

Abstract
Background:
Obsessive-compulsive disorder (OCD) is associated with affective and cognitive symptoms causing personal distress and reduced global functioning. These have considerable societal costs due to healthcare service utilization.
Objective:
Our aim was to assess the efficacy of pharmacological interventions in OCD and clinical guidelines, providing a comprehensive overview of this field.
Methods:
We searched the PubMed database for papers dealing with drug treatment of OCD, with a specific focus on clinical guidelines, treatments with antidepressants, antipsychotics, mood stabilizers, off-label medications, and pharmacogenomics.
Results:
Prolonged administration of selective serotonin reuptake inhibitors (SSRIs) is most effective. Better results can be obtained with a SSRI combined with cognitive behavioral therapy (CBT) or the similarly oriented exposure and response prevention (ERP). Refractory OCD could be treated with different strategies, including a switch to another SSRI or clomipramine, or augmentation with an atypical antipsychotic. The addition of medications other than antipsychotics or intravenous antidepressant administration needs further investigation, as the evidence is inconsistent. Pharmacogenomics and personalization of therapy could reduce treatment resistance.
Conclusions:
SSRI/clomipramine in combination with CBT/ERP is associated with the optimal response compared to each treatment alone or to other treatments. New strategies for refractory OCD are needed. The role of pharmacogenomics could become preponderant in the coming years.
Keywords: Obsessive compulsive disorder, psychopharmacology, pharmacogenomics, selective serotonin reuptake inhibitors, atypical antipsychotics, off-label treatments
1. INTRODUCTION
Obsessive-Compulsive Disorder (OCD) is a psychiatric disorder included in the DSM-5 Obsessive-Compulsive Spectrum Disorders. The main symptoms include intrusive thoughts (obsessions), and ritualistic behavior (compulsions) [1]. OCD affects more than 1% of the population worldwide [2, 3], with lifetime prevalence of 2-3% in the general population [4], and no difference in gender distribution, although
juvenile-onset OCD is more often familial and more prevalent in boys than in girls [5, 6]. Age at OCD onset is bimodal, with the first peak in late childhood or early adolescence, and the second in early adulthood (i.e., 20-29 years) [7, 8]. Onset is usually gradual and its clinical presentation in child-onset and adult-onset forms is generally similar [1]. However, these differ in associated comorbidities [5]. Illness course has a chronic but fluctuating pattern, which often relates to stressful life events [9, 10].
The life of patients with OCD is characterized by more years of disability than that of patients with multiple sclerosis and Parkinson disease combined [11, 12]. Despite the illness burden, it is often unrecognized or misrecognized in both primary and psychiatric settings, since its symptoms are often internally rather than externally expressed, and because many patients manifest self-stigma (symptoms experienced with shame, embarrassment, or guilt) [12-15]. Consequently, the mean time from OCD onset to introduction of a pharmacological treatment is nearly eight years [12, 16, 17]. Less than 40% of patients coming to clinician’s attention receive OCD-specific therapy, and less than 10% obtain evidence-based treatment [12, 18]. Epidemiological studies suggest that over 50% of patients with OCD have at least one comorbid psychiatric disorder, most commonly an anxiety disorder or major depressive disorder. Moreover, alcohol use disorder is more frequent in OCD than in the general population [19].
A preponderance of evidence supports the combined OCD treatment with selective serotonin reuptake inhibitors (SSRIs) and cognitive behavioral approaches. Most patients show symptom improvement with these interventions, either alone or in combination [20]. Given this, clinical practice usually consists of combining SSRI treatment with cognitive behavioral therapy (CBT) [21]. However, even when a theoretically appropriate treatment is established, 40-60% of OCD patients exhibit disabling residual symptoms, indicating the need for innovative pharmacological treatments, different augmentation strategies, and novel physical treatment techniques [12, 22].
The aim of this article is to provide a comprehensive review of the developments in the pharmacological management of OCD in adults within the past 10 years. We reviewed the most recent evidence of the effectiveness of antidepressant, antipsychotic, and mood stabilizing drugs, as well as off-label drug treatment. We summarized clinical guidelines and highlighted the possibilities of a positive impact of pharmacogenomics and of personalized mental health approaches.
2. METHODS
2.1. Study Selection
We performed a PubMed search to identify peer-reviewed studies investigating psychopharmacological treatments in adult patients with OCD. We used a stepwise procedure to identify relevant experimental articles focusing on OCD psychopharmacology. First, we identified studies in the last 10 years through a standard search with the title-abstract specification in PubMed (http://www.pubmed.gov). On 25 February 2017 we performed a search including the terms ‘obsessive compulsive disorder’, ‘pharmacol*’, ‘antidepress*’, ‘antipsych*’, ‘lithium’, ‘stabilis(z)er’, ‘antiepilept*’, and excluding the terms ‘p(a)ediatr*’, ‘child*’, ‘case report’, ‘tourette’, ‘schizophr*’, ‘bipolar’, ‘epilepsy’, ‘neuropsychol*’, ‘personality disorder’, ‘dTMS’, ‘rTMS’, ‘stimulation’, ‘ECT’, ‘surgery’, ‘*tomy’, ‘mice’, ‘animal’, ‘rat’, ‘dysmorphic’, ‘somatic symptom disorder’, ‘hoarding’, ‘skin’, ‘neuroimaging’. We retrieved 266 papers. We included pharmacological trials, and systematic reviews and meta-analyses. We excluded papers that included child/adolescent patients, case reports, diagnoses of Tourette syndrome, dysmorphic, hoarding, excoriation (skin picking), nail biting, personality, somatic symptom and other OCD spectrum disorders, schizophrenia, bipolar disorders, and epilepsy. We also excluded transcranial magnetic stimulations, surgery, neuroimaging, psychometrics, and animal studies. We excluded 182 studies for not meeting our inclusion- and/or meeting our exclusion-criteria. Of these, 3 were animal studies; case reports, 9; focused on CBT or psychometrics, 14; neuroimaging, 13; not focused on OCD, 63; non-systematic reviews, 20; mainly focused on clinical or psychopathological aspects, or non-pharmacological studies, 58; 2 were focused on child/adolescent patients. Then, we searched for studies prior to the considered period in article references and on PubMed through the function “Similar articles”, further including 93 other studies on the basis of our inclusion and exclusion criteria. Based on these criteria, we finally included 177 papers focusing on OCD psychopharmacology (see PRISMA flow-chart, Fig. (1).
Fig. (1).
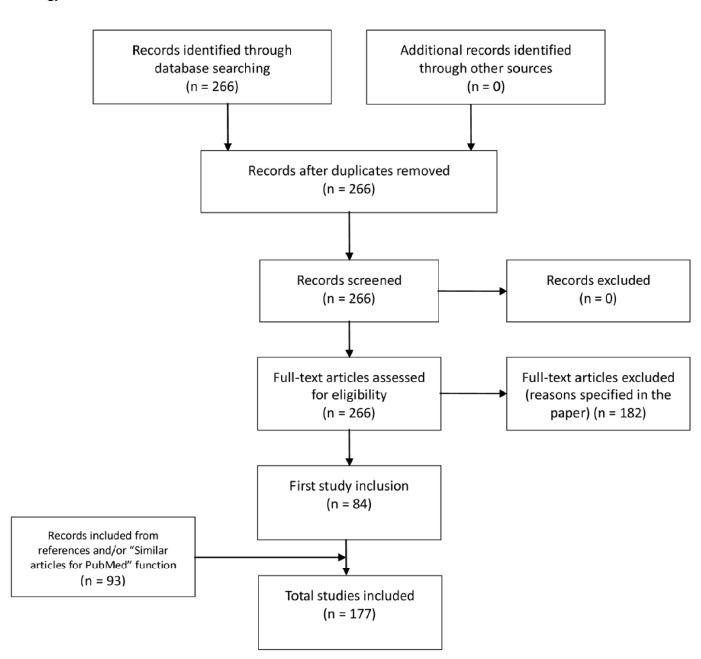
PRISMA flow diagram [362] showing search and inclusion strategy.
3. DISCUSSION
3.1. Antidepressant Medications
Changes in the serotonergic transmission, including the enhancement of postsynaptic signals induced by serotonin, have been associated with OC symptom improvement. In physiological neurotransmission, serotonin is transported from the synaptic cleft back to the presynaptic neuron through membrane transporter proteins and from there into the readily releasable synaptic pool through vesicular bioamine transporters. SSRIs can specifically block membrane transporters, resulting in an accumulation of serotonin in the synaptic cleft [23]. SSRIs are generally first-line, with good response rates and positive long-term results [23-25], despite the possible slight superiority of clomipramine in efficacy studies [26].
3.1.1. Selective Serotonin Reuptake Inhibitors (SSRIs)
Most of these drugs showed effectiveness in treating OCD both in the acute and in the maintenance phase and showed good tolerability. A Cochrane review confirmed the efficacy for all SSRIs (including citalopram, fluoxetine, fluvoxamine, paroxetine, and sertraline), without significant differences [27].
The response to SSRI treatment may be more delayed in patients with OCD than in those with major depression or anxiety disorders. However, a recent meta-analysis showed that a significant benefit from SSRI treatment compared to placebo occurred already after 2 weeks from the start of treatment [28]. Long-term treatment (24-52 weeks) with an SSRI compared to placebo was associated with significantly lower probability of relapse with SSRIs [29, 30]. SSRIs should be maintained at the maximum effective dose for at least 12 months. Treatment response is dose-related, with better clinical responses associated with higher dosages [29, 30], although lower doses (e.g., in the case of escitalopram) could be effective in preventing relapses [30]. OCD family history, aggressive, sexual, and religious obsessions, orbitofrontal cortex hypometabolism, and right caudate nucleus hypermetabolism correlated with high likelihood of responding to SSRI treatment [31, 32]. Hoarding behavior [33], poor insight, severe concomitant depressive episode [34], and higher levels of disability [35] correlated with limited SSRI treatment response.
Several studies have focused on paroxetine treatment of OCD. Doses of 20-60 mg/day generally correlated with significant symptom improvement. Paroxetine showed a marked anxiolytic effect and may be recommended as a first-line therapy in the treatment of OCD comorbidities [36]. It reduced avoidance related to phobic symptoms improving quality of life [37]. Its safety and long-term efficacy are supported by the literature [38]. It has been consistently associated with treatment response (i.e., drop of at least 25% on the Yale-Brown Obsessive-Compulsive Scale [Y-BOCS]) from baseline scores [25, 36, 39-42].
Placebo-controlled studies in OCD patients consistently associated fluvoxamine administration (dosage range 100-300 mg/day) with treatment response [43-47], although with some exceptions [48-52]. Fluvoxamine’s pharmacokinetic profile and its side effects may hinder rapid titration. The drug showed efficacy in social anxiety, avoidance, and phobic symptoms after 6-8 weeks of treatment and subsequently was associated with further improvement [53]. Long-term treatment (40-weeks with a dose of 100-300 mg/day) was associated with improvements of psychosocial skills and obsessive symptoms [54].
Citalopram proved to be effective in the treatment of OCD [55], with best results at doses of 60 mg/day [56], which correlated with improvements on psychosocial functioning, depressive symptoms, obsessive thoughts, repetitive behavior, and anxiety. It showed good tolerability [57] and appeared to be effective in patients with refractory OCD [58].
Escitalopram showed favorable pharmacokinetics and good tolerability. It is the most 5-HT-selective among SSRIs, with little or no affinity for other transmitter transporters or receptors [59]. Compared to other SSRIs, escitalopram may have weak or minimal interactions with the cytochrome P450 system [60, 61]. In a randomized, double-blind, placebo-controlled 24-week trial in OCD, escitalopram (20 mg/day) was associated with an increase in response rate compared to placebo after 12 weeks. Other placebo-controlled studies consistently showed escitalopram-related treatment response [25, 30]. 20 mg/day escitalopram has also been associated with better OCD symptom remission compared to 40 mg/day paroxetine or placebo at week 12 [30]. Three different escitalopram dosages (5, 10, and 20 mg/day) were compared with a fixed, 20 mg/day dose of paroxetine in a 12-week study, in which escitalopram showed both greater efficacy and better tolerability [62].
Fluoxetine was shown to be safe and effective at a dose of 40-60 mg/day [63, 64]. The effects of fluoxetine on different clinical OCD subtypes have been studied, showing improvement of obsessive thoughts, washing compulsions, psychosocial functioning, and quality of life [65]. Regarding the management of phobic symptoms, fluoxetine has been shown to be equally effective in both the short- and the medium-term (24 weeks), both in monotherapy and in combination with CBT [66]. Placebo-controlled studies consistently associated the administration of fluoxetine with treatment response (drop of at least 25% on the Y-BOCS from baseline) [63, 64, 67-69], although with some exception [70, 71]. Fluoxetine proved to be useful and safe in preventing recurrence of obsessive symptoms in patients who responded to short-term administration. The low overall relapse rates were evident at the maintenance dose of 40 mg/day, although 60 mg/day seemed to provide more protection.
Sertraline has shown efficacy and safety at doses of 50-200 mg/day [72] in treating phobic-related states, with a greater reduction in symptoms related to anxiety/fear, physical symptoms and avoidance behaviors [73]. Clinical improvements in obsessive symptoms and phobic behavior have been achieved with long-term therapy, with a good tolerability profile. A rapid sertraline titration up to 200 mg/day correlated with fast response rates. A 20-week study with sertraline 50-200 mg/day produced significant improvements both in functioning and social skills [74]. Stable sertraline treatment guaranteed lower recurrence rates, and a general improvement in quality of life. Placebo-controlled studies consistently showed sertraline-related treatment response [72, 75, 76], although with one exception [77]. Treatment of refractory OCD with high doses of sertraline (250-400 mg/day) resulted in a significant symptom improvement and a similar rate of adverse events observed with a 200 mg/day dose [78].
3.1.2. Clomipramine
Clomipramine, a tricyclic antidepressant (TCA) with a transporter blockade profile that is much similar to the profiles of most SSRIs as far as the serotonin/noradrenaline ratio is concerned [38], placing it midway between SSRIs and SNRIs and quite far from other TCAs, was the first drug used to treat OCD. In addition, one of the primary metabolites of clomipramine, desmethylclomipramine, is a potent noradrenaline uptake blocker [26]. It has a unique anti-obsessive effect due to its potent inhibition of serotonin reuptake, and this action has drawn attention to a possible role of serotonin in the neuropathophysiology of OCD [79]. The efficacy of clomipramine in treating OCD is well supported by the literature [26]. Among studies, a multicenter double blind, randomized, placebo-controlled trial conducted in 122 OCD patients compared clomipramine vs. exposure and response prevention (ERP) vs. ERP plus clomipramine combination vs. placebo. The study provided ERP for four weeks, with subsequent maintenance sessions for eight weeks and/or clomipramine (up to 250 mg/day) treatment for 12 weeks. At week 12, all active treatments proved to be superior to placebo. ERP did not show differences from clomipramine+ERP combination, which were more effective than clomipramine only [80]. Other data also showed that intravenous clomipramine could be effective in treating refractory OCD [81]. A 10-week double-blind, placebo-controlled trial conducted on 27 OCD outpatients treated with oral clomipramine showed that the drug was significantly superior to placebo [82]. Another 10-week double-blind study on thirty-two OCD patients without depression showed that the treatment with clomipramine was associated with significant improvement in OCD symptoms, although with more frequent and severe side effects than placebo [83]. Two multicentre (21 sites) double-blind studies focused on the efficacy, safety, and tolerability of clomipramine (up to 300 mg/day) vs. placebo in 520 OCD patients, of whom 239 with more than two years of illness (study 1), and 281 between one and two years of illness (study 2). Both studies demonstrated that clomipramine was significantly more effective than placebo. Among the most frequent clomipramine-related adverse effects (similar to the other tricyclic antidepressants), seizures and aminotransferase augmentation were the most dangerous. However, clomipramine was generally well-tolerated [84]. One more double-blind placebo-controlled study conducted on 25 patients with OCD for 10 weeks showed that clomipramine treatment vs. placebo significantly improved symptoms. Side effects mainly included heart rate increase. The authors showed clomipramine-related attenuation of autonomic reactivity to stressors, which they interpreted as a direct autonomic effect of clomipramine or an increased unresponsiveness to psychological stressors [85]. Twenty-five OCD patients with moderate to severe symptoms and at least 2 years of illness duration were involved in a double blind, placebo-controlled, 10-week study that showed the superiority of clomipramine over placebo. Another analysis focused on symptoms outcome and plasma drug concentrations in 33 OCD patients taking clomipramine showed that clomipramine plasma concentrations directly correlated with outcome measures. Patients with treatment response significantly showed higher plasma clomipramine and a trend toward lower desmethylclomipramine [86].
Clomipramine has been compared to paroxetine in a multinational randomised study involving 406 subjects with OCD of at least six months duration received double-blind medication for up to 12 weeks and doses adjusted according to therapeutic effect and side-effects. Both treatments proved to be an appropriate treatment for OCD [39].
Summarising, the efficacy of clomipramine in OCD is consistently reported and appeared to be equivalent to or slightly better than that of SSRIs, although its side effect profile is less favorable [39, 80, 82-86].
3.1.3. Serotonin–Norepinephrine Reuptake Inhibitors (SNRIs)
SNRIs combine the actions of SSRIs with inhibition of noradrenaline reuptake. These drugs have little effect on the activity of α1-adrenergic, muscarinic cholinergic or histaminergic receptors, thus showing better tolerability than clomipramine.
Venlafaxine short-term treatment of OCD showed similar efficacy to clomipramine, although with a more favorable safety profile [87]. Most studies have shown efficacy in both naïve and treatment-resistant OCD patients at daily dosages between 150 mg/day and 375 mg/day with satisfactory response rates (30-60%) [88-92]. OCD treatment with 300 mg/day venlafaxine compared to 60 mg/day paroxetine showed similar response rates, although paroxetine may be more effective than venlafaxine in refractory patients [93]. Duloxetine has shown some efficacy in the treatment of OCD, although most evidence comes from case reports or studies with small samples [94-96].
Some preliminary reports focused on OCD treatment with milnacipran, which has a recognized efficacy in fibromyalgia and major depression [97]. Milnacipran is used much in France, Canada and Japan, but its usefulness in OCD needs further examination.
3.1.4. Other Antidepressants
Agomelatine 5-HT2C antagonism could mediate anxiolytic effects, and melatonin modulation (MT1 and MT2 receptors antagonism) could contribute to circadian rhythm restoration in OCD patients [98]. It has been tested both in substitution [99] and in addition [100] to standard SSRI treatment, and to clomipramine [101]. Other antidepressants showed little or no effects in OCD. A double-blind discontinuation study showed for mirtazapine a significantly better effect of the drug with respect to placebo on Y-BOCS scores [102]. Another double-blind study showed poor improvement of obsessive-compulsive symptoms with trazodone [103]. Many antidepressants were reported to be useful mainly as add-ons on established pharmacotherapy in the attempt to overcome treatment-resistance in case reports, but none showed efficacy in double-blind studies.
3.1.5. Antidepressants in Refractory OCD
A management strategy for treatment-resistant OCD may consist of adding SSRIs to other drugs that further enhance serotoninergic transmission [104]. Some open studies suggested that the combined treatment with clomipramine and an SSRI is effective and well tolerated. Positive results have been reported with the addition of citalopram to clomipramine in the long term [58]. Encouraging data were also reported with the combination of clomipramine with fluoxetine or sertraline [54]. In any case, add-on treatment on clomipramine requires careful clinical monitoring [81].
Intravenous antidepressant administration, including clomipramine and citalopram, was associated with faster response, but eventually, with continued treatment, the result is similar to oral administration [105, 106]. Intravenous vs. oral clomipramine was more effective in two double-blind placebo-controlled studies [107, 108]. Treatment with high doses of serotonin reuptake inhibitors is another strategy to consider, including 250-400 mg/day sertraline [78], and 30-50 mg/day escitalopram [109, 110]. There is no evidence that switching from one first-line drug to another can produce benefits. Lower response rates were reported after switching from one SSRI to another, as compared to the shift from an SSRI to clomipramine [76]. Summarizing the evidence, it appears that the last resort could be clomipramine.
4. ADD-ON ANTIPSYCHOTIC TREATMENTS
About 40-60% of OCD patients do not satisfactorily respond to monotherapy with serotonergic drugs [111], considering for response a reduction of at least 25-35% of the values of the Y-BOCS [51]. The main lines of research on refractory OCD have focused on the study of psychotropic drugs as add-ons. The cortico-striatal OCD working model speculates on the existence of an imbalance of the direct vs. indirect pathway, with subsequent circuitry hyperactivations that may relate to OCD-related repetitive behaviors [112]. The amygdalocentric model hypothesises malfunctioning in the physiological top-down inhibition of the amygdala in OCD patients, which may relate to the more intrusive thoughts and chronic anxiety. Dysfunctional top-down inhibition of the amygdala may be affected by modifications of the mesolimbic dopaminergic system; increased dopamine adversely affects the ability of the prefrontal cortex to suppress anxiety-related activation of the amygdala [112]. Based on the hypotheses of dopaminergic hyperactivation in the etiology of the OCD, an important strategy is the use of antipsychotic drugs in add-ons to SSRIs.
4.1. Nosological Issues
From a clinical viewpoint, antipsychotics should be preferentially used for comorbid psychotic symptoms, which are not rare in OCD [113]. The overlap of symptoms between schizophrenia and OCD relates to difficulties in differential diagnosis and therapeutic management and constitutes an important research line of psychopathology since the beginning of modern psychiatry. “Folie raisonnante”, “folie lucide”, “folie avec conscience” already identified in the nineteenth century those clinical pictures between delusions and obsessions, in which ideas are egosyntonic and reality perception is preserved, and in which the diagnostic definition is borderline between neurosis and psychosis. Over time, increasing evidence indicated the existence of dynamic relationships between obsessive and psychotic symptoms, with the use of several terms, such as “obsessive psychosis”, “OCD with prevalent ideas”, “OCD with psychotic aspects”. Recently, the definition “OCD with poor insight” distinguishes an “atypical” subtype of OCD, which relates to worse outcome. It is characterized by the coexistence of compulsive obsessions and rituals with psychotic symptoms or by obsessions (considered realistic and reasonable by patients) that can be comparable to delusions or hallucinations [114, 115]. Conversely, prevalence of obsessive-compulsive symptoms/OCD is high in patients with schizophrenia [116]. According to a psychodynamic interpretation, obsessive-compulsive rituals could protect patients with schizophrenia from psychotic breakdown. The neuropathophysiology of these disorders involves the dopaminergic and serotonergic neurotransmitter systems, which are mutually interacting [117].
Overall, the manifestation of psychotic symptoms affects 1-12% of patients with OCD [118-121]. This subgroup has an earlier onset, a greater impairment of functioning at work, more severe depressive symptoms and a more frequent chronic course. It is also correlated to specific basic symptoms (mainly cognitive, thought and perception disorders) and schizotypal personality disorder [122-124]. Ganesan et al. [125] suggested that the manifestation of psychotic symptoms in OCD is an unfavorable prognostic factor, predicting worse illness course and poor response to standard treatments (both pharmacological and psychotherapeutic).
4.2. Guidelines
A short duration of SSRI therapy could be a source of bias because some patients may respond to these drugs more slowly than others. Hence, SSRIs should be administered for an adequate time before a treatment change. The American Psychiatric Association guidelines recommend a period of at least 8-12 weeks of SSRI treatment (with at least 4-6 weeks at the maximum tolerable dose) before considering a change in drug strategy [126]. Accordingly, in cases of partial initial treatment response, the addition of antipsychotics should be preferred over the switch to a different SSRI, which should be conducted only in case of non-response [126]. The World Federation of Societies of Biological Psychiatry (WFSBP) recommended a co-administration of SSRI-haloperidol, -quetiapine, -olanzapine or -risperidone for treatment-resistant OCD (grade 3 recommendation) [127].
To date, the addition of antipsychotics to standard serotonin enhancers is one of the most documented strategies for treatment-resistant OCD. The prevalence of antipsychotic prescriptions in OCD patients is currently high and increasing [128]. However, no antipsychotic agent is officially approved for the treatment of OCD. The use of add-on antipsychotics to SSRIs in OCD with comorbid Body Dysmorphic Disorder needs further study [129].
4.3. Use of Add-on Antipsychotics in OCD
Albert et al. [130, 131], comparing the efficacy of various antipsychotics in different mental disorders, found a significant role of prolonged-release quetiapine, risperidone and aripiprazole as possible adjuvant alternatives in treatment-resistant OCD.
Consistent evidence of efficacy in resistant OCD is related to risperidone. Komossa et al. [132], comparing 11 RCTs that examined the efficacy of the add-on strategy with SGA versus placebo in about 400 cases of refractory OCD, indicated risperidone as the most promising augmenting agent. Quetiapine did not appear to improve the response to antidepressant treatment but was statistically superior to placebo in reducing the mean Y-BOCS score and showed positive effects on anxiety and depressive symptoms. The least advantageous option was the add-on with olanzapine, which showed less efficacy and tolerability, especially in terms of weight gain, although the data were too limited to draw definite conclusions [132]. Similar conclusions emerged from another meta-analysis [133], which examined 12 other RCTs evaluating add-on strategies with quetiapine, risperidone, olanzapine, aripiprazole and haloperidol in 394 treatment-resistant OCD patients. Overall, about a third of patients were benefiting from the augmentation strategy with average antipsychotic doses; risperidone was confirmed as a potential first choice, both for response rates and for total Y-BOCS score drop. Li et al. [134] compared the treatments with add-on risperidone (1 mg/day) and haloperidol (2 mg/day) in a crossover study. Both drugs were significantly effective on obsessive symptomatology, but only haloperidol significantly reduced the total Y-BOCS score. Placebo-controlled studies showed add-on risperidone to reduce more than 20% Y-BOCS scores [104, 135, 136], while other studies confirmed reduction of Y-BOCS, although to a lesser degree [137, 138]. On the other hand, risperidone induced significant improvements in depressive symptoms and was significantly more tolerable than haloperidol [139]. Maina et al. [140] compared risperidone and olanzapine as add-on to a SSRI, demonstrating a significant improvement in obsessive-compulsive symptomatology with each strategy. Selvi et al. [141] showed the superiority of add-on risperidone (3 mg/day) compared to aripiprazole (15 mg/day). A very low dose of risperidone (0.5 mg/day) added on standard SSRI treatment showed a greater effect size than a moderate dose [137], but placebo-controlled studies showed a greater effect of higher doses (2-3 mg/day) [104, 135, 136].
The literature is not consistent regarding the usefulness of adding quetiapine to a SSRI for the treatment of OCD. Vulink et al. [142] examined the effect of the combination of quetiapine with citalopram in patients with non-refractory OCD, showing a significantly higher efficacy of quetiapine compared to placebo. All but one [143] placebo-controlled studies of 50-500 mg/day add-on quetiapine on SSRIs showed a greater than 20% reduction of Y-BOCS scores of treatment-refractory OCD patients [139, 144-147]. Significant efficacy was not demonstrated for olanzapine and quetiapine in a first meta-analysis [133], but subsequently shown by a second one by the same group [148]. Still another meta-analysis [149] did not show efficacy for quetiapine or olanzapine compared to placebo. Other studies showed remarkable response rates in treatment-resistant OCD with add-on antipsychotic treatment. Haloperidol [150], quetiapine [144, 151], olanzapine [152], and amisulpiride [153] have shown efficacy in more than 40% of treated patients. After 6 months of add-on to high-dose SSRIs treatment, ziprasidone was less effective than quetiapine in patients with resistant OCD (44.4% vs. 80% clinical response) [139].
Add-on aripiprazole to SSRIs has shown encouraging results in the treatment of resistant OCD. The efficacy of aripiprazole has been also observed for the treatment of compulsive obsessive symptoms in patients with bipolar disorder [154], schizophrenia [155], or children with Tic disorders [156]. Its therapeutic role in refractory OCD was initially evaluated as monotherapy. Already the first studies showed greater efficacy of aripiprazole in augmentation to antidepressant drugs rather than in monotherapy [157-163]. A recent meta-analysis showed that 10 mg/day aripiprazole was the most effective short-term option with an important overall effect size [149]. Risperidone also showed a small effect size in the short term in this study. Treatment with aripiprazole at a dose of 5-20 mg/day added on to paroxetine, fluvoxamine or clomipramine showed high response rates [164]. Aripiprazole was also well tolerated and the most commonly observed adverse reactions were akathisia, nausea, vomiting, and agitation [164]. Aripiprazole in addition to SSRIs showed significant improvements in obsessive-compulsive symptoms also in the midterm (12 months follow-up) [162, 165]. Confirmations of efficacy and tolerability of low doses of add-on aripiprazole (10 mg/day) in severe, treatment-resistant OCD also derive from other two randomized double-blind placebo-controlled trials [166, 167]. Compared to other antipsychotics, aripiprazole showed a lower risk of weight gain, sedation, and prolactin increase [168]. Long-term follow-up studies are needed to assess the efficacy and safety of aripiprazole added on to SSRIs in treatment-resistant OCD.
Overall, antipsychotics as augmenting agents compared to placebo showed a statistical superiority in terms of clinical improvement. Haloperidol, risperidone and aripiprazole showed more consistent positive effects on refractory OCD as add-ons. For other antipsychotics, like quetiapine, olanzapine, and paliperidone the evidence is less compelling, and some studies showed they did not significantly differ from placebo [138, 148, 167, 169]. In summary, the most recent studies suggested that risperidone and aripiprazole might be used as add-on agents to SSRIs/CBT in resistant OCD patients.
4.4. Clozapine and Clozapine-related Obsessive-compulsive Syndrome (OCS)
Clozapine is not recommended for OCD due to poor evidence of efficacy [170]. In addition, several case reports and clinical studies support the association of clozapine with worsening or onset of obsessive-compulsive symptoms in patients with a psychotic disorder [171-176]. At least 20% of individuals treated with clozapine (and other antiserotonergic antipsychotics) would experience worsening or emergence of obsessive-compulsive symptoms [177], which are dose-related [178] and generally reversible upon discontinuation of clozapine treatment and switch to a different antipsychotic [179]. The mechanism by which clozapine and other second-generation antipsychotics (SGAs) can induce or worsen obsessive-compulsive symptoms is unclear and probably related to 5-HT2A receptor blockade in areas known to be involved in the neuropathophysiology of OCD, such as the anterior cingulate cortex, the dorsal posterior prefrontal cortex and the orbitofrontal cortex [180-182]. Supporting the antiserotonergic hypothesis, there is evidence that first-generation antipsychotics (FGAs), which mainly have dopaminergic actions, are not implicated in iatrogenic OCS [183]. Patients exposed to a potent dopamine antagonist before clozapine would be more susceptible to the development of clozapine-induced OCS, pointing to hypersensitisation. The use of clozapine following the upregulation of striatal D2 receptors induced by chronic FGA exposure would result in a reduction of the dopaminergic block with consequent OCS. Finally, polymorphisms of various genes (i.e., SLC1A1, GRIN2B and GRIK2) may be related to clozapine-induced OCS [184].
OCS induced by clozapine should not be confused with worsening of psychosis; in fact, one would be prompted to increase dosages to obtain proper antipsychotics that could be associated with further symptom worsening. Clozapine-related OCS should not lead to clozapine withdrawal when primary psychotic symptomatology has clearly benefitted. Therapeutic options for clozapine-induced OCS include dosage reduction [185], introduction of a serotonin enhancer [186], or aripiprazole [187], which could be effective due to its partial 5-HT1A agonism, cautiously considering potential pharmacokinetic interactions. The possible introduction of fluoxetine, paroxetine or clomipramine deserves caution due to the mild-to-moderate inhibition of clozapine metabolism by these drugs [188, 189]. Fluvoxamine should be avoided, as it is a potent inhibitor of clozapine metabolism and may cause toxicity [190]. Some case reports described other clozapine-induced OCS management modalities, including the introduction of valproic acid and the use of electroconvulsive therapy [191, 192].
4.5. Pharmacodynamics
The mechanism of action of SGAs is the combination of D2 and 5-HT2A antagonism. To date, it is not clear which receptor, in addition to the serotonin uptake inhibition related to SSRI treatment, is at the heart of the therapeutic effects in resistant OCD. Haloperidol has slightly more affinity for D2 receptors than olanzapine and risperidone and much more than quetiapine. Since response rates to haloperidol and risperidone were found to be higher than those of quetiapine and olanzapine in meta-analytical studies, it can be assumed that besides antidopaminergic activity, there must be other mechanisms supporting the anti-psychotic efficacy of the former drugs in treatment-resistant OCD. The antidopaminergic hypothesis is supported by an open-label augmentation study with 200-600 mg/day amisulpiride, a selective and potent blocker of the D2 and D3 receptors, which showed promising results [153]. Since amisulpiride, like other substituted benzoamides, is highly specific for dopamine receptors, this would seem to confirm the involvement of D2 antagonism in the therapeutic action in resistant OCD. However, the study was not double blind, so the efficacy of amisulpiride in this condition remains undetermined.
According to positron emission tomography (PET) studies, low doses of atypical antipsychotics induced high levels of 5-HT2A/C antagonism, while relatively higher doses are necessary to determine significant blockade of D2 receptors [193]. However, SGAs were effective augmentation agents in treatment-resistant OCD at medium doses, lower than those currently recommended for the treatment of psychotic disorders, similarly to what occurs in the treatment of major depression. Both haloperidol (strong D2 and moderate 5-HT2A receptor blocker) and aripiprazole (the most peculiar among SGAs in terms of effects on D2, 5-HT1A, 5-HT2A, and 5-HT2C receptors) proved to be useful in refractory OCD. This could indicate that antipsychotic augmentation in OCD treatment mainly relies on the modulation of the interplay of serotonergic and dopaminergic transmissions [149]. Furthermore, since low doses of antipsychotics primarily antagonize the presynaptic dopamine autoreceptor, this mechanism is more likely to increase or modulate rather than antagonize dopaminergic transmission. The promising results of aripiprazole added on SSRI treatment may relate to its peculiar partial agonism of D2 and 5-HT1A receptors and antagonism of 5-HT2A/2C receptors.
4.6. Limitations
Different studies produced inconsistent results and were limited by small samples of treatment-resistant OCD patients, multiplicity of study designs, inconsistent definitions of treatment resistance, lack of homogeneity in the adopted response criteria, and heterogeneity of the clinical pictures of included OCD patients. Some symptom subsets may differently respond to a specific treatment, even if symptoms overlap and vary in severity. To date, there is no genotype or phenotype identified as a predictor of add-on antipsychotic treatment efficacy in resistant OCD. A further limitation is the variability of inclusion and exclusion criteria regarding comorbidities particularly tic disorders. Tourette and tic disorders tend to co-occur with OCD and are usually treated with antipsychotic drugs; it should be considered that OCD patients with comorbid tic disorder benefit more from additional antipsychotic drugs than patients with OCD without tic disorders [194].
4.7. Future Directions
There is a lack of studies focusing on high-dose antipsychotics in refractory OCD, and we cannot exclude that this strategy may increase the proportion of responders. Further studies are needed addressing these issues to allow for the optimization of treatment recommendations for refractory OCD. Considering the possibly low overall response to SSRI monotherapy, early co-administration of antipsychotics is a commonly recommended strategy for treatment-resistant OCD. There is still no precise guideline about antipsychotic choice, neither on optimal dosing, nor on appropriate treatment duration or long-term safety of increasing antipsychotic doses. Further investigations are needed to clarify the efficacy and safety of each antipsychotic drug and establish possible differences. There are no studies with a very long-term follow-up investigating the outcome or adverse events of add-on antipsychotics. Although benefits have been found, especially for aripiprazole and risperidone, potential long-term risks are not known. After one year of treatment, quetiapine, risperidone and olanzapine added on CBT and SSRIs in non-responder patients were associated with symptom improvement, but also with increases in body mass index (over 10%) and fasting blood glucose levels in more than half of treated patients [195]. The potential benefits of antipsychotic medications should be carefully balanced against the risk of side effects. Should a patient with standard treatment-resistance be judged to respond to a 4-week add-on antipsychotic, he/she should be advised to regularly monitor weight, blood glucose, and blood lipid profile; the clinician should monitor the patient for possible long-term adverse effects.
Alternative strategies to antipsychotic augmentation may be more efficacious and safer in the long run. For example, CBT showed more efficacy and less side effects than risperidone or placebo [138], which prompted the investigators to provide non-pharmacological treatment first, thus defining treatment-resistant patients as those who also had evidence of a failed CBT course. However, this study is flawed by the fact that there is no such a thing as a blind sham psychotherapy administration, so conclusions should be avoided. Investigators should be prompted to speak about drug-resistance when only drugs have been tried and of treatment resistance when all possible treatments have failed, otherwise they should define resistance as SSRI-, psychotherapy (CBT/ERP)- or somatic (TMS, DBS, ECT, or psychosurgery)-treatment–resistance (i.e., they should be more specific in their definition of a resistant/refractory patient in the titles of the articles they publish). Some evidence supported the add-on of clomipramine to a SSRI before trying an antipsychotic add-on treatment. The addition of clomipramine (25-75 mg/day) to fluoxetine showed more effectiveness than add-on quetiapine [196]; also, the use of add-on clomipramine to citalopram was superior to citalopram alone [197]. In such cases, a combination with clomipramine requires ECG monitoring [197], but this is just one of the precautions that should be taken, as this type of practice exposes the patient to the risk of a serotonin syndrome [198, 199].
To date, more data are needed to predict the response to SGAs in add-on to standard treatment. Further studies are needed to identify subgroups of patients that could benefit from this treatment option [200]. Further evidence showed that reducing the dose of SSRI after the introduction of an antipsychotic does not improve response to treatment [196]. Taking into account the chemical and pharmacodynamic heterogeneity of the SSRIs as a class, further studies should evaluate which of them is the most suitable for antipsychotic augmentation in refractory OCD.
5. OTHER ADD-ON PHARMACOLOGICAL TREATMENTS
5.1. Antiepileptics
Considering the significant proportion of drug-resistant OCD patients, further treatment strategies have been attempted, including augmentation with antiepileptic drugs. Overactivation of the cortico-striatal-thalamo-cortical circuit, in which a role could be played by glutamate, is apparently involved in OCD, justifying the assumption that antiepileptic medications antagonizing glutamatergic activity could reduce OCD symptoms [181, 182, 201].
Add-on topiramate at daily dose ranges up to 400 mg improved refractory OCD [201-204]. One study reported a positive effect of 225-675 mg/day pregabalin augmentation in 10 partial responder/resistant OCD patients to combined SSRI/SGA treatment [205].
Lamotrigine at 150 mg/day added on 225 mg/day clomipramine [206] in a case and at 100-200 mg/day added to the same clomipramine dose or to 60 mg/day paroxetine in two cases [207] obtained improvement; this was further confirmed in two placebo-controlled studies, both showing efficacy vs. placebo of 100 mg/day lamotrigine added on SSRIs in refractory OCD [208, 209]. The addition of gabapentin to fluoxetine reduced time to treatment response [210]. Deltito [211] (1994) reported that 8 of 10 patients who did not tolerate standard antiobsessional treatment, who were pretreated with valproate, responded to subsequent reintroduction of the antiobsessional with a reduction of OCD symptoms. Another report, in which one patient has been treated similarly; clinicians gradually tapered-off clomipramine and continued on valproate monotherapy, obtaining further reduction of obsessive-compulsive symptoms [212]. These finding have not been replicated to date.
5.2. Ondansetron
Ondansetron is a 5-HT3 serotonin receptor antagonist used primarily to reduce nausea and vomiting associated with chemotherapy, radiotherapy, post-surgery, and pregnancy. Since 5-HT3 blockade produces a weak inhibitory effect on dopaminergic neurotransmission [213], ondansetron has been tested in the treatment of schizophrenia [214], Tourette's disorder [215] tardive dyskinesia [216], alcoholism [217] (Johnson et al., 2011), and OCD [218]. Both uncontrolled and placebo-controlled studies showed that ondansetron was safe and effective in treating refractory OCD, both in monotherapy and added on SSRIs. In a pilot, 8-week, open-label trial, oral ondansetron monotherapy (3 mg/day) resulted in 29-55% reduction of Y-BOCS scores from baseline and to 45% worsening 2 weeks after suspension [219]. Fourteen patients with refractory OCD received ondansetron (0.5-1 mg/day) added on SSRIs and SGAs for 12 weeks, showing decrease of at least 23% of the Y-BOCS scores and some minor adverse events [220]. Twenty-one patients who did not respond adequately to a SSRI, received 12 weeks of 0.5-1 mg/day add-on ondansetron, obtaining a 27.2% average reduction of Y-BOCS (57% response rate). Four weeks after ondansetron discontinuation, Y-BOCS scores increased by 15.5% on the average in the entire sample and 38.3% in the responder sub-sample. No clinically significant side effects emerged [221].
Two RCTs investigated moderate-high (4-8 mg/day) doses ondansetron combination with SSRIs. In the first study [222], 42 patients with refractory OCD randomly received ondansetron 4 mg/day or placebo in addition to fluoxetine for 8 weeks, showing significant greater decrease of Y-BOCS scores with ondansetron compared to placebo. Heidari et al. [223] randomized 46 adults with severe refractory OCD to receive 8 mg/day ondansetron or placebo for 8 weeks in addition to 100-200 mg/day fluvoxamine. After 8 weeks of treatment the mean Y-BOCS scores dropped to 15 in the ondansetron group and to 21 in the placebo group; the Y-BOCS improvements that followed ondansetron vs. placebo were significant for obsessions, compulsions, and global symptoms. The efficacy of ondansetron in treating refractory OCD was superior in RCTs than in uncontrolled studies [220, 221]. Reported adverse events were very few and comparable between ondansetron and placebo. However, patients of uncontrolled studies had history of drug resistance, while RCTs did not report history of drug resistance and their patients were not taking medications in the six previous weeks, in spite of OCD severity. Moreover, ondansetron was given at higher doses in RCTs [222, 223] vs. uncontrolled studies [220, 221]. Ondansetron (1-8 mg/day) is a potential augmenting agent in patients for whom SGAs are problematic [224]. However, further studies are necessary to confirm these acquisitions, to establish long-term efficacy and safety, and to identify appropriate dosing and treatment duration.
5.3. Buprenorphine
The evidence for the use of buprenorphine and other opioids in the treatment of severe and refractory OCD is weak [225-229]. The mechanism underlying the therapeutic action of opiates in OCD is still debated. Buprenorphine, through partial agonism of the μ-opioid receptor, promotes the release of serotonin and dopamine in the central nervous system [230, 231]. Conversely, naloxone, i.e. a pure opioid antagonist with affinity for all three types of opioid receptors (μ, δ, κ) has been shown to rapidly worsen OCD symptoms [232, 233].
Buprenorphine 400-600 μg/day added on SSRIs (200 mg/day fluvoxamine or 200 mg/day sertraline) or 150 mg/day clomipramine correlated with improvement of symptoms in severe refractory OCD. Buprenorphine was administered at lower doses than those used to treat chronic pain, i.e., started at 200 μg/day, with the dosage doubled after one week, and further 200 μg/day increases based on clinical response [229]. Opioid treatment was not associated with significant side effects (cyclizine was prescribed in the initial treatment phase in case of nausea) and improvement was maintained without tapering-off. Patients that did not respond to buprenorphine augmentation were affected by severe OCD, severe depression, and were resistant to SSRI treatments and CBT [229]. Add-on buprenorphine to standard OCD treatment may result in a clinically significant improvement in a proportion of refractory patients, particularly in people who partially responded to SSRIs. This observation supports the hypothesis of a close interaction between opioid and serotonergic systems; however, further trials are needed to better understand the role of the opioid system in OCD and related disorders.
5.4. D-cycloserine
An emerging therapeutic approach for patients with refractory anxiety disorders, OCD, and PTSD, is the treatment with D-cycloserine (DCS) added on CBT. Originally designed as anti-tuberculosis, DCS has been tested in Alzheimer's dementia and in the treatment of negative symptoms of schizophrenia [234, 235]. DCS did not show anxiolytic properties and is not considered a first-line strategy for anxiety disorders. However, favorable effects on anxious symptomatology could derive from DCS-related associative learning enhancement [236].
Animal studies showed DCS to enhance conditioned fear extinction learning, a central mechanism in ERP [237]. Partial agonism at the site of glycine recognition of the glutamatergic N-methyl-D-aspartate (NMDA) glutamate receptor, which is linked in the amygdala to learning and memory, could be the basis of the mechanism of action of DCS. NMDA antagonists, on the other hand, would block learning of the extinction of fear. Human studies showed the potential therapeutic role of DCS in anxiety disorders, although the effect size of DCS seemed to be less than animal studies [238]. A meta-analysis conducted on patients with OCD, PTSD, and severe anxiety disorders showed that add-on DCS improved ERP, facilitating the extinction of fear [239]. Of note, interactions of DCS with other psychotropic drugs require further investigation.
A study conducted by Anderson et al. [240] in 128 OCD patients who underwent 5 sessions of 12-week guided exposure and were on stable antidepressant therapy, suggested that DCS added on CBT could be a promising strategy only in patients who were not receiving antidepressants. Long-term administration of different classes of antidepressants, including imipramine and citalopram, alters NMDA receptor subunits and DCS regulation of the glycine binding site, blocking its facilitatory effect on fear extinction [241]. A recent meta-analysis conducted on 21 RCTs [242], which included 1047 subjects with a severe anxiety disorder or OCD or PTSD randomized to receive DCS or placebo in addition to CBT, showed add-on DCS to correlate with symptom improvement only from pre-treatment to post-treatment, but not from pre-treatment to mid-treatment or from pre-treatment to follow-up. The CBT group also showed lower severity of symptoms at the end of treatment and at follow-up. In this study, the concomitant use of antidepressants did not moderate the effect of DCS [242]. Other RCTs conducted on pure OCD samples showed that DCS augmentation may lead to a faster response to treatment than placebo, although without beneficial effects at the end of the treatment or at follow-up [243-247].
To date, DCS has proven to be a promising strategy for strengthening CBT. It could reduce the number of CBT sessions needed, reduce the exposure-related anxiety, and facilitate adherence to treatment, leading to faster patient relief and lower healthcare costs [248]. DCS appears to be effective when administered 1-2 hours before or after exposure (during the period of consolidation of the memory that occurs after exposure rather than during exposure itself) [238-249]. The possible efficacy of a small number of DCS administrations can be explained by the progressive receptor desensitization with continued use of the substance [238]. However, clinical research should be performed to indicate adequate protocols, treatment time, and DCS doses for refractory OCD.
Add-on DCS dosage range of 50-500 mg/day did not show significant differences in CBT enhancement [250]. For doses lower than 500 mg/day, DCS was well tolerated and no significant adverse effects were reported. DCS administration infrequently correlated with nightmares the night after the CBT session and euphoric mood with hyperactivation in a person with chronic depression [251]. Other reported unwanted effects were increased anxiety, somnolence, xerostomia [244], mild gastrointestinal disorders, dizziness, tiredness [243], and nausea during the hour following DCS administration [251]. De Kleine et al. [252] did not find differences between DCS and placebo groups regarding adverse events. Stable high DCS doses (500-1000 mg/day) were related to headache, confusion, tremor, memory difficulties, paraesthesia and seizures [253]. Furthermore, DCS in animals seems to induce tolerance when administered at high and/or chronic doses, probably due to a paradoxical antagonistic effect on NMDA receptor [254], with consequent fear extinction reduction [255]. In summary, due to the minimal side effects of low-dose DCS, this drug appears to be a safe alternative for improving CBT outcomes [246].
Many aspects need further investigation, including characteristics of patients who could potentially benefit from DCS in addition to CBT, considering that this treatment could be effective in subtypes of OCD with prevalent cleansing/contamination symptoms [256]. More studies are needed to evaluate treatment modalities, including the number of CBT sessions to perform, treatment time, DCS dosages, methods of administration (it is not yet known if DCS can be effective if administered only after successful sessions), and interactions of DCS with antidepressant treatments.
5.5. Cannabidiol
Activation of the CB1 cannabinoid receptors is involved in fear extinction and prevention of reconsolidation of fear [257], i.e., the negative feedback of the neuroendocrine stress response and the protection from the adverse effects of chronic stress [258, 259]. As a consequence, CB1 receptor agonists, including Δ9-tetrahydrocannabinol and cannabidiol, and synthetic agents capable of enhancing CB1 activation, such as fatty acid amide hydrolase inhibitors, are being evaluated as new anti-anxiety treatments [260-262]. Preclinical data showed that cannabidiol could be safe and effective in reducing fear- and anxiety-related behaviors in schizoaffective, post-traumatic stress, anxiety and obsessive-compulsive disorders [262, 263]. Further preclinical and clinical studies are needed to assess the usefulness of drugs targeting the cannabinoid system in some psychiatric disorders. To date, the use of cannabinoids in the treatment of OCD is not recommended, also in consideration of the related risk of psychosis [264]. However, the use of cannabidiol-like molecules alone should not pose such safety questions and may constitute a viable strategy for the future, not only in OCD, but in anxiety and psychotic disorders as well.
5.6. Other Medications
Different placebo-controlled studies showed some effectiveness in refractory OCD of add-on treatments with mavoglurat [265], eicosapentaenoic acid [266], celecoxib [267], L-carnosine [268], inositol [269], the 5-HT3 antagonist granisetron [270], the μ-opioid agonist morphine [228], and the β-adrenoceptor/5-HT1A antagonist pindolol [271].
Promising results from placebo-controlled studies concerning the efficacy of add-on treatments with memantine [272-274] and N-acetylcysteine [275-277] (however, the latter showed some inconsistencies [278]) need replication.
Other placebo-controlled studies showed lack of effectiveness of add-on buspirone [279, 280], clonazepam [281], glycine powder [282], lithium [283], naltrexone [284], and riluzole [285].
6. PERSONALIZED TREATMENT STRATEGIES
6.1. Treatment Response Prediction
Given the significant rate of treatment resistance and the significant disability in OCD patients, an improved knowledge of the predictive factors of drug treatment response could allow better improvement through the implementation of personalized therapeutic regimens. The identification of homogeneous subgroups of OCD patients could help finding treatment response predictors and selecting better personalized pharmacological treatment options [286].
Autogenic obsessions (A-OCD) are generally sexual, aggressive or immoral, intrusive, unrelated thoughts and impulses with identifiable triggers. These are associated with avoidant control, magical rituals, and superstitious behavior or through thought-control strategies, and frequently associated with schizotypal personality and disorders of thought or perception. Reactive obsessions (R-OCD) concern contamination, errors, accidents, symmetry and loss, and can be triggered by specific external stimuli. R-OCD can lead to coping behaviors such as trying to avoid or actually avoiding any negative consequences related to the meaning of thought, and are associated with perfectionist personality traits [287, 288]. A-OCD and R-OCD subtypes showed different neurobiological correlates [289, 290].
The current literature on the different therapeutic approaches to autogenic or reactive obsessions reports inconsistent results. Some studies suggested that A-OCD might not respond to ERP and SSRI as well as R-OCD [9, 291, 292], others showed no subtype differences [34, 55, 293]. The augmentation with a SGA showed more clinically relevant improvements in the A-OCD vs. R-OCD group [294]. The increased symptom severity and frequent association with schizotypal personality traits could explain the higher antipsychotic prescription rate in the A-OCD subtype [288]. However, the presence of mixed obsessions is frequent, and the OCD subtype may change over time [9]. Treatment strategies may not be adaptable to specific OCD subtypes of symptoms, given that many other factors may influence clinical response and outcome, including symptom severity [111], age of onset [294], co-occurrence of schizotypal personality disorder [295], chronic tics [150], and depression [296]. The debate on the potential role of the OCD subtypes in pharmacological treatment strategies requires further and more detailed studies.
To date, predictors of response to SSRIs include positive family history [34], aggressive, sexual and religious obsessions [31], and OFC hypometabolism and right caudate hypermetabolism [32]. On the other hand, a poorer response to SSRI has been related to prevalence of hoarding symptoms [33], lack of insight [34], severe concomitant depression [292], and higher levels of basic disability [35].
The most consistent predictor of add-on antipsychotic response is a comorbid tic disorder [194]. Few studies on add-on benzodiazepines, which are commonly considered ineffective [297], and glutamatergic agents [298, 299] cannot fully clarify specific predictors of treatment response.
6.2. Pharmacokinetics Factors
CYP2D6 metabolizes most of the antidepressants, such as TCAs, SNRIs and most SSRIs. CYP2C19 metabolizes several TCAs and some SSRIs, including escitalopram and citalopram. Gene polymorphisms of CYP2D6 and CYP2C19 alter the metabolism of drugs, influencing their efficacy and the profile of adverse effects. Other CYP450 enzymes (such as CYP1A2, CYP2B6, CYP2C9 and CYP3A4) may also play a role in metabolizing psychoactive drugs. CYP2D6 and CYP2C19 polymorphisms could be related to antidepressant response in OCD patients [300-302]. Reduced CYP2D6 function has been associated with lack of response, and non-extensive CYP2D6 metabolizers, compared to extensive, showed a significantly higher number of failed responses to different antidepressant drugs [302].
6.3. Pharmacodynamics Factors
The serotonergic system is involved in the pathogenesis of OCD; in fact, SSRIs are the first-line treatment of this disorder, which is widely supported by the literature [126]. Many genes have been found to regulate the expression and function of serotonin, including SLC6A4 and its promoter HTTLPR, HTR2A, HTR2C, HTR1B and TPH [303].
There is no evidence supporting the hypothesis that a single genetic variation or gene can be related to antidepressant responses in patients with OCD. However, several single-nucleotide polymorphisms (SNPs) of candidate genes within the neural aminergic systems and the CYP450 liver system might be involved with both OCD neuropathophysiology and treatment response [303]. The SLC6A4 gene (chromosome 17) encodes the serotonin transporter, which carries on the reuptake of serotonin [304]. A polymorphism in the promoter region of SLC6A4 influences gene expression, with the long allele (L) correlating with higher levels of serotonin transporter expression, which is up to three times
than those of the short allele (S) [305]. The variation of the activity of this transporter influences the availability of serotonin in the synaptic cleft, having an impact on the activity of postsynaptic receptors.
The association of 5-HTTLPR polymorphisms with OCD has been reported in the literature, although somewhat inconsistently, with some studies not showing any significant association and others indicating an association of the L-allele expression with OCD [306]. Higher diencephalic expression of the transporter prior to treatment may correlate with increased transporter occupation and better response to antidepressants (e.g., sertraline) [307]. HTR2A gene polymorphisms may also influence the response to SSRI treatment [308]. A single nucleotide polymorphism of the COMT gene was associated with response to citalopram, indicating that the Met/Met (L/L) genotype of the COMT Val158Met polymorphism could predict a better response to antidepressant treatment [309].
There is increasing evidence of the role of the glutamatergic system in the etiology of many neuropsychiatric disorders, including OCD [310]. In fact, altered glutamatergic function is seen as one of the main biological correlates of hyperactivity of the cortico-striatal-thalamo-cortical circuit [311]. Drugs interfering with the glutamatergic system (such as phenobarbital, lamotrigine, topiramate, riluzole, N-acetylcysteine, memantine, ketamine, and DCS) have been used as potentiating agents in refractory OCD. Different haplotypes of the SLC1A1 gene, which encodes the neural glutamate transporter, have been associated with OCD [312].
Neurodevelopmental changes in ventral prefrontal-striatal circuitry causing developmentally-mediated network dysplasias were advanced to account for the onset of OCD [313]. This hypothesis received support from both neuroimaging [314] and genetic studies [315-317]. A study by Qin et al. [318] demonstrated that the top SNP associated with the response to SSRIs was rs17162912 (i.e., an intergene variation near the DISP1 gene), which is involved in neurodevelopmental cell-cell interaction [319].
Briefly, pharmacogenetics and personalised medicine may radically change the clinical practice for treating OCD, guiding physicians to indicate the best antidepressant treatment (and perhaps also alternative augmenting strategies) for each patient [303]. The continuous and rapid development of genomic testing and related studies focused on predictive factors, association studies, and pharmacoeconomy will prove or disprove the validity of the personalised approach in mental health. An important question regarding timing (i.e., when a psychiatrist should indicate a pharmacogenomic test) is still unclear [320].
Although no published studies to date examined this issue in OCD, pharmacogenomics in psychiatry can lead to improvement in patients’ adherence to treatment, decreases in healthcare costs [321], and better response to antidepressants in major depression [322]. Because of the lack of pharmacogenomic studies in OCD, we hypothesise that this method could at least be considered when a patient is refractory to the switch to a second SSRI, clomipramine, or SSRI/clomipramine with add-on atypical antipsychotics Fig. (2).
Fig. (2).
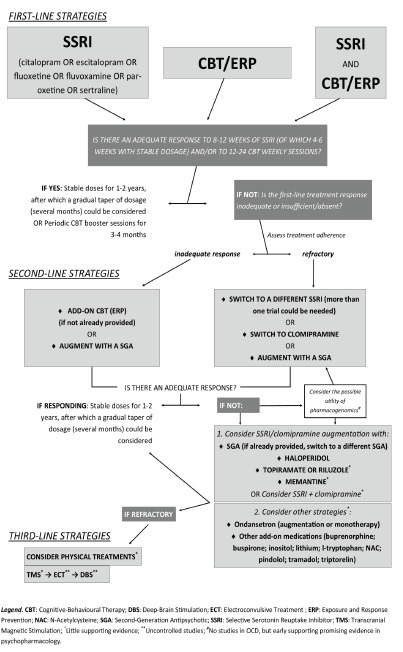
Algorithm on OCD treatment strategies.
6.4. OCD Treatment During Pregnancy
OCD is relatively common during the perinatal period. Pregnancy and postpartum are associated with higher risk of OCD onset [323] or recurrence, although some patients present symptom improvement [324-326]. Data on the safety and efficacy of OCD treatment during pregnancy are limited and mainly derive from retrospective studies. Furthermore, safety data of drug treatment during pregnancy mainly come from studies focused on other psychiatric disorders, and it is not certain that drug safety does not vary according to the specific disorder. Few data exist about the effects of untreated OCD during pregnancy on fetal and child development.
Stress and anxiety during pregnancy correlate with increased resistance to placental blood flow, preterm birth, low gestational age, and increased risk of placental detachment; sleep and eating disorders, ADHD and cognitive-behavioral and emotional problems may occur in the child [327-331]. Newborns of women with OCD showed significantly lower birth weight compared to controls and higher levels of the proinflammatory cytokine tumor necrosis factor-alpha (TNF-α) [332]. These findings suggest that maternal OCD can potentially influence future child neurodevelopment; however, conclusions cannot be drawn due to the lack of studies in literature on this topic.
Factors to be considered in treatment strategy decisions are family psychiatric history, previous adverse reactions to drug treatment, risks related to untreated maternal OCD, safety and effectiveness of drugs during pregnancy, the availability of non-pharmacological treatments [333], OCD severity, and related reduced global functioning [334]. Pharmacological treatment should be indicated in cases of severe depression and anxiety, elevated risk of suicide, OCD-related sleep and eating disorders, and unresponsiveness to CBT [335].
SSRIs are the first-line drugs also in OCD during pregnancy [333, 336], given the absence of related teratogenesis [333, 337-342]. Sertraline, citalopram and escitalopram appear to be the most favorable in the perinatal period [341], considering their effectiveness in OCD and the association lack with congenital malformations [333, 343, 344].
Pregnancy safety data on fluvoxamine are few, and its use during pregnancy is less frequent compared to other SSRIs. Therefore, caution is recommended with regard to the use of fluvoxamine [345, 346]. Paroxetine and fluoxetine correlated with an increased risk of cardiac malformations and “poor neonatal adaptation syndrome” (PNAS) [347]. On this basis, these drugs should be used only in case of non-response or intolerance to other SSRIs.
Clomipramine is another first-line agent for OCD treatment [336] but presents an unfavorable safety profile in pregnancy. During this period, the risk of cardiovascular defects of the future child doubles [348, 349]; this drug is the TCA that is most associated with PNAS [350]. In addition, the risk of maternal intolerance is high. Venlafaxine does not seem to be related to congenital malformations, but limited evidence exists about its effectiveness in OCD, and similarly to SSRIs, its use involves different risks, including miscarriage, premature birth, and PNAS [333, 334, 340, 351].
Generally, higher antidepressant doses are used in OCD than those used in the treatment of major depression [352]. For this reason, the risk of pre-term birth associated with overdose of SSRI [101, 353] should be taken into account, and the minimum effective dose should be used [335].
Uguz et al. recently suggested a scheme of pharmacological interventions in refractory OCD during pregnancy [335]. If clinical response to the first-line SSRIs appears to be only partial, it is recommended to increase the dose, carefully monitoring both the woman and future child. In cases of unresponsiveness to sertraline, citalopram or escitalopram, a switch to fluvoxamine vs. clomipramine should be preferred. Further refractoriness could be treated with higher doses of SSRIs or the combination of a SSRI with clomipramine (with all the caution that was mentioned before). Clinicians should consider that the latter strategy is related to risk of drug interactions and/or adverse reactions, including convulsions [354], and data on its effectiveness are inconsistent. Should the addition of clomipramine be necessary, it must be administered at the lowest possible dosage [58, 336, 355].
Safety data about SSRI augmentation with antipsychotics are scanty. Given that this strategy does not guarantee the remission of treatment-resistant OCD [133, 356, 357], its use during pregnancy should be considered only if all other pharmacological approaches and CBT fail. The dosages of add-on antipsychotic drugs must be as low as possible. Among available antipsychotics, risperidone is recommended as the first choice, because it has the best safety profile for the unborn child. Haloperidol and quetiapine, which have an established safety profile, in terms of efficacy are placed in an intermediate position between risperidone and olanzapine. Olanzapine use is related to a risk of gestational diabetes mellitus. Safety data about add-on aripiprazole are limited. Quetiapine and olanzapine should be preferred in case of severe sleep disorders and loss of appetite. Particular caution should be adopted for combinations of high doses of SSRIs with moderate-high doses of antipsychotics or clomipramine [133, 356, 357].
In conclusion, the recent acquisitions on OCD treatment during the perinatal period are still limited. Optimal treatment dosages and duration are still unknown. More information is needed regarding the relationship between congenital malformations and antidepressant doses, as well as safety and efficacy of the SSRI/antipsychotic combination options.
7. CLINICAL GUIDELINES
According to the National Institute for Health and Care Excellence (NICE) CG31 guidelines (updated to September 2013 and which in February 2014 showed no expected changes for the next 3-5 years) for the treatment of OCD in adults [358], patients with mild functional impairment should be directed towards low-intensity CBT/ERP (<10 hours of therapist input for patient). If ineffective, more intensive cycles of SSRI or CBT (more than 10 hours) are considered comparably effective. Adults with OCD with moderate functional impairment should have the opportunity to choose between an intensive SSRI or CBT cycle. If functional impairment is severe, combined treatment with a SSRI and CBT/ERP is recommended [358].
Initial drug treatment for adults with OCD includes a SSRI (fluoxetine, fluvoxamine, paroxetine, sertraline or citalopram). If treatment response is not adequate and no side effects have occurred, dosage increases may be considered after 4-6 weeks of treatment. SSRI administration should be reviewed if patient develops marked and/or prolonged akathisia, restlessness or agitation. Treatment should continue for at least 12 months after OCD remission (symptoms are not clinically significant, and patient’s functioning is good for at least 12 weeks) to prevent relapse and allow further improvement. A further prolongation of treatment duration should be reassessed, taking into account the severity and duration of the previous symptoms, number of previous episodes, presence of residual symptoms, and concomitant psychosocial difficulties [358].
Initial OCD treatment should not include other classes of antidepressants such as TCAs, SNRIs and monoamine oxidase inhibitors (MAOIs) (unless comorbid disorders for which these drugs are needed), anxiolytics (except for cautious, short-period use to treat possible activation/agitation induced by SSRIs during treatment introduction), combinations of antidepressants, and antipsychotic monotherapy or augmentation. Patient’s adherence to treatment, and alcohol or substance use should be assessed in case of failed response to a complete treatment cycle with a SSRI, before making changes to the pharmacological strategy [358].
If patient shows a partial response to 12 weeks of SSRI treatment, NICE CG31 recommends the combination with CBT/ERP. If this combination fails, or SSRI response lacks, or the patient does not endorse CBT, switching to a different SSRI or to clomipramine should be evaluated. Clomipramine should be considered in three circumstances, i.e., failure (inefficacy or intolerance) of an adequate trial of at least one SSRI, if he/she favors clomipramine, or if he/she showed previous response to this drug. If effective, treatment with clomipramine should be continued for at least 12 months, as there may be further improvements. Before starting clomipramine, both adults and children should perform an electrocardiogram to rule out cardiac conduction abnormalities. TCAs other than clomipramine, MAOIs, SNRIs, and antipsychotics should not be used for treating OCD in children and young adults. However, these can be considered in refractory OCD [358].
If there is a lack of response after a complete trial with at least one SSRI, another with a SSRI and CBT/ERP, and a further trial with clomipramine alone, NICE CG31 recommends considering strategies such as additional CBT/ERP, addition of an antipsychotic to a SSRI or clomipramine, or the combination of clomipramine with citalopram (with all the precautions we stressed above). The optimal selection sequence is not specified because there is no current evidence supporting the superiority of one strategy over another [358]. We summarize clinical guidelines in the algorithm shown in Fig. (2).
People with severe, chronic, and treatment-resistant OCD should have constant access to specific specialist and multidisciplinary teams of health professionals with specific skills in OCD treatment. Hospital services should carefully assess suicide risk, extreme discomfort or functional impairment, ineffectiveness of appropriate trials of pharmacological/psychological/combined treatments for long periods, severe comorbid depression, anorexia nervosa, or schizophrenia, inversion of the waking cycle, severe or habitual compulsive and avoidance behaviors interfering with normal activities and daily life.
In clinical practice, treatment strategies do not always follow evidence-based guidelines. Poppe et al. [359] collected prescription data of 842 OCD patients from 1994 to 2012 to analyze models and changes in prescription strategies. Nine/tenths of patients received at least one drug and about 68% a combination of at least two drugs. The most prescribed drugs were antidepressants (78%): the prescriptions consisted of SSRIs (58%), TCAs (18%), mainly including clomipramine, SGAs (38%), and FGAs (14%). Several patients received a tranquilizer (20%). The authors showed an increase over time of SSRI, SGA and tranquilizer prescriptions, and a decrease of clomipramine. FGA use remained stable. The high rate of SSRI use, preference for clomipramine and SGA augmentation were consistent with recommendations of international guidelines. The administration of tranquilizers and FGAs and the choice of individual strategies were not in line with the expert recommendations [359].
Other guidelines confirm the above approaches. For the World Federation of Biological Psychiatry (WFSBP), first-line treatments are SSRIs and clomipramine [360]. The use of medium-to-upper doses is recommended despite lack of evidence of a dose-response relationship for both in OCD. These recommendations are made to general practitioners and in case of non-response, psychiatric consultation in recommended. In still-resistant severe OCD cases and after all options have been attempted unsuccessfully, deep brain stimulation should be considered. The updated American Psychiatric Association guidelines [361] endorse similar approaches, but also stress the need for identifying response predictors, for assessing the long-term effectiveness and safety of augmentation strategies in refractory OCD, and for establishing adequate time points for intervention. Combining this, the way is paved for sequential treatment and for personalized medicine approaches, including genetic/pharmacogenomic/metabolomic assessment. We propose in our treatment algorithm Fig. (2) to adopt such assessment in totally refractory OCD patients, specifically in those who did not respond to augmentation with SGAs or to switch to clomipramine or to various SSRI trials.
Drug prescriptions in OCD patients significantly vary in different countries. Brakoulias et al. [297] compared the prescription rates in Brazil, Italy, South Africa, Japan, Australia, India, and Spain. Of 3139 OCD patients, almost 78% received a psychotropic drug, being in 73.5% of the cases of a SSRI, which was in line with international guidelines. The use of SSRIs varied from 59% in Australia to 96% in Japan, clomipramine ranged from 5% in Japan and South Africa to 26% in India and Italy, atypical antipsychotics from 12% in South Africa to 50% in Japan. Further prospective studies should be conducted to identifying cultural factors, pharmacoeconomics, and pharmacogenomics, which may play a role in improving prescriptions and treatment outcomes.
CONCLUSION
To date, the most effective pharmacological treatment is the combination of an SSRI agent with CBT. Refractory OCD symptoms can improve with high SSRI dosages or augmentation with an atypical antipsychotic drug, mainly risperidone and aripiprazole. Due to inconsistent evidence, the addition of medications other than antipsychotics and intravenous antidepressant administration needs further investigation. Intervention strategies based on personalized medicine are of promise but require further investigation.
ACKNOWLEDGEMENTS
We gratefully acknowledge the contribution of the Librarians of the School of Medicine and Psychology of Sapienza University, Ms. Mimma Ariano, Ms. Felicia Proietti, Ms. Ales Casciaro, Ms. Teresa Prioreschi, and Ms. Susanna Rospo for rendering precious bibliographical material accessible, as well as our Secretary Lucilla Martinelli for her assistance during the writing of this manuscript.
CONSENT FOR PUBLICATION
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
In the past three years, P.G. has received research support from Angelini, Janssen, Lundbeck, and Otsuka. All other authors of this paper have no relevant conflicts with the subject matter or materials discussed in the manuscript.
REFERENCES
- 1.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5). Arlington, VA: American Psychiatric Association; 2013. [Google Scholar]
- 2.Rasmussen S.A., Eisen J.L. The epidemiology and differential diagnosis of obsessive compulsive disorder. J. Clin. Psychiatry. 1994;55(Suppl.):5–10. [PMID: 7961532]. [PubMed] [Google Scholar]
- 3.Ruscio A.M., Stein D.J., Chiu W.T., Kessler R.C. The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Mol. Psychiatry. 2010;15(1):53–63. doi: 10.1038/mp.2008.94. [http://dx.doi.org/10.1038/mp.2008.94]. [PMID: 18725912]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kessler R.C., Berglund P., Demler O., Jin R., Merikangas K.R., Walters E.E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry. 2005;62(6):593–602. doi: 10.1001/archpsyc.62.6.593. [http://dx.doi. org/10.1001/archpsyc.62.6.593]. [PMID: 15939837]. [DOI] [PubMed] [Google Scholar]
- 5.Geller D.A., Biederman J., Jones J., Shapiro S., Schwartz S., Park K.S. Obsessive-compulsive disorder in children and adolescents: a review. Harv. Rev. Psychiatry. 1998;5(5):260–273. doi: 10.3109/10673229809000309. [http://dx.doi.org/10.3109/10673229809000309]. [PMID: 9493948]. [DOI] [PubMed] [Google Scholar]
- 6.Geller D.A. Obsessive-compulsive and spectrum disorders in children and adolescents. Psychiatr. Clin. North Am. 2006;29(2):353–370. doi: 10.1016/j.psc.2006.02.012. [http://dx.doi.org/10.1016/j.psc.2006.02.012]. [PMID: 16650713]. [DOI] [PubMed] [Google Scholar]
- 7.Heyman I., Fombonne E., Simmons H., Ford T., Meltzer H., Goodman R. Prevalence of obsessive-compulsive disorder in the British nationwide survey of child mental health. Int. Rev. Psychiatry. 2003;15(1-2):178–184. doi: 10.1080/0954026021000046146. [http://dx.doi.org/10.1080/0954026021 000046146]. [PMID: 12745330]. [DOI] [PubMed] [Google Scholar]
- 8.Anholt G.E., Aderka I.M., van Balkom A.J., Smit J.H., Schruers K., van der Wee N.J., Eikelenboom M., De Luca V., van Oppen P. Age of onset in obsessive-compulsive disorder: admixture analysis with a large sample. Psychol. Med. 2014;44(1):185–194. doi: 10.1017/S0033291713000470. [http:// dx.doi.org/10.1017/S0033291713000470]. [PMID: 23517651]. [DOI] [PubMed] [Google Scholar]
- 9.Mataix-Cols D., Marks I.M., Greist J.H., Kobak K.A., Baer L. Obsessive-compulsive symptom dimensions as predictors of compliance with and response to behaviour therapy: results from a controlled trial. Psychother. Psychosom. 2002;71(5):255–262. doi: 10.1159/000064812. [http:// dx.doi.org/10.1159/000064812]. [PMID: 12207105]. [DOI] [PubMed] [Google Scholar]
- 10.Stewart S.E., Geller D.A., Jenike M., Pauls D., Shaw D., Mullin B., Faraone S.V. Long-term outcome of pediatric obsessive-compulsive disorder: a meta-analysis and qualitative review of the literature. Acta Psychiatr. Scand. 2004;110(1):4–13. doi: 10.1111/j.1600-0447.2004.00302.x. [http://dx. doi.org/10.1111/j.1600-0447.2004.00302.x]. [PMID: 15180774]. [DOI] [PubMed] [Google Scholar]
- 11.World Health Organization (WHO) The Global Burden of Disease: 2004 Update. Geneva, Switzerland: World Health Organization; 2008. [Google Scholar]
- 12.Hirschtritt M.E., Bloch M.H., Mathews C.A. Obsessive-compulsive disorder: Advances in diagnosis and treatment. JAMA. 2017;317(13):1358–1367. doi: 10.1001/jama.2017.2200. [http://dx.doi.org/10.1001/jama.2017.2200]. [PMID: 28384832]. [DOI] [PubMed] [Google Scholar]
- 13.Leon A.C., Olfson M., Broadhead W.E., Barrett J.E., Blacklow R.S., Keller M.B., Higgins E.S., Weissman M.M. Prevalence of mental disorders in primary care. Implications for screening. Arch. Fam. Med. 1995;4(10):857–861. doi: 10.1001/archfami.4.10.857. [http://dx.doi.org/10.1001/ archfami.4.10.857]. [PMID: 7551133]. [DOI] [PubMed] [Google Scholar]
- 14.Veldhuis J., Dieleman J.P., Wohlfarth T., Storosum J.G., van Den Brink W., Sturkenboom M.C., Denys D. Incidence and prevalence of “diagnosed OCD” in a primary care, treatment seeking, population. Int. J. Psychiatry Clin. Pract. 2012;16(2):85–92. doi: 10.3109/13651501.2011.617454. [http:// dx.doi.org/10.3109/13651501.2011.617454]. [PMID: 22122660]. [DOI] [PubMed] [Google Scholar]
- 15.Glazier K., Calixte R.M., Rothschild R., Pinto A. High rates of OCD symptom misidentification by mental health professionals. Ann. Clin. Psychiatry. 2013;25(3):201–209. [PMID: 23926575]. [PubMed] [Google Scholar]
- 16.Dell’Osso B., Camuri G., Benatti B., Buoli M., Altamura A.C. Differences in latency to first pharmacological treatment (duration of untreated illness) in anxiety disorders: a study on patients with panic disorder, generalized anxiety disorder and obsessive-compulsive disorder. Early Interv. Psychiatry. 2013;7(4):374–380. doi: 10.1111/eip.12016. [http://dx.doi.org/10.1111/eip.12016]. [PMID: 23347385]. [DOI] [PubMed] [Google Scholar]
- 17.Altamura A.C., Buoli M., Albano A., Dell’Osso B. Age at onset and latency to treatment (duration of untreated illness) in patients with mood and anxiety disorders: a naturalistic study. Int. Clin. Psychopharmacol. 2010;25(3):172–179. doi: 10.1097/YIC.0b013e3283384c74. [http://dx.doi.org/10. 1097/YIC.0b013e3283384c74]. [PMID: 20305566]. [DOI] [PubMed] [Google Scholar]
- 18.Torres A.R., Prince M.J., Bebbington P.E., Bhugra D.K., Brugha T.S., Farrell M., Jenkins R., Lewis G., Meltzer H., Singleton N. Treatment seeking by individuals with obsessive-compulsive disorder from the british psychiatric morbidity survey of 2000. Psychiatr. Serv. 2007;58(7):977–982. doi: 10.1176/ps.2007.58.7.977. [http://dx.doi.org/ 10.1176/ps.2007.58.7.977]. [PMID: 17602015]. [DOI] [PubMed] [Google Scholar]
- 19.Torres A.R., Prince M.J., Bebbington P.E., Bhugra D., Brugha T.S., Farrell M., Jenkins R., Lewis G., Meltzer H., Singleton N. Obsessive-compulsive disorder: prevalence, comorbidity, impact, and help-seeking in the British National Psychiatric Morbidity Survey of 2000. Am. J. Psychiatry. 2006;163(11):1978–1985. doi: 10.1176/ajp.2006.163.11.1978. [http://dx. doi.org/10.1176/ajp.2006.163.11.1978]. [PMID: 17074950]. [DOI] [PubMed] [Google Scholar]
- 20.Skapinakis P., Caldwell D.M., Hollingworth W., Bryden P., Fineberg N.A., Salkovskis P., Welton N.J., Baxter H., Kessler D., Churchill R., Lewis G. Pharmacological and psychotherapeutic interventions for management of obsessive-compulsive disorder in adults: a systematic review and network meta-analysis. Lancet Psychiatry. 2016;3(8):730–739. doi: 10.1016/S2215-0366(16)30069-4. [http://dx.doi.org/10.1016/S2215-0366(16)30069-4]. [PMID: 27318812]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cottraux J., Bouvard M.A., Milliery M. Combining Pharmacotherapy with cognitive-behavioral interventions for obsessive-compulsive disorder. Cogn. Behav. Ther. 2005;34(3):185–192. doi: 10.1080/16506070510043750. [http://dx.doi.org/10.1080/16506070510043750]. [PMID: 16201063]. [DOI] [PubMed] [Google Scholar]
- 22.Pallanti S., Quercioli L. Treatment-refractory obsessive-compulsive disorder: methodological issues, operational definitions and therapeutic lines. Prog. Neuropsychopharmacol. Biol. Psychiatry. 2006;30(3):400–412. doi: 10.1016/j.pnpbp.2005.11.028. [http://dx.doi.org/10.1016/j.pnpbp.2005. 11.028]. [PMID: 16503369]. [DOI] [PubMed] [Google Scholar]
- 23.Kaplan A., Hollander E. A review of pharmacologic treatments for obsessive-compulsive disorder. Psychiatr. Serv. 2003;54(8):1111–1118. doi: 10.1176/appi.ps.54.8.1111. [http://dx.doi.org/10.1176/appi.ps.54.8.1111]. [PMID: 12883138]. [DOI] [PubMed] [Google Scholar]
- 24.Simpson H.B., Liebowitz M.R., Foa E.B., Kozak M.J., Schmidt A.B., Rowan V., Petkova E., Kjernisted K., Huppert J.D., Franklin M.E., Davies S.O., Campeas R. Post-treatment effects of exposure therapy and clomipramine in obsessive-compulsive disorder. Depress. Anxiety. 2004;19(4):225–233. doi: 10.1002/da.20003. [http://dx.doi.org/10. 1002/da.20003]. [PMID: 15274171]. [DOI] [PubMed] [Google Scholar]
- 25.Stein D.J., Andersen E.W., Tonnoir B., Fineberg N. Escitalopram in obsessive-compulsive disorder: a randomized, placebo-controlled, paroxetine-referenced, fixed-dose, 24-week study. Curr. Med. Res. Opin. 2007;23(4):701–711. doi: 10.1185/030079907x178838. [http://dx.doi.org/10.1185/ 030079907X178838]. [PMID: 17407626]. [DOI] [PubMed] [Google Scholar]
- 26.Dell’Osso B., Nestadt G., Allen A., Hollander E. Serotonin-norepinephrine reuptake inhibitors in the treatment of obsessive-compulsive disorder: A critical review. J. Clin. Psychiatry. 2006;67(4):600–610. doi: 10.4088/jcp.v67n0411. [http://dx.doi.org/10.4088/JCP.v67n0411]. [PMID: 16669725]. [DOI] [PubMed] [Google Scholar]
- 27.Soomro G.M., Altman D., Rajagopal S., Oakley-Browne M. Selective serotonin re-uptake inhibitors (SSRIs) versus placebo for obsessive compulsive disorder (OCD). Cochrane Database Syst. Rev. 2008;(1):CD001765. doi: 10.1002/14651858.CD001765.pub3. [PMID: 18253995]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Issari Y., Jakubovski E., Bartley C.A., Pittenger C., Bloch M.H. Early onset of response with selective serotonin reuptake inhibitors in obsessive-compulsive disorder: a meta-analysis. J. Clin. Psychiatry. 2016;77(5):e605–e611. doi: 10.4088/JCP.14r09758. [http://dx.doi.org/10.4088/JCP. 14r09758]. [PMID: 27249090]. [DOI] [PubMed] [Google Scholar]
- 29.Fineberg N.A., Pampaloni I., Pallanti S., Ipser J., Stein D.J. Sustained response versus relapse: the pharmacotherapeutic goal for obsessive-compulsive disorder. Int. Clin. Psychopharmacol. 2007;22(6):313–322. doi: 10.1097/YIC.0b013e32825ea312. [http://dx.doi.org/10.1097/YIC.0b013e32825 ea312]. [PMID: 17917549]. [DOI] [PubMed] [Google Scholar]
- 30.Fineberg N.A., Tonnoir B., Lemming O., Stein D.J. Escitalopram prevents relapse of obsessive-compulsive disorder. Eur. Neuropsychopharmacol. 2007;17(6-7):430–439. doi: 10.1016/j.euroneuro.2006.11.005. [http://dx.doi.org/ 10.1016/j.euroneuro.2006.11.005]. [PMID: 17240120]. [DOI] [PubMed] [Google Scholar]
- 31.Landeros-Weisenberger A., Bloch M.H., Kelmendi B., Wegner R., Nudel J., Dombrowski P., Pittenger C., Krystal J.H., Goodman W.K., Leckman J.F., Coric V. Dimensional predictors of response to SRI pharmacotherapy in obsessive-compulsive disorder. J. Affect. Disord. 2010;121(1-2):175–179. doi: 10.1016/j.jad.2009.06.010. [http://dx.doi.org/10. 1016/j.jad.2009.06.010]. [PMID: 19577308]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Saxena S., Brody A.L., Ho M.L., Zohrabi N., Maidment K.M., Baxter L.R., Jr Differential brain metabolic predictors of response to paroxetine in obsessive-compulsive disorder versus major depression. Am. J. Psychiatry. 2003;160(3):522–532. doi: 10.1176/appi.ajp.160.3.522. [http://dx.doi. org/10.1176/appi.ajp.160.3.522]. [PMID: 12611834]. [DOI] [PubMed] [Google Scholar]
- 33.Mataix-Cols D., Rauch S.L., Manzo P.A., Jenike M.A., Baer L. Use of factor-analyzed symptom dimensions to predict outcome with serotonin reuptake inhibitors and placebo in the treatment of obsessive-compulsive disorder. Am. J. Psychiatry. 1999;156(9):1409–1416. doi: 10.1176/ajp.156.9.1409. [PMID: 10484953]. [DOI] [PubMed] [Google Scholar]
- 34.Erzegovesi S., Cavallini M.C., Cavedini P., Diaferia G., Locatelli M., Bellodi L. Clinical predictors of drug response in obsessive-compulsive disorder. J. Clin. Psychopharmacol. 2001;21(5):488–492. doi: 10.1097/00004714-200110000-00006. [http://dx.doi.org/10.1097/00004714-200110000-00006]. [PMID: 11593074]. [DOI] [PubMed] [Google Scholar]
- 35.Tükel R., Bozkurt O., Polat A., Genç A., Atli H. Clinical predictors of response to pharmacotherapy with selective serotonin reuptake inhibitors in obsessive-compulsive disorder. Psychiatry Clin. Neurosci. 2006;60(4):404–409. doi: 10.1111/j.1440-1819.2006.01523.x. [PMID: 16884439]. [DOI] [PubMed] [Google Scholar]
- 36.Hollander E., Allen A., Steiner M., Wheadon D.E., Oakes R., Burnham D.B. Acute and long-term treatment and prevention of relapse of obsessive-compulsive disorder with paroxetine. J. Clin. Psychiatry. 2003;64(9):1113–1121. doi: 10.4088/jcp.v64n0919. [http://dx.doi.org/10.4088/ JCP.v64n0919]. [PMID: 14628989]. [DOI] [PubMed] [Google Scholar]
- 37.Stein M.B., Liebowitz M.R., Lydiard R.B., Pitts C.D., Bushnell W., Gergel I. Paroxetine treatment of generalized social phobia (social anxiety disorder): a randomized controlled trial. JAMA. 1998;280(8):708–713. doi: 10.1001/jama.280.8.708. [http://dx.doi.org/10.1001/jama.280.8.708]. [PMID: 9728642]. [DOI] [PubMed] [Google Scholar]
- 38.Goljevscek S., Carvalho L.A. Current management of obsessive and phobic states. Neuropsychiatr. Dis. Treat. 2011;7:599–610. doi: 10.2147/NDT.S17032. [http://dx.doi.org/10.2147/NDT.S17032]. [PMID: 22003299]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Zohar J., Judge R. Paroxetine versus clomipramine in the treatment of obsessive-compulsive disorder. Br. J. Psychiatry. 1996;169(4):468–474. doi: 10.1192/bjp.169.4.468. [http://dx.doi.org/10.1192/bjp.169.4.468]. [PMID: 8894198]. [DOI] [PubMed] [Google Scholar]
- 40.Li J., Xiang H., Du H. Clinical controlled study of paroxetine and clomipramine in treatment of obsessive- compulsive disorder. Chin. J. Psychiatry. 1998;31(4):215–217. [Google Scholar]
- 41.Geller D.A., Wagner K.D., Emslie G., Murphy T., Carpenter D.J., Wetherhold E., Perera P., Machin A., Gardiner C. Paroxetine treatment in children and adolescents with obsessive-compulsive disorder: a randomized, multicenter, double-blind, placebo-controlled trial. J. Am. Acad. Child Adolesc. Psychiatry. 2004;43(11):1387–1396. doi: 10.1097/01.chi.0000138356.29099.f1. [http://dx.doi.org/10.1097/01.chi.0000138356. 29099.f1]. [PMID: 15502598]. [DOI] [PubMed] [Google Scholar]
- 42.Kamijima K., Murasaki M., Asai M., Higuchi T., Nakajima T., Taga C., Matsunaga H. Paroxetine in the treatment of obsessive-compulsive disorder: randomized, double-blind, placebo-controlled study in Japanese patients. Psychiatry Clin. Neurosci. 2004;58(4):427–433. doi: 10.1111/j.1440-1819.2004.01278.x. [http://dx.doi.org/10.1111/j.1440-1819.2004.01278.x]. [PMID: 15298657]. [DOI] [PubMed] [Google Scholar]
- 43.Ushijima S., Kamijima K., Asai M., Murasaki M., Nakajima T., Kudo Y., Tashiro N., Kurihara M., Miura S. Clinical evaluation of sertraline hydrochloride, a selective serotonin reuptake inhibitor in the treatment of obsessive- compulsive disorder: A double blind placebo controlled trial. Jpn. J. Neuropsychoph. 1997;19(6):603–623. [Google Scholar]
- 44.Mallya G.K., White K., Waternaux C., Quay S. Short- and long-term treatment with obsessive-compulsive disorder with fluvoxamine. Ann. Clin. Psychiatry. 1992;4:77–80. [http://dx.doi.org/10. 3109/10401239209150443]. [Google Scholar]
- 45.Nakajima T., Kudo Y., Yamashita I., Asai M., Kamijima K., Murasaki M., Yamaguchi N., Saito M., Yamawaki S., Nishizono M., Hishikawa Y., Machiyama Y., Yamauchi T., Moriya N., Toru M., Hirose T., Kojima T., Shimizu M., Tamura A., Endo S., Suzuki J., Takemasa K., Uno M., Hasegawa K., Kariya T. Clinical usefulness of Fluvoxamine Maleate (SME3110), a selective serotonin reuptake inhibitor, in the treatment of obsessive compulsive disorder: A double blind, placebo-controlled study investigating the therapeutic dose range and the efficacy of SME3110. J. Clin. Ther. Med. 1996;12(3):409–437. [Rinshou Iyaku]. [Google Scholar]
- 46.Nakatani E., Nakagawa A., Nakao T., Yoshizato C., Nabeyama M., Kudo A., Isomura K., Kato N., Yoshioka K., Kawamoto M. A randomized controlled trial of Japanese patients with obsessive-compulsive disorder--effectiveness of behavior therapy and fluvoxamine. Psychother. Psychosom. 2005;74(5):269–276. doi: 10.1159/000086317. [http://dx. doi.org/10.1159/000086317]. [PMID: 16088264]. [DOI] [PubMed] [Google Scholar]
- 47.Hollander E., Koran L.M., Goodman W.K., Greist J.H., Ninan P.T., Yang H., Li D., Barbato L.M. A double-blind, placebo-controlled study of the efficacy and safety of controlled-release fluvoxamine in patients with obsessive-compulsive disorder. J. Clin. Psychiatry. 2003;64(6):640–647. doi: 10.4088/jcp.v64n0604. [http://dx.doi.org/10.4088/ JCP.v64n0604]. [PMID: 12823077]. [DOI] [PubMed] [Google Scholar]
- 48.Goodman W.K., Kozak M.J., Liebowitz M., White K.L. Treatment of obsessive-compulsive disorder with fluvoxamine: a multicentre, double-blind, placebo-controlled trial. Int. Clin. Psychopharmacol. 1996;11(1):21–29. [http://dx.doi.org/10.1097/ 00004850-199603000-00003]. [PMID: 8732310]. [PubMed] [Google Scholar]
- 49.Riddle M.A., Reeve E.A., Yaryura-Tobias J.A., Yang H.M., Claghorn J.L., Gaffney G., Greist J.H., Holland D., McConville B.J., Pigott T., Walkup J.T. Fluvoxamine for children and adolescents with obsessive-compulsive disorder: a randomized, controlled, multicenter trial. J. Am. Acad. Child Adolesc. Psychiatry. 2001;40(2):222–229. doi: 10.1097/00004583-200102000-00017. [http://dx.doi.org/10.1097/00004583-200102000-00017]. [PMID: 11211371]. [DOI] [PubMed] [Google Scholar]
- 50.O’Connor K.P., Aardema F., Robillard S., Guay S., Pélissier M.C., Todorov C., Borgeat F., Leblanc V., Grenier S., Doucet P. Cognitive behaviour therapy and medication in the treatment of obsessive-compulsive disorder. Acta Psychiatr. Scand. 2006;113(5):408–419. doi: 10.1111/j.1600-0447.2006.00767.x. [http://dx.doi.org/10.1111/j.1600-0447.2006.00767. x]. [PMID: 16603032]. [DOI] [PubMed] [Google Scholar]
- 51.Goodman W.K., Price L.H., Rasmussen S.A., Delgado P.L., Heninger G.R., Charney D.S. Efficacy of fluvoxamine in obsessive-compulsive disorder. A double-blind comparison with placebo. Arch. Gen. Psychiatry. 1989;46(1):36–44. doi: 10.1001/archpsyc.1989.01810010038006. [http://dx.doi. org/10.1001/archpsyc.1989.01810010038006]. [PMID: 2491940]. [DOI] [PubMed] [Google Scholar]
- 52.Jenike M.A., Hyman S., Baer L., Holland A., Minichiello W.E., Buttolph L., Summergrad P., Seymour R., Ricciardi J. A controlled trial of fluvoxamine in obsessive-compulsive disorder: implications for a serotonergic theory. Am. J. Psychiatry. 1990;147(9):1209–1215. doi: 10.1176/ajp.147.9.1209. [http://dx.doi.org/10.1176/ajp.147.9.1209]. [PMID: 2143637]. [DOI] [PubMed] [Google Scholar]
- 53.Stein M.B., Fyer A.J., Davidson J.R., Pollack M.H., Wiita B. Fluvoxamine treatment of social phobia (social anxiety disorder): a double-blind, placebo-controlled study. Am. J. Psychiatry. 1999;156(5):756–760. doi: 10.1176/ajp.156.5.756. [PMID: 10327910]. [DOI] [PubMed] [Google Scholar]
- 54.Ravizza L., Barzega G., Bellino S., Bogetto F., Maina G. Drug treatment of obsessive-compulsive disorder (OCD): long-term trial with clomipramine and selective serotonin reuptake inhibitors (SSRIs). Psychopharmacol. Bull. 1996;32(1):167–173. [PMID: 8927668]. [PubMed] [Google Scholar]
- 55.Stein D.J., Andersen E.W., Overo K.F. Response of symptom dimensions in obsessive-compulsive disorder to treatment with citalopram or placebo. Rev. Bras. Psiquiatr. 2007;29(4):303–307. doi: 10.1590/s1516-44462007000400003. [http://dx.doi.org/10.1590/S1516-44462007000400003]. [PMID: 18200396]. [DOI] [PubMed] [Google Scholar]
- 56.Montgomery S.A., Kasper S., Stein D.J., Bang Hedegaard K., Lemming O.M. Citalopram 20 mg, 40 mg and 60 mg are all effective and well tolerated compared with placebo in obsessive-compulsive disorder. Int. Clin. Psychopharmacol. 2001;16(2):75–86. doi: 10.1097/00004850-200103000-00002. [http://dx.doi.org/10.1097/00004850-200103000-00002]. [PMID: 11236072]. [DOI] [PubMed] [Google Scholar]
- 57.Atmaca M., Kuloglu M., Tezcan E., Unal A. Efficacy of citalopram and moclobemide in patients with social phobia: some preliminary findings. Hum. Psychopharmacol. 2002;17(8):401–405. doi: 10.1002/hup.436. [http://dx.doi.org/10.1002/hup.436]. [PMID: 12457375]. [DOI] [PubMed] [Google Scholar]
- 58.Marazziti D., Golia F., Consoli G., Presta S., Pfanner C., Carlini M., Mungai F., Catena Dell’osso M. Effectiveness of long-term augmentation with citalopram to clomipramine in treatment-resistant OCD patients. CNS Spectr. 2008;13(11):971–976. doi: 10.1017/s1092852900014024. [http:// dx.doi.org/10.1017/S1092852900014024]. [PMID: 19037176]. [DOI] [PubMed] [Google Scholar]
- 59.Sánchez C., Bergqvist P.B., Brennum L.T., Gupta S., Hogg S., Larsen A., Wiborg O. Escitalopram, the S-(+)-enantiomer of citalopram, is a selective serotonin reuptake inhibitor with potent effects in animal models predictive of antidepressant and anxiolytic activities. Psychopharmacology (Berl.) 2003;167(4):353–362. doi: 10.1007/s00213-002-1364-z. [http://dx.doi.org/10.1007/s00213-002-1364-z]. [PMID: 12719960]. [DOI] [PubMed] [Google Scholar]
- 60.von Moltke L.L., Greenblatt D.J., Giancarlo G.M., Granda B.W., Harmatz J.S., Shader R.I. Escitalopram (S-citalopram) and its metabolites in vitro: cytochromes mediating biotransformation, inhibitory effects, and comparison to R-citalopram. Drug Metab. Dispos. 2001;29(8):1102–1109. [PMID: 11454728]. [PubMed] [Google Scholar]
- 61.Burke W.J., Kratochvil C.J. Stereoisomers in Psychiatry: The Case of Escitalopram. Prim. Care Companion J. Clin. Psychiatry. 2002;4(1):20–24. doi: 10.4088/pcc.v04n0107. [http://dx.doi.org/10.4088/PCC.v04n0107]. [PMID: 15014731]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Lader M., Stender K., Bürger V., Nil R. Efficacy and tolerability of escitalopram in 12- and 24-week treatment of social anxiety disorder: randomised, double-blind, placebo-controlled, fixed-dose study. Depress. Anxiety. 2004;19(4):241–248. doi: 10.1002/da.20014. [http://dx.doi. org/10.1002/da.20014]. [PMID: 15274173]. [DOI] [PubMed] [Google Scholar]
- 63.Tollefson G.D., Rampey A.H., Jr, Potvin J.H., Jenike M.A., Rush A.J. kominguez, R.A.; Koran, L.M.; Shear, M.K.; Goodman, W.; Genduso, L.A. A multicenter investigation of fixed-dose fluoxetine in the treatment of obsessive-compulsive disorder. Arch. Gen. Psychiatry. 1994;51(7):559–567. doi: 10.1001/archpsyc.1994.03950070051010. [http://dx.doi.org/10.1001/ archpsyc.1994.03950070051010]. [PMID: 8031229]. [DOI] [PubMed] [Google Scholar]
- 64.Romano S., Goodman W., Tamura R., Gonzales J. Long-term treatment of obsessive-compulsive disorder after an acute response: a comparison of fluoxetine versus placebo. J. Clin. Psychopharmacol. 2001;21(1):46–52. doi: 10.1097/00004714-200102000-00009. [http://dx.doi.org/10.1097/00004714-200102000-00009]. [PMID: 11199947]. [DOI] [PubMed] [Google Scholar]
- 65.Phillips K.A., Rasmussen S.A. Change in psychosocial functioning and quality of life of patients with body dysmorphic disorder treated with fluoxetine: a placebo-controlled study. Psychosomatics. 2004;45(5):438–444. doi: 10.1176/appi.psy.45.5.438. [http://dx.doi.org/10.1176/appi.psy.45.5.438]. [PMID: 15345790]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Davidson J.R., Foa E.B., Huppert J.D., Keefe F.J., Franklin M.E., Compton J.S., Zhao N., Connor K.M., Lynch T.R., Gadde K.M. Fluoxetine, comprehensive cognitive behavioral therapy, and placebo in generalized social phobia. Arch. Gen. Psychiatry. 2004;61(10):1005–1013. doi: 10.1001/archpsyc.61.10.1005. [http://dx.doi.org/10.1001/archpsyc.61.10.1005]. [PMID: 15466674]. [DOI] [PubMed] [Google Scholar]
- 67.Riddle M.A., Scahill L., King R.A., Hardin M.T., Anderson G.M., Ort S.I., Smith J.C., Leckman J.F., Cohen D.J. Double-blind, crossover trial of fluoxetine and placebo in children and adolescents with obsessive-compulsive disorder. J. Am. Acad. Child Adolesc. Psychiatry. 1992;31(6):1062–1069. doi: 10.1097/00004583-199211000-00011. [http://dx.doi.org/10. 1097/00004583-199211000-00011]. [PMID: 1429406]. [DOI] [PubMed] [Google Scholar]
- 68.Montgomery S.A., McIntyre A., Osterheider M., Sarteschi P., Zitterl W., Zohar J., Birkett M., Wood A.J. A double-blind, placebo-controlled study of fluoxetine in patients with DSM-III-R obsessive-compulsive disorder. Eur. Neuropsychopharmacol. 1993;3(2):143–152. doi: 10.1016/0924-977x(93)90266-o. [http://dx.doi.org/10.1016/0924-977X(93)90266-O]. [PMID: 8364350]. [DOI] [PubMed] [Google Scholar]
- 69.Geller D.A., Hoog S.L., Heiligenstein J.H., Ricardi R.K., Tamura R., Kluszynski S., Jacobson J.G. Fluoxetine treatment for obsessive-compulsive disorder in children and adolescents: a placebo-controlled clinical trial. J. Am. Acad. Child Adolesc. Psychiatry. 2001;40(7):773–779. doi: 10.1097/00004583-200107000-00011. [http://dx.doi.org/10.1097/00004583-200107000-00011]. [PMID: 11437015]. [DOI] [PubMed] [Google Scholar]
- 70.Tollefson G.D., Birkett M., Koran L., Genduso L. Continuation treatment of OCD: double-blind and open-label experience with fluoxetine. J. Clin. Psychiatry. 1994;55(Suppl.):69–76. [PMID: 7961535]. [PubMed] [Google Scholar]
- 71.Jenike M.A., Baer L., Minichiello W.E., Rauch S.L., Buttolph M.L. Placebo-controlled trial of fluoxetine and phenelzine for obsessive-compulsive disorder. Am. J. Psychiatry. 1997;154(9):1261–1264. doi: 10.1176/ajp.154.9.1261. [http://dx.doi.org/10.1176/ajp.154.9.1261]. [PMID: 9286186]. [DOI] [PubMed] [Google Scholar]
- 72.Greist J., Chouinard G., DuBoff E., Halaris A., Kim S.W., Koran L., Liebowitz M., Lydiard R.B., Rasmussen S., White K., Sikes C. Double-blind parallel comparison of three dosages of sertraline and placebo in outpatients with obsessive-compulsive disorder. Arch. Gen. Psychiatry. 1995;52(4):289–295. doi: 10.1001/archpsyc.1995.03950160039008. [http://dx.doi. org/10.1001/archpsyc.1995.03950160039008]. [PMID: 7702445]. [DOI] [PubMed] [Google Scholar]
- 73.Liebowitz M.R., DeMartinis N.A., Weihs K., Londborg P.D., Smith W.T., Chung H., Fayyad R., Clary C.M. Efficacy of sertraline in severe generalized social anxiety disorder: results of a double-blind, placebo-controlled study. J. Clin. Psychiatry. 2003;64(7):785–792. doi: 10.4088/jcp.v64n0708. [http://dx.doi.org/10.4088/JCP.v64n0708]. [PMID: 12934979]. [DOI] [PubMed] [Google Scholar]
- 74.Van Ameringen M.A., Lane R.M., Walker J.R., Bowen R.C., Chokka P.R., Goldner E.M., Johnston D.G., Lavallee Y.J., Nandy S., Pecknold J.C., Hadrava V., Swinson R.P. Sertraline treatment of generalized social phobia: a 20-week, double-blind, placebo-controlled study. Am. J. Psychiatry. 2001;158(2):275–281. doi: 10.1176/appi.ajp.158.2.275. [http://dx.doi.org/10.1176/appi.ajp.158.2.275]. [PMID: 11156811]. [DOI] [PubMed] [Google Scholar]
- 75.Kronig M.H., Apter J., Asnis G., Bystritsky A., Curtis G., Ferguson J., Landbloom R., Munjack D., Riesenberg R., Robinson D., Roy-Byrne P., Phillips K., Du Pont I.J. Placebo-controlled, multicenter study of sertraline treatment for obsessive-compulsive disorder. J. Clin. Psychopharmacol. 1999;19(2):172–176. doi: 10.1097/00004714-199904000-00013. [http://dx.doi.org/10.1097/00004714-199904000-00013]. [PMID: 10211919]. [DOI] [PubMed] [Google Scholar]
- 76.Koran L.M., Hackett E., Rubin A., Wolkow R., Robinson D. Efficacy of sertraline in the long-term treatment of obsessive-compulsive disorder. Am. J. Psychiatry. 2002;159(1):88–95. doi: 10.1176/appi.ajp.159.1.88. [http://dx.doi.org/10.1176/appi.ajp.159.1.88]. [PMID: 11772695]. [DOI] [PubMed] [Google Scholar]
- 77.Chouinard G., Goodman W., Greist J., Jenike M., Rasmussen S., White K., Hackett E., Gaffney M., Bick P.A. Results of a double-blind placebo controlled trial of a new serotonin uptake inhibitor, sertraline, in the treatment of obsessive-compulsive disorder. Psychopharmacol. Bull. 1990;26(3):279–284. [PMID: 2274626]. [PubMed] [Google Scholar]
- 78.Ninan P.T., Koran L.M., Kiev A., Davidson J.R., Rasmussen S.A., Zajecka J.M., Robinson D.G., Crits-Christoph P., Mandel F.S., Austin C. High-dose sertraline strategy for nonresponders to acute treatment for obsessive-compulsive disorder: a multicenter double-blind trial. J. Clin. Psychiatry. 2006;67(1):15–22. doi: 10.4088/jcp.v67n0103. [http:// dx.doi.org/10.4088/JCP.v67n0103]. [PMID: 16426083]. [DOI] [PubMed] [Google Scholar]
- 79.Abramowitz J.S. Effectiveness of psychological and pharmacological treatments for obsessive-compulsive disorder: a quantitative review. J. Consult. Clin. Psychol. 1997;65(1):44–52. doi: 10.1037//0022-006x.65.1.44. [http://dx. doi.org/10.1037/0022-006X.65.1.44]. [PMID: 9103733]. [DOI] [PubMed] [Google Scholar]
- 80.Foa E.B., Liebowitz M.R., Kozak M.J., Davies S., Campeas R., Franklin M.E., Huppert J.D., Kjernisted K., Rowan V., Schmidt A.B., Simpson H.B., Tu X. Randomized, placebo-controlled trial of exposure and ritual prevention, clomipramine, and their combination in the treatment of obsessive-compulsive disorder. Am. J. Psychiatry. 2005;162(1):151–161. doi: 10.1176/appi.ajp.162.1.151. [http://dx.doi.org/10.1176/appi. ajp.162.1.151]. [PMID: 15625214]. [DOI] [PubMed] [Google Scholar]
- 81.Fallon B.A., Mathew S.J. Biological therapies for obsessive-compulsive disorder. J. Psychiatr. Pract. 2000;6(3):113–128. doi: 10.1097/00131746-200005000-00002. [http://dx.doi.org/10.1097/00131746-200005000-00002]. [PMID: 15990479]. [DOI] [PubMed] [Google Scholar]
- 82.Jenike M.A., Baer L., Summergrad P., Weilburg J.B., Holland A., Seymour R. Obsessive-compulsive disorder: a double-blind, placebo-controlled trial of clomipramine in 27 patients. Am. J. Psychiatry. 1989;146(10):1328–1330. doi: 10.1176/ajp.146.10.1328. [http://dx.doi.org/10.1176/ ajp.146.10.1328]. [PMID: 2675643]. [DOI] [PubMed] [Google Scholar]
- 83.Greist J.H., Jefferson J.W., Rosenfeld R., Gutzmann L.D., March J.S., Barklage N.E. Clomipramine and obsessive compulsive disorder: a placebo-controlled double-blind study of 32 patients. J. Clin. Psychiatry. 1990;51(7):292–297. [PMID: 2195006]. [PubMed] [Google Scholar]
- 84.Clomipramine in the treatment of patients with obsessive-compulsive disorder. Arch. Gen. Psychiatry. 1991;48(8):730–738. doi: 10.1001/archpsyc.1991.01810320054008. [http://dx.doi.org/10.1001/archpsyc.1991.01810320054008]. [PMID: 1883256]. [DOI] [PubMed] [Google Scholar]
- 85.Hoehn-Saric R., McLeod D.R., Zimmerli W.D., Hipsley P.A. Symptoms and physiologic manifestations in obsessive compulsive patients before and after treatment with clomipramine. J. Clin. Psychiatry. 1993;54(7):272–276. [PMID: 8335655]. [PubMed] [Google Scholar]
- 86.Mavissakalian M.R., Jones B., Olson S., Perel J.M. Clomipramine in obsessive-compulsive disorder: clinical response and plasma levels. J. Clin. Psychopharmacol. 1990;10(4):261–268. [http://dx.doi.org/10.1097/00004714-199008000-00005]. [PMID: 2286699]. [PubMed] [Google Scholar]
- 87.Albert U., Aguglia E., Maina G., Bogetto F. Venlafaxine versus clomipramine in the treatment of obsessive-compulsive disorder: a preliminary single-blind, 12-week, controlled study. J. Clin. Psychiatry. 2002;63(11):1004–1009. doi: 10.4088/jcp.v63n1108. [http://dx.doi.org/10.4088/JCP. v63n1108]. [PMID: 12444814]. [DOI] [PubMed] [Google Scholar]
- 88.Rauch S.L., O’Sullivan R.L., Jenike M.A. Open treatment of obsessive-compulsive disorder with venlafaxine: a series of ten cases. J. Clin. Psychopharmacol. 1996;16(1):81–84. doi: 10.1097/00004714-199602000-00017. [http://dx. doi.org/10.1097/00004714-199602000-00017]. [PMID: 8834427]. [DOI] [PubMed] [Google Scholar]
- 89.Sevincok L., Uygur B. Venlafaxine open-label treatment of patients with obsessive-compulsive disorder. Aust. N. Z. J. Psychiatry. 2002;36(6):817. doi: 10.1046/j.1440-1614.2002.t01-5-01101c.x. [http://dx.doi.org/10.1046/j.1440-1614.2002. t01-5-01101c.x]. [PMID: 12406128]. [DOI] [PubMed] [Google Scholar]
- 90.Hollander E., Friedberg J., Wasserman S., Allen A., Birnbaum M., Koran L.M. Venlafaxine in treatment-resistant obsessive-compulsive disorder. J. Clin. Psychiatry. 2003;64(5):546–550. doi: 10.4088/jcp.v64n0508. [http://dx.doi.org/10.4088/JCP.v64n0508]. [PMID: 12755657]. [DOI] [PubMed] [Google Scholar]
- 91.Liebowitz M.R., Gelenberg A.J., Munjack D. Venlafaxine extended release vs placebo and paroxetine in social anxiety disorder. Arch. Gen. Psychiatry. 2005;62(2):190–198. doi: 10.1001/archpsyc.62.2.190. [http://dx.doi.org/10. 1001/archpsyc.62.2.190]. [PMID: 15699296]. [DOI] [PubMed] [Google Scholar]
- 92.Stein M.B., Pollack M.H., Bystritsky A., Kelsey J.E., Mangano R.M. Efficacy of low and higher dose extended-release venlafaxine in generalized social anxiety disorder: a 6-month randomized controlled trial. Psychopharmacology (Berl.) 2005;177(3):280–288. doi: 10.1007/s00213-004-1957-9. [http://dx.doi.org/10.1007/s00213-004-1957-9]. [PMID: 15258718]. [DOI] [PubMed] [Google Scholar]
- 93.Denys D., van der Wee N., van Megen H.J., Westenberg H.G. A double blind comparison of venlafaxine and paroxetine in obsessive-compulsive disorder. J. Clin. Psychopharmacol. 2003;23(6):568–575. doi: 10.1097/01.jcp.0000095342.32154.54. [http://dx.doi.org/10.1097/01.jcp.0000095342.32154.54]. [PMID: 14624187]. [DOI] [PubMed] [Google Scholar]
- 94.Luís Blay S., Black D.W. A case of obsessive-compulsive disorder responding to duloxetine. Prim. Care Companion J. Clin. Psychiatry. 2007;9(3):234–235. doi: 10.4088/pcc.v09n0311c. [http://dx.doi.org/10.4088/PCC. v09n0311c]. [PMID: 17632660]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Dell’osso B., Mundo E., Marazziti D., Altamura A.C. Switching from serotonin reuptake inhibitors to duloxetine in patients with resistant obsessive compulsive disorder: a case series. J. Psychopharmacol. (Oxford) 2008;22(2):210–213. doi: 10.1177/0269881107079865. [http://dx.doi.org/10. 1177/0269881107079865]. [PMID: 18208931]. [DOI] [PubMed] [Google Scholar]
- 96.Yeh Y.W., Chen C.H., Kuo S.C., Wang S.C., Chen C.K., Feng H.M. High-dose duloxetine for treatment-resistant obsessive-compulsive disorder: a case report with sustained full remission. Clin. Neuropharmacol. 2009;32(3):174–176. doi: 10.1097/WNF.0b013e31817f8cef. [http://dx.doi.org/10. 1097/WNF.0b013e31817f8cef]. [PMID: 19483491]. [DOI] [PubMed] [Google Scholar]
- 97.Yoshida K., Higuchi H., Ozaki N. Successful treatment of severe antidepressant-induced nausea with a combination of milnacipran and olanzapine. Pharmacopsychiatry. 2007;40(2):84–85. doi: 10.1055/s-2007-970061. [http:// dx.doi.org/10.1055/s-2007-970061]. [PMID: 17447181]. [DOI] [PubMed] [Google Scholar]
- 98.De Berardis D., Conti C.M., Marini S., Ferri F., Iasevoli F., Valchera A., Fornaro M., Cavuto M., Srinivasan V., Perna G., Carano A., Piersanti M., Martinotti G., Di Giannantonio M. Is there a role for agomelatine in the treatment of anxiety disorders?A review of published data. Int. J. Immunopathol. Pharmacol. 2013;26(2):299–304. doi: 10.1177/039463201302600203. [http://dx.doi.org/10.1177/039463201302600203]. [PMID: 23755745]. [DOI] [PubMed] [Google Scholar]
- 99.Fornaro M. Switching from serotonin reuptake inhibitors to agomelatine in patients with refractory obsessive-compulsive disorder: a 3 month follow-up case series. Ann. Gen. Psychiatry. 2011;10(1):5. doi: 10.1186/1744-859X-10-5. [http://dx.doi.org/10.1186/1744-859X-10-5]. [PMID: 21356085]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Tzavellas E., Karaiskos D., Ilias I., Liappas I., Paparrigopoulos T. Agomelatine augmentation in obsessive compulsive disorder: a preliminary report. Psychiatriki. 2014;25(3):179–184. [PMID: 25367661]. [PubMed] [Google Scholar]
- 101.Roca A., Garcia-Esteve L., Imaz M.L., Torres A., Hernández S., Botet F., Gelabert E., Subirà S., Plaza A., Valdés M., Martin-Santos R. Obstetrical and neonatal outcomes after prenatal exposure to selective serotonin reuptake inhibitors: the relevance of dose. J. Affect. Disord. 2011;135(1-3):208–215. doi: 10.1016/j.jad.2011.07.022. [http://dx.doi. org/10.1016/j.jad.2011.07.022]. [PMID: 21890210]. [DOI] [PubMed] [Google Scholar]
- 102.Koran L.M., Gamel N.N., Choung H.W., Smith E.H., Aboujaoude E.N. Mirtazapine for obsessive-compulsive disorder: an open trial followed by double-blind discontinuation. J. Clin. Psychiatry. 2005;66(4):515–520. [http://dx.doi.org/10.4088/JCP. v66n0415]. [PMID: 15816795]. [PubMed] [Google Scholar]
- 103.Pigott T.A., L’Heureux F., Rubenstein C.S., Bernstein S.E., Hill J.L., Murphy D.L. A double-blind, placebo controlled study of trazodone in patients with obsessive-compulsive disorder. J. Clin. Psychopharmacol. 1992;12(3):156–162. [PubMed] [Google Scholar]
- 104.McDougle C.J., Epperson C.N., Pelton G.H., Wasylink S., Price L.H. A double-blind, placebo-controlled study of risperidone addition in serotonin reuptake inhibitor-refractory obsessive-compulsive disorder. Arch. Gen. Psychiatry. 2000;57(8):794–801. doi: 10.1001/archpsyc.57.8.794. [http://dx.doi.org/10.1001/archpsyc.57.8.794]. [PMID: 10920469]. [DOI] [PubMed] [Google Scholar]
- 105.Ravindran L.N., Jung S.M., Ravindran A.V. Intravenous anti-obsessive agents: a review. J. Psychopharmacol. (Oxford) 2010;24(3):287–296. doi: 10.1177/0269881108096508. [http://dx.doi.org/10.1177/0269881108096508]. [PMID: 18801828]. [DOI] [PubMed] [Google Scholar]
- 106.Pallanti S., Quercioli L., Koran L.M. Citalopram intravenous infusion in resistant obsessive-compulsive disorder: an open trial. J. Clin. Psychiatry. 2002;63(9):796–801. [http://dx.doi.org/10.4088/ JCP.v63n0908]. [PMID: 12363120]. [PubMed] [Google Scholar]
- 107.Fallon B.A., Liebowitz M.R., Campeas R., Schneier F.R., Marshall R., Davies S., Goetz D., Klein D.F. Intravenous clomipramine for obsessive-compulsive disorder refractory to oral clomipramine: a placebo-controlled study. Arch. Gen. Psychiatry. 1998;55(10):918–924. doi: 10.1001/archpsyc.55.10.918. [http://dx.doi.org/10.1001/archpsyc.55.10. 918]. [PMID: 9783563]. [DOI] [PubMed] [Google Scholar]
- 108.Koran L.M., Sallee F.R., Pallanti S. Rapid benefit of intravenous pulse loading of clomipramine in obsessive-compulsive disorder. Am. J. Psychiatry. 1997;154(3):396–401. doi: 10.1176/ajp.154.3.396. [http://dx.doi.org/10. 1176/ajp.154.3.396]. [PMID: 9054789]. [DOI] [PubMed] [Google Scholar]
- 109.Rabinowitz I., Baruch Y., Barak Y. High-dose escitalopram for the treatment of obsessive-compulsive disorder. Int. Clin. Psychopharmacol. 2008;23(1):49–53. doi: 10.1097/YIC.0b013e3282f0f0c5. [http://dx.doi.org/10.1097/YIC. 0b013e3282f0f0c5]. [PMID: 18090508]. [DOI] [PubMed] [Google Scholar]
- 110.Dougherty D.D., Jameson M., Deckersbach T., Loh R., Thompson-Hollands J., Jenike M., Keuthen N.J. Open-label study of high (30 mg) and moderate (20 mg) dose escitalopram for the treatment of obsessive-compulsive disorder. Int. Clin. Psychopharmacol. 2009;24(6):306–311. doi: 10.1097/YIC.0b013e32833119d8. [http://dx.doi.org/10.1097/YIC. 0b013e32833119d8]. [PMID: 19730388]. [DOI] [PubMed] [Google Scholar]
- 111.Hollander E., Bienstock C.A., Koran L.M., Pallanti S., Marazziti D., Rasmussen S.A., Ravizza L., Benkelfat C., Saxena S., Greenberg B.D., Sasson Y., Zohar J. Refractory obsessive-compulsive disorder: state-of-the-art treatment. J. Clin. Psychiatry. 2002;63(Suppl. 6):20–29. [PMID: 12027116]. [PubMed] [Google Scholar]
- 112.Denys D., Zohar J., Westenberg H.G. The role of dopamine in obsessive-compulsive disorder: preclinical and clinical evidence. J. Clin. Psychiatry. 2004;65(Suppl. 14):11–17. [PMID: 15554783]. [PubMed] [Google Scholar]
- 113.Schirmbeck F., Zink M. Comorbid obsessive-compulsive symptoms in schizophrenia: contributions of pharmacological and genetic factors. Front. Pharmacol. 2013;4:99. doi: 10.3389/fphar.2013.00099. [http://dx.doi.org/10. 3389/fphar.2013.00099]. [PMID: 23950745]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Gordon A. Transition of obsessions into delusions. Evaluation of obsessional phenomena from the prognostic standpoint. Am. J. Psychiatry. 1950;107(6):455–458. doi: 10.1176/ajp.107.6.455. [http://dx.doi.org/10.1176/ ajp.107.6.455]. [PMID: 14838150]. [DOI] [PubMed] [Google Scholar]
- 115.Klemperer F. Compulsions developing into command hallucinations. Psychopathology. 1996;29(4):249–251. doi: 10.1159/000285001. [http://dx.doi.org/ 10.1159/000285001]. [PMID: 8865357]. [DOI] [PubMed] [Google Scholar]
- 116.Devi S., Rao N.P., Badamath S., Chandrashekhar C.R., Janardhan Reddy Y.C. Prevalence and clinical correlates of obsessive-compulsive disorder in schizophrenia. Compr. Psychiatry. 2015;56:141–148. doi: 10.1016/j.comppsych.2014.09.015. [http://dx.doi.org/10.1016/j.comppsych.2014.09.015]. [PMID: 25308405]. [DOI] [PubMed] [Google Scholar]
- 117.Kapur S., Remington G. Serotonin-dopamine interaction and its relevance to schizophrenia. Am. J. Psychiatry. 1996;153(4):466–476. doi: 10.1176/ajp.153.4.466. [http://dx.doi.org/10.1176/ajp.153.4.466]. [PMID: 8599393]. [DOI] [PubMed] [Google Scholar]
- 118.Pollitt J.D. Natural history studies in mental illness. A discussion based on a pilot study of obsessional states. J. Ment. Sci. 1960;106:93–113. doi: 10.1192/bjp.106.442.93. [http://dx.doi.org/10.1192/bjp.106.442.93]. [PMID: 14433876]. [DOI] [PubMed] [Google Scholar]
- 119.Ingram I.M. Obsessional illness in mental hospital patients. J. Ment. Sci. 1961;107:382–402. doi: 10.1192/bjp.107.448.382. [http://dx.doi.org/10.1192/bjp.107. 448.382]. [PMID: 13717718]. [DOI] [PubMed] [Google Scholar]
- 120.Lo W.H. A follow-up study of obsessional neurotics in Hong Kong Chinese. Br. J. Psychiatry. 1967;113(501):823–832. doi: 10.1192/bjp.113.501.823. [http://dx.doi.org/10.1192/bjp.113.501.823]. [PMID: 6048368]. [DOI] [PubMed] [Google Scholar]
- 121.Welner A., Reich T., Robins E., Fishman R., Van Doren T. Obsessive-compulsive neurosis: record, follow-up, and family studies. I. Inpatient record study. Compr. Psychiatry. 1976;17(4):527–539. doi: 10.1016/0010-440x(76)90035-3. [http://dx.doi.org/10.1016/0010-440X(76)90035-3]. [PMID: 963994]. [DOI] [PubMed] [Google Scholar]
- 122.Jenike M.A., Baer L., Minichiello W.E., Schwartz C.E., Carey R.J., Jr Coexistent obsessive-compulsive disorder and schizotypal personality disorder: a poor prognostic indicator. Arch. Gen. Psychiatry. 1986;43(3):296. doi: 10.1001/archpsyc.1986.01800030114016. [http://dx.doi.org/10.1001/archpsyc. 1986.01800030114016]. [PMID: 3954553]. [DOI] [PubMed] [Google Scholar]
- 123.Joffe R.T., Swinson R.P., Regan J.J. Personality features of obsessive-compulsive disorder. Am. J. Psychiatry. 1988;145(9):1127–1129. doi: 10.1176/ajp.145.9.1127. [http://dx.doi.org/10.1176/ajp.145.9.1127]. [PMID: 3414855]. [DOI] [PubMed] [Google Scholar]
- 124.Baer L., Jenike M.A., Ricciardi J.N., II, Holland A.D., Seymour R.J., Minichiello W.E., Buttolph M.L. Standardized assessment of personality disorders in obsessive-compulsive disorder. Arch. Gen. Psychiatry. 1990;47(9):826–830. doi: 10.1001/archpsyc.1990.01810210034005. [http://dx.doi.org/10.1001/ archpsyc.1990.01810210034005]. [PMID: 2393341]. [DOI] [PubMed] [Google Scholar]
- 125.Ganesan V., Kumar T.C., Khanna S. Obsessive--compulsive disorder and psychosis. Can. J. Psychiatry. 2001;46(8):750–754. doi: 10.1177/070674370104600809. [http://dx.doi.org/10.1177/070674370104600809]. [PMID: 11692979]. [DOI] [PubMed] [Google Scholar]
- 126.American Psychiatric Association. Practice Guidelines for the Treatment of Patients with Obsessive-Compulsive Disorder. Arlington, VA: American Psychiatric Association; 2007. [Google Scholar]
- 127.Bandelow B., Zohar J., Hollander E., Kasper S., Möller H.J., Zohar J., Hollander E., Kasper S., Möller H.J., Bandelow B., Allgulander C., Ayuso-Gutierrez J., Baldwin D.S., Buenvicius R., Cassano G., Fineberg N., Gabriels L., Hindmarch I., Kaiya H., Klein D.F., Lader M., Lecrubier Y., Lépine J.P., Liebowitz M.R., Lopez-Ibor J.J., Marazziti D., Miguel E.C., Oh K.S., Preter M., Rupprecht R., Sato M., Starcevic V., Stein D.J., van Ameringen M., Vega J. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the pharmacological treatment of anxiety, obsessive-compulsive and post-traumatic stress disorders - first revision. World J. Biol. Psychiatry. 2008;9(4):248–312. doi: 10.1080/15622970802465807. [http://dx.doi.org/10.1080/15622970802465807]. [PMID: 18949648]. [DOI] [PubMed] [Google Scholar]
- 128.Van Ameringen M., Simpson W., Patterson B., Dell’Osso B., Fineberg N., Hollander E., Hranov L., Hranov G., Lochner C., Karamustafalioglu O., Marazziti D., Menchon J.M., Nicolini H., Pallanti S., Stein D.J., Zohar J. Pharmacological treatment strategies in obsessive compulsive disorder: A cross-sectional view in nine international OCD centers. J. Psychopharmacol. (Oxford) 2014;28(6):596–602. doi: 10.1177/0269881113517955. [http://dx.doi.org/10.1177/0269881113517955]. [PMID: 24429223]. [DOI] [PubMed] [Google Scholar]
- 129.Phillips K.A. Placebo-controlled study of pimozide augmentation of fluoxetine in body dysmorphic disorder. Am. J. Psychiatry. 2005;162(2):377–379. doi: 10.1176/appi.ajp.162.2.377. [http://dx.doi.org/10.1176/appi.ajp.162.2.377]. [PMID: 15677604]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Albert U., Carmassi C., Cosci F., De Cori D., Di Nicola M., Ferrari S., Poloni N., Tarricone I., Fiorillo A. Role and clinical implications of atypical antipsychotics in anxiety disorders, obsessive-compulsive disorder, trauma-related, and somatic symptom disorders: a systematized review. Int. Clin. Psychopharmacol. 2016;31(5):249–258. doi: 10.1097/YIC.0000000000000127. [http://dx.doi.org/10.1097/YIC. 0000000000000127]. [PMID: 26974213]. [DOI] [PubMed] [Google Scholar]
- 131.Albert U., Marazziti D., Di Salvo G., Solia F., Rosso G., Maina G. A systematic review of evidence-based treatment strategies for obsessive-compulsive disorder resistant to first-line pharmacotherapy. Curr. Med. Chem. 2018;25(41):5647–5661. doi: 10.2174/0929867325666171222163645. [http://dx. doi.org/10.2174/0929867325666171222163645]. [PMID: 29278206]. [DOI] [PubMed] [Google Scholar]
- 132.Komossa K., Depping A.M., Meyer M., Kissling W., Leucht S. Second-generation antipsychotics for obsessive compulsive disorder. Cochrane Database Syst. Rev. 2010;12(12):CD008141. doi: 10.1002/14651858.CD008141.pub2. [PMID: 21154394]. [DOI] [PubMed] [Google Scholar]
- 133.Dold M., Aigner M., Lanzenberger R., Kasper S. Antipsychotic augmentation of serotonin reuptake inhibitors in treatment-resistant obsessive-compulsive disorder: a meta-analysis of double-blind, randomized, placebo-controlled trials. Int. J. Neuropsychopharmacol. 2013;16(3):557–574. doi: 10.1017/S1461145712000740. [http://dx.doi.org/10.1017/S146114571 2000740]. [PMID: 22932229]. [DOI] [PubMed] [Google Scholar]
- 134.Li X., May R.S., Tolbert L.C., Jackson W.T., Flournoy J.M., Baxter L.R. Risperidone and haloperidol augmentation of serotonin reuptake inhibitors in refractory obsessive-compulsive disorder: a crossover study. J. Clin. Psychiatry. 2005;66(6):736–743. doi: 10.4088/jcp.v66n0610. [http://dx.doi.org/10.4088/JCP.v66n0610]. [PMID: 15960567]. [DOI] [PubMed] [Google Scholar]
- 135.Hollander E., Baldini R.N., Sood E., Pallanti S. Risperidone augmentation in treatment-resistant obsessive-compulsive disorder: a double-blind, placebo-controlled study. Int. J. Neuropsychopharmacol. 2003;6(4):397–401. doi: 10.1017/S1461145703003730. [http://dx.doi.org/10.1017/S14611 45703003730]. [PMID: 14604454]. [DOI] [PubMed] [Google Scholar]
- 136.Buchsbaum M.S., Hollander E., Pallanti S., Baldini R.N., Platholi J., Newmark R., Bloom R., Sood E. Positron emission tomography imaging of risperidone augmentation in serotonin reuptake inhibitor-refractory patients. Neuropsychobiology. 2006;53(3):157–168. doi: 10.1159/000093342. [http://dx.doi.org/10.1159/000093342]. [PMID: 16707915]. [DOI] [PubMed] [Google Scholar]
- 137.Erzegovesi S., Guglielmo E., Siliprandi F., Bellodi L. Low-dose risperidone augmentation of fluvoxamine treatment in obsessive-compulsive disorder: a double-blind, placebo-controlled study. Eur. Neuropsychopharmacol. 2005;15(1):69–74. doi: 10.1016/j.euroneuro.2004.04.004. [http://dx.doi.org/10. 1016/j.euroneuro.2004.04.004]. [PMID: 15572275]. [DOI] [PubMed] [Google Scholar]
- 138.Simpson H.B., Foa E.B., Liebowitz M.R., Huppert J.D., Cahill S., Maher M.J., McLean C.P., Bender J., Jr, Marcus S.M., Williams M.T., Weaver J., Vermes D., Van Meter P.E., Rodriguez C.I., Powers M., Pinto A., Imms P., Hahn C.G., Campeas R. Cognitive-behavioral therapy vs. risperidone for augmenting serotonin reuptake inhibitors in obsessive-compulsive disorder: a randomized clinical trial. JAMA Psychiatry. 2013;70(11):1190–1199. doi: 10.1001/jamapsychiatry.2013.1932. [http://dx.doi.org/10.1001/jamapsychiatry.2013.1932]. [PMID: 24026523]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Savas H.A., Yumru M., Ozen M.E. Quetiapine and ziprasidone as adjuncts in treatment-resistant obsessive-compulsive disorder: a retrospective comparative study. Clin. Drug Investig. 2008;28(7):439–442. doi: 10.2165/00044011-200828070-00005. [http://dx.doi.org/10.2165/00044011-200828070-00005]. [PMID: 18544004]. [DOI] [PubMed] [Google Scholar]
- 140.Maina G., Pessina E., Albert U., Bogetto F. 8-week, single-blind, randomized trial comparing risperidone versus olanzapine augmentation of serotonin reuptake inhibitors in treatment-resistant obsessive-compulsive disorder. Eur. Neuropsychopharmacol. 2008;18(5):364–372. doi: 10.1016/j.euroneuro.2008.01.001. [http://dx.doi.org/10.1016/j.euroneuro.2008. 01.001]. [PMID: 18280710]. [DOI] [PubMed] [Google Scholar]
- 141.Selvi Y., Atli A., Aydin A., Besiroglu L., Ozdemir P., Ozdemir O. The comparison of aripiprazole and risperidone augmentation in selective serotonin reuptake inhibitor-refractory obsessive-compulsive disorder: a single-blind, randomised study. Hum. Psychopharmacol. 2011;26(1):51–57. doi: 10.1002/hup.1169. [http://dx.doi.org/10.1002/hup. 1169]. [PMID: 21308781]. [DOI] [PubMed] [Google Scholar]
- 142.Vulink N.C., Denys D., Fluitman S.B., Meinardi J.C., Westenberg H.G. Quetiapine augments the effect of citalopram in non-refractory obsessive-compulsive disorder: a randomized, double-blind, placebo-controlled study of 76 patients. J. Clin. Psychiatry. 2009;70(7):1001–1008. doi: 10.4088/JCP.08m04269. [http://dx.doi.org/10.4088/JCP.08m04269]. [PMID: 19497245]. [DOI] [PubMed] [Google Scholar]
- 143.Fineberg N.A., Sivakumaran T., Roberts A., Gale T. Adding quetiapine to SRI in treatment-resistant obsessive-compulsive disorder: a randomized controlled treatment study. Int. Clin. Psychopharmacol. 2005;20(4):223–226. doi: 10.1097/00004850-200507000-00005. [http://dx.doi.org/10.1097/ 00004850-200507000-00005]. [PMID: 15933483]. [DOI] [PubMed] [Google Scholar]
- 144.Atmaca M., Kuloglu M., Tezcan E., Gecici O. Quetiapine augmentation in patients with treatment resistant obsessive-compulsive disorder: a single-blind, placebo-controlled study. Int. Clin. Psychopharmacol. 2002;17(3):115–119. doi: 10.1097/00004850-200205000-00004. [http://dx.doi.org/10.1097/ 00004850-200205000-00004]. [PMID: 11981352]. [DOI] [PubMed] [Google Scholar]
- 145.Denys D., de Geus F., van Megen H.J., Westenberg H.G. A double-blind, randomized, placebo-controlled trial of quetiapine addition in patients with obsessive-compulsive disorder refractory to serotonin reuptake inhibitors. J. Clin. Psychiatry. 2004;65(8):1040–1048. doi: 10.4088/jcp.v65n0803. [http://dx.doi.org/10.4088/JCP.v65n0803]. [PMID: 15323587]. [DOI] [PubMed] [Google Scholar]
- 146.Carey P.D., Vythilingum B., Seedat S., Muller J.E., van Ameringen M., Stein D.J. Quetiapine augmentation of SRIs in treatment refractory obsessive-compulsive disorder: a double-blind, randomised, placebo-controlled study. BMC Psychiatry. 2005;5(5):5. doi: 10.1186/1471-244X-5-5. [ISRCTN83050762]. [http://dx.doi.org/10.1186/1471-244X-5-5]. [PMID: 15667657]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147.Kordon A., Wahl K., Koch N., Zurowski B., Anlauf M., Vielhaber K., Kahl K.G., Broocks A., Voderholzer U., Hohagen F. Quetiapine addition to serotonin reuptake inhibitors in patients with severe obsessive-compulsive disorder: a double-blind, randomized, placebo-controlled study. J. Clin. Psychopharmacol. 2008;28(5):550–554. doi: 10.1097/JCP.0b013e318185e735. [http://dx.doi.org/10.1097/JCP.0b013e318185e735]. [PMID: 18794652]. [DOI] [PubMed] [Google Scholar]
- 148.Dold M., Aigner M., Lanzenberger R., Kasper S. Antipsychotic augmentation of serotonin reuptake inhibitors in treatment-resistant obsessive-compulsive disorder: an update meta-analysis of double-blind, randomized, placebo-controlled trials. Int. J. Neuropsychopharmacol. 2015;18(9) doi: 10.1093/ijnp/pyv047. [http://dx.doi.org/10.1093/ijnp/pyv047]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Veale D., Miles S., Smallcombe N., Ghezai H., Goldacre B., Hodsoll J. Atypical antipsychotic augmentation in SSRI treatment refractory obsessive-compulsive disorder: a systematic review and meta-analysis. BMC Psychiatry. 2014;14:317. doi: 10.1186/s12888-014-0317-5. [http://dx.doi. org/10.1186/s12888-014-0317-5]. [PMID: 25432131]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.McDougle C.J., Goodman W.K., Leckman J.F., Lee N.C., Heninger G.R., Price L.H. Haloperidol addition in fluvoxamine-refractory obsessive-compulsive disorder. A double-blind, placebo-controlled study in patients with and without tics. Arch. Gen. Psychiatry. 1994;51(4):302–308. doi: 10.1001/archpsyc.1994.03950040046006. [http://dx.doi.org/10.1001/archpsyc. 1994.03950040046006]. [PMID: 8161290]. [DOI] [PubMed] [Google Scholar]
- 151.Mohr N., Vythilingum B., Emsley R.A., Stein D.J. Quetiapine augmentation of serotonin reuptake inhibitors in obsessive-compulsive disorder. Int. Clin. Psychopharmacol. 2002;17(1):37–40. doi: 10.1097/00004850-200201000-00006. [http://dx.doi.org/10.1097/00004850-200201000-00006]. [PMID: 11800505]. [DOI] [PubMed] [Google Scholar]
- 152.Bogetto F., Bellino S., Vaschetto P., Ziero S. Olanzapine augmentation of fluvoxamine-refractory obsessive-compulsive disorder (OCD): a 12-week open trial. Psychiatry Res. 2000;96(2):91–98. doi: 10.1016/s0165-1781(00)00203-1. [http://dx.doi.org/10.1016/S0165-1781(00)00203-1]. [PMID: 11063782]. [DOI] [PubMed] [Google Scholar]
- 153.Metin O., Yazici K., Tot S., Yazici A.E. Amisulpiride augmentation in treatment resistant obsessive-compulsive disorder: an open trial. Hum. Psychopharmacol. 2003;18(6):463–467. doi: 10.1002/hup.512. [http://dx. doi.org/10.1002/hup.512]. [PMID: 12923825]. [DOI] [PubMed] [Google Scholar]
- 154.Uguz F. Successful treatment of comorbid obsessive-compulsive disorder with aripiprazole in three patients with bipolar disorder. Gen. Hosp. Psychiatry. 2010;32(5):556–558. doi: 10.1016/j.genhosppsych.2010.07.004. [http://dx.doi.org/10. 1016/j.genhosppsych.2010.07.004]. [PMID: 20851277]. [DOI] [PubMed] [Google Scholar]
- 155.Glick I.D., Poyurovsky M., Ivanova O., Koran L.M. Aripiprazole in schizophrenia patients with comorbid obsessive-compulsive symptoms: an open-label study of 15 patients. J. Clin. Psychiatry. 2008;69(12):1856–1859. doi: 10.4088/jcp.v69n1202. [http://dx.doi.org/10.4088/JCP.v69n1202]. [PMID: 19026264]. [DOI] [PubMed] [Google Scholar]
- 156.Murphy T.K., Mutch P.J., Reid J.M., Edge P.J., Storch E.A., Bengtson M., Yang M. Open label aripiprazole in the treatment of youth with tic disorders. J. Child Adolesc. Psychopharmacol. 2009;19(4):441–447. doi: 10.1089/cap.2008.0149. [http://dx.doi.org/10.1089/cap.2008.0149]. [PMID: 19702496]. [DOI] [PubMed] [Google Scholar]
- 157.Connor K.M., Payne V.M., Gadde K.M., Zhang W., Davidson J.R. The use of aripiprazole in obsessive-compulsive disorder: preliminary observations in 8 patients. J. Clin. Psychiatry. 2005;66(1):49–51. doi: 10.4088/jcp.v66n0107. [http://dx.doi.org/10.4088/JCP.v66n0107]. [PMID: 15669888]. [DOI] [PubMed] [Google Scholar]
- 158.da Rocha F.F., Correa H. Successful augmentation with aripiprazole in clomipramine-refractory obsessive-compulsive disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry. 2007;31(7):1550–1551. doi: 10.1016/j.pnpbp.2007.07.008. [http://dx.doi.org/10.1016/j.pnpbp.2007.07.008]. [PMID: 17692447]. [DOI] [PubMed] [Google Scholar]
- 159.Sarkar R., Klein J., Krüger S. Aripiprazole augmentation in treatment-refractory obsessive-compulsive disorder. Psychopharmacology (Berl.) 2008;197(4):687–688. doi: 10.1007/s00213-008-1091-1. [http://dx.doi.org/ 10.1007/s00213-008-1091-1]. [PMID: 18264798]. [DOI] [PubMed] [Google Scholar]
- 160.Fornaro M., Gabrielli F., Mattei C., Vinciguerra V., Fornaro P. Aripiprazole augmentation in poor insight obsessive-compulsive disorder: a case report. Ann. Gen. Psychiatry. 2008;7:26. doi: 10.1186/1744-859X-7-26. [http://dx.doi.org/10.1186/1744-859X-7-26]. [PMID: 19105842]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 161.Storch E.A., Lehmkuhl H., Geffken G.R., Touchton A., Murphy T.K. Aripiprazole augmentation of incomplete treatment response in an adolescent male with obsessive-compulsive disorder. Depress. Anxiety. 2008;25(2):172–174. doi: 10.1002/da.20303. [http://dx.doi.org/10.1002/ da.20303]. [PMID: 17340610]. [DOI] [PubMed] [Google Scholar]
- 162.Pessina E., Albert U., Bogetto F., Maina G. Aripiprazole augmentation of serotonin reuptake inhibitors in treatment-resistant obsessive-compulsive disorder: a 12-week open-label preliminary study. Int. Clin. Psychopharmacol. 2009;24(5):265–269. doi: 10.1097/YIC.0b013e32832e9b91. [http:// dx.doi.org/10.1097/YIC.0b013e32832e9b91]. [PMID: 19629012]. [DOI] [PubMed] [Google Scholar]
- 163.Masi G., Pfanner C., Millepiedi S., Berloffa S. Aripiprazole augmentation in 39 adolescents with medication-resistant obsessive-compulsive disorder. J. Clin. Psychopharmacol. 2010;30(6):688–693. doi: 10.1097/jcp.0b013e3181fab7b1. [http://dx.doi.org/10.1097/JCP.0b013e3181fab7b1]. [PMID: 21105283]. [DOI] [PubMed] [Google Scholar]
- 164.Delle Chiaie R., Scarciglia P., Pasquini M., Caredda M., Biondi M. Aripiprazole augmentation in patients with resistant obsessive compulsive disorder: a pilot study. Clin. Pract. Epidemiol. Ment. Health. 2011;7:107–111. doi: 10.2174/1745017901107010107. [http://dx.doi.org/10.2174/17450179011 07010107]. [PMID: 21686322]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 165.Matsunaga H., Hayashida K., Maebayashi K., Mito H., Kiriike N. A case series of aripiprazole augmentation of selective serotonin reuptake inhibitors in treatment-refractory obsessive compulsive disorder. Int. J. Psychiatry Clin. Pract. 2011;15(4):263–269. doi: 10.3109/13651501.2011.605958. [http:// dx.doi.org/10.3109/13651501.2011.605958]. [PMID: 22121999]. [DOI] [PubMed] [Google Scholar]
- 166.Muscatello M.R., Bruno A., Pandolfo G., Micò U., Scimeca G., Romeo V.M., Santoro V., Settineri S., Spina E., Zoccali R.A. Effect of aripiprazole augmentation of serotonin reuptake inhibitors or clomipramine in treatment-resistant obsessive-compulsive disorder: a double-blind, placebo-controlled study. J. Clin. Psychopharmacol. 2011;31(2):174–179. doi: 10.1097/JCP.0b013e31820e3db6. [http://dx.doi.org/10.1097/JCP. 0b013e31820e3db6]. [PMID: 21346614]. [DOI] [PubMed] [Google Scholar]
- 167.Sayyah M., Sayyah M., Boostani H., Ghaffari S.M., Hoseini A. Effects of aripiprazole augmentation in treatment-resistant obsessive-compulsive disorder (a double blind clinical trial). Depress. Anxiety. 2012;29(10):850–854. doi: 10.1002/da.21996. [http://dx.doi.org/10.1002/da. 21996]. [PMID: 22933237]. [DOI] [PubMed] [Google Scholar]
- 168.Leucht S., Cipriani A., Spineli L., Mavridis D., Orey D., Richter F., Samara M., Barbui C., Engel R.R., Geddes J.R., Kissling W., Stapf M.P., Lässig B., Salanti G., Davis J.M. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet. 2013;382(9896):951–962. doi: 10.1016/S0140-6736(13)60733-3. [http://dx.doi.org/10.1016/S0140-6736(13)60733-3]. [PMID: 23810019]. [DOI] [PubMed] [Google Scholar]
- 169.Storch E.A., Goddard A.W., Grant J.E., De Nadai A.S., Goodman W.K., Mutch P.J., Medlock C., Odlaug B., McDougle C.J., Murphy T.K. Double-blind, placebo-controlled, pilot trial of paliperidone augmentation in serotonin reuptake inhibitor-resistant obsessive-compulsive disorder. J. Clin. Psychiatry. 2013;74(6):e527–e532. doi: 10.4088/JCP.12m08278. [http://dx.doi.org/10.4088/JCP.12m08278]. [PMID: 23842022]. [DOI] [PubMed] [Google Scholar]
- 170.McDougle C.J., Barr L.C., Goodman W.K., Pelton G.H., Aronson S.C., Anand A., Price L.H. Lack of efficacy of clozapine monotherapy in refractory obsessive-compulsive disorder. Am. J. Psychiatry. 1995;152(12):1812–1814. doi: 10.1176/ajp.152.12.1812. [http://dx.doi.org/10.1176/ ajp.152.12.1812]. [PMID: 8526253]. [DOI] [PubMed] [Google Scholar]
- 171.Englisch S., Esslinger C., Inta D., Weinbrenner A., Peus V., Gutschalk A., Schirmbeck F., Zink M. Clozapine-induced obsessive-compulsive syndromes improve in combination with aripiprazole. Clin. Neuropharmacol. 2009;32(4):227–229. doi: 10.1097/WNF.0b013e31819cc8e6. [http://dx.doi. org/10.1097/WNF.0b013e31819cc8e6]. [PMID: 19644230]. [DOI] [PubMed] [Google Scholar]
- 172.Sa A.R., Hounie A.G., Sampaio A.S., Arrais J., Miguel E.C., Elkis H. Obsessive-compulsive symptoms and disorder in patients with schizophrenia treated with clozapine or haloperidol. Compr. Psychiatry. 2009;50(5):437–442. doi: 10.1016/j.comppsych.2008.11.005. [http://dx.doi.org/10.1016/j. comppsych.2008.11.005]. [PMID: 19683614]. [DOI] [PubMed] [Google Scholar]
- 173.Scheltema Beduin A.A., Swets M., Machielsen M., Korver N. Obsessive-compulsive symptoms in patients with schizophrenia: a naturalistic cross-sectional study comparing treatment with clozapine, olanzapine, risperidone, and no antipsychotics in 543 patients. J. Clin. Psychiatry. 2012;73(11):1395–1402. doi: 10.4088/JCP.11m07164. [http://dx.doi.org/10. 4088/JCP.11m07164]. [PMID: 23218156]. [DOI] [PubMed] [Google Scholar]
- 174.Gahr M., Rehbaum K., Connemann B.J. Clozapine-associated development of second-onset obsessive compulsive symptoms in schizophrenia: impact of clozapine serum levels and fluvoxamine add-on. Pharmacopsychiatry. 2014;47(3):118–120. doi: 10.1055/s-0034-1374611. [http://dx. doi.org/10.1055/s-0034-1374611]. [PMID: 24846087]. [DOI] [PubMed] [Google Scholar]
- 175.Grover S., Hazari N., Chakrabarti S., Avasthi A. Relationship of obsessive compulsive symptoms/disorder with clozapine: A retrospective study from a multispeciality tertiary care centre. Asian J. Psychiatr. 2015;15:56–61. doi: 10.1016/j.ajp.2015.05.002. [http://dx.doi.org/10.1016/j.ajp.2015. 05.002]. [PMID: 26013671]. [DOI] [PubMed] [Google Scholar]
- 176.Schirmbeck F., Mier D., Esslinger C., Rausch F., Englisch S., Eifler S., Meyer-Lindenberg A., Kirsch P., Zink M. Increased orbitofrontal cortex activation associated with “pro-obsessive” antipsychotic treatment in patients with schizophrenia. J. Psychiatry Neurosci. 2015;40(2):89–99. doi: 10.1503/jpn.140021. [PMID: 25268790]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 177.Schirmbeck F., Zink M. Clozapine-induced obsessive-compulsive symptoms in schizophrenia: a critical review. Curr. Neuropharmacol. 2012;10(1):88–95. doi: 10.2174/157015912799362724. [http://dx.doi.org/10.2174/1570159127 99362724]. [PMID: 22942882]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 178.Levkovitch Y., Kronnenberg Y., Gaoni B. Can clozapine trigger OCD? J. Am. Acad. Child Adolesc. Psychiatry. 1995;34(3):263. doi: 10.1097/00004583-199503000-00005. [http://dx.doi.org/10.1097/00004583-199503000-00005]. [PMID: 7896662]. [DOI] [PubMed] [Google Scholar]
- 179.Eales M.J., Layeni A.O. Exacerbation of obsessive-compulsive symptoms associated with clozapine. Br. J. Psychiatry. 1994;164(5):687–688. doi: 10.1192/bjp.164.5.687. [http://dx.doi.org/10.1192/bjp.164.5.687]. [PMID: 7921724]. [DOI] [PubMed] [Google Scholar]
- 180.Leung J.G., Palmer B.A. Psychosis or Obsessions? Clozapine Associated with Worsening Obsessive-Compulsive Symptoms. Case Rep. Psychiatry. 2016;2016:2180748. doi: 10.1155/2016/2180748. [http://dx.doi.org/ 10.1155/2016/2180748]. [PMID: 27313938]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 181.Del Casale A., Kotzalidis G.D., Rapinesi C., Serata D., Ambrosi E., Simonetti A., Pompili M., Ferracuti S., Tatarelli R., Girardi P. Functional neuroimaging in obsessive-compulsive disorder. Neuropsychobiology. 2011;64(2):61–85. doi: 10.1159/000325223. [http://dx.doi.org/10. 1159/000325223]. [PMID: 21701225]. [DOI] [PubMed] [Google Scholar]
- 182.Del Casale A., Rapinesi C., Kotzalidis G.D., De Rossi P., Curto M., Janiri D., Criscuolo S., Alessi M.C., Ferri V.R., De Giorgi R., Sani G., Ferracuti S., Girardi P., Brugnoli R. Executive functions in obsessive-compulsive disorder: An activation likelihood estimate meta-analysis of fMRI studies. World J. Biol. Psychiatry. 2016;17(5):378–393. doi: 10.3109/15622975.2015.1102323. [http://dx.doi.org/10.3109/15622975.2015. 1102323]. [PMID: 26642972]. [DOI] [PubMed] [Google Scholar]
- 183.Schirmbeck F., Esslinger C., Rausch F., Englisch S., Meyer-Lindenberg A., Zink M. Antiserotonergic antipsychotics are associated with obsessive-compulsive symptoms in schizophrenia. Psychol. Med. 2011;41(11):2361–2373. doi: 10.1017/S0033291711000419. [http://dx.doi.org/10.1017/ S0033291711000419]. [PMID: 21466748]. [DOI] [PubMed] [Google Scholar]
- 184.Cai J., Zhang W., Yi Z., Lu W., Wu Z., Chen J., Yu S., Fang Y., Zhang C. Influence of polymorphisms in genes SLC1A1, GRIN2B, and GRIK2 on clozapine-induced obsessive-compulsive symptoms. Psychopharmacology (Berl.) 2013;230(1):49–55. doi: 10.1007/s00213-013-3137-2. [http://dx.doi.org/10.1007/s00213-013-3137-2]. [PMID: 23660601]. [DOI] [PubMed] [Google Scholar]
- 185.Lin S.K., Su S.F., Pan C.H. Higher plasma drug concentration in clozapine-treated schizophrenic patients with side effects of obsessive/compulsive symptoms. Ther. Drug Monit. 2006;28(3):303–307. doi: 10.1097/01.ftd.0000211801.66569.80. [http://dx.doi.org/10.1097/01.ftd.0000211801.66569.80]. [PMID: 16778711]. [DOI] [PubMed] [Google Scholar]
- 186.Andrade C. Serotonin reuptake inhibitor treatment of obsessive-compulsive symptoms in clozapine-medicated schizophrenia. J. Clin. Psychiatry. 2012;73(11):e1362–e1364. doi: 10.4088/JCP.12f08200. [http://dx.doi.org/ 10.4088/JCP.12f08200]. [PMID: 23218164]. [DOI] [PubMed] [Google Scholar]
- 187.Eryılmaz G., Hızlı Sayar G., Ozten E., Gögcegöz Gül I., Karamustafalıoğlu O. Aripirazole augmentation in clozapine-associated obsessive-compulsive symptoms in schizophrenia. Ann. Gen. Psychiatry. 2013;12(1):40. doi: 10.1186/1744-859X-12-40. [http://dx.doi.org/10.1186/1744-859X-12-40]. [PMID: 24330737]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 188.Cassady S.L., Thaker G.K. Addition of fluoxetine to clozapine. Am. J. Psychiatry. 1992;149(9):1274. [PMID: 1503143]. [PubMed] [Google Scholar]
- 189.Strous R.D., Patel J.K., Zimmet S., Green A.I. Clozapine and paroxetine in the treatment of schizophrenia with obsessive-compulsive features. Am. J. Psychiatry. 1999;156(6):973–974. doi: 10.1176/ajp.156.6.973a. [http://dx.doi.org/10.1176/ajp.156.6.973a]. [PMID: 10360153]. [DOI] [PubMed] [Google Scholar]
- 190.Markowitz J.S., Gill H.S., Lavia M., Brewerton T.D., DeVane C.L. Fluvoxamine-clozapine dose-dependent interaction. Can. J. Psychiatry. 1996;41(10):670–671. doi: 10.1177/070674379604101027. [http://dx.doi.org/10.1177/ 070674379604101027]. [PMID: 8978949]. [DOI] [PubMed] [Google Scholar]
- 191.Zink M., Englisch S., Knopf U., Kuwilsky A., Dressing H. Augmentation of clozapine with valproic Acid for clozapine-induced obsessive-compulsive symptoms. Pharmacopsychiatry. 2007;40(5):202–203. doi: 10.1055/s-2007-985885. [http://dx.doi.org/10.1055/s-2007-985885]. [PMID: 17874353]. [DOI] [PubMed] [Google Scholar]
- 192.Phillips K.A. Placebo-controlled study of pimozide augmentation of fluoxetine in body dysmorphic disorder. Am. J. Psychiatry. 2005;162(2):377–379. doi: 10.1176/appi.ajp.162.2.377. [http://dx.doi.org/10.1176/appi.ajp.162.2. 377]. [PMID: 15677604]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 192.Rao N.P., Antony A., Raveendranathan D., Venkatasubramanian G., Behere R.V., Varambally S.S., Gangadhar B.N. Successful use of maintenance electroconvulsive therapy in the treatment of clozapine-associated obsessive-compulsive symptoms in schizophrenia: a case report. J. ECT. 2011;27(1):e37–e38. doi: 10.1097/YCT.0b013e3181ec0d64. [http://dx. doi.org/10.1097/YCT.0b013e3181ec0d64]. [PMID: 20938347]. [DOI] [PubMed] [Google Scholar]
- 193.Kapur S., Zipursky R.B., Remington G., Jones C., DaSilva J., Wilson A.A., Houle S. 5-HT2 and D2 receptor occupancy of olanzapine in schizophrenia: a PET investigation. Am. J. Psychiatry. 1998;155(7):921–928. doi: 10.1176/ajp.155.7.921. [http://dx.doi.org/10.1176/ajp.155.7.921]. [PMID: 9659858]. [DOI] [PubMed] [Google Scholar]
- 194.Bloch M.H., Landeros-Weisenberger A., Kelmendi B., Coric V., Bracken M.B., Leckman J.F. A systematic review: antipsychotic augmentation with treatment refractory obsessive-compulsive disorder. Mol. Psychiatry. 2006;11(7):622–632. doi: 10.1038/sj.mp.4001823. [http://dx.doi.org/10. 1038/sj.mp.4001823]. [PMID: 16585942]. [DOI] [PubMed] [Google Scholar]
- 195.Matsunaga H., Nagata T., Hayashida K., Ohya K., Kiriike N., Stein D.J. A long-term trial of the effectiveness and safety of atypical antipsychotic agents in augmenting SSRI-refractory obsessive-compulsive disorder. J. Clin. Psychiatry. 2009;70(6):863–868. doi: 10.4088/JCP.08m04369. [http://dx.doi.org/10.4088/JCP.08m04369]. [PMID: 19422759]. [DOI] [PubMed] [Google Scholar]
- 196.Diniz J.B., Shavitt R.G., Fossaluza V., Koran L., Pereira C.A., Miguel E.C. A double-blind, randomized, controlled trial of fluoxetine plus quetiapine or clomipramine versus fluoxetine plus placebo for obsessive-compulsive disorder. J. Clin. Psychopharmacol. 2011;31(6):763–768. doi: 10.1097/JCP.0b013e3182367aee. [http://dx.doi.org/10.1097/JCP. 0b013e3182367aee]. [PMID: 22020357]. [DOI] [PubMed] [Google Scholar]
- 197.Pallanti S., Quercioli L., Paiva R.S., Koran L.M. Citalopram for treatment-resistant obsessive-compulsive disorder. Eur. Psychiatry. 1999;14(2):101–106. doi: 10.1016/s0924-9338(99)80725-1. [http://dx.doi.org/10.1016/S0924-9338(99) 80725-1]. [PMID: 10572334]. [DOI] [PubMed] [Google Scholar]
- 198.Neuvonen P.J., Pohjola-Sintonen S., Tacke U., Vuori E. Five fatal cases of serotonin syndrome after moclobemide-citalopram or moclobemide-clomipramine overdoses. Lancet. 1993;342(8884):1419. doi: 10.1016/0140-6736(93)92774-n. [http://dx.doi.org/10.1016/0140-6736(93)92774-N]. [PMID: 7901695]. [DOI] [PubMed] [Google Scholar]
- 199.Rosebush P.I., Margetts P., Mazurek M.F. Serotonin syndrome as a result of clomipramine monotherapy. J. Clin. Psychopharmacol. 1999;19(3):285–287. doi: 10.1097/00004714-199906000-00021. [http://dx.doi.org/10.1097/00004714-199906000-00021]. [PMID: 10350043]. [DOI] [PubMed] [Google Scholar]
- 200.Carey P.D., Lochner C., Kidd M., Van Ameringen M., Stein D.J., Denys D. Quetiapine augmentation of serotonin reuptake inhibitors in treatment-refractory obsessive-compulsive disorder: is response to treatment predictable? Int. Clin. Psychopharmacol. 2012;27(6):321–325. doi: 10.1097/YIC.0b013e3283576881. [PMID: 22859064]. [DOI] [PubMed] [Google Scholar]
- 201.Berlin H.A., Koran L.M., Jenike M.A., Shapira N.A., Chaplin W., Pallanti S., Hollander E. Double-blind, placebo-controlled trial of topiramate augmentation in treatment-resistant obsessive-compulsive disorder. J. Clin. Psychiatry. 2011;72(5):716–721. doi: 10.4088/JCP.09m05266gre. [http://dx.doi.org/10.4088/JCP.09m05266gre]. [PMID: 20816027]. [DOI] [PubMed] [Google Scholar]
- 202.Mowla A., Khajeian A.M., Sahraian A., Chohedri A.H., Kashkoli F. Topiramate Augmentation in Resistant OCD: A Double-Blind Placebo-Controlled Clinical Trial. CNS Spectr. 2010;15(11):613–617. doi: 10.1017/S1092852912000065. [http://dx.doi.org/10.1017/S1092852912000065]. [PMID: 24726048]. [DOI] [PubMed] [Google Scholar]
- 204.Afshar H., Akuchekian S., Mahaky B., Zarean E. Topiramate augmentation in refractory obsessive-compulsive disorder: A randomized, double-blind, placebo-controlled trial. J. Res. Med. Sci. 2014;19(10):976–981. [PMID: 25538783]. [PMC free article] [PubMed] [Google Scholar]
- 205.Oulis P., Mourikis I., Konstantakopoulos G. Pregabalin augmentation in treatment-resistant obsessive-compulsive disorder. Int. Clin. Psychopharmacol. 2011;26(4):221–224. doi: 10.1097/YIC.0b013e3283466657. [http://dx.doi. org/10.1097/YIC.0b013e3283466657]. [PMID: 21460732]. [DOI] [PubMed] [Google Scholar]
- 206.Uzun O. Lamotrigine as an augmentation agent in treatment-resistant obsessive-compulsive disorder: a case report. J. Psychopharmacol. (Oxford) 2010;24(3):425–427. doi: 10.1177/0269881108098809. [http://dx.doi.org/ 10.1177/0269881108098809]. [PMID: 19010977]. [DOI] [PubMed] [Google Scholar]
- 207.Arrojo-Romero M., Tajes A.M., de Leon J. Lamotrigine augmentation of serotonin reuptake inhibitors in severe and long-term treatment-resistant obsessive-compulsive disorder. Case Rep. Psychiatry. 2013;2013:612459. doi: 10.1155/2013/612459. [http://dx.doi.org/10.1155/2013/ 612459]. [PMID: 23936714]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 208.Bruno A., Micò U., Pandolfo G., Mallamace D., Abenavoli E., Di Nardo F., D’Arrigo C., Spina E., Zoccali R.A., Muscatello M.R. Lamotrigine augmentation of serotonin reuptake inhibitors in treatment-resistant obsessive-compulsive disorder: a double-blind, placebo-controlled study. J. Psychopharmacol. (Oxford) 2012;26(11):1456–1462. doi: 10.1177/0269881111431751. [http://dx.doi.org/10.1177/0269881111431751]. [PMID: 22351381]. [DOI] [PubMed] [Google Scholar]
- 209.Khalkhali M., Aram S., Zarrabi H., Kafie M., Heidarzadeh A. Lamotrigine augmentation versus placebo in serotonin reuptake inhibitors-resistant obsessive-compulsive disorder: a randomized controlled trial. Iran. J. Psychiatry. 2016;11(2):104–114. [PMID: 27437007]. [PMC free article] [PubMed] [Google Scholar]
- 210.Onder E., Tural U., Gökbakan M. Does gabapentin lead to early symptom improvement in obsessive-compulsive disorder? Eur. Arch. Psychiatry Clin. Neurosci. 2008;258(6):319–323. doi: 10.1007/s00406-007-0798-z. [http:// dx.doi.org/10.1007/s00406-007-0798-z]. [PMID: 18297416]. [DOI] [PubMed] [Google Scholar]
- 211.Deltito J.A. Valproate pretreatment for the difficult-to-treat patient with OCD. J. Clin. Psychiatry. 1994;55(11):500. [PMID: 7989288]. [PubMed] [Google Scholar]
- 212.Corá-Locatelli G., Greenberg B.D., Martin J.D., Murphy D.L. Valproate monotherapy in an SRI-intolerant OCD patient. J. Clin. Psychiatry. 1998;59(2):82. doi: 10.4088/jcp.v59n0207b. [http://dx.doi.org/10.4088/JCP.v59n0207b]. [PMID: 9501891]. [DOI] [PubMed] [Google Scholar]
- 213.Thompson A.J., Lummis S.C. The 5-HT3 receptor as a therapeutic target. Expert Opin. Ther. Targets. 2007;11(4):527–540. doi: 10.1517/14728222.11.4.527. [http://dx.doi.org/10.1517/14728222.11.4.527]. [PMID: 17373882]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 214.Andrade C. Nonsteroidal anti-inflammatory drugs and 5-HT3 serotonin receptor antagonists as innovative antipsychotic augmentation treatments for schizophrenia. J. Clin. Psychiatry. 2014;75(7):e707–e709. doi: 10.4088/JCP.14f09292. [http://dx.doi.org/10.4088/JCP.14f09292]. [PMID: 25093487]. [DOI] [PubMed] [Google Scholar]
- 215.Toren P., Weizman A., Ratner S., Cohen D., Laor N. Ondansetron treatment in Tourette’s disorder: a 3-week, randomized, double-blind, placebo-controlled study. J. Clin. Psychiatry. 2005;66(4):499–503. doi: 10.4088/jcp.v66n0413. [http://dx.doi.org/10.4088/JCP.v66n0413]. [PMID: 15816793]. [DOI] [PubMed] [Google Scholar]
- 216.Sirota P., Mosheva T., Shabtay H., Giladi N., Korczyn A.D. Use of the selective serotonin 3 receptor antagonist ondansetron in the treatment of neuroleptic-induced tardive dyskinesia. Am. J. Psychiatry. 2000;157(2):287–289. doi: 10.1176/appi.ajp.157.2.287. [http://dx.doi.org/10.1176/appi. ajp.157.2.287]. [PMID: 10671405]. [DOI] [PubMed] [Google Scholar]
- 217.Johnson B.A., Ait-Daoud N., Seneviratne C., Roache J.D., Javors M.A., Wang X.Q., Liu L., Penberthy J.K., DiClemente C.C., Li M.D. Pharmacogenetic approach at the serotonin transporter gene as a method of reducing the severity of alcohol drinking. Am. J. Psychiatry. 2011;168(3):265–275. doi: 10.1176/appi.ajp.2010.10050755. [http://dx.doi.org/ 10.1176/appi.ajp.2010.10050755]. [PMID: 21247998]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 218.Serata D., Kotzalidis G.D., Rapinesi C., Janiri D., Di Pietro S., Callovini G., Piacentino D., Gasperoni C., Brugnoli R., Ferri V.R., Girardi N., Tatarelli R., Ferracuti S., Angeletti G., Girardi P., Del Casale A. Are 5-HT3 antagonists effective in obsessive-compulsive disorder? A systematic review of literature. Hum. Psychopharmacol. 2015;30(2):70–84. doi: 10.1002/hup.2461. [http://dx.doi.org/10.1002/ hup.2461]. [PMID: 25676060]. [DOI] [PubMed] [Google Scholar]
- 219.Hewlett W.A., Schmid S.P., Salomon R.M. Pilot trial of ondansetron in the treatment of 8 patients with obsessive-compulsive disorder. J. Clin. Psychiatry. 2003;64(9):1025–1030. doi: 10.4088/jcp.v64n0907. [http://dx.doi.org/ 10.4088/JCP.v64n0907]. [PMID: 14628977]. [DOI] [PubMed] [Google Scholar]
- 220.Pallanti S., Bernardi S., Antonini S., Singh N., Hollander E. Ondansetron augmentation in treatment-resistant obsessive-compulsive disorder: a preliminary, single-blind, prospective study. CNS Drugs. 2009;23(12):1047–1055. doi: 10.2165/11530240-000000000-00000. [http://dx.doi.org/10.2165/ 11530240-000000000-00000]. [PMID: 19958042]. [DOI] [PubMed] [Google Scholar]
- 221.Pallanti S., Bernardi S., Antonini S., Singh N., Hollander E. Ondansetron augmentation in patients with obsessive-compulsive disorder who are inadequate responders to serotonin reuptake inhibitors: improvement with treatment and worsening following discontinuation. Eur. Neuropsychopharmacol. 2014;24(3):375–380. doi: 10.1016/j.euroneuro.2013.12.003. [http://dx.doi.org/10.1016/j.euroneuro.2013.12.003]. [PMID: 24406025]. [DOI] [PubMed] [Google Scholar]
- 222.Soltani F., Sayyah M., Feizy F., Malayeri A., Siahpoosh A., Motlagh I. A double-blind, placebo-controlled pilot study of ondansetron for patients with obsessive-compulsive disorder. Hum. Psychopharmacol. 2010;25(6):509–513. doi: 10.1002/hup.1145. [http://dx.doi.org/10. 1002/hup.1145]. [PMID: 20737524]. [DOI] [PubMed] [Google Scholar]
- 223.Heidari M., Zarei M., Hosseini S.M., Taghvaei R., Maleki H., Tabrizi M., Fallah J., Akhondzadeh S. Ondansetron or placebo in the augmentation of fluvoxamine response over 8 weeks in obsessive-compulsive disorder. Int. Clin. Psychopharmacol. 2014;29(6):344–350. doi: 10.1097/YIC.0000000000000043. [http://dx.doi.org/10.1097/YIC.0000000000000043]. [PMID: 24850229]. [DOI] [PubMed] [Google Scholar]
- 224.Andrade C. Ondansetron augmentation of serotonin reuptake inhibitors as a treatment strategy in obsessive-compulsive disorder. J. Clin. Psychiatry. 2015;76(1):e72–e75. doi: 10.4088/JCP.14f09704. [http://dx.doi.org/ 10.4088/JCP.14f09704]. [PMID: 25650682]. [DOI] [PubMed] [Google Scholar]
- 225.Shapira N.A., Keck P.E., Jr, Goldsmith T.D., McConville B.J., Eis M., McElroy S.L. Open-label pilot study of tramadol hydrochloride in treatment-refractory obsessive-compulsive disorder. Depress. Anxiety. 1997;6(4):170–173. [http://dx.doi.org/10.1002/ (SICI)1520-6394(1997)6:4<170:AID-DA7>3.0.CO;2-G]. [PMID: 9559288]. [PubMed] [Google Scholar]
- 226.Warneke L. A possible new treatment approach to obsessive-compulsive disorder. Can. J. Psychiatry. 1997;42(6):667–668. doi: 10.1177/070674379704200624. [http://dx.doi.org/10.1177/070674379704200624]. [PMID: 9288436]. [DOI] [PubMed] [Google Scholar]
- 227.Goldsmith T.B., Shapira N.A., Keck P.E. Jr Rapid remission of OCD with tramadol hydrochloride. Am. J. Psychiatry. 1999;156(4):660–661. doi: 10.1176/ajp.156.4.660a. [PMID: 10200754]. [DOI] [PubMed] [Google Scholar]
- 228.Koran L.M., Aboujaoude E., Bullock K.D., Franz B., Gamel N., Elliott M. Double-blind treatment with oral morphine in treatment-resistant obsessive-compulsive disorder. J. Clin. Psychiatry. 2005;66(3):353–359. doi: 10.4088/jcp.v66n0312. [http://dx.doi.org/10.4088/JCP.v66n0312]. [PMID: 15766302]. [DOI] [PubMed] [Google Scholar]
- 229.Liddell M.B., Aziz V., Briggs P., Kanakkehewa N., Rawi O. Buprenorphine augmentation in the treatment of refractory obsessive-compulsive disorder. Ther. Adv. Psychopharmacol. 2013;3(1):15–19. doi: 10.1177/2045125312462233. [http://dx.doi.org/10.1177/2045125312462233]. [PMID: 23983988]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 230.Urraca N., Camarena B., Gómez-Caudillo L., Esmer M.C., Nicolini H. Mu opioid receptor gene as a candidate for the study of obsessive compulsive disorder with and without tics. Am. J. Med. Genet. B. Neuropsychiatr. Genet. 2004;127B(1):94–96. doi: 10.1002/ajmg.b.20170. [http://dx. doi.org/10.1002/ajmg.b.20170]. [PMID: 15108189]. [DOI] [PubMed] [Google Scholar]
- 231.Rojas-Corrales M.O., Gibert-Rahola J., Mico J.A. Role of atypical opiates in OCD. Experimental approach through the study of 5-HT(2A/C) receptor-mediated behavior. Psychopharmacology (Berl.) 2007;190(2):221–231. doi: 10.1007/s00213-006-0619-5. [http://dx.doi.org/10.1007/s00213-006-0619-5]. [PMID: 17102981]. [DOI] [PubMed] [Google Scholar]
- 232.Insel T.R., Pickar D. Naloxone administration in obsessive-compulsive disorder: report of two cases. Am. J. Psychiatry. 1983;140(9):1219–1220. doi: 10.1176/ajp.140.9.1219. [http://dx.doi.org/10.1176/ajp.140.9.1219]. [PMID: 6614234]. [DOI] [PubMed] [Google Scholar]
- 233.Keuler D.J., Altemus M., Michelson D., Greenberg B., Murphy D.L. Behavioral effects of naloxone infusion in obsessive-compulsive disorder. Biol. Psychiatry. 1996;40(2):154–156. doi: 10.1016/0006-3223(95)00632-X. [http:// dx.doi.org/10.1016/0006-3223(95)00632-X]. [PMID: 8793049]. [DOI] [PubMed] [Google Scholar]
- 234.Goff D.C., Tsai G., Levitt J., Amico E., Manoach D., Schoenfeld D.A., Hayden D.L., McCarley R., Coyle J.T. A placebo-controlled trial of D-cycloserine added to conventional neuroleptics in patients with schizophrenia. Arch. Gen. Psychiatry. 1999;56(1):21–27. doi: 10.1001/archpsyc.56.1.21. [http://dx.doi.org/10.1001/archpsyc.56.1.21]. [PMID: 9892252]. [DOI] [PubMed] [Google Scholar]
- 235.Tsai G.E., Falk W.E., Gunther J., Coyle J.T. Improved cognition in Alzheimer’s disease with short-term D-cycloserine treatment. Am. J. Psychiatry. 1999;156(3):467–469. doi: 10.1176/ajp.156.3.467. [PMID: 10080566]. [DOI] [PubMed] [Google Scholar]
- 236.Otto M.W., Basden S.L., Leyro T.M., McHugh R.K., Hofmann S.G. Clinical perspectives on the combination of D-cycloserine and cognitive-behavioral therapy for the treatment of anxiety disorders. CNS Spectr. 2007;12(1):51–56, 59-61. doi: 10.1017/s1092852900020526. [http://dx.doi.org/10.1017/ S1092852900020526]. [PMID: 17192764]. [DOI] [PubMed] [Google Scholar]
- 237.Walker D.L., Ressler K.J., Lu K.T., Davis M. Facilitation of conditioned fear extinction by systemic administration or intra-amygdala infusions of D-cycloserine as assessed with fear-potentiated startle in rats. J. Neurosci. 2002;22(6):2343–2351. doi: 10.1523/JNEUROSCI.22-06-02343.2002. [http://dx.doi.org/10.1523/JNEUROSCI.22-06-02343.2002]. [PMID: 11896173]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 238.Norberg M.M., Krystal J.H., Tolin D.F. A meta-analysis of D-cycloserine and the facilitation of fear extinction and exposure therapy. Biol. Psychiatry. 2008;63(12):1118–1126. doi: 10.1016/j.biopsych.2008.01.012. [http://dx.doi. org/10.1016/j.biopsych.2008.01.012]. [PMID: 18313643]. [DOI] [PubMed] [Google Scholar]
- 239.Rodrigues H., Figueira I., Lopes A., Gonçalves R., Mendlowicz M.V., Coutinho E.S., Ventura P. Does D-cycloserine enhance exposure therapy for anxiety disorders in humans? A meta-analysis. PLoS One. 2014;9(7):e93519. doi: 10.1371/journal.pone.0093519. [http://dx.doi.org/10.1371/journal. pone.0093519]. [PMID: 24991926]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 240.Andersson E., Hedman E., Enander J., Radu D.D., Ljótsson B., Cervenka S., Isung J., Svanborg C., Mataix-Cols D., Kaldo V., Andersson G., Lindefors N., Rück C. D-cycloserine vs. placebo as adjunct to cognitive behavioral therapy for obsessive-compulsive disorder and interaction with antidepressants: A randomized clinical trial. JAMA Psychiatry. 2015;72(7):659–667. doi: 10.1001/jamapsychiatry.2015.0546. [http://dx.doi.org/10.1001/jamapsychiatry.2015.0546]. [PMID: 25970252]. [DOI] [PubMed] [Google Scholar]
- 241.Werner-Seidler A., Richardson R. Effects of D-cycloserine on extinction: consequences of prior exposure to imipramine. Biol. Psychiatry. 2007;62(10):1195–1197. doi: 10.1016/j.biopsych.2007.04.010. [DOI:10.1016/j.biopsych. 2007.04.010]. [PMID: 17555721]. [DOI] [PubMed] [Google Scholar]
- 242.Mataix-Cols D., Fernández de la Cruz L., Monzani B., Rosenfield D., Andersson E., Pérez-Vigil A., Frumento P., de Kleine R.A., Difede J., Dunlop B.W., Farrell L.J., Geller D., Gerardi M., Guastella A.J., Hofmann S.G., Hendriks G.J., Kushner M.G., Lee F.S., Lenze E.J., Levinson C.A., McConnell H., Otto M.W., Plag J., Pollack M.H., Ressler K.J., Rodebaugh T.L., Rothbaum B.O., Scheeringa M.S., Siewert-Siegmund A., Smits J.A.J., Storch E.A., Ströhle A., Tart C.D., Tolin D.F., van Minnen A., Waters A.M., Weems C.F., Wilhelm S., Wyka K., Davis M., Rück C., Altemus M., Anderson P., Cukor J., Finck C., Geffken G.R., Golfels F., Goodman W.K., Gutner C., Heyman I., Jovanovic T., Lewin A.B., McNamara J.P., Murphy T.K., Norrholm S., Thuras P. D-Cycloserine Augmentation of Exposure-Based Cognitive Behavior Therapy for Anxiety, Obsessive-Compulsive, and Posttraumatic Stress Disorders: A Systematic Review and Meta-analysis of Individual Participant Data. JAMA Psychiatry. 2017;74(5):501–510. doi: 10.1001/jamapsychiatry.2016.3955. [http://dx.doi.org/10.1001/ jamapsychiatry.2016.3955]. [PMID: 28122091]. [DOI] [PubMed] [Google Scholar]
- 243.Kushner M.G., Kim S.W., Donahue C., Thuras P., Adson D., Kotlyar M., McCabe J., Peterson J., Foa E.B. D-cycloserine augmented exposure therapy for obsessive-compulsive disorder. Biol. Psychiatry. 2007;62(8):835–838. doi: 10.1016/j.biopsych.2006.12.020. [http://dx.doi.org/10.1016/j. biopsych.2006.12.020]. [PMID: 17588545]. [DOI] [PubMed] [Google Scholar]
- 244.Storch E.A., Merlo L.J., Bengtson M., Murphy T.K., Lewis M.H., Yang M.C., Jacob M.L., Larson M., Hirsh A., Fernandez M., Geffken G.R., Goodman W.K. D-cycloserine does not enhance exposure-response prevention therapy in obsessive-compulsive disorder. Int. Clin. Psychopharmacol. 2007;22(4):230–237. doi: 10.1097/YIC.0b013e32819f8480. [http:// dx.doi.org/10.1097/YIC.0b013e32819f8480]. [PMID: 17519647]. [DOI] [PubMed] [Google Scholar]
- 245.Wilhelm S., Buhlmann U., Tolin D.F., Meunier S.A., Pearlson G.D., Reese H.E., Cannistraro P., Jenike M.A., Rauch S.L. Augmentation of behavior therapy with D-cycloserine for obsessive-compulsive disorder. Am. J. Psychiatry. 2008;165(3):335–341. doi: 10.1176/appi.ajp.2007.07050776. [http://dx.doi.org/10.1176/appi.ajp.2007.07050776]. [PMID: 18245177]. [DOI] [PubMed] [Google Scholar]
- 246.Storch E.A., Murphy T.K., Goodman W.K., Geffken G.R., Lewin A.B., Henin A., Micco J.A., Sprich S., Wilhelm S., Bengtson M., Geller D.A. A preliminary study of D-cycloserine augmentation of cognitive-behavioral therapy in pediatric obsessive-compulsive disorder. Biol. Psychiatry. 2010;68(11):1073–1076. doi: 10.1016/j.biopsych.2010.07.015. [http://dx.doi.org/10.1016/j.biopsych.2010.07.015]. [PMID: 20817153]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 247.Mataix-Cols D., Turner C., Monzani B., Isomura K., Murphy C., Krebs G., Heyman I. Cognitive-behavioural therapy with post-session D-cycloserine augmentation for paediatric obsessive-compulsive disorder: pilot randomised controlled trial. Br. J. Psychiatry. 2014;204(1):77–78. doi: 10.1192/bjp.bp.113.126284. [http://dx.doi.org/10.1192/bjp.bp.113. 126284]. [PMID: 24262813]. [DOI] [PubMed] [Google Scholar]
- 248.Chasson G.S., Buhlmann U., Tolin D.F., Rao S.R., Reese H.E., Rowley T., Welsh K.S., Wilhelm S. Need for speed: evaluating slopes of OCD recovery in behavior therapy enhanced with d-cycloserine. Behav. Res. Ther. 2010;48(7):675–679. doi: 10.1016/j.brat.2010.03.007. [http://dx. doi.org/10.1016/j.brat.2010.03.007]. [PMID: 20362975]. [DOI] [PubMed] [Google Scholar]
- 249.Ganasen K.A., Ipser J.C., Stein D.J. Augmentation of cognitive behavioral therapy with pharmacotherapy. Psychiatr. Clin. North Am. 2010;33(3):687–699. doi: 10.1016/j.psc.2010.04.008. [http://dx.doi.org/10.1016/j.psc.2010. 04.008]. [PMID: 20599140]. [DOI] [PubMed] [Google Scholar]
- 250.Bontempo A., Panza K.E., Bloch M.H. D-cycloserine augmentation of behavioral therapy for the treatment of anxiety disorders: a meta-analysis. J. Clin. Psychiatry. 2012;73(4):533–537. doi: 10.4088/JCP.11r07356. [http://dx.doi.org/10.4088/JCP.11r07356]. [PMID: 22579153]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 251.Hofmann S.G., Pollack M.H., Otto M.W. Augmentation treatment of psychotherapy for anxiety disorders with D-cycloserine. CNS Drug Rev. 2006;12(3-4):208–217. doi: 10.1111/j.1527-3458.2006.00208.x. [http://dx.doi.org/10. 1111/j.1527-3458.2006.00208.x]. [PMID: 17227287]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 252.de Kleine R.A., Hendriks G.J., Kusters W.J., Broekman T.G., van Minnen A. A randomized placebo-controlled trial of D-cycloserine to enhance exposure therapy for posttraumatic stress disorder. Biol. Psychiatry. 2012;71(11):962–968. doi: 10.1016/j.biopsych.2012.02.033. [http://dx. doi.org/10.1016/j.biopsych.2012.02.033]. [PMID: 22480663]. [DOI] [PubMed] [Google Scholar]
- 253.D’Souza D.C., Gil R., Cassello K., Morrissey K., Abi-Saab D., White J., Sturwold R., Bennett A., Karper L.P., Zuzarte E., Charney D.S., Krystal J.H. IV glycine and oral D-cycloserine effects on plasma and CSF amino acids in healthy humans. Biol. Psychiatry. 2000;47(5):450–462. doi: 10.1016/s0006-3223(99)00133-x. [http://dx.doi.org/10.1016/S0006-3223(99)00133-X]. [PMID: 10704956]. [DOI] [PubMed] [Google Scholar]
- 254.Quartermain D., Mower J., Rafferty M.F., Herting R.L., Lanthorn T.H. Acute but not chronic activation of the NMDA-coupled glycine receptor with D-cycloserine facilitates learning and retention. Eur. J. Pharmacol. 1994;257(1-2):7–12. doi: 10.1016/0014-2999(94)90687-4. [http://dx.doi. org/10.1016/0014-2999(94)90687-4]. [PMID: 8082709]. [DOI] [PubMed] [Google Scholar]
- 255.Boje K.M., Wong G., Skolnick P. Desensitization of the NMDA receptor complex by glycinergic ligands in cerebellar granule cell cultures. Brain Res. 1993;603(2):207–214. doi: 10.1016/0006-8993(93)91239-o. [http://dx.doi.org/10. 1016/0006-8993(93)91239-O]. [PMID: 8096423]. [DOI] [PubMed] [Google Scholar]
- 256.de Leeuw A.S., van Megen H.J., Kahn R.S., Westenberg H.G. d-cycloserine addition to exposure sessions in the treatment of patients with obsessive-compulsive disorder. Eur. Psychiatry. 2017;40:38–44. doi: 10.1016/j.eurpsy.2016.06.011. [http://dx.doi.org/10.1016/j.eurpsy.2016.06.011]. [PMID: 27837671]. [DOI] [PubMed] [Google Scholar]
- 257.Marsicano G., Wotjak C.T., Azad S.C., Bisogno T., Rammes G., Cascio M.G., Hermann H., Tang J., Hofmann C., Zieglgänsberger W., Di Marzo V., Lutz B. The endogenous cannabinoid system controls extinction of aversive memories. Nature. 2002;418(6897):530–534. doi: 10.1038/nature00839. [http://dx.doi.org/10.1038/nature00839]. [PMID: 12152079]. [DOI] [PubMed] [Google Scholar]
- 258.Evanson N.K., Tasker J.G., Hill M.N., Hillard C.J., Herman J.P. Fast feedback inhibition of the HPA axis by glucocorticoids is mediated by endocannabinoid signaling. Endocrinology. 2010;151(10):4811–4819. doi: 10.1210/en.2010-0285. [http://dx.doi.org/10.1210/en.2010-0285]. [PMID: 20702575]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 259.Abush H., Akirav I. Cannabinoids ameliorate impairments induced by chronic stress to synaptic plasticity and short-term memory. Neuropsychopharmacology. 2013;38(8):1521–1534. doi: 10.1038/npp.2013.51. [http:// dx.doi.org/10.1038/npp.2013.51]. [PMID: 23426383]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 260.Micale V., Di Marzo V., Sulcova A., Wotjak C.T., Drago F. Endocannabinoid system and mood disorders: priming a target for new therapies. Pharmacol. Ther. 2013;138(1):18–37. doi: 10.1016/j.pharmthera.2012.12.002. [http://dx. doi.org/10.1016/j.pharmthera.2012.12.002]. [PMID: 23261685]. [DOI] [PubMed] [Google Scholar]
- 261.Schier A.R., Ribeiro N.P., Silva A.C., Hallak J.E., Crippa J.A., Nardi A.E., Zuardi A.W. Cannabidiol, a Cannabis sativa constituent, as an anxiolytic drug. Rev. Bras. Psiquiatr. 2012;34(Suppl. 1):S104–S110. doi: 10.1590/s1516-44462012000500008. [http://dx.doi.org/10.1016/S1516-4446(12)70057-0]. [PMID: 22729452]. [DOI] [PubMed] [Google Scholar]
- 262.Papini S., Sullivan G.M., Hien D.A., Shvil E., Neria Y. Toward a translational approach to targeting the endocannabinoid system in posttraumatic stress disorder: a critical review of preclinical research. Biol. Psychol. 2015;104:8–18. doi: 10.1016/j.biopsycho.2014.10.010. [http://dx.doi.org/10.1016/j. biopsycho.2014.10.010]. [PMID: 25448242]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 263.Blessing E.M., Steenkamp M.M., Manzanares J., Marmar C.R. Cannabidiol as a potential treatment for anxiety disorders. Neurotherapeutics. 2015;12(4):825–836. doi: 10.1007/s13311-015-0387-1. [http://dx.doi.org/10.1007/ s13311-015-0387-1]. [PMID: 26341731]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 264.Martinotti G., Di Iorio G., Sepede G., De Berardis D., De Risio L., Di Giannantonio M. Cannabis use and psychosis: theme introduction. Curr. Pharm. Des. 2012;18(32):4991–4998. doi: 10.2174/138161212802884627. [http://dx. doi.org/10.2174/138161212802884627]. [PMID: 22716149]. [DOI] [PubMed] [Google Scholar]
- 265.Rutrick D., Stein D.J., Subramanian G., Smith B., Fava M., Hasler G., Cha J.H., Gasparini F., Donchev T., Ocwieja M., Johns D., Gomez-Mancilla B. Mavoglurant augmentation in OCD patients resistant to selective serotonin reuptake inhibitors: a proof-of-concept, randomized, placebo-controlled, phase 2 study. Adv. Ther. 2017;34(2):524–541. doi: 10.1007/s12325-016-0468-5. [http://dx.doi.org/10.1007/s12325-016-0468-5]. [PMID: 28044255]. [DOI] [PubMed] [Google Scholar]
- 266.Fux M., Benjamin J., Nemets B. A placebo-controlled cross-over trial of adjunctive EPA in OCD. J. Psychiatr. Res. 2004;38(3):323–325. doi: 10.1016/S0022-3956(03)00077-3. [http://dx.doi.org/10.1016/S0022-3956(03)00077-3]. [PMID: 15003438]. [DOI] [PubMed] [Google Scholar]
- 267.Sayyah M., Boostani H., Pakseresht S., Malayeri A. A preliminary randomized double-blind clinical trial on the efficacy of celecoxib as an adjunct in the treatment of obsessive-compulsive disorder. Psychiatry Res. 2011;189(3):403–406. doi: 10.1016/j.psychres.2011.01.019. [http://dx.doi.org/ 10.1016/j.psychres.2011.01.019]. [PMID: 21329988]. [DOI] [PubMed] [Google Scholar]
- 268.Arabzadeh S., Shahhossenie M., Mesgarpour B., Rezaei F., Shalbafan M.R., Ghiasi Z., Akhondzadeh S. L-carnosine as an adjuvant to fluvoxamine in treatment of obsessive compulsive disorder: A randomized double-blind study. Hum. Psychopharmacol. 2017;32(4) doi: 10.1002/hup.2584. [http://dx.doi.org/10.1002/hup.2584]. [PMID: 28485008]. [DOI] [PubMed] [Google Scholar]
- 269.Fux M., Levine J., Aviv A., Belmaker R.H. Inositol treatment of obsessive-compulsive disorder. Am. J. Psychiatry. 1996;153(9):1219–1221. doi: 10.1176/ajp.153.9.1219. [http://dx.doi.org/10.1176/ajp.153.9.1219]. [PMID: 8780431]. [DOI] [PubMed] [Google Scholar]
- 270.Askari N., Moin M., Sanati M., Tajdini M., Hosseini S.M., Modabbernia A., Najand B., Salimi S., Tabrizi M., Ashrafi M., Hajiaghaee R., Akhondzadeh S. Granisetron adjunct to fluvoxamine for moderate to severe obsessive-compulsive disorder: a randomized, double-blind, placebo-controlled trial. CNS Drugs. 2012;26(10):883–892. doi: 10.2165/11635850-000000000-00000. [http://dx.doi.org/10.2165/11635850-000000000-00000]. [PMID: 22873680]. [DOI] [PubMed] [Google Scholar]
- 271.Dannon P.N., Sasson Y., Hirschmann S., Iancu I., Grunhaus L.J., Zohar J. Pindolol augmentation in treatment-resistant obsessive compulsive disorder: a double-blind placebo controlled trial. Eur. Neuropsychopharmacol. 2000;10(3):165–169. doi: 10.1016/s0924-977x(00)00065-1. [http://dx.doi. org/10.1016/S0924-977X(00)00065-1]. [PMID: 10793318]. [DOI] [PubMed] [Google Scholar]
- 272.Ghaleiha A., Entezari N., Modabbernia A., Najand B., Askari N., Tabrizi M., Ashrafi M., Hajiaghaee R., Akhondzadeh S. Memantine add-on in moderate to severe obsessive-compulsive disorder: randomized double-blind placebo-controlled study. J. Psychiatr. Res. 2013;47(2):175–180. doi: 10.1016/j.jpsychires.2012.09.015. [http://dx.doi.org/10.1016/j. jpsychires.2012.09.015]. [PMID: 23063327]. [DOI] [PubMed] [Google Scholar]
- 273.Haghighi M., Jahangard L., Mohammad-Beigi H., Bajoghli H., Hafezian H., Rahimi A., Afshar H., Holsboer-Trachsler E., Brand S. In a double-blind, randomized and placebo-controlled trial, adjuvant memantine improved symptoms in inpatients suffering from refractory obsessive-compulsive disorders (OCD). Psychopharmacology (Berl.) 2013;228(4):633–640. doi: 10.1007/s00213-013-3067-z. [http://dx.doi. org/10.1007/s00213-013-3067-z]. [PMID: 23525525]. [DOI] [PubMed] [Google Scholar]
- 274.Modarresi A., Sayyah M., Razooghi S., Eslami K., Javadi M., Kouti L. Memantine augmentation improves symptoms in serotonin reuptake inhibitor-refractory obsessive-compulsive disorder: a randomized controlled trial. Pharmacopsychiatry. 2017 doi: 10.1055/s-0043-120268. Epub ahead of print [http://dx.doi.org/10.1055/s-0043-120268]. [PMID: 29100251]. [DOI] [PubMed] [Google Scholar]
- 275.Sarris J., Oliver G., Camfield D.A., Dean O.M., Dowling N., Smith D.J., Murphy J., Menon R., Berk M., Blair-West S., Ng C.H. Menon.; R.; Berk, M.; Blair-West, S.; Ng, C.H. N-acetyl cysteine (NAC) in the treatment of obsessive-compulsive disorder: a 16-week, double-blind, randomised, placebo-controlled study. CNS Drugs. 2015;29(9):801–809. doi: 10.1007/s40263-015-0272-9. [http://dx.doi.org/10.1007/s40263-015-0272-9]. [PMID: 26374743]. [DOI] [PubMed] [Google Scholar]
- 276.Afshar H., Roohafza H., Mohammad-Beigi H., Haghighi M., Jahangard L., Shokouh P., Sadeghi M., Hafezian H. N-acetylcysteine add-on treatment in refractory obsessive-compulsive disorder: a randomized, double-blind, placebo-controlled trial. J. Clin. Psychopharmacol. 2012;32(6):797–803. doi: 10.1097/JCP.0b013e318272677d. [http://dx.doi.org/ 10.1097/JCP.0b013e318272677d]. [PMID: 23131885]. [DOI] [PubMed] [Google Scholar]
- 277.Paydary K., Akamaloo A., Ahmadipour A., Pishgar F., Emamzadehfard S., Akhondzadeh S. N-acetylcysteine augmentation therapy for moderate-to-severe obsessive-compulsive disorder: randomized, double-blind, placebo-controlled trial. J. Clin. Pharm. Ther. 2016;41(2):214–219. doi: 10.1111/jcpt.12370. [http://dx.doi.org/10.1111/jcpt.12370]. [PMID: 26931055]. [DOI] [PubMed] [Google Scholar]
- 278.Costa D.L.C., Diniz J.B., Requena G., Joaquim M.A., Pittenger C., Bloch M.H., Miguel E.C., Shavitt R.G. Randomized, double-blind, placebo-controlled trial of N-acetylcysteine augmentation for treatment-resistant obsessive-compulsive disorder. J. Clin. Psychiatry. 2017;78(7):e766–e773. doi: 10.4088/JCP.16m11101. [http://dx.doi.org/10.4088/JCP. 16m11101]. [PMID: 28617566]. [DOI] [PubMed] [Google Scholar]
- 279.Grady T.A., Pigott T.A., L’Heureux F., Hill J.L., Bernstein S.E., Murphy D.L. Double-blind study of adjuvant buspirone for fluoxetine-treated patients with obsessive-compulsive disorder. Am. J. Psychiatry. 1993;150(5):819–821. doi: 10.1176/ajp.150.5.819. [http://dx.doi.org/10.1176/ ajp.150.5.819]. [PMID: 8480832]. [DOI] [PubMed] [Google Scholar]
- 280.McDougle C.J., Goodman W.K., Leckman J.F., Holzer J.C., Barr L.C., McCance-Katz E., Heninger G.R., Price L.H. Limited therapeutic effect of addition of buspirone in fluvoxamine-refractory obsessive-compulsive disorder. Am. J. Psychiatry. 1993;150(4):647–649. doi: 10.1176/ajp.150.4.647. [http://dx.doi.org/10.1176/ajp.150.4.647]. [PMID: 8465885]. [DOI] [PubMed] [Google Scholar]
- 281.Hollander E., Kaplan A., Stahl S.M. A double-blind, placebo-controlled trial of clonazepam in obsessive-compulsive disorder. World J. Biol. Psychiatry. 2003;4(1):30–34. doi: 10.3109/15622970309167908. [http://dx.doi.org/10. 3109/15622970309167908]. [PMID: 12582975]. [DOI] [PubMed] [Google Scholar]
- 282.Greenberg W.M., Benedict M.M., Doerfer J., Perrin M., Panek L., Cleveland W.L., Javitt D.C. Adjunctive glycine in the treatment of obsessive-compulsive disorder in adults. J. Psychiatr. Res. 2009;43(6):664–670. doi: 10.1016/j.jpsychires.2008.10.007. [http://dx.doi.org/10.1016/j.jpsychires. 2008.10.007]. [PMID: 19046587]. [DOI] [PubMed] [Google Scholar]
- 283.McDougle C.J., Price L.H., Goodman W.K., Charney D.S., Heninger G.R. A controlled trial of lithium augmentation in fluvoxamine-refractory obsessive-compulsive disorder: lack of efficacy. J. Clin. Psychopharmacol. 1991;11(3):175–184. [http://dx. doi.org/10.1097/00004714-199106000-00005]. [PMID: 1820757]. [PubMed] [Google Scholar]
- 284.Amiaz R., Fostick L., Gershon A., Zohar J. Naltrexone augmentation in OCD: a double-blind placebo-controlled cross-over study. Eur. Neuropsychopharmacol. 2008;18(6):455–461. doi: 10.1016/j.euroneuro.2008.01.006. [http://dx. doi.org/10.1016/j.euroneuro.2008.01.006]. [PMID: 18353618]. [DOI] [PubMed] [Google Scholar]
- 285.Pittenger C., Bloch M.H., Wasylink S., Billingslea E., Simpson R., Jakubovski E., Kelmendi B., Sanacora G., Coric V. Riluzole augmentation in treatment-refractory obsessive-compulsive disorder: a pilot randomized placebo-controlled trial. J. Clin. Psychiatry. 2015;76(8):1075–1084. doi: 10.4088/JCP.14m09123. [http://dx.doi.org/10.4088/JCP.14m09123]. [PMID: 26214725]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 286.Besiroglu L., Agargun M.Y., Ozbebit O., Aydin A. A discrimination based on autogenous versus reactive obsessions in obsessive-compulsive disorder and related clinical manifestations. CNS Spectr. 2006;11(3):179–186. doi: 10.1017/s1092852900014292. [http://dx.doi.org/10.1017/ S1092852900014292]. [PMID: 16575374]. [DOI] [PubMed] [Google Scholar]
- 287.Lee H.J., Kwon S.M. Two different types of obsession: autogenous obsessions and reactive obsessions. Behav. Res. Ther. 2003;41(1):11–29. doi: 10.1016/s0005-7967(01)00101-2. [http://dx.doi.org/10.1016/S0005-7967(01)00101-2]. [PMID: 12488117]. [DOI] [PubMed] [Google Scholar]
- 288.Lee H.J., Telch M.J. Autogenous/reactive obsessions and their relationship with OCD symptoms and schizotypal personality features. J. Anxiety Disord. 2005;19(7):793–805. doi: 10.1016/j.janxdis.2004.10.001. [http://dx.doi.org/ 10.1016/j.janxdis.2004.10.001]. [PMID: 16076425]. [DOI] [PubMed] [Google Scholar]
- 289.Besiroglu L., Sozen M., Ozbebit O., Avcu S., Selvi Y., Bora A., Atli A., Unal O., Bulut M.D. The involvement of distinct neural systems in patients with obsessive-compulsive disorder with autogenous and reactive obsessions. Acta Psychiatr. Scand. 2011;124(2):141–151. doi: 10.1111/j.1600-0447.2011.01726.x. [http://dx.doi.org/10.1111/j.1600-0447.2011. 01726.x]. [PMID: 21627621]. [DOI] [PubMed] [Google Scholar]
- 290.Subirà M., Alonso P., Segalàs C., Real E., López-Solà C., Pujol J., Martínez-Zalacaín I., Harrison B.J., Menchón J.M., Cardoner N., Soriano-Mas C. Brain structural alterations in obsessive-compulsive disorder patients with autogenous and reactive obsessions. PLoS One. 2013;8(9):e75273. doi: 10.1371/journal.pone.0075273. [http://dx.doi.org/10.1371/ journal.pone.0075273]. [PMID: 24098688]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 291.Rufer M., Fricke S., Moritz S., Kloss M., Hand I. Symptom dimensions in obsessive-compulsive disorder: prediction of cognitive-behavior therapy outcome. Acta Psychiatr. Scand. 2006;113(5):440–446. doi: 10.1111/j.1600-0447.2005.00682.x. [http://dx.doi.org/10.1111/j.1600-0447.2005.0 0682.x]. [PMID: 16603035]. [DOI] [PubMed] [Google Scholar]
- 292.Shetti C.N., Reddy Y.C., Kandavel T., Kashyap K., Singisetti S., Hiremath A.S., Siddequehusen M.U., Raghunandanan S. Clinical predictors of drug nonresponse in obsessive-compulsive disorder. J. Clin. Psychiatry. 2005;66(12):1517–1523. doi: 10.4088/jcp.v66n1204. [http:// dx.doi.org/10.4088/JCP.v66n1204]. [PMID: 16401151]. [DOI] [PubMed] [Google Scholar]
- 293.Denys D., Burger H., van Megen H., de Geus F., Westenberg H. A score for predicting response to pharmacotherapy in obsessive-compulsive disorder. Int. Clin. Psychopharmacol. 2003;18(6):315–322. doi: 10.1097/00004850-200311000-00002. [http://dx.doi.org/10.1097/00004850-200311000-00002]. [PMID: 14571151]. [DOI] [PubMed] [Google Scholar]
- 294.Rosario-Campos M.C., Leckman J.F., Mercadante M.T., Shavitt R.G., Prado H.S., Sada P., Zamignani D., Miguel E.C. Adults with early-onset obsessive-compulsive disorder. Am. J. Psychiatry. 2001;158(11):1899–1903. doi: 10.1176/appi.ajp.158.11.1899. [http://dx.doi.org/10.1176/appi.ajp.158. 11.1899]. [PMID: 11691698]. [DOI] [PubMed] [Google Scholar]
- 295.Moritz S., Fricke S., Jacobsen D., Kloss M., Wein C., Rufer M., Katenkamp B., Farhumand R., Hand I. Positive schizotypal symptoms predict treatment outcome in obsessive-compulsive disorder. Behav. Res. Ther. 2004;42(2):217–227. doi: 10.1016/S0005-7967(03)00120-7. [http://dx.doi.org/ 10.1016/S0005-7967(03)00120-7]. [PMID: 14975782]. [DOI] [PubMed] [Google Scholar]
- 296.Overbeek T., Schruers K., Vermetten E., Griez E. Comorbidity of obsessive-compulsive disorder and depression: prevalence, symptom severity, and treatment effect. J. Clin. Psychiatry. 2002;63(12):1106–1112. doi: 10.4088/jcp.v63n1204. [http://dx.doi.org/10.4088/JCP.v63n1204]. [PMID: 12523869]. [DOI] [PubMed] [Google Scholar]
- 297.Brakoulias V., Starcevic V., Belloch A., Dell’Osso L., Ferrão Y.A., Fontenelle L.F., Lochner C., Marazziti D., Martin A., Matsunaga H., Miguel E.C., Reddy Y.C., do Rosário M.C., Shavitt R.G., Sundar A.S., Stein D.J., Viswasam K. International prescribing practices in obsessive-compulsive disorder (OCD). Hum. Psychopharmacol. 2016;31(4):319–324. doi: 10.1002/hup.2541. [http://dx.doi.org/10. 1002/hup.2541]. [PMID: 27271200]. [DOI] [PubMed] [Google Scholar]
- 298.Stewart S.E., Jenike E.A., Hezel D.M., Stack D.E., Dodman N.H., Shuster L., Jenike M.A. A single-blinded case-control study of memantine in severe obsessive-compulsive disorder. J. Clin. Psychopharmacol. 2010;30(1):34–39. doi: 10.1097/JCP.0b013e3181c856de. [http://dx.doi.org/10.1097/ JCP.0b013e3181c856de]. [PMID: 20075645]. [DOI] [PubMed] [Google Scholar]
- 299.Rodriguez C.I., Kegeles L.S., Levinson A., Feng T., Marcus S.M., Vermes D., Flood P., Simpson H.B. Randomized controlled crossover trial of ketamine in obsessive-compulsive disorder: proof-of-concept. Neuropsychopharmacology. 2013;38(12):2475–2483. doi: 10.1038/npp.2013.150. [http://dx.doi.org/10.1038/npp.2013.150]. [PMID: 23783065]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 300.Hicks J.K., Swen J.J., Thorn C.F., Sangkuhl K., Kharasch E.D., Ellingrod V.L., Skaar T.C., Müller D.J., Gaedigk A., Stingl J.C. Clinical Pharmacogenetics Implementation Consortium guideline for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants. Clin. Pharmacol. Ther. 2013;93(5):402–408. doi: 10.1038/clpt.2013.2. [http:// dx.doi.org/10.1038/clpt.2013.2]. [PMID: 23486447]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 301.Müller D.J., Brandl E.J., Hwang R., Tiwari A.K., Sturgess J.E., Zai C.C., Lieberman J.A., Kennedy J.L., Richter M.A. The AmpliChip® CYP450 test and response to treatment in schizophrenia and obsessive compulsive disorder: a pilot study and focus on cases with abnormal CYP2D6 drug metabolism. Genet. Test. Mol. Biomarkers. 2012;16(8):897–903. doi: 10.1089/gtmb.2011.0327. [http://dx.doi.org/10.1089/gtmb. 2011.0327]. [PMID: 22775532]. [DOI] [PubMed] [Google Scholar]
- 302.Brandl E.J., Tiwari A.K., Zhou X., Deluce J., Kennedy J.L., Müller D.J., Richter M.A. Influence of CYP2D6 and CYP2C19 gene variants on antidepressant response in obsessive-compulsive disorder. Pharmacogenomics J. 2014;14(2):176–181. doi: 10.1038/tpj.2013.12. [http:// dx.doi.org/10.1038/tpj.2013.12]. [PMID: 23545896]. [DOI] [PubMed] [Google Scholar]
- 303.Zai G., Brandl E.J., Müller D.J., Richter M.A., Kennedy J.L. Pharmacogenetics of antidepressant treatment in obsessive-compulsive disorder: an update and implications for clinicians. Pharmacogenomics. 2014;15(8):1147–1157. doi: 10.2217/pgs.14.83. [http://dx.doi.org/ 10.2217/pgs.14.83]. [PMID: 25084207]. [DOI] [PubMed] [Google Scholar]
- 304.Ramamoorthy S., Bauman A.L., Moore K.R., Han H., Yang-Feng T., Chang A.S., Ganapathy V., Blakely R.D. Antidepressant- and cocaine-sensitive human serotonin transporter: molecular cloning, expression, and chromosomal localization. Proc. Natl. Acad. Sci. USA. 1993;90(6):2542–2546. doi: 10.1073/pnas.90.6.2542. [http://dx.doi.org/10. 1073/pnas.90.6.2542]. [PMID: 7681602]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 305.Heils A., Teufel A., Petri S., Stöber G., Riederer P., Bengel D., Lesch K.P. Allelic variation of human serotonin transporter gene expression. J. Neurochem. 1996;66(6):2621–2624. doi: 10.1046/j.1471-4159.1996.66062621.x. [http://dx. doi.org/10.1046/j.1471-4159.1996.66062621.x]. [PMID: 8632190]. [DOI] [PubMed] [Google Scholar]
- 306.Bloch M.H., Landeros-Weisenberger A., Sen S., Dombrowski P., Kelmendi B., Coric V., Pittenger C., Leckman J.F. Association of the serotonin transporter polymorphism and obsessive-compulsive disorder: systematic review. Am. J. Med. Genet. B. Neuropsychiatr. Genet. 2008;147B(6):850–858. doi: 10.1002/ajmg.b.30699. [http://dx.doi.org/ 10.1002/ajmg.b.30699]. [PMID: 18186076]. [DOI] [PubMed] [Google Scholar]
- 307.Zitterl W., Stompe T., Aigner M., Zitterl-Eglseer K., Ritter K., Zettinig G., Hornik K., Asenbaum S., Pirker W., Thau K. Diencephalic serotonin transporter availability predicts both transporter occupancy and treatment response to sertraline in obsessive-compulsive checkers. Biol. Psychiatry. 2009;66(12):1115–1122. doi: 10.1016/j.biopsych.2009.07.009. [http://dx.doi.org/10.1016/j.biopsych.2009.07.009]. [PMID: 19717141]. [DOI] [PubMed] [Google Scholar]
- 308.Corregiari F.M., Bernik M., Cordeiro Q., Vallada H. Endophenotypes and serotonergic polymorphisms associated with treatment response in obsessive-compulsive disorder. Clinics (São Paulo) 2012;67(4):335–340. doi: 10.6061/clinics/2012(04)06. [http://dx.doi.org/10.6061/clinics/2012(04)06]. [PMID: 22522758]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 309.Vulink N.C., Westenberg H.G., van Nieuwerburgh F., Deforce D., Fluitman S.B., Meinardi J.S., Denys D. Catechol-O-methyltranferase gene expression is associated with response to citalopram in obsessive-compulsive disorder. Int. J. Psychiatry Clin. Pract. 2012;16(4):277–283. doi: 10.3109/13651501.2011.653375. [http://dx.doi.org/10.3109/ 13651501.2011.653375]. [PMID: 22414277]. [DOI] [PubMed] [Google Scholar]
- 310.Kariuki-Nyuthe C., Gomez-Mancilla B., Stein D.J. Obsessive compulsive disorder and the glutamatergic system. Curr. Opin. Psychiatry. 2014;27(1):32–37. doi: 10.1097/YCO.0000000000000017. [http://dx.doi.org/10.1097/YCO. 0000000000000017]. [PMID: 24270485]. [DOI] [PubMed] [Google Scholar]
- 311.Milad M.R., Rauch S.L. 2012. [Google Scholar]
- 312.Wendland J.R., Moya P.R., Timpano K.R., Anavitarte A.P., Kruse M.R., Wheaton M.G., Ren-Patterson R.F., Murphy D.L. A haplotype containing quantitative trait loci for SLC1A1 gene expression and its association with obsessive-compulsive disorder. Arch. Gen. Psychiatry. 2009;66(4):408–416. doi: 10.1001/archgenpsychiatry.2009.6. [http://dx.doi.org/10. 1001/archgenpsychiatry.2009.6]. [PMID: 19349310]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 313.Rosenberg D.R., Keshavan M.S.A.E.A.E. Bennett Research Award. Toward a neurodevelopmental model of of obsessive--compulsive disorder. Biol. Psychiatry. 1998;43(9):623–640. doi: 10.1016/s0006-3223(97)00443-5. [http:// dx.doi.org/10.1016/S0006-3223(97)00443-5]. [PMID: 9582996]. [DOI] [PubMed] [Google Scholar]
- 314.Huyser C., Veltman D.J., de Haan E., Boer F. Paediatric obsessive-compulsive disorder, a neurodevelopmental disorder? Evidence from neuroimaging. Neurosci. Biobehav. Rev. 2009;33(6):818–830. doi: 10.1016/j.neubiorev.2009.01.003. [http://dx.doi.org/10.1016/j.neubiorev.2009.01.003]. [PMID: 19428494]. [DOI] [PubMed] [Google Scholar]
- 315.Gassó P., Ortiz A.E., Mas S., Morer A., Calvo A., Bargalló N., Lafuente A., Lázaro L. Association between genetic variants related to glutamatergic, dopaminergic and neurodevelopment pathways and white matter microstructure in child and adolescent patients with obsessive-compulsive disorder. J. Affect. Disord. 2015;186:284–292. doi: 10.1016/j.jad.2015.07.035. [http://dx.doi.org/10.1016/j.jad.2015.07.035]. [PMID: 26254621]. [DOI] [PubMed] [Google Scholar]
- 316.Cappi C., Brentani H., Lima L., Sanders S.J., Zai G., Diniz B.J., Reis V.N., Hounie A.G., Conceição do Rosário M., Mariani D., Requena G.L., Puga R., Souza-Duran F.L., Shavitt R.G., Pauls D.L., Miguel E.C., Fernandez T.V. Whole-exome sequencing in obsessive-compulsive disorder identifies rare mutations in immunological and neurodevelopmental pathways. Transl. Psychiatry. 2016;6:e764. doi: 10.1038/tp.2016.30. [http://dx.doi.org/10.1038/tp.2016.30]. [PMID: 27023170]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 317.Melo-Felippe F.B., de Salles Andrade J.B., Giori I.G., Vieira-Fonseca T., Fontenelle L.F., Kohlrausch F.B. Catechol-O-methyltransferase gene polymorphisms in specific obsessive-compulsive disorder patients’ subgroups. J. Mol. Neurosci. 2016;58(1):129–136. doi: 10.1007/s12031-015-0697-0. [http://dx.doi.org/10.1007/s12031-015-0697-0]. [PMID: 26687156]. [DOI] [PubMed] [Google Scholar]
- 318.Qin H., Samuels J.F., Wang Y., Zhu Y., Grados M.A., Riddle M.A., Greenberg B.D., Knowles J.A., Fyer A.J., McCracken J.T., Murphy D.L., Rasmussen S.A., Cullen B.A., Piacentini J., Geller D., Stewart S.E., Pauls D., Bienvenu O.J., Goes F.S., Maher B., Pulver A.E., Valle D., Lange C., Mattheisen M., McLaughlin N.C., Liang K.Y., Nurmi E.L., Askland K.D., Nestadt G., Shugart Y.Y. Whole-genome association analysis of treatment response in obsessive-compulsive disorder. Mol. Psychiatry. 2016;21(2):270–276. doi: 10.1038/mp.2015.32. [http://dx.doi.org/10.1038/mp.2015. 32]. [PMID: 25824302]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 319.Etheridge L.A., Crawford T.Q., Zhang S., Roelink H. Evidence for a role of vertebrate Disp1 in long-range Shh signaling. Development. 2010;137(1):133–140. doi: 10.1242/dev.043547. [http://dx.doi.org/10.1242/dev. 043547]. [PMID: 20023168]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 320.Lister J.F. Pharmacogenomics: A focus on antidepressants and atypical antipsychotics. Ment Health Clin. 2016;6(1):48–53. doi: 10.9740/mhc.2016.01.048. [http://dx.doi.org/10.9740/mhc.2016.01.048]. [PMID: 29955447]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 321.Fagerness J., Fonseca E., Hess G.P., Scott R., Gardner K.R., Koffler M., Fava M., Perlis R., Brennan F.X., Lombard J. Pharmacogenetic-guided psychiatric intervention associated with increased adherence and cost savings. Am. J. Manag. Care. 2014;20(5):e146–e156. [PMID: 25326929]. [PubMed] [Google Scholar]
- 322.Singh A.B. Improved antidepressant remission in major depression via a pharmacokinetic pathway polygene pharmacogenetic report. Clin. Psychopharmacol. Neurosci. 2015;13(2):150–156. doi: 10.9758/cpn.2015.13.2.150. [http://dx.doi.org/10.9758/cpn.2015.13.2.150]. [PMID: 26243841]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 323.Russell E.J., Fawcett J.M., Mazmanian D. Risk of obsessive-compulsive disorder in pregnant and postpartum women: a meta-analysis. J. Clin. Psychiatry. 2013;74(4):377–385. doi: 10.4088/JCP.12r07917. [http://dx.doi. org/10.4088/JCP.12r07917]. [PMID: 23656845]. [DOI] [PubMed] [Google Scholar]
- 324.Labad J., Menchón J.M., Alonso P., Segalàs C., Jiménez S., Vallejo J. Female reproductive cycle and obsessive-compulsive disorder. J. Clin. Psychiatry. 2005;66(4):428–435. doi: 10.4088/jcp.v66n0404. [http://dx.doi. org/10.4088/JCP.v66n0404]. [PMID: 15816784]. [DOI] [PubMed] [Google Scholar]
- 325.Uguz F., Gezginc K., Zeytinci I.E., Karatayli S., Askin R., Guler O., Kir S.F., Emul H.M., Ozbulut O., Gecici O. Obsessive-compulsive disorder in pregnant women during the third trimester of pregnancy. Compr. Psychiatry. 2007;48(5):441–445. doi: 10.1016/j.comppsych.2007.05.001. [http://dx.doi.org/10.1016/j.comppsych.2007.05.001]. [PMID: 17707252]. [DOI] [PubMed] [Google Scholar]
- 326.Forray A., Focseneanu M., Pittman B., McDougle C.J., Epperson C.N. Onset and exacerbation of obsessive-compulsive disorder in pregnancy and the postpartum period. J. Clin. Psychiatry. 2010;71(8):1061–1068. doi: 10.4088/JCP.09m05381blu. [http://dx.doi.org/10.4088/JCP.09m05381blu]. [PMID: 20492843]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 327.Loomans E.M., van der Stelt O., van Eijsden M., Gemke R.J., Vrijkotte T., den Bergh B.R. Antenatal maternal anxiety is associated with problem behaviour at age five. Early Hum. Dev. 2011;87(8):565–570. doi: 10.1016/j.earlhumdev.2011.04.014. [http://dx.doi.org/10.1016/j.earlhumdev.2011.04. 014]. [PMID: 21576004]. [DOI] [PubMed] [Google Scholar]
- 328.Sanchez S.E., Puente G.C., Atencio G., Qiu C., Yanez D., Gelaye B., Williams M.A. Risk of spontaneous preterm birth in relation to maternal depressive, anxiety, and stress symptoms. J. Reprod. Med. 2013;58(1-2):25–33. [PMID: 23447915]. [PMC free article] [PubMed] [Google Scholar]
- 329.Van Batenburg-Eddes T., Brion M.J., Henrichs J., Jaddoe V.W., Hofman A., Verhulst F.C., Lawlor D.A., Davey Smith G., Tiemeier H. Parental depressive and anxiety symptoms during pregnancy and attention problems in children: a cross-cohort consistency study. J. Child Psychol. Psychiatry. 2013;54(5):591–600. doi: 10.1111/jcpp.12023. [http://dx.doi.org/10.1111/jcpp.12023]. [PMID: 23215861]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 330.Leis J.A., Heron J., Stuart E.A., Mendelson T. Associations between maternal mental health and child emotional and behavioral problems: does prenatal mental health matter? J. Abnorm. Child Psychol. 2014;42(1):161–171. doi: 10.1007/s10802-013-9766-4. [http://dx.doi.org/10.1007/s10802-013-9766-4]. [PMID: 23748337]. [DOI] [PubMed] [Google Scholar]
- 331.Ding X.X., Wu Y.L., Xu S.J., Zhu R.P., Jia X.M., Zhang S.F., Huang K., Zhu P., Hao J.H., Tao F.B. Maternal anxiety during pregnancy and adverse birth outcomes: a systematic review and meta-analysis of prospective cohort studies. J. Affect. Disord. 2014;159:103–110. doi: 10.1016/j.jad.2014.02.027. [http://dx.doi.org/10.1016/j.jad.2014.02.027]. [PMID: 24679397]. [DOI] [PubMed] [Google Scholar]
- 332.Uguz F., Onder Sonmez E., Sahingoz M., Gokmen Z., Basaran M., Gezginc K., Sonmez G., Kaya N., Yilmaz E., Erdem S.S., Dulger H.H., Cicekler H., Tasyurek E. Neuroinflammation in the fetus exposed to maternal obsessive-compulsive disorder during pregnancy: a comparative study on cord blood tumor necrosis factor-alpha levels. Compr. Psychiatry. 2014;55(4):861–865. doi: 10.1016/j.comppsych.2013.12.018. [http:// dx.doi.org/10.1016/j.comppsych.2013.12.018]. [PMID: 24480417]. [DOI] [PubMed] [Google Scholar]
- 333.Byatt N., Deligiannidis K.M., Freeman M.P. Antidepressant use in pregnancy: a critical review focused on risks and controversies. Acta Psychiatr. Scand. 2013;127(2):94–114. doi: 10.1111/acps.12042. [http://dx.doi.org/10. 1111/acps.12042]. [PMID: 23240634]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 334.Yonkers K.A., Wisner K.L., Stewart D.E., Oberlander T.F., Dell D.L., Stotland N., Ramin S., Chaudron L., Lockwood C. The management of depression during pregnancy: a report from the American Psychiatric Association and the American College of Obstetricians and Gynecologists. Gen. Hosp. Psychiatry. 2009;31(5):403–413. doi: 10.1016/j.genhosppsych.2009.04.003. [http://dx.doi.org/10.1016/j.genhosppsych.2009.04. 003]. [PMID: 19703633]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 335.Uguz F. Pharmacotherapy of obsessive-compulsive disorder during pregnancy: a clinical approach. Rev. Bras. Psiquiatr. 2015;37(4):334–342. doi: 10.1590/1516-4446-2015-1673. [http://dx.doi.org/10.1590/1516-4446-2015-1673]. [PMID: 26692431]. [DOI] [PubMed] [Google Scholar]
- 336.Kellner M. Drug treatment of obsessive-compulsive disorder. Dialogues Clin. Neurosci. 2010;12(2):187–197. doi: 10.31887/DCNS.2010.12.2/mkellner. [PMID: 20623923]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 337.Ellfolk M., Malm H. Risks associated with in utero and lactation exposure to selective serotonin reuptake inhibitors (SSRIs). Reprod. Toxicol. 2010;30(2):249–260. doi: 10.1016/j.reprotox.2010.04.015. [http://dx.doi.org/10.1016/ j.reprotox.2010.04.015]. [PMID: 20447455]. [DOI] [PubMed] [Google Scholar]
- 338.Gentile S. Drug treatment for mood disorders in pregnancy. Curr. Opin. Psychiatry. 2011;24(1):34–40. doi: 10.1097/YCO.0b013e3283413451. [http://dx.doi.org/10.1097/ YCO.0b013e3283413451]. [PMID: 21088587]. [DOI] [PubMed] [Google Scholar]
- 339.Malm H., Artama M., Gissler M., Ritvanen A. Selective serotonin reuptake inhibitors and risk for major congenital anomalies. Obstet. Gynecol. 2011;118(1):111–120. doi: 10.1097/AOG.0b013e318220edcc. [http://dx.doi.org/10. 1097/AOG.0b013e318220edcc]. [PMID: 21646927]. [DOI] [PubMed] [Google Scholar]
- 340.Lorenzo L., Byers B., Einarson A. Antidepressant use in pregnancy. Expert Opin. Drug Saf. 2011;10(6):883–889. doi: 10.1517/14740338.2011.583917. [http://dx. doi.org/10.1517/14740338.2011.583917]. [PMID: 21545242]. [DOI] [PubMed] [Google Scholar]
- 341.Myles N., Newall H., Ward H., Large M. Systematic meta-analysis of individual selective serotonin reuptake inhibitor medications and congenital malformations. Aust. N. Z. J. Psychiatry. 2013;47(11):1002–1012. doi: 10.1177/0004867413492219. [http://dx.doi.org/10.1177/0004867413492219]. [PMID: 23761574]. [DOI] [PubMed] [Google Scholar]
- 342.Grigoriadis S. VonderPorten, E.H.; Mamisashvili, L.; Roerecke, M.; Rehm, J.; Dennis, C.L.; Koren, G.; Steiner, M.; Mousmanis, P.; Cheung, A.; Ross, L.E. Antidepressant exposure during pregnancy and congenital malformations: is there an association? A systematic review and meta-analysis of the best evidence. J. Clin. Psychiatry. 2013;74(4):e293–e308. doi: 10.4088/JCP.12r07966. [http://dx.doi.org/10.4088/JCP.12r07966]. [PMID: 23656855]. [DOI] [PubMed] [Google Scholar]
- 343.Klieger-Grossmann C., Weitzner B., Panchaud A., Pistelli A., Einarson T., Koren G., Einarson A. Pregnancy outcomes following use of escitalopram: a prospective comparative cohort study. J. Clin. Pharmacol. 2012;52(5):766–770. doi: 10.1177/0091270011405524. [http://dx.doi.org/10.1177/ 0091270011405524]. [PMID: 22075232]. [DOI] [PubMed] [Google Scholar]
- 344.Bellantuono C., Bozzi F., Orsolini L., Catena-Dell’Osso M. The safety of escitalopram during pregnancy and breastfeeding: a comprehensive review. Hum. Psychopharmacol. 2012;27(6):534–539. doi: 10.1002/hup.2265. [http://dx.doi.org/10.1002/hup.2265]. [PMID: 23044635]. [DOI] [PubMed] [Google Scholar]
- 345.Alwan S., Reefhuis J., Rasmussen S.A., Friedman J.M. Patterns of antidepressant medication use among pregnant women in a United States population. J. Clin. Pharmacol. 2011;51(2):264–270. doi: 10.1177/0091270010373928. [http://dx.doi.org/10.1177/0091270010373928]. [PMID: 20663997]. [DOI] [PubMed] [Google Scholar]
- 346.Andrade S.E., Raebel M.A., Brown J., Lane K., Livingston J., Boudreau D., Rolnick S.J., Roblin D., Smith D.H., Willy M.E., Staffa J.A., Platt R. Use of antidepressant medications during pregnancy: a multisite study. Am. J. Obstet. Gynecol. 2008;198(2):194.e1–194.e5. doi: 10.1016/j.ajog.2007.07.036. [http://dx.doi.org/10.1016/j.ajog.2007.07. 036]. [PMID: 17905176]. [DOI] [PubMed] [Google Scholar]
- 347.Yonkers K.A., Blackwell K.A., Glover J., Forray A. Antidepressant use in pregnant and postpartum women. Annu. Rev. Clin. Psychol. 2014;10:369–392. doi: 10.1146/annurev-clinpsy-032813-153626. [http://dx.doi.org/10.1146/annurev-clinpsy-032813-153626]. [PMID: 24313569]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 348.Gentile S. Tricyclic antidepressants in pregnancy and puerperium. Expert Opin. Drug Saf. 2014;13(2):207–225. doi: 10.1517/14740338.2014.869582. [http://dx.doi.org/10. 1517/14740338.2014.869582]. [PMID: 24383525]. [DOI] [PubMed] [Google Scholar]
- 349.Källén B.A., Otterblad Olausson P. Maternal drug use in early pregnancy and infant cardiovascular defect. Reprod. Toxicol. 2003;17(3):255–261. doi: 10.1016/s0890-6238(03)00012-1. [http://dx.doi.org/10.1016/S0890-6238(03)00012-1]. [PMID: 12759093]. [DOI] [PubMed] [Google Scholar]
- 350.Källén B., Otterblad Olausson P. Antidepressant drugs during pregnancy and infant congenital heart defect. Reprod. Toxicol. 2006;21(3):221–222. doi: 10.1016/j.reprotox.2005.11.006. [http://dx.doi.org/10.1016/j.reprotox.2005. 11.006]. [PMID: 16406480]. [DOI] [PubMed] [Google Scholar]
- 351.Udechuku A., Nguyen T., Hill R., Szego K. Antidepressants in pregnancy: a systematic review. Aust. N. Z. J. Psychiatry. 2010;44(11):978–996. doi: 10.3109/00048674.2010.507543. [PMID: 21034181]. [DOI] [PubMed] [Google Scholar]
- 352.Seibell P.J., Hollander E. Management of obsessive-compulsive disorder. F1000Prime Rep. 2014;6:68. doi: 10.12703/P6-68. [http://dx.doi.org/10. 12703/P6-68]. [PMID: 25165567]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 353.Suri R., Altshuler L., Hellemann G., Burt V.K., Aquino A., Mintz J. Effects of antenatal depression and antidepressant treatment on gestational age at birth and risk of preterm birth. Am. J. Psychiatry. 2007;164(8):1206–1213. doi: 10.1176/appi.ajp.2007.06071172. [http://dx.doi.org/10.1176/ appi.ajp.2007.06071172]. [PMID: 17671283]. [DOI] [PubMed] [Google Scholar]
- 354.Andrade C. Augmenting selective serotonin reuptake inhibitors with clomipramine in obsessive-compulsive disorder: benefits and risks. J. Clin. Psychiatry. 2013;74(12):e1128–e1133. doi: 10.4088/JCP.13f08883. [http://dx. doi.org/10.4088/JCP.13f08883]. [PMID: 24434100]. [DOI] [PubMed] [Google Scholar]
- 355.Diniz J.B., Shavitt R.G., Pereira C.A., Hounie A.G., Pimentel I., Koran L.M., Dainesi S.M., Miguel E.C. Quetiapine versus clomipramine in the augmentation of selective serotonin reuptake inhibitors for the treatment of obsessive-compulsive disorder: a randomized, open-label trial. J. Psychopharmacol. (Oxford) 2010;24(3):297–307. doi: 10.1177/0269881108099423. [http://dx.doi.org/10.1177/0269881108099423]. [PMID: 19164490]. [DOI] [PubMed] [Google Scholar]
- 356.Skapinakis P., Papatheodorou T., Mavreas V. Antipsychotic augmentation of serotonergic antidepressants in treatment-resistant obsessive-compulsive disorder: a meta-analysis of the randomized controlled trials. Eur. Neuropsychopharmacol. 2007;17(2):79–93. doi: 10.1016/j.euroneuro.2006.07.002. [http://dx.doi.org/10.1016/j.euroneuro.2006.07.002]. [PMID: 16904298]. [DOI] [PubMed] [Google Scholar]
- 357.Bloch M.H., Peterson B.S., Scahill L., Otka J., Katsovich L., Zhang H., Leckman J.F. Adulthood outcome of tic and obsessive-compulsive symptom severity in children with Tourette syndrome. Arch. Pediatr. Adolesc. Med. 2006;160(1):65–69. doi: 10.1001/archpedi.160.1.65. [http://dx. doi.org/10.1001/archpedi.160.1.65]. [PMID: 16389213]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 358.National Institute for Health and Care Excellence. 2013 https:// www.nice.org.uk/guidance/cg31
- 359.Poppe C., Müller S.T., Greil W., Walder A., Grohmann R., Stübner S. Pharmacotherapy for obsessive compulsive disorder in clinical practice - Data of 842 inpatients from the International AMSP Project between 1994 and 2012. J. Affect. Disord. 2016;200:89–96. doi: 10.1016/j.jad.2016.04.035. [http://dx.doi.org/10.1016/j.jad.2016.04.035]. [PMID: 27130958]. [DOI] [PubMed] [Google Scholar]
- 360.Bandelow B., Sher L., Bunevicius R., Hollander E., Kasper S., Zohar J., Möller H.J. Guidelines for the pharmacological treatment of anxiety disorders, obsessive-compulsive disorder and posttraumatic stress disorder in primary care. Int. J. Psychiatry Clin. Pract. 2012;16(2):77–84. doi: 10.3109/13651501.2012.667114. [http://dx.doi.org/10.3109/13651501. 2012.667114]. [PMID: 22540422]. [DOI] [PubMed] [Google Scholar]
- 361.Koran L.M., Simpson H.B. Guideline Watch (March 2013): Practice Guideline for the Treatment of patients with Obsessive-Compulsive Disorder. Arlington, VA: American Psychiatric Association; 2013. [PubMed] [Google Scholar]
- 362.Moher D., Liberati A., Tetzlaff J., Altman D.G. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int. J. Surg. 2010;8(5):336–341. doi: 10.1016/j.ijsu.2010.02.007. [http://dx.doi.org/10. 1016/j.ijsu.2010.02.007]. [PMID: 20171303]. [DOI] [PubMed] [Google Scholar]