manuscript. J.R.-L. and A.S.W.: study concept and design, acquisition of data, and critical revision of the manuscript for important intellectual content. H.A. and D.J.K.: critical revision of the manuscript for important intellectual content. A.M.: acquisition of data and critical revision of the manuscript for important intellectual content. J.L.: study concept and design, acquisition of data, analysis and interpretation of data, critical revision of the manuscript for important intellectual content, and study supervision. All authors approved the final draft submitted.
Financial support: P.P.B. is supported by NIH T32 DK007191-43, recipient of an ACG Clinical Research Award, and the AASLD Fellow Ambassador Award. H.A. is the recipient of the National Hemophilia Foundation-Shire Clinical Fellowship, which provides partial salary support.
Potential competing interests: The authors have no conflicts relevant to the submitted work to report. Universal disclosures: P.P.B. and J.R.-L.: none. A.S.W.: Research funding (Actelion) and consultancy (Bayer). H.A.: Research funding (Agios and Dova) and consultancy (Agios, Dova, and Moderna). D.J.K.: Research funding (Protalex, Bristol-Myers Squibb, Rigel, Bioverativ, Agios, Syntimmune, Principia, and Alnylam) and consultancy (ONO, Pfizer, 3SBios, Eisai, GlaxoSmithKline, Genzyme, Shire, Alexion, Amgen, Shionogi, Rigel, Syntimmune, MedImmune, Novartis, Bioverativ, Argenx, and Zafgen). A.M. and J.L.: none.
Study Highlights.
WHAT IS KNOWN
✓ HHT commonly has hepatic involvement.
✓ Hepatic HHT can lead to high-output cardiac failure and encephalopathy.
WHAT IS NEW HERE
✓ Elevated ammonia is associated with hepatic HHT involvement.
✓ Ammonia predicts the development of pulmonary hypertension in HHT.
✓ Ammonia does not seem to predict development of encephalopathy in HHT.
TRANSLATIONAL IMPACT
✓ Ammonia may serve as a useful biomarker in trials of novel antiangiogenic agents and other therapies for HHT.
Supplementary Material
Footnotes
SUPPLEMENTARY MATERIAL accompanies this paper at http://links.lww.com/CTG/A165
REFERENCES
- 1.Felli E, Addeo P, Faitot F, et al. Liver transplantation for hereditary hemorrhagic telangiectasia: A systematic review. HPB (Oxford) 2017;19(7):567–72. [DOI] [PubMed] [Google Scholar]
- 2.Sopeña B, Pérez-Rodríguez MT, Portela D, et al. High prevalence of pulmonary hypertension in patients with hereditary hemorrhagic telangiectasia. Eur J Intern Med 2013;24(3):e30–4. [DOI] [PubMed] [Google Scholar]
- 3.Faughnan ME, Palda VA, Garcia-Tsao G, et al. International guidelines for the diagnosis and management of hereditary haemorrhagic telangiectasia. J Med Genet 2011;48(2):73–87. [DOI] [PubMed] [Google Scholar]
- 4.Garcia-Tsao G. Liver involvement in hereditary hemorrhagic telangiectasia (HHT). J Hepatol 2007;46(3):499–507. [DOI] [PubMed] [Google Scholar]
- 5.Buscarini E, Leandro G, Conte D, et al. Natural history and outcome of hepatic vascular malformations in a large cohort of patients with hereditary hemorrhagic teleangiectasia. Dig Dis Sci 2011;56(7):2166–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Shovlin CL, Buscarini E, Kjeldsen AD, et al. European reference network for rare vascular diseases (VASCERN) outcome measures for hereditary haemorrhagic telangiectasia (HHT). Orphanet J Rare Dis 2018;13(1):136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Buscarini E, Plauchu H, Garcia Tsao G, et al. Liver involvement in hereditary hemorrhagic telangiectasia: Consensus recommendations. Liver Int 2006;26(9):1040–6. [DOI] [PubMed] [Google Scholar]
- 8.Vorselaars VM, Velthuis S, Snijder RJ, et al. Pulmonary hypertension in hereditary haemorrhagic telangiectasia. World J Cardiol 2015;7(5):230–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Garcia-Tsao G, Korzenik JR, Young L, et al. Liver disease in patients with hereditary hemorrhagic telangiectasia. N Engl J Med 2000;343(13):931–6. [DOI] [PubMed] [Google Scholar]
- 10.Andrejecsk JW, Hosman AE, Botella LM, et al. Executive summary of the 12th HHT international scientific conference. Angiogenesis 2018;21(1):169–81. [DOI] [PubMed] [Google Scholar]
- 11.Dupuis-Girod S, Ginon I, Saurin JC, et al. Bevacizumab in patients with hereditary hemorrhagic telangiectasia and severe hepatic vascular malformations and high cardiac output. JAMA 2012;307(9):948–55. [DOI] [PubMed] [Google Scholar]
- 12.Wu JS, Saluja S, Garcia-Tsao G, et al. Liver involvement in hereditary hemorrhagic telangiectasia: CT and clinical findings do not correlate in symptomatic patients. AJR Am J Roentgenol 2006;187(4):W399–405. [DOI] [PubMed] [Google Scholar]
- 13.Nathan SD, Shlobin OA, Barnett SD, et al. Right ventricular systolic pressure by echocardiography as a predictor of pulmonary hypertension in idiopathic pulmonary fibrosis. Respir Med 2008;102(9):1305–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gossage JR. Role of contrast echocardiography in screening for pulmonary arteriovenous malformation in patients with hereditary hemorrhagic telangiectasia. Chest 2010;138(4):769–71. [DOI] [PubMed] [Google Scholar]
- 15.Gazzaniga P, Buscarini E, Leandro G, et al. Contrast echocardiography for pulmonary arteriovenous malformations screening: Does any bubble matter? Eur J Echocardiogr 2009;10(4):513–8. [DOI] [PubMed] [Google Scholar]
- 16.van Gent MWF, Post MC, Snijder RJ, et al. Grading of pulmonary right-to-left shunt with transthoracic contrast echocardiography: Does it predict the indication for embolotherapy? Chest 2009;135(5):1288–92. [DOI] [PubMed] [Google Scholar]
- 17.Buscarini E, Gandolfi S, Alicante S, et al. Liver involvement in hereditary hemorrhagic telangiectasia. Abdom Radiol (NY) 2018;43(8):1920–30. [DOI] [PubMed] [Google Scholar]
- 18.Krowka MJ, Wiesner RH, Heimbach JK. Pulmonary contraindications, indications and MELD exceptions for liver transplantation: A contemporary view and look forward. J Hepatol 2013;59(2):367–74. [DOI] [PubMed] [Google Scholar]
- 19.Chavan A, Luthe L, Gebel M, et al. Complications and clinical outcome of hepatic artery embolisation in patients with hereditary haemorrhagic telangiectasia. Eur Radiol 2013;23(4):951–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Al-Samkari H, Kritharis A, Rodriguez-Lopez JM, et al. Systemic bevacizumab for the treatment of chronic bleeding in hereditary haemorrhagic telangiectasia. J Intern Med 2019;285(2):223–31. [DOI] [PubMed] [Google Scholar]
- 21.Kritharis A, Al-Samkari H, Kuter DJ. Hereditary hemorrhagic telangiectasia: Diagnosis and management from the hematologist's perspective. Haematologica 2018;103(9):1433–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.