

Abstract
BACKGROUND:
Oral and systemic problems are common among pregnant women. Routine dental visits are important for the maintenance of optimal oral health which is linked with systemic health.
AIM:
To evaluate dental care utilization and related factors among pregnant women in the Eastern province of Saudi Arabia.
METHODS:
This cross-sectional study was conducted in hospitals and healthcare centers in the cities of Khobar, Dammam, and Qatif in the Eastern province of Saudi Arabia. A piloted tested self-administered questionnaire available in Arabic and English languages was distributed among a calculated sample of 341 pregnant women. Pearson’s chi-square test and multiple logistic regression analyses were performed.
RESULTS:
In the study, 270 questionnaires were analyzed giving a response rate of 79.2%. Mean age of the participants was 29 ± 5.9 years. There were 43.7% pregnant women who received dental treatment when they have a dental problem and only 13.7% performed routine dental visit. Half the sample (52.6%) avoided dental visits during pregnancy and dental treatment being unsafe was the most common reason for avoiding dental visits. After adjustment, routine dental visits during pregnancy were 7.38 times higher among Saudis compared with non-Saudis women (p 0.05). The participants who had a negative perception about the safety of dental treatment had significantly lower odds (OR 0.31, p 0.036) of dental attendance for routine dental visits.
CONCLUSION:
Routine dental visits were low among pregnant women and many visited dentists when they had a dental problem. Negative perception about the safety of dental treatment was associated with reduced regular dental visits during pregnancy. Pregnant women should be educated about the importance of receiving dental care for the maintenance of optimal oral health.
Keywords: Dental care, Treatment, Clinic visit, Pregnancy, Appointment
Introduction
In women’s life, pregnancy is a unique event with many emotional and physiological changes that involve cardiovascular, immune, respiratory, and endocrine systems [1]. Oral health is also affected during pregnancy and gingivitis is the most common oral condition in pregnant women [2]. It is known that about 40% of pregnant women are affected with periodontal diseases which have been linked to low birthweight, preterm birth, and preeclampsia [3]. It has been reported that the risk of low birthweight is seven times greater in pregnant women with periodontitis compared with pregnant women without periodontitis [4], [5]. Evidence shows that the treatment of periodontal disease during pregnancy can reduce the risk of both preterm birth and low birthweight [4].
In addition, there is a high risk of developing caries in pregnant women [6]. The composition of saliva in the late stages of pregnancy becomes more acidic, and it has high streptococcus mutans and reduced calcium and phosphate levels which predispose pregnant women to an increased caries risk [6]. Moreover, pregnant women with high levels of streptococcus mutans have increased potential of transmitting infection through placenta to fetus which later enhances the risk of early childhood caries in these babies [7]. Therefore, good oral health is important for both mother and the fetus during pregnancy [8]. The treatment of periodontal disease should be given as soon as possible to pregnant women to reduce the risk of perinatal complications [9].
There is a lack of dental care service utilization among pregnant women. In a study in the U.S. (2010), only 25% of pregnant women visited the dentist during pregnancy for routine dental check-up and the most commonly reported reason for not seeking dental care was not having dental insurance [10]. A study in Jordan (2014) reported that 42.4% of pregnant women did not visit the dentist because they believed that visiting dentist during pregnancy was not necessary [11]. In Riyadh (2014), 22% of pregnant women were shown to receive professional dental care during pregnancy and those who visited the dentist before pregnancy were more likely to do so during pregnancy [12].
There is limited evidence about the utilization of oral care services among pregnant women in the Eastern province of Saudi Arabia. Moreover, it is not known that what sociodemographic factors are associated with routine dental visits and dental attendance due to dental problems among pregnant women. Therefore, the study aimed to evaluate dental care utilization and its associated factors among pregnant women in the Eastern province.
Methods
This cross-sectional study included pregnant women who visited for prenatal checks the King Fahad University Hospital in Khobar, Qatif Central Hospital in Qatif, and Maternity and Children Hospital in Dammam, Eastern province of Saudi Arabia. In addition, health care centers in these three cities were visited to recruit participants to get a more representative sample. The administrators of hospitals and health centers were contacted to obtain permission to collect data from their respective institutions. A convenient sample of pregnant women was collected. A sample of 341 participants was calculated which was based on using approximate population of pregnant women, anticipated percentage of frequency, design effect, and 95% confidence interval. The women who were not pregnant or those who could not read and understand Arabic or English language were excluded from the study.
Ethical approval (EA 2016015) was obtained the ethics committee at the College of Dentistry Imam Abdulrahman Bin Faisal University, Dammam. The participants of the study were briefed about the purpose, details, benefits and start and expected end time of the research project. They were informed that their participation in the study was voluntary. A written informed consent was obtained from them. The privacy and confidentiality of the participants were maintained during the collection, analysis, and reporting of data.
Investigators developed a questionnaire based on the information collected from previous studies [10], [11], [12], [13]. The self-administered questionnaire included close-ended questions. The questionnaire had 17 questions divided into three sections. The first section was about demographic information which included nationality, educational attainment, employment status, monthly income, dental insurance, systemic disease, stages of pregnancy, and perception about oral health. Oral hygiene behavior information was sought in the second section where participants self-evaluated their oral hygiene practices. The third section inquired respondents about the utilization of dental care services. In addition, respondents were asked to provide the reasons of avoiding dental attendance.
Pilot testing of the questionnaire was done involving 40 participants (20 for the English version of questionnaire and 20 for the Arabic version of questionnaire) and subsequently, changes were made to improve clarity and understanding of the instrument before its final administration. The consent form and questionnaire were available in English and Arabic languages for Arabic and non-Arabic speaking participants. Hard copies of the questionnaire were delivered to participants in person.
Statistical Package for Social Sciences (IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY) was used to enter data and perform statistical analyses. Descriptive statistics analysis involved calculating means, standard deviations and frequencies of different variables and presenting in tables and graphs. Analytical statistics included using Pearson’s Chi-square test and logistic regression analysis. Pearson’s Chi-square test compare proportions of different categorical variables between those who visited the dentist and those who did not perform a dental visit during pregnancy. Multivariate logistic regression analyses were performed to assess the association between independent variables such as nationality, age, education, employment status etc. and dependent variables such as routine dental visits during pregnancy and dental attendance due to dental problems (oral health care service utilization). Statistical significance was set at p-value < 0.05.
Results
A total of 270 questionnaires were included in the analysis of the study and 45 questionnaires were excluded to due to incomplete information provided by the participants. The response rate was 79.2% (270/341). The mean age of the participants was 29 years (SD 5.9). The majority of the questionnaires were completed by Saudi women (86.3%). Most participants were without a systemic disease (85.2%) and had no dental insurance (67.4%). Almost half the subjects (51.1%) completed a bachelor’s degree or beyond and one-third of the sample (35.2%) was employed. There were 41.1% of the pregnant women in their third trimester, followed by the second trimester (33.3%) and first trimesters (25.6%) (Table 1).
Table 1.
Demographic information of study participants
| Factors | N/ (%) (N = 270) | 95% CI |
|---|---|---|
| Nationality: | ||
| Saudi | 233 (86.3) | (81.69, 89.9) |
| Non-Saudi | 37 (13.7) | (10.1, 18.31) |
| Education | ||
| School education | 132 (48.9) | (42.99, 54.83) |
| College/university education | 138 (51.1) | (45.17, 57.01) |
| Employment status | ||
| Employed | 95 (35.2) | (29.74, 41.06) |
| Not employed | 175 (64.8) | (58.94, 70.26) |
| Systemic disease | ||
| Yes | 40 (14.8) | (11.07, 19.54) |
| No | 230 (85.2) | (80.46, 88.93) |
| Insurance | ||
| Yes | 88 (32.6) | (27.28, 38.39) |
| No | 182 (67.4) | (61.61, 72.72) |
| Stage of pregnancy | ||
| First trimester | 69 (25.6) | (20.73, 31.08) |
| Second trimester | 90 (33.3) | (27.98, 39.15) |
| Third trimester | 111 (41.1) | (35.41, 47.06) |
| Perception of oral health: | ||
| Good | 236 (87.4) | (82.92, 90.85) |
| Poor | 34 (12.6) | (9.15, 17.08) |
| Age | Mean 29.026 | SD 5.9 |
In the study, 43.7% of pregnant women received dental treatment when they had a dental problem and the highest percentage of these women (40.7%) utilized dental care during the second trimester and there was a statistically significant difference in three semesters (p 0.049). There were 13.7% of participants who performed dental visit for regular dental visits. Almost half the sample (52.6%) indicated avoiding dental visits during pregnancy and the highest percentage of these women (43.7%) of avoided during third trimester (Table 2).
Table 2.
Dental visits during different trimester of pregnancy
| Dental attendance | Total N (%) | First trimester N (%) | Second trimester N (%) | Third trimester N (%) | p-value |
|---|---|---|---|---|---|
| Regular dental visits | 37 (13.7) | 13 (35.1) | 11 (29.7) | 13 (35.1) | 0.354 |
| Dental visits related to oral problems | 118 (43.7) | 30 (25.4) | 48 (40.7) | 40 (33.9) | 0.049* |
| Avoid dental visits | 142 (52.6) | 32 (22.5) | 48 (33.8) | 62 (43.7) | 0.458 |
The toothache (26.7%) was the most commonly reported condition for dental attendance, followed by bleeding gum (17.8%). Negative perception about the safety of dental treatment during pregnancy was the most common reason (24.8%) for avoiding dental care. The fear/anxiety of dental treatment (17%) was the second most common reason of not using dental services. Transportation problems (0.7%), dissatisfaction with the quality of dental services (1.5%), and lack of time to visit a dentist (2.2%) were least commonly reported reasons of avoiding dental visits (Figure 1).
Figure 1.
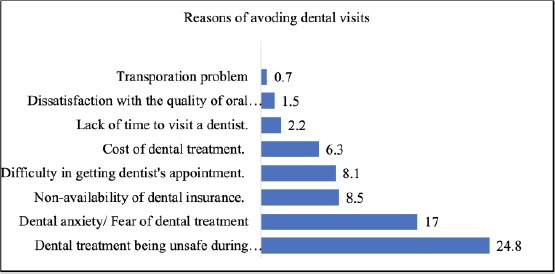
Reasons of avoiding dental visits among pregnant women
The analysis of data about the influence of different factors on routine dental visits among pregnant women is shown in Table 3. Saudi women were 6.58 times more likely to perform routine dental visits during pregnancy than non- Saudi women (p 0.036). The participants who had a negative perception about the safety of dental treatment during pregnancy had significantly lower odds (OR 0.33) of routine dental visits than those who had no such perceptions (p 0.034).
Table 3.
Association of different factors with routine dental visits among pregnant women
| Factors | Unadjusted OR (95% CI) | P value | Adjusted OR (95% CI) | P value |
|---|---|---|---|---|
| Nationality: | ||||
| Saudi | 6.58 (0.87,49.52) | 0.036* | 7.38 (0.97, 56.16) | 0.05* |
| Non-Saudi | ||||
| Age | ||||
| < 30 | 0.85 (0.42,1.69) | 0.639 | 0.86 (0.41,1.85) | 0.709 |
| ≥ 30 | ||||
| Education | ||||
| School education | 0.77 (0.38, 1.54) | 0.460 | 0.96 (0.4, 2.32) | 0.932 |
| College/university education | ||||
| Employment status | ||||
| Employed | 1.3 (0.64, 2.65) | 0.463 | 1.22 (0.49, 3.05) | 0.661 |
| Not employed | ||||
| Systemic disease | ||||
| Yes | 1.13 (0.44, 2.92) | 0.796 | 1.33 (0.48, 3.63) | 0.582 |
| No | ||||
| Insurance | ||||
| Yes | 1.31 (0.64, 2.68) | 0.464 | 1.24 (0.55, 2.78) | 0.607 |
| No | ||||
| Perception of oral health: | ||||
| Good | 0.91 (0.33, 2.52) | 0.856 | 0.92 (0.32, 2.68) | 0.880 |
| Poor | ||||
| Fear of dental treatment | 0.39 (0.11, 1.33) | 0.120 | 0.38 (0.11, 1.34) | 0.131 |
| Negative perception about the safety of dental treatment | 0.33 (0.11,0.96) | 0.034* | 0.31 (0.11, 0.93) | 0.036* |
Statistically significant.
After adjustments, ethnicity and the perception about the safety of dental treatment during pregnancy remained significant predictors of routine dental visits. There were significantly higher chances (OR 7.38, p 0.05) for Saudi versus non-Saudi pregnant women to perform routine dental visits.
The women with a negative perception about the safety of dental treatment during pregnancy were less likely to attend a dental office for routine dental visits (OR 0.31, p 0.036).
Table 4 shows the results of bivariate and multivariate logistic regression analyses about the association of different factors with dental visits related to oral problems. Interestingly, no statistically significant relationship was observed.
Table 4.
Association of different factors with dental visits related to oral problems among pregnant women
| Factors | Unadjusted OR (95% CI) | P value | Adjusted OR (95% CI) | P value |
|---|---|---|---|---|
| Nationality: | ||||
| Saudi | 0.90 (0.45, 1.81) | 0.85 (0.42, 1.74) | 0.853 | |
| Non-Saudi, | ||||
| Age | ||||
| < 30 | 1.09 (0.67, 1.76) | 0.735 | 1.07 (0.64, 1.81) | 0.788 |
| ≥ 30 | ||||
| Education | ||||
| School education | 0.90 (0.56, 1.46) | 0.678 | 1.01 (0.57, 1.8) | 0.975 |
| College/university education | ||||
| Employment status | ||||
| Employed | 1.18 (0.71, 1.95) | 0.524 | 1.12 (0.61, 2.07) | 0.705 |
| Not employed | ||||
| Systemic disease | ||||
| Yes | 0.74 (0.37, 1.47) | 0.391 | 0.72 (0.35, 1.48) | 0.376 |
| No | ||||
| Insurance | ||||
| Yes | 1.46 (0.87, 2.43) | 0.147 | 1.47 (0.84, 2.57) | 0.171 |
| No | ||||
| Perception of oral health | ||||
| Good | 0.85 (0.42, 1.76) | 0.673 | 0.75 (0.36, 1.58) | 0.451 |
| Poor | ||||
| Fear of dental treatment | 1.22 (0.65, 2.31) | 0.536 | 1.23 (0.64, 2.36) | 0.542 |
| Negative perception about the safety of dental treatment | 0.7 (0.4, 1.24) | 0.224 | 0.71 (0.39, 1.27) | 0.244 |
Discussion
This study demonstrated inequalities in dental care utilization among pregnant women. Our results confirmed that a small proportion of women (13.7%) visited dental office for regular dental visits. A previous study by Gaffar et al., (2016) showed that 18% of women regularly visited dentists in Dammam, Eastern province of Saudi Arabia [14]. The reason of slightly lower regular dental attendance in our study compared with the results by Gaffar et al. might be related to the method of data collection. Our sample was collected from various hospitals and health centers in different cities of the province whereas the study by Gaffar et al., included pregnant women from one government hospital in Dammam.
Although routine dental care utilization is important for good oral health of mothers and children, however, its distribution is low among pregnant women in different countries. Similar to our study findings, Hashim (2011) observed that 14.4% of pregnant women visited dentists for routine dental check-up in the United Arab Emirates [15]. Likewise, a small proportion of pregnant women (19.6%) attended dental office for routine dental examination in Greece [16]. Boggess et al., (2010) reported that 26% of pregnant women received routine dental care in the U.S. [10] Amin and ElSalhy (2014) found that about half the sample visited the dentist during pregnancy and 93% of them performed regular dental visits in Canada [17]. Bamanikar and Kee (2013) indicated that 26.9% of pregnant women received routine dental check-up at least twice a year in Brunei, Darussalam [18]. A study of pregnant women by Saddki et al. (2010) showed that 30.6% of participants visited dentists for routine dental visits in Malaysia [19].
Lack of regular dental visits can aggravate dental problems including pregnancy gingivitis [16]. Pregnant women are at increased risk of dental caries, erosion, periodontal diseases, gingival enlargement, loosening of teeth, and ill-fitting dental prostheses. Hormonal, dietary, and oral hygiene changes and repeated acid attacks due to nausea and vomiting can contribute to dental problems among pregnant women [20]. It is known that the lack of routine dental care utilization before pregnancy is strongly associated with decreased dental visits during pregnancy [10]. So, routine dental visits should be performed not only while being pregnant but also when not pregnant. Evidence also shows that women who perform routine dental visits demonstrate improved knowledge about the prevention of caries in children [14]. Therefore, the American Dental Association recommends that pregnant women should not be treated differently from non-pregnant women, and strongly advises on following the guidelines of treating pregnant women [21].
In our study, half the sample (43.7%) visited the dentist when they had a dental problem and the most common reason for dental attendance was toothache (26.7%). Similar to our study, half of the pregnant women performed dental visits due to dental problem mostly because of dental pain in Kuwait [22]. Likewise, the majority of pregnant women performed dental visits when they had a dental pain in United Arab Emirates [15]. A study by Marchi et al., (2013) found that pain was the most common cause of dental attendance among pregnant women in the U.S [23]. Vergnes et al., (2013) identified that 57% of French women suffered from at least one dental problem during pregnancy and the most commonly reported problem was gingival disease (42%) followed by dental pain (20%) [24]. Increased dental attendance due to dental problems in our study can be explained by high prevalence of the dental caries in Saudi Arabia. The prevalence of dental caries reaches 89% in adults aged 30 to 40 years in the country [25]. In addition, pregnant women demonstrate inflammation of periodontal tissues [26]. Moreover, there is high distribution of dental problems (69-72%) among pregnant women [12].
The present study showed that most of the women (40.7%) who performed dental visit due to dental problems did so during the second trimester which was significantly higher than in first (25.4%) and third (33.9%) trimesters (p 0.049). This disagrees with the findings of a study by Martins (2014), where the majority of Brazilian pregnant women (11.4%) received dental consultation in the first trimester [27]. Saddki et al., (2010) reported that most pregnant women (50.0%) visited the dentist during the first trimester in Malaysia [19]. It is known that dental treatment is safe during the second trimester since organogenesis is complete and the risk to developing fetus is low. On the other hand, dental treatment during the first trimester should be limited to oral health education, periodontal prophylaxis, and emergency treatments, because of fetus development and high risk of teratogenesis. Moreover, spontaneous abortions occur mostly (50-75%) during first the 4th weeks of pregnancy [28]. It is encouraging that most participants in our study performed dental visits during the second trimester. Almost half of our sample (52.6%) indicated to avoid dental visits during pregnancy. The most important reason was the negative perception about the safety of dental treatment during pregnancy (24.8%). This result comes in agreement with a study by Dar-Odeh (2018) in Al Madinah, Saudi Arabia in which 43.6% of pregnant women avoided dental visits due to a misconception regarding the safety of dental local anesthesia [29] Dinas et al., (2007) showed that 72.2% of women in Greece considered that dental treatment might cause adverse effects during pregnancy [16]. A recent systematic review found that limited use of dental care services during pregnancy was because the majority of women (72.2%) believe that dental treatment could lead to negative pregnancy outcomes [30]. According to the American Dental Association, dental treatment is safe and pregnant women who are identified to have dental problems should be referred to the dentist. The association also emphasizes the importance of providing all the necessary oral health services and maintaining good oral health throughout pregnancy. This eventually will contribute to increase the number of dental visits during pregnancy, improve oral health, and reduce the number of pregnant women without dental care [21].
Our study added valuable information to the knowledge base about the inequalities among pregnant women regarding access to oral care services. However, there were certain limitations of the study. One of the limitations of our study was self-reported data in cross-sectional study design which can be subject to recall bias. In addition, the study included pregnant women visiting three main hospitals and health centers in the major cities of the Eastern province of Saudi Arabia. Therefore, the generalization of study findings to pregnant women visiting other hospitals and healthcare centers in remote areas of the province should be done with caution.
In conclusion, dental care utilization was low in our sample of pregnant women. A small percentage of women visited the dentist for regular dental visits and non-Saudi women were less likely to perform routine dental visits. A considerable proportion of pregnant women attended a dentist due to dental problems. The misconception about the safety of dental treatment was the most common reason of avoiding dental visits among pregnant women. Oral health care services should be routinely provided to all pregnant women which should include oral health advice and education, preventive and necessary dental treatments. These measures would reduce inequalities regarding dental care utilization among pregnant women and improve their quality of life. It is important to raise knowledge about the importance of maintaining good oral health by visiting a dentist during pregnancy. Dentists and gynecologists should establish collaborations to improve the oral health of pregnant women.
Footnotes
Funding: This research did not receive any financial support
Competing Interests: The authors have declared that no competing interests exist
References
- 1.Little JW, Falace D, Miller C, Rhodus NL. Dental Management of the Medically Compromised Patient-E-Book. Elsevier Health Sciences; 2017. [Google Scholar]
- 2.Giglio JA, Lanni SM, Laskin DM, Giglio NW. Oral health care for the pregnant patient. Dent Assist. 2013;82(6):38. 40, 42 passim. [PubMed] [Google Scholar]
- 3.Srinivas SK, Parry S. Periodontal disease and pregnancy outcomes:time to move on? J Womens Health (Larchmt) 2012;21(2):121–5. doi: 10.1089/jwh.2011.3023. https://doi.org/10.1089/jwh.2011.3023 PMid:21992584 PMCid:PMC3270055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bobetsis YA, Barros SP, Offenbacher S. Exploring the relationship between periodontal disease and pregnancy complications. J Am Dent Assoc. 2006;137:S7–13. doi: 10.14219/jada.archive.2006.0403. https://doi.org/10.14219/jada.archive.2006.0403 PMid:17012730. [DOI] [PubMed] [Google Scholar]
- 5.Pihlstrom BL, Michalowicz BS, Johnson NW. Periodontal diseases. Lancet. 2005;366(9499):1809–20. doi: 10.1016/S0140-6736(05)67728-8. https://doi.org/10.1016/S0140-6736(05)67728-8. [DOI] [PubMed] [Google Scholar]
- 6.Laine MA. Effect of pregnancy on periodontal and dental health. Acta Odontol Scand. 2002;60(5):257–64. doi: 10.1080/00016350260248210. https://doi.org/10.1080/00016350260248210 PMid: 12418714. [DOI] [PubMed] [Google Scholar]
- 7.Boggess KA, Edelstein BL. Oral health in women during preconception and pregnancy:implications for birth outcomes and infant oral health. Matern Child Health J. 2006;10(5 Suppl):S169–74. doi: 10.1007/s10995-006-0095-x. https://doi.org/10.1007/s10995-006-0095-x PMid:16816998 PMCid:PMC1592159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ritter AV, Southerland JH. Pregnancy and oral health. J Esthet Restor Dent. 2007;19(6):373–4. doi: 10.1111/j.1708-8240.2007.00139.x. https://doi.org/10.1111/j.1708-8240.2007.00139.x PMid:18005289. [DOI] [PubMed] [Google Scholar]
- 9.Lopez NJ, Da Silva I, Ipinza J, Gutierrez J. Periodontal therapy reduces the rate of preterm low birth weight in women with pregnancy-associated gingivitis. J Periodontol. 2005;76(11 Suppl):2144–53. doi: 10.1902/jop.2005.76.11-S.2144. https://doi.org/10.1902/jop.2005.76.11-S.2144. [DOI] [PubMed] [Google Scholar]
- 10.Boggess KA, Urlaub DM, Massey KE, et al. Oral hygiene practices and dental service utilization among pregnant women. J Am Dent Assoc. 2010;141(5):553–61. doi: 10.14219/jada.archive.2010.0228. https://doi.org/10.14219/jada.archive.2010.0228 PMid:20436103 PMCid:PMC4380010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Malkawi ZA, Tubaishat RS. Knowledge, practice and utilization of dental services among pregnant women in the north of Jordan. J Contemp Dent Pract. 2014;15(3):345–51. doi: 10.5005/jp-journals-10024-1541. https://doi.org/10.5005/jp-journals-10024-1541 PMid:25307819. [DOI] [PubMed] [Google Scholar]
- 12.Al-Swuailem AS, Al-Jamal FS, Helmi MF. Treatment perception and utilization of dental services during pregnancy among sampled women in Riyadh, Saudi Arabia. The Saudi Journal for Dental Research. 2014;5(2):123–29. https://doi.org/10.1016/j.ksujds.2013.11.002. [Google Scholar]
- 13.Al Habashneh R, Guthmiller JM, Levy S, et al. Factors related to utilization of dental services during pregnancy. J Clin Periodontol. 2005;32(7):815–21. doi: 10.1111/j.1600-051X.2005.00739.x. https://doi.org/10.1111/j.1600-051X.2005.00739.x PMid:15966891. [DOI] [PubMed] [Google Scholar]
- 14.Gaffar BO, El Tantawi M, Al-Ansari A, AlAgl AS. Association between oral health knowledge and practices of Saudi pregnant women in Dammam, Saudi Arabia. East Mediterr Health J. 2016;22(6):411–16. doi: 10.26719/2016.22.6.411. https://doi.org/10.26719/2016.22.6.411 PMid:27686982. [DOI] [PubMed] [Google Scholar]
- 15.Hashim R. Self-reported oral health, oral hygiene habits and dental service utilization among pregnant women in United Arab Emirates. Int J Dent Hyg. 2012;10(2):142–6. doi: 10.1111/j.1601-5037.2011.00531.x. https://doi.org/10.1111/j.1601-5037.2011.00531.x PMid:22040165. [DOI] [PubMed] [Google Scholar]
- 16.Dinas K, Achyropoulos V, Hatzipantelis E, et al. Pregnancy and oral health:utilisation of dental services during pregnancy in northern Greece. Acta Obstet Gynecol Scand. 2007;86(8):938–44. doi: 10.1080/00016340701371413. https://doi.org/10.1080/00016340701371413 PMid:17653878. [DOI] [PubMed] [Google Scholar]
- 17.Amin M, ElSalhy M. Factors affecting utilization of dental services during pregnancy. J Periodontol. 2014;85(12):1712–21. doi: 10.1902/jop.2014.140235. https://doi.org/10.1902/jop.2014.140235 PMid:25119559. [DOI] [PubMed] [Google Scholar]
- 18.Bamanikar S, Kee LK. Knowledge, attitude and practice of oral and dental healthcare in pregnant women. Oman Med J. 2013;28(4):288–91. doi: 10.5001/omj.2013.80. https://doi.org/10.5001/omj.2013.80 PMid:23904926 PMCid:PMC3725248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Saddki N, Yusoff A, Hwang YL. Factors associated with dental visit and barriers to utilisation of oral health care services in a sample of antenatal mothers in Hospital Universiti Sains Malaysia. BMC Public Health. 2010;10:75. doi: 10.1186/1471-2458-10-75. https://doi.org/10.1186/1471-2458-10-75 PMid:20163741 PMCid:PMC2834630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.New York State Department of Health. Oral Health Care during Pregnancy and Early Childhood Practice Guidelines. New York State Department of Health; 2006. [Google Scholar]
- 21.American Dental Association. Oral health during pregnancy What to expect when expecting. American Dental Association; 2011. [Google Scholar]
- 22.Honkala S, Al-Ansari J. Self-reported oral health, oral hygiene habits, and dental attendance of pregnant women in Kuwait. J Clin Periodontol. 2005;32(7):809–14. doi: 10.1111/j.1600-051X.2005.00770.x. https://doi.org/10.1111/j.1600-051X.2005.00770.x PMid:15966890. [DOI] [PubMed] [Google Scholar]
- 23.Marchi KS, Fisher-Owens SA, Weintraub JA, Yu Z, Braveman PA. Most pregnant women in California do not receive dental care:findings from a population-based study. Public Health Rep. 2010;125(6):831–42. doi: 10.1177/003335491012500610. https://doi.org/10.1177/003335491012500610 PMid:21121228 PMCid:PMC2966664. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Vergnes JN, Pastor-Harper D, Constantin D, et al. Perceived oral health and use of dental services during pregnancy:the MaterniDent study. Sante Publique. 2013;25(3):281–92. https://doi.org/10.3917/spub.253.0281 PMid:24007904. [PubMed] [Google Scholar]
- 25.Al-Ansari AA. Prevalence, severity, and secular trends of dental caries among various Saudi populations:A literature review. Saudi Journal of Medicine and Medical Sciences. 2014;2(3):142. https://doi.org/10.4103/1658-631X.142496. [Google Scholar]
- 26.Machado FC, Cesar DE, Apolonio AC, Ribeiro LC, Ribeiro RA. Longitudinal study on clinical and microbial analysis of periodontal status in pregnancy. Braz Oral Res. 2016;30(1):e87. doi: 10.1590/1807-3107BOR-2016.vol30.0087. https://doi.org/10.1590/1807-3107BOR-2016.vvol30.0087. [DOI] [PubMed] [Google Scholar]
- 27.Martins RFM, de Azevedo JAP, Dourado CRL, et al. Oral health behaviors and dental treatment during pregnancy:a cross-sectional study nested in a cohort in Northeast Brazil. Pesquisa Brasileira em Odontopediatria e Clínica Integrada. 2014;14(1):5–11. https://doi.org/10.4034/PBOCI.2014.141.01. [Google Scholar]
- 28.Kurien S, Kattimani VS, Sriram RR, et al. Management of pregnant patient in dentistry. Journal of international oral health: JIOH. 2013;5(1):88. [PMC free article] [PubMed] [Google Scholar]
- 29.Dar-Odeh N, Binsaad SM, Gasim RA, et al. Why do Women avoid Dental Visits During Pregnancy?A Cross-Sectional Survey in Al Madinah, Western Saudi Arabia. Pesquisa Brasileira em Odontopediatria e Clinica Integrada. 2018;18(1):3934. https://doi.org/10.4034/PBOCI.2018.181.31. [Google Scholar]
- 30.Rocha JS, Arima L, Chibinski AC, et al. Barriers and facilitators to dental care during pregnancy:a systematic review and meta-synthesis of qualitative studies. Cad Saude Publica. 2018;34(8):e00130817. doi: 10.1590/0102-311X00130817. https://doi.org/10.1590/0102-311x00130817. [DOI] [PubMed] [Google Scholar]