

Abstract
Patient-specific 3D modeling is the first step towards image-guided surgery, the actual revolution in surgical care. Pediatric and adolescent patients with rare tumors and malformations should highly benefit from these latest technological innovations, allowing personalized tailored surgery. This study focused on the pelvic region, located at the crossroads of the urinary, digestive, and genital channels with important vascular and nervous structures. The aim of this study was to evaluate the performances of different software tools to obtain patient-specific 3D models, through segmentation of magnetic resonance images (MRI), the reference for pediatric pelvis examination. Twelve software tools freely available on the Internet and two commercial software tools were evaluated using T2-w MRI and diffusion-weighted MRI images. The software tools were rated according to eight criteria, evaluated by three different users: automatization degree, segmentation time, usability, 3D visualization, presence of image registration tools, tractography tools, supported OS, and potential extension (i.e., plugins). A ranking of software tools for 3D modeling of MRI medical images, according to the set of predefined criteria, was given. This ranking allowed us to elaborate guidelines for the choice of software tools for pelvic surgical planning in pediatric patients. The best-ranked software tools were Myrian Studio, ITK-SNAP, and 3D Slicer, the latter being especially appropriate if nerve fibers should be included in the 3D patient model. To conclude, this study proposed a comprehensive review of software tools for 3D modeling of the pelvis according to a set of eight criteria and delivered specific conclusions for pediatric and adolescent patients that can be directly applied to clinical practice.
Keywords: 3D modeling, MRI, Segmentation software, Pelvic surgery
Introduction
Thanks to the advances in medical imaging technologies, especially 3D visualization, the surgeon should better understand the patient’s anatomy, properly counsel the patient, predict possible complications, choose the surgical approach, and use image overlay to guide surgery. However, general surgeons, and even more pediatric surgeons, do not have access in routine to these tools. Imaging the pelvis for a 3D patient-specific model entails important difficulties. First, the involved structures are soft and deformable leading to a strong anatomical inter-patient variability. Secondly, simple automatic tools such as MIP (maximum intensity projection) or direct 3D volume rendering, only based on the intensity of the voxels, are ineffective for the pelvis due to the strong signal heterogeneity, especially in MRI. Hence, dedicated segmentation tools are mandatory to obtain a comprehensive, relevant, and useful 3D pelvic model. We here refer to segmentation of a 3D image as the process of assigning a given label to each voxel of the image, such that voxels with the same label belong to the same anatomical structure.
However, most of the available segmentation and 3D modeling software tools focus on CT images (e.g., segmentation of bones, liver, and vessels) or on brain MRI.
Our research focuses on pelvic malformations and tumors in children and adolescents. This anatomical region is complex to represent in 3D, especially in children presenting rare malformations and tumors and whose anatomy varies with age. Surgical planning of such challenging situations would highly benefit from the 3D segmentation of the structures of interest, providing the surgeon with a patient-specific 3D model or “digital twin” [1–3]. The advantages of the 3D models in daily practice are especially obvious for surgical planning in oncology, allowing the surgeon to better understand the spatial relationships between the tumor and the surrounding structures. For anorectal malformations, the 3D models of nerves and muscles may also be useful to better describe the anomalies of the spinal cord and/or muscles frequently associated with such malformations. This should be useful not only to refine the classification of these malformations, but also to evaluate the impact of the different types of surgical approaches and of potential rehabilitation techniques (neuromodulation, physiotherapy, etc.).
MRI is the gold standard modality for the pelvis in both adults and children and provides also specific imaging sequences for several structures such as, for instance, the nerves. Moreover, MRI does not produce any ionizing radiation, which is important for children that will require iterative imaging, especially those treated for cancer.
In this context, our aim was to evaluate existing segmentation software tools for pelvic MRI segmentation. The evaluation was performed according to our requirements in terms of daily surgical use of 3D modeling of patients with pelvic tumors and malformations, e.g., with a limited number of image processing steps.
We present here the selected software tools and a set of criteria for comparative analysis, and we provide surgeons and researchers with guidelines for choosing the best 3D modeling software according to their needs.
Material and Methods
Software Tools Selected for Evaluation
This review focuses on the most generally used software tools in the medical image community, in particular by radiologists. We only include the software tools equipped with segmentation tools, 3D rendering tools, and that are usable by a non-expert in image processing. All the analyzed software tools are freely available on the Internet, except for two commercial software tools currently used at the Imaging Department of the Pediatric Hospital Necker-Enfants Malades of Paris. All free software tools were tested on a Windows operating system (OS) (CPU at 3.10 GHz, 16-GB RAM, 64-bit OS), except for the OsiriX DICOM Viewer that was tested on a Macintosh OS (CPU at 2.7 GHz, 16-GB RAM, 64-bit OS). The possibility of running the software tools on different operating systems, in particular Linux, was also analyzed.
The selected software tools and the corresponding releases are listed in Table 1. They are described in Appendix.
Table 1.
Selected software tools. Commercial tools are indicated with a “$” in the cost column
| Software | Release | Cost | URL |
|---|---|---|---|
| 3D Slicer | 4.5.0–1 | Free | http://www.slicer.org/ |
| Anatomist | 4.0.0 | Free | http://brainvisa.info/web/anatomist.html |
| AW-Server | 3.2 | $ | http://www3.gehealthcare.com/en/products/categories/advanced_visualization/platforms/aw_server |
| Freesurfer | 5.3.0 | Free | http://surfer.nmr.mgh.harvard.edu/ |
| FSL | 4.0.1 | Free | http://www.fmrib.ox.ac.uk/fsl |
| ImageJ | 1.50b | Free | http://imagej.net/ |
| ITK-SNAP | 3.4.0-beta | Free | http://www.itksnap.org |
| Mango | 4.0.1 | Free | http://ric.uthscsa.edu/mango/ |
| MedInria | 2.2.3 | Free | http://med.inria.fr/ |
| MIPAV | 7.2.0 | Free | http://mipav.cit.nih.gov/ |
| Myrian Studio | 2.2.1 | Free | http://studio.myrian.fr/ |
| Olea Sphere | 3–0 | $ | http://www.olea-medical.com/en/olea-sphere-3-0/ |
| OsiriX | 5.8 | Free | http://www.osirix-viewer.com/ |
| Seg3D | 2.2.1 | Free | http://www.sci.utah.edu/software/seg3d.html |
Description of the Imaging Dataset
The imaging data used in this study were gathered from 81 patients, with a median age of 6 years (3 months 17 years), affected by pelvic-abdominal tumors or malformations. MRI exams were performed on a 3-T MRI, as part of a standard clinical protocol with the addition of two extra sequences: (i) a quasi-isotropic T2-w MRI, acquired in the coronal plane, chosen as reference anatomical sequence for the segmentation procedure, and (ii) a diffusion-weighted (DW) MRI, acquired in the axial plane, necessary to test the tractography algorithms.
All patients under 5 years of age received sedation with phenobarbital. No general anesthesia was required. All patients or patient’s parents gave their informed consent according to ethical board committee requirements (N°IMIS2015-04). An example of some MRI slices used in this study is shown in Fig. 1.
Fig. 1.
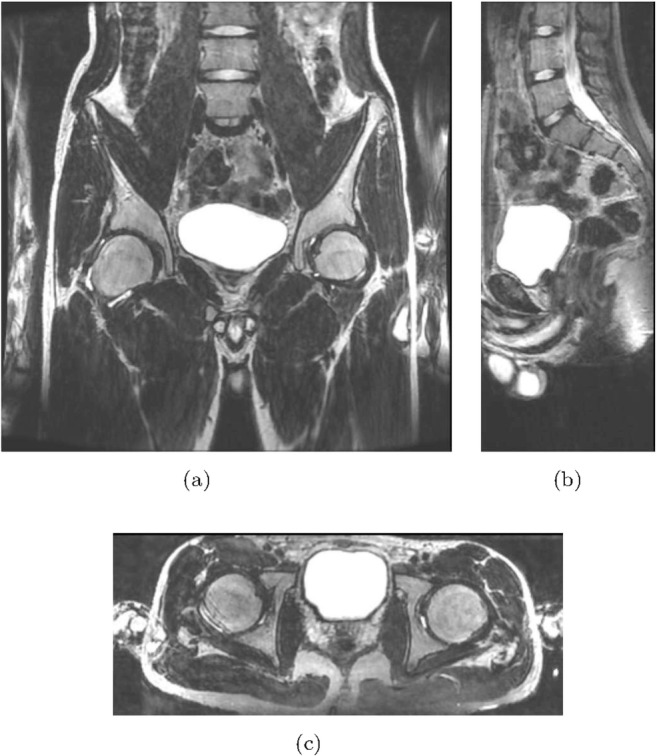
Example of (a) coronal, (b) sagittal, and (c) axial slices of one of the 3D T2-w MRI used in this study
Software tools were evaluated on imaging data issued from the complete patient’s cohort except for the segmentation time criterion, which is highly dependent on the patient’s age and pathology. We have thus chosen two adolescent patients with a normal pelvis anatomy, one female and one male of the same age (to take into account gender variation) to evaluate this criterion. Segmentation was performed with all the software tools for these two referent patients. Finally, in order not to bias the segmentation time results, T2-w images having both the same acquisition parameters were chosen for these two patients: echo time TE = 59 ms, repetition time TR = 5716 ms, flip angle FA = 90°, image size 512 × 512 × 208 voxels, and voxel size = 0.74 × 0.74 × 0.70 mm3.
DW MRI scans were acquired immediately after the T2-w acquisitions, in order to minimize the potential patient’s displacement between the two scans. The DW MRI was acquired using a sequence of 25 directions, a b value of 1000, and a voxel size of 1.4 × 1.4 × 4mm3.
Evaluation Criteria
In order to evaluate the performances of the software tools on the segmentation of the pelvic structures in MRI, we established a list of eight criteria: automatization degree, usability, 3D visualization, segmentation time, image registration functionalities, tractography functionalities, supported system, and potential addition of plugins.
These criteria were selected during a multi-disciplinary expert consensus meeting including anatomists, surgeons, radiologists, and specialists in image analysis (from a computer science point of view), which was also partially inspired by other software comparisons [1, 4–6].
These criteria are defined in this section.
Automatization Degree
This criterion was analyzed according to a score defined by the amount of manual interaction required by the user. Score 1 was assigned to a totally manual segmentation of the regions of interest, performed slice by slice; score 2 to the presence of generic semi-automatic tools for the segmentation of the 2D slices; score 3 to the presence of generic semi-automatic tools for the segmentation of a 3D region; and score 4 to the presence of semi-automatic tools optimized for a specific anatomical structure. Note that thresholding-based segmentation tools were present in all the analyzed software tools. In this study, we did not consider them as segmentation tools due to the fact that they do not provide suitable results for any structure of interest in the pelvis, especially in MRI, where no equivalent of the CT Hounsfield units exists.
Segmentation Time
For each analyzed software, the time required for the segmentation of the pelvic structures of interest in T2-w MRI, of the two test patients (one male and one female), was evaluated. The two images had the same features in terms of contrast, size, and resolution, and the patients had the same age and the same anatomical complexity (see “Description of the Imaging Dataset” for further details). Consequently, we can assume that the only factor that could generate a relevant difference on the total segmentation time is given by the different anatomy of the genital system. For this reason, the total segmentation time was evaluated for the male patient (bones, bladder, vessels, rectum, prostate, seminal vesicles).
For the female patient, only the uterus was segmented and the segmentation time was compared to the one needed for the segmentation of the genital system of the male patient (prostate and seminal vesicles). The segmentations were carried out using either manual or semi-automatic tools depending on the availability in the software tools. In both cases, the aim was to obtain a satisfying segmentation result. For this reason, in case the segmentation was obtained through semi-automatic tools, the segmentation time also includes the time needed for potential manual corrections of the segmentation.
In order to obtain a comparable segmentation among the different software tools, our aim was to obtain results as close as possible to a reference manual segmentation performed by an expert user. The similarity between the different segmentations was evaluated through the DICE index [7] and the value 0.9 was set as lower limit for our application (a DICE index equal to 1 means exact correspondence between the segmentations).
Usability
In order to evaluate the usability of the different platforms, we focused on the ease of use of the GUIs (graphical user interfaces). This includes the general functionalities of the GUI, the ease of use of the manual and semi-automatic segmentation tools, the easiness of the management of the input and output patient’s data, and the header access. Three different users (two surgeons and a researcher in image processing) performed this evaluation independently by assigning a score from 1 to 4 (the higher the score, the higher the user’s satisfaction). For each software, a single final score, which expresses a consensus among the three users, was retained.
3D Visualization
The aspects that mostly interest us were the generation of the 3D models starting from the segmented images, the easy navigation within the 3D model, and the availability of tools for the improvement of the quality of the visual representation (e.g., smoothing, lighting, colors, and transparency management). The same users, similarly to usability, qualitatively and independently evaluated 3D visualization by assigning a score from 1 to 4 (the higher the score, the higher the user’s satisfaction). For each software, a single final score, which expresses a consensus among the three users, was retained.
Image Registration
Image registration is defined as the process of aligning two images. In other words, image registration aims to ensure that, for a given spatial coordinate, the voxels of the two images correspond to the same anatomical location. For each software, the availability of automated registration tools was evaluated, assigning a binary positive or negative score. The details of registration tools (e.g., rigid, affine, thin-plate) were not listed, being out of the scope of this review.
Tractography
Tractography refers to the extraction of fiber bundles from the imaging data collected by diffusion MRI, allowing for 3D modeling and visualization of nerve fibers [8]. Availability of tractography tools was noted for each software, by a binary positive or negative score.
Operating Systems
Considering that different operating systems (OS) are used in the medical imaging community, the corresponding supported OS was reported for each software and the possibility of running the software tools with different OS was considered.
Potential Extensions
The ability of the software tools to be freely extended by add-ons or plugins was considered as important criteria. This possibility, through the work of independent developers, really enlarges the potential performances of the software tools. New tools dedicated to specific segmentation problems (e.g., tools for the segmentation of a specific structure on a specific MRI sequence) can then be developed and integrated in the basic version of the software. For each software, we report whether they are open-source or not, the different programming languages to use to eventually develop the extensions, and the availability of documentation (such as wiki pages or tutorials) and forums or mailing lists focused on the development issues.
Results
The performances of 14 segmentation software tools (12 free software tools and 2 commercial software tools) described in Appendix were analyzed. The results given by the analysis of the software performances, according to the criteria described in the previous section, are summarized in Table 2 (7 first criteria), Table 3 (comparison of the segmentation time for the different structures between male and female patients), and Table 4 (last criterion on plugins).
Table 2.
Software comparison
| Software | Automatization | Usability | 3D visualization | Segmentation time | Registration | Tractography | OS | ||
|---|---|---|---|---|---|---|---|---|---|
| Windows | Linux | Macintosh | |||||||
| 3D Slicer | 3 | 3 | 4 | 15th | x | x | x | x | x |
| Anatomist | 1 | 1 | 1 | > 25 h | x | x | x | ||
| AW Server | 3 | 3 | 3 | > 20 h | x | x | x | x | |
| Freesurfer | 2 | 2 | 1 | > 20 h | x | x | x | x | |
| FSL | 1 | 1 | 2 | > 25 h | x | x | x | x | |
| ImageJ | 2 | 2 | 1 | > 25 h | x | x | x | x | |
| ITK-SNAP | 3 | 4 | 4 | 10 h | x | x | x | ||
| Mango | 1 | 3 | 2 | > 20 h | x | x | x | x | |
| MedInria | 3 | 3 | 3 | > 20 h | x | x | x | x | x |
| MIPAV | 3 | 2 | 2 | > 20 h | x | x | x | x | x |
| Myrian Studio | 3 | 3 | 4 | 9 h | x | x | |||
| Olea Sphere | 3 | 33 | 4 | > 20 h | x | x | x | x | x |
| OsiriX | 3 | 3 | 4 | > 20 h | x | x | |||
| Seg3D | 2 | 4 | 3 | 20 h | x | x | x | ||
Table 3.
Segmentation time for the genital system
| Software | Segmentation time [min] | |
|---|---|---|
| Male | Female | |
| 3D Slicer | 7 | 19 |
| Anatomist | 13 | 28 |
| AW-Server | 8 | 20 |
| Freesurfer | 11 | 28 |
| FSL | 12 | 26 |
| ImageJ | 10 | 25 |
| ITK-SNAP | 6 | 18 |
| Mango | 9 | 20 |
| MedInria | 10 | 20 |
| MIPAV | 11 | 26 |
| Myrian Studio | 4 | 11 |
| Olea Sphere | 9 | 21 |
| OsiriX | 8 | 18 |
| Seg3D | 8 | 19 |
Table 4.
Development features
| Software | Extensible | Open-source | Documentation | Forum | Programming language |
|---|---|---|---|---|---|
| 3D Slicer | x | x | x | X | C++, Python, Matlab |
| Anatomist | x | x | x | X | C++, Python |
| AW-Server | – | – | – | – | |
| Freesurfer | x | x | x | X | C++ |
| FSL | x | x | x | X | C++ |
| ImageJ | x | x | x | X | Java, JavaScript, Python, Matlab, Ruby, Groovy, Lisp, R |
| ITK-SNAP | x | x | X | C++ | |
| Mango | x | x | X | Java, Python | |
| MedInria | x | x | x | X | C++ |
| MIPAV | x | x | x | X | Java |
| Myrian Studio | x | x | X | C++, Matlab | |
| Olea Sphere | – | – | – | – | |
| OsiriX | x | x | x | X | Objective C |
| Seg3D | x | x | x | X | C++, Python, Matlab |
Automatization Degree
In all the analyzed software tools, except for Anatomist, FSL, and Mango, different generic semi-automatic segmentation tools were present. In particular, the highest automatization degree score was assigned to 3D Slicer, AW-Server, ITK-SNAP, MedInria, Mipav, Myrian Studio, Olea Sphere, and OsiriX. This means that all these software tools include at least one semi-automatic tool for the segmentation of a 3D region, 3D Slicer being the one that offers the largest number of segmentation tools (both 2D and 3D). As shown in Table 2, none of the software tools includes organ-specific tools dedicated to the segmentation of the pelvic structures of interest in MRI. However, it is important to note that some of the software tools (e.g., 3D Slicer, Myrian Studio, Freesurfer, FSL) have organ-specific segmentation tools for other anatomical structures (e.g., brain, liver, lungs) or for other imaging modalities (e.g., CT, microscopy).
Usability
Our analysis ranks ITK-SNAP and Seg3D as the best tools in terms of usability. These software tools present a clear and intuitive GUI and the number of user interactions (clicks or selection) generally needed to perform a given operation is really limited. In particular, they easily allow the user to import the patient data, to access its information, to perform the segmentation tasks, and to finally save the processing results. The two software tools that obtained the lower score were Anatomist and FSL. The main reason is that they are mostly dedicated to users with a certain image processing background, and they actually do not focus on generic segmentation tasks. It is important to note that the usability scores express a consensus among the different evaluators, which was easily reached during the evaluation.
3D Visualization
The software tools that obtained the best score were 3D Slicer, ITK-SNAP, Myrian Studio, Olea Sphere, and OsiriX. These software tools allow the user to obtain, once the segmentation task is performed, the 3D models of the segmented regions and to easily navigate in the 3D views. Moreover, these software tools offer several tools for the management of the 3D surfaces such as opacity and lighting that clearly improve the visual quality of the visualization of the 3D models. On the other side, the lowest score was assigned to Anatomist, Freesurfer, and ImageJ, mostly due to the not intuitive steps needed to obtain the 3D models from the segmented images. It is important to note that the 3D Visualization scores express a consensus among the different evaluators, which was easily reached during the evaluation.
Segmentation Time
As shown in Table 2, the time required for the segmentation of the structures of interest of our male test patient (bones, colon, bladder, main vessels, prostate) is always at least 9 h. In particular, Myrian Studio is the software that gave the best segmentation time. The complete reconstructions of all the structures of interest were performed using only four of the analyzed software tools (3D Slicer, ITK-SNAP, Myrian Studio, Seg3D) and, consequently, the exact segmentation time is reported only for them. Using the other software tools, due to the long time needed for the segmentation, only a few structures have been segmented. In these cases, the time for the complete segmentation is estimated (in Table 2 the lower bound is reported) by considering both the time needed to fully segment the first structures and the time needed to partially segment the other structures. As shown in Table 3, the segmentation time needed for the segmentation of the female genital system was, for all the software analyzed, higher than for the male one.
It is important to remark that, due to the long time needed for the segmentation procedure, no inter- nor intra-rater variability was assessed for the segmentation time, which is a limit of this evaluation.
Registration Tools
All the software tools, except Anatomist, Seg3D, and ITK-SNAP, include image registration tools. In particular, 3D Slicer is the one that offers the largest number of different image registration tools.
Tractography Tools
Tractography algorithms that allow to track the nerve fibers from the diffusion MRI are present in 3D Slicer, AW-Server, Freesurfer, FSL, MedInria, MIPAV, and Olea Sphere. In Fig. 2, the full pelvic 3D reconstructions obtained using 3D Slicer, ITK-SNAP, and Myrian Studio are shown. Additionally, the nervous pelvic network was added on the 3D Slicer segmentation view since it could be obtained using this software.
Fig. 2.

Example of 3D pelvic reconstructions obtained through segmentation of the T2-w MRI volume, using (a) 3D Slicer, (b) ITK-SNAP, and (c) Myrian Studio
Potential Extensions
As reported in Table 4, all the software tools, except the two commercial software AW-Server and Olea Sphere, can be freely extended by independent developers, in order to improve the performances of the basic versions of the software. Specific documentation and forums in most of the cases support the development of extensions, and different programming languages can be used.
Discussion
In the previous section, we highlighted the differences in performances of different software tools, according to a set of criteria defined for our specific needs in 3D modeling of pelvic tumors and malformations in children and adolescents, from MRI acquisitions. In the literature, few papers reviewed the various software tools able to read DICOM images with the aim of integrating clinical research and medical imaging [4–6]. In these studies, the authors distinguish open-source, free, and commercial tools, and analyze them according to several general criteria such as usability, interface, data management, and 2D and 3D viewing tools. Particularly, Presti et al. [1] focused on the issues of image-guided surgery, by reviewing different software tools taking also into account the possibility of their integration in a portability workflow until the operating room. However, none of the previous studies considered the segmentation performances of the different software tools.
Software Comparison
The time required for the segmentation is surely the most important factor to consider in our evaluation, even if it is obviously related to the automatization degree of the software. In some cases, the semi-automatic segmentation tools did not allow obtaining suitable results for all the structures of interest, and time-consuming manual corrections had to be done. For example, using AW-Server, MedInria, MIPAV, OsiriX, and Olea Sphere, the 3D semi-automatic tools had suitable performances only on the bladder segmentation and the rest of the organs were manually segmented. Although none of the analyzed software tools respected the segmentation time limits imposed by the clinical practice, the fastest segmentation results were obtained using Myrian Studio and ITK-SNAP. In particular, Myrian Studio offers a powerful tool to interpolate several manual segmentations on the 2D slices to obtain a 3D segmentation, strongly reducing the segmentation time of all the structures of interest. The segmentation time with ITK-SNAP was also shorter than for the other software tools and benefits from a powerful and interactive 3D segmentation tool based on deformable models implemented in level-set algorithms. Even if this tool was not suitable for all the structures of interest, it allowed shortening the segmentation time for the bones and the bladder.
As mentioned in “Description of the Imaging Dataset,” two 16-year-old patients with a normal anatomy of the structures of interest were chosen for the evaluation of the segmentation time criterion, in order not to bias the software performance analysis with complex image interpretation issues. In this way, the segmentation time is really the one needed to use the analyzed software tools. Surely, strong malformations raise more difficulties on the segmentation task, and the segmentation time would potentially increase compared to our case. Moreover, in case the user wants also to segment a potential tumor, this additional time has to be taken into account. The amount of the additional segmentation time depends on different factors that cannot be easily quantified, such as the anatomical experience of the user, the type of the malformation, or the tumor anatomy. Another factor that could impact the segmentation time is the age of the patient. On the one side, considering younger patients will potentially lead to an additional time in the image understanding task, due to a more complex anatomy. On the other side, with the same acquisition protocol, younger patients also mean less slices and smaller structures to segment.
Thanks to clear interfaces and intuitive segmentation tools, both ITK-SNAP and Seg3D appear very usable. The easy use is especially guaranteed by the fact that these software tools have a limited number of functionalities and that they are strictly dedicated to segmentation problems. Software tools such as 3D Slicer, AW-Server, Olea Sphere, and Myrian Studio are also very usable but slightly less than the formers, due to a larger number of screen configurations and tools offered for various tasks (e.g., segmentation, filtering, analysis, registration, and tractography tools). As our team did not have previous experience of any of the software tools analyzed, the influence of the learning curve was not considered. However, we can expect that all computation times would be reduced after user’s training.
Regarding the segmentation process, the main difficulties were strongly related to each anatomical structure (see Fig. 3):
The structure that raises the biggest segmentation difficulties was the colon, due to its complex 3D shape and the strong inhomogeneities induced by the presence of both air and matter. Moreover, on T2-w images, there were often unclear boundaries between the colon and the surrounding perirectal fat (Fig. 3a). Hence, its segmentation was guided by a prior anatomical knowledge in addition to the image information.
The bones, even if not totally homogeneous, are better suited to be segmented with semi-automatic tools than the colon. Anyway, due to the large volume that they occupy on the image and the not totally suitable results given by the semi-automatic tools (manual corrections are needed), the bone structure is the one that requires the longest segmentation time (Fig. 3b).
The bladder, appearing on the T2-w images as a homogeneous hyperintense region, is the easiest organ to segment and the available semi-automatic tools allow us to generally perform a fast and accurate segmentation. However, the automatic segmentation tools do not allow taking into account both the bladder repletion (strongly hyperintense) and the bladder wall that eventually have to be segmented (Fig. 3c).
The main pelvic vessels (aortal and vena cava bifurcation, iliac veins, and arteries) are not difficult to visually identify but the available semi-automatic algorithms do not allow us to obtain suitable results. The main problems are related to the low contrast between the vessels and the surrounding tissues, and to the unclear boundaries between the veins and the arteries in the regions in which they are partially in contact (Fig. 3d).
The segmentation of the prostate and the uterus is difficult due to a poor contrast and not well-defined boundaries with the surrounding tissues (Fig. 3e, f). The segmentation time for the uterus is higher than for the prostate due to its more complex shape and its bigger volume (67.5 cm3 for the uterus, against 15.7 cm3 for the prostate1). However, both structures are relatively quickly segmented in comparison to the others due to their limited size.
Fig. 3.

Example of organ segmentations in a few MRI coronal slices. From top to bottom: (a) rectum, (b) bones, (c) bladder, (d) veins (blue) and arteries (red), (e) prostate, and (f) uterus
The problems encountered and the long time required to build the 3D models are thus related to the lack of organ-specific segmentation tools for the structures of interest in any of the software tools tested. For this reason, the extension criterion is crucial in the evaluation of the software potential. The plugins do not only improve the segmentation performances but can also be very useful in research works to test and evaluate innovative methods and algorithms. Even if most of the software tools can be extended by add-ons or plugins, as shown in Table 4, the ones that appear easier to extend, thanks to their modularity, their extensive documentation, tutorials, and support provided for the developers, are 3D Slicer, ImageJ, MIPAV, and Myrian Studio. As an example, we developed a plugin for the bone segmentation in MRI, specific for the pediatric patients, that allowed us to drastically reduce the time for bone segmentation from several hours to 10 min on average in 3D Slicer [9].
Guidelines for the Choice of the Best Software Tools for Pelvic Surgical Planning
Based on the results presented in “Results,” we can sum up some guidelines for the choice of a software for the pelvic surgical planning depending on the final result the user wants to achieve. If the aim of the user is to obtain the reconstruction of the organs of interest (bones, bladder, colon, vessels, genital system) by segmenting (manually/semi-automatically) the image volumes of the patient, the best-ranked tools, according to our criteria, are ITK-SNAP and Myrian Studio. These two software tools are the fastest in terms of segmentation time, are really usable, and offer a good 3D visualization of the segmentation results. Among these two software tools, the advantage of ITK-SNAP is the easier management of the output segmentation models that can be easily exported in standard formats (e.g., .vtk, .stl) and eventually imported in other software environments. Moreover, ITK-SNAP is multi-platform, while Myrian Studio runs only on Windows OS. However, neither ITK-SNAP nor Myrian Studio offers tractography tools for the 3D reconstruction of the nerve fibers that could be really useful to integrate in the patient-specific 3D model.
A possible solution, in order to obtain a complete patient model, could be to generate the segmentation models of the structures of interest within a software (e.g., ITK-SNAP), export the results, and subsequently import them in a software that offers tractography tools. However, this procedure requires several steps and it would be clearly better for the user to have all the needed tools in the same software platform.
Therefore, if the user also wants to consider the nerve fibers in the final 3D reconstruction, 3D Slicer is the software that best fits the requirements. In fact, even if using 3D Slicer, the segmentation time is higher than with ITK-SNAP or Myrian Studio, and the GUI slightly less easy to use than the one of ITK-SNAP, 3D Slicer has good 3D visualization features and has the strong advantage of offering tractography tools. Note that recent versions of 3D Slicer include a better GUI with useful interpolation and visualization tools. Moreover, in case of users willing to extend the software capabilities, since 3D Slicer can be easily extended with plugins, the segmentation time could be strongly reduced by implementing organ-specific segmentation methods.
3D Modeling of the Pelvis for Tumors and Malformation—Some Clinical Applications
Figures 4 and 5 give two examples of the potential benefit offered by 3D segmentation and tractography in the two major fields of pediatric surgery: tumors and malformations. Figure 4 represents a rhabdomyosarcoma of the obturator muscle after neoadjuvant chemotherapy. In that case, 3D modeling was crucial for surgical planning: it allowed proposing a procedure more conservative for the cotyleum without compromising the completeness of resection, which was R0. Figure 5 shows the 3D modeling of a non-repaired cloacal malformation, a partial sacral agenesia, and no dysraphism. The 3D modeling of the pelvic nervous network is currently unknown in this complex malformation and could be explored in other anorectal malformation: it should help not only to refine the classification of these malformations but also to evaluate the impact of the different types of surgical approaches and of potential rehabilitation techniques (e.g., neuromodulation, physiotherapy).
Fig. 4.

3D modeling of a 7-year-old patient with a rhabdomyosarcoma of the right obturator muscle
Fig. 5.

3D modeling of a 9-year-old patient with a non-repaired cloacal malformation (with a colostomy), a sacral agenesia, and no dysraphism. a Coronal view integrating the sacral tractogram. Note the asymmetry of levator ani muscles. b Left sagittal view. Note the compression by the hydrocolpos on the left ureter. c Coronal posterior view, showing the muscular system and the common channel in PSARP position
Conclusion
The availability of a 3D patient-specific model for surgical planning is currently a major goal for surgeons, whatever the specialty. A huge effort has been made, these last years, on the visualization of the 3D models [10, 11] (software applications, 3D printing, augmented reality glasses, etc.) but the achievement of the previous mandatory step, which is the building of the model, is not routinely available for pelvis anatomy. This is however an anatomical region that is highly complex, at the crossroad between digestive, genital, and urological tracts, where any lesion of vascular and/or nervous structure may have a major impact on the quality of life, especially in children.
In this paper, we reviewed 14 3D modeling software tools and we provided guidelines for the choice of the most suitable software tools for surgeons that would like to introduce a 3D patient-specific pelvic model, obtained from MRI, in their surgical planning routine. Moreover, we presented some clinical application showing the benefits of 3D modeling for surgery planning of pediatric pelvic pathologies. The methodology adopted here could also be useful to explore other anatomical regions in pediatric and adult patients with the same goal.
Appendix
A Software Tool Description
In this appendix, a short description of all the software tools of Table 1 is provided.
3D Slicer
3D Slicer [12] is a free, multi-platform, and open-source software for image analysis and visualization written in C++, Python, and Qt. The origin of this software was a project between different laboratories of the Brigham and Women’s Hospital and the MIT in 1998. In the following years, several improvements of the software capabilities were achieved through the support of the National Institute of Health (NIH). The main interface of 3D Slicer appears as a typical radiology workstation, allowing for a large number of different visualization configurations to analyze 2D, 3D, and 4D images. The platform also offers a large set of processing tools for different imaging modalities and applications (including segmentation, registration, and quantification).
Anatomist
Anatomist [13] is the visualization software generally associated with the software platform BrainVISA [14]. BrainVISA is an open-source software written in Python, offering different tools dedicated to the neuroimaging research and mainly developed by the French Alternative Energies and Atomic Energy Commission (CEA). Although BrainVISA is devoted to brain MRI, Anatomist can be used to visualize and segment other types of image volumes.
AW-Server
AW-Server is the commercial visualization software developed by GE Healthcare. The workstation, more than just allowing for the visualization and annotation of the images, offers a large number of advanced post-processing applications for different imaging modalities and clinical applications.
Freesurfer
Freesurfer [15] is an open-source software platform, written in C++, developed by the Martinos Center for Biomedical Imaging of Boston. The software is particularly devoted to the analysis and visualization of structural and functional neuroimaging data, offering several tools for the automated segmentation of anatomical MR images and the analysis of diffusion MR data. Despite the strong focus on brain MRI, Freesurfer can be used to visualize and analyze through generic tools various types of multi-dimensional medical images.
FSL
FSL (the FMRIB Software Library) [16] is an open-source software library, written in C++, mainly developed by the FMRIB Analysis Group of the University of Oxford. The software is strongly devoted to the analysis of functional, structural, and diffusion MRI brain imaging data. Similarly to Freesurfer, although FSL is strongly devoted to the brain MRI data, it offers a generic viewer (FSLView) that allows visualizing and manually segmenting 3D images.
ImageJ
ImageJ [17] is a Java-based, open-source platform for image processing, developed by the NIH and constantly updated since 1997. Thanks to the collaborative efforts of its developer community, ImageJ offers several functionalities for performing a wide variety of image processing tasks. However, even if ImageJ supports multi-dimensional data, it appears more focused on the processing of 2D images.
ITK-SNAP
ITK-SNAP [18] is an open-source software application based on ITK2 and VTK3 C++ libraries. It was developed by the University of Pennsylvania and the University of Utah, first released in 2004 but under a constant updating process. The platform allows for navigation within the images similar to a radiology workstation, and it was specifically developed for segmentation tasks, not focusing on other kinds of processing (e.g., filtering, registration).
Mango
Mango (Multi-image Analysis GUI) is a free Java-based viewer for medical images developed by the Research Imaging Institute of the University of Texas Health Science Center at San Antonio. The software includes a GUI for the visualization of 3D images as well as functionalities for different tasks such as registration, filtering, and segmentation. It can be extended through dedicated plugins.
MedInria
MedInria [19] is an open-source platform for medical image processing developed by Inria, the French National Institute for computer science and applied mathematics. This platform manages the visualization of multi-dimensional data, and it includes processing and analysis of diffusion MR images (e.g., to provide tractography). MedInria also offers basic segmentation, registration, and filtering tools based on the ITK library.
MIPAV
MIPAV [20], acronym for Medical Image Processing Analysis and Visualization, is a Java-based open-source software supported by the NIH. It manages multi-modal and 3D images, even if its main interface appears better suited for the processing and visualization of 2D images. MIPAV offers several functionalities for different tasks such as filtering, registration, and segmentation on both 2D and 3D images.
Myrian®
Myrian® is a commercial software for medical image processing and visualization developed by Intrasense. It supports multi-modal images and offers different functionalities for tasks such as segmentation, quantification, and registration. A non-commercial version, Myrian® Studio, is freely available for research purposes and can be extended through dedicated plugins.
Olea Sphere®
Olea Sphere® is a commercial processing platform for CT and MRI, developed by the company Olea Medical. The workstation includes a generic DICOM viewer and offers different packages developed for specific medical applications (e.g., breast, head and neck, prostate).
OsiriX
OsiriX [21] is one of the most widely used DICOM viewers in the medical community. The OsiriX project started in 2003 at UCLA, Los Angeles, and in 2010, the first commercial version of the software (OsiriX MD) was released. OsiriX Lite is the free version of the commercial software OsiriX MD, intended for research purposes and offering reduced computational performances, but it still includes the functionalities needed in our application domain. The platform appears as a typical radiology workstation, supporting multi-modal images and strongly devoted to the visualization tasks, even if it includes also post-processing tools such as registration and segmentation.
Seg3D
Seg3D [22] is an open-source software platform for image visualization and segmentation of 3D images developed by the NIH Center for Integrative Biomedical Computing at the University of Utah. The platform focuses on segmentation tasks, even if some other functionalities such as filtering using several methods from the ITK library are present.
Compliance with Ethical Standards
All patients or patient’s parents gave their informed consent according to ethical board committee requirements (N°IMIS2015-04).
Footnotes
Values estimated from the manual segmentations.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Lo Presti G, Carbone M, Ciriaci D, Aramini D, Ferrari M, Ferrari V. Assessment of DICOM viewers capable of loading patient-specific 3D models obtained by different segmentation platforms in the operating room. J Digit Imaging. 2015;28(5):518–527. doi: 10.1007/s10278-015-9786-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ferrari V, Carbone M, Cappelli C, Boni L, Melfi F, Ferrari M, Mosca F, Pietrabissa A. Value of multidetector computed tomography image segmentation for preoperative planning in general surgery. Surg Endosc. 2012;26(3):616–626. doi: 10.1007/s00464-011-1920-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Azagury DE, Dua MM, Barrese JC, Henderson JM, Buchs NC, Ris F, Cloyd JM, Martinie JB, Razzaque S, Nicolau S, Soler L, Marescaux J, Visser BC. Image-guided surgery. Curr Probl Surg. 2015;52(12):476–520. doi: 10.1067/j.cpsurg.2015.10.001. [DOI] [PubMed] [Google Scholar]
- 4.Haak D, Page C-E, Deserno TM. A survey of DICOM viewer software to integrate clinical research and medical imaging. J Digit Imaging. 2016;29(2):206–215. doi: 10.1007/s10278-015-9833-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Valeri G, Mazza FA, Maggi S, Aramini D, La Riccia L, Mazzoni G, Giovagnoni A. Open source software in a practical approach for post processing of radiologic images. Radiol Med. 2015;120(3):309–323. doi: 10.1007/s11547-014-0437-5. [DOI] [PubMed] [Google Scholar]
- 6.Liao W, Deserno TM, Spitzer K. Evaluation of free non-diagnostic DICOM software tools. Proc SPIE. 2008;6919:691903. doi: 10.1117/12.770431. [DOI] [Google Scholar]
- 7.Dice LR. Measures of the amount of ecologic association between species. Ecology. 1945;26(3):297–302. doi: 10.2307/1932409. [DOI] [Google Scholar]
- 8.Mukherjee P, Berman JI, Chung SW, Hess CP, Henry RG. Diffusion tensor MR imaging and fiber tractography: Theoretic underpinnings. Am J Neuroradiol. 2008;29(4):632–641. doi: 10.3174/ajnr.A1051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Virzì A, Marret J-B, Muller CO, Berteloot L, Boddaert N, Sarnacki S, Bloch I (2017) A new method based on template registration and deformable models for pelvic bones semi-automatic segmentation in pediatric MRI. In 2017 IEEE 14th International Symposium on Biomedical Imaging (ISBI 2017), pp. 323–326. IEEE
- 10.Barfield W: Fundamentals of wearable computers and augmented reality. CRC Press, 2015
- 11.Rengier F, Mehndiratta A, von Tengg-Kobligk H, Zechmann CM, Unterhinninghofen R, Kauczor H-U, Giesel FL. 3D printing based on imaging data: review of medical applications. Int J Comput Assist Radiol Surg. 2010;5(4):335–341. doi: 10.1007/s11548-010-0476-x. [DOI] [PubMed] [Google Scholar]
- 12.Fedorov A, Beichel R, Kalpathy-Cramer J, Finet J, Fillion-Robin J-C, Pujol S, Bauer C, Jennings D, Fennessy F, Sonka M, et al. 3D Slicer as an image computing platform for the quantitative imaging network. Magn Reson Imaging. 2012;30(9):1323–1341. doi: 10.1016/j.mri.2012.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rivière D, Geffroy D, Denghien I, Souedet N, Cointepas Y. Python in neuroscience workshop. 2011. Anatomist: A python framework for interactive 3D visualization of neuroimaging data. [Google Scholar]
- 14.Geffroy D, Rivière D, Denghien I, Souedet N, Laguitton S, Cointepas Y. Python in neuroscience workshop. Paris: Euroscipy; 2011. Brainvisa: A complete software platform for neuroimaging. [Google Scholar]
- 15.Fischl B. FreeSurfer. NeuroImage. 2012;62(2):774–781. doi: 10.1016/j.neuroimage.2012.01.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Jenkinson M, Beckmann CF, Behrens TEJ, Woolrich MW, Smith SM. FSL. NeuroImage. 2012;62(2):782–790. doi: 10.1016/j.neuroimage.2011.09.015. [DOI] [PubMed] [Google Scholar]
- 17.Schneider CA, Rasband WS, Eliceiri KW. NIH image to ImageJ: 25 years of image analysis. Nat Methods. 2012;9(7):671–675. doi: 10.1038/nmeth.2089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Yushkevich PA, Piven J, Hazlett HC, Smith RG, Ho S, Gee JC, Gerig G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. NeuroImage. 2006;31(3):1116–1128. doi: 10.1016/j.neuroimage.2006.01.015. [DOI] [PubMed] [Google Scholar]
- 19.Toussaint N, Souplet J-C, Fillard P, et al. MICCAI, volume 7, page 280. 2007. MedINRIA: Medical image navigation and research tool by INRIA. [Google Scholar]
- 20.McAuliffe MJ, Lalonde FM, McGarry D, Gandler W, Csaky K, Trus BL. 14th IEEE Symposium on Computer-Based Medical Systems (CBMS) 2001. Medical image processing, analysis and visualization in clinical research; pp. 381–386. [Google Scholar]
- 21.Rosset A, Spadola L, Ratib O. OsiriX: an open-source software for navigating in multidimensional DICOM images. J Digit Imaging. 2004;17(3):205{216. doi: 10.1007/s10278-004-1014-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.CIBC: Seg3D: Volumetric image segmentation and visualization. Scientific Computing and Imaging Institute (SCI), 2016, Downloaded from: http://www.seg3d.org