

Abstract
Background
Ulcerative colitis is an inflammatory condition affecting the colon, with an annual incidence of approximately 10 to 20 per 100,000 people. The majority of people with ulcerative colitis can be put into remission, leaving a group who do not respond to first‐ or second‐line therapies. There is a significant proportion of people who experience adverse effects with current therapies. Consequently, new alternatives for the treatment of ulcerative colitis are constantly being sought. Probiotics are live microbial feed supplements that may beneficially affect the host by improving intestinal microbial balance, enhancing gut barrier function and improving local immune response.
Objectives
To assess the efficacy of probiotics compared with placebo or standard medical treatment (5‐aminosalicylates, sulphasalazine or corticosteroids) for the induction of remission in people with active ulcerative colitis.
Search methods
We searched CENTRAL, MEDLINE, Embase, and two other databases on 31 October 2019. We contacted authors of relevant studies and manufacturers of probiotics regarding ongoing or unpublished trials that may be relevant to the review, and we searched ClinicalTrials.gov. We also searched references of trials for any additional trials.
Selection criteria
Randomised controlled trials (RCTs) investigating the effectiveness of probiotics compared to standard treatments or placebo in the induction of remission of active ulcerative colitis. We considered both adults and children, with studies reporting outcomes of clinical, endoscopic, histologic or surgical remission as defined by study authors
Data collection and analysis
Two review authors independently conducted data extraction and 'Risk of bias' assessment of included studies. We analysed data using Review Manager 5. We expressed dichotomous and continuous outcomes as risk ratios (RRs) and mean differences (MDs) with 95% confidence intervals (CIs). We assessed the certainty of the evidence using the GRADE methodology.
Main results
In this review, we included 14 studies (865 randomised participants) that met the inclusion criteria. Twelve of the studies looked at adult participants and two studies looked at paediatric participants with mild to moderate ulcerative colitis, the average age was between 12.5 and 47.7 years. The studies compared probiotics to placebo, probiotics to 5‐ASA and a combination of probiotics plus 5‐ASA compared to 5‐ASA alone. Seven studies used a single probiotic strain and seven used a mixture of strains. The studies ranged from two weeks to 52 weeks. The risk of bias was high for all except two studies due to allocation concealment, blinding of participants, incomplete reports of outcome data and selective reporting. This led to GRADE ratings of the evidence ranging from moderate to very low.
Probiotics versus placebo Probiotics may induce clinical remission when compared to placebo (RR 1.73, 95% CI 1.19 to 2.54; 9 studies, 594 participants; low‐certainty evidence; downgraded due to imprecision and risk of bias, number needed to treat for an additional beneficial outcome (NNTB) 5). Probiotics may lead to an improvement in clinical disease scores (RR 2.29, 95% CI 1.13 to 4.63; 2 studies, 54 participants; downgraded due to risk of bias and imprecision).
There may be little or no difference in minor adverse events, but the evidence is of very low certainty (RR 1.04, 95% CI 0.42 to 2.59; 7 studies, 520 participants). Reported adverse events included abdominal bloating and discomfort. Probiotics did not lead to any serious adverse events in any of the seven studies that reported on it, however five adverse events were reported in the placebo arm of one study (RR 0.09, CI 0.01 to 1.66; 1 study, 526 participants; very low‐certainty evidence; downgraded due to high risk of bias and imprecision). Probiotics may make little or no difference to withdrawals due to adverse events (RR 0.85, 95% CI 0.42 to 1.72; 4 studies, 401 participants; low‐certainty evidence).
Probiotics versus 5‐ASA There may be little or no difference in the induction of remission with probiotics when compared to 5‐ASA (RR 0.92, 95% CI 0.73 to 1.16; 1 study, 116 participants; low‐certainty evidence; downgraded due to risk of bias and imprecision). There may be little or no difference in minor adverse events, but the evidence is of very low certainty (RR 1.33, 95% CI 0.53 to 3.33; 1 study, 116 participants). Reported adverse events included abdominal pain, nausea, headache and mouth ulcers. There were no serious adverse events with probiotics, however perforated sigmoid diverticulum and respiratory failure in a patient with severe emphysema were reported in the 5‐ASA arm (RR 0.21, 95% CI 0.01 to 4.22; 1 study, 116 participants; very low‐certainty evidence).
Probiotics combined with 5‐ASA versus 5‐ASA alone Low‐certainty evidence from a single study shows that when combined with 5‐ASA, probiotics may slightly improve the induction of remission (based on the Sunderland disease activity index) compared to 5‐ASA alone (RR 1.22 CI 1.01 to 1.47; 1 study, 84 participants; low‐certainty evidence; downgraded due to unclear risk of bias and imprecision). No information about adverse events was reported.
Time to remission, histological and biochemical outcomes were sparsely reported in the studies. None of the other secondary outcomes (progression to surgery, need for additional therapy, quality of life scores, or steroid withdrawal) were reported in any of the studies.
Authors' conclusions
Low‐certainty evidence suggests that probiotics may induce clinical remission in active ulcerative colitis when compared to placebo. There may be little or no difference in clinical remission with probiotics alone compared to 5‐ASA. There is limited evidence from a single study which failed to provide a definition of remission, that probiotics may slightly improve the induction of remission when used in combination with 5‐ASA. There was no evidence to assess whether probiotics are effective in people with severe and more extensive disease, or if specific preparations are superior to others. Further targeted and appropriately designed RCTs are needed to address the gaps in the evidence base. In particular, appropriate powering of studies and the use of standardised participant groups and outcome measures in line with the wider field are needed, as well as reporting to minimise risk of bias.
Plain language summary
Probiotics for the treatment of active ulcerative colitis
What is the aim of this review?
The aim of this Cochrane Review was to find out whether probiotics can induce remission in people with ulcerative colitis. We analysed data from 14 studies to answer this question.
Key messages
Probiotics may be better at inducing remission than placebo (dummy treatment). It is unclear whether probiotics are better than 5‐aminosalicylic acid (5‐ASA, an anti‐inflammatory agent used to treat inflammatory bowel disease), however there is limited evidence that when both treatments are used as combined therapy they may be better than 5‐ASA alone in inducing remission. Most studies reported that no serious adverse events took place. For the studies that did report on it, serious adverse events did not occur in the probiotic group. Minor adverse events reported were bloating and diarrhoea.
What was studied in the review?
Ulcerative colitis is a relapsing and remitting disease which causes inflammation of the large bowel and leads to symptoms such as abdominal pain, diarrhoea and tiredness. There is some evidence to suggest that an imbalance in the bacteria of the gut is the cause of the disease, and therefore probiotics, which are live micro‐organisms, can alter the bacteria and possibly reduce the inflammation.
What are the main results of the review?
We searched for randomised controlled trials (RCTs; clinical studies where people are randomly put into one of two or more treatment groups) comparing probiotics with placebo, probiotics with 5‐ASA, and probiotics in combination with 5‐ASA. We found 14 RCTs looking at 865 participants. The trials looked at adult and paediatric participants. Eight studies allowed additional therapy to continue, whilst the other four studies were unclear about this.
1) Probiotics may improve induction of clinical remission when compared to placebo.
2) It is unclear whether probiotics lead to a difference in adverse events (minor and serious) when compared to placebo.
3) There is limited evidence to determine whether probiotics offer better disease improvement when compared to placebo.
4) There may be little or no difference in the induction of remission with probiotics when compared to 5‐ASA (low‐certainty evidence).
5) There is limited evidence to suggest that when probiotics plus 5‐ASA are compared to 5‐ASA alone, probiotics may offer a slightly better chance of induction of remission. This is based on low‐certainty evidence from one study, and we are not sure of the type of remission studied.
6) Serious adverse events were reported when probiotics were compared with placebo, but only occurred in the placebo group.
Conclusion
Whilst the evidence suggests that probiotics may be better at improving induction than placebo, our confidence in the estimate is limited because of the low‐certainty evidence. This is attributed to the small number of participants in each study along with the unreliable methods utilised by the trials. With the evidence presented in these studies, we are unable to make strong conclusions into the effectiveness of probiotics; better designed studies with more participants are needed.
How up‐to‐date is this review?
This review is up‐to‐date as of October 2019.
Summary of findings
Background
Description of the condition
Ulcerative colitis is a chronic relapsing disease, with the greatest reported incidence in mainland Europe and Scandinavia of 9.2 to 20.3 per 100,000 people (Loftus 2004), totalling approximately 2.2 million sufferers in Europe alone. The peak incidence of the disease occurs between 15 and 25 years of age and there is another smaller prevalence at ages 55 to 65. The disease is characterised by abdominal pain, bloody diarrhoea and faecal urgency. The diagnosis of ulcerative colitis is made on the basis of medical history, signs and symptoms, and any endoscopic or histopathological findings.
The disease is caused by diffuse inflammation, which starts at the rectum, spreads proximally, and is limited to the colon. The aetiology of the disease is unknown, but is likely to be multifactorial; consisting of a genetic predisposition, dysregulation of the mucosal and epithelial barrier and lastly dysbiosis, although whether dysbiosis causes or is a result of the disease remains unclear (Ungaro 2016). The genetic predisposition creates a four‐fold risk for first‐degree relatives.
Description of the intervention
Probiotics are live micro‐organisms, that when consumed, may provide multiple health benefits. They produce their benefits by altering the gut microbiome through either enhancing the activity, volume or both, of the normal flora. Lactobacillus spp, for example, is one of the more popular probiotics and is thought to secrete bacteriocin, blocking the adherence or translocation of harmful bacteria (Panigrahi 2014).
Lactobacillus rhamnosus GG (Lrhamnosus GG) produced mixed responses in animal models of colitis (Dieleman 2003; Shibolet 2002), as did Lactobacillus plantarum (L plantarum) 299V (Dieleman 2003; Kennedy 2000; Schultz 2002). Studies investigating combinations of probiotic species incorporated within the probiotic De Simone Formulation have demonstrated a partial reduction of colitis in animal models (Madsen 2001; Shibolet 2002). There has been increasing interest in the use of probiotics, as they are considered safe and easily accessible (Ong 2019). It is worth noting that there are a huge number of different preparations available, varying in the specific strains isolated, the use of mixed strains in a single preparation, the form of the preparation and finally the licensing arrangements surrounding the preparations (medicinal versus food products).
How the intervention might work
There is growing evidence looking at the effects of probiotics in the use of inducing remission in ulcerative colitis since a previous Cochrane review (Mallon 2007). Due to the part that dysbiosis plays in ulcerative colitis, there is potential benefit in trying to restore the indigenous flora. Several observations, both on humans and animal models, emphasised the importance of bacterial flora in inflammatory bowel disease pathogenesis, justifying the current interest in antibiotic and probiotic therapies, aimed at the manipulation of enteric flora (Cui 2004). The therapeutic efficacy of probiotics has been demonstrated in various models of experimental colitis, including interleukin‐10 deficient mice (Madsen 1999; Schultz 2002), and acetic acid‐induced colitis in rats (Fabia 1993).
Why it is important to do this review
In the UK, National Institute for Health and Care Excellence (NICE) and USA guidelines state that first‐line therapy for maintenance of remission in ulcerative colitis is 5‐aminosalicylic acid (5‐ASA) (NICE 2013). 5‐ASA works by binding to PPAR‐ỿ and reducing cytokine production. Some of the adverse effects associated with 5‐ASA include headache, rash, nausea (common), pancreatitis (uncommon), and agranulocytosis (rare). Due to these side effects, some people are unable to tolerate the drug. If 5‐ASA fails to provide any relief then steroids can be added as an adjunct. Steroids, such as prednisolone, can also be used alone, however if after two to four weeks an adequate response is not observed, then immune suppressant therapies, such as anti‐tumour necrosis factor (TNF) monoclonals, vedolizumab and tofacitinib may be used to induce remission. These drugs work by blocking leukocyte recruitment at the molecular and vascular level (Fiorino 2016), some of the side effects include headache, dizziness and arthralgia. Despite these medications, failure to induce remission occurs in 20% to 30% of people on current treatments, with a proportion of patients eventually requiring colectomy. Consequently, new alternatives for the treatment of ulcerative colitis are constantly being sought.
The relapsing and remitting nature of the disease means that people can be in and out of hospital, experimenting with different drug regimens. The treatment costs Europe between GBP 11 to 26 billion annually, with per patient costs approximately GBP 8011 to 9306 (Cohen 2010). If an alternative, cheaper treatment can be found for ulcerative colitis, then it would greatly benefit not only a budget stricken National Health Service (NHS), but also improve patients' quality of life. Whilst some studies have suggested that probiotics may be useful for maintenance of remission in mild to moderate ulcerative colitis (Kruis 2004; Zocco 2006), others have failed to show any benefit (Kruis 1997; Rembacken 1999). The previous published form of this review is more than 10 years old (Mallon 2007), and did not consider a paediatric population. As the burden of ulcerative colitis is shared within this population as well, consideration of studies in this group of patients would provide a greater understanding as to whether the intervention works differently in adults compared to children. In this review, we investigated the available evidence on the use of probiotics for the induction of remission in ulcerative colitis.
Objectives
To assess the efficacy of probiotics compared with placebo or standard medical treatment (5‐aminosalicylic acid (5‐ASA), sulphasalazine or corticosteroids) for the induction of remission in people with active ulcerative colitis.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs).
Types of participants
People of any age with active ulcerative colitis previously diagnosed by clinical, endoscopic, histologic or surgical remissionas defined by study authors
Types of interventions
RCTs comparing probiotics administered in any form (drink, powder, capsule) orally as a single species or as a cocktail of multiple species,versus placebo, probiotics standard therapy (e.g. 5‐aminosalicylic acid (5‐ASA), sulfasalazine or corticosteroids), or probiotics used in conjunction with standard therapy versus standard therapy for the induction of remission in active ulcerative colitis.
Types of outcome measures
Primary outcomes
Remission (clinical, endoscopic, histologic or surgical remission, as defined by study authors)
Secondary outcomes
Disease improvement (clinical or endoscopic, as defined by study authors)
Steroid withdrawal
Clinical activity scores
Histology scores
Biochemical markers of inflammation
Need for additional therapy
Progression to surgery
Symptomatic severity (stool frequency, abdominal pain)
Quality of life scores
Time to remission/improvement
Minor adverse events
Serious adverse events
Withdrawal due to adverse events
Search methods for identification of studies
We attempted to identify all relevant studies regardless of language or publication status.
Electronic searches
We conducted a comprehensive and systematic search to identify RCTs from inception to 31 October 2019, using the following databases.
Cochrane Inflammatory Bowel Disease Group Specialized Trials Register
Cochrane Central Register of Controlled Trials (CENTRAL)
MEDLINE
Embase
CINAHL
We did not place restrictions on publication dates (after 1966) or language. We reported the detailed search strategies in Appendix 1.
Searching other resources
We inspected the reference lists of all identified studies for additional trials. We also contacted leaders in the field and manufacturers of probiotics to identify potentially relevant studies. We also searched ClinicalTrials.gov for ongoing trials (clinicaltrials.gov).
Data collection and analysis
Selection of studies
We undertook study selection in Covidence.
Using the above search strategy, two review authors (LK, MG) identified titles that appeared to be potentially relevant. These were independently screened and in circumstances of disagreement, a third review author (AA) was involved to reach consensus.
There is some evidence that data from abstract publications can be inconsistent with data from published articles (Pitkin 1999), therefore we considered abstract publications, but only if sufficient data were presented to judge inclusion criteria fully and reports of the primary and secondary outcomes were given. If these were not available, we contacted authors directly, and if data were not provided, we excluded such studies.
The review authors, after reading the full texts, independently assessed the eligibility of all trials identified using ad hoc eligibility, based on the inclusion criteria above. Disagreement among review authors was again discussed, and agreement was reached by consensus after involvement of a third review author. We contacted authors of multiple publications, which appeared to report on the same study, for clarification. A flow chart was included (Figure 1).
1.
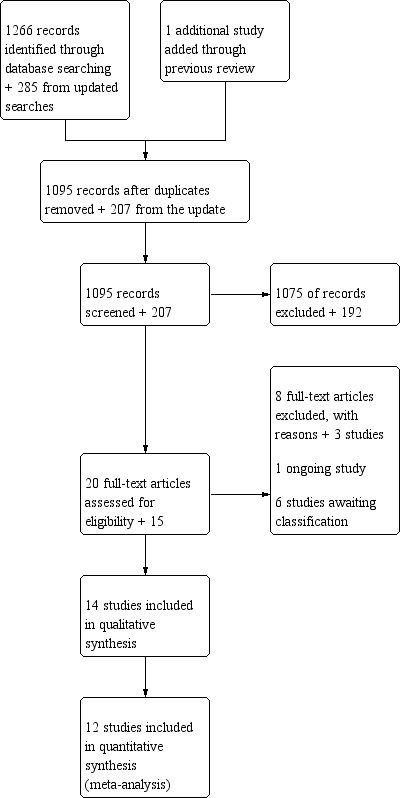
Study flow diagram
Data extraction and management
Two review authors (LK and MG) carried out data extraction independently by using piloted forms. The data collected included information on the study design, participants, intervention and comparator, as well as outcome. Discrepancies in data extraction were discussed and if necessary, a third review author was consulted. LK and MG then entered data into the review file.
Assessment of risk of bias in included studies
The review authors (LK and MG) independently carried out 'Risk of bias' assessment of the included studies. We used the Cochrane 'Risk of bias' tool in assessing the following domains (Higgins 2011).
Random sequence generation
Allocation concealment
Blinding of participants and personnel
Blinding of outcome assessors
Completeness of outcome data
Selective reporting
Other sources of bias
We considered subjective outcomes separately in our assessment of blinding and incompleteness of data. We judged studies to be at 'high', 'low' or 'unclear' risk of bias for each domain assessed. We judged the risk of bias across studies as follows.
Low risk of bias (plausible bias unlikely to seriously alter the results) if all domains are at low risk of bias.
Unclear risk of bias (plausible bias that raises some doubt about the results) if one or more domains are at unclear risk of bias.
High risk of bias (plausible bias that seriously weakens confidence in the results) if one or more domains are at high risk of bias.
Disagreements were resolved by consensus. We contacted study authors when insufficient information was provided to determine the risk of bias. Where we obtained information supporting our judgement on risk of bias through correspondence with study authors, we indicated this in the 'Risk of bias' table.
Measures of treatment effect
We expressed the treatment effect of dichotomous outcomes as risk ratios (RRs) and continuous outcomes as mean differences (MDs). In future updates, where studies measure the same outcome using different scales, we will express continuous outcomes as standardised mean differences (SMDs). For continuous data, we preferred final scores to change scores. We planned to express time to remission as median or hazard ratio (HR), but as data were not sufficiently reported this was unnecessary.
Unit of analysis issues
The participant was the unit of analysis. We dealt with studies involving multiple trial arms according to methods proposed in Higgins 2011 (Section 16.5.4). We did not combine groups, but rather we used relevant groups as per the appropriate pair wise comparison. We considered unit of analysis issues arising from the measurement of outcomes at different time points.
Dealing with missing data
We contacted study authors for missing data. Where possible, we applied intention‐to‐treat analysis. We calculated missing standard deviations (SDs) from other reported data (such as P values, confidence intervals (CIs) and standard errors), where possible. However, we imputed missing data. If data was recorded from a graph, this was stated. In reporting adverse events, we assumed 'worst case' to avoid under reporting. For instance, we assumed that minor and serious adverse events were related to the intervention.
Assessment of heterogeneity
The decision to pool the results of individual studies depended on an assessment of clinical and methodological heterogeneity. If we considered studies sufficiently homogeneous for data pooling, we assessed statistical heterogeneity by visual inspection of the forest plots, and using the Chi2 test with a significance level at P < 0.1 and the I2 statistic. We based our interpretation of the I2 statistic results on those suggested by Higgins 2011 (Section 9.5.2):
0% to 40%: might not be important;
30% to 60%: may represent moderate heterogeneity;
50% to 90%; may represent substantial heterogeneity;
75% to 100%: considerable heterogeneity.
Assessment of reporting biases
We avoided various reporting biases by undertaking an extensive literature search without restrictions on publication date or language. We used study protocols and trial registrations in assessing studies for selective reporting. If we had more than 10 studies, we would have generated a funnel plot. The magnitude of publication bias would have been initially determined by visual inspection of the asymmetry of the funnel plot. If this appeared asymmetric, we would have performed a linear regression of intervention effect estimate against its standard error, weighted by the inverse of the variance of the intervention effect estimate (Egger 1997). P < 0.1 would be an indication of a publication bias or small‐study effect.
Data synthesis
We analysed data using Review Manager 5 (Review Manager 2014). For dichotomous outcomes, we derived RRs and 95% CIs for each study. For continuous outcomes, we derived MDs and 95% CIs. We combined the results of included studies for each outcome if appropriate. We used either fixed‐effect or random‐effects models, depending on the presence of statistical heterogeneity and the number or size of studies available. We considered not pooling data where there was considerable heterogeneity (I2 ≥ 75%) which was not explained by clinical or methodological differences between the studies. However, we presented data which we were unable to pool as a narrative summary.
Subgroup analysis and investigation of heterogeneity
We attempted to investigate unexplained heterogeneity. We checked the data, adjusted for heterogeneity by using a random‐effects model and then changed the measure of treatment effects from RR to odds ratios (OR), as proposed in section 9.5.3 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We undertook the following subgroup analyses.
Paediatric versus adult population
Single versus multiple strain probiotics
Sensitivity analysis
We undertook sensitivity analyses to assess whether results of the review are robust to the decisions which were taken during the review process. We examined the effect on the review findings of:
excluding studies at high risk of bias; and
comparing the use of fixed‐effect versus random‐effects models.
Summary of findings and assessment of the certainty of the evidence
We used the GRADE approach to assess the certainty of evidence related to the primary outcomes listed in Types of outcome measures (Schünemann 2011). The four levels of evidence certainty are 'high', 'moderate', 'low' or 'very low'. We downgraded the certainty of evidence due to study limitations (risk of bias), imprecision, inconsistency, indirectness or publication bias.
Where there was sufficient evidence, we prepared 'Summary of findings' tables for our main comparisons; we presented the results for remission, disease improvement and adverse events. Two review authors (LK and MG) independently produced 'Summary of findings' tables using the GRADEpro GDT software (GRADEpro GDT 2015).
Results
Description of studies
Results of the search
The literature search conducted in December 2017 and updated in November 2019 provided 1302 studies once duplicates were removed, and one study identified through the previous review was added. Once we screened the titles and abstracts, and removed further duplicates, we found 35 studies that met the inclusion criteria. Full‐text copies were available for 33 of these studies. Further scrutiny identified 14 studies that met the inclusion criteria and we excluded 11 studies with reasons. We contacted authors of all 14 included studies (Kato 2004; Li 2013; Liu 2014; Matthes 2010; Miele 2009; Oliva 2011; Rembacken 1999; Sanchez‐Morales 2019; Solovyeva 2014; Sood 2009; Tamaki 2016; Tursi 2010; Vejdani 2017; Zhang 2018a); two authors replied (Sanchez‐Morales 2019; Sood 2009).
We identified one ongoing study and six studies are awaiting classification (Characteristics of ongoing studies; Characteristics of studies awaiting classification).
The results of the search are presented in the PRISMA diagram (Figure 1). Full details of the included and excluded studies are available in the Characteristics of included studies and Characteristics of excluded studies.
Included studies
Study design and setting
We included 14 studies published between 1999 and 2019 (Kato 2004; Li 2013; Liu 2014; Matthes 2010; Miele 2009; Oliva 2011; Rembacken 1999; Sanchez‐Morales 2019; Solovyeva 2014; Sood 2009; Tamaki 2016; Tursi 2010; Vejdani 2017; Zhang 2018a). These studies were either single‐centred (Li 2013; Miele 2009; Oliva 2011; Sanchez‐Morales 2019; Zhang 2018a), or multicentred (Kato 2004; Matthes 2010; Sood 2009; Tamaki 2016; Tursi 2010) parallel group RCTs. In two of these studies (Liu 2014; Solovyeva 2014), it was unclear whether they were single‐ or multicentred. The studies were conducted in China (Li 2013; Liu 2014; Zhang 2018a), Japan (Kato 2004; Tamaki 2016), Mexico (Sanchez‐Morales 2019), Germany (Matthes 2010), Italy (Miele 2009; Oliva 2011), UK (Rembacken 1999), Iran (Vejdani 2017) and India (Sood 2009). For two studies, it is unclear where the studies took place and therefore we have assumed this to be the authors' affiliation and included Solovyeva 2014 (Russia) and Tursi 2010 (Italy).
Participants
The average age of participants was between 12.5 years in Oliva 2011 and 47.7 years in Tursi 2010. Only three studies reported age ranges and two of these were looking at paediatric participants; 1.7 years in Miele 2009 to 18 years in Oliva 2011. The studies randomised 20 participants in Kato 2004 to 147 in Sood 2009, and had a mixture of male and females. One study did not mention the number of participants it had nor the demographics of the participants (Solovyeva 2014). All participants may or may not have been receiving medication concurrently in the studies. Five studies described the extent of disease in participants, which included proctitis, left colon involved, proctosigmoiditis and total/subcolitis (Kato 2004; Miele 2009; Sood 2009; Tamaki 2016; Tursi 2010). Two studies reported on smoking amongst participants (Matthes 2010; Sanchez‐Morales 2019). Five studies used either clinical, endoscopic, histological and/or radiological criteria to confirm that its participants had active colitis on recruitment (Kato 2004; Liu 2014; Miele 2009; Oliva 2011; Tamaki 2016). Only one study provided information that its participants had disease duration of more than five years (Oliva 2011).
Interventions
All of the included studies had two trial arms, apart from Li 2013 and Matthes 2010, with four arms. Matthes 2010 had three probiotic arms with increasing strengths and one control group. Li 2013 had one trial arm with probiotics, one with conventional treatment, one with a combination, and one control group that received nothing.
The studies investigated the following comparisons.
Probiotic versus placebo (Kato 2004; Matthes 2010; Miele 2009; Oliva 2011; Sanchez‐Morales 2019; Sood 2009; Tamaki 2016; Tursi 2010; Vejdani 2017).
Probiotic versus 5‐aminosalicylic acid (5‐ASA) (Rembacken 1999; Zhang 2018a).
Probiotic and 5‐ASA versus 5‐ASA (Liu 2014; Solovyeva 2014).
Probiotic and 5‐ASA versus 5‐ASA versus probiotic versus nothing (Li 2013).
Single strains of bacteria were tested in seven studies (Matthes 2010; Oliva 2011; Rembacken 1999; Solovyeva 2014; Tamaki 2016; Vejdani 2017; Zhang 2018a). The other seven tested multiple strains. The single strains of bacteria that were tested include Echerichia coli (E coli) strain Nissle 1917 (Matthes 2010), Lactobacillus reuteri (L reuteri) ATCC 55730 (Oliva 2011), E Coli (serotype 06:K5:H1) (Rembacken 1999), Bifidobacterium 536 (Tamaki 2016), L casei strain ATCC PTA‐3945 (Vejdani 2017), Enteroccus faecium (E faecium) L‐3 (Solovyeva 2014).
We studied the following combinations.
Six strains of Lactobacillus plantarum (L plantarum), Lactobacillus acidophilus (L acidophilus), Lactobacillus rhamnosus (L rhamnosus), Lactobacillus bifidus (L bifidus), L casei and Bifidobacterium infantis (B infantis) (Sanchez‐Morales 2019).
Bifidobacterium breve (B breve), Bifidobacterium bifidum (B bifidum) and Lactobacillus acidophilus (L acidophilus) YIT 0168 (Kato 2004).
Four strains of Lactobacillus (L paracasei, L plantarum, L acidophilus, L delbrueckii subsp bulgaricus), three strains of Bifidobacterium (B longum, B breve and B infantis), and one strain of Streptococcus salivaria (S salivaria) subsp thermophiles (Miele 2009; Sood 2009; Tursi 2010).
Four and three strains of Bifidobacterium in Zhang 2018a and Liu 2014, respectively.
Two strains of probiotic and one strain of prebiotic (Bifidobacterium (B bifidum), lactobacillus bulgaricus (L bulgaricus), streptococcus thermophilus (S thermophilus)) (Li 2013).
Interventions were administered daily for two weeks in Matthes 2010 to 52 weeks in Miele 2009. Concomitant treatments were used in nine studies (Matthes 2010; Miele 2009; Oliva 2011; Rembacken 1999; Sanchez‐Morales 2019; Sood 2009; Tamaki 2016; Tursi 2010; Vejdani 2017), and it was unclear in the other four studies if concomitant treatment was allowed. Concomitant treatment ranged from loperamide drops (Matthes 2010), gentamicin for one week (Rembacken 1999), oral 5‐ASA (Oliva 2011; Sanchez‐Morales 2019), oral 5‐ASA, azathioprine and 6‐mercaptopurine (Sood 2009; Tamaki 2016; Tursi 2010; Vejdani 2017), and/or steroid therapy (Matthes 2010; Miele 2009).
Two studies administered their probiotic therapy rectally (Matthes 2010; Oliva 2011), whilst the rest did so orally.
Outcomes
Remission was reported in 12 of the 14 studies (Kato 2004; Liu 2014; Matthes 2010; Miele 2009; Oliva 2011; Rembacken 1999; Sanchez‐Morales 2019; Solovyeva 2014; Sood 2009; Tamaki 2016; Tursi 2010; Vejdani 2017). Of the 12 studies reporting on remission, Solovyeva 2014 did not provide a definition of remission, Liu 2014 assessed remission based on the Sunderland disease activity index, and the remaining studies reported on clinical remission.
Withdrawals due to adverse events were reported in one study (Sood 2009).
Serious adverse events were reported in eight studies (Kato 2004; Liu 2014; Matthes 2010; Miele 2009; Oliva 2011; Sood 2009; Tamaki 2016; Tursi 2010).
Minor adverse events were reported in nine studies (Kato 2004; Liu 2014; Matthes 2010; Miele 2009; Sood 2009; Tamaki 2016; Tursi 2010; Vejdani 2017; Zhang 2018a).
Time to remission was reported in three studies (Matthes 2010; Rembacken 1999; Vejdani 2017).
Disease improvement was reported as improvement in clinical (Kato 2004; Sanchez‐Morales 2019), endoscopic (Tursi 2010), and histological scores (Sanchez‐Morales 2019).
Histology scores were reported in five studies (Kato 2004; Matthes 2010; Miele 2009; Oliva 2011; Sanchez‐Morales 2019).
Biochemical scores were reported in two studies (Oliva 2011; Zhang 2018a).
Steroid withdrawal, need for additional therapy, progression to therapy, clinical scores and quality of life scores were not reported in any of the studies.
Data on the above outcomes were collected and presented in Table 4.
1. Table showing outcome data.
| Study ID | Number induced | Definition of remission | Time to remission | Minor adverse events | Serious adverse events | Adverse events requiring withdrawal |
| Kato 2004 | 4/10 versus 3/10 40% versus 33% |
Absence of rectal bleeding, a rectal mucosa without erythaema, granularity, or friability and normal or near‐normal sigmoidoscopic findings | Not reported | 0/10 versus 0/10 | 0/10 versus 0/10 | 0/10 versus 1/10 |
| Matthes 2010 | 20/70 versus 2/20 49% versus 45% |
Clinical DAI ≤ 2 | Reported on graph | 37/10 versus 10/20 | 0/70 versus 0/20 | 16/70 versus 3/20 |
| Miele 2009 | 13/14 versus 4/15 93% versus 27% |
Occurrence or worsening of symptoms, accompanied by an increase in LCAI > 3, sufficient to require treatment with corticosteroids, azathioprine/immunosuppressive agents or surgery | Not reported | 0/14 versus 0/15 | 0/14 versus 0/15 | Not reported |
| Oliva 2011 | 5/20 versus 0/20 25% versus 0% |
Final DAI score < 2 points | Not reported | Not reported | 0/20 versus 0/20 | Not reported |
| Rembacken 1999 | 39/57 versus 44/59 66% versus 77% |
General well‐being with the passage of no more than three formed stools per day, a rectal mucosa without erythaema, granularity or friability as well as histological confirmation | (Mean) 42 days versus 44 days |
9/57 versus 7/59: unable to differentiate induction versus maintenance data |
0/57 versus 2/59: unable to differentiate induction versus maintenance data |
0/57 versus 2/59: unable to differentiate induction versus maintenance data |
| Tamaki 2016 | 15/28 versus 12/28 54% versus 43% |
UCDAI scores of 0‐2 | Not reported | 1/28 versus 0/28 | 0/28 versus 0/28 | 0/28 versus 0/28 |
| Vejdani 2017 | 14/17 versus 13/17 82% versus 76% |
Patient not having more than 3 well‐formed stools per day and without visible blood in the stools and any clinical symptoms of ulcerative colitis and had a clinical activity index < 4 | (Mean) 25 days versus 32 days |
4/17 versus 12/17: unable to differentiate induction versus maintenance data |
0/17 versus 0/17: unable to differentiate induction versus maintenance data |
Not reported |
| Tursi 2010 | 31/71 versus 23/73 44% versus 32% |
UCDAI score < 2 | Not reported | 8/71 versus 9/73 | 0/71 versus 0/73 | Not reported |
| Sood 2009 | 33/77 versus 11/70 43% versus 16% |
UCDAI scores not specified | Not reported | 14/77 versus 0/70 | 0/77 versus 0/73 | Unclear |
| Liu 2014 | 39/42 versus 32/42 90% versus 76% |
Based on the Suntherland disease activity index | Not reported | 0/42 versus 0/42 | 0/42 versus 0/42 | 0/42 versus 0/42 |
| Sanchez‐Morales 2019 | 1/17 versus 0/17 | Clinical remission, considered in patient without bloody diarrhoea, without tachycardia, without fever, without anaemia and normal ESR and/or CRP (provided by author via email on 17/12/2019) | Not reported | Unclear | Unclear | Unclear |
| Solovyeva 2014 | Unclear | Unclear | Unclear | Unclear | Unclear | |
| Zhang 2018a | Unclear | Unclear | Unclear | Unclear | Unclear | |
| Li 2013 | Unclear | Unclear | Unclear | Unclear | 0/20, 0/20, 0/20 |
Note: steroid withdrawal, biochemical markers of inflammation, histology scores, need for additional therapy, progression to surgery, clinical scores, and quality of life scores have not been reported in any of the studies.
DAI: disease activity index; CRP: c‐reactive protein; ESR: erythrocyte sedimentation rate; LCAI: Lichtiger colitis activity index; UCDAI: ulcerative colitis activity index;
Funding and declaration of interest
Funding was not stated for seven studies (Kato 2004; Li 2013; Matthes 2010; Sanchez‐Morales 2019; Solovyeva 2014; Vejdani 2017; Zhang 2018a). Two studies stated that they received no external sources of funding (Miele 2009; Oliva 2011). Two studies were funded by pharmaceutical industries (Sood 2009; Tursi 2010), one study by an independent foundation (Tamaki 2016), one study by a charity (Rembacken 1999), and one study was funded by several government bodies (Liu 2014).
Seven studies declared no conflicts of interest (Miele 2009; Rembacken 1999; Sanchez‐Morales 2019; Sood 2009; Tamaki 2016; Tursi 2010; Vejdani 2017). The other seven studies did not report on conflicts of interest (Kato 2004; Li 2013; Liu 2014; Matthes 2010; Oliva 2011; Solovyeva 2014; Zhang 2018a).
Excluded studies
Eleven studies failed to meet the inclusion criteria for the following reasons.
Full text article could not be found (Bataga 2015).
Induction and maintenance data presented together (Fujimori 2009).
Crohn's disease and ulcerative colitis data presented together (Ballini 2019; IRCT20120415009475N5).
Commentary piece (Turcotte 2011).
Cross‐over study that presented induction and maintenance results together (Krag 2013).
Participants had inactive disease (Bjarnason 2019).
Outcomes did not include inducing remission (Ishikawa 2003).
Not randomised (Santana 2010).
Insufficient information on study details and no response from authors when contacted (NCT00895336; NCT00374725).
Risk of bias in included studies
The studies were either at high or unclear risk of bias. The risk of bias for the studies is summarised in Figure 2 and Figure 3. Further details are available in the Characteristics of included studies table.
2.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Sequence generation
All of the included studies described their studies as random with regards to allocation of participants to intervention or control groups. The method of randomisation was adequately described in 10 studies (Kato 2004; Li 2013; Liu 2014; Matthes 2010; Miele 2009; Oliva 2011; Rembacken 1999; Sood 2009; Tursi 2010; Vejdani 2017). The remaining studies did not mention their methods of randomisation; we contacted the authors for clarification, but received no response (Sanchez‐Morales 2019; Solovyeva 2014; Zhang 2018a). There was also insufficient information on how the randomisation list was generated in Tamaki 2016.
Allocation sequence concealment
We judged this as low risk of bias for three studies (Matthes 2010; Rembacken 1999; Sood 2009). These studies described the use of central allocation (Rembacken 1999), opaque, sealed and numbered envelopes (Sood 2009), and identical interventions with specific participant numbers being used to mark delivery containers (Matthes 2010).
We judged risk of bias as unclear for 11 studies (Kato 2004; Li 2013; Liu 2014; Miele 2009; Oliva 2011; Sanchez‐Morales 2019; Solovyeva 2014; Tamaki 2016; Tursi 2010; Vejdani 2017; Zhang 2018a).
Blinding
Eight studies were described as double‐blinded (Matthes 2010; Miele 2009; Rembacken 1999; Sanchez‐Morales 2019; Sood 2009; Tamaki 2016; Tursi 2010; Vejdani 2017). However, we only judged two of the 11 studies as low risk for both performance and detection bias (Kato 2004; Miele 2009). We judged six studies as low risk for performance bias (Kato 2004; Matthes 2010; Miele 2009; Tamaki 2016; Tursi 2010; Vejdani 2017), five as unclear, due to insufficient detail (Liu 2014; Oliva 2011; Rembacken 1999; Sood 2009; Zhang 2018a), and three studies as high risk due to the intake of medication for the probiotic and control group being different (Li 2013; Sanchez‐Morales 2019; Solovyeva 2014).
For detection bias, we judged 11 studies as unclear (Liu 2014; Matthes 2010; Oliva 2011; Rembacken 1999; Sanchez‐Morales 2019;Solovyeva 2014; Sood 2009; Tamaki 2016; Tursi 2010; Vejdani 2017;Zhang 2018a).
Incomplete outcome data
Six studies were at low risk of bias for reporting data for all participants (Kato 2004; Matthes 2010; Miele 2009; Sanchez‐Morales 2019;Tamaki 2016; Tursi 2010). Four studies were unclear (Liu 2014; Rembacken 1999; Solovyeva 2014;Zhang 2018a). Four studies were at high risk of bias due to high attrition rates (Oliva 2011; Sood 2009; Vejdani 2017), and non‐reporting of outcome data for all participants in one study group (Li 2013).
Selective reporting
Trial registration was available for one study (Sood 2009), which failed to report on all prespecified outcomes. We judged four additional studies as high risk of bias for mentioning non‐significant results without reporting outcome data (Kato 2004; Matthes 2010; Tamaki 2016), and measuring outcomes without reporting them (Vejdani 2017).
We judged seven studies as low risk of bias. Six studies did not have a trial registration, but all expected outcomes were reported (Liu 2014; Miele 2009; Oliva 2011; Rembacken 1999; Sanchez‐Morales 2019; Tursi 2010). Two studies were unclear due to insufficient information (Li 2013; Solovyeva 2014).
Other potential sources of bias
We judged 10 studies as low of bias (Kato 2004; Liu 2014; Matthes 2010; Miele 2009; Oliva 2011; Solovyeva 2014; Sood 2009; Tamaki 2016; Tursi 2010; Vejdani 2017). We judged two studies as high risk of bias due to participants being classified according to disease severity and being given specific concomitant treatments, which put randomisation into question (Rembacken 1999), and imbalance in important baseline characteristics (Sanchez‐Morales 2019). We judged two studies as unclear, as no clear statement was made that the participants were equally matched in Li 2013, and Zhang 2018a failed to provide sufficient information for a judgement to be made.
Effects of interventions
See: Table 1; Table 2; Table 3
Summary of findings 1. Probiotics compared to placebo for induction of remission in ulcerative colitis.
| Probiotics compared to placebo for induction of remission in ulcerative colitis (follow‐up 2 to 52 weeks) | ||||||
| Patient or population: people with active ulcerative colitis Setting: hospital Intervention: probiotic Comparison: placebo | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with placebo | Risk with probiotic | |||||
| Clinical remission | Study population | RR 1.73 (1.19 to 2.54) | 594 (9 RCTs) | ⊕⊕⊝⊝ Lowa | Remission was defined as the absence of rectal bleeding, a rectal mucosa without erythaema, granularity, or friability and normal or near‐normal sigmoidoscopic findings (Kato 2004); clinical DAI ≤ 2 (Matthes 2010); occurrence or worsening of symptoms, accompanied by an increase in LCAI > 3, sufficient to require treatment with corticosteroids, azathioprine/immunosuppressive agents or surgery (Miele 2009); final DAI score < 2 (Oliva 2011); UCDAI scores of 0‐2 (Tamaki 2016); UCDAI score < 2 (Tursi 2010); not having more than three well‐formed stools per day and without visible blood in the stools and any clinical symptoms of ulcerative colitis and had a clinical activity index < 4 (Vejdani 2017); remission was based on UCDAI, however, no further information was provided (Sood 2009), bloody diarrhoea, without tachycardia, without fever, without anaemia and normal ESR and/or CRP (Sanchez‐Morales 2019). | |
| 252 per 1000 | 436 per 1000 (300 to 640) | |||||
| Disease improvement (based on clinical scores) | Study population | RR 2.29 (1.13 to 4.63) | 54 (2 RCTs) | ⊕⊕⊝⊝ Lowa | One additional RCT (144 participants) showed that probiotics improved disease based on endoscopic scores (RR 1.45, 95% CI 1.03 to 2.05). | |
| 259 per 1000 | 594 per 1000 (249 to 1000) | |||||
| Minor adverse events | Study population | RR 1.04 (0.42 to 2.59) | 520 (7 RCTs) | ⊕⊝⊝⊝ Very lowb | Adverse events reported were gastrointestinal disorders, unpleasant taste in the mouth, dizziness, flu‐like symptoms, acne, alopecia and dyspepsia. | |
| 133 per 1000 | 138 per 1000 (56 to 345) | |||||
| Serious adverse events | Study population | RR 0.09 (0.01 to 1.66) | 526 (7 RCTs) | ⊕⊝⊝⊝ Very lowc | Aggravated proctosigmoiditis was reported in the placebo group in one study as the only adverse event. No other study provided further details. | |
| 21 per 1000 | 2 per 1000 (0 to 35) | |||||
| Withdrawal due to adverse events | Study population | RR 0.85 (0.42 to 1.72) | 401 (4 RCTs) | ⊕⊕⊝⊝ Lowd | No study provided details on the adverse events leading to withdrawal from trial. | |
| 156 per 1000 | 133 per 1000 (66 to 268) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the mean risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; CRP: c‐reactive protein; DAI; disease activity index; ESR: erythrocyte sedimentation rate; LCAI: Lichtiger colitis activity index; RCT: randomised controlled trial; RR: risk ratio; UCDAI: ulcerative colitis disease activity index | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
aDowngraded two times for high risk of bias in most of the studies and serious imprecision due to sparse data. We did not downgrade for inconsistency (substantial heterogeneity, I2 = 66%) as effect estimates were fairly consistent across studies and heterogeneity was attributed to the differences in probiotic preparation. 2bDowngraded three times for risk of bias, very serious inconsistency (substantial heterogeneity, I2 = 69%) and very serious imprecision due to CIs which include a risk of benefit and harm. cDowngraded three times for risk of bias and very serious imprecision as CI includes a risk of benefit and harm. dDowngraded two times for very serious imprecision as CI includes a risk of benefit and harm.
Summary of findings 2. Probiotics compared to 5‐aminosalicylic acid (5‐ASA) (mesalazine) for induction of remission in ulcerative colitis.
| Probiotic compared to 5‐ASA for induction of remission in ulcerative colitis (52 weeks follow‐up; one study unclear) | ||||||
| Patient or population: people with active ulcerative colitis Setting: hospitals Intervention: probiotic Comparison: 5‐ASA | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with 5‐ASA | Risk with probiotic | |||||
| Clinical remission | Study population | RR 0.92 (0.73 to 1.16) | 116 (1 RCT) | ⊕⊕⊝⊝ Lowa | Remission was defined as general well‐being with the passage of no more than three formed stools per day, a rectal mucosa without erythaema, granularity or friability as well as histological confirmation. | |
| 746 per 1000 | 686 per 1000 (544 to 865) | |||||
| Minor adverse events | Study population | RR 1,23 (0.56 to 2.70 |
192 (2 RCTs) | ⊕⊝⊝⊝ Very lowb | Minor adverse events were abdominal pain, nausea, headache and mouth ulcer. | |
| 119 per 1000 | 158 per 1000 (63 to 395) | |||||
| Serious adverse events | Study population | RR 0.21 (0.01 to 4.22) |
116 (1 RCT) | ⊕⊝⊝⊝ Very lowb | Serious adverse events reported were perforated sigmoid diverticulum and respiratory failure in a patient with severe emphysema. | |
| 34 per 1000 | 7 per 1000 (0 to 143) |
|||||
| Withdrawal due to adverse events | Study population | RR 0.21 (0.01 to 4.22) |
116 (1 RCT) | ⊕⊝⊝⊝ Very lowb | Withdrawals were due to perforated sigmoid diverticulum and respiratory failure in a patient with severe emphysema. | |
| 34 per 1000 | 7 per 1000 (0 to 143) |
|||||
| Disease improvement | Not reported | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the mean risk in the comparison group and the relative effect of the intervention (and its 95% CI). 5‐ASA: 5‐aminosalicylates; CI: confidence interval; RCT: randomised controlled trial; RR: risk ratio. | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
aDowngraded two times for risk of other bias (participants were classified according to disease severity and given specific concomitant treatments based on this classification, this puts the randomisation into question) and serious imprecision due to small sample size in a single study. b Downgraded two times for risk of other bias; (participants were classified according to disease severity and given specific concomitant treatments based on this classification, this puts the randomisation into question) and once due to serious imprecision due to low event numbers.
Summary of findings 3. Probiotics plus 5‐aminosalicylic acid (5‐ASA) (mesalazine) compared to 5‐aminosalicylic acid (5‐ASA) (mesalazine) for induction of remission in ulcerative colitis.
| Probiotics plus 5‐ASA compared to 5‐ASA for induction of remission in ulcerative colitis (follow‐up 4 weeks to 24 months) | ||||||
| Patient or population: people with active ulcerative colitis Setting: hospitals Intervention: probiotic plus 5‐ASA Comparison: 5‐ASA | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with 5‐ASA | Risk with probiotic plus 5‐ASA | |||||
| Remission | Study population | RR 1.22 (1.01 to 1.47) | 84 (1 RCT) | ⊕⊕⊝⊝ Lowa | Remission was assessed based on the Sunderland activity score | |
| 762 per 1000 | 930 per 1000 (770 to 1000) | |||||
| Disease improvement | Not reported | |||||
| Minor adverse events | Not reported | |||||
| Serious adverse events | Not reported | |||||
| Withdrawal due to adverse events | Not reported | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the mean risk in the comparison group and the relative effect of the intervention (and its 95% CI). 5‐ASA: 5‐aminosalicylic acid; CI: confidence interval; RCT: randomised controlled trial; RR: risk ratio. | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
aDowngraded two times for unclear risk of bias in most domains and serious imprecision due to small sample size in a single study.
Probiotics versus placebo
Ten studies compared probiotics with placebo (Kato 2004; Li 2013; Matthes 2010; Miele 2009; Oliva 2011; Sanchez‐Morales 2019; Sood 2009; Tamaki 2016; Tursi 2010; Vejdani 2017). See Table 1.
Primary outcomes
Clinical remission
There is low‐certainty evidence that probiotics may improve induction of clinical remission, when compared with placebo (risk ratio (RR) 1.73, 95% confidence interval (CI) 1.19 to 2.54; 9 studies, 594 participants; I2 = 55%; random‐effects model; Analysis 1.1, number needed to treat for an additional beneficial outcome of 5). We downgraded the evidence for high risk of bias in the majority of studies and imprecision due to sparse data. We did not downgrade for inconsistency as the effect estimates appeared to be fairly consistent across studies and we judged heterogeneity to be as a result of differences in probiotic preparations.
1.1. Analysis.

Comparison 1: Probiotics versus placebo, Outcome 1: Clinical remission
Sensitivity analysis
We analysed the data using a fixed‐effect model and obtained similar, but more precise results (RR 1.78, 95% CI 1.41 to 2.25; 9 studies, 560 participants; I2 = 55%; low‐certainty evidence). Further exclusion of the studies at high risk of bias from the main analysis found that it is uncertain whether probiotics lead to a difference in clinical remission (RR 2.04, 95% CI 0.83 to 4.96; 2 studies, 71 participants; I2 = 72%; very low‐certainty evidence).
Subgroup analysis
We carried out the subgroup analysis to investigate whether age is an effect modifier. The analysis found probiotics to be beneficial in both adults (RR 1.49, 95% CI 1.07 to 2.08; 525 participants, 7 studies; I2 = 43%; very low‐certainty evidence, number needed to treat for an additional beneficial outcome of 7) and children (RR 3.83, 95% 1.69 to 8.66; 2 studies, 69 participants; I2 = 0%; low‐certainty evidence, number needed to treat for an additional beneficial outcome of 3), with a slightly greater effect in the paediatric population (test for subgroup differences: Chi² = 4.42, P = 0.04, I² = 77.4%) (Analysis 1.2, Figure 4). These results are similar to those obtained in the main analysis, but should be interpreted cautiously, given the small number of studies analysed.
1.2. Analysis.

Comparison 1: Probiotics versus placebo, Outcome 2: Clinical remission: subgroup analysis by age
4.

Forest plot of comparison: 1 Probiotics versus placebo, outcome: 1.2 Clinical remission: subgroup analysis by age.
We also assessed whether clinical remission was affected by the number of strains in probiotics. There was neither a qualitative nor quantitative difference between probiotics with multiple strains (RR 2.02, 95% CI 1.31 to 3.12; 5 studies, 374 participants; I2 = 32%) and those with single strains (RR 1.44, 95% CI 0.79 to 2.63; 4 studies, 220 participants; I2 = 57%) (Analysis 1.3). Subgroup analyses are rarely informative when there are sparse data, therefore, these results should be interpreted with caution.
1.3. Analysis.

Comparison 1: Probiotics versus placebo, Outcome 3: Clinical remission: subgroup analysis by number of strains
Histological remission
It is unclear whether probiotics lead to a difference in histological remission when compared with placebo due to very low‐certainty evidence (RR 2.50, 95% CI 0.56 to 11.16; 1 study, 34 participants). We downgraded the evidence once due to high risk of bias and twice for very serious imprecision (Analysis 1.4).
1.4. Analysis.

Comparison 1: Probiotics versus placebo, Outcome 4: Histological remission
Secondary outcomes
Disease improvement
There was improved clinical disease severity when probiotics were compared with placebo (RR 2.29, 95% CI 1.13 to 4.63; 2 studies, 54 participants; low‐certainty evidence). We downgraded the evidence once for risk of bias and once due to serious imprecision. There is moderate‐certainty evidence showing that probiotics probably reduce disease severity assessed by endoscopic scores when compared with placebo (RR 1.45, 95% CI 1.03 to 2.05; 1 study, 144 participants). We downgraded the evidence once due to imprecision due to the small number of participants. It is uncertain whether probiotics result in a difference in histological improvement when compared with placebo because the evidence is of very low certainty (RR 2.00, 95% CI 1.09 to 3.68; 1 study, 34 participants) (Analysis 1.5).
1.5. Analysis.

Comparison 1: Probiotics versus placebo, Outcome 5: Disease improvement
Steroid withdrawal
This outcome was not reported.
Clinical activity scores
Clinical activity scores were reported in one study (Miele 2009). In the probiotics and placebo groups, the mean was 10.9 versus 11.1. However, measures of variance were not reported.
Histology scores
Histology scores were reported in three studies (Kato 2004; Miele 2009; Oliva 2011). MDs ranged between ‐3.38 and ‐0.95 in the three studies (79 participants). We did not pool data due to considerable heterogeneity (I2 = 90%; Analysis 1.7). However, two studies with sufficient data consistently showed lower histology scores in the probiotics group (low‐certainty evidence).
1.7. Analysis.

Comparison 1: Probiotics versus placebo, Outcome 7: Histology scores
Biochemical markers of inflammation
Kato 2004 measured C‐reactive protein (CRP) and erythrocyte sedimentation rate (ESR), however, no data were reported. Other markers of inflammation were reported in Oliva 2011. We manually extracted the data on tumour necrosis factor (TNF)TNF ‐ α, interleukin 10 (IL‐10), interleukin 1 beta (IL‐1β) and interleukin 8 (IL‐8) from graphs, as shown in Analysis 1.8.
1.8. Analysis.

Comparison 1: Probiotics versus placebo, Outcome 8: Biochemical markers of inflammation
Need for additional therapy
This outcome was not reported.
Progression to surgery
This outcome was not reported.
Symptomatic severity (stool frequency, abdominal pain)
This outcome was reported in five studies in different ways (Matthes 2010; Miele 2009, Sood 2009; Tamaki 2016; Tursi 2010).
Matthes 2010 measured defecation frequency, occurrence of rectal bleeding, general disease activity, self‐assessments by participants and investigators, as well as global assessment of health. However, data were not shown.
Miele 2009 reported on physicians global assessment of disease and the proportion with moderate (42% versus 33%) and severe (58% versus 67%) activity of disease were reported. The mean clinical activity scores were 10.9 (14 participants) versus 11.11 (15 participants) in the probiotics and placebo groups, respectively. Measures of variance were not reported, therefore, we could not analyse this data (Analysis 1.6).
Sood 2009 reported a physician global assessment score of 0.68 (probiotics) versus 1.1 (placebo); stool frequency score 1.04 (probiotics) versus 1.66 (placebo); and rectal bleeding score 0.48 (probiotics) versus 1.01 (placebo).
Tamaki 2016 measured rectal bleeding (figures reported in text and graph were inconsistent, therefore, not presented); stool frequency (data not shown); and physicians global score (data not shown).
Tursi 2010 reported on the proportion of participants with improvement in stool frequency (48% for probiotics versus 38% for placebo); improvement of physician rating of disease activity (43% for probiotics versus 25% for placebo); and reduction of rectal bleeding (55% for probiotics versus 31% for placebo).
1.6. Analysis.

Comparison 1: Probiotics versus placebo, Outcome 6: Clinical activity scores
Quality of life scores
Matthes 2010 measured quality of life (using a visual analogue scale (VAS)), however, data were not shown.
Time to remission/improvement
Time to remission was reported in two studies (Matthes 2010; Vejdani 2017). Matthes 2010 stated that "time to remission was shorter in the 40 mL and 20 mL Escherichia coli Nissle (EcN) groups than in the 10 mL EcN and placebo groups. Vejdani 2017 reported median time to remission of 23 days and 25 days with probiotics and placebo, respectively. Data were not sufficiently reported in either study, to allow further analysis.
Minor adverse events
It is uncertain whether probiotics lead to a difference in the occurrence of minor adverse events when compared with placebo (RR 1.04, 95% CI 0.42 to 2.59; I2 = 69%; 7 studies, 520 participants; random‐effects model; Analysis 1.9). We downgraded the evidence for high risk of bias, inconsistency (I2 = 69%), and imprecision, as the CI included a risk of benefit and harm.
1.9. Analysis.

Comparison 1: Probiotics versus placebo, Outcome 9: Minor adverse events
Serious adverse events
It is uncertain whether probiotics lead to a difference in the occurrence of serious adverse events when compared with placebo (RR 0.09, CI 0.01 to 1.66; 7 studies, 526 participants; very low‐certainty evidence; Analysis 1.10, Figure 5). We downgraded the evidence for high risk of bias and imprecision, as the CI included a risk of benefit and harm.
1.10. Analysis.

Comparison 1: Probiotics versus placebo, Outcome 10: Serious adverse events
5.

Forest plot of comparison: 1 Probiotics versus placebo, outcome: 1.10 Serious adverse events.
Withdrawal due to adverse events
There is low‐certainty evidence showing that probiotics make little or no difference in the number of people needing to withdraw due to adverse events when compared with placebo (RR 0.85, CI 0.42 to 1.72; 4 studies, 401 participants; low‐certainty evidence; Analysis 1.11). We downgraded the evidence for imprecision due to wide CIs which includes a risk of benefit and harm.
1.11. Analysis.

Comparison 1: Probiotics versus placebo, Outcome 11: Withdrawal due to adverse events
Probiotics versus 5‐aminosalicylic acid (5‐ASA) (mesalazine)
Two studies compared probiotics with 5‐ASA (Li 2013; Rembacken 1999). See Table 2.
Primary outcome
Clinical remission
It is uncertain whether probiotics lead to a difference in the number of people who attain remission when compared with 5‐ASA (RR 0.92, 95% CI 0.73 to 1.16; 1 study, 116 participants; low‐certainty evidence; Analysis 2.1). We downgraded the evidence for high risk of bias and imprecision due to this being a single study with a small number of participants.
2.1. Analysis.

Comparison 2: Probiotics versus 5‐aminosalicylic acid (5‐ASA) (mesalazine), Outcome 1: Clinical remission
Secondary outcomes
Disease improvement
This outcome was not reported.
Steroid withdrawal
This outcome was not reported.
Clinical activity scores
There is low‐certainty evidence that probiotics may slightly reduce clinical activity scores compared to 5‐ASA (mean difference (MD) ‐2.07, 95% CI ‐3.22 to ‐0.92; 1 study, 76 participants; Analysis 2.2). Our confidence in the result is limited as the evidence is from a small study which reported no information to allow us to judge risk of bias in any of the domains.
2.2. Analysis.

Comparison 2: Probiotics versus 5‐aminosalicylic acid (5‐ASA) (mesalazine), Outcome 2: Clinical activity scores
Histology scores
This outcome was not reported.
Biochemical markers of inflammation
One study (76 participants) reported on the effect of probiotics compared to 5‐ASA on serum IL‐4 (MD 2.53, 95% CI 0.47 to 4.59), serum IL‐8 (MD ‐66.10, 95% CI ‐71.63 to ‐60.57) and high‐sensitivity C‐reactive protein (hs‐CRP) (MD ‐3.03, 95% CI ‐3.45 to ‐2.61). Our confidence in the result is limited as the evidence is from a small study which reported no information to allow us to judge risk of bias in any of the domains (Analysis 2.3).
2.3. Analysis.

Comparison 2: Probiotics versus 5‐aminosalicylic acid (5‐ASA) (mesalazine), Outcome 3: Biochemical markers of inflammation
Need for additional therapy
This outcome was not reported.
Progression to surgery
This outcome was not reported.
Symptomatic severity (stool frequency, abdominal pain)
This outcome was not reported.
Quality of life scores
This outcome was not reported.
Time to remission/improvement
There is low‐certainty evidence that in any given number of people receiving therapy for the induction of remission, 50% may achieve remission in less time with probiotics than placebo (37 days versus 42 days; 116 participants; reported P = 0.0092). We downgraded for high risk of bias and imprecision due to small sample size from a single study.
Minor adverse events
It is uncertain whether probiotics lead to a difference in minor adverse events because the certainty of the evidence is very low (RR 1.23, 95% CI 0.56 to 2.70; 2 studies, 192 participants; very low‐certainty evidence; Analysis 2.4). We downgraded the evidence due to high risk of bias and imprecision due to small sample size and sparse data.
2.4. Analysis.

Comparison 2: Probiotics versus 5‐aminosalicylic acid (5‐ASA) (mesalazine), Outcome 4: Minor adverse events
Serious adverse events
It is uncertain whether probiotics lead to a difference in serious adverse events because the certainty of the evidence is very low (RR 0.21, 95% CI 0.01 to 4.22; 1 study, 116 participants; very low‐certainty evidence; Analysis 2.5). We downgraded the evidence due to high risk of bias and imprecision due to small sample size and sparse data from a single study.
2.5. Analysis.

Comparison 2: Probiotics versus 5‐aminosalicylic acid (5‐ASA) (mesalazine), Outcome 5: Serious adverse events
Withdrawal due to adverse events
It is uncertain whether probiotics lead to a difference in withdrawals due to adverse events because the certainty of the evidence is very low (RR 0.21, 95% CI 0.01 to 4.22; 1 study, 116 participants; very low‐certainty evidence; Analysis 2.6). We downgraded the evidence due to high risk of bias and imprecision due to small sample size and sparse data from a single study.
2.6. Analysis.

Comparison 2: Probiotics versus 5‐aminosalicylic acid (5‐ASA) (mesalazine), Outcome 6: Withdrawal due to adverse events
Probiotics plus 5‐aminosalicylic acid (5‐ASA) (mesalazine) versus 5‐ASA (mesalazine)
Three studies compared probiotics plus 5‐ASA to 5‐ASA (Li 2013; Liu 2014; Solovyeva 2014). See Table 3.
Primary outcome
Remission (based on Sunderland disease activity scores)
There is low‐certainty evidence that probiotics, when coupled with 5‐ASA, may slightly increase the number of people who attain remission when compared with 5‐ASA alone (RR 1.22, CI 1.01 to 1.47; 1 study, 84 participants; low‐certainty evidence; Analysis 3.1). We downgraded the evidence for unclear risk of bias in most of the domains and imprecision due to small sample size of a single study.
3.1. Analysis.

Comparison 3: Probiotics plus 5‐aminosalicylic acid (5‐ASA) (mesalazine) versus 5‐ASA (mesalazine), Outcome 1: Remission (based on Sunderland disease activity index)
Secondary outcomes
Symptomatic severity (stool frequency, abdominal pain)
Clinical activity scores were reported in Solovyeva 2014. However, the number of participants randomised to each group was not stated, therefore we were unable to analyse the data. Mean scores were 4.5 (SD 1.5) versus 6.7 (SD 1.3) in 47 participants.
None of the other secondary outcomes were reported.
Discussion
Summary of main results
This review included 14 parallel group randomised controlled trials (RCTs) assessing the effectiveness of probiotics in inducing remission in ulcerative colitis. All the studies except Li 2013 provided sufficient data for inclusion in a meta‐analysis. The comparisons assessed by the studies were probiotics versus placebo, probiotics versus 5‐aminosalicylic acid (5‐ASA) and probiotics plus 5‐ASA versus 5‐ASA alone. See Table 1; Table 2; Table 3.
We analysed and summarised data from 865 participants.
Probiotics may improve induction of clinical remission when compared with placebo (low‐certainty evidence).
There may be little or no difference in the induction of remission with probiotics when compared with 5‐ASA (low‐certainty evidence).
There is limited evidence to show that probiotics plus 5‐ASA may slightly improve the induction of remission (based on the Sunderland disease activity index) when compared with 5‐ASA alone (low‐certainty evidence).
Probiotics probably reduce disease severity, based on endoscopic scores, when compared with placebo (moderate‐certainty evidence).
Probiotics may improve clinical disease severity when compared with placebo (low‐certainty evidence).
The most common minor adverse events were abdominal bloating and discomfort (very low‐certainty evidence).
All seven studies comparing probiotics with placebo, which recorded serious adverse events, reported no events occurring with probiotics (very low‐certainty evidence).
Probiotics may make little or no difference in the number of people withdrawing from treatment due to adverse events compared to placebo (low‐certainty evidence).
There were insufficient data on biochemical markers of inflammation, time to remission, symptomatic severity, histology scores and clinical activity scores.
None of the studies reported on steroid withdrawal, need for additional therapy, or quality of life scores.
Overall completeness and applicability of evidence
The range of studies analysed in this review led to heterogeneity in all aspects. This produces limitations when trying to apply a guide to decision making. When shared decision making is made by clinicians and practitioners, they need not only facts, but pragmatic and useful ways of applying those facts to their individual patients. The clinical heterogeneity in almost all areas (e.g. methods of identifying disease activity as baseline, methods of defining remission, improvement, adverse events, the huge range of individual patient demographics, the routes of administration, and specific strains of probiotics) really limits the way in which these findings can be confidently applied to individual patients.
Updating this review after almost 10 years has highlighted the growing body of evidence, but it is disappointing that these barriers to the utility of the evidence base exists. Indeed, this raises the question, as to why strategically over the years, studies have not looked to build sequentially on one another. When synthesising studies in this review, the field appears to comprise of disparate works produced in isolation of the wider clinical research field.
There is insufficient information to fully describe the relevance of the evidence due to poor reporting across the studies. None of the studies were restrictive in terms of gender or age, there were some restrictions on the severity of ulcerative colitis, as no study chose to include participants with severe disease. Apart from two studies (Miele 2009; Oliva 2011), all studies recruited adults. A formal subgroup analysis looking at age as an effect modifier, found no qualitative difference in remission between the adult and paediatric population. However, there is a quantitative difference between adults and children. When we further analysed the data by number of strains, there was neither a qualitative nor quantitative difference. Given the insufficient data these findings should be interpreted with caution. We intend to explore these subgroups in future updates when more trials become available.
Follow‐up ranged from two weeks to 52 weeks. Eight out of the 12 studies used concomitant treatment, and for a further two studies it was not clear whether concomitant treatment was allowed. This causes uncertainty in terms of attributing treatment effects or adverse events to the concomitant treatment or the study intervention itself. Rembacken 1999 also reported on adverse outcomes, however it presented its data from induction and maintenance together, which made it unclear to analyse, it also used gentamicin for one week prior to the start of the study, so it is difficult to assess whether the adverse events were caused by the intervention or prior treatment.
Six out of the 12 studies had probiotics that were directly supplied by the pharmaceutical manufacturer. For the other six studies, it was possible to search for an online retailer who sold the probiotic, however the studies themselves did not identify the source of their intervention. The probiotics used were both yogurt drinks and food supplements.
Time to remission was reported in two studies, however one study reported this as mean number of days, and the second study provided a graph, which made it unclear to derive statistical data from.
Certainty of the evidence
The certainty of the evidence ranged from moderate to very low. However, the moderate graded evidence only included one study. The main reasons for low grades of evidence were imprecision, due to small numbers, or high/unclear risk of bias. The issue with risk of bias is particularly pervasive in the field, and is a largely avoidable barrier impacting the certainty of the evidence in this review. Most of the studies failed to describe the blinding of outcome assessors adequately and also failed to adequally report on allocation concealment. Two studies mentioned that histopathologists were blinded, but failed to explicitly mention if other outcome assessors were also blinded. Two studies had to be translated into English, and one study was an abstract, which was unclear for most domains in risk of bias. Whilst it is possible that there was genuine bias within the studies, most of these sources would easily be managed through following international guidance on trial design. Similarly, poor reporting should also be easily addressed through peer review, ensuring these are addressed prior to publication. As it stands, we downgraded every outcome comparison due to the risk of bias.
The study samples ranged from 20 to 147 participants; these small numbers resulted in wide confidence intervals (CIs). Indeed, whilst some studies produced power calculations, the assumptions they used are very much out of keeping with the size of treatment effects that are seen across Cochrane Inflammatory Bowel Disease portfolios of reviews, and as such the question as to whether these studies were underpowered remains. This is once again a pervasive problem across the field.
Due to moderate and substantial heterogeneity, we downgraded for inconsistency. These inconsistencies may be explained by significant differences in clinical characteristics across the studies, however, there were insufficient data to investigate further.
There was no indirectness, as the included studies all addressed the objectives of the review, and were within the scope. The number of studies included in the meta‐analysis was insufficient to assess for publication bias (less than 10).
Potential biases in the review process
Some studies reported outcomes as proportions; in order to include the data in the analysis, we calculated the number of events. We were able to minimise errors by having two independent review authors extract the data. The review authors contacted study authors for additional information and clarifications, however some authors failed to reply. We aim to include any data which become available in future updates.
We had less than the recommended number of studies required to carry out a subgroup analysis, but still analysed the results by age to assess whether it was an effect modifier. We are aware that this can lead to type I error and have advised that the results be interpreted cautiously.
One study is only available as an abstract and a second study did not provide sufficient data. We did not explore the impact of these studies in a sensitivity analysis.
We are aware of the possible impact of industry funding on the validity of trial results. Funding form manufacturing companies or any conflicts of interests that were declared were noted in the relevant studies, but in many studies these details were simply omitted. We did not take these into account in carrying out the 'Risk of bias' assessment of the studies or GRADE assessment of the evidence.
Agreements and disagreements with other studies or reviews
There is currently no other known evidence‐based guidance or systemic review around the use of probiotics for the induction of remission in ulcerative colitis, except the previous version of the review (Mallon 2007). The European Crohn's and Colitis Organisation (ECCO) and European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPHGAN) guideline recommends the use of probiotics as add‐on therapy for adults and children with mild ulcerative colitis (Turner 2018), but not as a first‐line therapy, despite the findings and relatively low number needed to treat for an additional beneficial outcome (NNTB). Our review found evidence from one study supporting this recommendation, however, we consider it insufficient to draw conclusions on the use of probiotics as add‐on therapy. The current NICE guidelines do not recommend the use of probiotics in the conservative management of ulcerative colitis (NICE 2013). Mallon 2007 found that as a stand alone or combined therapy, probiotics led to no differences in remission rates. This was based on scant evidence from four studies. The results of the current review show that probiotics may improve remission in comparison with placebo. When combined with 5‐ASA it may slightly improve remission than 5‐ASA alone. Even though this is based on low‐certainty evidence, it changes the conclusion of the previous review, and in particular has specific implications for future research (see below).
Authors' conclusions
Implications for practice.
There is low‐certainty evidence that probiotics may induce clinical remission in active ulcerative colitis compared to placebo, with a number needed to treat for an additional beneficial outcome of 5. The certainty of the evidence means that the true effect may be substantially different from the estimate of the effect, and future research may therefore change this finding. This is due to the flaws in reporting of studies and the inclusion of inadequate numbers of study participants. There may be little or no difference in the effects of probiotics alone compared with 5‐aminosalicylic acid (5‐ASA), due to very low‐certainty evidence. There is limited evidence from a single study which failed to provide a definition of remission, that probiotics may confer a small added benefit in inducing remission when combined with 5‐ASA, over 5‐ASA alone. There is no clear difference in withdrawals due to adverse events between probiotics and placebo. This is also based on low‐certainty evidence. Minor and serious adverse events were poorly reported (very low‐certainty evidence). The applicability of the evidence in clinical practice is limited due to the heterogenous studies and this is reflected in the low to very low rating in certainty of the evidence. Commonly reported minor adverse events were abdominal bloating and discomfort. None of the studies reported any serious adverse events with probiotics.
Implications for research.
This review highlights the need for further research in this area that targets relevant clinical questions, uses appropriate and improved trial procedures, and reports in a manner that will allow future integration with this current evidence base to produce the clearer answers clinicians and patients require. There is only one trial ongoing.
In terms of trial quality, first the conception of trials must be considered. Eight studies had compared probiotics to placebo, which is not representative of current clinical practice, where patients will be on standard therapy to aid being induced. Therefore, it would be more suited for studies to compare probiotics plus standard care versus standard care alone, or indeed three‐armed trials.
The question of sample size is also a major concern, as stated above. The effect sizes reported in this review should form an appropriate source of data for future power calculations, and allow suitable sample sizes to be recruited.
As there is some limited evidence from a single trial of probiotics added to 5‐ASA therapy conferring a benefit when compared to 5‐ASA alone, this may form a natural foundation for future investigation.
The length of the studies were variable, and the time to relapse was not reported in most studies, and again these are key pragmatic questions that will support decision making from such trial data. Future studies should also consider whether they will also measure the rates of longer‐term relapse after initial induction. However, if they choose to do this, suitably lengthy follow‐up times must be used.
Adverse events were capriciously reported amongst the studies, which was a concern with our service user author. Given that the class of agent can be directly available to patients, it is important for their safety and autonomy that adverse events are graded as minor and severe, and defined in the study to aid future systematic reviews, and allow patients to make informed decisions if they choose to obtain the agent independently.
Studies should also consider the effects of different probiotics, different dosing regimens and specific patient subgroups, for example patients with severe disease who may benefit from probiotic treatment or children.
Service user involvement in the review process has brought to the forefront key issues, which are important to patients and need to be taken into account in future research. As probiotics can be available both as prescribed medical agents and food supplements direct to patients, both cohorts are recognised in the studies included. Future research may wish to explicitly state the local status of studied products as this has implications for patients in terms of availability and autonomy in considering the potential role of probiotics, in addition to efficacy and safety concerns.
What's new
| Date | Event | Description |
|---|---|---|
| 4 May 2020 | Amended | Correction: Three of the included studies in this review assessed a probiotic formulation known as VSL#3. The probiotic formulation that was assessed in these studies is now known by the generic name 'De Simone Formulation'. To the best of our knowledge, there are no randomized trials that have assessed the current product known as VSL#3 in people with UC. The current product known as VSL#3 is not the same formulation as the original product invented by Professor De Simone. De Simone Formulation is available under the brand names Visbiome in the USA and Vivomixx in the EU. |
History
Protocol first published: Issue 1, 2006 Review first published: Issue 4, 2007
| Date | Event | Description |
|---|---|---|
| 29 November 2019 | New citation required and conclusions have changed | A previous review found no evidence for probiotics (Mallon 2007), whereas this review concludes that probiotics may induce remission in ulcerative colitis and may enhance rates of remission when added to 5‐aminosalicylic acid (5‐ASA) therapy. |
| 31 October 2019 | New search has been performed | We updated searches in December 2017 and reran them in October 2019; we added 10 new studies to this update. |
| 15 May 2008 | Amended | Converted to new review format |
| 4 July 2007 | New citation required and conclusions have changed | Substantive amendment |
Acknowledgements
Andre On Chung Chu for assisting with translation and data extraction for one study.
Yuhong Yuan, Information Specialist, Cochrane Upper Gastrointestinal and Pancreatic Diseases (UGPD) for rerunning the search strategy in October 2019.
Appendices
Appendix 1. Search strategy
EMBASE
1. random$.tw.
2. factorial$.tw.
3. (crossover$ or cross over$ or cross‐over$).tw.
4. placebo$.tw.
5. single blind.mp.
6. double blind.mp.
7. triple blind.mp.
8. (singl$ adj blind$).tw.
9. (double$ adj blind$).tw.
10. (tripl$ adj blind$).tw.
11. assign$.tw.
12. allocat$.tw.
13. crossover procedure/
14. double blind procedure/
15. single blind procedure/
16. triple blind procedure/
17. randomized controlled trial/
18. or/1‐17
19. exp ulcerative colitis/
20. colitis.mp.
21. inflammatory bowel disease.mp.
22. IBD.mp.
23. UC.mp.
24. Or/19‐23
25. exp Probiotics/
26. exp Synbiotics/
27. probiotic*.tw.
28. synbiotic*.tw.
29. exp Lactobacillus/
30. lactobacill*.tw.
31. bacill*.tw.
32. exp Bifidobacterium/
33. (bifidus or bifidobacter*).tw.
34. exp Streptococcus thermophilus/
35. streptococcus thermophilus.tw.
36. streptococc*.tw.
37. exp Lactococcus/
38. lactococc*.tw.
39. Bacillus subtilis/
40. bacillus subtilis.tw.
41. exp Enterococcus/
42. exp Enterococcus faecium/ or Enterococcus faecalis/
43. exp Saccharomyces/
44. saccharomyc*.tw.
45. leuconostoc.tw.
46. pediococc*.tw.
47. bulgarian bacillus.tw.
48. (beneficial adj3 bacter*).tw.
49. (Escherichia coli or "E. coli").tw.
50. Yeast.tw.
51. (fungus or fungi).tw.
52. (VSL# 3 or VSL 3).tw.
53. Or/25‐52
54. 18 and 24 and 53
Medline
random$.tw.
factorial$.tw.
(crossover$ or cross over$ or cross‐over$).tw.
placebo$.tw.
single blind.mp.
double blind.mp.
triple blind.mp.
(singl$ adj blind$).tw.
(double$ adj blind$).tw.
(tripl$ adj blind$).tw.
assign$.tw.
allocat$.tw.
randomized controlled trial/
or/1‐13
exp ulcerative colitis/
colitis.mp.
inflammatory bowel disease.mp.
IBD.mp.
UC.mp.
Or/15‐19
exp Probiotics/
exp Synbiotics/
probiotic*.tw.
synbiotic*.tw.
exp Lactobacillus/
lactobacill*.tw.
bacill*.tw.
exp Bifidobacterium/
(bifidus or bifidobacter*).tw.
exp Streptococcus thermophilus/
streptococcus thermophilus.tw.
streptococc*.tw.
exp Lactococcus/
lactococc*.tw.
Bacillus subtilis/
bacillus subtilis.tw.
exp Enterococcus/
exp Enterococcus faecium/ or Enterococcus faecalis/
exp Saccharomyces/
saccharomyc*.tw.
leuconostoc.tw.
pediococc*.tw.
bulgarian bacillus.tw.
(beneficial adj3 bacter*).tw.
(Escherichia coli or "E. coli").tw.
Yeast.tw.
(fungus or fungi).tw.
(VSL# 3 or VSL 3).tw.
Or/21‐48
14 and 20 and 49
Cochrane CENTRAL
#1 MeSH descriptor: [Probiotics] explode all trees
#2 MeSH descriptor: [Synbiotics] explode all trees
#3 probiotic*
#4 synbiotic*
#5 MeSH descriptor: [Lactobacillus] explode all trees
#6 lactobacill*
#7 bacill*
#8 MeSH descriptor: [Bifidobacterium] explode all trees
#9 (bifidus or bifidobacter*)
#10 MeSH descriptor: [Streptococcus thermophilus] explode all trees
#11 streptococcus thermophilus
#12 streptococc*
#13 MeSH descriptor: [Lactococcus] explode all tree
#14 lactococc*
#15 MeSH descriptor: [Bacillus subtilis] explode all trees
#16 bacillus subtilis
#17 MeSH descriptor: [Enterococcus] explode all trees
#18 enterococcus faec*
#19 MeSH descriptor: [Saccharomyces] explode all trees
#20 saccharomyc*
#21 leuconostoc*
#22 pediococc*
#23 bulgarian bacillus
#24 (Escherichia coli or "E. coli").tw.
#25 Yeast.tw.
#26 (fungus or fungi).tw.
#27 Or/ #1‐ #26
#28 MeSH: [Ulcerative colitis] explode all trees
#29 UC
#30 Inflammatory bowel disease
#31 IBD
#32 #28 or #29 #30 and #31
#33 #27 and #32
The Cochrane IBD/FBD Review Specialised Trials Register
1. Probiotics and Inflammatory bowel disease
2. Probiotics and Ulcerative colitis
3. Synbiotics and Inflammatory bowel disease
4. Synbiotics and Ulcerative colitis
CINAHL
1. (TI probiotic* or AB probiotic*) OR (TI synbiotic* or AB synbiotic*) OR (TI probiotics* or AB probiotics*) OR (TI lactobacill* or AB lactobacill*) OR (TI bacill* or AB bacill*) OR (TI bifidobacter* or AB bifidobacter*) OR (TI bifidus* or AB bifidus*) OR (TI streptococc* or AB streptococc*) OR (TI lactococc* or AB lactococc*) OR (TI enterococcus* or AB enterococcus*) OR (TI saccharomyc* or AB saccharomyc*) OR (TI leuconostoc* or AB leuconostoc*) OR (TI pediococc* or AB pediococc*) OR (TI *coli or AB *coli) OR (TI yeast* or AB yeast*) OR (TI fung* or AB fung*) OR (TI VSL* or AB VSL*)
2. (TI Inflammatory bowel disease or AB Inflammatory bowel disease) OR (TI Ulcerative colitis or AB Ulcerative colitis) OR (TI UC or AB UC) OR (TI IBD or AB IBD)
3. 1 and 2
ClinicalTrials.gov
1. Probiotics and inflammatory bowel disease (37)
2. Probiotics and Ulcerative colitis (23)
3. Synbiotic and inflammatory bowel disease (3)
4. Synbiotic and Ulcerative colitis (1)
Data and analyses
Comparison 1. Probiotics versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 Clinical remission | 9 | 594 | Risk Ratio (M‐H, Random, 95% CI) | 1.73 [1.19, 2.54] |
| 1.2 Clinical remission: subgroup analysis by age | 9 | 594 | Risk Ratio (M‐H, Random, 95% CI) | 1.73 [1.19, 2.54] |
| 1.2.1 Adult population | 7 | 525 | Risk Ratio (M‐H, Random, 95% CI) | 1.49 [1.07, 2.08] |
| 1.2.2 Paediatric population | 2 | 69 | Risk Ratio (M‐H, Random, 95% CI) | 3.83 [1.69, 8.66] |
| 1.3 Clinical remission: subgroup analysis by number of strains | 9 | 594 | Risk Ratio (M‐H, Random, 95% CI) | 1.73 [1.19, 2.54] |
| 1.3.1 Single strain | 4 | 220 | Risk Ratio (M‐H, Random, 95% CI) | 1.44 [0.79, 2.63] |
| 1.3.2 Multiple strains | 5 | 374 | Risk Ratio (M‐H, Random, 95% CI) | 2.02 [1.31, 3.12] |
| 1.4 Histological remission | 1 | 34 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.50 [0.56, 11.16] |
| 1.5 Disease improvement | 3 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.5.1 Clinical improvement | 2 | 54 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.29 [1.13, 4.63] |
| 1.5.2 Endoscopic improvement | 1 | 144 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.45 [1.03, 2.05] |
| 1.5.3 Histological improvement | 1 | 34 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.00 [1.09, 3.68] |
| 1.6 Clinical activity scores | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.7 Histology scores | 3 | Std. Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.8 Biochemical markers of inflammation | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.8.1 TNF‐alpha | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.8.2 IL‐10 | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.8.3 IL‐1beta | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.8.4 IL‐8 | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.9 Minor adverse events | 7 | 520 | Risk Ratio (M‐H, Random, 95% CI) | 1.04 [0.42, 2.59] |
| 1.10 Serious adverse events | 7 | 526 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.09 [0.01, 1.66] |
| 1.11 Withdrawal due to adverse events | 4 | 401 | Risk Ratio (M‐H, Random, 95% CI) | 0.85 [0.42, 1.72] |
Comparison 2. Probiotics versus 5‐aminosalicylic acid (5‐ASA) (mesalazine).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 2.1 Clinical remission | 1 | 116 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.92 [0.73, 1.16] |
| 2.2 Clinical activity scores | 1 | 76 | Mean Difference (IV, Fixed, 95% CI) | ‐2.07 [‐3.22, ‐0.92] |
| 2.3 Biochemical markers of inflammation | 1 | 228 | Mean Difference (IV, Fixed, 95% CI) | ‐3.16 [‐3.57, ‐2.75] |
| 2.3.1 Serum IL‐4 | 1 | 76 | Mean Difference (IV, Fixed, 95% CI) | 2.53 [0.47, 4.59] |
| 2.3.2 Serum IL‐8 | 1 | 76 | Mean Difference (IV, Fixed, 95% CI) | ‐66.10 [‐71.63, ‐60.57] |
| 2.3.3 hs‐CRP | 1 | 76 | Mean Difference (IV, Fixed, 95% CI) | ‐3.03 [‐3.45, ‐2.61] |
| 2.4 Minor adverse events | 2 | 192 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.23 [0.56, 2.70] |
| 2.5 Serious adverse events | 1 | 116 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.21 [0.01, 4.22] |
| 2.6 Withdrawal due to adverse events | 1 | 116 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.21 [0.01, 4.22] |
Comparison 3. Probiotics plus 5‐aminosalicylic acid (5‐ASA) (mesalazine) versus 5‐ASA (mesalazine).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 3.1 Remission (based on Sunderland disease activity index) | 1 | 84 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.22 [1.01, 1.47] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Kato 2004.
| Study characteristics | ||
| Methods | Randomised placebo‐controlled trial Setting: multicentre, Tokyo, Japan, hospital and outpatients Study period: September 2001 to March 2003 |
|
| Participants |
Inclusion criteria: active mild to moderate UC (8 mild and 12 moderate) according to the criteria of Truelove 1955, no prednisolone for at least 1 year before starting the trial Exclusion criteria: topical or systemic steroids or antibiotics within the preceding 4 weeks Age (mean): 30.2 (probiotics) 33.7 (placebo) Sex (M/F): 5/5 (probiotic), 5/5 (placebo) Site of disease: proctitis 3, left colon involved 2, proctosigmoiditis 0, total colitis/sub 5 (probiotics) proctitis 4, left colon involved 3, proctosigmoiditis 0, total colitis/sub 3 (Placebo) Use of concurrent medication: salazosulfapyridine, aminosalicylate Treatment before study: not stated Number randomised: 10 (probiotic), 10 (placebo) Number analysed: 10 (probiotic), 9 (placebo) Postrandomisation exclusion: 1‐ worsening symptoms 2 days after trial starting |
|
| Interventions |
|
|
| Outcomes |
|
|
| Notes | Funding‐ not stated Conflicts of interests‐ not stated Contacted author 29 March 2018 ‐ no response |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comment: a random number table was used. Quote: "The 20 subjects were then randomly assigned to either the group (n = 10) receiving BFM supplementation (BFM group), or the control group (n = 10) receiving a placebo (placebo group), using a random number table" |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Delivered to the homes of BFM group members....the BFM placebo product, was delivered to the homes of placebo group members." Comment: does not state whether was adequately concealed before being given to the participants |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Placebo and intervention were similar in taste and appearance. Quote: "There was no difference in either taste or appearance between the two preparations." |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The endoscopic activity index score was first determined at the time of the procedure, based on a review of endoscopic photographs taken by experienced endoscopists, blinded to the mode of treatment[…]Histopathological inflammatory activity was assessed before and 12 weeks after starting treatment with at least four biopsy specimens taken from actively inflamed mucosa, including a rectal biopsy, with the most severe inflammation being documented by pathologists who had no knowledge of the treatment" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All reported No significant difference in attrition across study group |
| Selective reporting (reporting bias) | High risk | Quote: "There were no significant changes in routine biochemical data or urine analyses after treatment [...]. There was a slight improvement in inflammatory reaction [...], but it did not reach statistical significance" Comment: trial registration not available and non‐significant results were mentioned, but not adequately reported. |
| Other bias | Low risk | Comment: participants used in both groups were comparable. Quote: "No significant differences were found between the two groups in age, gender, extent of disease, disease severity, disease duration or treatment". No other apparent biases. |
Li 2013.
| Study characteristics | ||
| Methods | Randomised Setting: single centre, China Study period: May 2007 to June 2010 |
|
| Participants |
Inclusion criteria: diagnosis of UC, chronic recurrent or active patients Exclusion criteria: fulminant UC, infectious enteritis, ischaemic enteritis, radioactive enteritis, any UC with colorectal cancer Age (mean SD): 39 +/‐ 6 (probiotic) 32 +/‐ 8 (combination) 36 +/‐7 (olsalazine) Sex (M/F): 8/12 (probiotic), 11/9 (combination), 12/8 (olsalazine) Site of disease: not stated Use of concurrent medication: not clearly stated Treatment before study: not stated Number randomised: 20 (probiotic), 20 (combination), 20 (olsalazine), 20 (control) Number analysed: 20 (probiotic), 20 (combination), 20 (olsalazine) Postrandomisation exclusion: 0 |
|
| Interventions |
|
|
| Outcomes |
|
|
| Notes | Translated article from simple Chinese to English Funding ‐ not stated Conflicts of interest ‐ not stated Contacted author 30 August 2018 ‐ no response |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Table of random numbers used |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Different intake of medication |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Pathologist blinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Not reporting data on the control group which received no intervention/medication |
| Selective reporting (reporting bias) | Unclear risk | Trial registration not available. Insufficent information to determine whether all prespecified outcomes were reported |
| Other bias | Unclear risk | Not stated if participants matched across all groups |
Liu 2014.
| Study characteristics | ||
| Methods | Randomised, two intervention arms Setting: China, suggests single centre provincial hospital Study period: September 2010 to September 2012 |
|
| Participants |
Inclusion criteria: unclear ‐ suggests 25‐62 age, (Sutherland disease activity index was used) Exclusion criteria: not clearly stated Age (mean SD): 42.8 (4.8) (probiotics + mesalazine) 40.2 (5.2) (mesalazine) Sex (M/F): 20/22 (probiotic + mesalazine, 19/23 (mesalazine) Site of disease: not clearly stated Use of concurrent medication: not clearly stated Treatment before study: not stated Number randomised: 42 (probiotic + mesalazine), 42 (mesalazine) Number analysed: 42 (probiotic + mesalazine), 42 (mesalazine) Postrandomisation exclusion: 0 |
|
| Interventions | 3 strains of Bifidobacterium plus mesalazine, made by Dr Falk Control group: mesalazine Method: oral, 1 g 3 times/day or 2 g 2 times/day Follow‐up 8 weeks |
|
| Outcomes |
|
|
| Notes | Mandarin ‐ translated Combined treatment, DIA goes from 5.36 (+/‐ 1.01) to 1.85 (+/‐ 1.40) and control group, 5.42 (+/‐1.53) to 3.60 (+/‐1.22) P (0.043) Funding ‐ Natural National Science Foundation of China and several other national Chinese funding bodies (All public) Conflicts of interest ‐ not stated Contacted author on 16 January 2018 |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer method |
| Allocation concealment (selection bias) | Unclear risk | Contacted author, but no response |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No mention in translated text |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No mention in translated text |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No flow diagram |
| Selective reporting (reporting bias) | Low risk | All primary outcomes reported |
| Other bias | Low risk | Both groups similar No other apparent risk of biases. |
Matthes 2010.
| Study characteristics | ||
| Methods | Explorative, randomised, double‐blind, placebo‐controlled, parallel group, multicentre, phase 2, dose‐finding study Setting: multicentre, German hospital and community Study period: November 1999 to June 2002 |
|
| Participants |
Inclusion criteria: 18 to 70 years, DAI according to Sutherland disease activity index 4‐9, proctitis with inflammation beginning at the anus < 15 cm, and proctosigmoiditis with inflammation beginning at the anus up to the end of the colon sigmoideum (about 25‐30cm from anus), two confirmed prior manifestation of disease Exclusion criteria: other causes of acute proctitis/proctosigmoiditis such as infections, medical drugs, radiation, ischaemias of affected intestinal segments, and Crohns disease. A history of stool incontinence, perianal fistulae, major colonic surgery, colorectal carcinoma or stenoses. Other severe accompanying disease. Participation in other clinical trial either simultaneously or within 30 days, no medication such as oral EcN within 4 weeks prior to study, rectal treatment with steroids or aminosalicylates within 2 weeks before the study, immunosuppressants within 90 days before inclusion and antibiotics or sulphonamides during the study course. Lack of co‐operation, inadequate contraception, pregnancy or breast feeding and obesity. Age (mean SD): 40.1 +/‐ 11.7 (probiotics) 47.4 +/‐ 13.8 (placebo) Sex (M/F): 37/31 (probiotic), 12/8 (placebo) Site of disease: not stated Use of concurrent medication: loperamide drops to improve retention capacity for enemas, and oral UC maintenance treatment with aminosalicylates or steroids at a constant level for at least two weeks prior to the study Treatment before study: not stated Number randomised: 70 (probiotic), 20 (placebo) Number analysed: 68 (probiotic), 20 (placebo) Postrandomisation exclusion: 2 (probiotic) no intake of medication |
|
| Interventions | Non‐pathogenic Escherichia coli strain Nissle 1917, Argeypharm, Herdecke, Germany 10 to power of 8 micro‐organisms per mL Enema of 40 mL, 20 mL and 10 mL Placebo: enema devoid of the active substance Followed up for 2, 4 and 8 weeks |
|
| Outcomes |
|
|
| Notes | Funding ‐ not stated Declaration of conflicts ‐ not stated Contacted author 13 April 2018 ‐ no response |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | A random number table was used. Quote: "Using standard predetermined randomisation tables and the order of enrolment, patients received a randomisation number". |
| Allocation concealment (selection bias) | Low risk | Quote: "blinding of the investigator and patient was ensured by the provision of study medication identical in appearance, with a patient specific randomisation number" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Placebo controlled trial Quote: "blinding of the investigator and patient was ensured by the provision of study medication identical in appearance, with a patient specific randomisation number" |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient evidence to determine whether blinding was maintained until end of study. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Attrition rates were low and balanced across groups |
| Selective reporting (reporting bias) | High risk | Trial registration not available, however, the methods section shows that health related quality of life was measured using a 100 mm VAS. The results of this outcome were not reported. |
| Other bias | Low risk | No apparent differences between baseline characteristics of the two groups were seen. Conconimant diseases and therapies were not different between the groups. Quote: "there were no apparent differences between the study groups at baseline. Similarly, their case histories were comparable". |
Miele 2009.
| Study characteristics | ||
| Methods | Prospective, single centre, placebo‐controlled, double‐blind, 1‐year study Setting: single centre, Italy, hospital Study period: not stated |
|
| Participants |
Inclusion criteria: new diagnosis of UC, established on accepted historical, endoscopic, histologic, and/or radiologic criteria, which needed a steroid therapy to induce the remission of the disease Exclusion criteria: children who had received therapy inducing remission of UC; Children who required outpatient antibiotic therapy and/or required surgery for complications related to UC; children with documented history of allergic reaction to lactobacillus or other probiotic compound or with history of endocarditis, rheumatic valvular disease, congential cardiac malformations, or cardiac surgery; and children who had received any other probiotic bacterial supplement within the past 10 days. Age (mean SD): not stated (probiotics); not stated (placebo) Sex (M/F): 8/6 (probiotic), 8/7 (placebo) Site of disease: proctitis 0, left colon involved 5, proctosigmoiditis 4, total colitis/sub 5 (probiotics) proctitis 0, left colon involved 4, proctosigmoiditis 3, total colitis/sub 8 (placebo) Use of concurrent medication: oral methylprednisolone for 4 weeks, oral mesalamine maintenance Treatment before study: not stated Number randomised: 14 (probiotic), 15 (placebo) Number analysed: 14 (probiotic), 15 (placebo) Postrandomisation exclusion: none |
|
| Interventions | 4 strains of Lactobacillus (L Paracasei, L Planatum, L Acidophykus, L Delbrueckii subsp. bulgaricus), 3 strains of Bifidobacterium (B Londum, B Breve, and B infantis), and 1 strain of Streptococcus salivarius subsp thermophilus. 900 billion viable lyophilised bacteria, weight‐based dose Placebo: 3g of corn starch |
|
| Outcomes |
|
|
| Notes | Funding‐ states received none Conflicts of interests ‐ declared none Contaced author 23 April 2018 ‐ no response |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation scheme |
| Allocation concealment (selection bias) | Unclear risk | Randomisation codes kept by one investigator until end of study. However, it is unclear whether the investigator was involved in the study. Quote: "Randomization was performed by one blind clinical trial investigator, who kept the codes until completion of the study. None of the staff or patients had access to the randomization codes during the study." |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Intervention agent and placebo were similar. Quote: "Placebo was provided in identical bags...taste and smell of the active drugs were not readily identifiable" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Pathologist who analysed biopsy samples was blinded. Quote: "All histologic specimens were reviewed under code by a single pathologist experienced in analysing paediatric intestinal biopsies, blinded to the patients' clinical details." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There was no attrition. |
| Selective reporting (reporting bias) | Low risk | Trial registration not found, however authors report on all outcomes. |
| Other bias | Low risk | Baseline characteristics were well matched and no other sources of bias were found. |
Oliva 2011.
| Study characteristics | ||
| Methods | Prospective randomised, placebo‐controlled study Setting: single centre, Rome, Italy, hospital Study period: November 2008 to February 2011 |
|
| Participants |
Inclusion criteria: confirmed endoscopic and histological diagnosis of ulcerative proctitis/proctosigmoiditis with mild to moderate disease activity Exclusion criteria: other causes of active proctitis or proctosigmoiditis such as infections, medical drugs and CD; furthermore, patients who had received either oral or topical corticosteroids, topical aminosalicylates, antibiotics during the previous 12 weeks and immunomodulator's during the previous 20 weeks were excluded from the trial. Age (mean SD): 13 (probiotics) 12.5 (placebo) Sex (M/F): 8/6 (probiotic, 9/7(placebo) Site of disease: proctitis 3, left colon involved 2, proctosigmoiditis 0, total colitis/sub 5 (probiotics) proctitis 4, left colon involved 3, proctosigmoiditis 0, total colitis/sub 3 (placebo) Use of concurrent medication: oral mesalazine Treatment before study: chronic administration of oral mesalazine at a dose ranging from 50 mg/kg/day to 75 mg/kg/day during the last 12 weeks Number randomised: 20 (probiotic), 20 (placebo) Number analysed: 16 (probiotic), 15 (placebo) Postrandomisation exclusion: low compliance 3 (probiotic) 4 (placebo); acute infectious episode 1 (probiotic) 1 (placebo) |
|
| Interventions | 10 to the power of 10 CFU L reuteri ATCC 55730 Placebo: not stated |
|
| Outcomes |
|
|
| Notes | Funding ‐ declares none Conflicts of interests ‐ declares none Contacted author 29 March 2018 ‐ no response |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated list used. Quote: "Randomisation was performed according to a computer‐generated list by means of sequentially numbered sealed envelopes indicating their medication" |
| Allocation concealment (selection bias) | Unclear risk | The study states that they used sequentially numbered sealed envelopes indicating their medication to conceal from participants, however did not mention that the envelopes were opaque. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Study referred to as "placebo‐controlled". However, further details were not provided |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not gone into detail |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Over 20% attrition rate and ITT analysis not conducted |
| Selective reporting (reporting bias) | Low risk | Trial registration not available but all outcomes reported |
| Other bias | Low risk | Balance of baseline characteristics across both groups. No other sources of bias found. Quote: "At baseline, all patients had a moderate active UC and the two groups were comparable for the Mayo DAI." |
Rembacken 1999.
| Study characteristics | ||
| Methods | Double‐blind, double‐dummy, Setting: single centre, German Hospital Study period: not stated Only used induction data |
|
| Participants | 57 patients received probiotics, steroids and gentamicin
59 patients received mesalazine, steroids and gentamicin Inclusion criteria: 18 to 80 years, active UC (> 4 liquid stools for 7 days), erythema on sigmoidoscopy as well as histological confirmation of active UC Exclusion criteria: patients not in remission after a maximum of 12 weeks were excluded from the further trial, as was any patient who deteriorated clinically Age (mean SD): unable to differentiate Sex (M/F): unable to differentiate Site of disease: unable to differentiate data Use of concurrent medication: gentamicin 1 week Treatment before study: prednisolone and in remission for 12 weeks Number randomised: 57 (probiotic), 59 (placebo) Number analysed: 52 (probiotic), 50 (placebo) Postrandomisation exclusion: 14 ‐ withdrawn from study (no reason given) |
|
| Interventions |
E coli (serotype 06:K5:H1) Mutaflor, 2 capsules a day (2.5 x 1010) Comparison: mesalazine (Asacol formulation) 800 mg three times a day for 12 weeks Steroid type and dose were dependent upon disease severity Gentamicin 80 mg three times a day per day for 1 week after entry Follow up: 12 weeks |
|
| Outcomes |
|
|
| Notes | Funded by Sir Jules thorn trust (charity) Conflicts of interest ‐ not stated Contacted author in previous review 17 February 2015 ‐ reply received 23 February 2015 Contacted author for current review 13 April 2018 ‐ no reply received |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comment: confirmed via correspondence with author that randomisation was done centrally by independent pharmacy using software |
| Allocation concealment (selection bias) | Low risk | Comment: confirmed via correspondence with author that randomisation was done centrally by independent pharmacy using software |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Different intake of medication. Quote: "all patients....to receive either mesalazine 800 mg three times daily or a non‐pathogenic strain of E Coli at a dose of two capsules twice daily." |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No mention in text |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | States 'withdrawn' in flow diagram, but no clear reason |
| Selective reporting (reporting bias) | Low risk | Trial registration not available, however, all expected outcomes were reported |
| Other bias | High risk | Participants were classified according to disease severity and given specific concomitant treatments based on this classification, this puts the randomisation into question. Quote: "Randomisation was then stratified to ensure that the two treatment groups received the same proportion of patients with mild colitis and proctitis...." No other apparent risk of biases. |
Sanchez‐Morales 2019.
| Study characteristics | ||
| Methods | RCT, open Setting: not stated Study period: September 2014 to January 2015 |
|
| Participants |
Inclusion criteria: > 18 years, histologically‐confirmed UC, who despite their pharmacological treatment remained with mild to moderate activity of the disease (according to the Truelove and Witts scales, mild/moderate baseline UC level =12/5(probiotics), 6/11(control)) and were treated at the coloproctology service of a reference hospital Exclusion criteria: Patients with severe disease activity or concomitant cancer diagnosis, patients receiving TNF‐alpha antagonist drugs Age (mean SD): 42.6+/‐11.8 (probiotics), 53.6+/‐10.3 (control) years Sex (M/F): 12/5(probiotics), 6/11(control) Site of disease: not stated Use of concurrent medication: mesalazine (2 g/day on average, maximum dose 3 g/day) Treatment before study: not stated Number randomised: 17 (probiotics), 17 (control) Number analysed: 17 (probiotics), 17 (control) Postrandomisation exclusion: 0 |
|
| Interventions |
All participants continued to receive their conventional pharmacological treatment. Follow‐up: 3 months |
|
| Outcomes |
|
|
| Notes | The authors declared no conflict of interest. Funding not mentioned Study report written in Spanish. Google Translate was used for the translation. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomisation is mentioned but no there are not enough details to determine bias. Emailed author on the 18 December 2019 but no response received |
| Allocation concealment (selection bias) | Unclear risk | There is no mention of allocation concealment and not enough details to determine allocation bias. Emailed author on the 18 December 2019 but no response received |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | This was an open study and there is no mention of placebo and blinding of participants or personnel. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Authors mention that biopsies were interpreted by a pathologist who did not know the clinical status of the patients. However, there is no other mention of blinding of outcome assessors, and there is not enough information to determine bias. This was considered unclear risk for the outcome of clinical remission and low risk for histological remission. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Outcomes reported for all randomised patients. In the methods section authors mention that patients were excluded when they required a change in pharmacological treatment due to worsening of their illness. However, no withdrawals or discontinuations are mentioned in the results. |
| Selective reporting (reporting bias) | Low risk | Outcomes were not explicitly stated in the methods section and in their result section the authors report results on food consumption, diarrhoea frequency and blood in stools, which were not mentioned as an outcome in the methods section. However, clinical and histological outcomes, as mentioned in the methods have been reported. |
| Other bias | High risk | Age, gender and disease activity were imbalanced between the two groups |
Solovyeva 2014.
| Study characteristics | ||
| Methods |
Setting: unclear Study period: not stated |
|
| Participants |
Inclusion criteria: active moderate UC Exclusion criteria: not stated Age (mean SD): not stated Sex (M/F): not stated Site of disease: not stated Use of concurrent medication: not stated Treatment before study: not stated Number randomised: not stated Number analysed: not stated Postrandomisation exclusion: not stated |
|
| Interventions | Two treatment arms Enterococcus faecium L‐3 (3 dragees 3 times/day, oral) plus mesalazine 3 g/day Stand alone mesalazine 3 g/day |
|
| Outcomes |
|
|
| Notes | Funding: not stated Conflicts of interests: not stated Only abstract available Contacted author 23 April 2018 ‐ no response received |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Participants were reportedly randomised into groups, no further detail provided. Quote: "Patients with active moderate ulcerative colitis (47) were randomized on 2 groups." |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "patients of the first group received standard therapy by Mesalazine in a dose 3 g/day, patients of the second group received therapy by Mesalazine in a dose 3 g/day in a combination with probiotic containing Enterococcus faecium L‐3..." Comment: there is no indication of the use placebo in the standard group |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not stated |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to determine whether data were available for all participants |
| Selective reporting (reporting bias) | Unclear risk | Authors appear to have collected data on number of remissions, however, this was not clearly reported |
| Other bias | Low risk | Prior to the beginning of treatment both groups of patients were statistically comparable. Comment: baseline characteristics were probably balanced across groups and no additional biases were identified |
Sood 2009.
| Study characteristics | ||
| Methods | Multicentre, double‐blind, placebo‐controlled, randomised trial Setting: India, multicentre, tertiary care centre Study period: 5 June to 7 Aug |
|
| Participants |
Inclusion criteria: >18 with mild‐to‐moderately active UC UCDAI score 3‐9, with minimum sigmoidoscopic score of 2, extending for more than 15 cm form the anal verge with at least one previously documented attack of active disease Exclusion criteria: disease limited to the rectum, evidence of severe disease (UCDAI > 10), concurrent enteric infection, use of oral steroids within the past 4 weeks, use of antibiotics within the past 2 weeks, change in dose of oral mesalamine within the past 4 weeks, and use of rectal mesalamine or steroids within 7 days before entry into the study, patients requiring hospitalisations and imminent need for surgery, lactating and pregnant women, and those who received any investigational medicines within 3 months were excluded, patients with significant hepatic, renal, endocrine, respiratory, neurologic or cardiovascular diseases were also excluded. Age (mean SD): 39.8 (13) (probiotics) 38.3 (12.5) (placebo) Sex (M/F): 43/3 (probiotic), 45/25 (placebo) Site of disease: proctitis 0, left colon involved 21, proctosigmoiditis 38, total colitis/sub 18 (probiotics) proctitis 0, left colon involved 26, proctosigmoiditis 28, total colitis/sub 16 (placebo) Use of concurrent medication: oral mesalamine therapy (taken 4 weeks at stable dose before study entry) continued to do so, azathioprine or 6‐mercaptopurine were maintained on a stable dose for at least 3 months before entry and throughout the study Treatment before study: not stated Number randomised: 77 (probiotic), 70 (placebo) Number analysed: 55 (probiotic), 29 (placebo) Postrandomisation exclusion: 17 ‐ worsening symptoms; 18 lost to follow‐up, 28 ‐ discontinued therapy |
|
| Interventions | De Simone Formulation, containing 900 billion viable lyophilised bacteria, comprising four strains of lactobacilli (L paracasei, L Planatarum, L Acidophilus, and L delbrueckii subs bulgaricus), three strains of bifidobacteria (B longum, B breve and B infantis) and one strain of Streptococcus thermophilus, supplied by VSL pharmaceuticals, MD) 4 Sachets, oral, daily Placebo: maize powder, taken twice daily |
|
| Outcomes |
|
|
| Notes | Funded by CD Pharma India Private LT Conflicts of interests ‐ none declared Contacted author 13 April 2018 ‐ replied 24 April 2018 |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated system used for randomisation. Quote: "The random numbers were generated by computerized random number. The randomization list and numbered packing of the intervention was prepared by a person not involved in the study. Randomization was performed using permuted blocks of 10. There was a separate randomization list for each study center. Patients were randomized separately at all 3 study enters." |
| Allocation concealment (selection bias) | Low risk | Quote: "All the randomization numbers were concealed in separate envelopes and marked by patient number on the outer envelope. Randomization implementation. The randomization was performed by staff not involved with the study. The intervention was provided at each center. Patients were assigned the next serial number (corresponding to the randomization code) of the intervention.” Comment: trial registration also describes the trial as using "opaque, sealed and numbered envelopes" |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Contrary to the study report which indicates there was double‐blinding, the protocol suggests that the study might have been triple‐blinded. Sealed envelopes were used in maintaining blinding, however, it is unclear if blinding of investigators remained unbroken. Due to this inconsistency between trial registration and study, it is unclear whether outcome assessment was blinded. Quote: "The individual sealed envelope method was used to maintain blinding of the investigators and study participants" |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Contrary to the study report which indicates there was double‐blinding, the protocol suggests that the study might have been triple‐blinded. Sealed envelopes were used in maintaining blinding, however, it is unclear if blinding of investigators remained unbroken. Due to this inconsistency between trial registration and study, it is unclear whether outcome assessment was blinded. Quote: "The individual sealed envelope method was used to maintain blinding of the investigators and study participants" |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Over 40% attrition |
| Selective reporting (reporting bias) | High risk | Trial registration available (CTRI/2008/091/000076), however, not all prespecified outcomes were reported |
| Other bias | Low risk | Both groups comparable. Quote: “The demographic and clinical characteristics such as age, sex, number of previous relapses, extent of disease, and the use of steroids or immunosuppressive drugs in both groups were comparable” No other apparent risk of biases. |
Tamaki 2016.
| Study characteristics | ||
| Methods | Multicentre, double‐blinded, placebo‐controlled, randomised trial Setting: multicentre, Japan, Hospital Study period: Jan 2007 to May 2009 |
|
| Participants |
Inclusion criteria: > 18 years with mild to moderate UC (UC disease activity index (UCDAI) score 3‐9) Exclusion criteria: evidence of severe disease (UCDAI > 10, concurrent enteric infection, use of antibiotics within the past 2 weeks, change in dose of oral 5‐ASA within the past 4 weeks, and use of rectal 5‐ASA or steroids within 7 days before entry into the study. Patients requiring hospitalisations and imminent need for surgery, lactating and pregnant women, and those who received any investigational medicines within 3 months were excluded. Significant hepatic, renal, endocrine, respiratory, neurological or cardiovascular disease were also excluded. Age (mean SD): 44.9 (14.5) (probiotics) 45.5 (13.8) (placebo) Sex (M/F): 11/17 (probiotic, 16/12 (placebo) Site of disease: proctitis 0, left colon involved 17, proctosigmoiditis 10, total colitis/sub 1 (probiotics) proctitis 0, left colon involved 19, proctosigmoiditis 7, total colitis/sub 2 (placebo) Use of concurrent medication: 5‐ASA, prednisolone, azathioprine and 6‐mercaptopuirne Treatment before study: not stated Number randomised: 28 (probiotic), 28 (placebo) Number analysed: 28 (probiotic), 28 (placebo) Postrandomisation exclusion: none |
|
| Interventions | 2‐3 x 1011 freeze‐dried viable BB536 (Moringa Milk Industry Co) Placebo: dextrin Both ‐ Oral three times per day, 8 weeks |
|
| Outcomes |
|
|
| Notes | Funding ‐ Japanese society for the promotion of science 'Kakenhi' Grants‐in‐aid for scientific research Conflicts of interest ‐ none declared Contacted author 23 April 2018 ‐ no response |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Insufficient information on how list was generated. Quote: "randomisation list, randomisation number was strictly given according to the order of the patients enrolment with each patient assigned the first available number on the list." |
| Allocation concealment (selection bias) | Unclear risk | Quote: "the study product BB536 was provided in sealed plastic individual dose sachets..." However. whether these were numbered is not clear. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Placebo blinded Quote: "randomisation was carried out in a double‐blind manner using 1:1 allocation to the two groups" |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | The study was reportedly double‐blinded, however, there was insufficient information on blind outcome assessment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Attirition rate were similar across groups and ITT analysis was carried out |
| Selective reporting (reporting bias) | High risk | Quote: "In contrast, there were no significant differences in stool frequency and physician's global assessment in either group (data not shown)" Comment: trial registration not available and non‐significant results were mentioned, but not reported adequately |
| Other bias | Low risk | Groups were comparable. Quote: "No significant differences were identified in terms of demographic characteristics (mean age; sex...." No other apparent risk of biases. |
Tursi 2010.
| Study characteristics | ||
| Methods | Double‐blind, randomised, placebo‐controlled parallel study Setting: multicentre Study period: not stated |
|
| Participants |
Inclusion criteria: aged more than 18 years, diagnosis of UC established by previous colonoscopy, with consistent histology and clinical course, UC involving at least the rectosigmoid region; activity confirmed by colonoscopy at the beginning of the study, mild‐to moderate relapsing UC, defined as a UCDAI score ranging from 3‐8, symptoms (relapsing episodes) for less than 4 weeks before study entry, a minimum endoscopic score of 3 on the UCDAI at screening (mucosal appearance), use of oral 5‐ASA at least 4 weeks before study entry and a stable dose (Mesalazine at least 1.6G/day or balsalazide at 4.5 g/day) and/or use of azathioprine (at least 1.5 mg/kg/day) or 6‐mertcaptopurine (at least 1 mg/kg/day at least 3 months before study entry at a stable dose Exclusion criteria: Crohns or pouchitis, a UCDAI score greater than 8 (need for emergency surgery or the presence of severe disease), use of oral steroids within the last 4 weeks before study entry, use of antibiotics within the last 2 weeks before study entry, change in dose of oral 5‐ASA within the last 4 weeks before study entry and throughout the 8‐week study period or a change in dose of oral 6‐mercaptopurine and azathioprine drugs within the last 3 months before the study, use of rectal 5‐ASA or steroids within 1 weeks before entering the study or throughout the 8‐week study period, use of probiotic preparations either prescribed or over‐the‐counter within 2 weeks before study entry, use of Non‐steriodal anti‐inflammatory for 1 week before and throughout the 8‐week study period, significant hepatic, renal endocrine, respiratory, neurological, or cardiovascular diseases. History of severe adverse reaction or known hypersensitivity to maltose and/or silicon dioxide, patients requiring hospitalisations, use of any investigational drug and/or participation in any clinical trial within 3 months before entering this study Age (mean ± SD): 47.7 ± 14.1) (probiotics) 46.4 (14.4) (placebo) Sex (M/F): 49/22 (probiotic), 44/29 (placebo) Site of disease: proctitis 0, left colon involved 24, proctosigmoiditis 36, total colitis/sub1 (probiotics) proctitis 0, left colon involved 21, proctosigmoiditis 38, total colitis/sub 14 (placebo) Use of concurrent medication: maintenance oral 5‐ASA and/or azathioprine or 6‐mercapropurine Treatment before study: maintenance oral 5‐ASA and/or azathioprine or 6‐mercapropurine continued to do so at stable doses Number randomised: 71 (probiotic), 73 (placebo) Number analysed: 65 (probiotic), 66 (placebo) Postrandomisation exclusion: no patient was withdrawn before treatment assignment |
|
| Interventions | Probiotic: De Simone Formulation, containing 900 billion viable lyophilised bacteria, comprising four strains of lactobacilli (L paracasei, L Planatarum, L Acidophilus, and L delbrueckii subs bulgaricus), three strains of bifidobacteria (B longum, B breve and B infantis) and one strain of Streptococcus thermophilus, supplied by VSL pharmaceuticals, MD) Placebo: contains no lyophilised bacteria |
|
| Outcomes |
|
|
| Notes | Funding ‐ Sponsored by VSL pharmaceuticals Towson MD Conflicts of interest ‐ none declared Contacted author 23 April 2018 ‐ no response |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomisation used. Quote: "randomization was carried out in a double‐blind manner in blocks of four patients using 1:1 allocation to the two groups" |
| Allocation concealment (selection bias) | Unclear risk | Quote: “The study product, De Simone Formulation, was provided in plastic sealed individual dose sachets. Placebo was supplied in identical sachets.” Comment: unclear whether the sachets were sequentially numbered |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Placebo was supplied in identical sachets |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear: Quote: “The statistical analysis of all the data sets pertaining to efficacy (specifically, primary and secondary end points) and safety specifically, serious adverse events as defined by federal guidelines) has been independently performed by a biostatistician who is not employed by the corporate entity." However, there is no mention of whether the outcome assessment was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Atrition rates were similar across groups. ITT analysis applied |
| Selective reporting (reporting bias) | Low risk | Trial registration not available, however, all expected outcomes were reported |
| Other bias | Low risk | Groups comparable. Quote: “The clinical characteristics of patients in the two groups were comparable. No significant differences were identified in terms of demographic characteristics (mean age, male – female..." No other apparent risk of biases. |
Vejdani 2017.
| Study characteristics | ||
| Methods | Randomised, double‐blind, placebo‐controlled study Setting: multicentre, Iran, private practises Study period: not stated |
|
| Participants |
Inclusion criteria: newly diagnosed or recently relapsed UC, based on clinical, endoscopic, and histological findings and had a mild to moderately active UC according to Truelove and Witts criteria and clinical activity index ≥ 4 and ≥ 12 Exclusion criteria: substantial cardiac, renal or hepatic diseases, severe immunocompromised patients, existing or intended pregnancy or breast feeding, regular treatment with NSAID drugs, intestinal major operation, steroids dependency, known intolerance to sulfur‐free preparations of mesalazine, ulcerative colitis exacerbated by infectious colitis, toxic megacolon, use of antibiotic within 14 days prior to first visit for more than 1 weeks, use of corticosteroid injection within the last 30 days, use of immunosuppressive treatment within the last 90 days and use of mesalazine enema or corton enema within the last 14 days. Age (mean ± SD): not stated Sex (M/F): not stated Site of disease: not stated Use of concurrent medication: conventional medical treatment for active ulcerative colitis Treatment before study: not stated Number randomised: 17 (probiotic), 17 (placebo) Number analysed: 14 (probiotic), 13 (placebo) Postrandomisation exclusion: worsening symptoms 2 days after trial starting |
|
| Interventions |
L casei strain ATCC PTA‐3945, 5x105 live active cells Oral, 1 capsule twice daily Placebo: not gone into detail Follow‐up: 8 weeks |
|
| Outcomes |
|
|
| Notes | Funding ‐ not stated Conflicts of interests ‐ none declared Contacted author 23 April 2018 ‐ no response |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random number table used. Quote: “Randomisations were done using a random number table with odd numbers for probiotic and even numbers for placebo; randomisation was stratified according to the use of mesa lazing or sulfasalazine and to the clinical severity of disease (mild or moderate)" |
| Allocation concealment (selection bias) | Unclear risk | No information was provided on allocation concealment |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Intervention agent and placebo used were similar. Quote: “Placeboes were indistinguishable from the L casei preparation” |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | The study was reportedly double‐blinded however, there is no indication that outcome assessment was blinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Attrition rate was over 20% |
| Selective reporting (reporting bias) | High risk | Trial registration not available, however, biochemical tests were recorded both at entry, remission and relapse and not reported |
| Other bias | Low risk | Groups were comparable. Quote: "There was not a significant difference between the two groups in factors such as age, sex, disease duration and extent, smoking, education taken and clinical activity index” No other apparent risk of biases. |
Zhang 2018a.
| Study characteristics | ||
| Methods | RCT Setting: Department of Gastroenterology, Zhenjiang Huanhua Hospital Study duration: January 2013 to December 2016 |
|
| Participants | Total of 76 UC patients 38 patients in the non‐IV group (mild UC 21, severe UC 17) 38 patients in the IV group (mild UC 19, severe UC 19) Inclusion criteria
Exclusion criteria
Age (mean ± SD): 36 +/‐ 6.9 in non‐IV group; 36 +/‐ 8.9 in IV group Sex (M/F): 20/28 in non‐IV group; 22/26 in IV group Site of disease: left half colon 20, whole colon 18 in non‐IV group; left colon 18, whole colon 20 in IV group Use of concurrent medication: not stated Treatment before study: not stated Number randomised: 38 in IV group, 38 in non‐IV group Number analysed: not stated Postrandomisation exclusion: not stated |
|
| Interventions |
Follow‐up: 8 weeks |
|
| Outcomes |
|
|
| Notes | Conflict of interest and funding are not stated in the article. Author was contacted via the email provided in the article on the 18 December 2019 and we received an error message that the email was not delivered. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not discussed in the article. Author was contacted via the email provided in the article on the 18 December 2019 and we received an error message that the email was not delivered. |
| Allocation concealment (selection bias) | Unclear risk | Not discussed in the article |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not discussed in the article |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not discussed in the article |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not discussed in the article |
| Selective reporting (reporting bias) | Low risk | All stated outcomes were reported |
| Other bias | Unclear risk | Funding and conflict of interest not discussed in the article |
5‐ASA: 5 Aminosalycilic acid; BFM: bifidobacteria‐fermented milk; CD: Crohn's disease; CFU: colony forming unit; CRP: c‐reactive protein; DAI: disease activity index; EcN: escherichia coli Nissle; ESR: erythrocyte sedimentation rate; hs‐CRP: high sensitivity c‐reactive protein; IL‐4: interleukin 4; IL‐8: interleukin 8; ITT: intention to treat; IV: intervention; LCAI: Lichtiger colitis activity index; NSAIDs: non‐steroidal anti‐inflammatory drugs; RCT: randomised controlled trial; SASP: salazosulphapyridine; SD: standard deviation; UC: ulcerative colitis; UCDAI: ulcerative colitis disease activity index; VAS: visual analogue scales
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Ballini 2019 | Mixed group of UC and CD |
| Bataga 2015 | Cannot find article |
| Bjarnason 2019 | Maintenance study |
| Fujimori 2009 | Wrong comparator ‐ data for induction and remission presented together |
| IRCT20120415009475N5 | IBD patients not recruited for the purpose of inducing or maintaining remission – possibly mixed disease type and activity. Author contacted for data as trial was registered retrospectively. |
| Ishikawa 2003 | Wrong comparator ‐ not aiming for induction |
| Krag 2013 | Wrong study type: cross‐over study that presented results together for induction and remission |
| NCT00374725 | Insufficient information: emailed author with no reply |
| NCT00895336 | Insufficient information; emailed author with no reply |
| Santana 2010 | Wrong study type: patients not randomised |
| Turcotte 2011 | Wrong study type: commentary piece |
IBD: inflammatory bowel disease
Characteristics of studies awaiting classification [ordered by study ID]
Fan 2019.
| Methods | RCT, single centre Setting: The First Affiliated Hospital of Fujian Medical University Study duration: January 2015 to June 2016 |
| Participants | 40 with IBD randomised (19 control group, 21 observation group) UC total: 31, CD total: 9; UC control 15, CD IV 4; CD control 4, CD IV 5 Inclusion: confirmed IBD diagnosis with mild to moderate symptoms as per the current standards in China; no previous probiotic treatment; no allergy to drugs used in the present study; cognizance of the purpose of the present study and willingness to sign an informed consent Exclusion: severe heart, liver, kidney and other systemic diseases; pregnancy or lactation; unresponsive to medical treatment and with complications; immune system disorders Sex (M/F): 10/9 control group; 10/11 observation group Age (mean +/‐ SD): 39.97 +/‐ 8.68 control group; 42.56 +/‐ 7.58 observation group Site of disease: not stated Use of medication: not stated Length of time remission at study entry: not stated Number randomised: 40 Number assessed: not stated Postrandomisation exclusion: not stated Follow‐ up: 40 days |
| Interventions | IV: pentasa (mesalazine extended action tablet) as in the control regimen + probiotics (2 tablets Bifico once and three times a day + "a largely liquid‐based high nutrition diet" control: 1‐2 pentasa tablets once and three times a day and a maintenance dose of 1 tablet once and three times a day |
| Outcomes |
|
| Notes | Mixed: contacted author for UC data This work was supported by the Fujian Province Natural Science Fund Project The authors declare that there are no conflicts of interest |
Fang 2019.
| Methods | RCT multicentre Setting: Chunan County First People's Hospital and Taizhou Hospital Study duration: February 2016 to September 2017 |
| Participants | 84 patients with UC (42 control, 42 IV) control: 18 mild, 24 moderate; IV: 19 mild, 23 moderate Inclusion: meet the relevant diagnostic criteria for UC, confirmed by colonoscopy, barium enema, etc; course of disease ≥ 4 weeks; accompanied by persistent or recurrent diarrhoea, hemorrhagic stool with abdominal pain, acute aftermath etc; age ≥ 18 years; volunteer to participate in this study and sign informed consent Exclusion: those with allergies; combined with infectious colitis such as amoebiasis, bacterial disease, intestinal tuberculosis, chronic schistosomiasis; severe intestinal perforation, intestinal obstruction, toxic colonic dilatation etc; people with unconsciousness, serious insufficiency of important organs such as heart and kidney; people with radiation colitis, ischaemic colitis, Crohn's disease, mental illnesses, history of drug and alcohol abuse; pregnant, lactating women Sex (M/F): 26/16 control; 28/14 IV Age: 45.12 +/‐ 6.21 control; 45.13 +/‐ 6.2 IV Site of disease: whole colon 15, right half colon 19, left half colon 8 control; whole colon 16, right half colon 17, left half colon 9 Use of medication: not stated Length of time remission at study entry: not stated Number randomised: 84 Number assessed: not stated Postrandomisation exclusion: not stated Follow‐up: 2 months |
| Interventions | IV: mesalazine + gold bifid control: mesalazine only |
| Outcomes |
|
| Notes | Disease activity to be clarified. 95 versus 76% effective rate Main article in Chinese. Google translate was used for the translation. Funding and conflict of interest were not discussed in the article. |
Huang 2018.
| Methods | RCT, single centre Study duration: May 2014 to February 2018 Setting: Bai'an Affiliation Sanxia Central Hospital of Chongqing |
| Participants | Abstract: 120 UC patients (control 60, IV 60) Main text: 360 UC patients (control 180, IV 180) Inclusion: not stated Exclusion: not stated Sex (M/F): 81/99 control; 90/90 IV Age (mean +/‐ SD): 41.5 +/‐ 8.3 control; 42.2 +/‐ 9.4 IV Site of disease: not stated Use of medication: not stated Length of time remission at study entry: not stated Number randomised: 120 or 360 Number assessed: not stated Postrandomisation exclusion: not stated Follow‐ up: 8 weeks |
| Interventions | Control: mesalazine only IV: mesalazine + bifid triple viable capsules enteric‐coated tablet of mesalazine (Sunflower Group Jiamusi Luling Pharmaceutical Co. Ltd. 0.25 g/tablet, batch No.: 13001830), four tablets oral administration before meal, 3 time/day. Those in the research group would additionally take two bifid triple viable capsules (Jincheng Haisi Pharmaceutical Co. Ltd. 0.21 g/capsule, Batch No.: 13012365) prior to meal, 3 times/day |
| Outcomes |
|
| Notes | Unclear whether active or inactive UC ‐ emailed authors. Effectiveness rate = 90% versus 72% Funding and conflict of interest not discussed in the article. |
Shi 2018.
| Methods | RCT, single centre Setting: Department of Gastroenterology, Anji County People's Hospital of Huzhou City Study duration: August 2014 to November 2016 |
| Participants | 86 UC patients (43 control, 43 IV) Inclusion criteria: all who meet the diagnosis of ulcerative colitis in the "Consensus Opinions on the Diagnosis and Treatment of Inflammatory Bowel Diseases in China" formulated by the Collaborative Group of Inflammatory Bowel Diseases of the Chinese Medical Association Gastroenterology Branch Criterion, with typical clinical manifestations (diarrhoea, mucus, pus, blood, stool, etc.) and colonoscopy (continuous, diffuse distribution of ulcer surface); patients agreed to the study and signed informed consent Exclusion criteria: those who used contraindications to the study; those who had poor compliance during treatment; other reasons were not suitable for inclusion in the study. Sex (M/F): IV: 14/27; control: 17/24 Age (mean +/‐ SD): IV: 47.1+/‐4.9; control: 47.3+/‐6.2 Site of disease: not stated Use of medication: not stated Length of time remission at study entry: not stated Number randomised: 86 Number assessed: not stated Postrandomisation exclusion: not stated Follow‐up: treatment 2 months + 6 months |
| Interventions | IV: Bacillus subtilis and Enterococcus faecium + mesalazine control; mesalazine only Mesalazine enteric‐coated tablets (Sunflower Pharmacy, Chinese Medicine Standard: H19980148, (Specification: 0.25g/tablet), oral, 1 g/time, 6 h/time; the observation group was combined with the Bacillus subtilis double live enteric‐coated capsules (trade name: Mei Changan, Beijing Hanmei Pharmaceutical Co. Ltd. based on the control group). Company, National Medicine Standard: S20030087, Specification: 250 mg/capsule), 500 mg, orally, 3 times/day; two groups of patients were continuously taking medication for 2 months |
| Outcomes |
|
| Notes | Disease activity to be clarified. 93% versus 76% effective rate Article in Chinese. Google Translate was used for the translation. Funding and conflict of interest were not discussed in the article. |
Yilmaz 2019.
| Methods | RCT, single centre, prospective, open‐label Study duration: May 2015 to December 2016 |
| Participants | 45 IBD patients (25 IV, 20 control) UC = 15, CD = 10 Inclusion/exclusion: "Patients with IBD participated in the study. In the trial, CD Activity Index for CD and Truelove‐Witts scoring systems for UC were used for disease assessment scores. If the score was < 450, patients with CD were admitted to the study. If the score was higher, patients with UC were not admitted to the study. Volunteers also had to be > 18 years old. Patients with alcohol consumption > 20 g/day, allergies or intolerance to milk, antibiotic treatment within the last 1 month, column or bowel operation history up to 3 months before the start of the study, and the presence of active infection within 1 month prior to the start of the study or during the study were excluded from the study. In addition, if a patient requested to leave on his/her own will, or if kefir was not consumed continuously for 2 weeks, the trial protocol was assessed and was not approved." Sex (M/F): IV: total 13/12, UC 9/6, CD: 4/6, control: total 10/10, UC: 4/6, CD: 6/4 Age (median): IV: 33, control: 43 Site of disease: IV: UC colon 15, CD colon 1, ileum 6, colon + ileum 3; control: UC colon 10, CD ileum 10 Use of medication: not stated Length of time remission at study entry: not stated Number randomised: 45? Number assessed: 45 Postrandomisation exclusion: either 0 or 3. Authors mention 3 patients left the trial willingly, however participant and completer number are the same (n = 45) Follow‐up: 4 weeks |
| Interventions | IV: 400 mL/day kefir x 2 day Control:unclear "The control group did not consume placebo because it was not possible to prepare a control product with a similar flavor, texture, and taste as those of kefir. Ayran and yogurt were similar to kefir, but they also have Lactobacillus and can affect the microbiota results." |
| Outcomes |
|
| Notes | Disease activity not clear. 96% versus 85% effective rate The authors declare no conflict of interest and that this study has received no financial support |
Zhang 2018b.
| Methods | RCT, single centre Setting: Department of Gastroenterology, Longyou County People's Hospital, Luzhou, Zhejiang Province Study duration: October 2016 to November 2017 |
| Participants | 110 UC patients (55 control (38 UC, 17 CD); 55 observation (36 UC, 19 CD)) Inclusion: in accordance with the diagnostic criteria of the "Consensus on the diagnosis and treatment of inflammatory bowel disease in China" formulated by the Chinese Medical Association; no significant abnormalities in liver and kidney function; no other severe chronic diseases; informed consent Exclusion: severe liver and kidney diseases; intestinal diseases such as intestinal tuberculosis, Crohn's disease, intestinal tumours; hormones, 5‐aminosalicylic acid, and intestinal probiotics for nearly 4 weeks; patients with other drugs; patients who are allergic to drugs such as mesalazine, bifidobacterium quadruplex, etc.; pregnant and lactating women; patients with mental illness; patients who do not co‐operate with treatment; younger than 18 years old Sex (M/F): IV 29/26; control 32/23 Age (mean +/‐ SD): IV: 44.6+/‐5.8; control 45.3 +/‐5.5 Site of disease: not stated Use of medication: not stated Length of time remission at study entry: not stated Number randomised: Number assessed: not stated Postrandomisation exclusion: not stated Follow‐up: 2 months |
| Interventions | IV: Bifidobacterium quadruplex bacteria tablets + mesalazine Control: mesalazine Both groups were given mesalazine enteric‐coated tablets (trade name: Huidi, Manufacturer: Sunflower Pharmaceutical Group Jiamusi Luling Pharmaceutical Co., Ltd., National Medicine Standard H19980148, 0.25 g/tablet), oral, 1 g/time, 3 times/day. The observation group was given a bifidobacterium quadruple live bacteria tablets (brand name: Siliankang, manufacturer: Hangzhou Longda Xinke Biopharmaceutical Co., Ltd., National Medicine Standard) S20060010, 0.5 g/tablet), oral, 1.5 g/time, 3 times/day |
| Outcomes |
|
| Notes | Article in Chinese. Google Translate was used for the translation. Funding and conflict of interest were not discussed in the article. |
CD: Crohn's disease; IBD: inflammatory bowel disease; IV: intervention; SD: standard deviation; UC: ulcerative colitis;
Characteristics of ongoing studies [ordered by study ID]
NCT04006977.
| Study name | Multistrain probiotics reduces UC depression and anxiety scores |
| Methods | RCT, double‐blind, parallel assignment |
| Participants | 60 UC patients |
| Interventions | IV: multistrain probiotic product (DSF) Control: placebo |
| Outcomes | Primary outcome measures: reduction of anxiety and depression scores (time frame: 0 week, 8 weeks, 12 weeks, 16 weeks) reduction of anxiety and depression scores (with points as standard units) using HADS at 8 weeks and 16 weeks after randomised treatment Secondary outcome measures: clinical response (time frame: 4 weeks, 8 weeks, 12 weeks, 16 weeks) measured by a ≥ 1.5(3) point reduction in Simple Clinical Colitis Activity Index score at week 8 and 16 Clinical remission (time frame: 4 weeks, 8 weeks, 12 weeks, 16 weeks) measured by Simple Clinical Colitis Activity Index score ≤ 5(2) points at week 8 and 16 Endoscopic remission/response (time frame: 0 week, 16 weeks) measured by a Mayo endoscopic subscore of < 1 point, or at least a 1 point reduction from baseline in the endoscopy subscore at week 16 Changes in faecal‐associated microbiota following probiotic therapy (time frame: 0 week, 16 weeks); changes in faecal‐associated microbiota using 16S ribosomal RNA sequencing and changes in the metabolomic profile of the faeces following probiotic therapy (at baseline and 16 weeks) will be assessed, stratified by both change in Simple Clinical Colitis Activity Index score following probiotic therapy and randomisation. Identification of potential stressors (time frame: 0 weeks, 16 weeks). Participants will be asked to complete a modified practical and family problem list to identify 13 potential stressors. Adverse events (time frame: 4 weeks, 8 weeks, 12 weeks, 16 weeks) were assessed at week 8 and 16 by patient survey. |
| Starting date | October 2019 |
| Contact information | Prof Jie Liang liangjie@fmmu.edu.cn |
| Notes | Sponsors and collaborators: Xijing Hospital of Digestive Diseases, MENDES SA |
DSF: De Simone fomulation; HADS: hospital anxiety and depression scale; RNA: ribonucleic acid; UC: ulcerative colitis
Differences between protocol and review
In this update, we redesigned the search strategies and updated the risk of bias and GRADE in line with current Cochrane approaches.
We updated the consideration of adverse events to take into account the three key forms used across Cochrane Inflammatory Bowel Disease (minor adverse events, serious adverse events, withdrawal due to adverse events).
We also included children, who had previously been excluded.
Contributions of authors
Lakhbir Kaur took the lead in writing the review, extracted data and contacted authors; checked the quality of data extraction; analysed and interpreted data; undertook and checked quality assessment; performed statistical analysis; checked the quality of the statistical analysis; produced the first draft of the review; contributed to writing and editing the review; made an intellectual contribution to the review; and approved the final review prior to submission.
Morris Gordon performed screening of titles and abstracts and full‐text articles, data extraction and contacted authors, analysed and interpreted data; contributed to writing and editing the review; made an intellectual contribution to the review; contributed to previous versions of the review; and approved the final review prior to submission.
Patricia Baines contributed to writing and editing the review; made an intellectual contribution to the review; and approved the final review prior to submission.
Zipporah Iheozor‐Ejiofor extracted data; checked the quality of data extraction; analysed and interpreted data; checked quality assessment; checked the quality of statistical analysis; contributed to writing and editing the review; made an intellectual contribution to the review; and approved the final review prior to submission.
Vasiliki Sinopoulou made update changes to all sections of the review following peer review and repeated searches; and approved the final review.
Anthony Akobeng initiated and conceptualised the review; contributed to the previous versions of the review; and approved the final review prior to submission.
Declarations of interest
Lakhbir Kaur: none known
Morris Gordon: received travel grants from various companies to attend scientific meetings in the last three years, including Biogaia, Synergy, Tillots, Ferring and Allergan. None of these companies have had any involvement in the planning, completion, analysis or write up of this or any other reviews. This review has been completed as part of a UK funded National Institute for Health Research (NIHR) Cochrane Programme grant, with some time funded.
Patricia Baines: none known
Zipporah Iheozor‐Ejiofor: my employment at the University of Central Lancashire is funded by the National Institute for Health Research (NIHR) UK and focuses on high‐priority Cochrane Reviews in inflammatory bowel disease.
Vasilliki Sinopoulou: none known
Anthony Akobeng: none known
Edited (no change to conclusions)
References
References to studies included in this review
Kato 2004 {published data only}
- Kato K, Mizuno S, Umesaki Y, Ishii Y, Sugitani M, Imaoka A, et al. Randomized placebo-controlled trial assessing the effect of bifidobacteria-fermented milk on active ulcerative colitis. Alimentary Pharmacology & Therapeutics 2004;20(10):1133-41. [DOI] [PubMed] [Google Scholar]
Li 2013 {published data only}
- Li K, Zhang CF, Xia YH, Li Z J, Han Y. Efficacy of probiotics on ulcerative colitis and it's mechanism. Zhonghua Weichang Waike Zazhi 2013;16(4):336-9. [PubMed] [Google Scholar]
Liu 2014 {published data only}
- Liu P, Sun L, Zhang ZH, Zhang P, Zhang J. Clinical efficacy of Salofalk combined with beneficial bacteria in patients with ulcerative colitis. World Chinese Journal of Digestology 2014;22:3344-8. [Google Scholar]
Matthes 2010 {published data only}
- Matthes H, Krummernerl T, Giensch M, Wolff C, Schulze J. Clinical trial: Probiotic treatment of acute distal ulcerative colitis with rectally administered Escherichia Colu Nissle 1917. BMC Complementary and Alternative Medicine 2010;10:13. [DOI] [PMC free article] [PubMed] [Google Scholar]
Miele 2009 {published data only}
- Miele E, Pascarella F, Giannetti E, Quaglietta L, Baldassano RN, Staiano A. Effect of probiotic preparation (VSL#3) on induction and maintenance of remission in children with ulcerative colitis. American Journal of Gastroenterology 2009;104(2):437-43. [DOI] [PubMed] [Google Scholar]
Oliva 2011 {published data only}
- Olivia S, Di Nardo G, Aloi M, Falconieri P, Ferrari F, Mallardo S, et al. Rectal infusion of lactobacillus reuteri ATCC 55730 improves inflammation and down regulates mucosal pro-inflammatory cytokines in distal ulcerative colitis. Journal of Paediatric Gastroenterology and Nutrition 2011;52:E156. [Google Scholar]
Rembacken 1999 {published data only}
- Rembacken BJ, Snelling AM, Hawkey PM, Chalmers DM, Axon AT. Non-pathogenic Eshcherichia coli versus mesalazine for the treatment of ulcerative colitis: a randomized trial. Lancet 1999;354(9179):635-9. [DOI] [PubMed] [Google Scholar]
Sanchez‐Morales 2019 {published data only}
- Sánchez-Morales A, Pérez-Ayala MF, Cruz-Martínez M, Arenas-Osuna J, Ramírez-Mendoza P, Ceniceros RA, et al. Probiotics’ effectiveness on symptoms, histological features and feeding tolerance in ulcerative colitis [Efectividad de probióticos sobre síntomas, histología y tolerancia alimentaria en colitis ulcerativa]. Revista Medica del Instituto Mexicano del Seguro Social 2019;57(1):9-14. [PubMed] [Google Scholar]
Solovyeva 2014 {published data only}
- Solovyeva O. Probiotics can extend the remission of ulcerative colitis. Journal of Crohn's and Colitis 2014;8:S221. [Google Scholar]
Sood 2009 {published data only}
- Sood A, Midha V, Makharia GK, Ahuja V, Singal D, Goswami P, et al. The probiotic preparation VSL#3 induces remission in patients with mild-moderate active ulcerative colitis. Clinical Gastroenterology and Hepatology 2009;7(22):1202-9. [DOI] [PubMed] [Google Scholar]
Tamaki 2016 {published data only}
- Tamaki H, Nakase H, Inoue S, Kawanami C, Itani T, Ohana M, et al. Efficacy of probiotic treatment with Bifidobacterium longum 536 for induction of remission in active ulcerative colitis: A randomized, double-blinded, placebo-controlled multicenter trial. Digestive Endoscopy 2016;28(1):67-74. [DOI] [PubMed] [Google Scholar]
Tursi 2010 {published data only}
- Tursi A, Brandimarte G, Papa A, Giglio A, Elisei W, Giorgetti GM, et al. Treatment of relapsing mild-to-moderate ulcerative colitis with the probiotic VSL#3 as adjunctive to a standard pharmaceutical treatment: a double-blind, randomized, placebo-controlled study. American Journal of Gastroenterology 2010;105(10):2218-27. [DOI] [PMC free article] [PubMed] [Google Scholar]
Vejdani 2017 {published data only}
- Vejdani R, Bahari A, Zadeh AM, Azmi M, Ebrahimi-Daryani N, Hashtroudi AA, et al. Effects of lactobacillus casei probiotic on mild to moderate ulcerative colitis: A placebo controlled study. Indian Journal of Medical Sciences 2017;69(1):24-8. [Google Scholar]
Zhang 2018a {published data only}
- Zhang J. Effects of Bifidobacterium quadruplex live bacteria tablets on Mayo score and hs-CRP, IL-4, IL-8 in patients with mild to moderate ulcerative colitis. World Chinese Journal of Digestology 2018;26(6):373-7. [Google Scholar]
References to studies excluded from this review
Ballini 2019 {published data only}
- Ballini A, Santacroce L, Cantore S, Bottalico L, Dipalma G, Topi S, et al. Probiotics efficacy on oxidative stress values in inflammatory bowel disease: a randomized double-blinded placebo-controlled pilot study. Endocrine, Metabolic & Immune Disorders - Drug Targets 2019;19(3):373-81. [DOI] [PubMed] [Google Scholar]
Bataga 2015 {published data only}
- Bataga SM, Torok I, Macarie M, Negovan A, Botianu A. Rifaximine and probiotics in the treatment of mild relapse of left sided ulcerative colitis. European Journal of Clinical Investigation 2015;45:39-40. [Google Scholar]
Bjarnason 2019 {published data only}
- Bjarnason I, Sission G, Hayee B. A randomised, double-blind, placebo-controlled trial of a multi-strain probiotic in patients with asymptomatic ulcerative colitis and Crohn’s disease. Inflammopharmacology 2019;27:465-73. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fujimori 2009 {published data only}
- Fujimori S, Gudis K, Mitsui K, Seo T, Yonezawa M, Tanaka S, et al. A randomized controlled trial on the efficacy of symbiotic versus probiotic or prebiotic treatment to improve the quality of life in patients with ulcerative colitis. Nutrition 2009;25(5):520-5. [DOI] [PubMed] [Google Scholar]
IRCT20120415009475N5 {published data only}
- IRCT20120415009475N5. Evaluation of the effects of lyophilized Saccharomyces Boulardii capsules on quality of life and clinical outcomes in children with inflammatory bowel disease (IBD) [Evaluation of the effects of lyophilized Saccharomyces Boulardii capsules on quality of life and clinical outcomes in children with inflammatory bowel disease (IBD)]. www.irct.ir/trial/32179 Registration date 10 October 2018.
Ishikawa 2003 {published data only}
- Ishikawa H, Akedo I, Umesaki Y, Tanaka R, Imaoka, Otani T. Randomized controlled trial of the effect of bifidobacteria-fermented milk on ulcerative colitis. Journal of the American College of Nutrition 2003;22(1):56-63. [DOI] [PubMed] [Google Scholar]
Krag 2013 {published data only}
- Krag A, Munkholm P, Israelsen H, Ryberg B, Andersen KK, Bendtsen F. Profermin is efficacious in patients with active ulcerative colitis - a randomized controlled trial. Inflammatory Bowel Disease 2013;19(12):2584-92. [DOI] [PubMed] [Google Scholar]
NCT00374725 {published data only}
- NCT00374725. Treatment of ulcerative colitis with a combination of lactobacillus rhamnosus and lactobacillus acidophilus. www.clinicaltrials.gov/ct2/show/NCT00374725 (first received 11 September 2006).
NCT00895336 {published data only}
- NCT00895336. Lactobacillus GG in pediatric ulcerative colitis. clinicaltrials.gov/show/NCT00895336 (first received 8 May 2009).
Santana 2010 {published data only}
- Santana Porben S. Influence of a combination of lactobacilli and bifidobacteria upon disease activity, stool pattern and nutritional status of ulcerative colitis patients. Spanish society of parenteral and enteral nutrition 2010;25(6):971-83. [PubMed] [Google Scholar]
Turcotte 2011 {published data only}
- Turcotte JF, Huynh HQ. Treatment with the probiotic VSL#3 as an adjunctive therapy in relapsing mild-to-moderate ulcerative colitis significantly reduces ulcerative colitis disease activity. Evidence-Based Medicine 2011;16(4):108-9. [DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
Fan 2019 {published data only}
- Fan H, Du J, Liu X, Zheng WW, Zhuang ZH, Wang CD, et al. Effects of pentasa-combined probiotics on the microflora structure and prognosis of patients with inflammatory bowel disease. Turkish Journal of Gastroenterology 2019;30(8):680-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fang 2019 {published data only}
- Fang W, Qingfeng C. Effect of mesalazine combined with bifid on inflammatory response and rectal-anal dynamics in patients with ulcerative colitis. World Chinese Journal of Digestology 2018;26(10):594-600. [Google Scholar]
Huang 2018 {published data only}
- Huang M, Chen Z, Lang C, Chen J, Yang B, Xue L, et al. Efficacy of mesalazine in combination with bifid triple viable capsules on ulcerative colitis and the resultant effect on the inflammatory factors. Pakistan Journal of Pharmaceutical Sciences 2018;31(6):2891-5. [PubMed] [Google Scholar]
Shi 2018 {published data only}
- Shi XH, Tan FP, Jiang WH. Bacillus subtilis and Enterococcus faecium enteric-coated capsules combined with mesalazine for treatment of patients with ulcerative colitis: Efficacy and impact on serum levels of SOD, MDA, interleukins, and TNF-α. World Chinese Journal of Digestology 2018;26(12):748-54. [Google Scholar]
Yilmaz 2019 {published data only}
- Yilmaz İ, Dolar ME, Özpınar H. Effect of administering kefir on the changes in fecal microbiota and symptoms of inflammatory bowel disease: A randomized controlled trial. Turkish Journal of Gastroenterology 2019;30(3):242-53. [DOI] [PMC free article] [PubMed] [Google Scholar]
Zhang 2018b {published data only}
- Zhang Y, Wu M, Chen Y. Effects of adjuvant therapy with bifidobacterium quadruplex on lipid peroxidation injury indexes, inflammatory factors and immune function in patients with ulcerative colitis. World Chinese Journal of Digestology 2018;26(22):1348-54. [Google Scholar]
References to ongoing studies
NCT04006977 {published data only}
- NCT04006977. Multistrain Probiotics Reduces UC Depression and Anxiety Scores. clinicaltrials.gov/ct2/show/NCT04006977 First posted 5 July 2019.
Additional references
Cohen 2010
- Cohen RD. Systematic review: the costs of ulcerative colitis in Western countries. Alimentary Pharmaology and Therapeutics 2010;31(7):693-707. [DOI] [PubMed] [Google Scholar]
Covidence [Computer program]
- Veritas Health Innovation Covidence. Version accessed prior to 4 February 2020. Melbourne, Australia: Veritas Health Innovation.Available at covidence.org.
Cui 2004
- Cui HH, Chen CL, Wang JD, Yang YJ, Cun Y, Wu JB, et al. Effects of probiotics on intestinal mucosa of patients with ulcerative colitis. World Journal of Gastroenterology 2004;10(10):1521-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Dieleman 2003
- Dieleman LA, Goerres MS, Arends A, Sprengers D, Torrice C, Hoentjen F, et al. Lactobacillus GG prevents recurrence of colitis in HLA-B27 transgenic rats after antibiotic treatment. Gut 2003;53(3):370-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Egger 1997
- Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fabia 1993
- Fabia R, Ar'Rajab A, Johannsson ML, Willen R, Andersson R, Molin G, et al. The effect of exogenous administration of Lactobacillus reuteri R2LC and oat fiber on acetic acid-induced colitis in the rat. Scandinavian Journal of Gastroenterology 1993;28(2):155-62. [DOI] [PubMed] [Google Scholar]
Fiorino 2016
- Fiorino G. The clinical potential of etrolizumab in ulcerative colitis: hypes and hopes. Therapeutic Advances in Gastroenerology 2016;9(4):503-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
GRADEpro GDT 2015 [Computer program]
- McMaster University GRADEpro GDT: GRADEpro Guideline Development Tool. McMaster University, 2015 (developed by Evidence Prime, Inc.).Available from gradepro.org.
Higgins 2011
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Kennedy 2000
- Kennedy RJ, Hoper M, Deodhar K, Kirk SJ, Gardiner KR. Probiotic therapy fails to improve gut permeability in a hapten model of colitis. Scandinavian Journal of Gastroenterology 2000;35(12):1266-71. [DOI] [PubMed] [Google Scholar]
Kruis 1997
- Kruis W, Schutz E, Fric P, Fixa B, Judmaier G, Stolte M. Double-blind comparison of an oral Escherichia coli preparation and mesalazine in maintaining remission of ulcerative colitis. Alimentary Pharmacology and Therapeutics 1997;11(5):853-8. [DOI] [PubMed] [Google Scholar]
Kruis 2004
- Kruis W, Fric P, Pokrotnieks J, Lukas M, Fixa B, Kascak M, et al. Maintaining remission of ulcerative colitis with the probiotic Escherichia coli Nissle 1917 is as effective as with standard mesalazine. Gut 2004;53(11):1617-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
Loftus 2004
- Loftus EV Jr. Clinical epidemiology of inflammatory bowel disease: Incidence, prevalence and environmental influences. Gastroenterology 2004;126(6):1504-17. [PMID: ] [DOI] [PubMed] [Google Scholar]
Madsen 1999
- Madsen KL, Doyle JS, Jewell LD, Tavernini MM, Fedorak RN. Lactobacillus species prevents colitis in interleukin 10 gene-deficient mice. Gastroenterology 1999;116(5):1107-14. [DOI] [PubMed] [Google Scholar]
Madsen 2001
- Madsen K, Cornish A, Soper P, McKaigney C, Jijon H, Yachimec C, et al. Probiotic bacteria enhance murine and human intestinal epithelial barrier function. Gastroenterology 2001;121(3):580-91. [DOI] [PubMed] [Google Scholar]
NICE 2013
- National Institute for Health and Care Excellence. Ulcerative Colitis Mangagement in adults, children and Young people CG166. NICE 2013. [https://www.nice.org.uk/guidance/ng130/evidence/june-2013-full-guideline-pdf-6777262190]
Ong 2019
- Ong TG, Gordon M, Banks SS, Thomas MR, Akobeng AK. Probiotics to prevent infantile colic. Cochrane Database of Systematic Reviews 2019, Issue 3. [DOI: 10.1002/14651858.CD012473.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Panigrahi 2014
- Panigrahi P. Probiotics and prebiotics in neonatal necrotizing enterocolitis: New opportunities for translational research. Pathophysiology 2014;21(1):35-46. [DOI] [PubMed] [Google Scholar]
Pitkin 1999
- Pitkin RM, Branagan MA, Burmeister LF. Accuracy of data in abstracts of published research articles. JAMA 1999;281:1110-1. [DOI] [PubMed] [Google Scholar]
Review Manager 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Schultz 2002
- Schultz M, Veltkamp C, Dieleman LA, Grenther WB, Wyrick PB, Tonkonogy SL, et al. Lactobacillus plantarum 299V in the treatment and prevention of spontaneous colitis in interleukin-10-deficient mice. Inflammatory Bowel Diseases 2002;8(2):71-80. [DOI] [PubMed] [Google Scholar]
Schünemann 2011
- Schünemann H, Hill S, Guyatt G, et al. The GRADE approach and Bradford Hill's criteria for causation. Journal of Epidemiology & Community Health 2011;65:392-5. [DOI] [PubMed] [Google Scholar]
Shibolet 2002
- Shibolet O, Karmeli F, Eliakim R, Swennen E, Brigidi P, Gionchetti P, et al. Variable response to probiotics in two models of experimental colitis in rats. Inflammatory Bowel Diseases 2002;8(6):399-406. [DOI] [PubMed] [Google Scholar]
Truelove 1955
- Truelove SC, Witts LJ. Cortisone in ulcerative colitis; final report on a therapeutic trial. British medical journal 1955;2:1041. [DOI] [PMC free article] [PubMed] [Google Scholar]
Turner 2018
- Turner D, Ruemmele FM, Orlanski-Meyer E, Griffiths AM, Carpi JM, Bronsky J, et al. Management of paediatric ulcerative colitis, part 1: ambulatory care—an evidence-based guideline from European Crohn's and Colitis Organization and European Society of Paediatric Gastroenterology, Hepatology and Nutrition. Journal of Pediatric Gastroenterology and Nutrition 2018;62(2):257-91. [DOI: 10.1097/mpg.0000000000002035] [DOI] [PubMed] [Google Scholar]
Ungaro 2016
- Ungaro R, Mehandru S, Allen PB, Peyrin-Biroulet L, Colombel J-F. Ulcerative Colitis. Lancet 2017;389(10080):1756-70. [DOI] [PMC free article] [PubMed] [Google Scholar]
Zocco 2006
- Zocco MA, dal Verme LZ, Cremonini F, Piscaglia AC, Nista EC, Candelli M, et al. Efficacy of Lactobacillus GG in maintaining remission of ulcerative colitis. Alimentary Pharmacology and Therapeutics 2006;23(11):1567-74. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Mallon 2005
- Mallon P, McKay D, Kirk S, Gardiner K. Probiotics for induction of remission in ulcerative colitis. Cochrane Database of Systematic Reviews 2006, Issue 1. [DOI: 10.1002/14651858.CD005573] [DOI] [PubMed] [Google Scholar]
Mallon 2007
- Mallon PT, McKay D, Kirk SJ, Gardiner K. Probiotics for induction of remission in ulcerative colitis. Cochrane Database of Systematic Reviews 2007, Issue 4. [DOI: 10.1002/14651858.CD005573] [DOI] [PubMed] [Google Scholar]