

Abstract
Objective
The aim of this study is to evaluate the presence of significant differences regarding the lateral acromial angle, critical shoulder angle, and the acromial index between patients with and without rotator cuff tears.
Method
The MRIs (Magnetic Resonnance Imaging) of 82 patients were studied. The rotator cuff tear group (RCT group) included 41 patients while the control group also included 41 patients without rotator cuff tears. Acromial parameters and demographical data were extracted for statistical analysis.
Results
No statistical significant difference was found in terms of the studied acromial parameters between patients with and without rotator cuff tears. No correlation was found between age and any of the studied parameters. LAA (Lateral Acromial Angle) was found to be significantly different between males and females of the studied sample. However, no difference was found between patients with and without rotator cuff tears when both genders were studied separately. Moreover, no statistical significant difference was found in terms of the studied acromial parameters between males and females when the RCT group and the control group were studied separately. When gender was the covariate in the one-way MANCOVA test, gender was not significantly dependent on the type of groups (RCT group vs control group).
Conclusion
The results obtained from this study suggested that the studied acromial parameters in patients with rotator cuff tears were not different from the parameters found in patients without rotator cuff tears. Moreover, gender was not found to influence the acromial parameters, with no subsequent effect on the development of rotator cuff tears. Further studies may be required for better understanding on the biomechanics, taking into consideration age, gender, and the given population.
Keywords: Shoulder, Rotator cuff, Biomechanics, Acromion, Magnetic resonance images, Parameters
Introduction
Shoulder pain remains one of the most prevalent chief complaints within the general population that leads to doctor visits, being second only to lower back pain. The literature implies that shoulder impingement syndrome is responsible for 30–35% of shoulder disorders making it the most common cause of shoulder pain1, 2, 3, 4, 5. Regardless of the symptomatology of rotator cuff disease, the prevalence is around 10% among people younger than 20 years of age and 62% among people older than 80 years of age.6 The etiology behind rotator cuff tears is still poorly understood as debate in the literature continues of whether rotator cuff tears are due to degenerative changes of the tendons (intrinsic etiology/genetic) or due to mechanical compression by the acromion (extrinsic etiology/anatomic).7 In 1983, Neer attributed mechanical impingement as the cause of 95% of rotator cuff tear cases. Henceforth, Neer reported the success of the anterior approach in acromioplasty for the treatment of cuff tears.8,9 Acromioplasty remains the standard surgical approach in the management of impingement lesions. The indication for an acromioplasty is based on evaluating the patient clinically, and then supported later by acromial morphological changes seen on imaging modalities.8,10 The most common morphological classification of the acromion was described by Bigliani et al., in 1986. Based on outlet-view X-rays, Bigliani et al. described a flat acromion (type I), a curved acromion (type II), and a hooked acromion (type III).10 Some studies have found an association between type III acromion and an increased risk prevalence to cuff tears.10, 11, 12 On the other hand, other studies have failed to find such association.13 Balke et al. (2013) reported that a hooked acromion (type III) was a common morphological feature among patients with rotator cuff tears. Moreover, their results showed lack of significant correlation between acromion type and age was in correspondence with the literature.7,14,15
Certain authors took the attempt to describe the morphology of the acromion via certain parameters such as the acromial slope (AS),10,16 and the acromial tilt (AT).16,17 The acromial slope is represented by the δ angle which is formed by the intersection of two lines. The first line is that connecting the most anterior point and the midway point of the inferior acromion. The second line is the one connecting the most posterior point and the same midway point of the inferior acromion.7,10,16 In 1995, Tuite et al. reported that the acromial slope can be used in identifying patients with a greater likelihood of developing a cuff tear. Their results showed that patients with a major rotator cuff tear had a mean acromial slope angle of 29° compared to a mean AS slope angle of 24° among patients with an intact cuff.18 On the other hand, Balke et al. (2013) maintained that the AS was of no use in predicting the likelihood of rotator cuff tears. However, it was suggested that the rare presence of Bigliani type III acromion with a high AS angle (higher than 43°) increases the prevalence of rotator cuff tears among the younger population.7
The acromial tilt is represented by the β angle which is formed by the intersection of a line connecting the most posterior and the most anterior point of the inferior acromion and a line connecting that same most posterior point of the inferior acromion to the coracoid process’s inferior tip.7,16,17 Although, the AT depicts the relationship between the coracoid process and the anterior acromion, the literature remains to contain controversial results regarding the relationship between the AT and the development of rotator cuffs tears. Henceforth, one would expect that the lower the AT angle, the higher rotator cuff tears incidence. Some studies are in accordance with such statement while other studies found that the AT angle was lower among the control group when compared to the AT angle of patients with a rotator cuff tears.7,16,17,19,20 Stehle et al. (2007) attributed the disparities of these results to the variability in the outlet-view radiographs.21
Hence, the literature remains to contain controversial reports regarding the influence of acromial parameters in the development of rotator cuff tears (RCT). However, as to our knowledge, the literature contains limited descriptions of other acromial morphological parameters such the lateral acromial angle (LAA), the critical shoulder angle (CSA), and the acromial index (AI), especially those of a Middle Eastern population. Moreover, we will evaluate the presence of any correlation between age and any of these parameters. We also investigate the influence of gender on these parameters and whether any association is present regarding rotator cuff tears risk.
Population and methods
Sampling
82 magnetic resonance (MR) images were retrospectively analysed for the purpose of this study. These MRIs were done at St George Hospital University Medical Center (SGHUMC) between March 2018 and July 2019.
The sample size is 82 patients divided into two groups. The first group includes the patients that underwent arthroscopic rotator cuff repair (patient group/RCT group, n = 41) while the second group includes those who had no findings of rotator cuff tears based on MR images (control group, n = 41). The sample size of the group that include patients with rotator cuff tears was reached based on the number of patients who presented to SGHUMC for rotator cuff repair between March 2018 and July 2019 with respect to the inclusion and exclusion criteria, and not based on the general population. Individuals in the control group were randomly selected based on MR records of patients with healthy shoulders at SGHUMC between March 2018 and July 2019.
Inclusion criteria
The inclusion criterias for the RCT group were met under two conditions: the patient is presenting for arthroscopic rotator cuff repair after being evaluated via physical exam and MR images (MRI) and that the MRIs were done at SGHUMC.
The number of patients who underwent an arthroscopic repair for their rotator cuff tears was 225 patients. A total of 61 patients met the inclusion criteria.
The inclusion criteria for the control group were met under one condition which is shoulder MRI done at SGHUMC.
Exclusion criteria
For the exclusion criteria, patients with any past or present shoulder pathology were excluded from the purpose of this study. Moreover, any patient with a positive past surgical history for shoulder surgery of any type was also excluded from the study.
An additional 20 patients were excluded thus reaching the number of patients in RCT group to 41 patients.
97 patients met the inclusion and exclusion criteria from which 41 individuals were randomly selected for the control group.
Statistical analysis
Statistical analysis was performed using SPSS software (version 20; SPSS, Chicago). Data were analysed using descriptive statistics (mean, standard deviation, median, frequency, percentage minimum and maximum).
Measurements
The distance from the glenoid plane to the lateral border of the acromion (GA) is divided by the distance from the glenoid plane to the lateral aspect of the humeral head (GH) and called the acromion index (Fig. 1). A high acromion index represents an acromion that projects far laterally and covers the biggest portion of the humeral head.
Fig. 1.
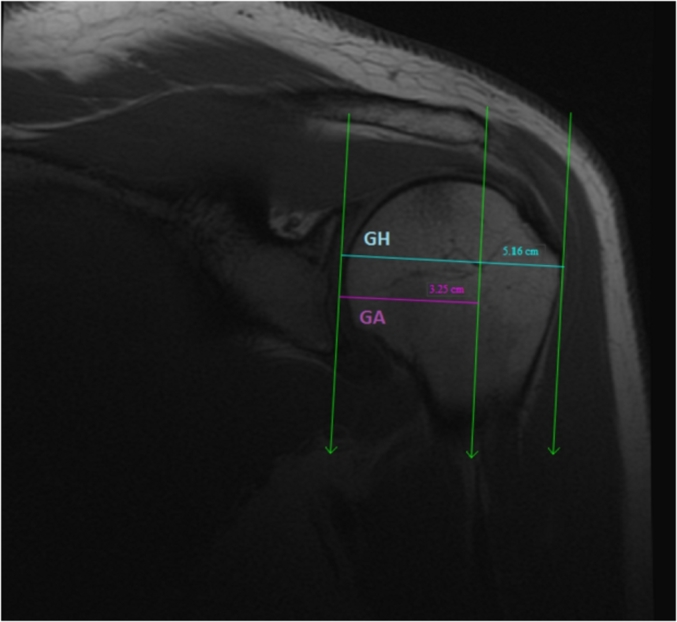
The acromion index (AI) represented by the distance from the glenoid plane to the lateral border of the acromion (GA) divided by the distance from the glenoid plane to the lateral aspect of the humeral head (GH).
The lateral acromion angle is determined on coronal MR arthrograms and represents the angle enclosed between the glenoid plane and the undersurface of the acromion (Fig. 2).
Fig. 2.
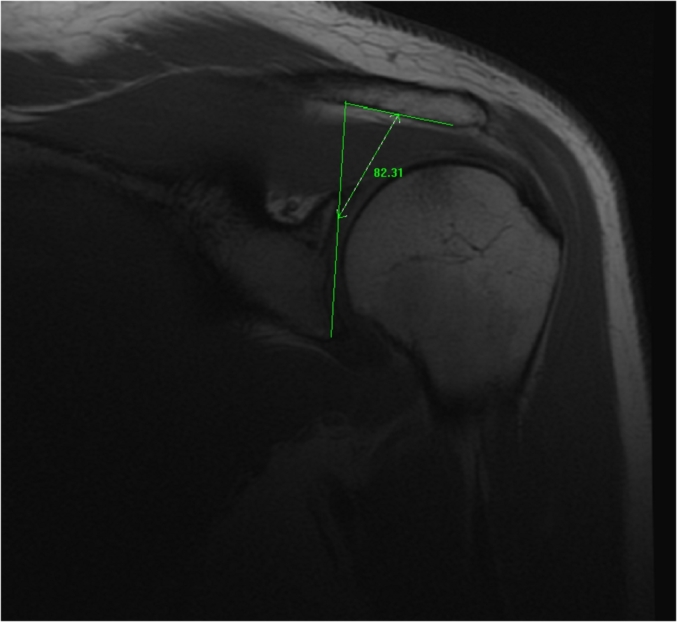
The lateral acromial angle (LAA) represented by the angle enclosed between the glenoid plane and the undersurface of the acromion.
The critical shoulder angle is defined as a line connecting the superior and inferior bony margins of the glenoid and an intersecting line drawn from the inferior bony margin of the glenoid to the most lateral border of the acromion (Fig. 3).
Fig. 3.
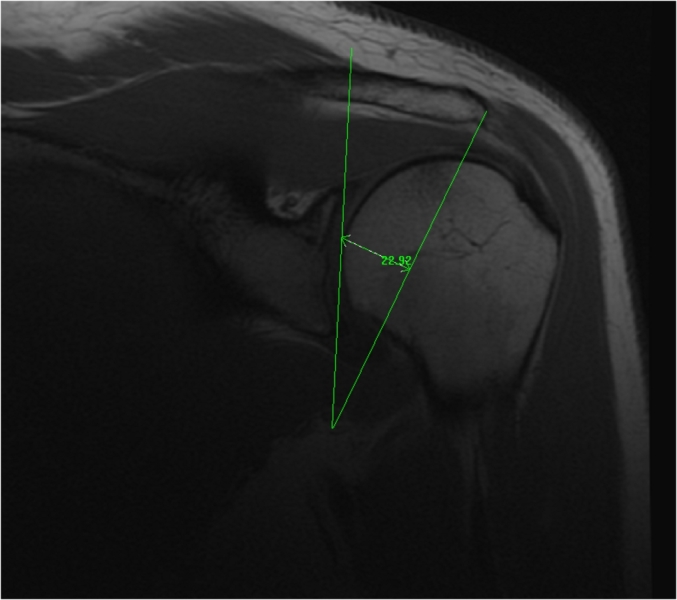
The critical shoulder angle represented by the line connecting the superior and inferior bony margins of the glenoid and an intersecting line drawn from the inferior bony margin of the glenoid to the most lateral border of the acromion.
Results
82 MRIs were retrospectively analysed and subsequently included in this study. Table 1 shows the demographic distribution of the studied sample.
Table 1.
The demographic characteristics of the RCT group and the control groups.
| Groups | Patient group (n = 41) | Control group (n = 41) | Total | |
|---|---|---|---|---|
| Gender | Female | 11 (27%) | 16 (39%) | 27 (33%) |
| Male | 30 (73%) | 25 (61%) | 55 (67%) | |
| Age (years) | Mean ± SD | 46.54 ± 15.84 | 38.37 ± 13.69 | 42.45 ± 15.27 |
| Range | 19–73 | 17–76 | 17–76 | |
Comparison of acromial parameters between RCT group and control group
The T-test was used to compare the means of the acromial parameters between RCT group and control group to assess the presence of any statistical significance in which the p-value would be lower than α (error ratio = 5% i.e. 0.05). In the independent t-test, the variances of the RCT group and the control group are assumed to be equal in the given population. The Type I error rate can be affected if the variances are not equal. The Levene’s Test of Equality of Variances is used to study the homogeneity of the variances, in which an F-statistic and a significance value (p-value) are obtained. As such, the p-value is compared to α = 0.05 (Table 2).
Table 2.
The comparison of the morphological parameters of the acromion of the two groups. NB. EVA= Equal variances assumed, EVNA= Equal variances not assumed. ∗Significant at level 0.05, ∗∗Significant at level 0.01
| Acromial parameters | Group | Group Statistics |
Levene’s Test for Equality of Variances |
t-test for Equality of Means |
|||||
|---|---|---|---|---|---|---|---|---|---|
| N | Mean | SD | Variances | F | P-value | t | P-value | ||
| LAA | Rotator cuff tear | 41 | 79.70 | 5.59 | EVA | 0.486 | 0.488 | −1.267 | 0.209 |
| No rotator cuff tear | 41 | 81.27 | 5.61 | EVNA | −1.267 | 0.209 | |||
| CSA | Rotator cuff tear | 41 | 34.67 | 5.14 | EVA | 0.006 | 0.938 | −0.442 | 0.660 |
| No rotator cuff tear | 41 | 35.18 | 5.26 | EVNA | −0.442 | 0.660 | |||
| AI | Rotator cuff tear | 41 | 0.68 | 0.08 | EVA | 0.189 | 0.665 | 1.113 | 0.269 |
| No rotator cuff tear | 41 | 0.66 | 0.09 | EVNA | 1.113 | 0.269 | |||
No statistically significant difference was found in terms of the LAA, CSA, and AI between the RCT group and the control group, as all p-values are above 0.05.
Multivariate analysis
One-way multivariate analysis of variance (one-way MANOVA)
The one-way MANOVA was used to determine whether there are any statistically significant differences between independent groups (RCT vs control) on more than one continuous dependent variable (the acromial parameters).
As per Table 3, the p-value in Wilks’ Lambda row is higher than 0.05 with a value of 0.208. Hence, the acromial parameters were not significantly dependent on the type of group (RCT vs Control).
Table 3.
Multivariate tests. ∗∗Significant at level 0.01
| Multivariate Tests | ||||||
|---|---|---|---|---|---|---|
| Effect | Value | F | Hypothesis df | Error df | P-value | |
| Intercept | Pillai’s Trace | 0.997 | 9516.390 | 3.000 | 78.000 | 0.000∗∗ |
| Wilks’ Lambda | 0.003 | 9516.390 | 3.000 | 78.000 | 0.000∗∗ | |
| Hotelling’s Trace | 366.015 | 9516.390 | 3.000 | 78.000 | 0.000∗∗ | |
| Roy’s Largest Root | 366.015 | 9516.390 | 3.000 | 78.000 | 0.000∗∗ | |
| Group | Pillai’s Trace | 0.056 | 1.551 | 3.000 | 78.000 | 0.208 |
| Wilks’ Lambda | 0.944 | 1.551 | 3.000 | 78.000 | 0.208 | |
| Hotelling’s Trace | 0.060 | 1.551 | 3.000 | 78.000 | 0.208 | |
| Roy’s Largest Root | 0.060 | 1.551 | 3.000 | 78.000 | 0.208 | |
Correlation between age and acromial parameters
For the evaluation of any correlation between age and any of the acromial parameters between the RCT group and the control group, Pearson correlation was used (Table 4).
Table 4.
Correlation between acromion parameters and age in general and age in the two groups. ∗Significant at level 0.05
| Group | Total (n = 82) |
RCT group (n = 41) |
Control group (n = 41) |
||||
|---|---|---|---|---|---|---|---|
| Pearson Correlation | P-value | Pearson Correlation | P-value | Pearson Correlation | P-value | ||
| Acromion parameters | LAA | −0.136 | 0.225 | −0.140 | 0.382 | −0.060 | 0.711 |
| CSA | −0.120 | 0.282 | −0.185 | 0.246 | −0.028 | 0.863 | |
| AI | −0.033 | 0.770 | −0.120 | 0.455 | −0.019 | 0.906 | |
No correlation was found between age and any of the acromial parameters as seen in Table 4.
Gender and morphological parameters of the acromion
The results portrayed in Table 5 showed that gender had a significant effect on LAA (P-value < 0.05), in which females had a higher LAA. However, this statistical significance may not be correlated with clinical significance.
Table 5.
General comparison of acromial parameters by gender among the sample. ∗Significant at level 0.05, ∗∗Significant at level 0.01
| Group | Group Statistics |
Levene’s Test for Equality of Variances |
t-test for Equality of Means |
||||||
|---|---|---|---|---|---|---|---|---|---|
| N | Mean | SD | Variances | F | P-value | t | P-value | ||
| LAA | Female | 27 | 82.31 | 6.36 | EVA | 1.619 | 0.207 | 2.102 | 0.039∗ |
| Male | 55 | 79.59 | 5.04 | EVNA | 1.942 | 0.059 | |||
| CSA | Female | 27 | 33.53 | 4.27 | EVA | 1.384 | 0.243 | −1.725 | 0.088 |
| Male | 55 | 35.60 | 5.48 | EVNA | −1.876 | 0.065 | |||
| AI | Female | 27 | 0.65 | 0.10 | EVA | 1.420 | 0.237 | −1.170 | 0.246 |
| Male | 55 | 0.68 | 0.08 | EVNA | −1.093 | 0.280 | |||
The results showed no statistically significant difference between RCT group and control group in terms of any of the acromial parameters by gender (Table 6).
Table 6.
Comparison of acromial parameters by gender among patients with rotator cuff tears (RCT group). ∗Significant at level 0.05, ∗∗Significant at level 0.01
| Group | Group Statistics |
Levene’s Test for Equality of Variances |
t-test for Equality of Means |
||||||
|---|---|---|---|---|---|---|---|---|---|
| N | Mean | SD | Variances | F | P-value | T | P-value | ||
| LAA | Female | 11 | 82.34 | 6.30 | EVA | 0.605 | 0.441 | 1.887 | 0.067 |
| Male | 30 | 78.73 | 5.08 | EVNA | 1.704 | 0.109 | |||
| CSA | Female | 11 | 32.89 | 4.26 | EVA | 0.784 | 0.381 | −1.351 | 0.184 |
| Male | 30 | 35.32 | 5.35 | EVNA | −1.502 | 0.147 | |||
| AI | Female | 11 | 0.68 | 0.07 | EVA | 0.218 | 0.643 | −0.081 | 0.936 |
| Male | 30 | 0.68 | 0.09 | EVNA | −0.087 | 0.932 | |||
All p-values in Table 7 are higher than 0.05, hence; no statistically significant difference between RCT group and control group in terms of any of the acromial parameters.
Table 7.
Comparison of acromial parameters by gender among individuals without a rotator cuff tear.
| Group | Group Statistics |
Levene’s Test for Equality of Variances |
t-test for Equality of Means |
||||||
|---|---|---|---|---|---|---|---|---|---|
| N | Mean | SD | Variances | F | P-value | T | P-value | ||
| LAA | Female | 16 | 82.29 | 6.61 | EVA | 0.803 | 0.376 | 0.930 | 0.358 |
| Male | 25 | 80.61 | 4.90 | EVNA | 0.871 | 0.392 | |||
| CSA | Female | 16 | 33.97 | 4.36 | EVA | 0.515 | 0.477 | −1.180 | 0.245 |
| Male | 25 | 35.95 | 5.71 | EVNA | −1.252 | 0.218 | |||
| AI | Female | 16 | 0.64 | 0.11 | EVA | 1.732 | 0.196 | −1.255 | 0.217 |
| Male | 25 | 0.67 | 0.08 | EVNA | −1.157 | 0.259 | |||
For both females (Table 7) and males (Table 8), the type of groups did not have any statistically significant effect on the acromial parameters (p > 0.05).
Table 8.
Comparison of acromial parameters between females with rotator cuff tears and females without cuff tears. ∗∗Significant at level 0.01
| Group | Group Statistics |
Levene’s Test for Equality of Variances |
t-test for Equality of Means |
||||||
|---|---|---|---|---|---|---|---|---|---|
| N | Mean | SD | Variances | F | P-value | t | P-value | ||
| LAA | Rotator cuff tear | 11 | 82.34 | 6.30 | EVA | 0.049 | 0.826 | 0.020 | 0.984 |
| No rotator cuff tear | 16 | 82.29 | 6.61 | EVNA | 0.020 | 0.984 | |||
| CSA | Rotator cuff tear | 11 | 32.89 | 4.26 | EVA | 0.009 | 0.924 | −0.637 | 0.530 |
| No rotator cuff tear | 16 | 33.97 | 4.36 | EVNA | −0.639 | 0.529 | |||
| AI | Rotator cuff tear | 11 | 0.68 | 0.07 | EVA | 0.960 | 0.337 | 1.099 | 0.282 |
| No rotator cuff tear | 16 | 0.64 | 0.11 | EVNA | 1.188 | 0.246 | |||
For both females (Table 8) and males (Table 9), the type of groups did not have any statistically significant effect on the acromial parameters (p > 0.05).
Table 9.
Comparison of acromial parameters between males with rotator cuff tears and males without cuff tears. ∗∗Significant at level 0.01
| Group | Group Statistics |
Levene’s Test for Equality of Variances |
t-test for Equality of Means |
||||||
|---|---|---|---|---|---|---|---|---|---|
| N | Mean | SD | Variances | F | P-value | t | P-value | ||
| LAA | Rotator cuff tear | 30 | 78.73 | 5.08 | EVA | 0.282 | 0.598 | −1.390 | 0.170 |
| No rotator cuff tear | 25 | 80.61 | 4.90 | EVNA | −1.394 | 0.169 | |||
| CSA | Rotator cuff tear | 30 | 35.32 | 5.35 | EVA | 0.003 | 0.953 | −0.421 | 0.676 |
| No rotator cuff tear | 25 | 35.95 | 5.71 | EVNA | −0.418 | 0.678 | |||
| AI | Rotator cuff tear | 30 | 0.68 | 0.09 | EVA | 0.491 | 0.487 | 0.344 | 0.732 |
| No rotator cuff tear | 25 | 0.67 | 0.08 | EVNA | 0.348 | 0.730 | |||
One-way multivariate analysis of covariance (MANCOVA)
One-way MANCOVA was used to determine whether there are any differences between independent groups (RCT group vs Control group) on more than one continuous dependent variable (the acromial morphological parameters) where the gender is the covariate and its linearly related to the dependent variables and its inclusion into the analysis can increase the ability to detect differences between groups of an independent variable.
The "P-value" value of Wilks’ Lambda in the “Group” row has a value of 0.235, which means p > 0.05. Consequently, the results showed that the acromion parameters were not significantly dependent on the type of group (RCT group vs Control group).
Discussion
Shoulder pain remains one of the leading causes for doctor visits, with rotator cuff tears being common causes of shoulder pain and decreased functionality. Cuff tears are associated with a reduced quality of life and increased utilisation of health care resources.22,23 In addition to the previously stated acromial parameters (AS, AT, Bigliani types), some authors relied on MRIs to describe the acromial frontal plane slope and found an increased incidence of rotator cuff disease among patients with a lower lateral acromial angle (LAA).14 In 1995, Banas et al. measured the LAA basing on the anteroposterior (AP) radiographs in which the α angle was the intersection between a parallel line to the acromial undersurface and a line connecting the most lateral superior and inferior points of the glenoid (thus representing the glenoid surface).7,14 Banas et al. (1995) and Balke et al. (2013) showed a statistically significant correlation between the lateral acromial angle and cuff disease incidence as determined by MRI.7,14 Tetreault et al. (2004) explained that the smaller the LAA, the smaller the volume for the shoulder components to fit, which results in increased pressure on the rotator cuff. When the lateral acromial angle was less than 70°, the average age of patients with a complete rotator cuff tear was 54 years compared to an average age of 70 years in patients with cuff tears but an LAA greater than 70°.7,14,24 However, no statistically significant difference was found between RCT group and the control group in terms of LAA.
Other authors noticed a more lateral extension of the acromion in patients with rotator cuff tears when compared to patient with intact rotator cuffs and thus describing the acromion index (AI).25 In 2006, Nyffeler et al. measured the AI on true AP radiographs. As the acromial extension becomes larger, the AI becomes higher since AI is the distance from glenoid plane to the acromion (GA) divided by the distance from the same glenoid plane to the lateral aspect of the humeral head (GH). Thus, the acromial index is defined as AI = GA/GH.7,25 Several studies found a significantly higher acromial index in patients with rotator cuff tears.7,25,26 In the current study, patients with rotator cuff tears were found to have a higher AI. However, that difference was not found to be statistically significant.
These results may be related to population-based anatomic differences that may be present in a Middle Eastern population such as the Lebanese population. Also, our sample population consisted of only 82 patients divided into two groups which likely underestimated the association. Moreover, our study relied on three acromial parameters to evaluate the association with rotator cuff tears. The lack of studies available in our population sample makes this an interesting study for the evaluation of acromion with rotator cuff tears. Furthermore, our study relied on MRI imaging modality for the evaluation of these parameters.
In 2013, Moor et al. introduced the notion of critical shoulder angle (CSA) which combines the lateral roof extension of the acromion and the glenoid inclination (GI). The CSA is formed by the intersection of the line connecting the superior and inferior points of the lateral aspect of the glenoid and the line connecting the inferior point of the lateral aspect of the glenoid to the lateral edge of the acromion.27,28 When the CSA is large, an increased supraspinatus activity is necessary to preserve the stability of the joint which put increased pressure on the muscle-tendon unit of the supraspinatus. Consequently, a CSA larger than 35° was found to be associated with rotator cuff tears.27,28, 29 However, such statistical significance was not found in terms of CSA between the RCT group and the Control group. As previously stated by Moor et al., a large CSA was found to be associated specifically with supraspinatus tears. Hence, one might conclude the results of the current study were affected by an insufficient numbers of patients with isolated supraspinatus tear which may be a limitation in this study in terms of the CSA.
As such, we concluded that the LAA, CSA, and AI could not be used to assess the risk for cuff tears in the Lebanese population.
Pearson correlation was used to investigate whether any correlation is present between the acromial parameters and age in each of the two group (RCT group vs Control group). We found no correlation between age and any of the 3 studied acromial parameters (CSA, AI, LAA).
Limited data is present in the literature that evaluate the influence of gender on the acromial parameters, and its association with rotator cuff tears. While taking into consideration the gender of the studied sample, our analysis of the acromial morphological parameters showed that gender had a statistically significant effect on LAA. The results showed that females had a higher LAA. Despite the difference is statistically significant, the clinical significance is questionable. Moreover, there was no statistically significant difference in terms of LAA between the RCT group and the control group. Furthermore, in both females (Table 8) and males (Table 10), there were no statistically significant differences in any of the acromial parameters between patients with rotator cuff tears and patients without cuff tears among each of the two genders studied. When the RCT group and the control group were studied separately, there was no statistically significant difference in terms of the LAA, CSA, and AI between males and females. These results may suggest that despite the anatomic differences at the musculoskeletal level between males and females, these differences may not be of major significance at the acromion level.
Table 10.
Multivariate analysis used to determine whether there are any differences between independent groups (RCT group vs Control group) on more than one continuous dependent variable (the acromial morphological parameters) where the gender is the covariate and its linearly related to the dependent variables. ∗∗Significant at level 0.01
| Multivariate Tests | ||||||
|---|---|---|---|---|---|---|
| Effect | Value | F | Hypothesis df | Error df | P-value | |
| Intercept | Pillai’s Trace | 0.965 | 709.007 | 3.000 | 77.000 | 0.000∗∗ |
| Wilks’ Lambda | 0.035 | 709.007 | 3.000 | 77.000 | 0.000∗∗ | |
| Hotelling’s Trace | 27.624 | 709.007 | 3.000 | 77.000 | 0.000∗∗ | |
| Roy’s Largest Root | 27.624 | 709.007 | 3.000 | 77.000 | 0.000∗∗ | |
| Group | Pillai’s Trace | 0.053 | 1.448 | 3.000 | 77.000 | 0.235 |
| Wilks’ Lambda | 0.947 | 1.448 | 3.000 | 77.000 | 0.235 | |
| Hotelling’s Trace | 0.056 | 1.448 | 3.000 | 77.000 | 0.235 | |
| Roy’s Largest Root | 0.056 | 1.448 | 3.000 | 77.000 | 0.235 | |
| Sex | Pillai’s Trace | 0.069 | 1.896 | 3.000 | 77.000 | 0.137 |
| Wilks’ Lambda | 0.931 | 1.896 | 3.000 | 77.000 | 0.137 | |
| Hotelling’s Trace | 0.074 | 1.896 | 3.000 | 77.000 | 0.137 | |
| Roy’s Largest Root | 0.074 | 1.896 | 3.000 | 77.000 | 0.137 | |
The one-way MANCOVA, in which gender was the covariate, was used to evaluate if any differences are present between the group type (RCT group vs control group) on the studied acromial parameters (LAA, CSA, and AI). The results showed that none of the acromial parameters was not significantly dependent on the type of group (RCT group vs Control group). Therefore, further follow-up tests could not be performed.
Conclusion
The results of this study are suggestive that the LAA, CSA, and AI of patient with rotator cuff tears were not different from the acromial parameters of the patients in the control group. Consequently, these measurements may be less helpful in assessing the risk of rotator cuff tears when it comes to the Lebanese population. Furthermore, no correlation was found between age and any of the acromial parameters, which may be suggestive that the acromion sustains less changes with age. The studied parameters did not differ between females with cuff tears and control females, males with cuff tears and control males. Moreover, there was no significant difference in terms of acromial parameters between males and females when each of the 2 group (RCT group and control group) were studied separately. However, statistically significant difference was found between males and females in terms of LAA when the whole sample was studied. Further studies, preferably population based and prospective in nature, should be conducted for further understanding of the cuff tears mechanisms, and the impact of the population, gender, and age on the development of tears.
Limitations
Our study is a retrospective study that relied on three acromial parameters to evaluate the association with rotator cuff tears. Furthermore, our study relied only on MRI imaging modality for the evaluation of these parameters. Our sample consisted of only 82 patients divided into control and rotator cuff tear group, a bigger sample might be more representative and may lead to similar results as those studies previously published.
Financial disclosure
The authors declared that this study has received no financial support.
Consent
Written informed consents were obtained from each patient for the purpose of this study.
Funding
No funds were received in support of this study.
Declaration of competing interest
The authors declare no conflict of interest regarding the publication of this article.
Contributor Information
Joseph Maalouly, Email: Josephmaalouly2@gmail.com.
Antonios Tawk, Email: Antoniostawk@gmail.com.
Dany Aouad, Email: dany_aouad@hotmail.com.
Ali Abdallah, Email: Ali.h.abdallah90@gmail.com.
Mohammad Darwiche, Email: Mohammaddarwish2@gmail.com.
Ghadi Abboud, Email: Ghadi.abboud11@gmail.com.
Georges El Rassi, Email: georgeelrassi@hotmail.com.
References
- 1.Michener L.A., Walsworth M.K., Burnet E.N. Effectiveness of rehabilitation for patients with subacromial impingement syndrome: a systematic review. J Hand Ther. 2004;17(2):152–164. doi: 10.1197/j.jht.2004.02.004. [DOI] [PubMed] [Google Scholar]
- 2.Schröder J., Van Dijk C.N., Wielinga A., Kerkhoffs G.M.M.J., Marti R.K. Open versus arthroscopic treatment of chronic rotator cuff impingement. Arch Orthop Trauma Surg. 2001;121(5):241–244. doi: 10.1007/s004020100259. [DOI] [PubMed] [Google Scholar]
- 3.Faber E., Kuiper J.I., Burdorf A., Miedema H.S., Verhaar J.A. Treatment of impingement syndrome: a systematic review of the effects on functional limitations and return to work. J Occup Rehabil. 2006;16(1):6–24. doi: 10.1007/s10926-005-9003-2. [DOI] [PubMed] [Google Scholar]
- 4.Van der Windt D.A., Koes B.W., de Jong B.A., Bouter L.M. Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis. 1995;54(12):959–964. doi: 10.1136/ard.54.12.959. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Juel N.G., Natvig B. Shoulder diagnoses in secondary care, a one year cohort. BMC Muscoskel Disord. 2014;15(1):89. doi: 10.1186/1471-2474-15-89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Teunis T., Lubberts B., Reilly B.T., Ring D. A systematic review and pooled analysis of the prevalence of rotator cuff disease with increasing age. J Shoulder Elbow Surg. 2014;23(12):1913–1921. doi: 10.1016/j.jse.2014.08.001. [DOI] [PubMed] [Google Scholar]
- 7.Balke M., Schmidt C., Dedy N., Banerjee M., Bouillon B., Liem D. Correlation of acromial morphology with impingement syndrome and rotator cuff tears. Acta Orthop. 2013;84(2):178–183. doi: 10.3109/17453674.2013.773413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Charles S Neer I.I. Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report. JBJS. 1972;54(1):41–50. [PubMed] [Google Scholar]
- 9.Neer C.S. Impingement lesions. Clin Orthop Relat Res. 1983;173:70–77. 1976-2007. [PubMed] [Google Scholar]
- 10.Bigliani L.U. The morphology of the acromion and its relationship to rotator cuff tears. Orthop Trans. 1986;10:228. [Google Scholar]
- 11.Bigliani L.U., Ticker J.B., Flatow E.L., Soslowsky L.J., Mow V.C. The relationship of acromial architecture to rotator cuff disease. Clin Sports Med. 1991;10(4):823–838. [PubMed] [Google Scholar]
- 12.MacGillivray J.D., Fealy S., Potter H.G., O’Brien S.J. Multiplanar analysis of acromion morphology. Am J Sports Med. 1998;26(6):836–840. doi: 10.1177/03635465980260061701. [DOI] [PubMed] [Google Scholar]
- 13.Ozaki J., Fujimoto S., Nakagawa Y., Masuhara K., Tamai S. Tears of the rotator cuff of the shoulder associated with pathological changes in the acromion. A study in cadavera. J Bone Joint Surg. 1988;70(8):1224–1230. American volume. [PubMed] [Google Scholar]
- 14.Banas M.P., Miller R.J., Totterman S. Relationship between the lateral acromion angle and rotator cuff disease. J Shoulder Elbow Surg. 1995;4(6):454–461. doi: 10.1016/s1058-2746(05)80038-2. [DOI] [PubMed] [Google Scholar]
- 15.Vähäkari M., Leppilahti J., Hyvönen P., Ristiniemi J., Päivänsalo M., Jalovaara P. Acromial shape in asymptomatic subjects: a study of 305 shoulders in different age groups. Acta Radiol. 2010;51(2):202–206. doi: 10.3109/02841850903476556. [DOI] [PubMed] [Google Scholar]
- 16.Kitay G.S., Iannotti J.P., Williams G.R., Haygood T., Kneeland B.J., Berlin J. Roentgenographic assessment of acromial morphologic condition in rotator cuff impingement syndrome. J Shoulder Elbow Surg. 1995;4(6):441–448. doi: 10.1016/s1058-2746(05)80036-9. [DOI] [PubMed] [Google Scholar]
- 17.Aoki M. The slope of the acromion and rotator cuff impingement. Orthop Trans. 1986;10:228. [Google Scholar]
- 18.Tuite M.J., Toivonen D.A., Orwin J.F., Wright D.H. Acromial angle on radiographs of the shoulder: correlation with the impingement syndrome and rotator cuff tears. AJR. Am J Roentgenol. 1995;165(3):609–613. doi: 10.2214/ajr.165.3.7645479. [DOI] [PubMed] [Google Scholar]
- 19.Prato N., Peloso D., Franconeri A. The anterior tilt of the acromion: radiographic evaluation and correlation with shoulder diseases. Eur Radiol. 1998;8(9):1639–1646. doi: 10.1007/s003300050602. [DOI] [PubMed] [Google Scholar]
- 20.Zuckerman J.D., Kummer F.J., Cuomo F., Simon J., Rosenblum S., Katz N. The influence of coracoacromial arch anatomy on rotator cuff tears. J Shoulder Elbow Surg. 1992;1(1):4–14. doi: 10.1016/S1058-2746(09)80010-4. [DOI] [PubMed] [Google Scholar]
- 21.Stehle J., Moore S.M., Alaseirlis D.A., Debski R.E., McMahon P.J. Acromial morphology: effects of suboptimal radiographs. J Shoulder Elbow Surg. 2007;16(2):135–142. doi: 10.1016/j.jse.2006.05.004. [DOI] [PubMed] [Google Scholar]
- 22.Jeanfavre M., Husted S., Leff G. Exercise therapy in the non-operative treatment of full-thickness rotator cuff tears: a systematic review. Int J Sports Phys Ther. 2018;13(3):335. [PMC free article] [PubMed] [Google Scholar]
- 23.Pribicevic M. Pain in Perspective. IntechOpen; 2012. The epidemiology of shoulder pain: a narrative review of the literature. [Google Scholar]
- 24.Tètreault P., Krueger A., Zurakowski D., Gerber C. Glenoid version and rotator cuff tears. J Orthop Res. 2004;22(1):202–207. doi: 10.1016/S0736-0266(03)00116-5. [DOI] [PubMed] [Google Scholar]
- 25.Nyffeler R.W., Werner C.M., Sukthankar A., Schmid M.R., Gerber C. Association of a large lateral extension of the acromion with rotator cuff tears. JBJS. 2006;88(4):800–805. doi: 10.2106/JBJS.D.03042. [DOI] [PubMed] [Google Scholar]
- 26.Torrens C., López J.M., Puente I., Cáceres E. The influence of the acromial coverage index in rotator cuff tears. J Shoulder Elbow Surg. 2007;16(3):347–351. doi: 10.1016/j.jse.2006.07.006. [DOI] [PubMed] [Google Scholar]
- 27.Moor B.K., Bouaicha S., Rothenfluh D.A., Sukthankar A., Gerber C. Is there an association between the individual anatomy of the scapula and the development of rotator cuff tears or osteoarthritis of the glenohumeral joint? A radiological study of the critical shoulder angle. The Bone Joint J. 2013;95(7):935–941. doi: 10.1302/0301-620X.95B7.31028. [DOI] [PubMed] [Google Scholar]
- 28.Li X., Olszewski N., Abdul-Rassoul H., Curry E.J., Galvin J.W., Eichinger J.K. Relationship between the critical shoulder angle and shoulder disease. JBJS Rev. 2018;6(8) doi: 10.2106/JBJS.RVW.17.00161. e1-e1. [DOI] [PubMed] [Google Scholar]
- 29.Moor B.K., Röthlisberger M., Müller D.A. Age, trauma and the critical shoulder angle accurately predict supraspinatus tendon tears. J Orthop Traumatol: Surg Res. 2014;100(5):489–494. doi: 10.1016/j.otsr.2014.03.022. [DOI] [PubMed] [Google Scholar]