

Abstract
Background:
Flow 800 is microscope-integrated analytical visualization tool which analyses the indocyanine green (ICG) video sequence and converts it into an intensity diagram. This allows an objective evaluation of the result rather than subjective assessment of ICG fluorescence. The anatomy of anterior communicating artery region is complex because of multiple vessels and perforators in small space; hence, there is a need of objective assessment tool which can give precise idea about vascular compromise. Flow 800 can serve as a valuable tool in this complex surgery.
Objective:
The objective of this study was to evaluate the utility of microscope-integrated fluorescent ICG videoangiography (Flow 800) in A-com aneurysm surgery.
Materials and Methods:
We used Flow 800 in ten consecutive patients of A-com aneurysm surgery from July 2019 to October 2019. We studied patient characteristics, intraoperative observation of ICG and Flow 800, and corresponding changes made in the operative decisions.
Results:
The use of Flow 800 helped in intraoperative decision of four out of ten patients of A-com aneurysm. In two patients, incomplete clipping was confirmed with Flow 800 and the second clip was applied. In the third patient, perforator compromise was found hence needed clip readjustment, whereas in the fourth patient, ICG was inconclusive and Flow 800 confirmed complete clipping of aneurysm.
Conclusion:
Flow 800 is a conclusive reproducible and objective tool for early detection of vascular compromise of multiple vessels and perforators in A-com aneurysm surgery. It gives a better idea of vasculature, especially where ICG is ambiguous or inconclusive.
Keywords: A-com aneurysm surgery, Flow 800, indocyanine green
Introduction
The goal of successful aneurysm surgery is a complete clipping of aneurysm sac and prevention of vascular compromise. Neurosurgeons traditionally rely on direct inspection of cerebral vessels to detect vascular compromise; however, visual inspection can miss many things. Intraoperative use of digital subtraction angiography (DSA) is a method of choice for intraoperative diagnosis of vessel patency; however, its use is time and resource consuming. Its routine use in unselected cases is unrealistic.[1]
Raabe et al.[2] published their experience in 2003 about the use of indocyanine green videoangiography (ICG-VA) during vascular surgery. They used intraoperative ICG for 21 times in 14 patients, and they got good quality and spatial resolution images allowing intraoperative real-time assessment of cerebral circulation in total 17 cases. In all cases, the postoperative angiographic results correspond to the intraoperative ICG videoangiographic findings. In three cases, the information provided by intraoperative ICG angiography significantly changed the surgical procedure. Intraoperative use of ICG-VA is well established now in vascular neurosurgery. Potential drawbacks of conventional ICG-VA are that it can assess only the vasculature directly within the field of view; it is subjective and lacks any quantitative interpretation of imaging data.[3]
Flow 800 is a surgical microscope-integrated software program that allows semi-quantitative analysis of ICG data through fluorescence dynamics.[4] Flow 800 data are objective and reproducible, whereas ICG data are susceptible to subjective interpretation. Anterior communicating artery anatomy is very complex with multiple vessels; hence, it is better to have objective investigation like Flow 800 for surgery in this region. To our knowledge, there are very few papers describing the use of Flow 800 in A-com aneurysm surgery. We present our experience with the use of Flow 800 in A-com aneurysm surgery.
Materials and Methods
We selected ten serial cases of A-com aneurysms (all were unruptured aneurysms) which were operated between July 2019 and October 2019 in Bantane Hospital, Fujita Health University, Japan, and we used Flow 800 during surgery. All patients were preoperatively investigated with either computed tomography angiography or DSA. Informed consents were taken prior to surgery, and previous anaphylactic reactions to contrast dye were ruled out. During surgery after aneurysm was visualized, ICG angiography using near-infrared video camera was performed with an intravenous bolus of 0.25 mg/kg ICG dye diluted in 5 ml of distilled water with a saline flush. The Flow 800 color coding of the ICG videos was obtained using software integrated into the operating microscope (Kinevo, Carl Zeiss Co., Oberkochen, Germany). The vessel and the aneurysm were color coded, and their fluorescence intensity (y-axis) was plotted over time (x-axis). The entire process was completed within a few seconds and was available for interpretation by a surgical team.
Results
We performed ICG-VA before clipping of aneurysm in all the ten patients. The minimal interval between two consecutive procedures was 5 min. None of the patients had any adverse effects related to the ICG dye. Flow 800 was generated after ICG and then clipping was performed. After clipping, again, ICG-VA was repeated and Flow 800 data were generated. Pre- and postclipping ICG-VA and Flow 800 data were analyzed, and the following observations were made [Table 1].
Table 1.
Observation on Flow 800
| Age (years) | Sex | Size of aneurysm (mm) | Observation on flow 800 | Change in operative plan |
|---|---|---|---|---|
| 1. 47 | Male | 5 | Complete clipping of aneurysm | No change |
| 2. 71 | Female | 7 | Atherosclerotic aneurismal sac visualized, after the first clip application, residual sac could not be confirmed on ICG because of less fluorescence due to atherosclerosis, but on flow 800, residual was confirmed | Application of the second clip to obliterate residual sac |
| 3. 79 | Female | 7 | Perforator was seen attached to dome after clipping. ICG showed flow in perforator, but on flow 800, it was confirmed that flow in perforator is compromised | Clip readjustment was done and perforator was separated from dome |
| 4. 73 | Female | 5 | Complete clipping of aneurysm | No change |
| 5. 41 | Male | 5 | After clip application, ICG showed faint glow on dome, so there was doubt regarding complete clipping. Flow 800 confirmed complete clipping | No change |
| 6. 70 | Female | 5 | After the first clip application, ICG did not show any fluorescence, so complete clipping was assumed, but on doing flow 800, it was observed to have residual filling | Second clip application |
| 7. 65 | Male | 3 | Complete occlusion of aneurysm | No change |
| 8. 75 | Female | 2 | Complete occlusion of aneurysm | No change |
| 9. 70 | Female | 3 | Complete occlusion of aneurysm | No change |
| 10. 81 | Male | 3 | Complete occlusion of aneurysm | No change |
ICG – Indocyanine green
Of ten cases, intraoperative decision was changed in three cases after Flow 800 analysis. In one case, ICG was inconclusive about complete clipping, but Flow 800 confirmed it. These cases are discussed below.
Case 1: Atherosclerotic aneurysm
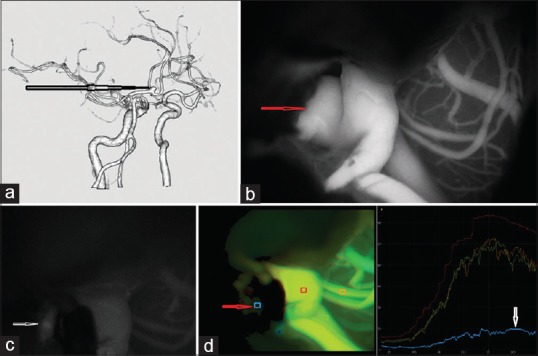
A 71-year-old female was diagnosed with left A-com-A1 junction aneurysm [Figure 1a] which was projecting anteriorly and toward the left side. The patient was operated with left pterional craniotomy and transsylvian approach. Aneurysm dome and neck was found atherosclerotic [Figure 1b]. Preclipping Flow 800 was done [Figure 1c]. After application of the first clip, ICG [Figure 1d] and Flow 800 were repeated [Figure 1e]. On ICG neck, remnant was not very much clear because of atherosclerotic neck. Flow 800 analysis was showing a rising graph confirming remnant [Figure 1e]. Hence, the second clip was applied, and repeat ICG and Flow 800 confirmed complete clipping [Figure 1f]. This case demonstrates how ICG can be ambiguous in atherosclerotic aneurysms, and in such cases, Flow 800 can be useful.
Figure 1.

(a) Preoperative three-dimensional computed tomography scan showing aneurysm (black arrow) at A-com left A1 junction. (b) Intraoperative photo of atherosclerotic aneurysm. (c) Preclipping Flow 800 graph showing flow in aneurysm. (d) Indocyanine green after the first clip application. Red arrow showing clip while white arrow showing decreased fluorescence in atherosclerotic aneurysm neck. (e) Postclipping Flow 800 graph. Red arrow showing ROI in region of atherosclerotic neck and black arrow showing rising graph in that region. (f) Flow 800 graph after application of the second clip. White arrow showing ROI at neck region and black arrow showing flat graph in that region
Case 2: Indocyanine green inconclusive Flow 800 confirms complete clipping
A 41-year-old male presented with A-com aneurysm with left A1 dominance [Figure 2a]. The patient was operated with left pterional craniotomy with transsylvian approach. After aneurysm was found, ICG was done [Figure 2b]. ICG was repeated after clipping. On arterial phase of ICG, aneurysm dome was found to have fluorescence [Figure 2c]. This could be interpreted as either residual dye from previous ICG injections or partially clipped aneurysm. To confirm this, we did Flow 800 analysis which showed complete clipping of aneurysm [Figure 2d].
Figure 2.
(a) Preoperative three-dimensional computed tomography scan showing aneurysm, arrow pointing at aneurysm. (b) Preclipping indocyanine green showing filling of aneurysm. (c) Postclipping indocyanine green. Arrow pointing at fluorescence in aneurismal dome. (d) Postclipping Flow 800 graph. Red arrow pointing at ROI of aneurismal dome and white arrow showing flat graph in corresponding region
Case 3: Indocyanine green misleading but Flow 800 showed incomplete clipping
A 70-year-old female presented with A-com aneurysm [Figure 3a]. A baseline Flow 800 analysis graph before clipping is shown in Figure 3b. ICG done after clipping showed no fluorescence in aneurysm dome [Figure 3c]. This was interpreted as complete clipping; however, on doing Flow 800 analysis, it was found that fluorescent intensity from aneurysm dome was higher than baseline and graph was slightly rising [Figure 3d] confirming incomplete clipping; hence, the second clip application was done. After the second clip application, Flow 800 analysis confirmed complete obliteration of aneurysm sac [Figure 3e].
Figure 3.

(a) Preoperative three-dimensional computed tomography showing aneurysm, arrow pointing at aneurysm. (b) Baseline Flow 800 graph before the first clip application with black arrows showing aneurysm and its corresponding graph. (c) Indocyanine green after the first clip application. Red and black arrow pointing at aneurismal dome showing no florescence. (d) Flow 800 graph after the first clip application. White arrow showing graph higher than baseline and slightly rising. (e) Flow 800 graph after the second clip application. White arrow pointing at flat graph at baseline in region of aneurysm
Discussion
ICG is a near-infrared fluorescent tricarbocyanine dye used in medical diagnostics. The dye is injected intravenously; it binds with the plasma proteins and remains confined to the intravascular system. ICG has a half-life of 3–4 min, and it is eliminated by hepatic metabolism. ICG is used widely in retinal microcirculation.[5] In 2003, Raabe et al.[1] reported their clinical experience with ICG-VA in neurovascular patients. In this study, the postoperative angiographic result corresponds to the ICG-VA findings. Subsequently, several authors have recommended ICG-VA as a useful adjunct to DSA.[6,7] Some authors found intraoperative DSA as a useful tool and have reported that it had a significant impact on the surgical procedure in 7%–34% of cases.[8,9] Intraoperative DSA is unlikely to become the standard of care in many centers because it is time-consuming, expensive, and requires additional experienced people and it has a complication rate of 0.4%–2.6%.[1,10] Intraoperative ICG overcomes these limitations of intraoperative DSA; hence, its use has become widespread in neurovascular surgery. Intraoperative ICG use has some limitations like its usefulness is limited in atherosclerotic or calcified aneurysm walls.[11] In atherosclerotic or calcified aneurysms, fluorescence due to ICG can be easily missed by naked eyes of operating surgeons since ICG-VA is a subjective investigation. Repeated ICG injections within short intervals may give false-positive results depending on surgeons' interpretations.[12]
Flow 800 (Zeiss Meditec, Oberkochen, Germany) is a newer modality of computing the flow dynamics in an ICG fluorescent angiographic study and provides a semi-quantitative analysis of the contrast enhancement utilizing software program and identifies the temporal distribution direction and relation of flow to surrounding vasculature. The data are presented as color-coded maps where the high flow arteries are represented in the red and the low flow vessels (veins) are represented by blue color of the color spectrum. Kamp et al. have described the physics that is applied by the Flow 800 software as it displays two-dimensional tissue maps of the surgical site and are color coded based on maximal fluorescence intensities or the time to half-maximal fluorescence.[13] The Flow 800 software can also be utilized to measure the course of fluorescence intensities in freely definable regions of interest (ROIs) which can detect delayed perfusion in suspected areas of ischemia in various vascular pathologies/surgeries and can be classified into ischemic, penumbra, and oligemic zones.[13] Flow 800 gives objective data in graphical format; hence, it is not susceptible to interobserver variations.
A-com aneurysm surgery is very challenging due to the complex anatomy of multiple vessels and perforators in small area. Hence, intraoperative use of objective investigation like Flow 800 can be very useful in this region compared to ICG-VA which is a subjective investigation. Flow 800 can easily pick up the slightest of flow changes in small perforators and can help to save them. Multiple injections of ICG during surgery can make interpretation of ICG-VA very confusing, and in such cases, graphical data generated by Flow 800 can be very useful in definitive diagnosis. With the help of Flow 800, area of perfusion by the vessel can be marked as ROI. The analysis of the cerebral blood flow index in the ROIs and its color-coded user-friendly display gives a chance to make quick intraoperative decisions.[14] Flow 800 technique is safe, inexpensive, quick, and requires no additional human or hardware resources in the operating room.[15]
Flow 800 has certain limitations similar to ICG angiograph. It is a surface imaging modality with limited penetration, and thus, it captures only the field visible within the microscope or exposed during dissection.[15] Various factors such as blood pressure, heart rate, ejection fraction, and rate of injection can also lead to alteration of results.[14]
Conclusion
Flow 800 is a conclusive, reproducible, and objective tool for early detection of vascular compromise of multiple vessels and perforators in A-com aneurysm surgery. It gives a better idea of vasculature, especially where ICG is ambiguous or inconclusive. By repositioning the clip or making adjustments in the clipping without time delay, cerebral ischemia, especially in the smaller vessels, is effectively avoided and can result in better outcome in patients.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Raabe A, Nakaji P, Beck J, Kim LJ, Hsu FP, Kamerman JD, et al. Prospective evaluation of surgical microscope-integrated intraoperative near-infrared indocyanine green videoangiography during aneurysm surgery. J Neurosurg. 2005;103:982–9. doi: 10.3171/jns.2005.103.6.0982. [DOI] [PubMed] [Google Scholar]
- 2.Raabe A, Beck J, Gerlach R, Zimmermann M, Seifert V. Near-infrared indocyanine green video angiography: A new method for intraoperative assessment of vascular flow. Neurosurgery. 2003;52:132–9. doi: 10.1097/00006123-200301000-00017. [DOI] [PubMed] [Google Scholar]
- 3.Washington CW, Zipfel GJ, Chicoine MR, Derdeyn CP, Rich KM, Moran CJ, et al. Comparing indocyanine green videoangiography to the gold standard of intraoperative digital subtraction angiography used in aneurysm surgery. J Neurosurg. 2013;118:420–7. doi: 10.3171/2012.10.JNS11818. [DOI] [PubMed] [Google Scholar]
- 4.Shah KJ, Cohen-Gadol AA. The application of FLOW 800 ICG videoangiography color maps for neurovascular surgery and intraoperative decision making. World Neurosurg. 2019;122:e186–e197. doi: 10.1016/j.wneu.2018.09.195. [DOI] [PubMed] [Google Scholar]
- 5.Holm C, Mayr M, Höfter E, Dornseifer U, Ninkovic M. Assessment of the patency of microvascular anastomoses using microscope-integrated near-infrared angiography: A preliminary study. Microsurgery. 2009;29:509–14. doi: 10.1002/micr.20645. [DOI] [PubMed] [Google Scholar]
- 6.Hanel RA, Nakaji P, Spetzler RF. Use of microscope-integrated near-infrared indocyanine green videoangiography in the surgical treatment of spinal dural arteriovenous fistulae. Neurosurgery. 2010;66:978–84. doi: 10.1227/01.NEU.0000368108.94233.22. [DOI] [PubMed] [Google Scholar]
- 7.de Oliveira JG, Beck J, Seifert V, Teixeira MJ, Raabe A. Assessment of flow in perforating arteries during intracranial aneurysm surgery using intraoperative near-infrared indocyanine green videoangiography. Neurosurgery. 2008;62:1300–10. doi: 10.1227/01.neu.0000333795.21468.d4. [DOI] [PubMed] [Google Scholar]
- 8.Allcock JM, Drake CG. Postoperative angiography in cases of ruptured intracranial aneurysm. J Neurosurg. 1963;20:752–9. doi: 10.3171/jns.1963.20.9.0752. [DOI] [PubMed] [Google Scholar]
- 9.Macdonald RL, Wallace MC, Kestle JR. Role of angiography following aneurysm surgery. J Neurosurg. 1993;79:826–32. doi: 10.3171/jns.1993.79.6.0826. [DOI] [PubMed] [Google Scholar]
- 10.Alexander TD, Macdonald RL, Weir B, Kowalczuk A. Intraoperative angiography in cerebral aneurysm surgery: A prospective study of 100 craniotomies. Neurosurgery. 1996;39:10–7. doi: 10.1097/00006123-199607000-00004. [DOI] [PubMed] [Google Scholar]
- 11.Balamurugan S, Agrawal A, Kato Y, Sano H. Intra operative indocyanine green video-angiography in cerebrovascular surgery: An overview with review of literature. Asian J Neurosurg. 2011;6:88–93. doi: 10.4103/1793-5482.92168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Dashti R, Hernesniemi J, Niemela M. The role of intra operative Indocyanine green video angiography in cerebrovascular surgery. Eur Neurol Dis. 2007;2:112. [Google Scholar]
- 13.Kamp MA, Slotty P, Turowski B, Etminan N, Steiger HJ, Hänggi D, et al. Microscope-integrated quantitative analysis of intraoperative indocyanine green fluorescence angiography for blood flow assessment: First experience in 30 patients. Neurosurgery. 2012;70:65–73. doi: 10.1227/NEU.0b013e31822f7d7c. [DOI] [PubMed] [Google Scholar]
- 14.Ye X, Liu XJ, Ma L, Liu LT, Wang WL, Wang S, et al. Clinical values of intraoperative indocyanine green fluorescence video angiography with Flow 800 software in cerebrovascular surgery. Chin Med J (Engl) 2013;126:4232–7. [PubMed] [Google Scholar]
- 15.Jhawar SS, Kato Y, Oda J, Oguri D, Sano H, Hirose Y. FLOW 800-assisted surgery for arteriovenous malformation. J Clin Neurosci. 2011;18:1556–7. doi: 10.1016/j.jocn.2011.01.041. [DOI] [PubMed] [Google Scholar]