

Abstract
Background
Accuracy of electrocardiogram (ECG) interpretation is important for identification of ST-elevation myocardial infarction (STEMI) by Emergency Medical Services (EMS) personnel who recognize STEMI in the field and activate the coronary catheterization laboratory. According to previous research, there is improvement in diagnosis of STEMIs for healthcare providers who read an average of > 20 ECGs per week. This study evaluated the effectiveness of online ECG modules on improving diagnostic accuracy.
Methods
EMS personnel received 25 ECGs per week to interpret via an online program. Diagnostic accuracy was assessed for improvement via completion of an ECG evaluation package before and after the intervention. Job satisfaction data were collected to determine the impact of the educational initiative.
Results
A total of 64 participants completed the study. Overall, there was an improvement in ECG diagnostic accuracy from 50.8% to 61.2% (95% confidence interval [CI], 7.7-13.2; P < 0.0001). Specifically, there was significant improvement in the diagnosis of STEMI (8.5%; 95% CI, 4.9-12.3; P < 0.003) and supraventricular tachycardia (39.0%; 95% CI, 17.2-60.8; P < 0.008), with a trend toward improvement in all other diagnoses. These effects were sustained to 3 months (9.6%; 95% CI, 6.4-12.7; P < 0.0001). Improvement was seen regardless of employment experience and training. There was no significant impact on job satisfaction.
Conclusions
ECG exposure remains an important factor in improving the accuracy of ECG diagnosis in EMS personnel. Online education modules provide an easily accessible way of improving ECG interpretation with the opportunity for positive downstream effects on patient outcomes and resource use.
Résumé
Introduction
L’interprétation de l’électrocardiogramme (ECG) doit être précise pour détecter l’infarctus du myocarde avec élévation du segment ST (STEMI) puisque le personnel des services médicaux d’urgence (SMU) doit reconnaître sur le terrain le STEMI et faire démarrer le processus vers le laboratoire de cathétérisme coronarien. Selon une étude antérieure, on note une amélioration dans le diagnostic du STEMI chez les prestataires de soins de santé qui lisent en moyenne > 20 ECG par semaine. La présente étude a permis d’évaluer l’efficacité des modules d’ECG en ligne en fonction de l’amélioration de la précision du diagnostic.
Méthodes
Le personnel des SMU recevait chaque semaine 25 ECG à interpréter au moyen d’un programme en ligne. On évaluait la précision du diagnostic en fonction de son amélioration en remplissant un module d’évaluation d’ECG avant et après l’intervention. Les données sur la satisfaction professionnelle étaient collectées pour déterminer les répercussions de l’initiative éducative.
Résultats
Un total de 64 participants ont complété l’étude. Dans l’ensemble, on a noté une amélioration de la précision du diagnostic à l’ECG, soit de 50,8 % à 61,2 % (intervalle de confiance [IC] à 95 %, 7,7-13,2; P < 0,0001). Notamment, on a noté une amélioration importante dans le diagnostic du STEMI (8,5 %; IC à 95 %, 4,9-12,3; P < 0,003) et de la tachycardie supraventriculaire (39,0 %; IC à 95 %, 17,2-60,8; P < 0,008), ainsi qu’une tendance à l’amélioration pour tous les autres diagnostics. Ces effets se sont maintenus jusqu’à 3 mois (9,6 %; IC à 95 %, 6,4-12,7; P < 0,0001). On a observé une amélioration, quelles que soient l’expérience professionnelle et la formation. Il n’y a eu aucune répercussion importante sur la satisfaction professionnelle.
Conclusions
L’exposition à l’ECG demeure un facteur important dans l’amélioration de la précision du diagnostic à l’ECG chez le personnel des SMU. Les modules éducatifs en ligne constituent des outils facilement accessibles pour améliorer l’interprétation de l’ECG en plus d’offrir la possibilité d’effets positifs en aval sur les résultats cliniques des patients et l’utilisation des ressources.
Creation of regional systems for ST-elevation myocardial infarction (STEMI) care and incorporating direct transport by Emergency Medical Services (EMS) personnel to hospitals capable of percutaneous coronary intervention are essential in achieving the goal of first medical contact to device time within 90 minutes or less.1 The level of care provided by the EMS is dependent on legislation and varies between countries and regions. In some systems, physician staff ambulances and, in others, EMS personnel are considered the most trained individuals. Although EMS training varies among different regions, the common focus is advanced life support. EMS personnel often have minimal, if any, formal training in electrocardiogram (ECG) interpretation, leading to inaccuracy in diagnoses compared with other healthcare providers who participate in the care of patients with STEMI.2, 3 This is a concern, because a key factor in the STEMI chain of survival is accurate ECG interpretation by EMS personnel.4, 5 Incorporating paramedics in cardiac catheterization laboratory (CCL) activation has been associated with a reduction in first medical contact to device time or reperfusion and greater likelihood of achieving reperfusion in a timely manner.1, 6, 7, 8, 9 However, incorrect ECG interpretation may lead to false activation, unnecessary procedures, and delay in diagnosis of patients who may have other serious conditions.10, 11, 12, 13, 14
We have previously shown that the diagnostic accuracy of STEMI interpretation by healthcare providers is linked to exposure to ECG reading, with significant improvement when more than 20 ECGs are read per week.2 This improvement was seen regardless of previous training or current level of expertise, thereby making it a potentially useful target in improving ECG interpretation across a heterogeneous population of healthcare providers. EMS personnel have been shown to be the least accurate diagnosticians in regard to STEMI, when compared with other healthcare providers.2, 3 Considering that ECG interpretation by EMS personnel is one of the weakest links in the STEMI chain of survival, our aim was to assess how ECG exposure on a weekly basis affects their accuracy of ECG interpretation. Because professional development is key for employee satisfaction, we also assessed how ECG training of EMS personnel affects their job satisfaction.15
Methods
Study population and setting
EMS personnel, including Primary Care Paramedics (PCPs) and Advanced Care Paramedics (ACPs), from Middlesex-London (Ontario, Canada) Medical Services Department participating in the regional STEMI program were recruited.
Each participant was invited to complete a baseline ECG evaluation package followed by an 8-week online education module consisting of weekly interpretation of 25 ECGs. After completion of the training module, participants completed a second evaluation. Subsequently, without further training, a third evaluation was performed to assess the impact 3 months after completion of the training module. The evaluation packages were also preceded by an online version of the short form of the Minnesota Job Satisfaction Questionnaire (MSQ) (with permission from University of Minnesota’s Vocational Psychology Research Center) for each of the 3 evaluation periods.16 The short form of the MSQ was chosen because it is a well-known instrument that has been shown to be stable over time and has excellent alpha coefficient values (0.85-0.91) in previous studies. It is also concise compared with other available instruments and has been used and validated in various healthcare worker populations.16, 17, 18, 19
The link for study materials, including evaluation and training modules, was sent by email linking to Research Electronic Data Capture, a secure web application. Participant characteristics were collected via a standardized online survey.
Study protocol
This study was approved by the Western University Research Ethics Board, and each participant was provided with informed consent form before enrollment. The evaluation package contained 40 ECGs that were selected from a patient-derived database of common ECG presentations with a focus on STEMI and STEMI mimics. STEMI ECGs were chosen from patients who had primary percutaneous coronary intervention with confirmation of a culprit lesion. Prehospital ECGs were used, including those with confirmed STEMIs and false STEMIs representing mimics. These mimics included left ventricular hypertrophy, left bundle branch block, supraventricular tachycardia, non–ST-elevation myocardial infarction (NSTEMI), early repolarization, ventricular tachycardia, paced rhythm, and pericarditis. NSTEMI ECGs featured changes consistent with myocardial ischemia including ST-segment depression and T-wave inversions. Upon completion of the preintervention evaluation package, each participant received access to the education module. Each of the 8 weekly modules contained 25 ECGs, which were made up of a similar composition to the evaluation package. The same drop-down menu of diagnoses was provided as in the evaluation package; additionally, the correct response and a short explanation were given for each ECG in the education module (Fig. 1). There was no didactic ECG teaching component to the ECG module.
Figure 1.

Example of a prehospital electrocardiogram (ECG) representing an inferior STEMI used in the education module. The radio buttons (drop-down menu in online version) represent included options for diagnosis. The correct response stem includes an explanation of the correct diagnosis (only visible after choosing an answer and confirming in online version). NSTEMI, non–STEMI; STEMI, ST-elevation myocardial infarction.
The subsequent weekly module was only sent on completion of the previous week within the specified time limit. After completion of the modules, a postintervention evaluation package, which included the same 40 ECGs as the preintervention package in a different sequence, was provided to participants to measure their performance. Three months after the completion of all participant modules, a third iteration or “long-term” evaluation package was distributed. To proceed through the study, each subsequent step needed to be preceded by a completed prerequisite step, which included the previous ECG module or evaluation. To assess if this type of training improves job satisfaction, an online version of the short form MSQ was distributed with each of the ECG evaluation packages.
Analysis
Continuous variables are summarized by mean and standard deviation and compared using paired t test or analysis of variance. Comparison of effectiveness of training is reported as confidence intervals (CIs) in relation to mean improvement. The accuracy of ECG interpretation was also analyzed according to level of training and years of experience.
P values less than 0.05 were considered to be significant. GraphPad Prism 7 (GraphPad Software, La Jolla, CA) was used to perform statistical analysis.
Results
A total of 64 participants from Middlesex-London EMS, who were actively involved in the STEMI program at our institution, completed the study protocol (Fig. 2). Participants included 41 PCPs and 23 ACPs. ACPs have at least 2 years of paramedic field training before being able to qualify for a third year of intensive in-class didactic and in-hospital clinical training. There was a significant improvement in diagnostic accuracy after completing the 8-week ECG education module (Fig. 3). Overall, EMS participants improved 9.5% above baseline and an average score of 50.8% to 61.2% (9.5% CI, 7.7-13.2; P < 0.0001). This effect was sustained to the 3-month follow up period, with maintenance of diagnostic improvement compared with baseline values (9.6%; 95% CI, 6.4-12.7; P < 0.0001). There was no significant difference (P = 0.79) between the postintervention and 3-month follow-up accuracy, representing a sustained intervention effect. There was a significant improvement in recognition of the diagnoses of STEMI and, supraventricular tachycardia (Fig. 4). Before intervention, EMS participants had a sensitivity of 0.7 and a specificity of 0.3 for diagnosing STEMI in the given ECG package. After the 8-week intervention, EMS sensitivity improved to 0.8 and specificity to 0.3. Anterior STEMIs were the most readily diagnosed, whereas posterior STEMIs were least accurately diagnosed. The most common diagnoses mistaken for STEMI included pericarditis, left bundle branch block, NSTEMI, and left ventricular hypertrophy. Pericarditis was the least well-recognized diagnosis overall.
Figure 2.
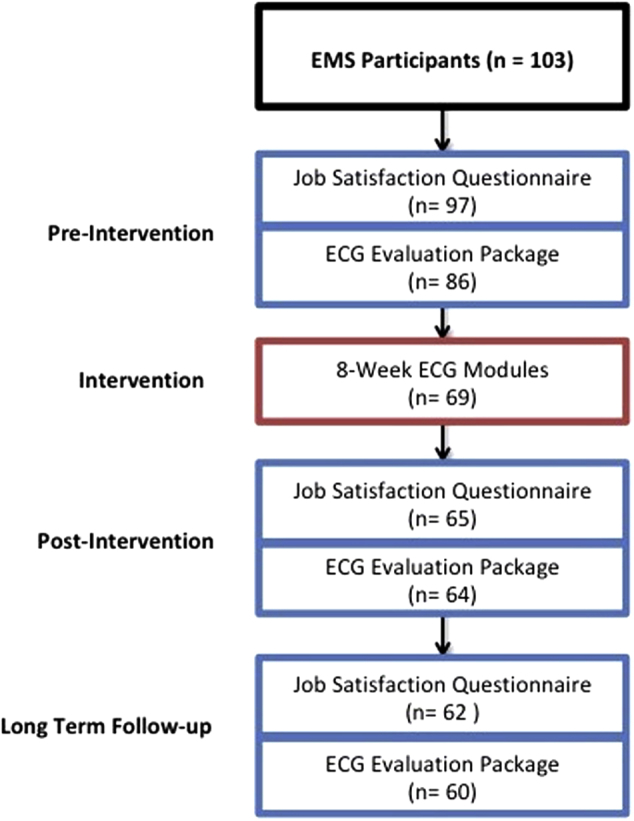
Study flow diagram. ECG = electrocardiogram; EMS = Emergency Medical Services.
Figure 3.

Accuracy of ECG interpretation represented as mean accuracy. Improvement in accuracy seen postintervention (Post) compared with baseline (Pre) (95% confidence interval [CI], 7.7-13.2; P < 0.0001). This difference was also seen between the baseline (Pre) and 3-month follow-up (long-term) means (95% CI, 6.4-12.7; P < 0.0001). There was no significant difference between the postintervention (Post) and 3-month follow up (long-term) accuracy, representing a sustained effect of the intervention.
Figure 4.

Accuracy of ECG diagnosis by diagnosis. Mean improvement in accuracy stratified by diagnosis. There was significant improvement in recognition of the diagnoses of STEMI (8.6%; 95% CI, 4.9-12.3; P < 0.003) and supraventricular tachycardia (39%; 95% CI, 17.2-60.8; P < 0.008). *Significant improvement. **Groups with < 3 data points could not be analyzed. LBBB, left bundle branch block; LVH, left ventricular hypertrophy; NSTEMI, non–STEMI; STEMI, ST-elevation myocardial infarction; SVT, supraventricular tachycardia.
Improvement in ECG diagnostic accuracy was equally seen across all levels of training and experience (Fig. 5). Most study participants (43/64, 67%) had more than 5 years of experience. Although there was a significant difference in baseline accuracy between ACPs and PCPs, with mean scores of 56.3% and 48.8%, respectively (7.5%, CI, −13.3 to 1.7; P = 0.012), there was no significant difference in accuracy improvement between ACPs and PCPs (1.2%, CI, −6.5 to 4.1; P = 0.64). There was no difference in baseline accuracy of ECG interpretation when participants were stratified by years of experience. EMS participants did not report any significant impact on job satisfaction related to their participation in the STEMI program at our institution upon study completion.
Figure 5.

Improvement in accuracy (%) by years of experience. Mean improvement from baseline in ECG diagnostic accuracy, stratified by years of working experience. There was no significant difference between groups (P = 0.71). The coloured dots delineate the difference in training between the participating paramedics; there was no significant difference in baseline improvement related to paramedic training (P = 0.64). ACP, Advanced Care Paramedic; PCP, Primary Care Paramedic.
Discussion
The results of this study show that an ECG education module, using an online platform based simply on ECG exposure, is effective at improving ECG diagnostic accuracy in EMS personnel. This effect was seen immediately after the distribution of the 8-week module but was also sustained to 3 months after the intervention.
Paramedics currently in training receive classroom sessions on ECG interpretation and STEMI recognition before graduation, as well as base training before working in the field. More experienced paramedics may have received no formal training at all. Given the prehospital activation of extensive hospital resources and patient outcome-associated factors, optimizing CCL activation and diagnosis of STEMI should be a key educational objective. Studies that have examined ECG education in various healthcare provider streams have generally focused on delivery via classroom lectures or handouts, with varying effect.20, 21, 22, 23 Online or web-based teaching has been shown to have comparable efficacy with more traditional lecture or workshop-based teaching in regard to ECGs.24, 25, 26 It has been postulated that web-based training may, in fact, be more effective than traditional teaching methods.27, 28 Medical students appreciated a web-based program and attributed its success to greater immediacy, improved visualization, and interactivity. The ease of use for this method of teaching is especially applicable to a population of EMS personnel who work varying hours, often spending the majority of their shifts in-transit. The improvement in sensitivity of diagnosing STEMI after the intervention is important because EMS are responsible for initially screening patients at the time of first medical contact. In our institution, ECGs are electronically transmitted to an Interventional Cardiologist for review before activating the CCL. This type of system emphasizes the importance in improving sensitivity of diagnosis rather than specificity because the ECGs are over-read by an expert. Acceptable false-positive rates range from 7% to 14%.10, 13, 29 Our study shows a false-positive rate of 17% to 20% that could be attributed to EMS interpreting the ECG in isolation, rather than in clinical context, as they would in real-life situations.
Most ECG interpretation is based on recognition-primed decision making. In complex situations with multiple confounders, experts use reason based on underlying principles when recognition is insufficient to make accurate diagnoses.30 Effort was made to incorporate ECGs that were representative of what EMS would learn about in training, as well as what would be commonly encountered in the field. Package material was reviewed by the local Middlesex-London EMS, Superintendent of Education to ensure compliance with these goals. Although effective at improving accuracy, the overall accuracy of diagnosis may appear low, considering the EMS responsibility in the STEMI chain of survival. The low accuracy does compare with previous studies that looked at ECG interpretation in a similar educational manner and showed that confounding factors decrease accuracy.3, 23 We chose ECGs for the study that are encountered by EMS personnel, including many that are not easy to interpret in an effort to perform a comprehensive assessment. This approach resulted in relatively low accuracy rate. Therefore, the degree of accuracy is less important in our study compared with the improvement in diagnosis.
This tool’s usefulness to educate a heterogeneous population of healthcare professionals is evidenced in the resulting improvement in accuracy seen postintervention. Despite the baseline difference between ACPs and PCPs preintervention, there was no difference seen in mean improvement. This reinforces the validity of using this type of ECG training in heterogeneous populations of participants. ACPs spend 1 year longer in school before starting work, and during that time they spend more time on cardiology modules and ECG teaching; therefore, they would be expected to be superior at ECG interpretation. Despite this fact, the web-based delivery of ECG modules is a new and different technique for teaching ECGs that has not been used routinely before. This may explain why both groups had similar improvement, because they would not have been previously exposed to this type of teaching, without a didactic component.
Of note, there was also no difference seen related to years of paramedic experience. Prior studies echo this finding among various healthcare providers, which have a wider breadth of practice including EMS.3, 31 ECG and specialized cardiac care exposure, such as that gained in a Cardiac Care Unit, affect diagnostic accuracy.2, 31 The widespread applicability of the education module simplifies the development and delivery of the tool, the possible beneficiaries, and the implications for system wide impact. These results also help to support the use of this education initiative across various healthcare groups, including resident physicians who are active participants in CCL activations.
Although our educational model leads to improvement in ECG interpretation, there was no effect on EMS job satisfaction. Organizational professional training provides attention to the employees, a fact that increases satisfaction with the workplace. There is limited research exploring the relationship between e-learning and employee satisfaction.32 The benefits of online training are significant (using time, space, technology integration, and individualization).33 However, in terms of the contribution to employee workplace satisfaction, interpersonal interaction is lost and less attention is given to the individual.34 It is important to consider that CCL activation and treatment of patients with STEMI are small components of EMS responsibility. Therefore, it is plausible that this intervention may not have affected a big enough component of EMS activities to improve job satisfaction.
Limitations
This study was performed in a single EMS population. However, Middlesex-London EMS serves 10 areas with a population of approximately 500,000. Our sample size was small, and therefore we may have been unable to detect small differences within groups. As seen in Figure 2, there was drop-out from the beginning to the end of the study. Completion of the study itself required up to 10 hours of time commitment with little compensation; therefore, we may not have reached the optimal number of EMS providers. Also, it is possible that the characteristics of those who completed the study are different from those who did not complete the study. However, considering the importance of ECG exposure and training, such a module may be incorporated as part of mandatory paramedics continuing medical education, resulting in a high level of participation and higher impact on patient outcomes. Future studies would be useful to assess clinical implications of EMS improvement in ECG diagnostic accuracy.
Conclusions
This study shows that simple ECG exposure is an effective way to improve ECG diagnostic accuracy among EMS personnel, who play an important role in expediting care to patients with STEMI. Online ECG modules provide an easily accessible way of improving interpretation with the opportunity for positively affecting health systems, outcomes, and resource use.
Acknowledgements
The authors acknowledge the contribution of Jay Loosely, Superintendent of Education for Middlesex-London EMS, and the EMS personnel from Middlesex-London EMS who participated in our study.
Disclosures
The authors have no conflicts of interest to disclose.
Footnotes
See page 33 for disclosure information.
Ethics Statement: This study was approved by the Western University Research Ethics Board, and each participant was provided with informed consent form before enrollment.
References
- 1.O’Gara P.T., Kushner F.G., Ascheim D.D. 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:e362–e425. doi: 10.1161/CIR.0b013e3182742cf6. [DOI] [PubMed] [Google Scholar]
- 2.Huitema A.A., Zhu T., Alemayehu M., Lavi S. Diagnostic accuracy of ST-segment elevation myocardial infarction by various healthcare providers. Int J Cardiol. 2014;177:825–829. doi: 10.1016/j.ijcard.2014.11.032. [DOI] [PubMed] [Google Scholar]
- 3.Sejersten M., Young D., Clemmensen P. Comparison of the ability of paramedics with that of cardiologists in diagnosing ST-segment elevation acute myocardial infarction in patients with acute chest pain. Am J Cardiol. 2002;90:995–998. doi: 10.1016/s0002-9149(02)02685-1. [DOI] [PubMed] [Google Scholar]
- 4.Rokos I.C., French W.J., Mattu A. Appropriate cardiac cath lab activation: optimizing electrocardiogram interpretation and clinical decision-making for acute ST-elevation myocardial infarction. Am Heart J. 2010;160:995–1003.e8. doi: 10.1016/j.ahj.2010.08.011. [DOI] [PubMed] [Google Scholar]
- 5.Ornato J.P. The ST-segment–elevation myocardial infarction chain of survival. Circulation. 2007;116:6–9. doi: 10.1161/CIRCULATIONAHA.107.710970. [DOI] [PubMed] [Google Scholar]
- 6.Stowens J.C., Sonnad S.S., Rosenbaum R.A. Using EMS dispatch to trigger STEMI alerts decreases door-to-balloon times. West J Emerg Med. 2015;16:472–480. doi: 10.5811/westjem.2015.4.24248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Grosgurina O., Plojouxa J., Kellerb P.F. Prehospital emergency physician activation of interventional cardiology team reduces door-to-balloon time in ST-elevation myocardial infarction. Swiss Med Wkly. 2010;140:228–232. doi: 10.4414/smw.2010.12927. [DOI] [PubMed] [Google Scholar]
- 8.Le May M.R., So D.Y., Dionne R. A citywide protocol for primary PCI in ST-segment elevation myocardial infarction. N Engl J Med. 2008;358:231–240. doi: 10.1056/NEJMoa073102. [DOI] [PubMed] [Google Scholar]
- 9.Swor R., Hegerberg S., McHugh-McNally A., Goldstein M., McEachin C.C. Prehospital 12-lead ECG: efficacy or effectiveness? Prehosp Emerg Care. 2006;10:374–377. doi: 10.1080/10903120600725876. [DOI] [PubMed] [Google Scholar]
- 10.Larson D.M., Menssen K.M., Sharkey S.W. “False-positive” cardiac catheterization laboratory activation among patients with suspected ST-segment elevation myocardial infarction. JAMA. 2007;298:2754–2760. doi: 10.1001/jama.298.23.2754. [DOI] [PubMed] [Google Scholar]
- 11.Lu J., Bagai A., Buller C. Incidence and characteristics of inappropriate and false-positive cardiac catheterization laboratory activations in a regional primary percutaneous coronary intervention program. Am Heart J. 2016;173:126–133. doi: 10.1016/j.ahj.2015.10.027. [DOI] [PubMed] [Google Scholar]
- 12.Chaudhry U., Mavroudis C., Rakhit R.D. Emergency ambulance triggered “false activation” callout for primary percutaneous coronary intervention is not a benign phenomenon. Int J Cardiol. 2013;168:3018–3019. doi: 10.1016/j.ijcard.2013.04.025. [DOI] [PubMed] [Google Scholar]
- 13.Nfor T., Kostopoulos L., Hashim H. Identifying false-positive ST-elevation myocardial infarction in emergency department patients. J Emerg Med. 2012;43:561–567. doi: 10.1016/j.jemermed.2011.09.027. [DOI] [PubMed] [Google Scholar]
- 14.Zhu T., Huitema A., Alemayehu M. Clinical presentation and outcome of patients with ST-segment elevation myocardial infarction without culprit angiographic lesions. Cardiovasc Revasc Med. 2015;16:217–220. doi: 10.1016/j.carrev.2015.04.004. [DOI] [PubMed] [Google Scholar]
- 15.Egan T., Yang B., Barlett R.K. The effects of organizational learning culture and job satisfaction on motivation to transfer learning and turnover intentions. Hum Resour Dev Q. 2004;15:279–301. [Google Scholar]
- 16.Weiss D.J., Dawis R., England G., Lofquist L. Manual for the Minnesota Satisfaction Questionnaire. Man Minnesota Satisf Surv. 1967:125. [Google Scholar]
- 17.Hirschfield R.R., Louisiana S.U. Does revising the intrinsic and extrinsic subscales of the Minnesota Satisfaction Questionnaire short form make a difference? Educ Psychol Meas. 2000;60:255–270. [Google Scholar]
- 18.Ozyurt A., Hayran O., Sur H. Predictors of burnout and job satisfaction among Turkish physicians. QJM. 2006;99:161–169. doi: 10.1093/qjmed/hcl019. [DOI] [PubMed] [Google Scholar]
- 19.Martins H., Proenca T. Minnesota Satisfaction Questionnaire - psychometric properties and validation in a population of Portuguese hospital workers. Econ Manag. 2012;471:1–20. [Google Scholar]
- 20.Cantor W.J., Hoogeveen P., Robert A. Prehospital diagnosis and triage of ST-elevation myocardial infarction by paramedics without advanced care training. Am Heart J. 2012;164:201–206. doi: 10.1016/j.ahj.2012.05.009. [DOI] [PubMed] [Google Scholar]
- 21.Levis J.T., Koskovich M. Ability of first-year paramedic students to identify ST-segment elevation myocardial injury on 12-lead electrocardiogram: a pilot study. Prehosp Disaster Med. 2010;25:527–532. doi: 10.1017/s1049023x00008712. [DOI] [PubMed] [Google Scholar]
- 22.Satterlee W.G., Eggers R.G., Grimes D.A. Effective medical education: insights from the Cochrane Library. Obstet Gynecol Surv. 2008;63:329–333. doi: 10.1097/OGX.0b013e31816ff661. [DOI] [PubMed] [Google Scholar]
- 23.Mencl F., Wilber S., Frey J. Paramedic ability to recognize ST-segment elevation myocardial infarction on prehospital electrocardiograms. Prehosp Emerg Care. 2012;17:203–210. doi: 10.3109/10903127.2012.755585. [DOI] [PubMed] [Google Scholar]
- 24.Pourmand A., Tanski M., Davis S. Educational technology improves ECG interpretation of acute myocardial infarction among medical students and emergency medicine residents. West J Emerg Med. 2015;16:133–137. doi: 10.5811/westjem.2014.12.23706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Porras L., Drezner J., Dotson A. Novice interpretation of screening electrocardiograms and impact of online training. J Electrocardiol. 2016;49:462–466. doi: 10.1016/j.jelectrocard.2016.02.004. [DOI] [PubMed] [Google Scholar]
- 26.Debonis K., Blair T.R., Payne S.T., Wigan K., Kim S. Viability of a web-based module for teaching electrocardiogram reading skills to psychiatry residents: learning outcomes and trainee interest. Acad Psychiatry. 2015;39:645–648. doi: 10.1007/s40596-014-0249-x. [DOI] [PubMed] [Google Scholar]
- 27.Mahler S.A., Wolcott C.J., Swoboda T.K., Wang H., Arnold T.C. Techniques for teaching electrocardiogram interpretation: self-directed learning is less effective than a workshop or lecture. Med Educ. 2011;45:347–353. doi: 10.1111/j.1365-2923.2010.03891.x. [DOI] [PubMed] [Google Scholar]
- 28.Nilsson M., Bolinder G., Held C. Evaluation of a web-based ECG-interpretation programme for undergraduate medical students. BMC Med Educ. 2008;8:25. doi: 10.1186/1472-6920-8-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Youngquist S.T., Shah A.P., Niemann J.T., Kaji A.H., French W.J. A comparison of door-to-balloon times and false-positive activations between emergency department and out-of-hospital activation of the coronary catheterization team. Acad Emerg Med. 2008;15:784–787. doi: 10.1111/j.1553-2712.2008.00186.x. [DOI] [PubMed] [Google Scholar]
- 30.Gilhooly K.J., McGeorge P., Hunter J. Biomedical knowledge in diagnostic thinking: the case of electrocardiogram (ECG) interpretation. Eur J Cogn Psychol. 1997;9:199–223. [Google Scholar]
- 31.Werner K., Kander K., Axelsson C. Electrocardiogram interpretation skills among ambulance nurses. Eur J Cardiovasc Nurs. 2016;15:262–268. doi: 10.1177/1474515114566158. [DOI] [PubMed] [Google Scholar]
- 32.Jafari N., Zareie B. A model for assessing the impact of e-learning systems on employees’ satisfaction. Comput Human Behav. 2015;53:475–485. [Google Scholar]
- 33.Steiner O.L., Segal Z. E-Learning in high education. Int J Learn. 2004;11:45–53. [Google Scholar]
- 34.Lahti M., Hatonen H., Valimaki M. Impact of e-learning on nurses’ and student nurses knowledge, skills, and satisfaction: a systematic review and meta-analysis. Int J Nurs Stud. 2014;51:136–149. doi: 10.1016/j.ijnurstu.2012.12.017. [DOI] [PubMed] [Google Scholar]