

Abstract
Background
Pneumonia is an important cause of mortality in intensive care units (ICUs). The incidence of pneumonia in ICU patients ranges between 7% and 40%, and the crude mortality from ventilator‐associated pneumonia may exceed 50%. Although not all deaths in patients with this form of pneumonia are directly attributable to pneumonia, it has been shown to contribute to mortality in ICUs independently of other factors that are also strongly associated with such deaths.
Objectives
To assess the effects of prophylactic antibiotic regimens, such as selective decontamination of the digestive tract (SDD) for the prevention of respiratory tract infections (RTIs) and overall mortality in adults receiving intensive care.
Search methods
We searched the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2009, issue 1), which contains the Cochrane Acute Respiratory Infections (ARI) Group's Specialised Register; MEDLINE (January 1966 to March 2009); and EMBASE (January 1990 to March 2009).
Selection criteria
Randomised controlled trials (RCTs) of antibiotic prophylaxis for RTIs and deaths among adult ICU patients.
Data collection and analysis
At least two review authors independently extracted data and assessed trial quality.
Main results
We included 36 trials involving 6914 people. There was variation in the antibiotics used, patient characteristics and risk of RTIs and mortality in the control groups. In trials comparing a combination of topical and systemic antibiotics, there was a significant reduction in both RTIs (number of studies = 16, odds ratio (OR) 0.28, 95% confidence interval (CI) 0.20 to 0.38) and total mortality (number of studies = 17, OR 0.75, 95% CI 0.65 to 0.87) in the treated group. In trials comparing topical antimicrobials alone (or comparing topical plus systemic versus systemic alone) there was a significant reduction in RTIs (number of studies = 17, OR 0.44, 95% CI 0.31 to 0.63) but not in total mortality (number of studies = 19, OR 0.97, 95% CI 0.82 to 1.16) in the treated group.
Authors' conclusions
A combination of topical and systemic prophylactic antibiotics reduces RTIs and overall mortality in adult patients receiving intensive care. Treatment based on the use of topical prophylaxis alone reduces respiratory infections but not mortality. The risk of resistance occurring as a negative consequence of antibiotic use was appropriately explored only in one trial which did not show any such effect.
Plain language summary
Antibiotics to help reduce mortality and respiratory infections in people receiving intensive care in hospital
Infections acquired in intensive care units (ICUs) are important complications of the treatment of patients with very severe diseases who need ventilation (mechanical breathing support). Some people will die because of these infections. Considerable efforts have been made to evaluate methods for reducing this problem; one of these involves the use of antibiotics administered as preventative intervention, usually referred to as selective decontamination of the digestive tract (SDD). This review includes 36 studies involving 6914 patients treated in ICUs to investigate whether the administration of antibiotics prevents the development of infections. Antibiotics were administered in two different ways. In some studies antibiotics were applied both directly to the oropharynx via a nasogastric tube (topical) and intravenously (systemic). In other studies they were applied only topically. Our results show that when patients received the combination of topical plus systemic antibiotics there were less infections and deaths. When patients received only topical treatment there were less infections but the number of deaths was not changed. Although this treatment seems to work it is not widely used in clinical practice because there is concern about the possible development of antibiotic resistance (that is, bacteria become unresponsive to drugs).
Background
Description of the condition
Infections acquired in the intensive care unit (ICU), especially pneumonia, are important complications of the treatment of critically ill patients, increasing morbidity and mortality. The incidence of pneumonia has been reported to vary from 7% to more than 40% in ICU patients (Chevret 1996; Fagon 1996). The mortality rate for patients with ventilator‐associated pneumonia (VAP) may exceed 50%. Although not all deaths in patients with pneumonia are directly attributable to pneumonia, it has been shown to contribute to ICU mortality, independently of other factors that are also strongly associated with deaths in these patients (Fagon 1996). In a case‐controlled study an increase in mortality of 27% attributable to pneumonia was evidenced in ventilated patients (Fagon 1996).
Description of the intervention
Considerable efforts have been made to evaluate methods for reducing respiratory tract infections (RTIs). One strategy involves the use of selective decontamination of the digestive tract (SDD). Different SDD protocols have been used in different trials and investigators often disagree on which is the most appropriate definition of SDD. Traditionally, SDD indicates a method designed to prevent infection by eradicating and preventing carriage of aerobic, potentially pathogenic micro‐organisms from the oropharynx, stomach and gut. It consists of antimicrobials applied topically to the oropharynx through a nasogastric tube. In some trials systemic antibiotic therapy has been added in the first days after the patients' admission to prevent 'early' infections.
How the intervention might work
The use of oral non‐absorbable antibiotics was first reported by Stoutenbeek (Stoutenbeek 1994) in an SDD protocol based upon a group of multiple trauma patients. The incidence of nosocomial (hospital‐acquired) infection was reduced from 81% to 16% in a non‐randomised comparison with an historical control group. Further studies tested the efficacy of SDD in ICU patients, with infection‐related morbidity as the main endpoint. The results showed that SDD reduced infection but it was not clear whether there was a reduction in mortality.
Between 1991 and 2008 nine different systematic review and meta‐analyses (D'Amico 1998; Heyland 1994; Hurley 1995;Kollef 1994; Nathens 1999; Redman 2001; Silvestri 2007; SDD Group 1993; Vanderbrouk‐Gra 1991) on the effect of SDD on RTIs and mortality were published. Their results are summarised in the table below.
| SR | N° of studies | N° of patients | Mortality | RTIs |
|
Vanderbrouk‐Gra 1991 |
6 | 491 | Odds ratio (OR) 0.70 95% confidence intervals (CI) 0.45 to 1.09 | OR 0.12 95% CI 0.08 to 0.19 |
| SDD Group 1993 | 22 | 4142 | OR 0.90 95% CI 0.79 to 1.04 | OR 0.37 95% CI 0.31 to 0.43 |
| Heyland 1994 | 24 | 3312 | Risk ratio (RR) 0.87 95% CI 0.79 to 0.97 | RR 0.46 95% CI 0.39 to 0.56 |
| Kollef 1994 | 16 | 2270 | Risk difference (RD) 0.019 95% CI ‐ 0.016 to 0.054 |
Pneumonia
RD 0.145
95% CI 0.116 to 0.174 Tracheobronchitis RD 0.052 95% CI 0.017 to 0.087 |
| Hurley 1995 | 26 | 3768 | OR 0.86 95% CI 0.74 to 0.99 | OR 0.35 95% CI 0.30 to 0.42 |
| D'Amico 1998 | 33 | 5727 |
Topical plus systemic (16 trials; 3361 pts)
OR 0.80
95% CI 0.69 to 0.93 Topical alone (17 trials; 2366 pts) OR 1.01 95% CI 0.84 to 1.22 |
Topical plus systemic (16 trials; 3361 pts)
OR 0.35
95% CI 0.29 to 0.41 Topical alone (17 trials; 2366 pts) OR 0.56 95% CI 0.46 to 0.68 |
|
Nathens 1999 |
21 | Not reported |
Surgical patients
OR 0.7
95% CI 0.52 to 0.93 Medical patients OR 0.91 95% CI 0.71 to 1.18 |
NA |
|
Redman 2001 |
Not reported | Not reported | NA | Ventilator‐associated pneumonia (VAP) OR 0.36 95% CI 0.28 to 0.46 |
| Silvestri 2007 | 51 | 8065 | OR 0.8 95% CI 0.69 to 0.94 | NA |
All studies assessing RTIs confirmed their statistically significant reduction, though the magnitude of the treatment effect varied from one review to another probably due to different numbers of studies and inclusion criteria among them. The estimated impact on overall mortality was less evident.
This is an update to the previous version published in The Cochrane Library which included trials published up to 2003.
Objectives
To determine whether antibiotic prophylaxis reduces RTIs and overall mortality in adult patients treated in ICUs.
Specifically, the main question left unanswered by existing randomised controlled trials (RCTs) and previous meta‐analyses was whether different forms of antibiotic prophylaxis (that is, topical antimicrobials or a combination of topical and systemic drugs) are effective in reducing overall mortality.
Methods
Criteria for considering studies for this review
Types of studies
RCTs on antibiotic prophylaxis for preventing RTIs and deaths in adult ICU patients.
Types of participants
Adult patients admitted to an ICU. Studies based on specific pre‐selected types of patients (that is, patients undergoing elective oesophageal resection, cardiac or gastric surgery, liver transplant or suffering from acute liver failure) were excluded because these patients need co‐interventions that may interact with the main treatment. Studies where the majority of patients (> 50%) did not undergo mechanical ventilation for more than 48 hours were also excluded. The characteristics of excluded studies are reported in the 'Characteristics of excluded studies' table.
Types of interventions
Available RCTs have been grouped into two categories, defined according to the type of antibiotic prophylaxis:
studies where a combination of systemic and topical antibiotics was tested against no prophylactic treatment (thereafter referred to as 'topical plus systemic versus no prophylaxis'); and
studies where the experimental treatment tested was a topical preparation applied in the oropharynx (thereafter referred to as 'topical versus control').
For further details about preparation and administration of antibiotic prophylaxis see the 'Characteristics of included studies' table.
In this latter category two RCT subgroups have been lumped together, that is, those where topical antibiotics were tested against an untreated control group and those where the combination of topical plus systemic drugs was compared with a protocol based on a systemic antimicrobial only.
Any topical or systemic antimicrobial combination (that is: type of drugs) was accepted, because there was no data to assume a difference in effect among the considered prophylactic treatments. This obviously does not mean that all topical and systemic regimens are truly equivalent, but simply reflects our pragmatic working assumption.
Types of outcome measures
Primary outcomes
Primary outcome measures considered for this review were RTIs and overall mortality. No restriction was made on the type of RTIs considered, or on the RTIs diagnostic criteria chosen by the trialists. Both tracheobronchitis and pneumonia were acceptable. Pragmatically, both primary (diagnosed within 48 hours from admission) and acquired (diagnosed after 48 hours from admission) infections were considered, even though we used data on acquired infections (the most appropriate outcome to assess treatment effect) when both pieces of information were available. Mortality was evaluated at hospital discharge if this information was provided; otherwise mortality in ICU was used.
Search methods for identification of studies
Electronic searches
We searched the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2009, issue 1); MEDLINE (January 1966 to March 2009); and EMBASE (January 1990 to March 2009).
MEDLINE was searched using the following search strategy in conjunction with the Cochrane Highly Sensitive Search Strategy for identifying randomised trials in MEDLINE: sensitivity‐ and precision‐maximising version (2008 revision); Ovid format (Lefebvre 2008). The same strategy was used to search CENTRAL and adapted to search EMBASE.com (see Appendix 1).
MEDLINE (Ovid) 1 exp Respiratory Tract Infections/ 2 respiratory tract infection*.tw. 3 exp Pneumonia/ 4 pneumon*.tw. 5 (HAP or VAP).tw. 6 bronchopneumonia*.tw. 7 pleuropneumonia*.tw. 8 exp Bronchitis/ 9 bronchit*.tw. 10 bronchiolit*.tw. 11 exp Pharyngitis/ 12 pharyngit*.tw. 13 Tracheitis/ 14 tracheit*.tw. 15 or/1‐14 16 exp Intensive Care Units/ 17 icu.tw. 18 exp Critical Care/ 19 critical care.tw. 20 intensive care.tw. 21 burn unit*.tw. 22 care unit*.tw. 23 recovery room*.tw. 24 Critical Illness/ 25 (critic* adj ill*).tw. 26 exp Ventilators, Mechanical/ 27 mechanical ventilat*.tw. 28 ventilator*.tw. 29 Respiration, Artificial/ 30 artificial respiration*.tw. 31 respirator*.tw. 32 or/16‐31 33 15 and 32 34 Pneumonia, Ventilator‐Associated/ 35 33 or 34 36 Antibiotic Prophylaxis/ 37 exp Anti‐Bacterial Agents/ 38 antibiotic*.tw. 39 or/36‐38 40 35 and 39
Searching other resources
There were no language or publication restrictions. We searched reference lists of articles from January 1984 to March week 1 2009 and proceedings of scientific meetings from January 1984 to April 2002. We also contacted investigators in the field. We evaluated other studies listed in previous meta‐analyses. We did not make any formal enquiries through pharmaceutical companies. We stopped the search for conference proceedings after the early phase of this review in 2002 when we decided that in subsequent updates we will include new data only if reported in fully published papers.
Data collection and analysis
Selection of studies
Three review authors (LB, EP, SP) independently screened the titles and abstracts of all the references retrieved by the search strategy. The full text of relevant studies were assessed independently to determine whether they met the inclusion criteria. Disagreements were resolved by discussion with the two review authors (AL, RD).
Data extraction and management
Three review authors (LB, EP, SP) independently extracted data from all the included studies using an ad hoc extraction form. Disagreements were solved by discussion with two review authors (AL, RD).
Assessment of risk of bias in included studies
At least two review authors (LB, EP, SP) independently assessed the methodological validity of selected trials according to two quality criteria:
quality of randomisation procedures ('adequate' versus 'unclear, inadequate or not done' which will be referred hereafter as 'not adequate'); and
blinding of patients and doctors to allocated treatment ('double‐blind' versus 'open').
We resolved outstanding issues by consensus.
Only RCTs were accepted in order to prevent possible selection bias. Studies including adult patients admitted to an ICU were included. Studies based on specific pre‐selected types of patients (that is, patients undergoing elective oesophageal resection, cardiac or gastric surgery, liver transplant or suffering from acute liver failure) were excluded.
Measures of treatment effect
Crude proportions of RTIs and mortality were our main treatment end‐points. Odds ratios (OR) for each trial and for each outcome were calculated and they were summarised by using the fixed‐effect model, whereas the random‐effects model was used in cases of statistically significant heterogeneity (P = 0.1). We also computed the number of ICU patients who need to be treated in order to prevent one infection and one death. The calculation was based on the median rates of RTIs and deaths in untreated controls and the common OR for all trials.
Dealing with missing data
We contacted study investigators in order to obtain data for intention‐to‐treat analysis. In 25 out of 36 studies we obtained data on patients lost to follow‐up while for the remaining 11 studies we relied on published information only.
Data synthesis
Results from the trials were combined using a fixed‐effect model to calculate odds ratio (OR) with 95% confidence intervals (CI) for dichotomous data. In case of statistically significant heterogeneity a random‐effects model was used. The number needed to treat to benefit (NNTB) was calculated.
Subgroup analysis and investigation of heterogeneity
Two pre‐specified subgroup analyses based on quality criteria were carried out within the two main groups of RCTs specified above:
quality of randomisation procedures; and
blinding of patients and doctors to allocated treatment.
Results
Description of studies
Results of the search
Sixty potentially eligible RCTs were identified from the electronic searches.
Included studies
Thirty‐six RCTs were finally included, all of them were published (34 as full reports and two in abstract form). Seventeen RCTs compared topical and systemic antibiotic treatment versus no treatment or placebo; 14 RCTs compared topical treatment to no treatment or placebo; and five trials compared topical and systemic antibiotic treatment versus systemic antibiotic only.
We included two studies (Gaussorgues 1991; Laggner 1994) among the 'topical SDD plus systemic antibiotic versus systemic antibiotic only' group even if their design did not explicitly foresee the use of systemic antibiotics because all patients in both arms were treated with systemic antibiotics on admission. Similarly, we included the Jacobs (Jacobs 1992) study among the 'topical SDD plus systemic antibiotics versus control' group because more than 90% of patients received a systemic antibiotic on admission.
The four studies with a three‐arm comparison were analysed as follows. In two studies (Aerdts 1991; Verwaest 1997) the two control groups were pooled together and compared to the treatment group. In another study (Lingnau 1997) we split the study into two comparisons in which two different treatment arms were compared to the same control arm. In one study (Palomar 1997) one of the two control arms was excluded because patients received only sucralfate. Another study (Camus 2005) was a four‐arm factorial design in which we considered only two arms comparing antibiotic prophylaxis versus placebo.
Overall, the total number of patients randomised to either antibiotic prophylaxis versus placebo or no treatment was 6914. The final meta‐analysis was based upon 36 trials with 37 comparisons.
Two studies (Cerra 1992; Gaussorgues 1991) could not contribute to the RTIs analysis as they reported the number of episodes of RTIs and not the number of infected patients. Moreover, one trial (de Jonge 2003) did not assess RTIs as an endpoint.
Mortality was evaluated in ICU in 24 trials; hospital mortality was available only for six RCTs; two trials reported mortality in both ICU and hospital (de Jonge 2003; Georges 1994) and the exact time of assessment of mortality was not determined in four trials (Cerra 1992; Jacobs 1992; Kerver 1988; Pneumatikos 2002).
Most RCTs included general ICU patients. A few trials included mostly trauma (Boland 1991; Georges 1994; Lingnau 1997; Pneumatikos 2002; Quinio 1995; Stoutenbeek 1996; Stoutenbeek 2007) or surgical patients (Cerra 1992; Krueger 2002).
One‐hundred percent of patients were mechanically ventilated in 26 studies; this percentage was lower in six trials (Brun‐Buisson 1989; Blair 1991; Cockerill 1992; de Jonge 2003; Ulrich 1989; Winter 1992) and unknown in four (Camus 2005; Cerra 1992; Finch 1991; Krueger 2002). In Brun‐Buisson's study (Brun‐Buisson 1989) the percentage of ventilated patients was very low (59%) probably because the setting of the study included both 'acute' and 'intermediate' areas of a medical ICU.
The percentage of immunocompromised patients was usually lower than 10%; it was higher only in four trials (Brun‐Buisson 1989; Finch 1991; Gastinne 1992; Laggner 1994). Sucralfate was routinely used in all patients for stress ulcer prophylaxis in nine trials (Abele‐Horn 1997; Bergmans 2001; Ferrer 1994; Gaussorgues 1991; Jacobs 1992; Krueger 2002; Laggner 1994; Quinio 1995; Verwaest 1997). In many RCTs only RTIs acquired in ICU (that is, diagnosed after 48 hours from admission) were considered. Data on primary and acquired infections were considered together only in three trials (Boland 1991; Stoutenbeek 1996; Stoutenbeek 2007). Most studies (26 RCTs) evaluated only the occurrence of pneumonia, while seven RCTs also evaluated tracheobronchitis; information was lacking in three RCTs. Diagnostic criteria differed across trials. Few trial authors provided quantitative details on the cut‐off point used as positive bacteriological confirmation.
Excluded studies
Twenty‐six trials were excluded (see 'Charateristics of excluded studies' table) (Arnow 1996; Barret 2001; Bion 1994; Bouter 2002; de la Cal 2005; de Smet 2009; Flaherty 1990; Garbino 2002; Hellinger 2002; Hunefeld 1989; Jacobs 1995; Lipman 1994; Luiten 1995; Martinez 1994; Martinez‐Pellus 1993; Nardi 2001; Rayes 2002; Rolando 1996; Ruza 1998; Lenhart 1994; Stoutenbeek 2; Schardey 1997; Smith 1993; Tetteroo 1990; Zobel 1991; Zwaveling 2002).
Risk of bias in included studies
Study quality was assessed looking at two criteria. These two quality criteria were used to perform one‐way subgroup analyses for two treatment comparisons (topical plus systemic versus no treatment and topical alone versus no treatment) on the two main outcomes (RTIs and overall mortality).
Allocation
A = adequate; B = unclear; C = inadequate; D = not used. Allocation concealment was evaluated according to the criteria in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2008).
Blinding
Double‐blind, open.
Effects of interventions
RTIs
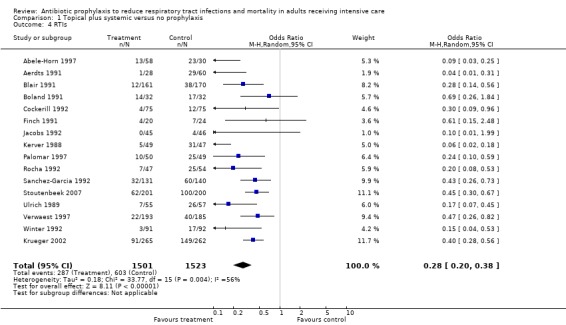
Results from 33 RCTs including 5697 patients were available for the analysis on the effects of different types of antibiotic prophylaxis on RTIs. The frequency of RTIs was 19% among treated patients and 40% among controls in RCTs using a combination of topical plus systemic antibiotic and 20% and 31%, respectively, in RCTs testing the effectiveness of topical prophylaxis. Overall, the ORs were less than 1 in all but two trials (Lingnau 1997; Wiener 1995) and reached conventional statistical significance (P < 0.05) in 22/34 comparisons.
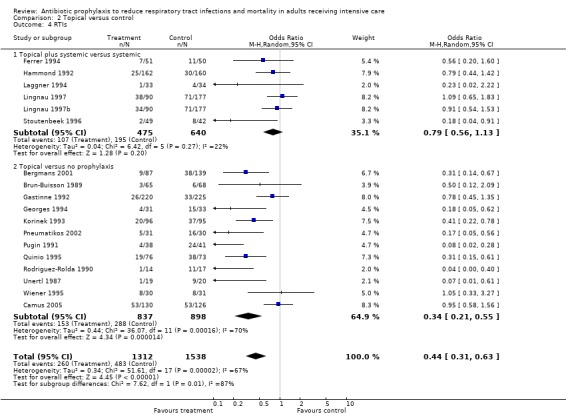
Since statistically significant heterogeneity was observed, a random‐effects model was used to summarise study results. Results indicate a strong protective effect in RCTs where the combination of topical and systemic treatment (OR 0.28, 95% CI 0.20 to 0.38) was tested. A significant protection emerged when topical prophylaxis was considered (OR 0.44, 95% CI 0.31 to 0.63). The effect was stronger in RCTs where topical antimicrobials were tested against no prophylaxis (OR 0.34, 95% CI 0.21 to 0.55). Less extreme results were observed in trials testing the combination of topical and systemic antibiotic against systemic prophylaxis (OR 0.79, 95% CI 0.56 to 1.13).
These results indicate that four (95% CI 3 to 5) or seven (95% CI 6 to 12) patients need to be treated to prevent at least one infection, depending on whether a combination of topical and systemic treatment or topical antimicrobials alone were tested (assuming, as baseline risk, the median values of 46% and 27%, respectively, among control patients).
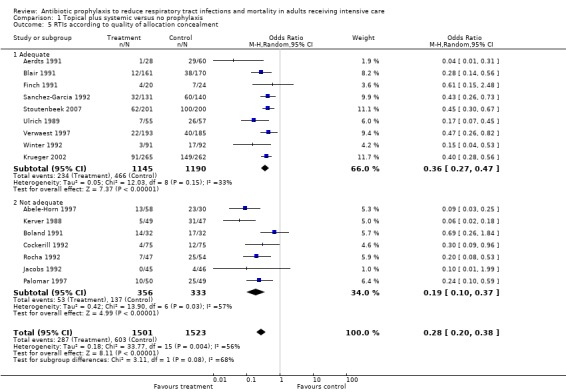
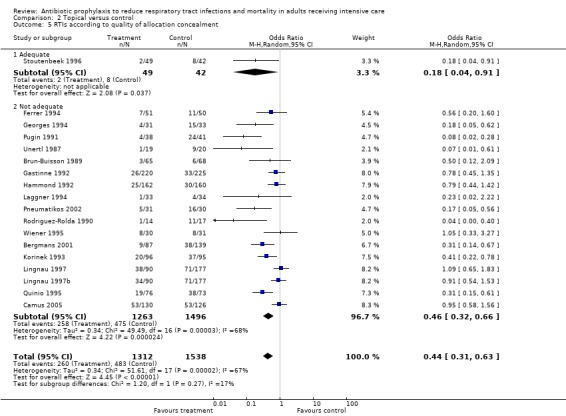
Regarding the pre‐defined subgroup analyses, a statistically significant difference in the estimates of treatment effect was only found for quality of allocation concealment in the topical versus control comparison.
Mortality
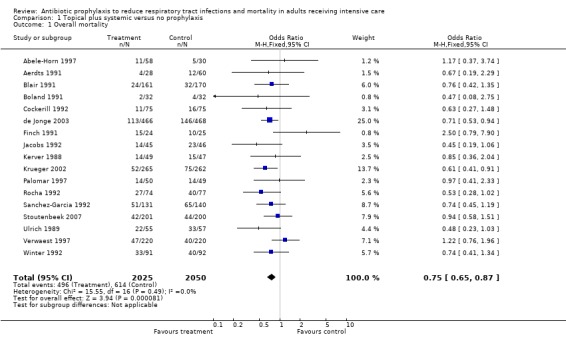
Overall, 36 RCTs including 6,914 patients were available for the mortality analysis. The mortality was 24% among treated patients and 30% among controls on RCTs using a combination of topical plus systemic antibiotic; while it was 26% and 25% respectively in RCTs testing the effectiveness of topical SDD. The ORs were less than 1 in 26/38 comparisons but reached conventional statistical significance in three RCTs (de Jonge 2003; Krueger 2002; Stoutenbeek 1996); no trial showed a significant harmful effect of antibiotic prophylaxis.
Regarding mortality no statistically significant heterogeneity was observed among study results.
Results indicated a statistically significant reduction in mortality attributable to the use of a combination of topical and systemic treatment (OR 0.75, 95% CI 0.65 to 0.87). This suggests that 18 patients (95% CI 12 to 36) (assuming a baseline risk of 29%, median among control patients) need to be treated to prevent one death. On the other hand, no treatment effect emerged when RCTs testing topical antimicrobials were analysed (OR 0.97; 95% CI 0.82 to 1.16).
The subgroup analyses produced the following results:
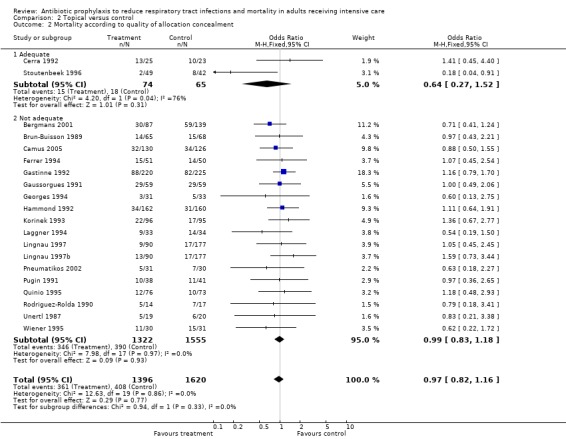
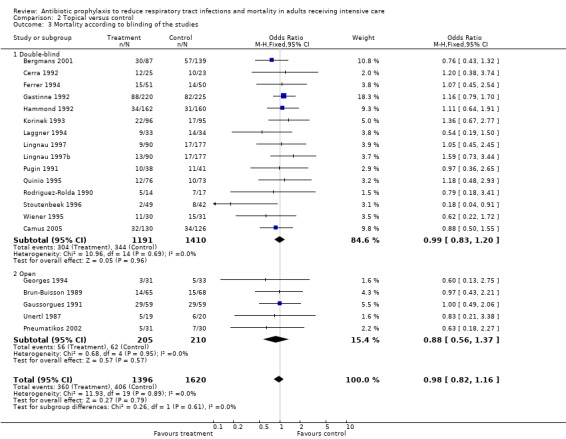
Topical versus control
Allocation concealment: adequate (OR 0.64, 95% CI 0.27 to 1.52), not adequate (OR 0.99, 95% CI 0.83 to 1.18). Blind design: double blind (OR 0.99, 95% CI 0.83 to 1.20), open (OR 0.88, 95% CI 0.56 to 1.37).
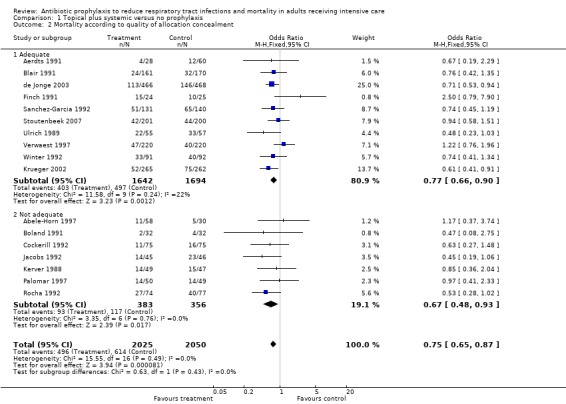
Topical plus systemic versus no prophylaxis
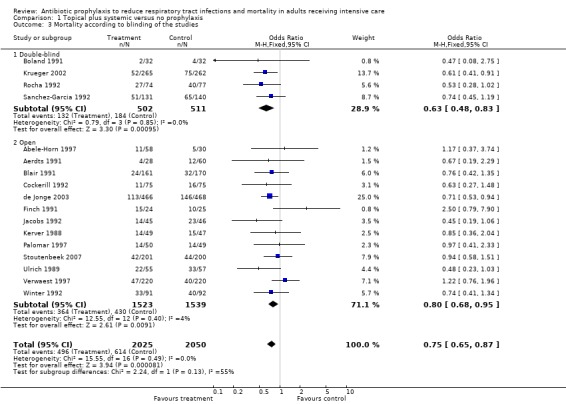
Allocation concealment: adequate (OR 0.77, 95% CI 0.66 to 0.90), not adequate (OR 0.67, 95% CI 0.48 to 0.93). Blind design: double blind (OR 0.63, 95% CI 0.48 to 0.83), open (OR 0.80, 95% CI 0.68 to 0.95).
Discussion
Since antibiotic prophylaxis based on SDD was introduced as a preventative measure against infection in critically ill patients, it has remained a controversial intervention (Stoutenbeek 1994). Due to the lack of a standard protocol and insufficient patient numbers, it has proved difficult to derive meaningful conclusions from individual clinical trials. Following initial enthusiasm from results of early uncontrolled studies and RCTs, antibiotic prophylaxis is not widely used as a routine treatment in ICUs. Concerns about the risk of antimicrobial resistance and increased costs are often quoted as important factors preventing its widespread adoption. A conservative attitude in introducing a new treatment into practice is understandable as long as doubts about its efficacy exist. Studies on prevention of VAP in ICU patients are complex, as patients are heterogeneous, diagnosis of pneumonia is controversial and outcomes depend upon a variety of factors. Despite the fact that antibiotic prophylaxis reduces the emergence of RTIs with remarkable consistency across individual trials, the effect on mortality was individually statistically significant in only three trials. An historical examination of review articles and editorials in this area indicates that for many years it was not fully realised that this could have been due to the small sample sizes of individual studies.
The meta‐analysis reported here combines data across several studies in order to estimate treatment effects with more precision than is possible in a single study. The main limitation of this type of pooled analysis is that the patient population, the antibiotic regimen and the outcome definitions are not the same across studies. Nonetheless, we believe that it provides the best global picture of the effectiveness of the intervention despite some recent criticisms on the quality of primary studies and their combination (van Nieuwenhove 2001) which we feel we have convincingly addressed (Liberati 2001). Compared to the other six published meta‐analyses (Heyland 1994; Hurley 1995; Kollef 1994; Nathens 1999; SDD Group 1993; Vanderbrouk‐Gra 1991) we decided in our previously published review (D'Amico 1998) to analyse separately trials testing a combination of systemic and topical antibiotics and those testing topical antimicrobials. Though there is no consensus on the best way to classify antibiotic prophylaxis regimens, eventually it seemed more appropriate to consider the two groups of trials as two distinct approaches to antibiotic prophylaxis. This decision was made a priori, independently of knowing their results.
As already shown in our previous review (D'Amico 1998) and confirmed in this update, both types of prophylaxis have a strong protective effect on RTIs ‐ with the effect being more marked when patients are treated with a protocol using topical plus systemic antibiotics. This effect looks consistent in all subgroup analyses, regardless of study design (adequate / not adequate allocation concealment, double‐blind / open design). Overall, these results appear convincing even though it is acknowledged that no diagnostic test or procedure is ideal to diagnose RTIs in ICU patients.
More importantly, this updated review confirms that the use of a combination of topical and systemic antibiotics reduces overall mortality significantly. This treatment effect looks important from a clinical and public health point of view (in terms of the therapeutic implications for the care of ventilated patients in ICUs) and is also relevant from the scientific standpoint, as it suggests the future directions that research in this field should take.
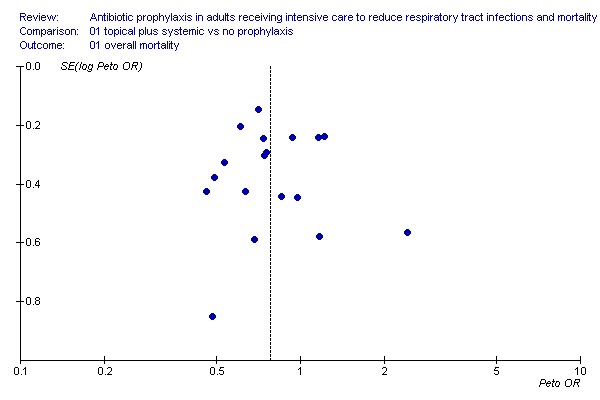
Publication bias is unlikely to have influenced our results because we made a thorough effort to trace unpublished studies and because the vast majority of trials did not show statistically significant reduction in mortality on their own. Moreover, inspection of the relevant funnel plot for overall mortality reduction in patients receiving the combined treatment (see additional analysis, Figure 1) does not provide evidence of publication bias. Finally, if one ranks studies by their size, larger ones are those showing a statistically significant treatment effect on their own.
1.
Authors' conclusions
Implications for practice.
This systematic review indicates that a protocol testing a combination of topical and systemic antibiotics reduces the occurrence of RTIs and overall mortality. These results were initially obtained in an individual patient meta‐analysis reported elsewhere (D'Amico 1998), which we have now updated using data reported in trials published between 1999 and 2007. The yield of the treatment expressed in terms of patients needed to be treated to prevent one infection and one death is substantial ‐ 4 and 18 respectively ‐ and compares very favourably with several interventions largely used in clinical practice. Though 11/17 trials used an identical regimen, including polymyxin, tobramycin and amphotericin as the topical combination and cefotaxime as the systemic component (Abele‐Horn 1997; Blair 1991; de Jonge 2003; Ferrer 1994; Hammond 1992; Jacobs 1992; Kerver 1988; Palomar 1997; Rocha 1992; Stoutenbeek 1996; Stoutenbeek 2007), this review does not allow a unique regimen to be recommended. The use of a prophylaxis testing topical antimicrobials is, on the other hand, not warranted by available data.
Results of this review should be carefully considered by those who have been sceptical about the effectiveness of antibiotic prophylaxis, mostly on the grounds of a potentially harmful effect in terms of antibiotic resistance (Collard 2003). Moreover, important new information has become available in a large randomised trial (de Jonge 2003) that was the first to be formally designed to reliably assess the occurrence of antibiotic resistance by randomising ICUs rather than patients and monitoring the units for more than two years after the inception of treatment use: de Jonge et al reported that no patients were colonised with meticillin‐resistant staphylococcus aureus, only 1% was colonised with vancomicin‐resistant enterococcus and in 16% and 26% (in SDD and control patients, respectively) colonisation with gram negative bacteria resistant to ceftazidime, ciprofloxacin, imipenem, polymyxin E and tobramycin occurred (de Jonge 2003).
We believe that insufficient data on cost‐effectiveness and antibiotic resistance should stimulate future research rather than preventing the adoption of a seemingly effective intervention. The impact of antibiotic prophylaxis on costs has so far been evaluated only rarely and, more importantly, in an improper way (the analysis being essentially based on comparisons of lengths of stay and computation of charges due to antibiotic use). A proper economic analysis is, on the other hand, likely to be difficult in a highly specialised setting such as an ICU, given that it is hard to quantify the relative contribution of single procedures.
Implications for research.
The number of RCTs so far conducted on antibiotic prophylaxis is substantial and provides sufficient statistical power to detect a moderate but humanly worthwhile effect of the treatment on mortality. According to this systematic review, the combination of topical and systemic antibiotics should be the standard against which new treatments should be tested. A logical next step for future trials would be the comparison of this protocol against a regimen based on a systemic antimicrobial only; only six trials included in this review chose this as their study design. However, it is unlikely that one or more even large conventional trial can satisfy the concerns of those who are afraid that antimicrobial resistance may occur as a consequence of widespread use of antibiotics. However, the trial by de Jonge (de Jonge 2003) has shown that trials with innovative designs are possible and that they allow for a more reliable assessment of the occurrence of antibiotic resistance.
At the current stage of development of this intervention there does not seem to be a commercial interest by pharmaceutical companies to support further trials. Similarly, the intensivists' community seems rather sceptical about the merits of the intervention and it is not willing to embark on new, properly designed and conducted studies. A systematic analysis of the quality and reliability of existing data on resistance might, in this sense, be important to get a more comprehensive view of the yield of the treatment. Such a review should be carried out even though it is highly likely that the necessary harms data are not available in published trials.
What's new
| Date | Event | Description |
|---|---|---|
| 20 March 2012 | Amended | Byline citation updated. |
History
Review first published: Issue 3, 1997
| Date | Event | Description |
|---|---|---|
| 19 May 2011 | New search has been performed | Searches conducted |
| 13 March 2009 | New search has been performed | Searches conducted. |
| 13 March 2009 | New citation required but conclusions have not changed | One study has been included in this update (Camus 2005). Two studies, whose data were reported in congress proceedings (Lenhart 1994) and were unpublished (Stoutenbeek 2), have been replaced by Krueger 2002 and Stoutenbeek 2007 which are their published versions in peer‐reviewed journals. One study (Jacobs 1995) included in the previous version of this review as a personal contact with the principal investigator, has been excluded due to lack of feedback from the trial author. To date, this study has not been published. |
| 30 January 2008 | Amended | Converted to new review format |
| 5 September 2003 | New search has been performed | Searches conducted. Updated review published Issue 4, 2002 |
| 5 December 1999 | New search has been performed | Searches conducted. Review published Issue 3, 1997 |
| 5 December 1995 | New search has been performed | Searches conducted. Updated review published Issue 1, 2004 |
Acknowledgements
This systematic review would have not been possible without the continuous and enthusiastic support of most of the trials investigators. They collaborated in the different phases of this review up to the publication of our earlier review (D'Amico 1998) by providing information on the design and conduct of their studies, checking the accuracy of the data before the final analysis, attending a meeting where preliminary results were presented and, finally, reviewing earlier drafts of the manuscript. They are listed below: M Abele‐Horn 1997 (Ludwig‐Maximilians‐Universitat, Munich, Germany); SJA Aerdts 1991 (Sophia Hospital, Zwolle, The Netherlands); P Blair 1991, B J Rowlands, H Webb and K Lowry (Royal Victoria Hospital, Belfast, Northern Ireland); JP Boland 1991, D Sadler, A Stewart and J Pollock (Health Science Center Charlestone, West Virginia University, West Virginia, USA); C Brun‐Buisson 1989 (Hopital Henry Mondor, Creteil, France); FB Cerra 1992 (University of Minnesota Hospital and Clinic, Minneapolis, USA); FR Cockerill 1992 and RL Thompson (Mayo Clinic, Rochester, Minnesota, USA); M Ferrer 1992 and A Torres (Servei de Pneumologia, Hospital Clinic, Barcelona, Spain); RG Finch 1991, P Tomlinson and G Rocker (Nottingham City Hospital, Nottingham, United Kingdom); H Gastinne 1992 (on behalf of the French study group on Selective Decontamination of the Digestive Tract ‐ France); P Gaussorgues 1991 (Hopital Eduoard Herriot, Lyon, France); B Georges 1994 (Hopital de Rangueil, Toulouse, France); JMJ Hammond 1992, PD Potgieter (Groote Schuur Hospital, Cape Town, South Africa); S Jacobs (University Hospital of Wales, Cardiff, United Kingdom); S Jacobs and M Zuleika (Riyadh Armed Forces Hospital, Riyadh, Saudi Arabia); AJH Kerver 1988 (Sint Franciskus Hospital, Rotterdam, Utrecht, The Netherlands); AM Korinek 1993 (Hopital Pitie‐Salpetriere, Paris, France); AN Laggner 1994 (Vienna General Hospital, Vienna, Austria); FP Lenhart 1994 (University of Munich, Germany); W Lingnau (Leopold‐Franzens‐Universitat Innsbruck, Innsbruck, Austria); A Martinez‐Pellus and J Rodriguez‐Rolda 1990 (University Hospital Virgen de la Arrixaca, El Palmar, Murcia, Spain); M Palomar 1997 (Hospital Vall d'Hebron, Barcelona, Spain); J Pugin 1991 and P Suter (University Hospital, Geneva, Switzerland); C Martin, B Quinio 1995 and J Albanese (Hopital Nord, Marseilles, France); LA Rocha 1992 (Hospital Juan Canalejo, La Coruna, Spain); M Sanchez‐Garcia 1992 (Hospital PPE Asturias, Alcala de Henares, Spain); CP Stoutenbeek 1994 (Academisch Ziekenhuis, Universiteit van Amsterdam, Amsterdam, The Netherlands); C Ulrich 1989 and J E Harinck‐De Weerd (Westeinde Hospital, The Hague, The Netherlands); K Unertl 1987 (Klinikum Grosshadern, Munich, Germany); J Verhaegen and C Verwaest (University Hospital Gasthuisberg, Leuven, Belgium); J Wiener 1995 (Michael Reese Hospital, Chicago, USA); R Winter 1992 (Queens Medical Centre University Hospital, Nottingham, United Kingdom).
This review was originally initiated at the request of the French Society of Intensive Care in preparation for the consensus conference on Selective Decontamination of the Digestive Tract (Paris, December 1991) and led to the first publication in 1993 (SDD Group 1993). It was then continued and updated between 1993 and 1998 through resources made available from the Mario Negri Institute, Milan, Italy and an unrestricted grant provided by Hoechst Marion Roussel Italy, the sponsors had no control on the protocol preparation, data analysis and manuscript review and their support was sought after the decision of undertaking the review by the review authors. Since 2004 the review has been updated without any specific research grant attached using institutional resources of the review authors. Finally, the review authors wish to thank the following referees for commenting on the 2009 updated review: Janet Wale, Tim Kenealy, Max Bulsara, and Jenny Doust.
Appendices
Appendix 1. Embase.com search strategy
1. 'respiratory tract infection'/exp 2. 'respiratory tract infection':ti,ab OR 'respiratory tract infections':ti,ab 3. 'pneumonia'/exp 4. pneumon*:ti,ab 5. hap:ti,ab OR vap:ti,ab 6. bronchopneumonia*:ti,ab OR pleuropneumonia*:ti,ab 7. 'bronchitis'/exp 8. bronchit*:ti,ab OR bronchiolit*:ti,ab 9. 'pharyngitis'/exp 10. pharyngit*:ti,ab 11. 'tracheitis'/exp 12. tracheit*:ti,ab 13. #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 14. 'intensive care unit'/exp 15. icu:ti,ab OR 'critical care':ti,ab OR 'intensive care':ti,ab OR 'burn unit':ti,ab OR 'burn units':ti,ab OR 'care unit':ti,ab OR 'care units':ti,ab OR 'recovery room':ti,ab OR 'recovery rooms':ti,ab 16. 'critical illness'/exp 17. 'critically ill':ti,ab OR 'critical illness':ti,ab 18. 'ventilator'/exp 19. ventilator*:ti,ab 20. 'artificial ventilation'/exp 21. respirator*:ti,ab 22. #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR # 21 23. #13 AND #22 24. 'ventilator associated pneumonia'/exp 25. 'ventilator associated pneumonia':ti,ab 26. #24 OR #25 27. #23 OR #26 28. 'antibiotic prophylaxis'/exp 29. 'antibiotic agent'/exp 30. antibiotic*:ti,ab 31. #28 OR #29 OR #30 32. #27 AND #31 33. 'randomized controlled trial'/exp 34. 'controlled clinical trial'/exp 35. 'single blind procedure'/exp 36. 'crossover procedure'/exp 37. random*:ti,ab OR placebo*:ti,ab OR factorial*:ti,ab OR crossover*:ti,ab OR assign*:ti,ab OR allocat*:ti,ab OR volunteer*:ti,ab OR 'double blind':ti,ab OR 'double blinding':ti,ab OR 'double blinded':ti,ab OR 'single blind':ti,ab OR 'single blinded':ti,ab OR 'single blinding':ti,ab 38. #33 OR #34 OR #35 OR #36 OR #37 39. #32 AND #38
Data and analyses
Comparison 1. Topical plus systemic versus no prophylaxis.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Overall mortality | 17 | 4075 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.75 [0.65, 0.87] |
| 2 Mortality according to quality of allocation concealment | 17 | 4075 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.75 [0.65, 0.87] |
| 2.1 Adequate | 10 | 3336 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.77 [0.66, 0.90] |
| 2.2 Not adequate | 7 | 739 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.67 [0.48, 0.93] |
| 3 Mortality according to blinding of the studies | 17 | 4075 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.75 [0.65, 0.87] |
| 3.1 Double‐blind | 4 | 1013 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.63 [0.48, 0.83] |
| 3.2 Open | 13 | 3062 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.80 [0.68, 0.95] |
| 4 RTIs | 16 | 3024 | Odds Ratio (M‐H, Random, 95% CI) | 0.28 [0.20, 0.38] |
| 5 RTIs according to quality of allocation concealment | 16 | 3024 | Odds Ratio (M‐H, Random, 95% CI) | 0.28 [0.20, 0.38] |
| 5.1 Adequate | 9 | 2335 | Odds Ratio (M‐H, Random, 95% CI) | 0.36 [0.27, 0.47] |
| 5.2 Not adequate | 7 | 689 | Odds Ratio (M‐H, Random, 95% CI) | 0.19 [0.10, 0.37] |
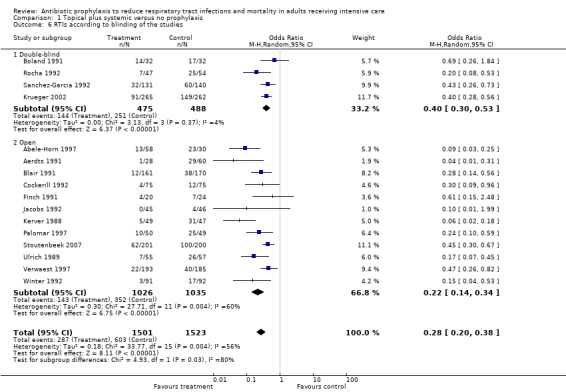
| 6 RTIs according to blinding of the studies | 16 | 3024 | Odds Ratio (M‐H, Random, 95% CI) | 0.28 [0.20, 0.38] |
| 6.1 Double‐blind | 4 | 963 | Odds Ratio (M‐H, Random, 95% CI) | 0.40 [0.30, 0.53] |
| 6.2 Open | 12 | 2061 | Odds Ratio (M‐H, Random, 95% CI) | 0.22 [0.14, 0.34] |
1.1. Analysis.
Comparison 1 Topical plus systemic versus no prophylaxis, Outcome 1 Overall mortality.
1.2. Analysis.
Comparison 1 Topical plus systemic versus no prophylaxis, Outcome 2 Mortality according to quality of allocation concealment.
1.3. Analysis.
Comparison 1 Topical plus systemic versus no prophylaxis, Outcome 3 Mortality according to blinding of the studies.
1.4. Analysis.
Comparison 1 Topical plus systemic versus no prophylaxis, Outcome 4 RTIs.
1.5. Analysis.
Comparison 1 Topical plus systemic versus no prophylaxis, Outcome 5 RTIs according to quality of allocation concealment.
1.6. Analysis.
Comparison 1 Topical plus systemic versus no prophylaxis, Outcome 6 RTIs according to blinding of the studies.
Comparison 2. Topical versus control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
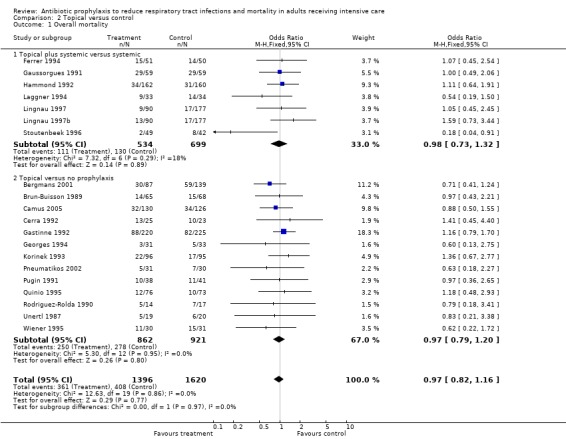
| 1 Overall mortality | 20 | 3016 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.82, 1.16] |
| 1.1 Topical plus systemic versus systemic | 7 | 1233 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.98 [0.73, 1.32] |
| 1.2 Topical versus no prophylaxis | 13 | 1783 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.79, 1.20] |
| 2 Mortality according to quality of allocation concealment | 20 | 3016 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.82, 1.16] |
| 2.1 Adequate | 2 | 139 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.64 [0.27, 1.52] |
| 2.2 Not adequate | 18 | 2877 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.83, 1.18] |
| 3 Mortality according to blinding of the studies | 20 | 3016 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.98 [0.82, 1.16] |
| 3.1 Double‐blind | 15 | 2601 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.83, 1.20] |
| 3.2 Open | 5 | 415 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.56, 1.37] |
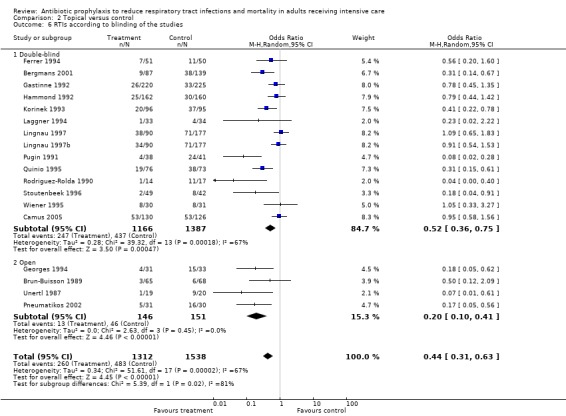
| 4 RTIs | 18 | 2850 | Odds Ratio (M‐H, Random, 95% CI) | 0.44 [0.31, 0.63] |
| 4.1 Topical plus systemic versus systemic | 6 | 1115 | Odds Ratio (M‐H, Random, 95% CI) | 0.79 [0.56, 1.13] |
| 4.2 Topical versus no prophylaxis | 12 | 1735 | Odds Ratio (M‐H, Random, 95% CI) | 0.34 [0.21, 0.55] |
| 5 RTIs according to quality of allocation concealment | 18 | 2850 | Odds Ratio (M‐H, Random, 95% CI) | 0.44 [0.31, 0.63] |
| 5.1 Adequate | 1 | 91 | Odds Ratio (M‐H, Random, 95% CI) | 0.18 [0.04, 0.91] |
| 5.2 Not adequate | 17 | 2759 | Odds Ratio (M‐H, Random, 95% CI) | 0.46 [0.32, 0.66] |
| 6 RTIs according to blinding of the studies | 18 | 2850 | Odds Ratio (M‐H, Random, 95% CI) | 0.44 [0.31, 0.63] |
| 6.1 Double‐blind | 14 | 2553 | Odds Ratio (M‐H, Random, 95% CI) | 0.52 [0.36, 0.75] |
| 6.2 Open | 4 | 297 | Odds Ratio (M‐H, Random, 95% CI) | 0.20 [0.10, 0.41] |
2.1. Analysis.
Comparison 2 Topical versus control, Outcome 1 Overall mortality.
2.2. Analysis.
Comparison 2 Topical versus control, Outcome 2 Mortality according to quality of allocation concealment.
2.3. Analysis.
Comparison 2 Topical versus control, Outcome 3 Mortality according to blinding of the studies.
2.4. Analysis.
Comparison 2 Topical versus control, Outcome 4 RTIs.
2.5. Analysis.
Comparison 2 Topical versus control, Outcome 5 RTIs according to quality of allocation concealment.
2.6. Analysis.
Comparison 2 Topical versus control, Outcome 6 RTIs according to blinding of the studies.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Abele‐Horn 1997.
| Methods | Randomised controlled study Blinding: Open Randomisation method: list block randomised assignments maintained by the main investigator Accrual period: not available | |
| Participants | Eligibility criteria: intubation within 24 hrs of admission, expected ventilation for at least four days, first microbial culture within 36 hrs of admission Exclusion criteria: transfer from other hospitals, evidence of infection, prior antibiotic therapy, ARDS, leucopenia, myelosuppression Patients enrolled in the study: 125; 37 patients were excluded leaving 88 patients for analysis Percentage of ventilated patients: 100% ICU length of stay, mean: 19.3 days Type of admission diagnosis: surgical unscheduled = 16% trauma = 84% Severity score on admission: APACHE II mean = 17, ISS not available Percentage of immunocompromised patients:not available Percentage of patients treated with systemic antibiotic therapy (not stated by protocol) in the first three days: not available Stress ulcer prophylaxis applied: sucralfate 1 g x four to all patients | |
| Interventions | Group A, Treatment:
‐ polymyxin 100 mg, tobramycin 80 mg, amphotericin B 500 mg applied orally four times a day as a 2% paste during the ICU stay
‐ cefotaxime 2 g x 3 iv x three days Group B, CTR: ‐ No prophylaxis Antibiotic prophylaxis was performed only for abdominal, orthopedic and neurologic surgery |
|
| Outcomes | Respiratory infections (acquired pneumonia):
Diagnosis was based on Clinical Pulmonary Infection Score as defined by Pugin 1991: new pulmonary infiltrate on X‐ray, increasing amount of tracheal secretions containing > 3 x 104 granulocytes/mcl and at least two of the following: temperature > 38.5°C, WBC > 12,000/mm3 or < 4,000/mm3, decrease in PaO2 requiring an increase in FiO2. Besides a bacteriological confirmation is required: tracheal aspirates yielding bacteria > 104 CFU/ml and granulocytes > 10/field Mortality: in ICU |
|
| Notes | Data about 37 excluded patients are not available | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Aerdts 1991.
| Methods | Randomised study with three arms (one treatment arm versus two control arms) Blinding: outcome assessor Randomisation method: sealed envelopes, permuted block method. Accrual period: May 86 to Sept 87 | |
| Participants | Eligibility criteria: expected ventilation for at least five days, inclusion within 24 hrs of admission Exclusion criteria: age < 16 yrs, pregnancy, allergy to one of the component of the regimen Patients enrolled in the study: 88 Percentage of ventilated patients: 100% ICU length of stay, median: 16 days Type of admission diagnosis: medical = 40% surgical scheduled = 6% surgical unscheduled = 20% trauma = 34% Severity score on admission: APACHE II mean = 21.8, ISS not available Percentage of immunocompromised patients: 4.6% Percentage of patients treated with systemic antibiotic therapy (not stated by protocol) in the first three days: Treatment = 35% CTR = 80% Stress ulcer prophylaxis applied: antiacids until enteral feeding was possible | |
| Interventions | Group A, CTR 1: ‐ No prophylaxis, infections of unknown origin were treated with ampicillin+gentamicin Group B, CTR 2: ‐ No prophylaxis, infections of unknown origin were treated with cefotaxime+gentamicin and metronidazole if indicated. Group C, Treatment: ‐ polymyxin E 200 mg, norfloxacin 50 mg, amphotericin B 500 mg applied enterally four times a day and, as a 2% paste, to the oropharynx until extubation ‐ cefotaxime 500 mg x 3 iv x five days. Infections of unknown origin were treated as group B | |
| Outcomes | Respiratory infections (acquired pneumonia and tracheobronchitis):
Diagnosis of tracheobronchitis was based on: positive culture of the tracheal aspirate and a gram stain showing many leukocytes as well as the causative organism, associated with two of the following: temperature > 38°C, WBC > 12000/mm3, purulent tracheal aspirate
Diagnosis of pneumonia was based on: a new and persistent pulmonary infiltrate on X‐ray and criteria of tracheobronchitis Mortality: in ICU |
|
| Notes | The study presents two control groups that are considered as a whole in the meta‐analysis Personal contact with the main investigator provided data about 32 patients who were excluded from the published paper (16 early extubation, seven early deaths, five protocol violation, three other, one unknown); these data are considered in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Bergmans 2001.
| Methods | Randomised, placebo‐controlled study. Blinding: double blind. | |
| Participants | Elegibility criteria: intubation within 24 hrs of admission and need for mechanical ventilation with an expected duration > two hours Esclusion criteria: age < 16 yrs. Patients enrolled in the study: 226 Percentage of ventilated patients: 100% ICU length of stay, median treatment group: 13 days; median control A group: 15 days, median control B group: 12 days Type of admission diagnosis: Medical = 35%, Surgery = 39%, Trauma = 19%, Neurology = 6%, Other = 1%. Severity score on admission: APACHE II mean = 21.4, ISS not available Percentage of immuncompromised patients: 2% Percentage of patients treated with systematic antibiotic therapy at admission: Treatment: 47% CTR = 42% Stress ulcer prophylaxis applied: Treatment = 61% Control = 76% | |
| Interventions | Group A, Treatment:
Orabase with 2% gentamicin, 2% colistin and 2% vancomycin
Orabase was applied in the buccal cavities on a gloved finger every six hrs.
The application of Orabase was started within 24 h of intubation.
Application of treatment was limited to 21 days. Group B, CTR1 no prophylaxis ‐ this group was studied in ICU in which there was the presence of patients receiving topical antimicrobial prophylaxis Group C: CTR2 no prophylaxis This control group was studied in ICU in which where no topical antimicrobial prophylaxis was used |
|
| Outcomes | Ventilator‐associated pneumonia (VAP); diagnosis of VAP was established on the basis of positive quantitative cultures from BAL (cutoff point >= 104 colony‐forming units [cfu]/ml) or PSB (cutoff point >= 103 cfu/ml), or a positive blood culture unrelated to another source of infection, or a positive culture from pleural fluid in the absence of previous pleural instrumentation. Mortality: in hospital |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Blair 1991.
| Methods | Randomised study Blinding: Open. Randomisation method: sealed envelopes. Accrual period: Sept. 1988 to Jan 1990 | |
| Participants | Eligibility criteria: all admitted patients who do not fulfil the exclusion criteria
Exclusion criteria: patients discharged within 48 hrs of ICU admission; admission from CCU; patients expected to die after six hrs of ICU admission; patients with discharge anticipated within 48 hrs but remaining more than 48 hrs; drug overdose; security patients; age < 18 yrs; patients not randomised within six hrs of admission; readmission to ICU; burns; miscellaneous Patients enrolled in the study: 331 Percentage of ventilated patients: 93% Length of stay in ICU, median: five days Type of admission diagnosis: medical = 14% surgical scheduled = 33% surgical unscheduled = 13% trauma = 40% Severity score on admission: APACHE II mean = 14.4, ISS mean = 24.8 Percentage of immunocompromised patients: 1.8% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 42% CTR = 74% Stress ulcer prophylaxis applied: all patients received ranitidine iv plus antiacid therapy if gastric pH was low |
|
| Interventions | Group A, CTR:
‐ Standard antibiotic therapy (no prophylaxis) Group B, Treatment: ‐ polymyxin 100 mg, tobramycin 80 mg, amphotericin B 500 mg applied enterally four times a day and, as a 2% gel, to the oropharynx ‐ cefotaxime 50 mg/kg/day iv x four days |
|
| Outcomes | Respiratory infections (pneumonia acquired after 48 hrs). Diagnosis of infection was based on the fulfilment of Criteria I or Criteria II.
Criteria I: temperature > 38.5°C on two separate occasion, WBC > 12 x 109/l or < 4 x 109 and a new pulmonary infiltrate on X‐ray.
Criteria II: temperature > 37.5°C, a new pulmonary infiltrates on X‐ray, purulent sputum and drop in PaO2 Mortality: in ICU |
|
| Notes | Personal contact with the main investigator provided data about 75 patients who were excluded from the published paper for short length of stay; these data are considered in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Boland 1991.
| Methods | Randomised, placebo‐controlled study Blinding: double blind Randomisation method: computer generated randomisation directed by the pharmacy department Accrual period: Apr 89 to Mar 91 | |
| Participants | Eligibility criteria: all multiple traumatised patients, intubated at the time of admission and likely to stay intubated at least five days
Exclusion criteria: patients who did not remain intubated for five days Patients enrolled in the study: 64 Percentage of ventilated patients: 100% Length of stay in ICU, median: eight days Type of admission diagnosis: trauma = 100% Severity score on admission: APACHE II mean = 16.8, ISS not available Percentage of immunocompromised patients: 0% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 0% CTR = 0% Stress ulcer prophylaxis applied: H2‐blockers or sucralfate (78%) |
|
| Interventions | Group A, CTR:
‐ Placebo Group B, Treatment: ‐ polymyxin 100 mg, tobramycin 80 mg, nystatin 1,600,000 units applied enterally four times a day and, as a 2% paste plus 60,000 units of nystatin, to the oropharynx until extubation or discharge ‐ cefotaxime 1 g x 3 iv for the first three days |
|
| Outcomes | Respiratory infections (acquired pneumonia and tracheobronchitis).
Diagnosis of infection was based on:
positive sputum culture for bacteria, fever > 38°C and leukocytosis (> 10,000 WBC/mm3 of blood) Mortality: in ICU |
|
| Notes | Personal contact with the main investigator provided data about 23 patients who were excluded from the published paper (20 early extubations, three early deaths); these data are considered in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Brun‐Buisson 1989.
| Methods | Randomised trial Blinding: Open Randomisation method: odd and even birth year technique Accrual period: Apr 87 to May 87 | |
| Participants | Eligibility criteria: patients with an admission SAPS > 2 and staying in the ICU more than 48 hrs Exclusion criteria: patients with severe neutropenia routinely receiving oral antibiotic prophylaxis Patients enrolled in the study: 133 Percentage of ventilated patients: 59% Length of stay in ICU, median: 3.5 days Type of admission diagnosis: medical 75% surgical unscheduled 23% trauma 2% Severity score on admission: SAPS mean = 10.4, ISS not available Percentage of immunocompromised patients: 12.8% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 41% CTR = 53% Stress ulcer prophylaxis applied: none | |
| Interventions | Group A, Treatment:
‐ polymyxin E 50 mg, neomycin 1 g, nalidixic acid 1 g, applied orally and enterally four times a day until discharge
‐ Oropharyngeal disinfectant in intubated patients Group B, CTR: ‐ Oropharyngeal disinfectant in intubated patients |
|
| Outcomes | Respiratory infections (pneumonia acquired in the ICU or within 48 hrs from discharge)
Diagnosis of infection was based on:
purulent sputum or tracheal aspirate associated with a new and persistent pulmonary infiltrate on X‐ray and the culture of at least 109 CFU/l from a protected wedged catheter sample of bronchial aspirate, temperature > 38°C, WBC > 10 x 109 Mortality: in ICU |
|
| Notes | Setting: acute and intermediate areas of a medical ICU Personal contact with the main investigator provided data about 47 patients who were excluded from the published paper (seven early deaths, one transferred, 39 other); these data are considered in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | High risk | C ‐ Inadequate |
Camus 2005.
| Methods | Randomised trial Blinding: double Randomisation method: performed by computer Accrual period: April 1996 to October 1998 | |
| Participants | Elegibility criteria: adults intubated for < 48 hrs and likely to require mechanical ventilation for > 48 hrs Exclusion criteria: patients with SAPS II > 80 and life expectancy of < 48 hrs resulting from brain death of a palliative treatment, a polymorphonuclear count of < 500 cells/mm3, severe diarrhoea and anyone who had received either a prior decontamination regimen or was already participating in another ongoing clinical trial. Patients enrolled: 256 Pecentage of ventilated patients: not reported Length of stay in ICU: not reported Type of admission diagnosis: home/emergency department = 43%, hospital ward = 57% Severity score on admission: median SAPS II = 46 Percentage of immunocompromised patients: 3.9% Percentage of patients treated with systemic antibiotic therapy (not stated in protocol) in the first three days: none Stress ulcer prophylaxis applied: not reported | |
| Interventions | Group A ‐ Treatment: solution containing 15 mg/ml polymyxin E and 10 mg/ml tobramycin Group B ‐ Control: placebo | |
| Outcomes | Respiratory infections: acquired infections Mortality: in ICU | |
| Notes | The study is a four arm, 2 x 2 factorial design. In this review we considered only two arms comparing SDD regimen versus placebo | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Cerra 1992.
| Methods | Randomised, placebo‐controlled study Blinding: double blind Randomisation method: sealed envelopes Accrual period: Sept 1988 to Jan 1990 | |
| Participants | Eligibility criteria: admission within 48 hrs from surgery, trauma or other acute event, expected stay at least five days, hypermetabolism (VO2 > 140 ml/m2 or urinary nitrogen excretion > 10 g/day) without progressive MOSF (normal transaminases, stable bilirubin and creatinine)
Exclusion criteria: Cirrhosis, allergy to used drugs, chemo‐radiotherapy, progressive MOSF, gastrointestinal leak or fistula Patients enrolled in the study: 48 Percentage of ventilated patients: not available ICU length of stay, median: not available Type of admission diagnosis: surgical = 96% trauma = 4% Severity score on admission: not available Percentage of immunocompromised patients: not available Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: not available Stress ulcer prophylaxis applied: not available |
|
| Interventions | Group A, Treatment:
‐ norfloxacin 500 mg x 3, nystatin one million U x 4 applied enterally until discharge Group B, CTR: ‐ Placebo |
|
| Outcomes | Respiratory infections: not possible to evaluate Mortality |
|
| Notes | Personal contact with the main investigator provided data about two patients who were excluded from the published paper for short length of stay); these data are considered in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Cockerill 1992.
| Methods | Randomised study. Intention‐to‐treat Blinding: outcome assessor Randomisation method: randomisation table at a remote site in the pharmacy Accrual period: 1986 to 1989 | |
| Participants | Eligibility criteria: all patients admitted to the mixed ICU if their condition suggested a prolonged stay (> three days), age > 18 yrs
Exclusion criteria: age < 18 yrs, pregnancy, allergy to one of the component of the regimen, infections, antibiotic therapy 24 hrs before randomisation Patients enrolled in the study: 150 Percentage of ventilated patients: 85% ICU length of stay, median: 4.5 days Type of admission diagnosis: medical = 18% surgical scheduled = 27% surgical unscheduled = 21% trauma = 34% Severity score on admission: APACHE II mean = 19.4, ISS mean 24.3 Percentage of immunocompromised patients: 4% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 75% CTR = 80% Stress ulcer prophylaxis applied: H2‐blockers (80%) |
|
| Interventions | Group A, CTR:
‐ No prophylaxis Group B, Treatment: ‐ gentamycin 80 mg, polymyxin B 100 mg, nystatin 2,000,000 units, applied enterally and as a 2% paste to the oropharynx four times a day during the ICU stay ‐ cefotaxime 1 g/8 hrs iv for the first three days |
|
| Outcomes | Respiratory infections (only acquired infections)
Diagnosis of pneumonia was based on clinical and laboratory criteria:
a new or progressive pulmonary infiltrate, purulent secretions, isolation of a potential pathogen and fever with or without leukocytosis.
Diagnosis of tracheobronchitis was based on:
the presence of increased purulent endotracheal secretions requiring frequent suctioning and the presence of a potential pathogen Mortality: in hospital |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
de Jonge 2003.
| Methods | Randomised study Blinding: Open Randomisation method:computer‐generated random‐number codes kept in sealed envelopes | |
| Participants | Eligibility criteria: adult patients admitted to ICU: with an expected stay of at least 72 hours and an expected duration of mechanical ventilation of at least 48 hours
Exclusion criteria:
previous admission in ICU within three months iper sensitivity to study medication, pregnancy and perceived imminent death Number of patients enrolled in the study: 934 Percentage of ventilated patients: 85% Length of stay in ICU: median SDD group = 6.8 days control group = 8.5 days Type of admission diagnosis: medical: 41% surgical urgent: 25% surgical elective: 34% Severity score at admission: APACHE II mean = 18.7 SAPS II in SDD group mean = 17.9 SAPSII in control group mean = 17.1 Percentage of immunocompromised patients SDD group = 2.4% control group = 1.7% Information on prescribed antibiotics per 1,000 patients available in the main publication No stress ulcer prophylaxis by protocol |
|
| Interventions | SDD group: topical plus systemic treatment
Topical: oral paste containing 2% polymyxin E, 2% tobramycin, 2% amphotericin
500 mg amphotericin B through gastric tubes
Systemic: cefotaxime 1000 mg four times daily for four days Control group: No antibiotic prophylaxis; antibiotic treatment based on clinical needs |
|
| Outcomes | Colonisation, antibiotic resistance Mortality: in ICU and hospital | |
| Notes | Patients were allocated to either an SDD or a control unit to prevent cross‐colonisation between SDD and ICU control patients. Standard care was the same in the two units | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Ferrer 1994.
| Methods | Randomised, placebo‐controlled study Blinding: double blind Randomisation method: computer generated table Accrual period: Jan 91 to Mar 92 | |
| Participants | Eligibility criteria: all mechanically ventilated patients expected to remain intubated for more than three days
Exclusion criteria: patients with HIV‐related diseases or treated with antineoplastic chemotherapy as well as patients who received transplants, extubation or death within 72 hrs Number of patients enrolled in the study: 101 Percentage of ventilated patients:100% Length of stay in ICU, median: 7.5 days Type of admission diagnosis: medical 66% surgical scheduled 6.9% surgical unscheduled 6.9% trauma = 19.8% Severity score admission: SAPS mean = 12.1, ISS not available Percentage of immunocompromised patients: 0% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: not available treatment = 73% CTR = 74% Stress ulcer prophylaxis applied: sucralfate except in patients with paralytic ileus or with upper gastrointestinal bleeding, who were treated with ranitidine |
|
| Interventions | Group A, Treatment:
‐ polymyxin E 100 mg, tobramycin 80 mg, amphotericin B 500 mg applied enterally and, as a 2% paste, to the oropharynx four times a day until extubation or death
‐ cefotaxime 2 g/day iv for the first four days or others if required Group B, CTR: ‐ Placebo ‐ cefotaxime 2 g/day iv for the first four days or others if required* *patients infected on admission received adequate antibiotic treatment instead of cefotaxime |
|
| Outcomes | Respiratory infections (pneumonia acquired after four days of mechanical ventilation)
Diagnosis of infection was based on clinical criteria plus brush or BAL confirmation.
Clinical criteria: new or progressive pulmonary X‐ray infiltrate for at least 48 hrs, purulent tracheal secretions, temperature > 38.5 °C and leukocytosis >= 12 x 109 WBC/l or leukopenia <= 4 x 109 Mortality: in ICU |
|
| Notes | Personal contact with the main investigator provided data about 21 patients who were excluded from the published paper (14 early extubations, six early deaths, one transfer); these data are considered in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Finch 1991.
| Methods | Randomised study Blinding: Open Randomisation method: sealed envelopes. Randomisation series made available to the hospital Pharmacy only Accrual period: Aug 87 to Sept 89 | |
| Participants | Eligibility criteria: all patients whose length of stay was > 60 hrs, age > 16 yrs
Exclusion criteria: none Number of patients enrolled in the study: 49 Percentage of ventilated patients: not available Length of stay in ICU: not available Type of admission diagnosis: medical 59% surgical scheduled 27% surgical unscheduled 10% trauma = 4% Severity score on admission: SAPS mean = 10.5, ISS not available Percentage of immunocompromised patients: 22% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 58% CTR = 68% Stress ulcer prophylaxis applied: not available |
|
| Interventions | Group A, Treatment:
‐ polymyxin B 100 mg, gentamycin 120 mg, amphotericin B 500 mg applied enterally and, as a 2% paste, to the oropharynx four times a day
‐ cefotaxime 1 g x 3 iv for the first four days Group B, CTR: ‐ Conventional antibiotic therapy |
|
| Outcomes | Respiratory infections (acquired pneumonia)
Diagnosis of pneumonia was based on:
tracheal aspirate with numerous leukocytes associated with any of the following: a single bacterial species with a growth density > 105 CFU, diagnosis of septicaemia, clinical signs of pulmonary infections (fever, leukocytosis and appropriate radiological findings) Mortality: in ICU |
|
| Notes | Personal contact with the main investigator provided information about mortality on five patients who were excluded from the published paper (one early extubation, two early deaths, one transferring, one unknown); these data are considered in the analysis. Data about respiratory infections in patients excluded from published paper are not available | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Gastinne 1992.
| Methods | Randomised, placebo‐controlled, multicenter (15 ICUs) study Intention to treat Blinding: double blind Randomisation method: a randomised list of consecutive treatment assignments, performed separately in each unit. Accrual period: Feb 90 to Jun 90 | |
| Participants | Eligibility criteria: all patients > 15 yrs who required mechanical ventilation and with intubation performed no more than 48 hrs before randomisation
Exclusion criteria: patients with ventilation for less than 24 hrs, drug or alcohol overdose, neutropenia (WBC < 500/mm3), SAPS > 24 or GCS < 4, chronic degenerative central nervous system disease or spinal cord injury above level of C4, acute severe enteropathy, pregnancy, participation in another ongoing clinical trial, refusal of consent, patients with conditions in which survival was strongly related to status on admission Number of patients enrolled in the study: 445 Percentage of ventilated patients: 100% Length of stay in ICU, median: 12 days Type of admission diagnosis: medical 72% surgical scheduled 3% surgical unscheduled 10% trauma = 15% Severity score on admission: SAPS mean = 13.5, ISS not available GCS mean = 11.7 Percentage of immunocompromised patients: 18% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 89% CTR = 84% Stress ulcer prophylaxis applied: sucralfate (43% patients), H2‐blockers (13% patients) |
|
| Interventions | Group A, CTR:
‐ Placebo Group B, Treatment: ‐ tobramycin 80 mg, polymyxin E 100 mg, amphotericin B 100 mg applied enterally and, as a 2% paste, to the oropharynx four times a day throughout the period of ventilation |
|
| Outcomes | Respiratory infections (pneumonia diagnosed within 48 hrs and acquired):
Diagnosis of infection was based on:
purulent tracheal aspirate, temperature > 38.5°C, peripheral leukocytosis (> 10,000 WBC/mm3 of blood) and a new and persistent infiltrate on the chest film. Brushing was recommended but not mandatory. Mortality: in hospital |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Gaussorgues 1991.
| Methods | Randomised study. Intention to treat Blinding: Open Randomisation method: odd‐even numbers Accrual period: Sept 88 to Sept 89 | |
| Participants | Eligibility criteria: all patients admitted to the ICU, who required mechanical ventilation and inotropic drugs for haemodynamic reasons
Exclusion criteria: neutropenia Patients enrolled in the study: 118 Percentage of ventilated patients: 100% ICU length of stay: not available Type of admission diagnosis: medical = 83% surgical scheduled = 17% (all patients were infected on admission) Severity score on admission: SAPS mean = 17.5 Percentage of immunocompromised patients: not available Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 100% CTR = 100% Stress ulcer prophylaxis applied: sucralfate 4 g to all patients |
|
| Interventions | Group A, Treatment:
‐ polymyxin E 36 mg, gentamycin 80 mg, Vancomycin 50 mg, amphotericin B 500 mg applied enterally four times a day until extubation
‐ amphotericin B, Clorexidine applied orally four times a day
‐ systemic antibiotic therapy Group B, CTR: ‐ amphotericin B, Clorexidine applied orally four times a day ‐ systemic antibiotic therapy |
|
| Outcomes | Respiratory infections: not possible to evaluate Mortality: in ICU |
|
| Notes | All patients were infected on admission Data about respiratory infections are not provided | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | High risk | C ‐ Inadequate |
Georges 1994.
| Methods | Randomised, placebo‐controlled study Blinding: open Randomisation method: sealed envelopes Accrual period: Jun 1990 to April 1992 | |
| Participants | Eligibility criteria: Polytrauma, expected mechanical ventilation for at least four days, age > 18 years
Exclusion criteria: Hypersensitivity to the used agents, protocol violation, obesity, ventilation < four days, patients on mechanical ventilation two days before admission, severe maxillo‐facial lesions Patients enrolled in the study: 138, but only 64 patients were analysed Length of stay in ICU, mean: 33 days Percentage of ventilated patients: 100%. Length of ventilation, mean: 16 days Type of admission diagnosis: trauma 100% Severity score on admission: APACHE II mean = 15, ISS = 41 Percentage of immunocompromised patients: 0% Percentage of patients treated with systemic antibiotic therapy in the first 3 days: almost 100% Stress ulcer prophylaxis: H2‐blockers |
|
| Interventions | Group A:
Treatment: polymyxin E 75 mg, Netilmicin 150 mg, amphotericin B 400 mg applied enterally four times a day and, as a 2% paste, to the oropharynx until extubation
‐ Systemic antibiotic prophylaxis was free Group B: CTR ‐ Placebo ‐ Systemic antibiotic prophylaxis was free |
|
| Outcomes | Respiratory infections (acquired pneumonia)
Diagnosis of infection was based on:
Fever > 38.5 °C, leukocytosis > 12000/mm3, new infiltrates in the chest X‐rays, purulent pulmonary secretions, positive bacteriologic findings (> 10^3 CFU/ml) obtained through a protected catheter Mortality: in ICU and hospital |
|
| Notes | Antibiotic prophylaxis was free and almost all patients of both groups were treated with systemic antibiotics 74 potentially eligible patients were excluded from analysis; it is not evident if this happened before or after randomisation; these data are not available | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Hammond 1992.
| Methods | Randomised, placebo‐controlled study Blinding: double blind Randomisation method: computer generated random numbers. Accrual period: Jan 89 to Dec 90 | |
| Participants | Eligibility criteria: expected intubation for longer than 48 hrs and stay in ICU for at least five days
Exclusion criteria: hypersensitivity to the study drugs, patients with asthma, drug overdose and patients admitted electively after surgery Number of patients enrolled in the study: 322 Percentage of ventilated patients: 100% Length of stay in ICU, median: 11 days Type of admission diagnosis: medical 55% surgical scheduled 3% surgical unscheduled 11% trauma = 31% Severity score on admission: APACHE II mean = 13.9, ISS mean = 28.7 Percentage of immunocompromised patients: 0.8% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 54% CTR = 58% Stress ulcer prophylaxis applied: none, H2‐blockers only to high risk patients |
|
| Interventions | Group A, Treatment:
‐ polymyxin E 100 mg, tobramycin 80 mg, amphotericin B 500 mg applied enterally and, as a 2% gel, to the oropharynx four times a day until 48 hrs after extubation
‐ cefotaxime 1 g x 3 iv for the first three days to patients untreated on admission Group B, CTR: ‐ Placebo ‐ cefotaxime 1 g x 3 iv for the first three days to patients untreated on admission |
|
| Outcomes | Respiratory infections (infections acquired after 48 hrs)
Diagnosis of pneumonia was based on:
a new infiltrate on X‐ray and purulent bronchial secretions with many leukocytes, temperature > 38°C, WBC > 1010/l, substantial number of organism on gram stain with a pure growth culture from tracheal aspirate, deterioration of gas exchange of > 2 kPa
Diagnosis of bronchial infection was based on:
all the previous criteria except the X‐ray changes Mortality: in hospital |
|
| Notes | Personal contact with the main investigator provided data on 82 patients who were excluded and separately considered in the published paper (78 short stay, three protocol violation, one unknown); these data are considered in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Jacobs 1992.
| Methods | Randomised study Blinding: open Randomisation method: sealed envelopes. Accrual period: Jul 89 to Aug 90 | |
| Participants | Eligibility criteria: expected stay in ICU > three days
Exclusion criteria: none Patients enrolled in the study: 91 Percentage of ventilated patients: 100% ICU length of stay, median: unknown Type of admission diagnosis: medical = 25% surgical = 57% trauma = 18% (high percentage of neurologic and neurosurgical patients 52%) Severity score on admission: APACHE II mean = 17.5, ISS not available Percentage of immunocompromised patients: unknown Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: next to 100% Stress ulcer prophylaxis applied: policy of maintenance a low gastric pH, H2‐blockers only if peptic ulcer or steroid therapy (33%), sucralfate 4 g to all patients not on enteral feeding |
|
| Interventions | Group A, Treatment:
‐ polymyxin E 100 mg, tobramycin 80 mg, amphotericin B 500 mg applied orally and enterally four times a day until extubation
‐ cefotaxime 50 mg/kg/day iv x four days Group B, CTR: ‐ No prophylaxis |
|
| Outcomes | Respiratory infections (acquired pneumonia)
Diagnosis of infection was based on:
alveolar infiltrates on two or more chest X‐rays, moderate or copious purulent tracheal aspirate, rectal temperature > 38.4°C, leucocytosis > 13 x 109/l, a heavy growth of organisms from tracheal aspirate with a high polymorphonuclear leucocytes/epithelial cell ratio Mortality |
|
| Notes | Almost 100% of patients received systemic antibiotic therapy on admission Personal contact with the main investigator provided data about 12 patients who were excluded from the published paper (11 short stay in ICU, one HIV+); these data are considered in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Kerver 1988.
| Methods | Randomised study Blinding: open Randomisation method: odd/even numbers Accrual period: Jan 85 to May 86 | |
| Participants | Eligibility criteria: all patients admitted to the surgical ICU who required care > five days
Exclusion criteria: none Patients enrolled in the study: 96 Percentage of ventilated patients: 100% ICU length of stay, not available Type of admission diagnosis: surgical = 60% trauma = 28% other = 12% Severity score on admission: APACHE II mean = 14.8, ISS not available Percentage of immunocompromised patients: not available Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: about 85% Stress ulcer prophylaxis applied: not available |
|
| Interventions | Group A, Treatment:
‐ polymyxin E 200 mg, tobramycin 80 mg, amphotericin B 500 mg applied orally and enterally four times a day
‐ Oral disinfectant
‐ cefotaxime 50 to 70 mg/kg/day iv x five to seven days Group B, CTR: ‐ Oral disinfectant |
|
| Outcomes | Respiratory infections (primary pneumonia and pneumonia acquired after 48hs)
Diagnosis of infection was based on X‐ray findings and the presence of three of the following criteria on the same day: rectal temperature > 38.5°C for at least 12 hrs, WBC count > 10 x 103 or < 4 x 103/mcl, at least 3% band forming granulocytes, unexplained decrease in platelet count < 100,000/mcl, deterioration of renal function due to acute tubular necrosis, unexplained decrease in systolic blood pressure of > 30 mmHg, progressive respiratory failure Mortality |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | High risk | C ‐ Inadequate |
Korinek 1993.
| Methods | Randomised, placebo‐controlled, dual‐centre study Blinding: double blind Randomisation method: randomisation performed by the hospital pharmacist on each unit separately Accrual period: Mar 89 to Sep 90 | |
| Participants | Eligibility criteria: all comatosed patients with emergency admission to two neurosurgical ICUs and intubated within 24 hrs for at least five days, age > 16 yrs
Exclusion criteria: age < 16 yrs, known immunosuppression, antibiotic treatment during the two weeks preceding ICU admission, serious injury of oropharyngeal mucosa or epistaxis, abnormal chest X‐ray on admission, extubation or infection occurring within the first five days of neurosurgical care Number of patients enrolled in the study: 191 Percentage of ventilated patients: 100% Length of stay in ICU, mean: 26 days Type of admission diagnosis: surgical scheduled 11% surgical unscheduled 39% trauma 50% Severity score on admission: SAPS mean = 10.9, ISS not available Percentage of immunocompromised patients: 0% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 0% CTR = 0% Stress ulcer prophylaxis applied: sucralfate (32%), antiacids (14%), H2‐blockers (20%) until enteral feeding was started |
|
| Interventions | Group A, Treatment:
‐ polymyxin E 100 mg, tobramycin 80 mg, amphotericin B 500 mg applied enterally and, as a 2% paste, to the oropharynx four times a day for 15 days
‐ Vancomicin x os Group B, CTR: ‐ Placebo The non‐absorbable antibiotics were discontinued if any infection requiring a parenteral antibiotic treatment occurred and at the time of patient's extubation |
|
| Outcomes | Respiratory infections (pneumonia acquired after five days)
Diagnosis of infection was based on:
fever > 38.5°C, leukocytosis > 12,000 cells/mm3, purulent sputum, new and persistent infiltrates on chest X‐ray and a culture of > 103 CFU/ml obtained with either brush or plugged telescoping catheter Mortality: in ICU |
|
| Notes | Setting: neurosurgical ICU Personal contact with the main investigator provided data about 68 patients who were excluded from the published paper (early extubation, early death, protocol violation, transferring, other); these data are considered in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Krueger 2002.
| Methods | Randomised, double blind, placebo‐controlled, double centre study Randomisation method: computer‐generated randomisation Accrual period: Apr 89 to Mar 91 | |
| Participants | Eligibility criteria: expected stay in ICU > two days and at least one risk factor for infection Exclusion criteria: patients expected to die within 48 hrs or randomisation was not achieved within 12 hrs after admission to ICU. Patients enrolled in the study: 546, 19 patients were excluded leaving 527 patients for analysis Percentage of ventilated patients: not available ICU length of stay: 10 days for both groups Type of admission diagnosis: surgical Severity score on admission: APACHE II mean = 20, ISS not available Percentage of immunocompromised patients: not available Percentage of patients treated with systemic antibiotic therapy (not stated by protocol) in the first three days: not available Stress ulcer prophylaxis applied: sucralfate to all patients | |
| Interventions | Group A, Treatment:
‐ polymyxin B 50 mg, gentamycin 80 mg, applied nasally, orally and enterally four times a day during the ICU stay
‐ ciprofloxacin 400 mg x 2 iv x four days to uninfected patients Group B, CTR: ‐ Placebo applied nasally, orally and enterally ‐ Placebo iv to uninfected patients |
|
| Outcomes | Respiratory infections (acquired pneumonia) Mortality in ICU |
|
| Notes | Information about accrual period and severity score was reported on an abstract previously published | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Laggner 1994.
| Methods | Randomised, placebo‐controlled study Blinding: double blind Randomisation method: computer generated randomisation in time blocks. Open Accrual period: Aug 87 to Nov 90 | |
| Participants | Eligibility criteria: expected ventilation for five days, age > 18 yrs and < 80 yrs, acute onset of respiratory failure
Exclusion criteria: age < 18 yrs and > 80 yrs, bleeding of the nasopharynx and of the upper gastrointestinal tract on admission, stress ulcer prophylaxis with other drug therapy than sucralfate, mechanical ventilation for less than five days, patients on enteral nutrition or with known allergy to sucralfate or gentamicin Number of patients enrolled in the study: 88, but only 67 patients were analysed Percentage of ventilated patients: 100% Length of stay in ICU, mean: 28.8 days Type of admission diagnosis: medical 88% surgical scheduled 9% surgical unscheduled 1% trauma = 2% Severity score on admission: APACHE II mean = 23, ISS not available Percentage of immunocompromised patients: 15% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: 100% Stress ulcer prophylaxis applied: sucralfate |
|
| Interventions | Group A, Treatment:
‐ gentamycin 40 mg, amphotericin B 100 mg applied to the oropharynx four times a day until extubation
‐ Oropharyngeal disinfectant
‐ aminopenicillin and clavulanic acid or other appropriate regimens Group B, CTR: ‐ Placebo ‐ Amphotericin B 100 mg ‐ Oropharyngeal disinfectant ‐ Aminopenicillin and clavulanic acid or other appropriate regimens |
|
| Outcomes | Respiratory infections (acquired pneumonia):
Diagnosis of infection was based on:
appearance of a new infiltrate on the chest film with concomitant tracheal colonisation, fever > 38°C and > 15,000 or < 5,000 WBC/mm3 of blood Mortality: in ICU |
|
| Notes | Data about 21 patients who were excluded from the published paper (18 short mechanical ventilation, three early enteral nutrition) are not available | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Lingnau 1997.
| Methods | Randomised, placebo‐controlled study with three arms (one control arm and two treatment arms). Intention to treat Blinding: double blind Randomisation method: continuous random numbers assigned to blinded study drugs or vehicle by Biometric department. Accrual period: Aug 89 to Jan 94 | |
| Participants | Eligibility criteria: non infected trauma patients, age > 18 yrs, expected ventilation for at least two days, expected ICU stay for at least three days, ISS > 16 and < 74, inclusion within 24 hrs of admission
Exclusion criteria: isolated brain injury, prior antibiotic treatment, history of infection Patients enrolled in the study: 357 Percentage of ventilated patients: 100% ICU length of stay, mean: 20 days Type of admission diagnosis: trauma = 100% Severity score on admission: APACHE II mean = 15.6, ISS mean = 35.2 Percentage of immunocompromised patients: 0% Percentage of patients treated with systemic antibiotic therapy (not stated by protocol) in the first three days: treatment 1 = 2% treatment 2 = 2% CTR = 6% Stress ulcer prophylaxis applied: free |
|
| Interventions | Group A, Treatment 1:
‐ polymyxin E 100 mg, tobramycin 80 mg, amphotericin B 500 mg applied orally and enterally four times a day during the ICU stay
‐ ciprofloxacin 200 mg x 2 iv, for four days Group C, CTR: ‐ Placebo ‐ ciprofloxacin 200 mg x 2 iv, for four days |
|
| Outcomes | Respiratory infections (acquired pneumonia):
Diagnosis of infection was based on:
concomitant occurrence of purulent sputum, positive cultures of bronchial secretions and deterioration of lung function Mortality: in ICU |
|
| Notes | This three arm study has been split in two comparisons; the control group C has been used twice: comparison Lingnau a (group A versus group C) comparison Lingnau b (group B versus group C) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Lingnau 1997b.
| Methods | see Lingnau 1997 | |
| Participants | see Lingnau 1997 Only two groups of patients, group B and C, are considered in this comparison, totaling 267 patients | |
| Interventions | Group B, Treatment 2:
‐ polymyxin E 100 mg, ciprofloxacin 50 mg, amphotericin B 500 mg applied orally and enterally four times a day during the ICU stay
‐ ciprofloxacin 200 mg x 2 iv, for four days Group C, CTR: ‐ Placebo ‐ ciprofloxacin 200 mg x 2 iv, for four days |
|
| Outcomes | see Lingnau 1997 | |
| Notes | see Lingnau 1997 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | D ‐ Not used |
Palomar 1997.
| Methods | Randomised, multicentric (10 ICUs) study with three arms (one treatment arm and two control arms; one control arm was excluded from meta‐analysis because it was the only one receiving sucralfate) Blinding: open Randomisation method: sealed envelopes. Accrual period: Jul 89 to Aug 91 | |
| Participants | Eligibility criteria: patients requiring mechanical ventilation for more than four days, not infected at the time of entry and not receiving antibiotic therapy
Exclusion criteria: ARDS, leukopenia, pregnancy Number of patients enrolled in the study: 97 Percentage of ventilated patients: 100% Length of stay in ICU, median 10 days Type of admission diagnosis: medical 40% surgical 10% trauma 50% Severity score on admission: APACHE II mean = 16.8, ISS not available Percentage of immunocompromised patients: 0% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 0% CTR = 6% Stress ulcer prophylaxis applied: sucralfate to one control group (excluded from meta‐analysis), antiacids or H2‐blockers to the two other groups |
|
| Interventions | Group A, CTR 1:
‐ No prophylaxis Group B, Treatment: ‐ polymyxin E + B 100 mg, tobramycin 80 mg, amphotericin B 500 mg applied enterally and, as a 2% paste, to the oropharynx four times a day until extubation ‐ cefotaxime 1 g x 3 iv for the first four days Group C*, CTR 2: ‐ cefotaxime 1 g x 3 iv for the first four days ‐ sucralfate * This group was excluded from analysis because it was the only one receiving sucralfate |
|
| Outcomes | Respiratory infections (acquired infections)
Diagnosis of pneumonia was based on the CDC criteria of 1980 (clinical or radiologic suspicion with: purulent sputum, organism isolated from blood culture, isolation of pathogen from tracheal aspirate, brush or biopsy. Bacteriologic evaluation was performed with brush or BAL in 50% of patients)
Diagnosis of tracheobronchitis was based on the CDC criteria of 1980 Mortality: in ICU |
|
| Notes | Personal contact with the main investigator provided data about 16 patients who were excluded from the published paper (seven early extubations, five early deaths, three protocol violation, one other); these data are considered in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Pneumatikos 2002.
| Methods | Randomised, placebo‐controlled Blinding: outcome assessor Randomisation method: not stated | |
| Participants | Elegibility criteria: patients with multiple trauma admitted to the intensive care unit who required intubation and had an expected time for mechanical ventilation exceeding five days
Absence of cardiopulmonary disease, negative chest radiography, and a PaO2/FIO2 ratio higher than 300 mmHg Patients enrolled in the study: 61 Percentage of ventilated patients: 100% ICU length of stay, median: Treatment = 16 days Control = 23 days Type of admission diagnosis: trauma = 100% Severity score on admission: APACHE II treatment = 18.1 control = 19.1 Percentage of immunocompromised patients: not stated Percentage of patients treated with systemic antibiotic therapy: not stated Stress ulcer prophylaxis applied: H2 blockers or sucralfate Treatment = 26% Control = 19% |
|
| Interventions | Group A, treatment:
polymyxin 73 mg,
tobramycin 73 mg, amphotericin 500 ml in 500 ml 0.9 saline solution at an infusion rate of 2 ml/hr in the subglottic area for the entire period of the study Group B CTR: placebo |
|
| Outcomes | Ventilator associated pneumonia (VAP) defined as presence of new and persistent pulmonary infiltrates in addition to two of the following criteria: body temperature > 38.3 °C, leukocytes/mm3) or leukopenia (< 4000 leukocytes/mm3) and purulent tracheal secretions. The diagnosis of VAP was confirmed by quantitative cultures. Mortality: not specified |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Pugin 1991.
| Methods | Randomised, placebo‐controlled study Blinding: double blind Randomisation method: sealed envelopes Accrual period: Apr 89 to Nov 89 | |
| Participants | Eligibility criteria: all adult patients admitted to the surgical ICU, at high risk of developing pneumonia and intubated for more than 48 hrs
Exclusion criteria: organ transplantation Number of patients enrolled in the study: 79 Percentage of ventilated patients: 100% Length of stay in ICU, mean 13.8 days Type of admission diagnosis: medical 11% surgical scheduled 11% surgical unscheduled 22% trauma 56% Severity score on admission: APACHE II mean = 15.2, ISS not available Percentage of immunocompromised patients: not available Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 46% CTR = 53% Stress ulcer prophylaxis applied: sucralfate (61%), ranitidine (11%) |
|
| Interventions | Group A, Treatment:
‐ polymyxin B sulfate 150 mg, neomycin sulfate 1 g, vancomycin hydrochloride 1 g applied as a solution to the retropharynx six times a day within 24 hrs after intubation until extubation or death Group B, CTR: ‐ Placebo Withdrawal from the study was possible at any time if the treating physicians estimated that there was any problem related to administration of the drugs or side effects |
|
| Outcomes | Respiratory infections (pneumonia acquired after 48 hrs): Pneumonia are defined by the "clinical pulmonary infections score" (CPIS) greater or equal to seven during the course of intubation and that remained elevated (=7) for at least three days (i.e. for two consecutive measurements) Mortality: in hospital |
|
| Notes | Personal contact with the main investigator provided data about 27 patients who were excluded from the published paper (20 early extubations, seven early deaths); these data are considered in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Quinio 1995.
| Methods | Randomised, placebo‐controlled study. Intention to treat Blinding: double blind Randomisation method: randomisation made by the Pharmacy's Service according to computer generated random numbers. Accrual period: Jan 91 to Jan 93 | |
| Participants | Eligibility criteria: trauma patients intubated within 24 hrs and ventilated for more than 48 hrs, ICU stay > five days and decontamination for more than four days
Exclusion criteria: age < 16 yrs, antibiotic treatment in the week precedent to ICU admission, pregnancy Number of patients enrolled in the study: 149 Percentage of ventilated patients: 100% Length of stay in ICU, mean = 20.5 days Type of admission diagnosis: medical 2% trauma 98% Severity score on admission: SAPS mean = 11.2, ISS mean = 31.3 GCS mean 6.5 Percentage of immunocompromised patients: 0% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 35% CTR = 26% Stress ulcer prophylaxis applied: sucralfate until enteral feeding was effective, H2‐blockers in high risk patients |
|
| Interventions | Group A,Treatment:
‐ polymyxin E 100 mg, gentamycin 80 mg, amphotericin B 500 mg applied enterally and in the nares and, as a 2% paste, to the oropharynx four times a day until extubation or starting of enteral nutrition Group B, CTR: ‐ Placebo |
|
| Outcomes | Respiratory infections (pneumonia acquired after 48 hrs): Diagnosis of infection was based on:
purulent tracheal aspirate, fever > 38.5°C, leukocytosis > 10,000 WBC/mm3, new and persistent infiltrate on chest X‐ray Mortality: in ICU |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Rocha 1992.
| Methods | Randomised, placebo‐controlled study Blinding: double blind Randomisation method: made by the Pharmacy's service according to computer generated random numbers Accrual period: Sept 89 to Oct 90 | |
| Participants | Eligibility criteria: expected mechanical ventilation for more than three days, stay in ICU more than five days
Exclusion criteria: infection or strong suspicion of this at the start of ventilation, antibiotic treatment in the previous seven days, neutropenia (WBC < 500/mm3) and fever, pregnancy, history of hypersensitivity to the topical agents Number of patients enrolled in the study: 151 Percentage of ventilated patients: 100% Length of stay in ICU, median eight days Type of admission diagnosis: medical 28% surgical scheduled 3% surgical unscheduled 1% trauma 68% Severity score on admission: APACHE II mean = 16.3, ISS not available, GCS mean = nine Percentage of immunocompromised patients: 0.7% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 0% CTR = 0% Stress ulcer prophylaxis applied: H2‐blockers and antiacids |
|
| Interventions | Group A, Treatment:
‐ polymyxin E 100 mg, tobramycin 80 mg, amphotericin B 500 mg applied enterally and, as a 2% paste, to the oropharynx four times a day
‐ cefotaxime 6 g/day iv for the first four days Group B, CTR: ‐ Placebo ‐ No systemic prophylaxis |
|
| Outcomes | Respiratory infections (acquired pneumonia):
Diagnosis of infection was based on:
purulent pulmonary secretions, new infiltrates in the chest X‐ray and one of the following: fever/hypothermia, leukocytosis/leukopenia, positive physical examination, drop in arterial partial oxygen pressure. Bacteriologic diagnosis, even if performed (with brush in few patients), was not essential Mortality: in ICU |
|
| Notes | Personal contact with the main investigator provided mortality data about 50 patients who were excluded from the published paper (15 early extubations, 31 early deaths, two protocol violation, two other); these data are considered in the analysis. Data about respiratory infections in excluded patients are not available | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Rodriguez‐Rolda 1990.
| Methods | Randomised, placebo‐controlled, dual‐center study Blinding: double blind Randomisation method: odd and even numbers Accrual period: Jun 88 to Dec 88 | |
| Participants | Eligibility criteria: patients intubated an mechanically ventilated for more than 72 hrs
Exclusion criteria: patients whose chest X‐rays was difficult to interpret, with suspected inflammatory images during the first 72 hrs, patients ventilated for less time Number of patients enrolled in the study: 31 Percentage of ventilated patients: 100% Length of stay in ICU, median 13.5 days Type of admission diagnosis: medical 39% surgical scheduled 16% surgical unscheduled 3% trauma 42% Severity score on admission: APACHE II mean = 17.1, ISS not available Percentage of immunocompromised patients: 0% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 36% CTR = 35% Stress ulcer prophylaxis applied: sucralfate or alkaline agents plus ranitidine according to a randomised open protocol |
|
| Interventions | Group A, Treatment:
‐ polymyxin E, Tobramicin or Netilmicin, amphotericin B and antiseptic applied enterally and, as a 2% paste, to the oropharynx four times a day
‐ Antiseptic Group B, CTR: ‐ Placebo ‐ Antiseptic |
|
| Outcomes | Respiratory infections (pneumonia acquired after 72 hrs): Diagnosis of infection was based on the presence of at least one in each category of criteria:
A) Clinical criteria: temperature > 38°C, purulent bronchorrhoea, leukocytosis > 15,000 WBC/mm3, increased alveolar‐arterial oxygen gradient;
B) Radiologic criteria: new and persistent infiltrate;
C) Bacteriologic criteria: quantitative culture of tracheal aspirates > 103 CFU/ml (in six patients either bronchoscopy or a telescoped catheter were used to obtain the sample) Mortality: in ICU |
|
| Notes | Personal contact with the main investigator provided data about three patients who were excluded from the published paper (two early deaths, one other); these data are considered in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | High risk | C ‐ Inadequate |
Sanchez‐Garcia 1992.
| Methods | Randomised, placebo‐controlled, multicentric (five ICUs) study Blinding: double blind Randomisation method: sealed envelopes. Accrual period: not available | |
| Participants | Eligibility criteria: expected ventilation for longer than 48 hrs, age > 16 yrs
Exclusion criteria: death or extubation before 48 hrs, pregnancy, allergy to study antibiotics, organ transplantation, absence or contraindication to nasogastric tube Number of patients enrolled in the study: 271 Percentage of ventilated patients: 100% Length of stay in ICU, median 13 days Type of admission diagnosis: medical 70% surgical scheduled 3% surgical unscheduled 9% trauma 18% Severity score on admission: APACHE II mean = 26.6, ISS not available Percentage of immunocompromised patients: 4.4% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 70% CTR = 69% Stress ulcer prophylaxis applied: each group was randomised to receive either sucralfate or H2‐blockers |
|
| Interventions | Group A, Treatment:
‐ polymyxin E 100 mg, gentamycin 80 mg, amphotericin B 500 mg applied orally and enterally four times a day until extubation
‐ Ceftriaxone 2 g/day iv x three days to uninfected patients Group B, CTR: ‐ Placebo ‐ Systemic placebo to uninfected patients |
|
| Outcomes | Respiratory infections (early and late acquired pneumonia):
Diagnosis of infection was based on:
new and persistent infiltrate on chest X‐ray and three of the following: temperature > 38.5°C, leukocytosis > 12,000 WBC/mm3 or leukopenia < 3,000 WBC/mm3, purulent tracheal aspirate with growth of a potentially pathogenic micro‐organism Mortality: in ICU |
|
| Notes | Personal contact with the main investigator provided data about 45 patients who were excluded from the published paper (12 early extubations, 12 early deaths, 17 protocol violation, two transferring, two other); these data are considered in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Stoutenbeek 1996.
| Methods | Randomised, placebo‐controlled study Blinding: double blind. Randomisation method: closed envelope method (the code was known by the pharmacist only). Accrual period: Nov 84 to Aug 86 | |
| Participants | Eligibility criteria: all patients admitted to the surgical ICU with blunt trauma and an HTI‐ISS > 18, age > 18 yrs
Exclusion criteria: patients mechanically ventilated for less than five days or discharged from ICU within seven days and with an HTI‐ISS < 18 after 24 hrs Number of patients enrolled in the study: 91 Percentage of ventilated patients: 100% Length of stay in ICU, mean = 15 days Type of admission diagnosis: trauma 100% Severity score on admission: APACHE II mean = 10.6, HTI‐ISS mean = 35.1 Percentage of immunocompromised patients: 0% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 0% CTR = 0% Stress ulcer prophylaxis applied: none except for patients with history of preexisting ulcer or on H2‐blockers |
|
| Interventions | Group A, Treatment:
‐ polymyxin E 100 mg, tobramycin 80 mg, amphotericin 500 mg applied enterally and, as a 2% paste, to the oropharynx four times a day until ICU discharge
‐ cefotaxime 50 to 100 mg/kg/day iv for the first five days Group B, CTR: ‐ Placebo ‐ cefotaxime 50 to 100 mg/kg/day iv for the first five days The blinded medication was discontinued and topical prophylaxis was started when a patient developed MOSF not responding to conventional therapy. The code was not broken and the patient was further evaluated |
|
| Outcomes | Respiratory infections (tracheobronchitis and pneumonia ‐ early and late infections)
Diagnosis of infection was based on clinical criteria: temperature > 38.5°C, WBC > 12.5 x 109/l or leukopenia < 4 x 10^9/l, purulent secretions or X‐ray changes and significant growth of bacteria Mortality: in ICU |
|
| Notes | Data about 32 patients who were initially excluded (25 early extubations, four early deaths, three other) are considered in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Stoutenbeek 2007.
| Methods | Randomised, multicenter study. Intention to treat Blinding: open Randomisation method: randomisation lists prepared by the Biometrical Department and supplied with sealed envelopes Accrual period: Oct 91 to Jun 94 | |
| Participants | Eligibility criteria: patients admitted within 24 hrs after nonpenetrating blunt trauma with an HTI‐ISS >= 16, necessitating mechanical ventilation, age > 18 yrs
Exclusion criteria: previous antibiotic use for more than three days at study entry, allergy to cefotaxime, referred patients from other hospital or secondary admissions with trauma occurred > 24 hrs before Number of patients enrolled in the study: 405, but 401 patients were analysed Percentage of ventilated patients: 100% Median length of ICU stay: SDD = 13 days, CTR = 12 days Median duration of mechanical ventilation: SDD = nine days, CTR = eight days Type of admission diagnosis: trauma 100% Severity score on admission ‐ APACHE II median: SDD = 15, CTR = 14 and HTI‐ISS median: SDD = 34, CTR = 29 Percentage of immunocompromised patients: 0% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 46% CTR = 88% Stress ulcer prophylaxis applied: sucralfate, H2‐blockers, omeprazole; no sucralfate |
|
| Interventions | Group A, Treatment:
‐ polymyxin E, tobramycin, amphotericin B administered through the nasogastric tube and applied to the buccal mucosa four times a day until discharge
‐ cefotaxime 1 g every six hours for four days Group B, CTR: ‐ Standard antibiotic prophylaxis used in each centres (no fluoroquinolones) |
|
| Outcomes | Primary: Mortality from infection or multiple organ failure in ICU or up to two weeks after discharge Secondary: incidence of infection, multiple organ failure and antibiotic usage The maximum observation period was three months Patients dying within 24 hours after injury or dying from craniocerebral trauma were excluded Diagnosis of pneumonia was based on any of the following: presence of a new and progressive pulmonary infiltrate on chest X‐ray for >= 48 hrs, purulent tracheal aspirate, fever > 38.5°C, leukocytosis > 12,000/ml or leukopenia < 4000/ml Diagnosis of tracheobronchitis was based on the same criteria except for the radiographic changes Mortality: in ICU or up to two weeks after discharge |
|
| Notes | four patients were excluded from the final analysis after randomisation: two because they did not fulfil the inclusion criteria, the data for one patient were not available and one was lost to follow‐up after the 7th day | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Ulrich 1989.
| Methods | Randomised, placebo‐controlled study Blinding: open Randomisation method: sealed envelopes containing a random code for clusters of four patients Accrual period: Oct 86 to Sep 87 | |
| Participants | Eligibility criteria: patients expected to stay in the ICU more than five days and ventilated more than 48 hrs
Exclusion criteria: patients who died within 24 hrs after randomisation Number of patients enrolled in the study: 112 Percentage of ventilated patients: about 80% Length of stay in ICU, median = 10 days Type of admission diagnosis: medical 34% surgical scheduled 19% surgical unscheduled 31% trauma 16% Severity score on admission: SAPS mean = 11.7, ISS mean = 36.9 Percentage of immunocompromised patients: 3% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 83% CTR = 81% Stress ulcer prophylaxis applied: not available |
|
| Interventions | Group A,Treatment:
‐ polymyxin E 100 mg, norfloxacin 50 mg, amphotericin B 500 mg, applied enterally and, as a 2% paste, to the oropharynx four times a day
‐ Trimethoprim 500 mg iv Group B, CTR: ‐ Placebo |
|
| Outcomes | Respiratory infections (acquired pneumonia):
Diagnosis of infection was based on clinical and radiologic signs of pulmonary infiltrations with fever and leukocytosis and a dense growth in cultures of sputum of tracheal aspirate Mortality: in ICU |
|
| Notes | Personal contact with the main investigator provided data about 12 patients who were excluded from the published paper (early death); these data are considered in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Unertl 1987.
| Methods | Randomised study Blinding: outcome assessor Randomisation method: blocked randomisation scheme and the sealed envelope technique. Blind Accrual period: May 84 to Jan 85 | |
| Participants | Eligibility criteria: all patients admitted to the ICU with: intubation within 24 hrs after the onset of an acute disease or surgery, expected ventilation > six days, interval between intubation and first microbiologic culture < 36 hrs
Exclusion criteria: Patients with infection, systemic antibiotic treatment, respiratory distress syndrome, leucopenia and myelosuppression on admission, renal failure Number of patients enrolled in the study: 39 Percentage of ventilated patients: 100% Length of stay in ICU: not available Type of admission diagnosis: medical 52%, surgical 15%, trauma 33% Severity score on admission: SAPS mean = 12.5, GCS (75% of patients have GCS < 7) Percentage of immunocompromised patients: not available Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: not available Stress ulcer prophylaxis applied: H2‐blockers to all patients and antiacids if pH < 4 |
|
| Interventions | Group A, Treatment:
‐ polymyxin B 50 mg, gentamycin 80 mg, applied orally, nasally and enterally four times a day until extubation
‐ Amphoterycin B 300 mg applied orally four times a day Group B, CTR: ‐ No prophylaxis |
|
| Outcomes | Respiratory infections (acquired pneumonia):
Diagnosis of infection was based on:
new 'definite' infiltrate on chest X‐ray together with increasing amounts of purulent tracheobronchial secretion containing > 3 x 104 granulocytes/mcl and at least two of the following: new febrile spikes > 38.5°C, blood leukocyte count > 12000/mcl or < 4000/mcl, decrease of PaO2 requiring an increase of the FiO2 of at least 15% to maintain oxygen tension.
'Definite' is an infiltrate confirmed by two blind independent radiologists and not reversible after chest physiotherapy Mortality: in ICU |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Verwaest 1997.
| Methods | Randomised study with three arms (one control arm and two treatment arms) Blinding: open Randomisation method: sealed envelopes with computer generated random numbers Accrual period: Sept 89 to Mar 91 | |
| Participants | Eligibility criteria: expected ventilation > 48 hrs
Exclusion criteria: age < 18 yrs, pregnancy, recent organ transplantation, serious granulocytopenia (<= 500 WBC/mm3), ventilation < 48 hrs, death before 48 hrs, missing of essential data in the clinical or bacteriological dossier Number of patients enrolled in the study: 660 (only two groups of patients, A and B, are considered in this comparison, totaling 440 patients) Percentage of ventilated patients: 100% Length of stay in ICU, mean = 19.6 days Type of admission diagnosis: medical 10%, surgical 67% trauma 23% Severity score on admission: APACHE II mean = 18.1, ISS not available Percentage of immunocompromised patients: not available Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment one = 34% treatment twp = 31% CTR = 34% Stress ulcer prophylaxis applied: sucralfate 2 g x 4 |
|
| Interventions | Group A, CTR:
‐ No prophylaxis, antibiotic therapy was used only if an infection was suspected Group B, Treatment 1: ‐ Ofloxacin 200 mg x 2, Amphoterycin B 500 mg x 4 applied enterally and, as a 2% paste, to the oropharynx four times a day until discharge ‐ Ofloxacin 200 mg iv x four days |
|
| Outcomes | Respiratory infections (pneumonia acquired after 48 hrs):
Diagnosis of infection was based on:
Fever > 38.5°C, leukocytosis > 10,000 cells/mcl, luxuriant growth of potentially pathogenic micro‐organisms in culture of bronchial aspirate, new and persistent infiltrate on chest X‐ray Mortality: in ICU |
|
| Notes | Personal contact with the main investigator provided mortality data about 82 patients who were excluded (33 early deaths, 49 other); these data are considered in the analysis.Data about respiratory infections in excluded patients are not available | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Wiener 1995.
| Methods | Randomised, placebo‐controlled study Blinding: double blind Randomisation method: random number table in blocks of six patients Accrual period: eight months | |
| Participants | Eligibility criteria: expected intubation for more than 48 hrs, inclusion within 18 hrs of intubation, age > 18 yrs
Exclusion criteria: refusal to consent, allergy to one of the components of the regimen, active inflammatory bowel disease Patients enrolled in the study: 121, but 60 patients were excluded leaving 61 patients for analysis Percentage of ventilated patients: 100% Length of stay in ICU, mean: 11.3 days Type of admission diagnosis: not available Severity score on admission: APACHE II mean = 27.2, ISS not available Percentage of immunocompromised patients: > 5% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 93% CTR = 81% Stress ulcer prophylaxis applied: H2‐blockers to most patients |
|
| Interventions | Group A, Treatment:
‐ polymyxin E 100 mg, gentamycin 80 mg, nystatin 2,000,000 UI applied enterally four times a day and, as a 2% paste, to the oropharynx until extubation or tracheostomy Group B, CTR: ‐ Placebo |
|
| Outcomes | Respiratory infections (pneumonia acquired after 48 hrs):
Diagnosis of infection was based on the presence of the following: persistence of a new or progressive infiltrate on chest‐film, fever > 38.5°C and/or leukocytosis > 12,000/mm3, growth of > 103 bacteria from a quantitative culture of lower respiratory tract secretions obtained with a blind protected catheter Mortality: in ICU |
|
| Notes | 60 patients were excluded after randomisation; data are not available | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Winter 1992.
| Methods | Randomised study Blinding: open. Randomisation method: sealed envelopes based on a computer generated table of random numbers. Accrual period: Jul 88 to May 90 | |
| Participants | Eligibility criteria: patients likely to remain in the ICU for at least 48 hrs
Exclusion criteria: allergy to the antibiotics used, age > 85 yrs, pregnancy Patients enrolled in the study: 183 Percentage of ventilated patients: 92% Length of stay in ICU, median = four days Type of admission diagnosis: medical 40% surgical scheduled 10% surgical unscheduled 37% trauma 13% Severity score on admission: APACHE II mean = 15.3, ISS mean = 26.2 Percentage of immunocompromised patients: 2.2% Percentage of patients treated with systemic antibiotic therapy (not stated in the protocol) in the first three days: treatment = 47% CTR = 64% Stress ulcer prophylaxis applied: all CTR patients received sucralfate; H2‐blockers were used in patients of both groups with peptic ulcer or pancreatitis |
|
| Interventions | Group B, CTR:
‐ Conventional infections treatment and prophylaxis Group C, Treatment: ‐ polymyxin E 100mg, tobramycin 80mg, amphotericin B 500 mg applied enterally and, as a 2% gel, to the oropharynx four times a day ‐ Ceftazidime 50mg/kg/day iv x three days |
|
| Outcomes | Respiratory infections (pneumonia acquired after 48 hrs): Diagnosis of infection was based on:
temperature > 38.5°C two times in 24 hrs, WBC < 4 or > 12 x 109/l, positive BAL, two of the following: new pulmonary infiltrates on chest X‐ray, purulent sputum, increase of 15% in FiO2 to maintain previous oxygenation Mortality: in hospital |
|
| Notes | Few patients were excluded after randomisation; data are not available | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
APACHE Acute Physiology and Chronic Health Evaluation ARDS Acute Respiratory Distress Syndrome BAL Broncho‐Alveolar‐Lavage CCU Coronary Care Unit CDC Centre for Disease Control CFU Colony Forming Unit CI Confidence Interval CTR Control group GCS Glasgow Coma Score hrs hours HTI‐ISS Hospital Trauma Index‐Injury Severity Score ICU Intensive Care Unit ISS Injury Severity Score iv intravenous MOSF Multi‐Organ‐System‐Failure OR Odds Ratio RCTs Randomised Controlled Trials RD Risk Differences RR Relative Risk RTIs Respiratory Tract Infections SAPS Symplified Acute Physiology Score SDD Selective Decontamination of the Digestive Tract VAP Ventilator Associated Pneumonia VO2 Oxygen Consumption yrs years WBC White Blood Count
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Arnow 1996 | The study included a selected population of patients undergoing liver transplant |
| Barret 2001 | The study included only paediatric burns patients |
| Bion 1994 | The study included a selected population of patients undergoing liver transplant |
| Bouter 2002 | The study included only patients undergoing cardiopulmonary by‐pass |
| de la Cal 2005 | The study included only critically ill burns patients |
| de Smet 2009 | The study adopted a cluster design with type of treatments alternated for specific periods of time across participating hospitals. As a consequence patients were not properly randomised and the study could be affected by selection bias. |
| Flaherty 1990 | The study included a selected population of cardio surgical patients |
| Garbino 2002 | The study tested the effectiveness of fluconazole as both groups received SDD |
| Hellinger 2002 | The study included only liver transplant patients |
| Hunefeld 1989 | After contacting the principal investigator it become apparent that it was not a randomised study |
| Jacobs 1995 | This study, included in the previous version of this review as a personal contact with the principal investigator, has been excluded due to lack of feedback from the trial author. To date, this study has never been published |
| Lenhart 1994 | This study, included in the previous version of this review as a congress proceeding, has been replaced by its published article (Krueger 2002) |
| Lipman 1994 | After contacting the principal investigator it become apparent that it was not a randomised study |
| Luiten 1995 | The study included a selected population of patients affected by pancreatitis characterised by a low percentage of ICU admissions. |
| Martinez 1994 | The study compared the effect of two different prophylactic regimens without a control group |
| Martinez‐Pellus 1993 | The study included a selected population of cardio surgical patients |
| Nardi 2001 | The study tested the effectiveness of mupirocin as both groups received SDD |
| Rayes 2002 | The study included only liver transplant patients |
| Rolando 1996 | The study included a selected population of patients with acute hepatic failure |
| Ruza 1998 | The study included only paediatric burns patients |
| Schardey 1997 | The study included a selected population of patients undergoing gastric surgery and characterised by a low percentage of ICU admission |
| Smith 1993 | The study included only paediatric, liver transplant patients |
| Stoutenbeek 2 | This unpublished study, included in the previous version of this review, has been replaced by its published article (Stoutenbeek 2007) |
| Tetteroo 1990 | The study included a selected population of patients undergoing oesophageal resection and characterised by a short length of stay in ICU |
| Zobel 1991 | The study included only paediatric patients |
| Zwaveling 2002 | The study included only liver transplant patients |
Contributions of authors
Alessandro Liberati prepared the protocol and review, oversaw the data collection and critical appraisal of studies, updated the review and prepared the final version of the manuscript. Roberto D'Amico prepared the protocol and review, oversaw the data collection and critical appraisal of studies, carried out the statistical analysis, updated the review and prepared the final version of the manuscript. Luca Brazzi collaborated in the preparation of the protocol, the identification of trials and their critical appraisal. Valter Torri collaborated in the preparation of the protocol and the statistical analysis. Silvia Pifferi collaborated in the identification and critical appraisal of trials. Elena Parmelli collaborated in the update of the review.
Sources of support
Internal sources
Italian Cochrane Centre, Italy.
External sources
No sources of support supplied
Declarations of interest
None known.
Deceased
Edited (no change to conclusions)
References
References to studies included in this review
Abele‐Horn 1997 {published data only}
- Abele‐Horn M, Dauber A, Bauernfeind A, Russwurm W, Seyfarth‐Metzger I, Gleich P, et al. Decrease in nosocomial pneumonia in ventilated patients by selective oropharyngeal decontamination (SOD). Intensive Care Medicine 1997;23(2):187‐95. [DOI] [PubMed] [Google Scholar]
Aerdts 1991 {published and unpublished data}
- Aerdts SJA, Dalen R, Clasener HAL, Festen J, Lier HJJ, Vollaard EJ. Antibiotic prophylaxis of respiratory tract infection in mechanically ventilated patients. Chest 1991;100(3):783‐91. [DOI] [PubMed] [Google Scholar]
Bergmans 2001 {published data only}
- Bergmans DCJJ, Bonten MJM, Gailard CA, Paling JC, Geest S, Tiel FH, et al. Prevention of ventilator‐associated pneumonia by oral decontamination: a prospective randomized, double blind, placebo controlled study. American Journal of Respiratory and Critical Care Medicine 2001;164(3):382‐8. [DOI] [PubMed] [Google Scholar]
Blair 1991 {published and unpublished data}
- Blair P, Rowlands BJ, Lowry K, Webb H, Amstrong P, Smilie J. Selective decontamination of the digestive tract: a stratified, randomized, prospective study in a mixed intensive care unit. Surgery 1991;110(2):303‐10. [PubMed] [Google Scholar]
Boland 1991 {published and unpublished data}
- Boland JP, Sadler DL, Stewart W, Wood DJ, Zerick W, Snodgrass KR. Reduction of nosocomial respiratory tract infections in the multiple trauma patients requiring mechanical ventilation by selective parenteral and enteral antisepsis regimen (SPEAR) in the intensive care. XVII Congress of Chemotherapy. 1991.
Brun‐Buisson 1989 {published and unpublished data}
- Brun‐Buisson C, Legrand P, Rauss A, Richard C, Montravers F, Besbes M, et al. Intestinal decontamination for control of nosocomial multiresistant Gram‐negative bacilli. Annals of Internal Medicine 1989;110(11):873‐81. [DOI] [PubMed] [Google Scholar]
Camus 2005 {published data only}
- Camus C, Bellissant E, Sebille W, Perrotin D, Garo B, Legras A, et al. Prevention of acquired infections in intubated patients with combination of two decontaminations regimens. Critical Care Medicine 2005;33(2):307‐14. [DOI] [PubMed] [Google Scholar]
Cerra 1992 {published and unpublished data}
- Cerra FB, Maddaus MA, Dunn DL, Wells CL, Konstantinides NN, Lehmann SL, et al. Selective gut decontamination reduces nosocomial infections and length of stay but not mortality or organ failure in surgical intensive care unit patients. Archives of Surgery 1992;127(2):163‐9. [DOI] [PubMed] [Google Scholar]
Cockerill 1992 {published and unpublished data}
- Cockerill FR III, Muller SR, Anhalt JP, Marsh HM, Farnell MB, Mucha P, et al. Prevention of infection in critically ill patients by selective decontamination of the digestive tract. Annals of Internal Medicine 1992;117(7):545‐53. [DOI] [PubMed] [Google Scholar]
de Jonge 2003 {published data only}
- Jonge E, Schultz JM, Spanjaard L, Bossuyt PMM, Vroom MB, Dankert J, et al. Effects of selective decontamination of digestive tract on mortality and acquisition of resistant bacteria in intensive care: a randomised controlled trial. Lancet 2003;362(9389):1011‐6. [DOI] [PubMed] [Google Scholar]
Ferrer 1994 {published and unpublished data}
- Ferrer M, Torres A, Gonzàles J, Bellacasa JP, El‐Ebiary M, Roca M, et al. Utility of selective digestive decontamination in mechanically ventilated patients. Annals of Internal Medicine 1994;120:389‐95. [DOI] [PubMed] [Google Scholar]
Finch 1991 {published and unpublished data}
- Finch RG, Tomlinson P, Holliday M, Sole K, Stack C, Rocker G. Selective decontamination of the digestive tract (SDD) in the prevention of secondary sepsis in a medical/surgical intensive care unit. XVII International Congress Chemotherapy. 1991.
Gastinne 1992 {published and unpublished data}
- Gastinne H, Wolff M, Delatour F, Faurisson F, Chevret S. A controlled trial in intensive care units of selective decontamination of the digestive tract with nonabsorbable antibiotics. New England Journal of Medicine 1992;326:594‐9. [DOI] [PubMed] [Google Scholar]
Gaussorgues 1991 {published and unpublished data}
- Gaussorgues P, Salord F, Sirodot M, Tigaud S, Cagnin S, Gerard M, et al. [Efficacité de la décontamination digestive sur la survenue des bactériémies nosocomiales chez les patients sous ventilation mécanique et recevant des betamimétiques]. Reanimation, Soins Intensifs, Medicine d'Urgence 1991;7:169‐74. [Google Scholar]
Georges 1994 {published data only}
- Georges B, Mazerolles M, Decun JF, Rouge P, Pomies S, Cougot P, et al. [Décontamination digestive sélective résultats d'une ètude chez le polytraumatisé]. Reanimation d'Urgence 1994;3:621‐7. [Google Scholar]
Hammond 1992 {published and unpublished data}
- Hammond JMJ, Potgieter PD, Saunders GL, Forder AA. Double blind study of selective decontamination of the digestive tract in intensive care. Lancet 1992;340:5‐9. [DOI] [PubMed] [Google Scholar]
Jacobs 1992 {published and unpublished data}
- Jacobs S, Foweraker JE, Roberts SE. Effectiveness of selective decontamination of the digestive tract (SDD) in an ICU with a policy encouraging a low gastric pH. Clinical Intensive Care 1992;3:52‐8. [Google Scholar]
Kerver 1988 {published and unpublished data}
- Kerver AJH, Rommes JH, Mevissen‐Verhage EAE, Hulstaert PF, Vos A, Verhoef J, et al. Prevention of colonization and infection in critically ill patients: A prospective randomized study. Critical Care Medicine 1988;16:1087. [DOI] [PubMed] [Google Scholar]
Korinek 1993 {published and unpublished data}
- Korinek AM, Laisne MJ, Raskine L, Deroin V, Sanson‐Lepors MJ. Selective decontamination of the digestive tract in neurosurgical care units patients: a double blind, randomized, placebo‐controlled study. Critical Care Medicine 1993;21:1466‐73. [DOI] [PubMed] [Google Scholar]
Krueger 2002 {published data only}
- Krueger WA, Lenhart FP, Neeser G, Ruckdeschel G, Schreckhase H, Eissner HJ, et al. Influence of combined intravenous and topical antibiotic prophylaxis on the incidence of infections, organ dysfunctions and mortality in critically ill surgical patients. American Journal of Respiratory and Critical Care Medicine 2002;166:1029‐37. [DOI] [PubMed] [Google Scholar]
Laggner 1994 {published and unpublished data}
- Laggner AN, Tryba M, Georgopoulos A, Lenz K, Grimm G, Graninger W, et al. Oropharyngeal decontamination with gentamicin for long‐term ventilated patients on stress ulcer prophylaxis with sucralfate?. Wiener Klinische Wochenschrift 1994;106:15‐9. [PubMed] [Google Scholar]
Lingnau 1997 {published and unpublished data}
- Lingnau W, Berger J, Javorsky F, Lejeune P, Mutz N, Benzer H. Selective intestinal decontamination in multiple trauma patients: prospective, controlled trials. Journal of Trauma 1997;42:687‐94. [DOI] [PubMed] [Google Scholar]
Lingnau 1997b {published and unpublished data}
- Lingnau W, Berger J, Javorsky F, Lejeune P, Mutz N, Benzer H. Selective intestinal decontamination in multiple trauma patients: prospective, controlled trials. Journal of Trauma 1997;42:687‐94. [DOI] [PubMed] [Google Scholar]
Palomar 1997 {published and unpublished data}
- Palomar M, Alvarez‐Lerma F, Jorda R, Bermejo B. Prevention of nosocomial infection in mechanically ventilated patients: Selective digestive decontamination versus sucralfate. Clinical Intensive Care 1997;8:228‐35. [Google Scholar]
Pneumatikos 2002 {published data only}
- Pneumatikos I, Koulouras V, Nathanail C, Goe D, Nakos G. Selective decontamination of subgloottic area in mechanically ventilated patients with multiple trauma. Intensive Care Medicine 2002;28:432‐7. [DOI] [PubMed] [Google Scholar]
Pugin 1991 {published and unpublished data}
- Pugin J, Auckenthaler R, Lew DP, Suter PM. Oropharyngeal decontamination decreases incidence of ventilator‐associated pneumonia. JAMA 1991;265:2704‐10. [PubMed] [Google Scholar]
Quinio 1995 {published and unpublished data}
- Quinio B, Albanèse J, Bues‐Charbit M, Viviand X, Martin C. Selective Decontamination of the digestive tract in multiple trauma patients: prospective, double blind, randomised, placebo‐controlled study. Chest 1996;109:765‐72. [DOI] [PubMed] [Google Scholar]
Rocha 1992 {published and unpublished data}
- Rocha LA, Martin MJ, Pita S, Paz J, Seco C, Margusino L, et al. Prevention of nosocomial infection in critically ill patients by selective decontamination of digestive tract. Intensive Care Medicine 1992;18:398‐404. [DOI] [PubMed] [Google Scholar]
Rodriguez‐Rolda 1990 {published and unpublished data}
- Rodrìguez‐Roldàn JM, Altuna‐Cuesta A, Lòpez A, Carrillo A, Garcia J, Leòn J, et al. Prevention of nosocomial lung infection in ventilated patients:use of an antimicrobial pharyngeal nonabsorbable paste. Critical Care Medicine 1990;18:1239‐42. [DOI] [PubMed] [Google Scholar]
Sanchez‐Garcia 1992 {published and unpublished data}
- Sanchez‐Garcia M, Cambronero JA, Lopez J, Cerda E, Rubio J, et al. Effectiveness and cost of selective decontamination of the digestive tract (SDD) in critically ill intubated patients. A randomized, double blind, placebo‐controlled, multicentric trial. American Journal of Respiratory and Critical Care Medicine 1998;158:908‐16. [DOI] [PubMed] [Google Scholar]
Stoutenbeek 1996 {published data only}
- Stoutenbeek CP, Saene HKF, Miranda D R, Zandstra DF. The effect of selective decontamination of the digestive tract on colonization and infection rate in multiple trauma patients. Intensive Care Medicine 1984;10:185‐92. [DOI] [PubMed] [Google Scholar]
Stoutenbeek 2007 {published data only}
- Stoutenbeek CP, Saene HKF, Little RA, Whitehead A. The effect of selective decontamination on the digestive tract on mortality in multiple trauma patients: a multicentre randomized controlled trial. Intensive Care Medicine 2007;33:261‐70. [DOI] [PubMed] [Google Scholar]
Ulrich 1989 {published and unpublished data}
- Ulrich C, Harinck‐deWeerd JE, Bakker NC, Jacz K, Doornbos L, Ridder VA. Selective decontamination of the digestive tract with norfloxacin in the prevention of ICU‐acquired infections: a prospective randomized study. Intensive Care Medicine 1989;15:424‐31. [DOI] [PubMed] [Google Scholar]
Unertl 1987 {published and unpublished data}
- Unertl K, Ruckdeschel G, Selbmann HK, Jensen U, Forst H, Lenhart FP, et al. Prevention of colonization and respiratory infections in long term ventilated patients by local antimicrobial prophylaxis. Intensive Care Medicine 1987;13:106‐13. [DOI] [PubMed] [Google Scholar]
Verwaest 1997 {published and unpublished data}
- Verwaest C, Verhaegen J, Ferdinande P, Schets M, Berghe G, Verbist L, et al. Randomized, controlled trial of selective digestive decontamination in 600 mechanically ventilated patients in a multidisciplinary intensive care unit. Critical Care Medicine 1997;25:63‐71. [DOI] [PubMed] [Google Scholar]
Wiener 1995 {published data only}
- Wiener J, Itokazu G, Nothan C, Kabins SA, Weinstein RA. A randomized, double‐blind, placebo‐controlled trial of selective digestive decontamination in a medical‐surgical intensive care unit. Clinical Infectious Diseases 1995;20:861‐7. [DOI] [PubMed] [Google Scholar]
Winter 1992 {published and unpublished data}
- Winter R, Humphreys H, Pick A, MacGowan AP, Willatts SM, Speller DCE. A controlled trials of selective decontamination of the digestive tract in intensive care and its effect on nosocomial infection. Journal of Antimicrobial Chemotherapy 1992;30:73‐87. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Arnow 1996 {published data only}
- Arnow PM, Carandanq GC, Irwin ME. Randomized controlled trial of selective bowel decontamination for prevention of infections following liver transplantation. Clinical Infectious Diseases 1996;22:997‐1003. [DOI] [PubMed] [Google Scholar]
Barret 2001 {published data only}
- Barret JP, Jeschke MG, Herndon DN. Selective decontamination of the digestive tract in severely burned pediatric patients. Burns 2001;27:439‐45. [DOI] [PubMed] [Google Scholar]
Bion 1994 {published data only}
- Bion JF, Badger I, Crosby HA, Hutchings P, Kong KL, Baker J, et al. Selective decontamination of the digestive tract reduces Gram‐negative pulmonary colonization but not systemic endotoxemia in patients undergoing elective liver transplantation. Critical Care Medicine 1994;22:40‐9. [DOI] [PubMed] [Google Scholar]
Bouter 2002 {published data only}
- Bouter H, Schippers EF, Luelmo SAC, Verteegh MIM, et al. No effect of preoperative selective gut decontamination on endotoxemia and cytokine activation during cardiopulmonary bypass: A randomized, placebo controlled study. Critical Care Medicine 2002;30:38‐43. [DOI] [PubMed] [Google Scholar]
de la Cal 2005 {published data only}
- Cal MA, Cerdà E, Garcia‐Hierro P, et al. Survival benefit in critically hill burned patients receiving selective decontamination of the digestive tract. A randomized, placebo‐controlled, double‐blind trial. Annals of Internal Medicine 1992;117:545‐53. [DOI] [PMC free article] [PubMed] [Google Scholar]
de Smet 2009 {published data only}
- Smet AMGA, Kluytmans JAJW, Cooper BS, Mascini EM, Benus RFJ, Werf TS, et al. Decontamination of the digestive tract and oropharynx in ICU patients. NEJM 2009;360:20‐31. [DOI] [PubMed] [Google Scholar]
Flaherty 1990 {published data only}
- Flaherty J, Nathan C, Kabins SA, Weinstein RA. Pilot trial of selective decontamination for prevention of bacterial infection in an intensive care unit. Journal of Infectious Diseases 1990;162:1393‐7. [DOI] [PubMed] [Google Scholar]
Garbino 2002 {published data only}
- Garbino J, Lew DP, Romand JA, Hogonnet S, Auckenthaler R, Pittet D. Prevention of severe candida infections in nonneutropenic high risk, crically ill patients: a randomized, double blinded, placebo controlled trial in patients treated by severe digestive decontamination. Intensive Care Medicine 2002;28:1708‐17. [DOI] [PubMed] [Google Scholar]
Hellinger 2002 {published data only}
- Hellinger WC, Yao JD, Alvarez S, Blair JE, et al. A randomized, prospective, double blinded evaluation of selective bowel decontamination in liver transplantation. Transplantation 2002;73:1904‐9. [DOI] [PubMed] [Google Scholar]
Hunefeld 1989 {published and unpublished data}
- Hunefeldt G. [Klinische Studie zur selectiven Darmdekolonisation bei 204 langzeitbeatmeten abdominal und unfallchirurgischen Intensivpatienten]. Anaesthesiologie und Reanimation 1989;14:131‐53. [PubMed] [Google Scholar]
Jacobs 1995 {unpublished data only}
- Jacobs S, Zuleika M. no title. provided by the authors.
Lenhart 1994 {published data only}
- Lenhart FP, Unertl K, Neeser G, Ruckdeschel G, Eckart J, Peter K. Selective decontamination and sucralfate for prevention of acquired infections in intensive care. 17th International Congress Chemotherapy, Vienna 1994 (K101). 1994.
Lipman 1994 {published and unpublished data}
- Lipman J, Klugman K, Luyt D, Kraus P, Litmanovitch M, Johnson D, et al. Unique trial design shows SDD to decrease and alter colonization of upper respiractory tract in a multidisciplinary ICU. Critical Care Medicine 1994;22:1. [Google Scholar]
Luiten 1995 {published data only}
- Luiten EJ, Hop WC, Lange JF, Bruining HA. Controlled clinical trial of selective decontamination for the treatment of severe acute pancreatitis. Annals of Surgery 1995;222:57‐65. [DOI] [PMC free article] [PubMed] [Google Scholar]
Martinez 1994 {published data only}
- Martinez PAE, Bru M, Jara P, Ruiz J, Sanmiguel MT, Garcia PT. Does cefotaxime prevent early pneumonia in trauma patients receiving pharyngeal decontamination?. Medicina Intensiva 1994;18:245‐9. [Google Scholar]
Martinez‐Pellus 1993 {published data only}
- Martinez‐Pellus AE, Merino P, Bru M, Coneyero R, Seller G, Munoz C, et al. Can selective digestive decontamination avoid the endotoxemia and cytokine activation promoted by cardiopulmonary bypass?. Critical Care Medicine 1993;2:1684‐91. [DOI] [PubMed] [Google Scholar]
Nardi 2001 {published data only}
- Nardi G, Silvestre A, Monte A, Massarutti D, Proietti A, Grazia Troncon M, et al. Reduction in gram positive pneumonia and antibiotic consumption following the use of a SDD protocol including nasal nad oral mupirocin. European Journal of Emergency Medicine 2001;8:203‐14. [DOI] [PubMed] [Google Scholar]
Rayes 2002 {published data only}
- Rayes N, Seehofer D, Hansen S, Boucsein K, et al. Early enteral supply of lactobacillus and fiber versus selective bowel decontamination: a controlled trial in liver transplant recipients. Transplatation 2002;74:123‐8. [DOI] [PubMed] [Google Scholar]
Rolando 1996 {published and unpublished data}
- Rolando N, Wade J, Stangou A, Gimson AE, Wendon J, Philpott‐Howard J, et al. Prospective study comparing the efficacy of prophylactic parenteral antimicrobials, with or without enteral decontamination, in patients with acute liver failure. Liver Transplantation and Surgery 1996;2:8‐13. [DOI] [PubMed] [Google Scholar]
Ruza 1998 {published data only}
- Ruza F, Alvarado F, Herruzo R, Delgado MA, García S, Dorao P, et al. Prevention of nosocomial infection in a pediatric intensive care unit (PICU) through the use of selective digestive decontamination. European Journal of Epidemiology 1998;14:719‐27. [DOI] [PubMed] [Google Scholar]
Schardey 1997 {published and unpublished data}
- Schardey HM, Joosten U, Finke U, Stanbach KH, Schauer R, Heiss A, et al. The prevention of anastomotic leakage after total gastrectomy with local decontamination. A prospective double‐blind, randomized and placebo‐controlled clinical multicenter trial. Annals of Surgery 1997;225:172‐80. [DOI] [PMC free article] [PubMed] [Google Scholar]
Smith 1993 {published data only}
- Smith SD, Jackson RJ, Hannakan CJ, Wadowsky RM, Tzakis AG, Rowe MI, et al. Selective decontamination in pediatric liver transplant. A randomized prospective study. Transplantation 1993;55:1306‐9. [DOI] [PubMed] [Google Scholar]
Stoutenbeek 2 {unpublished data only}
- Stoutenbeek CP, Saene HKF, Little RA, Whitehead A. The effect of selective decontamination of the digestive tratct on mortality in multiple trauma patients.. Contact with authors.
Tetteroo 1990 {published and unpublished data}
- Tetteroo GWM, Wagenvoort JHT, Castelei A, Tilanus HW, Ince C, Bruining HA. Selective decontamination to reduce gram‐negative colonisation and infections after oesophageal resection. Lancet 1990;335:704‐7. [DOI] [PubMed] [Google Scholar]
Zobel 1991 {published data only}
- Zobel G, Kutting M, Grubbauer HM, Semmelrock HJ, Thiel W. Reduction of colonization and infection rate during pediatric intensive care by selective decontamination of digestive tract. CritIical Care Medicine 1991;19:1242‐6. [DOI] [PubMed] [Google Scholar]
Zwaveling 2002 {published data only}
- Zweveling JH, Maring JK, Klompmaker IJ, Haagsma EB Bottema JT, Laseur M, et al. Selective decontamination of the digestive tract to prevent postoperative infection: a randomized placebo‐controlled trial in liver transplant patients. Critical Care Medicine 2002;30(6):1204‐9. [DOI] [PubMed] [Google Scholar]
Additional references
Chevret 1996
- Chevret S, Hemmer M, Carlet J, Langer M. Incidence and risk factors of pneumonia acquired in intensive care units. Results from a multicenter prospective study on 996 patients. European Cooperative Group on Nosocomial Pneumonia. JAMA 1996;275(11):866‐9. [DOI] [PubMed] [Google Scholar]
Collard 2003
- Collard HR, Saint S, Matthay MA. Prevention of ventilator‐associated pneumonia: an evidence‐based systematic review. Annals of Internal Medicine 2003;138(6):494‐501. [DOI] [PubMed] [Google Scholar]
Fagon 1996
- Fagon JY, Chastre J, Vuagnat A, Trouillet JL, Novara A, Gibert C. Nosocomial pneumonia and mortality among patients in Intensive care unit. JAMA 1996;275:866‐9. [PubMed] [Google Scholar]
Heyland 1994
- Heyland DK, Cook DJ, Jaescher R, Griffith L, Lee HN, Guyatt GH. Selective decontamination of the digestive tract. An overview. Chest 1994;105:1221‐9. [DOI] [PubMed] [Google Scholar]
Higgins 2008
- Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.0.0. The Cochrane Collaboration, 2008. [Google Scholar]
Hurley 1995
- Hurley JC. Prophylaxis with enteral antibiotics in ventilated patients: selective decontamination or selective cross‐infection?. Antimicrobial Agents and Chemotherapy 1995;39:941‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kollef 1994
- Kollef MH. The role of selective digestive tract decontamination on mortality and respiratory tract infections. A meta‐analysis. Chest 1994;105:1101‐8. [DOI] [PubMed] [Google Scholar]
Lefebvre 2008
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JP, Green S editor(s). Cochrane Handbook for Systematic Reviews of Interventions. Chichester, UK: Wiley, 2008. [Google Scholar]
Liberati 2001
- Liberati A, D'Amico R, Brazzi L, Pifferi S. Influence of methodological quality on study conclusions. JAMA 2001;286:2544‐5. [DOI] [PubMed] [Google Scholar]
Nathens 1999
- Nathens AB. Selective decontamination of digestive tract in surgical patients: a systematic review of evidence. Archives of Surgery 1999;134:170‐6. [DOI] [PubMed] [Google Scholar]
Redman 2001
- Redman R, Ludington E. Analysis of respiratory and non‐respiratory infections in published trials of selective digestive decontamination. Intensive Care Medicine (14th Annual Congress of the European Society of Intensive Care Medicine 2001). 2001, issue Suppl 2:285.
Silvestri 2007
- Silvestri L, Saene HKF, et al. Selective decontamination of the digestive tract reduces bacterial bloodstreem infection and mortality in critically ill patients. Systematic review of randomized controlled trials. Journal of Hospital Infection 2007;65:187‐203. [DOI] [PubMed] [Google Scholar]
Stoutenbeek 1994
- Stoutenbeek CP, Saene HKF, Miranda DR, Zandstra DF. The effect of selective decontamination of the digestive tract on colonization and infection rate in multiple trauma patients. Intensive Care Medicine 1994;10:185‐92. [DOI] [PubMed] [Google Scholar]
van Nieuwenhove 2001
- Nieuwenhoven CA, Buskens E, Tiel FH, Bonten MJ. Reletionship between methodological trial quality and the effects of selective digestive decontamination on pneumonia and mortality in critically ill patients. JAMA 2001;286:335‐40. [DOI] [PubMed] [Google Scholar]
Vanderbrouk‐Gra 1991
- Vanderbrouk‐Grauls CM, Vanderbrouke‐Grauls JP. Effect of selective decontamination of the digestive tract on respiratory tract infections and mortality in intensive care unit. Lancet 1991;338:859‐62. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
D'Amico 1998
- D'Amico R, Pifferi S, Leonetti C, Torri V, Tinazzi A, Liberati A, et al. Effectiveness of antibiotic prophylaxis in critically ill adult patients: systematic review of randomised controlled trials. BMJ 1998;316:1275‐85. [DOI] [PMC free article] [PubMed] [Google Scholar]
Liberati 1997
- Liberati A, D'Amico R, Pifferi S, Leonetti C, Torri V, Brazzi L, et al. Antibiotic prophylaxis in adult patients treated in Intensive Care Units. Cochrane Database of Systematic Reviews 1997, Issue 3. [DOI: 10.1002/14651858.CD000022.pub2] [DOI] [Google Scholar]
Liberati 2002
- Liberati A, D'Amico R, Pifferi S, Leonetti C, Torri V, Brazzi L, et al. Antibiotics for preventing respiratory tract infections in adults receiving intensive care. Cochrane Database of Systematic Reviews 2002, Issue 4. [DOI: 10.1002/14651858.CD000022.pub2] [DOI] [PubMed] [Google Scholar]
Liberati 2004
- Liberati A, D'Amico R, Pifferi, Torri V, Brazzi L. Antibiotic prophylaxis to reduce respiratory tract infections and mortality in adults receiving intensive care. Cochrane Database of Systematic Reviews 2004, Issue 1. [DOI: 10.1002/14651858.CD000022.pub2] [DOI] [PubMed] [Google Scholar]
SDD Group 1993
- SDD Trialists' Collaborative Group. Meta‐analysis of randomised controlled trials of selective decontamination of the digestive tract. British Medical Journal 1993;307:525‐32. [DOI] [PMC free article] [PubMed] [Google Scholar]