

Abstract
Successful longevity is achieved when individuals can continue to plan, pursue, and reach their goals across the lifespan. However, normative age-related impairments can make goal attainment more difficult, unless there are interventions to mitigate such changes. Behavioral interventions that use technology are increasing in frequency. I outline a hierarchy of approaches to mitigating impairments. The first strategy to promote successful longevity is prevention of normative age-related decline. When impairments develop, they can be addressed by rehabilitation, augmentation, and substitution approaches.
The purpose of this essay is to offer a framework to guide intervention research, particularly ways to structure technology-based interventions that will increase their acceptability by aging adults. I start by outlining two important trends that highlight the challenges and potential benefits for technology-based interventions.
Societies are being challenged by two broad trends: rapid introduction and dissemination of technology, particularly information and communication technology (ICT), such as computer and mobile phone technologies, as well as the rapid aging of the population, driven by increased longevity and decreased fertility (1,2). Unsurprisingly, technology also plays an important role in promoting population aging by enhancing food production and distribution, efficacy of and access to healthcare services, and improving fertility control. However, there is also a significant age-related lag in technology adoption that means that aging adults are among the least likely segment of the population to benefit from technology advances.
Technology Adoption and Age.
For adoption of ICT in adulthood the trends are quite consistent and powerful: earlier born cohorts lag later ones (3,4, 5) and such lags are replicated across countries. Figure 1 shows internet access in the past month by age group and year averaged across more than 20 countries in the European Union. It shows striking age/cohort gradients and impressive increases for older cohorts over the nine-year interval, though the youngest cohorts are constrained in growth by their nearness to asymptote of 100%.
Fig. 1.
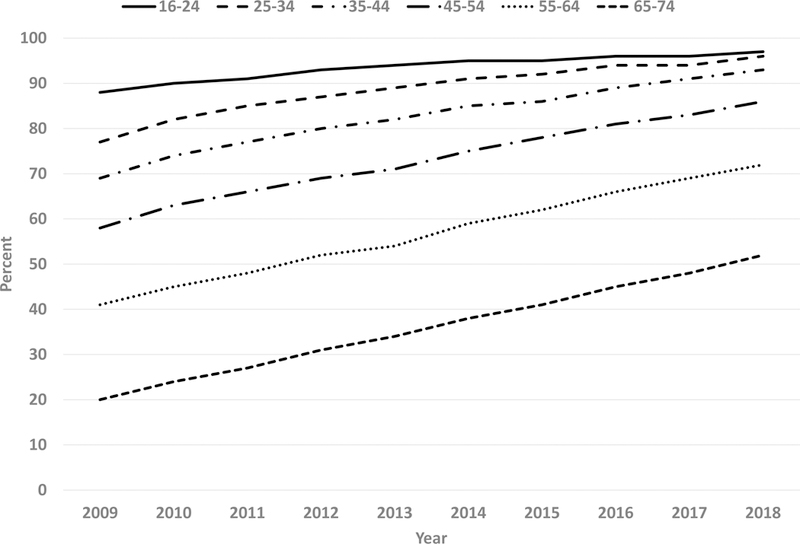
Percent persons with weekly or higher Internet access in the European Union Countries by age group (16–24, 25–34, 35–44, 45–54, 55–64, 65–74) and year (2009–2018). Data from Eurostat, available from http://appsso.eurostat.ec.europa.eu/nui/submitViewTableAction.do
In early 2018 in the United States, 94% of 18–29-year-olds owned smartphones, compared to 46% of those age 65+ years (http://www.pewinternet.org/fact-sheet/mobile/). There are many potential reasons for this ICT adoption lag (4) including cost and knowledge barriers, familiarity differentials in part because earlier born cohorts left the workforce before widespread introduction of ICT, design of ICT systems that ignores normative changes in abilities with age (2), and the fact that learning cost accelerates as people age, with older adult novice learners in their 70s taking twice as long as younger ones in their 20s to acquire skill using such systems (6).
Benefits and Costs of Technology.
Technology enables greater productivity in work environments, in part through education, increasing human capital and societal wealth in the form of added goods and services. It also enables potentially greater social connectivity, improving human social capital. As an example of the former, think of idea dissemination. A clerk in the 19th century equipped with paper, a quill, and an inkwell would be no match for a clerk in the 20th century equipped with a computer and a printer, who probably was even less capable than a worker in the 21st century with a smartphone and access to social media. However, technology may also serve as a multiplier force (8) that widens the wealth gap between those schooled in its use and those unable to access it. Further there is controversy over whether technology helps or hurts integration into society.
The story on social media technology as supporting social capital formation and improving wellbeing is still not clear at the level of association investigations. A large-scale representative study of adolescents showed that amount of social media technology use seems to be slightly negatively related to wellbeing, accounting for 0.4% of variance (8). When it comes to showing technology-enhanced social relationship benefits for aging adults, there are relatively few investigations because of the age-related “digital divide” for ICT use, wherein older users are atypical of their cohort. This may be partly mediated by the finding across all age cohorts that higher SES leads to higher ICT use. Using population-representative HRS data, Cotten, Ford and Hale (9) showed less depression in older internet users. In a convenience sample, Sims, Reed, and Carr (10) showed that for ICT users age 80+ wellbeing was related to higher ICT use.
However, randomized clinical trial studies with community-dwelling adults have found either no effects (11), or modest positive effects of technology training and deployment on wellbeing (5). To echo the 1987 quip of Nobel economist Robert Solow, “you can see the computer age everywhere but in the productivity statistics”, I can say that we see gains for ICT everywhere but in wellbeing. Like the case for computer technology adoption and productivity, any gains will likely lag ICT diffusion until users climb the learning curve for efficient use. Interventions for caregivers do seem to provide moderate positive benefits for mental health (12). Despite the uncertainty over efficacy, technology-based behavioral interventions are apparently increasing.
Technology Intervention increases
The clinicaltrials.gov web site is approaching 20 years of existence, having opened to the public in Feb. 2000 (https://clinicaltrials.gov/ct2/about-site/history). The site indicates that you can “Explore 294,925 research studies in all 50 states and 207 countries” (as of Jan. 21, 2019). A search for “behavioral clinical trial and technology” on clinicaltrials.gov found 819 trials that have ever been registered for those age 18–64 and 65+. If behavioral trials involving technology were starting evenly across the 19 years and if each lasted about a year you would expect about 819/19 = 43 trials currently active in any year. Assume that after initial registration (in the year 2000) a study takes about 3 years to complete recruiting and running. So, you would estimate about 130 trials ongoing in a given year with constant initiation per year. Filtering the 819 trials returns 255 trials (31%) that are in a stage of not yet recruiting or recruiting, hence ongoing, roughly twice the number expected for constant deployment of behavioral technology trials. Filtering further finds most of those, 195 (76%), are planning to recruit people age 65+ years. Behavioral trials involving technology interventions with aging adults are clearly increasing in frequency.
Given the ubiquity of ICT in almost every sphere of life, do technology interventions represent a special case for intervention research? Here I argue that they are special in one respect, their ability to provide adaptive interventions. One of the characteristic features of ICT devices, those systems containing microprocessors (and radios), is that they are programmable: they can change their interactions with the world depending on the programs that they run and the inputs they receive. One major advantage to computer-based training/interventions is that a program can adapt to the user’s current level of performance, offering them graded challenges to promote maximal change (13). For rehabilitation, such personalized training may optimize individual outcomes, fitting in with the trend toward pragmatic clinical trials that avoid a one-size-fits-all intervention strategy. Still, if aging adults are reluctant to adopt ICT, empirical demonstrations of efficacy may not be enough to prompt adoption and use.
Technological advances have significant potential to support successful longevity, sometimes termed successful aging (14). For instance, technology can assist in part by compensating for normative age-related declines in perceptual, cognitive, and psychomotor performance. Intervention studies, such as Advanced Cognitive Training for Independent and Vital Elderly (ACTIVE) (15), and others (16) have shown promise in modifying aging adult cognitive abilities directly (e.g., through speed of processing training) though such studies suffer from significant weaknesses that make it difficult to conclude that they improve everyday performance (17). Further, the cost of computing technology is dropping accompanied by enormous increases in processor capability (18) making potential ITC products both more capable and less expensive, hence more accessible to aging adults.
Why Intervene? Aging as Deficit
Although it is certainly not a full description of the balance between gains and losses associated with aging (19), normatively, people show consistent declines in bodily and brain functions with increased adult age (20). Normatively-developing chronic conditions dominate the second half of the life-span with about half of those age 45–64 years old and over 80% of the US population age 65+ years suffering from multiple chronic conditions compared to less than 7% of those age 17 or younger (21). Some of the developing chronic conditions are clearly behaviorally and environmentally influenced, for instance, adult onset (type 2) diabetes is associated with too much food intake and too little exercise. However, it has been known for many years that even in athletes, maximum heart rate shows robust age-related decline (22). As a result, even for those who devote significant effort to building up physical stamina through exercise and diet, masters athletes, world record performances are robustly related to age (http://www.mastersathletics.net/index.php?id=masters). Nonetheless, there are striking individual differences in physiological functioning as a function of age, such as in ventilatory capacity (v02max) between athletes and non-athletes.
Thus, there exists considerable plasticity in aging bodies and brains, though reducing with age, and deliberate practice can boost performance enormously for many tasks (23). Athletes represent a special case of a “testing-the-limits” (24, 25) approach to interventions given the enormous number of hours that they invest in self-improvement on relatively “simple” tasks such as running quickly. Despite this plasticity, the best 90-year-old runner is unlikely to ever be competitive with the best 20-year-old runner at a 100-meter race without either some very sophisticated genetic engineering or bionic assistance. It needs to be acknowledged, however, that there have been huge secular gains in performance. For instance, the current masters’ world record in the 100 m run for a 60-year-old male, 11.7 s, set in Athens, Greece in 1994, is faster than that for the fastest runner (12 s) in the first modern Olympic games staged in 1896. When it comes to world record performance for the 100 m race, one could claim that age sixty is the new twenty.
One can observe similar declines in function longitudinally in cognitive domains, such as chess playing performance indexed by Elo rating (26, 27). Such declines are occurring against a backdrop of generational gains in some aspects of cognition, for instance, fluid ability performance: the Flynn effect (28, 29). Nonetheless, generational gains are not ubiquitous; for instance, there may be losses in vocabulary size for more recent compared to older cohorts (30).
That declining function should occur with increased age past maturity is unsurprising, whether from the point of view of a physical system undergoing the entropy increase predicted by the second law of thermodynamics, or a biological system undergoing degradation by environmentally-induced insults to cell and organ systems resulting in cell mutation, senescence, and apoptosis. Otherwise gerontology might not exist as a discipline. It is important to note that there are also gains in wellbeing measures associated with increased age in adulthood (31), gains in median usual weekly earnings into the 50s for full-time workers in the United States (32), and perhaps, increased sense of meaning in life into middle age (31) and early old age (33).
Given the normative nature of functional decline with increasing age, how might technology contribute to supporting successful longevity? We can define successful longevity as occurring when a person can set, pursue, and (hopefully) achieve their goals across their lifespan, however long or short (e.g., https://isl.fsu.edu/blog/2015/03/24/directors-blog-successful-longevity/). Before assigning a role to technology, we first need to develop a framework for choosing among different types of interventions.
The PRAS framework for selecting the type of intervention
The aim of an intervention is to change functional capacity to enhance performance, be it vision, cognition, or psychomotor functioning (e.g., dexterity), thereby enabling people to reach important personal goals. I suggest that there should be a hierarchy of approaches ranging from prevention of functional decline, to changing the person, to changing the available tools and the environment. In this respect, I am taking inspiration from the World Health Organization (WHO) model of functioning and disability (https://www.cdc.gov/nchs/data/icd/icfoverviewfinalforwho10sept.pdf ) that notes that functional ability depends on both a person’s capabilities and the characteristics of the surrounding environment. I am also drawing on the framework of the role of environmental support developed in human factors engineering (34) that stresses how aspects of the task environment mediate the relationship between ability levels and human performance.
The hierarchy includes 1) Prevention, 2) Rehabilitation 3) Augmentation, and 4) Substitution (PRAS), as seen in Figure 2. Note that these alternative approaches are not mutually exclusive. Even substitution probably requires training in the use of a prosthesis, a form of rehabilitation.
Fig. 2.

The Prevent, Rehabilitate, Augment, Substitute (PRAS) hierarchy for technology interventions to promote successful longevity. Prevention of impairment should be the base strategy. Should impairments develop those who design technology products and interventions should prefer to (1) rehabilitate function, and failing that (2) augment function, and failing that (3) substitute for lost function.
Prevention of functional loss is the first line of defense for entering old age in the best possible shape. Take the case of hearing acuity, with a known, steep age-related decline function (35). The recent introduction of ear protective equipment in work places with high intensity sound sources (e.g., aircraft docking areas, manufacturing plants) along with the decline of noisy manufacturing work and the rise of quieter office work may account for the finding that recent birth cohorts have better hearing at older ages than less recent ones (36). Similarly, increased education levels in the population, possibly building up cognitive reserve (37), may be responsible for recently identified declines in dementia prevalence (38). Education is a powerful tool for helping people change behaviors and avoid preventable age-related losses in functioning. However, when inevitable age-related declines occur, if people wish to surmount those declines, intervention strategies need to be chosen. For least intrusive to most intrusive, from the perspective of altering a human body, they fall along the continuum of rehabilitation to augmentation to substitution.
Rehabilitation represents the case where, following a loss or precipitous decline of functional ability, training exercises successfully strengthen and restore partial or full function. A common case with increased age is the occurrence of a stroke (infarct or bleed) that results in loss of brain tissue and function (e.g., motor function, such as the ability to raise your arm, or cognitive function such as speech production loss). Training can sometimes restore at least partial functional ability (e.g., by recruiting other parts of the brain to take over the function of the damaged brain tissue). The same reorganization mechanism, in less stark form, can be seen with age-related loss of cognitive ability, where the brain compensates for declining function by recruiting contralateral tissue (e.g., using both hemispheres) for a task that was once accomplished unilaterally in one hemisphere (39).
Augmentation represents the case of compensating for an impairment by providing additional capacity. A good example is eyewear, glasses with corrective lenses, that transparently correct faulty visual functioning allowing someone to scan the environment with high visual acuity. The visual system is still functioning but augmenting light-bending capability in front of the eye enhances focus capability and hence visual functioning.
Finally, substitution is the most extreme solution to loss of function. If hair cells in the cochlea die or lose function, normal hearing becomes impossible as these cells are a critical piece of the chain conducting complex sound waves from eardrum to the auditory nerve and into other brain regions. The only way to restore hearing in such cases is with a cochlear implant that bypasses the hair cells and transmits sound vibration information by directly stimulating auditory nerve fibers. The cochlear implant substitutes for hair cells, somewhat imperfectly with present technology, but permits some auditory information to be transmitted to the appropriate brain regions. A much more common medical procedure, cataract surgery, substitutes a plastic or glass lens for a natural eye lens that is partially obscured by opaque regions that form on or in the lens capsule. That procedure, when successful, can significantly improve or completely restore clear vision.
Why argue for a hierarchy of interventions? Although I haven’t done the experiment, I am quite confident that when people are given the choice between a short period of rehabilitation or substitution, with both guaranteeing restored function, they would prefer rehabilitation to maintain their sense of self. Substitution is probably a last choice unless people are quite time-pressured and can’t engage in rehabilitation or augmentation. Similarly, when choosing between rehabilitation and augmentation, for instance, training to enhance balance versus using a cane or walker to avoid falls and improve mobility, I am confident that most aging individuals will choose the option that renders them “whole”. The stigma of being perceived as impaired is a well-known inhibitor of assistive device adoption and use (40).
However, in line with affirming the value of self-determination, all options should be available. Also, there is evidence that time demand can be a significant dimension for decision making and old age is perceived as a period of life with a short time horizon ahead (41). People may be willing to adopt a technological aid to augment their capabilities, such as learning to use a mobile device to provide reminders, rather than engaging in prolonged training that might marginally improve functioning such as extensive “brain training” to improve prospective memory.
Summary
We are at an inflection point where technology seems increasingly likely to meet lofty expectations for improving quality of life for our aging populations. Technology is becoming more sophisticated (e.g., artificial intelligence tools such as convolutional neural networks) and less expensive. Aging adults, on balance, are still experiencing significant functional decline, including cognitive decline, and they are still falling behind in technology adoption, experiencing a digital divide. For technology to fulfill its promise, it needs to be developed and deployed thoughtfully, keeping in mind aging adult capabilities (2). The PRAS hierarchy introduced here presents one way to categorize and choose among interventions.
2.1. Acknowledgments
2.3 Funding Sources
This work was supported by a grant from the National Institutes of Health/National Institute on Aging, under the auspices of the Center for Research and Education on Aging and Technology Enhancement (CREATE), 4 P01 AG 17211
Footnotes
2.2 Disclosure Section.
The author has no conflicts of interest to declare.
3. References
- 1.Foreword Charness N.. In Kwon S editor Gerontechnology: Research, practice, and principles in the field of technology and aging (pp xxvii–xxix). New York: Springer; ISBN: 978–0-8261–2888-1, 2016. [Google Scholar]
- 2.Czaja SJ, Boot WR, Charness N, & Rogers WA. Designing for older adults: Principles and creative human factors approaches 3rd ed Boca Raton: CRC Press; 2019. [Google Scholar]
- 3.Anderson M, & Perrin A. Technology use among seniors. Pew Research Center, May 2017, “Tech Adoption Climbs Among Older Adults”. Available from http://assets.pewresearch.org/wp-content/uploads/sites/14/2017/05/16170850/PI 2017May17 Older-Americans-Tech FINAL.pdf [Google Scholar]
- 4.Charness N, & Boot WR. Technology, Gaming, and Social Networking In Schaie KW & Willis SL editors. The Handbook of the Psychology of Aging 8th edition., Chapter 20 (pp. 390–407). London, UK: Academic Press/Elsevier; 2016. [Google Scholar]
- 5.Czaja SJ, Boot WR, Charness N, Rogers WA, & Sharit J. Improving social support for older adults through technology: Findings from the PRISM randomized control trial. Gerontologist. 2017. May 8;58(3):467–477. doi: 10.1093/geront/gnw249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Charness N, Kelley CL, Bosman EA, & Mottram M. Word processing training and retraining: Effects of adult age, experience, and interface. Psychol Aging. 2001. March;16(1):110–27. [DOI] [PubMed] [Google Scholar]
- 7.Charness N Technology as multiplier effect for an aging work force In Schaie KW & Abeles R editors. Social structures and aging individuals: Continuing challenges (pp. 167–192). New York: Springer, 2008. [Google Scholar]
- 8.Orben A, & Przybylski AK. The association between adolescent well-being and digital technology use. Nature Human Behaviour. 2019, 10.1038/s41562-018-0506-1 [DOI] [PubMed] [Google Scholar]
- 9.Cotton SR, Ford G, Ford S, & Hale TM. Internet use and depression among retired older adults in the United States: A longitudinal analysis. J Gerontol B Psychol Sci Soc Sci. 2014. September;69(5):763–71. doi: 10.1093/geronb/gbu018. [DOI] [PubMed] [Google Scholar]
- 10.Sims T, Reed AE, & Carr DC. Information and communication technology use is related to higher well-being among the oldest-old. J Gerontol B Psychol Sci Soc Sci. 2017. September 1;72(5):761–770. doi: 10.1093/geronb/gbw130. [DOI] [PubMed] [Google Scholar]
- 11.Slegers K, van Boxtel MPJ, & Jolles J. Effects of computer training and Internet usage on the well-being and quality of life of older adults: A randomized, controlled study. J Gerontol B Psychol Sci Soc Sci. 2008. May;63(3):P176–84. [DOI] [PubMed] [Google Scholar]
- 12.Sherifali D, Ali MU, Ploeg J, Markle-Reid M, Valaitis R, Bartholomew A, Fitzpatrick-Lewis D, & McAiney C. (2018). Impact of Internet-Based Interventions on Caregiver Mental Health: Systematic Review and Meta-Analysis. J Med Internet Res. 2018 July 3;20(7):e10668. doi: 10.2196/10668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lövdén M, Bäckman L, Lindenberger U, Schaefer S, & Schmiedek F. A theoretical framework for the study of adult cognitive plasticity. Psychol Bull. 2010. July;136(4):659–76. doi: 10.1037/a0020080. [DOI] [PubMed] [Google Scholar]
- 14.Editorial. Successful Aging: Contentious Past, Productive Future. Gerontologist. 2015. February;55(1):1–4. doi: 10.1093/geront/gnv002. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ball K, Berch DB, Helmers KF, et al. Effects of cognitive training interventions with older adults: a randomized controlled trial. JAMA. 2002;288(18):2271–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mahncke HW, Connor BB, Appelman J, Ahsanuddin ON, Hardy JL, Wood RA, Joyce NM, Boniske T, Atkins SM, & Merzenich MM. Memory enhancement in healthy older adults using a brain plasticity-based training program: a randomized, controlled study. Proc Natl Acad Sci U S A. 2006. August 15;103(33): 12523–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Simons DJ, Boot WR, Charness N, Gathercole SE, Chabris CF, Hambrick DZ, & Stine-Morrow EAL. Do “Brain Training” programs work? Psychol Sci Public Interest. 2016. October;17(3):103–186. [DOI] [PubMed] [Google Scholar]
- 18.National Research Council. 2011. The Future of Computing Performance: Game Over or Next Level? Washington, DC: The National Academies Press; Available from 10.17226/12980. [DOI] [Google Scholar]
- 19.Baltes PB. The aging mind: Potential and limits. Gerontologist. 1993. October;33(5):580–94. [DOI] [PubMed] [Google Scholar]
- 20.Schaie KW & Willis SL. Editors. The Handbook of the Psychology of Aging 8th edition London, UK: Academic Press/Elsevier; 2016. [Google Scholar]
- 21.Gerteis J, Izrael D, Deitz D, LeRoy L, Ricciardi R, Miller T, & Basu J. (2014). Multiple chronic conditions chartbook AHRQ Publications No, Q14–0038. Rockville, MD: Agency for Healthcare Research and Quality; April 2014 Available from http://www.ahrq.gov/sites/default/files/wysiwyg/professionals/prevention-chronic-care/decision/mcc/mccchartbook.pdf [Google Scholar]
- 22.Heath GW, Hagberg JM, Ehsani AA, Holloszy JO. A physiological comparison of young and older endurance athletes. J Appl Physiol Respir Environ Exerc Physiol. 1981. September;51(3):634–40. [DOI] [PubMed] [Google Scholar]
- 23.Krampe RT, & Charness N. Aging and Expertise In Ericsson KA, Hoffman R, Kozbelt A, & Williams M editors. Cambridge Handbook on Expertise and Expert Performance, 2nd Edition (pp. 835–856). Cambridge, UK: Cambridge University Press; 2018. [Google Scholar]
- 24.Baltes PB, & Kliegl R. Further testing of limits in cognitive plasticity: Negative age differences in a mnemonic skill are robust. Developmental Psychology. 1992; 28: 121–125. 10.1037/0012-1649.28.1.121 [DOI] [Google Scholar]
- 25.Kliegl R, Smith J, & Baltes PB. Testing-the-limits and the study of adult age differences in cognitive plasticity of a mnemonic skill. Developmental Psychology. 1989; 25: 247–256. [Google Scholar]
- 26.Roring RW, & Charness N. A multilevel model analysis of expertise in chess across the lifespan. Psychol Aging. 2007. June;22(2):291–9. [DOI] [PubMed] [Google Scholar]
- 27.Vaci N, Bartosz G, & Bilalic M. Is age really cruel to experts? Compensatory effects of activity. Psychol Aging. 2015. December;30(4):740–54. doi: 10.1037/pag0000056. [DOI] [PubMed] [Google Scholar]
- 28.Fox MC, & Mitchum AL. (2013). A knowledge-based theory of rising scores on “culture-free” tests. J Exp Psychol Gen. 2013 August;142(3):979–1000. doi: 10.1037/a0030155. [DOI] [PubMed] [Google Scholar]
- 29.Trahan L, Stuebig KK, Hiscock MK, & Fletcher JM. The Flynn Effect: A Meta-analysis. Psychol Bull. 2014. September;140(5):1332–60. doi: 10.1037/a0037173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ben-David BM, Erel H, Goy H, & Schneider BA. “Older Is always better”: Age-related differences in vocabulary scores across 16 years. Psychol Aging. 2015. December;30(4):856–62. doi: 10.1037/pag0000051. [DOI] [PubMed] [Google Scholar]
- 31.Ryff CD. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. Journal of Personality and Social Psychology. 1989; 57(6), 1069–1081. 10.1037/0022-3514.57.6.1069 [DOI] [Google Scholar]
- 32.Charness N Can Acquired Skill and Technology Mitigate Age-Related Declines in Learning Rate? In Czaja SJ, Sharit J & James J, editors. Current and emerging trends in aging and work. New York: Springer; 2019. [Google Scholar]
- 33.Steger MF, Oishi S, & Kashdan TB. (2009). Meaning in life across the life span: Levels and correlates of meaning in life from emerging adulthood to older adulthood. The Journal of Positive Psychology, 4 (1), 43–52. DOI: 10.1080/17439760802303127 [DOI] [Google Scholar]
- 34.Morrow DG & Rogers WA. Environmental support: An integrative framework. Hum Factors. 2008. August;50(4):589–613. [DOI] [PubMed] [Google Scholar]
- 35.Fozard JL. Vision and hearing in aging In Birren JE & Schaie KW editors. Handbook of the psychology of aging 3rd edition pp. 150–170. San Diego: Academic Press; 1990. [Google Scholar]
- 36.Hoffman HJ, Dobie RA, Losonczy KG, Themann CLO, & Flamme GA. (Declining prevalence of hearing loss in US adults aged 20 to 69 years. JAMA Otolaryngol Head Neck Surg. 2017. March 1;143(3):274–285. doi: 10.1001/jamaoto.2016.3527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Stern Y Cognitive reserve in ageing and Alzheimer’s disease. Lancet Neurol. 2012. Nov; 11(11): 1006–1012.doi: 10.1016/S1474-4422(12)70191-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Langa KM, Larson EB, Crimmins EM, Faul JD, Levine DA, Kabeto MU, & Weir DR. (2017). A comparison of the prevalence of dementia in the United States in 2000 and 2012. JAMA Internal Medicine, 177 (1), 51–58. doi: 10.1001/jamainternmed.2016.6807 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Cabeza R Hemispheric asymmetry reduction in older adults: the HAROLD model. Psychol Aging. 2002. March;17(1):85–100. [DOI] [PubMed] [Google Scholar]
- 40.Gitlin LN. Why older people accept or reject assistive technology. Generations;1995. Spring95, Vol. 19 Issue 1, 41–47. [Google Scholar]
- 41.Carstensen LL, Isaacowitz DM, & Charles ST. Taking time seriously: A theory of socioemotional selectivity. Am Psychol. 1999. March;54(3):165–81. [DOI] [PubMed] [Google Scholar]