

Abstract
Background and Aims
Despite the many known health benefits of physical activity (PA), older adults are the least active citizens in many countries. Regular PA significantly decreases the odds of functional limitation and social disengagement. However, there is a dearth of publicly funded support services for older adults. The primary objective of this study is to conduct a formative evaluation to examine the implementation of community‐driven health promotion programs for older adults in British Columbia, Canada.
Methods
The Active Aging Grant (AAG) initiative funded 30 community‐based organizations in British Columbia to design and deliver community‐driven health promotion programs for older adults, with an explicit focus on PA and social connectedness. Guided by the Framework for Successful Implementation, we recruited program coordinators and participants and used semistructured interview guides to focus on design, delivery, and experience within the program. Framework analysis was used with NVivo 11.
Results
Thirty‐six in‐depth, semistructured interviews were conducted in 2017, after program completion. Data saturation was achieved after interviewing 10 coordinators and 26 program participants from seven of the organizations. Eighteen were female; nine were male; 68% fell in the age range of 65‐84. We detail the innovation characteristics, provider characteristics, and contextual factors that facilitate and impede program implementation. Aspects that facilitate implementation include that they promote PA, foster social connectedness, and address isolation and loneliness; personal accountability; affordability; program design; providers' appropriate skills; community collaborations; and transportation support. Aspects that hinder implementation include lack of resources for marketing and communications, lack of volunteers and dedicated staff, and access to transportation. We also highlight two themes that emerged outside the theoretical framework, the roles of gender and funding in program implementation.
Conclusions
As part of a formative evaluation, the information will help adapt and enhance implementation of a larger scale‐out intervention aimed to increase PA and social connectedness amongst older adults in British Columbia, Canada.
Keywords: physical activity, social connectedness, community‐based service sector
1. INTRODUCTION
Despite the many known health benefits of physical activity (PA),1 older adults are the least active citizens globally.2 Regular PA significantly decreases the odds of functional limitation, including “mobility‐disability”3 and social disengagement.4 These broad‐sweeping physical and social health benefits are crucial to maintain older adult independence. The quality and quantity of a person's social relationships are also strongly linked to mental health, morbidity, and mortality.5 When older adults are socially isolated, they are at an increased risk of loneliness,6 cognitive decline, depression, physical inactivity, and falling.7, 8, 9
Notwithstanding the importance of opportunities for older adults to be physically active and socially connected, there is a dearth of publicly funded support services for older adults, particularly in Canada.10 This is in part due to the decline of centrally supported services11 and increased demands on the community‐based service sector (CBSS). CBSS organizations (operated primarily by nongovernmental organizations) are increasingly tasked with delivering health promotion programs within very limited budgets.10, 12
In addition to a dearth of programs, only 3% of PA interventions are ever put into practice in the community.13 That is, few are effectively implemented, evaluated, and scaled‐up.14 With the exception of two recent evidence reviews,15, 16 which demonstrate the positive impact of community‐based PA interventions in a general population, little is known about how to implement and, ultimately, scale up community‐based programs for older adults. However, recent work by McKay et al.,17 and McKay, Sims‐Gould, Nettlefold, Hoy, & Bauman18 has shown that a partner‐based health promotion intervention can be effectively implemented across settings to enhance PA, mobility, and social connectedness in older adults.
This study is part of a formative evaluation that will build off the work by McKay, Sims‐Gould, Nettlefold, Hoy, & Bauman18 and McKay et al.17 and inform a larger scale‐out of community‐driven PA and social connectedness programs for older adults in rural and remote regions of British Columbia, Canada, and with marginalized older adults in urban settings. Formative evaluations provide critical insight as to barriers and enablers that can then be used to improve implementation in a specific context and with a specific population.19, 20, 21 Results can then be used to adapt interventions for scale‐up and scale‐out to context and population and in so doing, enhance the likelihood of sustaining the intervention.22, 23 We define scale‐up as “the process by which health interventions shown to be efficacious on a small scale and or under controlled conditions are expanded under real world conditions into broader policy or practice”.14 We define scale‐out as the “deliberate use of strategies to implement, test, improve, and sustain an evidence‐based intervention as it is delivered to new populations and/or through new delivery systems”.24
The primary objective of this study is to examine implementation of community‐driven health promotion programs aimed to increase PA and social connectedness for older adults in remote and rural regions across British Columbia.
1.1. CONTEXT OF THE CURRENT STUDY
In 2015, British Columbia's Ministry of Health released its PA strategy (Active People, Active Places: A PA Action Plan for BC; http://www.health.gov.bc.ca/library/publications/year/2015/active-people-active-places-web-2015.pdf, accessed on November, 2019), where older adults are identified as a priority area. To address this priority, the Ministry entered into a partnership with the Active Aging Research Team (AART; comprised of university‐based researchers and highly qualified support staff; http://www.activeagingrt.ca). AART undertook a number of province‐wide initiatives to support implementation of programs to increase older adults' PA and social connectedness in community settings (McKay et al.17). Among them, there was a signature initiative called Choose to Move (McKay et al.17) and a grant program called Active Aging Grants (AAGs). In this study, we focus on AAG, conducted in a partnership between AART and United Way of the Lower Mainland (UWLM). AAGs seek to support community‐driven health promotion programs that aim to increase PA and social connectedness of older adults.
1.2. Frameworks that guide implementation of programs for older adults
Implementation science is broadly defined as the use of methods and strategies to promote the uptake of interventions that have proven effective in research and practice, with the aim of improving population health. Implementation frameworks commonly examine barriers and facilitators to implementation and the interdependency across multiple levels of influence, as described within socioecological models of behavior change.22, 25 Ultimately, multilevels and multisectors,26, 27 collaborative partnerships, ongoing stakeholder interactions,28 and defined progression through stages of implementation29 are key to scaled and sustained implementation.30 In this formative evaluation, we are guided by the Framework for Successful Implementation (Figure 1). The Framework for Successful Implementation embeds elements of the Interactive Systems Framework (ISF)25 deemed essential for implementation.
Figure 1.
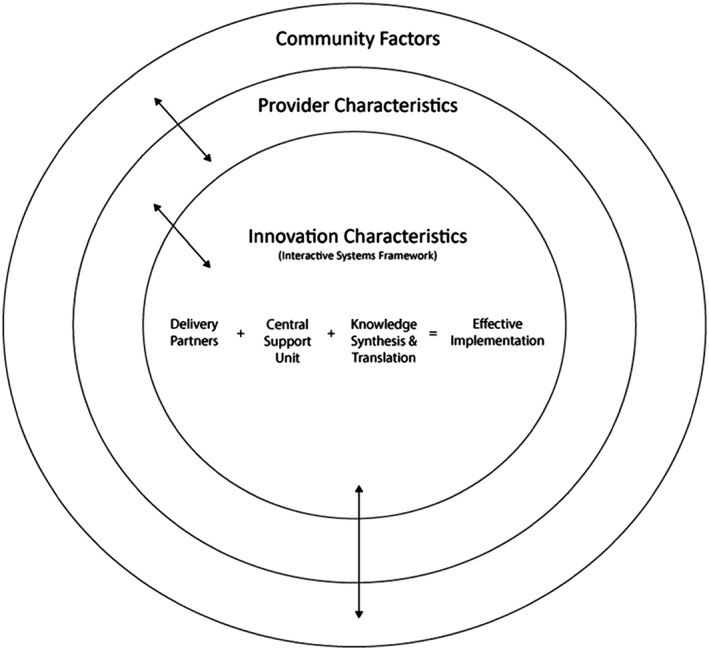
Framework for successful implementation. The framework for successful implementation that we present, integrates elements from Wandersman's interactive systems framework.25 Specifically, we pull the three specific systems which are deemed essential for effective implementation: The delivery system (which implements innovations in the world of practice), prevention support system (which provides training, technical assistance or other support to users in the field), and knowledge synthesis and translation system (which distills information about innovations and translates it into user‐friendly formats). Within the framework we present, we denote these systems as features of the innovation, or “innovation characteristics.” Arrows represent interaction across contextual levels in which the innovation operates
At the core of the Framework for Successful Implementation is the “innovation” (or intervention). The innovation can take the form of a specific program, policy, or process, or can be shaped around general consensus on knowledge considered meritorious for inclusion in health promotion efforts.25
The Framework for Successful Implementation describes three key systems that drive successful implementation—delivery, support, and research systems. In our study, the delivery system was comprised of delivery partners, whereby AART struck a project team who collaborated with UWLM to actively support organizations in receipt of AAGs. UWLM was the steward of funds for awardees and oversaw operations of the grant funding agreement. Grant recipients and their staff (ie, coordinators), with guidance from the project team, designed and delivered the AAG program. Coordinators oversaw the delivery of programs at local sites.
The project team also served as the “central” support system. In this role, they facilitated all aspects of AAG‐funded projects. Specifically, in collaboration with those in receipt of AAGs, the project team guided recipients toward integrating a PA piece into their projects, liaised continuously with communities, evaluated progress, and addressed challenges. The research system (also called knowledge synthesis and translation system) works to “distill information generated through research and to prepare it for implementation in the field.”25 ,p.175 In this role, the project team, in close collaboration with community partners, adopted a knowledge to action framework.31 Briefly, we synthesized knowledge to design the intervention, adapted the innovation for context, supported implementation, evaluated effectiveness (implementation and impact), adapted the innovation based on evaluation outcomes, supported implementation of the adapted model, and so on. Finally, the Framework for Successful Implementation contends that successful implementation of the innovation resides within the influence of provider characteristics (ie, whether the organization perceives a need for the innovation and its potential benefits and whether they have the skills and training to deliver it), and community factors (ie, organizational policies, political, and social climates).
2. METHODS
AAG recipients were small‐scale health and social societies or small municipalities located in urban, suburban, rural, and remote areas across British Columbia (Table 1). AAG recipients had direct reach to older adults in their jurisdictions.
Table 1.
Programs and the physical and social activities of the funded Active Aging Grants from the 2016‐2017 year
| City/town | Physical and social activities offered | # Seniors in program |
|---|---|---|
| Hope | A walk and roll group (a “walking” group for those with nonlimited and limited mobility), coordinating dance/movement and Garden Club activities, swim programs, exercise programs, among others | 33 |
| Aggasi | Preprogram and postprogram mobility assessments; biweekly Tai‐Chi classes | 20 |
| Invermere | Walking club, gardening club, dance and social events, and monthly health education workshops | 166 |
| Creston | Adult day program for seniors with memory changes and their caregivers, with walking and group‐based exercises; therapeutic activation program for seniors with exercise classes, peer support, and referral to community programs | 70 |
| Kelowna, Peachland | Waking group and Osteo‐Fit classes | 122 |
| Quarda Island | Indoor walking group, chair exercise classes; movement and balance training | 128 |
| Duncan | Build and maintain 2.5 acre bee‐garden; activities include lifting, walking, and socializing | No data |
| Campbell River | Group‐based exercise classes and a lunch social | 142 |
| Port hardy | Games with a focus on physical activity (PA), provided by a qualified instructor | 45 |
| Victoria | PA planning and support for homebound seniors; other essential services, such as house repair and tax return supports are also provided | 424 |
| Pender Island | Meals, singing, dance, exercises, group walks, carpet bowling | No data |
| Gabriola | Exercises and yoga; movement activities aimed at reducing falls, increasing self‐confidence, and providing opportunity for social engagement | 130 |
| Vancouver | Intergenerational focus; youth supported outings where homebound seniors are encouraged to participate in community activities | 250 |
| Burnaby | Dance, Tai Chi, and walking clubs | 371 |
| Vancouver | Yoga, Qi Gong, dance, walking groups, mobility clinics, urban farming and volunteer opportunities | 285 |
| North Vancouver | Walking meetings with a support worker | 106 |
| Maple Ridge | Transportation to a nearby destination, a short walk, lunch, and other activities | 63 |
| Vancouver | Group‐based activities and workshops. Working in collaboration with nursing students and local community center | 70 |
| North Vancouver | Light exercise, massage, blood pressure checks, educational workshops, and social events | 371 |
| Vancouver | Intergenerational, aboriginal focus. Friendship and round dances taught by youth and peer volunteers; walking groups that share indigenous knowledge (ie, place names, plants); map of community resources and opportunities; intergenerational walking groups; creative movement sessions with nurse practitioners | 134 |
| Vancouver | Culturally informed PA programming, including traditional dances, exercise to cultural music, mindful walking (for frail) | 196 |
| Burnaby, Vancouver | Outdoor education focused on local plants, birds, first nations traditions, music, yoga, meditation. Intergenerational Spring Break event. Transportation provided | 126 |
| Squamish | Skill sharing and social time while pursing building projects | 63 |
| Surrey | Tai Chi, walking, cultural dance; skills for transit; registration support for recreation subsidy passes | 188 |
| Vancouver | Outings by bus with the goal reduce sedentary time at home, guided chair aerobics, group walks, gentle strength, flexibility and balance classes led by a certified fitness instructor | 115 |
| Richmond | Cross cultural, intergenerational skill sharing; organic gardening for food bank, community meals | 62 |
| Vancouver | Language education and social peer support circles to help navigate community resources and transit | 76 |
| Vancouver | Targets low‐income housing buildings; activities include, social tea time, creative movement and dance, balance and group exercises and chair workouts | 578 |
| Hixon | Walking with pedometers, fitness trainer attends establish programs, games, resource provision for PA programs | 70 |
| Prince George | Support connection to community recreation programs and transit training and navigation | 102 |
After receipt of ethics approval (H16‐03351) from the University of British Columbia, we sent a letter to AAG recipient organizations' program coordinators and participants describing the study. An invitation to participate in the study was circulated by email to all 30 AAG coordinators. Coordinators contacted the project team for more information and/or to participate in the study. The project team contacted coordinators to discuss their participation and to provide instructions regarding how best to recruit older adults enrolled in their AAG‐funded program (the program). Figure 2 illustrates the geographical location of AAG programs funded in 2016‐2017.
Figure 2.
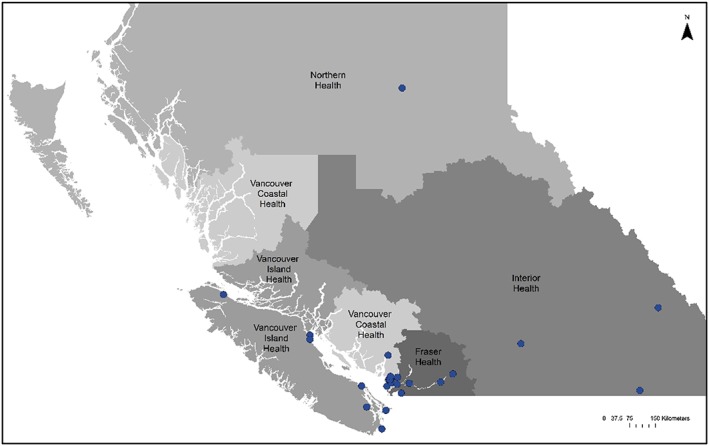
Location of the 2016‐2017 funded Active Aging Grant programs; British Columbia, Canada
Upon return of the consent forms, the project team contacted older adults and coordinators to schedule an interview. To be eligible to participate in the study, program coordinators and older adults had to speak English and provide informed consent. Older adults had to be actively participating in the program for its entire duration (from 2016 to 2017) and 65 years of age or older. Those who were unable to provide informed consent or unable to speak English were excluded from the study.
A grocery store gift card honorarium was mailed to the older adult participants ($20 CDN) and coordinators ($50 CDN) in recognition of their time. For interviews, we used a semistructured interview guide (Appendices S1 and S2). Interviews were conducted by telephone by two AART research assistants (both female) between March and June 2017, and ranged from 30 to 60 minutes in duration. Both research assistants had training in conducting qualitative interviews and had not met coordinators or participants prior to the interview. Coordinators' interview guide focused on questions related to the design, delivery, and sustainability of the program. Older adult participants' interview guide focused on questions related to their experiences within the program, with specific probes with regard to PA and social connectedness. Interviews were digitally recorded and transcribed verbatim by a professional transcription agency. For analyses, we used data from the verbatim interview transcripts. We saved interviews and progress reports using ID numbers and pseudonyms to ensure anonymity, and uploaded data into the qualitative software analysis program NVivo 11.
Annual progress reports submitted to UWLM were completed by program coordinators and collected 6 and 12 months after program launch. We analyzed reports as secondary data to verify themes from semistructured interviews. Reports included sections on reach (numbers of participants, volunteers), partnerships, organizational capacity and leveraged resources, targeted outcomes, and open fields to describe experiences.
2.1. Analysis
Transcripts were reviewed using framework analysis, an appropriate approach when the research has a predesigned sample and an a priori understanding of key issues.32 As a comprehensive method, framework analysis33 is heavily based on, and driven by, original accounts and observations, and it allows within‐case and between‐case analyses. As per the framework analysis approach, data were sifted, charted, and sorted in accordance with key issues and themed using five steps: (1) familiarize; (2) identify a thematic framework; (3) index; (4) chart; and (5) map and interpret.32, 33 Two AART staff read through the transcripts to get a sense of the interviews (familiarize), and developed preliminary thematic framework guided by the ISF. Using NVivo 11 software, staff coded interviews based on the ISF, with discussion among team members as new themes and subthemes were identified. Full paragraphs were coded so that contextual meaning was not lost. As part of the interpretive process, a series of team meetings were held to discuss the data for common themes and subthemes, and gain consensus. For comparing and contrasting themes within and across participants, we adopted the constant comparison method,34 which allowed us to discover similarities and differences in the data.
We used a number of strategies to reinforce the rigor of our analysis: crosschecking full transcripts against original audio files for quality and completeness and reflexive memoing throughout the data generation and data analysis process.35 Saturation was determined in relation to themes across participants' stories, when no new codes or themes were arising during analysis.36
3. RESULTS
Of the 30 funded AAGs, programs ranged in the number of older adults they served from 45‐250, age range was 54‐85+, with 50% of participants being between the ages of 65 and 84, and programs varied based on their context and content (see Table 1). A total of 10 coordinators and 26 program participants from seven of the 30 programs who met eligibility criteria, volunteered to participate in this formative evaluation. Eighteen were female, and nine were male. Eighteen participants (68%) fell in the age range of 65‐84.
We present themes within each of the elements of The Framework for Successful Implementation (innovation characteristics, provider characteristics, and contextual factors) (Figure 1.). Themes highlight what facilitates or impedes program implementation, according to participants and coordinators. Themes under innovation characteristics included promote PA, foster social connectedness, address isolation and loneliness, personal accountability, affordability, program design, and marketing and communication. Themes under provider characteristics included appropriate skills, and lack of volunteers and dedicated staff. Themes under contextual factors included transportation and community collaboration. We also highlight two themes that emerged outside of our theoretical framework, the roles of both gender and funding in program implementation.
3.1. Innovation characteristics
3.1.1. Promote PA
Although each organization designed its own program, the project team supported them to integrate some form of PA. Having the opportunity to engage in PA was noted by most participants as beneficial, enjoyable, and at times, life altering.
It gets you out of the house and it gets you with a group of people and usually it's an active thing that we do. …there's quite a lot of walking involved to go to different things. (Participant)
3.1.2. Foster social connectedness
Opportunities to connect socially were overwhelmingly the most dominant driver for participation in the different programs. All coordinators and participants spoke about the value of bringing together older adults from the community who normally do not have the occasion to socialize with one another.
Participants have produced a group of ten individuals who meet regularly for a meal to local restaurants. This group not only socializes regularly in the neighborhood, they also have a check‐in system with each other where if someone is not coming to the Program once or twice, they will call each other to ensure everyone is OK. These participants are individuals who live on their own and have no family or friends nearby. They completely rely on each other for any extra help or support. (Coordinator)
3.1.3. Address isolation and loneliness
Coordinators were proud of how their programs attracted participants who identified as lonely, isolated, or facing other challenges in their lives. Offering programs of this sort was seen as a “lifesaver.”
I think creating a safe space for elders to come together. So they're completely comfortable with the instructor. […] for people that have trouble getting out, so particularly those people that are less socialized, it's been really a great boon for that segment of our population. (Coordinator)
I find that I start feeling isolated if I don't get out and if I call up my friends and no, they don't want to do anything. It's nice to have something that, … I can go and do this if I choose or if something else is scheduled and, yeah, I want to go. (Participant)
3.1.4. Personal accountability
Participants identified that personal accountability was an important component of participation. Without a commitment and responsibility to themselves and the members of their groups, ongoing participation was seen as less likely to occur.
Well, as I said, it's responsibility… I feel that I'm being relied on… I'm one of the younger members. I think if it wasn't for the younger members we wouldn't have been able to do what we've done, because there's a lot of physical stuff, lifting, building… I think it's having people relying on you. Having responsibility of just participating in the whole program. (Participant)
3.1.5. Affordability
All programs were offered at no cost or low cost. Affordability was a theme noted by coordinators and participants as a key facilitator to participation, especially for those on low income. Low or no cost programs meant participants could attend on a regular basis, have opportunities to get out of their homes, get active, socialize, and in some cases, have a hot meal.
We have some people that can't afford to go on outings like this on their own, and they're very grateful for the opportunity to have a meal with their peers… They wouldn't be able to afford it and—because their income is limited. (Coordinator)
3.1.6. Program design
In general, participants were very satisfied with the design of programs. However, some provided critical feedback that could be adopted to strengthen participant interest. Suggestions included group activities instead of lectures, and alternating activities over the course of the program to accommodate a range of interests and abilities of participants.
Some coordinators noted the benefit of including older adults in the design and delivery of the programs:
The key learnings from the program is including seniors in the decision making … The purpose of their input is to help [them] feel more involved and that their opinion is important and valued. It also encourages independence and a sense of belonging. (Coordinator)
3.1.7. Marketing and communications
Coordinators spoke about their efforts to market their programs. However, having limited resources, they felt that they missed being able to share the program with the older adults in their community who could benefit most from it.
Yeah, that's a hard one, and I can't say we have totally figured out because maybe there's a whole bunch of people we're missing. And so I think the way to do it is through word of mouth. So having those seniors come and go tell their sister who's really not leaving her house about it and try to get her out to an event. So I don't know if we're doing the best job at that. We could be missing people. (Coordinator)
3.2. Provider characteristics
3.2.1. Appropriate skills
Some coordinators did not feel they had the skills to deliver the PA components of the program. They sought volunteers or partnerships with other organizations with the appropriate skill set. In many cases, these people in partner organizations were older adults.
We identified, trained and supported seniors who were already highly engaged in the community to deliver the program. We identified volunteers who had PA knowledge such as Tai‐Chi to teach the PA portion of the program. (Coordinator)
3.2.2. Lack of volunteers and dedicated staff
Lack of volunteers in some programs was a challenge. Hiring staff was often not feasible due to limited funding, therefore, coordinators relied on volunteers to help run the program. Without the volunteers in place, coordinators felt burdened and likely unable to run the program alone.
The other thing is the lack of volunteers. I found that by the end of this year, I was pretty tired. And I tried to—I don't know whether I tried to outdo myself or I tried to do too much. So I found it tiring. (Coordinator)
Programs that did well with recruitment of volunteers were often self‐sufficient and thriving.
The success of the [our] outreach program relies very heavily on teamwork amongst the volunteers. We hope to adopt an effective volunteer management system to recruit, train, evaluate, and motivate different levels of volunteers. We like to encourage and empower them to excel in their golden years. (Coordinator)
From the participant perspective, having dedicated, reliable staff was seen as essential. At times, due to coordinator burnout or scheduling conflicts, participants were left with no one to lead their program.
Well, the only thing I want to change is that—our coordinator hardly shows up. And I'd sure like her to be there every time we're there. Sometimes we don't know where she is and sometimes we don't see her for a couple days so we don't know what's going on. But we go about what we normally do. That's about it. (Participant)
3.3. Contextual factors
3.3.1. Community collaborations
All coordinators spoke about the essential role that community collaboration plays in health promoting programs. Collaborations provide in‐kind funds or offset costs for space, field trip activities, volunteers, transportation, marketing support, and materials to enrich the program content. The programs could not function solely on AAG funds, but rather depend on an assemblage of collaborations and agreements.
We have a seniors planning table in our community made up of every agency and business connected with seniors, as well as seniors themselves. So a huge resource… for connecting people up with our program and connecting our people up with [other] programs. (Coordinator)
3.3.2. Transportation
Though transportation support was a noted as a key facilitator when provided by organizations, it was also seen as an ongoing logistical and cost challenge for program delivery.
There is limited resources in our community. So we do the best to use the Parks and Leisure bus when we can. We have a couple of vans of our own, and we have volunteer drivers. (Coordinator)
In many cases, participants do not have access to transportation, and this severely limits participation, especially for more isolated and vulnerable older adults. Some AAG organizations budgeted for transportation services, such as taxis, public transit, or other community center vehicles.
Another thing, I think, that makes us unique is that we will help with transportation. If they don't have a vehicle or they're fearful of getting to the place and finding a parking spot, there are some people that say, “No, I can't go. I don't have any way of getting there.” And we tell them, “Well, we can help you with that.” And then they are able to participate. So I think transportation is huge as well. (Coordinator)
3.4. Gender
Most program participants were women, many of whom were widowed and living alone. Coordinators spoke about the importance of also attracting men to the programs. Of the men who did participate, they typically preferred to do their own activities rather than group‐based activities.
There's a few men that go, but it's—the majority is women and I think a lot of that could be because a lot of them don't have their husbands now. (Participant)
…we did not expect the enrolment of male seniors to be so low. It is commonly understood that older men tend to become more isolated as they age or become widowed; however, I did not expect the gap in enrolment to be this wide. (Coordinator)
For men who did join the program, knowing other men were participating was an important and attractive feature.
The majority are women. But there are some men that are participating, which is kind of… really neat to see. So they're kind of trickling in, and once they're in, they're finding that they're enjoying it and getting positive feedback from the men. So we're definitely encouraging that. (Coordinator)
3.5. Funding
Even with leveraged capacity and resources from collaborations and partnerships, some level of ongoing funding is required. From the perspective of the coordinators, the funding process was complex, and grants difficult to obtain. From the participant perspective, having a program that was funded ensured its affordability. This was critical to sustain participation, especially for those who are more vulnerable.
But we have no committed funding. We have some funding … for three years, and then we have to jump through hoops again. And the rest of the time we are just snooping anywhere and everywhere to find money to sustain the program. (Coordinator)
Because most seniors, as you know, we don't get a whole bunch of money. So most of us can't afford to cough up hundreds of dollars. (Participant)
4. DISCUSSION
There is clear evidence that PA and socialization are important predictors of health outcomes. However, there is little information about how to implement and, ultimately, scale‐up programs. Therefore, this formative evaluation will enhance implementation of a larger scale‐out intervention aimed to increase PA and social connectedness amongst older adults in remote and rural regions across British Columbia and with marginalized older adults in urban settings.
In the results, we describe innovation characteristics, provider characteristics, and contextual factors that were perceived to facilitate or impede program implementation, despite differences in program implementation and content (Table 1). The importance of these factors is also reflected in previous studies across sectors. For example, within the implementation science literature, it is clear that programs must be adapted to setting and population to ensure “best fit”.30, 37 This promotes successful implementation and sustainability of programs at scale‐up. Other attributes such as strong leadership, enabling local implementers, phased approach to scale‐up, an integrated approach, and an engaged community, among others, were commonly cited as key among scale‐up “leaders” in global health.30
Despite the vast range of programs offered by AAG recipients, all were tasked with integrating elements of PA and social connectedness into their programs. Importantly, regardless of the type of program implementation strategies, all programs effectively promoted social connectedness among older people. Opportunities to meet new people was highlighted as a dominant facilitator for participation in a community‐based PA program.38, 39 Newfound connections for participants in programs existed within the program itself, and extended to outside connections and support in the community. Community‐based organizations that offer health promotion programs that explicitly focus on PA and socialization yield a myriad of health‐related cost savings.40
We highlight the important role volunteers and partnerships with community collaborators played in delivery of programs. For example, many programs were provided in‐kind space and engaged volunteers to offset personnel costs. In many cases, coordinators felt they lacked the knowledge or skill set to effectively deliver the PA component of the program and, therefore, leveraged community expertise in order to deliver aspects of the program. Examples included doctors, physiotherapists, and older adult volunteers. Thus, implementation of programs was effectively adapted through partnerships to accommodate available resources and capacity. Adaptation to context is critical to effective implementation at scale‐up.41, 42
Community‐based organizations can struggle to find personnel with the appropriate knowledge and skills to design and deliver a program. This can limit appropriateness, feasibility, attractiveness, and, thus, participation.43, 44 Mechanisms that enable community‐based organizations to gain in‐house skills, knowledge, and resources would greatly enable the provision of programs that focus on PA and social connectedness.45 In addition, coordinators may vary in their years of experience, as in our study, and it seems essential to provide program coordinators with skills to deliver and adapt programs based on the needs of participants (ie, physical, cultural) and also, to foster attentive leaders that are responsive, nurturing, and connected to participants (ie, enthusiastic, encouraging, inclusive).45 This also fosters sustained participation and enjoyment.46 Engaging older adults in the design of the program47 may prove fruitful in sustaining participation.
Women participants outnumbered men in all programs. Men's “reluctance” to participate in health promoting activities that are not aligned with perceptions of masculinity, has been reported elsewhere,48, 49, 50 and may be one of the reasons at play here as well. Regardless, there is need for strategies to specifically design community‐based health promotion programs for and with men. Men who participated spoke positively about their experience and recounted the physical and social benefits of health promoting programs. They also identified the need to target marketing and recruitment to other men. This may require marketing and health communication strategies that reframe the discourse on PA and socialization.15 In addition, program design needs to consider male preferences as well. As women attended programs more often than men, activities and ways of interacting are likely gendered based on this asymmetry. This highlights the importance of flexible PA programs that can be adapted to individual preferences and capacities.
Programs that were affordable and offered consistent and reliable transportation for participants, effectively promoted participation. Not surprisingly, adequate funding was deemed essential to design, deliver, and sustain programs. Reliable funding is an ongoing challenge for especially small organizations. Too few program coordinators can find themselves responding to increased demands that challenge their capacity to deliver; in response, they try to offer more with less.10 Organizations that had adequate funding required for participation, including transportation, had greater attendance and sustained participation. This was especially true for vulnerable older adults, such as low‐income older adults or those unable to drive. Rural communities struggled with limited transportation options.
While governments acknowledge the important support community‐based organizations provide, funding and access to services has not increased significantly, or has even declined, despite the growing demand for these programs and services as the population ages.10 These resource limitations can undermine the capacity of an organization, and consequently, how effective it can be. Efforts and resources that enable organizations to deliver safe, effective, inclusive, and sustainable health promotion programs for older adults are needed.
Our future work will target communication strategies to initiate greater participation of men in programs and look more closely at program content and implementation strategies that are key to scale‐out. We will adapt the intervention to context and population for scale‐out across rural and remote regions of British Columbia, Canada, and with marginalized older adults in urban settings. We aim to improve the sustainability of large scale‐out community‐driven health promotion programs aimed to improve PA and social connectedness of older adults.
5. LIMITATIONS
This formative evaluation included seven of 30 AAG‐funded programs in the 2016‐2017 funding cycle. As participation was voluntary, this may have introduced volunteer bias whereby organizations ‘most keen' to participate may have volunteered. Detailed sociodemographic characteristics of participants, beyond gender, age, and whether or not they spoke English, were not collected. To be eligible participants had to be over the age of 65, speak English, and participate in one of the AAG‐funded programs. It is possible that themes that emerged do not fully represent the experience of all AAG‐funded programs. However, there was substantial diversity across organizations that did participate in the study. Sites varied in geographical setting, organizational size, target population, type of programming provided, among other characteristics. We believe that this variability might enhance transferability of findings to other settings.
6. CONCLUSIONS
Insufficient evidence creates a barrier to better understanding the impact of government policy and funding on delivery of older adult health promotion initiatives at broad scale in the community,51 and ultimately, on the health of older adults. Thus, there is a clear and urgent need for a collaborative effort among policy makers, community organizations, and researchers to find ways to design, implement, scale‐up, and evaluate effective community‐driven health promotion programs for older adults. As part of a formative evaluation, we adopted the Framework for Successful Implementation for this study to address factors that help or hinder implementation of community‐driven health promoting innovations for older adults aimed to increase PA and social connectedness. The literature, however, is rife with many other frameworks and many elements are common among them.30, 52, 53 In small communities, accountability, affordability, personalized program design, and transportation all contributed to successful implementation, and should be considered by others who seek to design community‐driven health promotion programs for older adults. Governments might heed the loud call for sustained funding to support adequate resources, training, communications, and transportation for activities that support the health of older people in small communities.
CONFLICT OF INTEREST
The authors claim no conflict of interest.
AUTHOR CONTRIBUTIONS
Conceptualization: Joanie Sims‐Gould, Heather McKay, Sarah Lusina‐Furst.
Formal Analysis: Joanie Sims‐Gould, Thea Franke, Heather McKay.
Investigation: Thea Franke, Sarah Lusina‐Furst.
Supervision: Sarah Lusina‐Furst.
Writing—Original Draft Preparation: Joanie Sims‐Gould, Thea Franke, Heather McKay, Sarah Lusina‐Furst.
Writing—Review and Editing: Joanie Sims‐Gould, Thea Franke, Sarah Lusina‐Furst, Heather McKay.
All authors have read and approved the final version of the manuscript.
Joanie Sims‐Gould had full access to all of the data in this study and takes complete responsibility for the integrity of the data and the accuracy of the data analysis.
FUNDING
This work was supported by a Grant‐in‐Aid from the BC Ministry of Health as well as a Canadian Institutes of Health Research project grant (PJT‐153248). Dr. Sims‐Gould is supported by a New Investigator award from the Canadian Institutes of Health Research and a Scholar award from the Michael Smith Foundation for Health Research. The supporting source/financial relationships had no involvement in study design; collection, analysis, and interpretation of data; writing of the report; or the decision to submit the report for publication.
TRANSPARENCY STATEMENT
Joanie Sims‐Gould affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Supporting information
Appendix S1: Coordinator Interview
Appendix S2: Participant Interview
ACKNOWLEDGMENTS
We extend sincere thanks to our study participants for generously sharing their experiences and time. Thank you to research assistants Kaitlin Hong‐Tai and Neville Li who assisted with data collection and study coordination. Thank you to the United Way of the Lower Mainland for their partnership on the Active Aging Grant Initiative.
Sims‐Gould J, Franke T, Lusina‐Furst S, McKay HA. Community health promotion programs for older adults: What helps and hinders implementation. Health Sci Rep. 2020;3:e144 10.1002/hsr2.144
DATA AVAILABILITY STATEMENT
The data sets used during the current study are not publicly available as stipulated in our participant consent forms but are available from the corresponding author on reasonable request.
REFERENCES
- 1. Warburton DER. Health benefits of physical activity: the evidence. Can Med Assoc J. 2006;174(6):801‐809. https://doi.org/10.1503/cmaj.051351 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. 2012;380(9838):247‐257. https://doi.org/10.1016/S0140‐6736(12)60646‐1 [DOI] [PubMed] [Google Scholar]
- 3. Paterson DH, Warburton DE. Physical activity and functional limitations in older adults: a systematic review related to Canada's physical activity guidelines. Int J Behav Nutr Phys Act. 2010;7(1):38. https://doi.org/10.1186/1479‐5868‐7‐38 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Robins LM, Hill KD, Finch CF, Clemson L, Haines T. The association between physical activity and social isolation in community‐dwelling older adults. Aging Ment Health. 2018;22(2):175‐182. https://doi.org/10.1080/13607863.2016.1242116 [DOI] [PubMed] [Google Scholar]
- 5. Holt‐Lunstad J, Smith TB, Layton JB. Social relationships and mortality risk: a meta‐analytic review. PLoS Med. 2010;7(7):e1000316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Nicholson N. A review of social isolation: an important but underassessed condition in older adults. J Prim Prev. 2012. [DOI] [PubMed] [Google Scholar]
- 7. Hawkley LC, Thisted RA, Cacioppo JT. Loneliness predicts reduced physical activity: cross‐sectional and longitudinal analyses. Health Psychol. 2009;28(3):354‐363. https://doi.org/10.1037/a0014400 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Luo Y, Hawkley LC, Waite LJ, Cacioppo JT. Loneliness, health, and mortality in old age: a national longitudinal study. Soc Sci Med. 2012;74(6):907‐914. https://doi.org/10.1016/j.socscimed.2011.11.028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Tilvis RS, Laitala V, Routasalo PE, Pitkälä KH. Suffering from loneliness indicates significant mortality risk of older people. J Aging Res. 2011;2011:1‐5. https://doi.org/10.4061/2011/534781 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Kadowaki L, Cohen M. Raising the Profile of the Community‐Based Seniors' Services Sector in B.C.: A Review of the Literature. Vancouver, BC; 2017. [Google Scholar]
- 11. Cohen M. Caring for BC's Aging Population: Improving Health Care for All. Vancouver, BC: BC Health Coalition and CCPA–BC; 2012. [Google Scholar]
- 12. Pardasani MP, Sporre K, Thompson PM. New Models of Senior Centers Taskforce: Final Report. Washington, DC; 2009. [Google Scholar]
- 13. Milat AJ, Bauman AE, Redman S, Curac N. Public health research outputs from efficacy to dissemination: a bibliometric analysis. BMC Public Health. 2011;11:934. https://doi.org/10.1186/1471‐2458‐11‐934 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Milat AJ, Bauman A, Redman S. Narrative review of models and success factors for scaling up public health interventions. Implement Sci. 2015;10(1):113. https://doi.org/10.1186/s13012‐015‐0301‐6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Bauman A, Merom D, Bull FC, Buchner DM, Fiatarone Singh MA. Updating the evidence for physical activity: summative reviews of the epidemiological evidence, prevalence, and interventions to promote “active aging”. Gerontologist. 2016;56(Suppl 2):S268‐S280. https://doi.org/10.1093/geront/gnw031 [DOI] [PubMed] [Google Scholar]
- 16. Olanrewaju O, Kelly S, Cowan A, Brayne C, Lafortune L. Physical activity in community dwelling older people: a systematic review of reviews of interventions and context. PLoS One. 2016;11(12):e0168614. https://doi.org/10.1371/journal.pone.0168614 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. McKay H, Nettlefold L, Bauman A, et al. Implementation of a co‐designed physical activity program for older adults: positive impact when delivered at scale. BMC Public Health. 2018;18(1):1289. https://doi.org/10.1186/s12889‐018‐6210‐2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. McKay H, Sims‐Gould J, Nettlefold L, Hoy C, Bauman A. Implementing and evaluating an older adult physical activity model at scale: framework for action. Trans J Am Coll Sports Med. 2017;2(2):10. https://doi.org/10.1249/TJX.0000000000000026 [Google Scholar]
- 19. Bauman A, Nutbeam D. Evaluation in a nutshell: a practical guide to the evaluation of health promotion programs. Sydney, AU: McGraw‐Hill; 2013. [Google Scholar]
- 20. O'Hara BJ, Phongsavan P, King L, et al. “Translational formative evaluation”: critical in up‐scaling public health programmes. Health Promot Int. 2014;29(1):38‐46. https://doi.org/10.1093/heapro/dat025 [DOI] [PubMed] [Google Scholar]
- 21. Stetler CB, Legro MW, Wallace CM, et al. The role of formative evaluation in implementation research and the QUERI experience. J Gen Intern Med. 2006;21(S2):S1‐S8. https://doi.org/10.1111/j.1525‐1497.2006.00355.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Durlak JA, DuPre EP. Implementation matters: a review of research on the influence of implementation on program outcomes and the factors affecting implementation. Am J Community Psychol. 2008;41(3–4):327‐350. [DOI] [PubMed] [Google Scholar]
- 23. Fixsen DL, Naoom SF, Blasé KA, Friedman RM, Wallace F. Implementation Research a Synthesis of the Literature. Tampa, FL; 2005. [Google Scholar]
- 24. Aarons GA, Sklar M, Mustanski B, Benbow N, Brown CH. “Scaling‐out” evidence‐based interventions to new populations or new health care delivery systems. Implement Sci. 2017;12(1):111. https://doi.org/10.1186/s13012‐017‐0640‐6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Wandersman A, Duffy J, Flaspohler P, et al. Bridging the gap between prevention research and practice: the interactive systems framework for dissemination and implementation. Am J Community Psychol. 2008;41(3–4):171‐181. https://doi.org/10.1007/s10464‐008‐9174‐z [DOI] [PubMed] [Google Scholar]
- 26. King AC, Stokols D, Talen E, Brassington GS, Killingsworth R. Theoretical approaches to the promotion of physical activity: forging a transdisciplinary paradigm. Am J Prev Med. 2002;23(2):15‐25. [DOI] [PubMed] [Google Scholar]
- 27. Stokols D. Bridging the theoretical and applied facets of environmental psychology. Am Psycho. 1996. [Google Scholar]
- 28. Haggis C, Sims‐Gould J, Winters M, Gutteridge K, McKay HA. Sustained impact of community‐based physical activity interventions: key elements for success. BMC Public Health. 2013;13(1):892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Meyers DC, Durlak JA, Wandersman A. The quality implementation framework: a synthesis of critical steps in the implementation process. Am J Community Psychol. 2012;50(3–4):462‐480. https://doi.org/10.1007/s10464‐012‐9522‐x [DOI] [PubMed] [Google Scholar]
- 30. Yamey G. Scaling up global health interventions: a proposed framework for success. PLoS Med. 2011;8(6):e1001049. https://doi.org/10.1371/journal.pmed.1001049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Graham ID, Tetroe JM. The knowledge to action framework In: Models and Frameworks for Implementing Evidence‐Based Practice: Linking Evidence to Action. Oxford: Wiley‐Blackwell; 2010:1‐21. [Google Scholar]
- 32. Ritchie J, Spencer L. Qualitative data analysis for applied policy research In: The Qualitative Researcher's Companion; 2002:305‐329. [Google Scholar]
- 33. Srivastava A, Thomson SB. Framework analysis: a qualitative methodology for applied policy research. JOAAG. 2009;4(2):72‐79. [Google Scholar]
- 34. Glaser BG, Strauss AL. The Discovery of Grounded Theory: Strategies for Qualitative Research. New York: Aldine de Gruyter; 1967. [Google Scholar]
- 35. Lincoln YS, Guba EG. In: L. S. Bowman & Sarah , ed. Naturalistic Inquiry. Beverly Hills, CA: Sage Publications; 1985. [Google Scholar]
- 36. Saunders B, Sim J, Kingstone T, et al. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quant. 2018;52(4):1893‐1907. https://doi.org/10.1007/s11135‐017‐0574‐8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Bopp M, Saunders RP, Lattimore D. The tug‐of‐war: fidelity versus adaptation throughout the health promotion program life cycle. J Prim Prev. 2013;34(3):193‐207. https://doi.org/10.1007/s10935‐013‐0299‐y [DOI] [PubMed] [Google Scholar]
- 38. Dare J, Wilkinson C, Marquis R, Donovan RJ. “The people make it fun, the activities we do just make sure we turn up on time.” Factors influencing older adults' participation in community‐based group programmes in Perth, Western Australia. Health Soc Care Community. 2018;26(6):871‐881. https://doi.org/10.1111/hsc.12600 [DOI] [PubMed] [Google Scholar]
- 39. Grant G, Machaczek K, Pollard N, Allmark P. Walking, sustainability and health: findings from a study of a walking for health group. Health Soc Care Community. 2017;25(3):1218‐1226. https://doi.org/10.1111/hsc.12424 [DOI] [PubMed] [Google Scholar]
- 40. Hildebrandt H, Hermann C, Knittel R, Richter‐Reichhelm M, Siegel A, Witzenrath W. Gesundes Kinzigtal integrated care: improving population health by a shared health gain approach and a shared savings contract. Int J Integrat Care. 2010;10(2). https://doi.org/10.5334/ijic.539 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Stirman SW, Miller CJ, Toder K, Calloway A. Development of a framework and coding system for modifications and adaptations of evidence‐based interventions. Implement Sci. 2013;8(1):65. https://doi.org/10.1186/1748‐5908‐8‐65 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Wiltsey Stirman S, Baumann AA, Miller CJ. The FRAME: an expanded framework for reporting adaptations and modifications to evidence‐based interventions. Implement Sci. 2019;14(1):58. https://doi.org/10.1186/s13012‐019‐0898‐y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Hickerson B, Moore A, Oakleaf L, et al. The role of a senior centre in promoting physical activity for older adults. Park Recreat Admin. 2008;26(1):22‐39. [Google Scholar]
- 44. Li F, Eckstrom E, Harmer P, Fitzgerald K, Voit J, Cameron KA. Exercise and fall prevention: narrowing the research‐to‐practice gap and enhancing integration of clinical and community practice. J Am Geriatr Soc. 2016;64(2):425‐431. https://doi.org/10.1111/jgs.13925 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Victorian Active Ageing Partnership (VAAP) into Year Four ! (2018). Retrieved from https://www.msk.org.au/vaap/%0D%0Ahttps://fitness.org.au/articles/exercise-science/victorian-active-ageing-partnership-vaap-into-year-four/6/1616%0D%0A
- 46. Winterton R, Hulme Chambers A. Developing sustainable social programmes for rural ethnic seniors: perspectives of community stakeholders. Health Soc Care Community. 2017;25(3):868‐877. https://doi.org/10.1111/hsc.12373 [DOI] [PubMed] [Google Scholar]
- 47. Wagland R, Windle K, Wistow G, D'Amico F. Involving older people in health and social care services: why good intentions are not enough. Health Social Care Community. 2018. [Google Scholar]
- 48. Connell RW, Messerschmidt JW. Hegemonic masculinity. Gender & Society. 2005;19(6):829‐859. https://doi.org/10.1177/0891243205278639 [Google Scholar]
- 49. Courtenay WH. Constructions of masculinity and their influence on men's well‐being: a theory of gender and health. Soc Sci Med. 2000;50(10):1385‐1401. https://doi.org/10.1016/S0277‐9536(99)00390‐1 [DOI] [PubMed] [Google Scholar]
- 50. Sims‐Gould J, Ahn R, Li N, Ottoni CA, Mackey DC, McKay HA. “The social side is as important as the physical side”: older men's experiences of physical activity. Am J Mens Health. 2018;12(6):2173‐2182. https://doi.org/10.1177/1557988318802691 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Phillipson C, Scharf T. The Impact of Government Policy on Social Exclusion Among Older People: A Review of the Literature for the Social Exclusion Unit in the Breaking the Cycle series. London, UK; 2004. [Google Scholar]
- 52. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4(1):50. https://doi.org/10.1186/1748‐5908‐4‐50 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Simmons R, Shiffman J. Scaling up health service innovations: a framework for action In: Simmons R, ed. Scaling Up Health Service Delivery: From Pilot Innovations to Policies and Programmes. Geneva, Switzerland: World Health Organization; 2007:1‐30. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1: Coordinator Interview
Appendix S2: Participant Interview
Data Availability Statement
The data sets used during the current study are not publicly available as stipulated in our participant consent forms but are available from the corresponding author on reasonable request.