

Abstract
Background.
Pancreatic cancer is a disease of older adults, who may present with limited physiologic reserve. The authors hypothesized that a frailty index can predict postoperative outcomes after pancreaticoduodenectomy (PD).
Methods.
All patients who underwent PD were identified in the 2005–2012 NSQIP Participant Use File. Patients undergoing emergency procedures, those with an American Society of Anesthesiologists (ASA) classification of five, and those with a diagnosis of preoperative sepsis were excluded from the study. A modified frailty index (mFI) was defined by 11 variables within the National Surgical Quality Improvement Program (NSQIP) previously used for the Canadian Study of Health and Aging-Frailty Index. An mFI score of 0.27 or higher was defined as a high mFI. Uni- and multivariate analyses were performed to evaluate postoperative outcomes.
Results.
This study enrolled 9986 patients (age 65 ± 12 years, 48.8% female) who underwent PD. Of these patients, 6.4% (n = 637) had a high mFI (>0.27). Increasing mFI was associated with higher prevalence of postoperative morbidity (p < 0.001) and 30-days mortality (p < 0.001). In the univariate analysis, high mFI was associated with increased morbidity (odds ratio [OR] 1.68; 95% confidence interval [CI] 1.43–1.97; p < 0.001) and 30-days mortality (OR 2.45; 95% CI 1.74–3.45; p < 0.001). After adjustment for age, sex, ASA classification, albumin level, and body mass index (BMI), high mFI remained an independent preoperative predictor of postoperative morbidity (OR 1.544; 95% CI 1.289–1.850; p < 0.0001) and 30-days mortality (OR 1.536; 95% CI 1.049–2.248; p = 0.027).
Conclusions.
High mFI is associated with postoperative morbidity and mortality after PD and can aid in preoperative risk stratification.
Pancreatic cancer is an aggressive malignancy that disproportionately affects older adults, with 70% of new cases diagnosed for individuals older than 65 years.1 Surgical resection currently is the only potentially curative treatment option, providing a 5-year survival rate ranging from 15 to 25%.2–4 However, pancreaticoduodenectomy (PD) is associated with high complication rates, including a 30-days morbidity rate of 40–50%5–7 and a mortality rate of 1–3%.7–9
Outcomes after PD estimated by risk prediction tools rely on patient- and tumor-related factors, some of which cannot be assessed preoperatively.10 Although recent studies have devised models based on parameters measured preoperatively, they require high-quality imaging and interpretation and have not been validated with large samples of patients in the general population.11–13 Other predictive tools such as the Physiological and Operative Scoring System for enUmeration of Morbidity and mortality (POSSUM)14 and the Estimation of Physiologic Ability and Surgical Stress Score (E-PASS)15 are complex and have demonstrated inconsistent results in their ability to predict morbidity and mortality for patients undergoing PD.16–19 Although sarcopenia has been used, it usually is combined with other measures of decreased physiologic reserve, and its use requires complex evaluation of imaging parameters.20 A multifactorial measure of overall physiologic reserve, such as frailty, may serve as a more accurate predictor of outcomes after this high-risk procedure.
Frailty has been defined as a clinical syndrome that involves the progressive loss of physical and mental function with or without the coexistence of disease.21 With decreased physiologic reserves, frail individuals have a decreased ability to maintain homeostasis and an increased vulnerability to acute stressors, including surgery.21–23 Findings have shown frailty to be an independent predictor of postoperative complications, hospital length of stay, discharge to a skilled- or assisted-living facility, and mortality.23–25
Although frailty is highly prevalent among the elderly, chronological age alone is a poor predictor of adverse outcomes after acute stress.26–28 The Canadian Study of Health and Aging has created a standardized frailty index (CSHA-FI) based on a cumulative deficit model.29,30 This model defines frailty as the cumulative effect of individual deficits based on clinical signs, symptoms, disease states, and disabilities, which provide a more accurate assessment of aging than chronological age.25
The CSHA-FI has been mapped to 11 variables contained in the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database to create a modified frailty index (mFI).31–33 The NSQIP mFI accurately predicts postoperative morbidity and mortality after vascular surgery or colectomy, as well as outcomes in other patient populations.31,34,35 However, no studies have specifically examined the mFI in the context of PD. Therefore, we hypothesized that the NSQIP mFI can predict postoperative outcomes after PD. A measurement of frailty that can aid in preoperative risk stratification could facilitate shared decision making, improve patient selection, and help to optimize patients preoperatively so as to reduce surgical complications.
METHODS
Patient Selection
All patients who underwent PD (Common Procedural Terminology code 48150—Classic Whipple procedure, and CPT code 48153—pylorus-sparing Whipple procedure) were identified in the 2005–2012 NSQIP Participant Use File (PUF).36 The PUF contains pre-, intra-, and postoperative data collected by specially trained surgical clinical reviewers from each NSQIP-participating institution. Patients undergoing emergency procedures, those classified as American Society of Anesthesiology (ASA) 5, and those with a diagnosis of preoperative sepsis were excluded from the analysis. Institutional review board approval was obtained for the study.
Definition of the mFI
The preoperative variables within the NSQIP dataset were reviewed to determine an mFI for each patient. The mFI, described previously by Velanovich et al.,33 includes the following 11 items in the NSQIP: diabetes; functional status (not independent); chronic obstructive pulmonary disease or pneumonia; congestive heart failure; history of myocardial infarction; hypertension requiring medication; peripheral vascular disease or rest pain; impaired sensorium; history of either transient ischemic attack or cerebrovascular accident; history of cerebrovascular accident with neurologic deficit; and prior percutaneous coronary intervention, previous coronary surgery, or history of angina. Each item was allocated the same weight (1 point) in the calculation of the index. The mFI then was calculated as the proportion of the total 11 items used in the study that were expressed in a given individual patient (total points as the sum of all the items divided by 11). Although the mFI is not meant to be a dichotomous variable, a cutoff of 0.27 was used based on previous data demonstrating the overlap in deficit accumulation between persons who are ‘‘robust’’ and those who are ‘‘frail’’ to be approximately 0.25.32,37,38
Definition of Morbidity and Mortality
Major complications were defined as Clavien–Dindo class 3 or 4 complications (life threatening or requiring intensive care management such as unplanned intubation, failure to wean from ventilator in >48 h, acute renal insufficiency requiring dialysis, new-onset neurologic deficit or coma, myocardial infarction, cardiac arrest, pulmonary embolism, graft failure, organ space infection). Minor complications were defined as Clavien–Dindo class 1 or 2 complications (surgical-site infection, pneumonia, deep vein thrombosis, urinary tract infection, peripheral nerve injury, postoperative bleeding requiring transfusion). Mortality was defined as death within 30 days after surgery. Failure to rescue was defined as previously described.39,40
Statistical Analysis
The sample means and standard deviations were computed for the continuous descriptive characteristics, and the count and proportions were calculated for the discrete descriptive characteristics by frailty groups (mFI ≥.27 vs <0.27). Demographic characteristics between patients with an mFI of 0.27 or higher and those with an mFI lower than 0.27 were compared using Chi square statistics for categorical variables and two-sample t tests for continuous variables. Univariate analysis using logistic regression identified clinically significant factors associated with the development of any complication, with major complications and mortality expressed as odds ratios (ORs). Those preoperative variables shown to be clinically relevant were then used to construct multiple variable models for the aforementioned outcomes. The covariates included age, sex, ASA, albumin (≥3 vs <3), and obesity (body mass index [BMI] ≥30 vs <30). All analyses were performed using SAS version 9.4 (SAS Inc., Cary, NC, USA).
RESULTS
Of the 13,851 patients who underwent PD, 3865 had at least 1 of the 11 frailty items missing and were therefore excluded from the analysis. The study sample comprised 9986 patients, and 6.4% (n = 637) of these patients had a high mFI (≥0.27). The mean age of the patients was 64.1 ± 12.4 years, and 48.8% (n = 4865) were women. The patients with a high mFI tended to be older and male, to have a higher BMI and a lower serum albumin level, to be less likely preoperatively to have fully independent functional status and more likely to have an ASA classification of 3 or 4, to be diabetic, to have major cardiovascular and neurologic comorbidities, and to have a major complication or die within 30 days after surgery (Table 1).
TABLE 1.
Patient characteristics
| Missing | mFI < 0.27 (n = 9349) n (%) |
mFI ≥ 0.27 (n = 637) n (%) |
Overall (n = 9986) n (%) |
p value | |
|---|---|---|---|---|---|
| Age (years) | 63.7 (12.5) | 70.1 (8.9) | 64.1 (12.4) | <0.0001 | |
| Female sex | 14 | 4655 (49.9) | 210 (33.0) | 4865 (48.8) | <0.0001 |
| Race | 3361 | 0.5871 | |||
| White | 5379 (86.7) | 375 (89.1) | 5754 (86.9) | ||
| Black | 603 (9.7) | 36 (8.6) | 639 (9.7) | ||
| Other | 222 (3.4) | 10 (2.3) | 232 (3.6) | ||
| Obesity (BMI ≥ 30 kg/m2) | 79 | 2201 (23.7) | 187 (29.7) | 2388 (24.1) | 0.0007 |
| Operative time (min) | 375.1 (129.0) | 381.5 (132.3) | 375.5 (129.3) | 0.2264 | |
| Hospital stay (days) | 29 | 13.0 (10.6) | 16.6 (13.4) | 13.2 (10.8) | <0.0001 |
| Total no. of complications | 0.7 (1.3) | 1.2 (1.8) | 0.8 (1.4) | <0.0001 | |
| Preoperative serum albumin (g/dL) | 1107 | 7321 (88.0) | 447 (79.8) | 7768 (87.5) | <0.0001 |
| ASA class | 10 | <0.0001 | |||
| 1–2 | 3002 (32.1) | 31 (4.9) | 3033 (30.4) | ||
| 3–4 | 6338 (67.8) | 605 (95.0) | 6943 (69.5) | ||
| Any complications | 3364 (36.0) | 309 (48.5) | 3673 (36.8) | <0.0001 | |
| Major complications | 2592 (27.7) | 260 (40.8) | 2852 (28.6) | <0.0001 | |
| Minor complications | 1359 (14.5) | 111 (17.4) | 1470 (14.7) | 0.0464 | |
| 30-days mortality | 249 (2.7) | 40 (6.3) | 289 (2.9) | <0.0001 | |
| Current smoker within 1 year | 1 | 1983 (21.2) | 150 (23.6) | 2133 (21.4) | 0.1642 |
| >10% Loss body weight in last 6 months | 1680 (18.0) | 152 (23.9) | 1832 (18.3) | 0.0002 | |
| Bleeding disorder | 193 (2.1) | 49 (7.7) | 242 (2.4) | <0.0001 | |
| Chemotherapy for malignancy in ≤30 days preoperatively | 289 (3.1) | 15 (2.4) | 304 (3.0) | 0.2952 | |
| Dyspnea | <0.0001 | ||||
| At rest | 33 (0.4) | 10 (1.6) | 43 (0.4) | ||
| Moderate exertion | 647 (6.9) | 135 (21.2) | 782 (7.8) | ||
| Preoperative variables included in calculation of the mFI | |||||
| Functional health status before surgery (totally or partially dependent) | 108 (1.2) | 105 (16.5) | 213 (2.1) | <0.0001 | |
| Diabetes | 1780 (19.0) | 472 (74.1) | 2252 (22.6) | <0.0001 | |
| Hypertension | 4691 (50.2) | 619 (97.2) | 5310 (53.2) | <0.0001 | |
| History of PVD | 59 (0.6) | 69 (10.8) | 128 (1.3) | <0.0001 | |
| CHF within 30 days before surgery | 8 (0.1) | 18 (2.8) | 26 (0.3) | <0.0001 | |
| MI 6 months before surgery | 9 (0.1) | 19 (3.0) | 28 (0.3) | <0.0001 | |
| History of severe COPD | 285 (3.0) | 152 (23.9) | 437 (4.4) | <0.0001 | |
| Previous PCI | 367 (3.9) | 272 (42.7) | 639 (6.4) | <0.0001 | |
| History of impaired sensorium | 3 (0.0) | 4 (0.6) | 7 (0.1) | <0.0001 | |
| History of transient ischemic attack | 106 (1.1) | 104 (16.3) | 210 (2.1) | <0.0001 | |
| CVA/stroke with neurologic deficit | 56 (0.6) | 74 (11.6) | 130 (1.3) | <0.0001 |
mFI modified frailty index, BMI body mass index, ASA American Society of Anesthesiology, PVD peripheral vascular disease, CHF congestive heart failure, MI myocardial infarction, COPD chronic obstructive pulmonary disease, PCI percutaneous cardiac intervention, CVA cerebrovascular accident
Most of the patients (n = 3829) had an mFI of 0. Of these patients, 33.7% (n = 1292) experienced a complication, 25.7% (n = 983) experienced a major complication, and 1.3% (n = 51) died within 30 days after surgery. As mFI increased, the total number of patients within an mFI category declined. Increasing mFI was associated with a higher incidence of any complication (p < 0.001), a major complication (p < 0.001), or 30-days mortality (p < 0.001) (Table 2; Fig. 1).
TABLE 2.
Trends of mFI and outcomes
| mFI | Any complication |
Major complication |
30-days mortality |
|||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| 0.00000 | 1292 | 33.7425 | 983 | 25.6725 | 51 | 1.3319 |
| 0.09091 | 1368 | 36.3154 | 1051 | 27.9002 | 117 | 3.1059 |
| 0.18182 | 704 | 40.1597 | 558 | 31.8311 | 81 | 4.6207 |
| 0.27273 | 251 | 48.2692 | 209 | 40.1923 | 29 | 5.5769 |
| 0.36364 | 46 | 47.4227 | 41 | 42.2680 | 6 | 6.1856 |
| 0.45455 | 9 | 56.2500 | 8 | 50.0000 | 3 | 18.7500 |
| 0.54545 | 3 | 75.0000 | 2 | 50.0000 | 2 | 50.0000 |
| p value | <0.0001 | <0.0001 | <0.0001 | |||
mFI modified frailty index
FIG. 1.
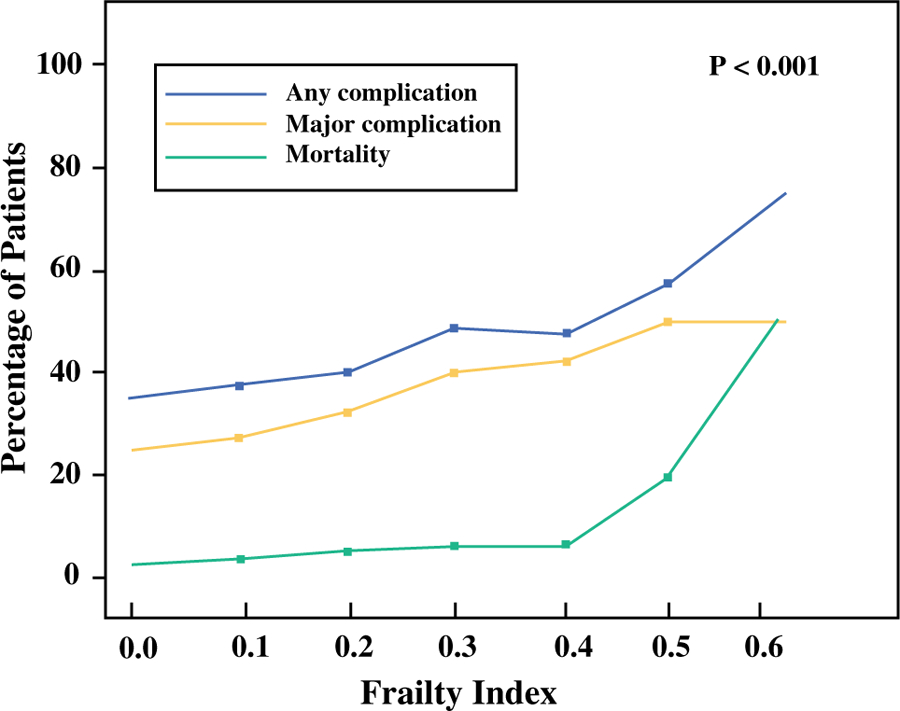
Percent of patients with postoperative 30-day morbidity and morality based on modified frailty index
Of 9349 patients with an mFI of 0.27 or lower, 8.3% (n = 772) experienced a minor complication, 27.7% (n = 2592) experienced a major complication, and 2.7% (n = 249) died within 30 days after surgery. Of 637 patients with an mFI higher than 0.27, 7.7% (n = 49) experienced a minor complication, 40.8% (n = 260) experienced a major complication, and 6.3% (n = 40) died within 30 days after surgery. Failure to rescue occurred for 10% (n = 289) of the patients and was significantly associated with frailty and low mFI (9.5% vs a high mFI of 15.1%; p = 0.007).
In the univariate analysis, the development of any complication was predicted by increasing age, male sex, obesity (BMI > 30 kg/m2), low albumin, more than 10% weight loss, longer operative time, longer hospital length of stay, higher ASA, loss of functional status, transfer from a place other than home, and an mFI of 0.27 or higher. Increasing age, male sex, obesity, longer operative time, longer hospital length of stay, higher ASA (3 or 4), loss of functional status, low albumin, more than 10% weight loss, and an mFI of 0.27 or higher predicted the development of a major complication (Table 3). Increasing age, obesity, longer operative time, longer hospital length of stay, higher ASA status, loss of functional status, and high mFI predicted 30-days mortality (Table 3).
TABLE 3.
Univariate analysis of major complications and 30-days mortality
| Outcome | Major complication |
30-days mortality |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | OR | Lower CL | Upper CL | p Value | Overall p value | OR | Lower CL | Upper CL | p value | Overall p Value |
| Age (10-year increase) | 1.095 | 1.057 | 1.135 | <0.0001 | 1.525 | 1.367 | 1.702 | <0.0001 | ||
| Sex (male vs female) | 1.225 | 1.123 | 1.337 | <0.001 | 1.240 | 0.979 | 1.570 | 0.0739 | ||
| Race | 0.043 | 0.36 | ||||||||
| Black vs white | 0.988 | 0.823 | 1.187 | 0.8991 | 0.679 | 0.384 | 1.201 | 0.1837 | ||
| Other vs white | 1.207 | 1.040 | 1.402 | 0.0136 | 1.080 | 0.728 | 1.604 | 0.7023 | ||
| BMI > 30 kg/m2 | 1.274 | 1.153 | 1.407 | <0.0001 | 1.298 | 1.001 | 1.683 | 0.0490 | ||
| Weight loss (yes vs no) | 0.886 | 0.791 | 0.993 | 0.0382 | 1.249 | 0.941 | 1.660 | 0.1242 | ||
| Albumin > 3 g/dL | 0.676 | 0.593 | 0.772 | <0.0001 | 0.470 | 0.350 | 0.631 | <0.0001 | ||
| Smoking (no vs yes) | 1.027 | 0.924 | 1.143 | 0.6184 | 1.308 | 0.960 | 1.780 | 0.0885 | ||
| Operative time (10-min increase) | 1.014 | 1.011 | 1.018 | <0.0001 | 1.019 | 1.011 | 1.027 | <0.0001 | ||
| Total hospital length stay (per day) | 1.117 | 1.110 | 1.124 | <0.0001 | 1.016 | 1.009 | 1.024 | <0.0001 | ||
| Transferred from other vs home | 1.765 | 1.430 | 2.179 | <0.0001 | 1.524 | 0.911 | 2.552 | 0.1086 | ||
| ASA (3/4 vs 1/2) | 1.378 | 1.250 | 1.519 | <0.0001 | 3.336 | 2.326 | 4.784 | <0.0001 | ||
| Functional status | <0.0001 | <0.0001 | ||||||||
| Partially dependent vs independent | 2.447 | 1.835 | 3.263 | <0.0001 | 3.698 | 2.242 | 6.099 | <0.0001 | ||
| Totally dependent vs independent | 1.361 | 0.577 | 3.215 | 0.4816 | 3.365 | 0.785 | 14.423 | 0.1022 | ||
| mFI (≥0.27 vs <0.27) | 1.798 | 1.526 | 2.120 | <0.0001 | 2.449 | 1.736 | 3.454 | <0.0001 | ||
OR odds ratio, CL confidence limit, BMI body mass index, ASA American Society of Anesthesiology, mFI modified frailty index
Older patients (age >75 years) represented 19.6% (n = 1947) of the patients undergoing PD. In this sub-group, high mFI was significantly more common (9.7%, n = 208) than among younger patients (5.5%, n = 427), p < 0.001.
In the multivariate analysis, age, male sex, higher ASA, albumin level lower than 3, obesity, and an mFI of 0.27 or higher remained independent preoperative predictors of any complication, major postoperative morbidity, and 30-days mortality (Table 4). The frailty index was a strong predictor of major morbidity (OR 1.54; 95% confidence interval [CI] 1.29–1.85; p < 0.001) and 30-days mortality (OR 1.54; 95% CI 1.05–2.25; p = 0.027).
TABLE 4.
Multivariable analysis of major complications and 30-days mortality
| Outcome | Major complication |
30-days mortality |
||||||
|---|---|---|---|---|---|---|---|---|
| Variable | OR | Lower CL | Upper CL | p value | OR | Lower CL | Upper CL | p value |
| Age (10-year increase) | 1.076 | 1.034 | 1.119 | 0.0003 | 1.438 | 1.275 | 1.622 | <0.0001 |
| Sex (male vs female) | 1.214 | 1.105 | 1.334 | <0.0001 | 1.193 | 0.926 | 1.537 | 0.1721 |
| BMI > 30 | 1.317 | 1.182 | 1.467 | <0.0001 | 1.456 | 1.101 | 1.925 | 0.0084 |
| Albumin > 3 g/dL | 0.741 | 0.647 | 0.849 | <0.0001 | 0.585 | 0.432 | 0.792 | 0.0005 |
| ASA (3/4 vs 1/2) | 1.281 | 1.149 | 1.429 | <0.0001 | 2.287 | 1.562 | 3.349 | <0.0001 |
| mFI (≥0.27 vs <0.27) | 1.544 | 1.289 | 1.850 | <0.0001 | 1.536 | 1.049 | 2.248 | 0.0274 |
OR odds ratio, CL confidence limit, BMI body mass index, ASA American Society of Anesthesiology, mFI modified frailty index
DISCUSSION
In the current study, high mFI was associated with worse outcomes after PD. Frailty is considered to be a state of decreased physiologic reserves arising from cumulative deficits in multiple homeostatic systems that results in greater susceptibility and less resilience to physiologic stressors.41 Importantly, although frailty traditionally has been described in the form of physical weakness as a function of aging, it is well known that besides chronological age, several other factors contribute to physiologic aging and determine functional reserve and response to stress.20,21,23,42 Surgeons often rely too much a patient’s age and not enough on an objective measure of physiologic reserve, whereas patients may tend to overestimate their ability to tolerate major surgical stresses, potentially leading to unrealistic expectations of their outcome and recovery.43
Both pancreatic cancer and PD are major physiologic stressors, so the concept of frailty is particularly important in this population of cancer patients. Accordingly, several authors have advocated the routine incorporation of frailty assessment for older cancer patients, including comprehensive geriatric assessment (CGA).44–46
The CGA, although very specific, is complex and very time consuming, making it less than ideal as a screening tool in the everyday clinical setting.47–50 Studies have shown that the CGA is infrequently used by surgeons in preoperative frailty assessment of cancer patients.51 Therefore, abbreviated indices that efficiently assess frailty are essential for risk stratification of patients and for helping to determine eligibility for surgery. The mFI is a simple frailty assessment tool that uses easily available historical variables that can be reliably and consistently collected in the preoperative setting.
In the current study, 25.7% of the patients not considered frail (mFI = 0) had major complications, and 1.3% of these patients had postoperative mortality. This is consistent with the published data on outcomes after PD in several large series.2,3,5 We found that the mFI correlates well with the development of postoperative complications and 30-days mortality after PD. As the mFI increases, so does the percentage of patients experiencing an adverse outcome. Importantly, only 6.4% of the patients in our study cohort had a high mFI (mFI > 0.27), which likely represents a selection bias toward healthier or less frail patients for PD. The high-mFI group had significant morbidity (41%) and mortality (5.6%).
Whereas age, BMI, ASA status, and nutritional status (low albumin level) were independent determinants of adverse outcomes, mFI remained a predictor of postoperative outcomes in the multivariable analysis. The results from the current study mirror reports from prior studies using the mFI.31,33,52–55 However, to our knowledge, this is the first study to use a large national database to validate the ability of the mFI to predict development of postoperative adverse events after PD.
Our study had several important implications. First, the variables used to calculate the mFI are physical, readily available from the history, and easily reproducible. The identification of frailty allows for an objective assessment of the potential for the development of complications and recovery from them. This can in turn help in better informing the shared decision-making process, which is essential for preoperative counseling and patient selection.
Second, frailty, instead of being an irreversible state, occurs as a continuum within a spectrum, with the possibility of transitions between higher and lower states of frailty.56 Therefore, identification of frail patients and implementation of prehabilitation strategies to treat modifiable factors that determine frailty may prevent further deterioration in physical and functional impairment and potentially improve postoperative outcomes.57–59 These strategies include measures such as referral to specialty geriatrics clinics for an in-depth assessment and incorporation of physical and cognitive exercise, social support, and nutrition for patients in earlier stages of frailty.60 Although several individual variables within the mFI are likely not modifiable during the preoperative period, a multidisciplinary team approach can help to mitigate the risks associated with specific preoperative risk factors.
Our study had a several limitations. First, we chose 11 of the 70 variables described in the original CHSA study, which mapped to the preoperative variables used in the NSQIP dataset. Arguably, these variables may not fully represent the entire spectrum of frailty parameters. A previous analysis indicates that one need not use the same items or even the same number of items to estimate the proportion of patients that represent a certain value within the index.61 Although the inclusion of more variables does increase the precision of the estimate, the differences in the mean mFI values between similar distributions of phenotypic categories of frailty are not statistically significant.37
Second, variables used in the mFI are based on subjective assessment. The NSQIP database also was not specifically designed to assess frailty. Therefore, its use for preoperative patient assessment needs to be validated in prospective studies.
Finally, given its retrospective nature, the study was limited by an inherent selection bias, with inclusion of lower-risk patients who were de facto operative candidates. Nonetheless, within the study sample, the mFI was a strong, objective, and reproducible indicator of postoperative outcomes.
CONCLUSIONS
In conclusion, the mFI is a strong predictor of postoperative complications and mortality after PD. Its use in the preoperative setting can help to risk-stratify patients, identify subgroups at increased risk for the development of adverse events, and subsequently institute prehabilitative measures to potentially optimize modifiable factors and minimize complications.
ACKNOWLEDGEMENT
This study was supported by Wake Forest University Biostatistics shared resource NCI CCSG P30CA012197.
Footnotes
DISCLOSURES There are no conflicts of interest.
REFERENCES
- 1.Howlader N, Noone A, Krapcho M, Garshell J, Miller D, Altekruse S, et al. SEER Cancer Statistics Review, 1975–2012. National Cancer Institute, Bethesda, MD, 2015, pp 1–101, based on November 2014 SEER data submission posted to the SEER website April 2015. [Google Scholar]
- 2.Cameron JL, He J. Two thousand consecutive pancreaticoduodenectomies. J Am Coll Surg 2015;220:530–6. [DOI] [PubMed] [Google Scholar]
- 3.Sohn TA, Yeo CJ, Cameron JL, Koniaris L, Kaushal S, Kaushal RA, et al. Resected adenocarcinoma of the pancreas–616 patients: results, outcomes, and prognostic indicators. J Gastrointest Surg. 2000;4:567–79. [DOI] [PubMed] [Google Scholar]
- 4.Oettle H, Post S, Post P, Gellert K, Langrehr J, Ridwelski K, et al. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer: a randomized controlled trial. JAMA. 2007;297:267–77. [DOI] [PubMed] [Google Scholar]
- 5.Winter JM, Cameron JL, Campbell KA, Arnold MA, Chang DC, Coleman J, et al. 1423 Pancreaticoduodenectomies for pancreatic cancer: a single-institution experience. J Gastrointest Surg. 2006;10:1199–211. [DOI] [PubMed] [Google Scholar]
- 6.Pratt WB, Vollmer CM, Callery MP. Outcomes in pancreatic resection are negatively influenced by preoperative hospitalization. HPB. 2009;11:57–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ceppa EP, Pitt HA, Nakeeb A, Schmidt CM, Zyromski NJ, House MG, et al. Reducing readmissions after pancreatectomy: limiting complications and coordinating the care continuum. J Am Coll Surg 2015;221:708–16. [DOI] [PubMed] [Google Scholar]
- 8.Balcom JH, Rattner DW, Warshaw AL, Chang Y, Fernandez-del Castillo C. Ten-year experience with 733 pancreatic resections: changing indications, older patients, and decreasing length of hospitalization. Arch Surg. 2001;136:391–8. [DOI] [PubMed] [Google Scholar]
- 9.Riall TS, Nealon WH, Goodwin JS, Townsend CM, Freeman JL. Outcomes following pancreatic resection: variability among high-volume providers. Surgery. 2008;144:133–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Callery MP, Pratt WB, Kent TS, Chaikof EL, Vollmer CM. A prospectively validated clinical risk score accurately predicts pancreatic fistula after pancreatoduodenectomy. J Am Coll Surg. 2013;216:1–14. [DOI] [PubMed] [Google Scholar]
- 11.Roberts KJ, Storey R, Hodson J, Smith AM, Morris-Stiff G. Preoperative prediction of pancreatic fistula: is it possible? Pancreatology. 2013;13:423–8. [DOI] [PubMed] [Google Scholar]
- 12.Roberts KJ, Hodson J, Mehrzad H, Marudanayagam R, Sutcliffe RP, Muiesan P, et al. A preoperative predictive score of pancreatic fistula following pancreatoduodenectomy. HPB. 2014;16:620–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kirihara Y, Takahashi N, Hashimoto Y, Sclabas GM, Khan S, Moriya T, et al. Prediction of pancreatic anastomotic failure after pancreatoduodenectomy: the use of preoperative, quantitative computed tomography to measure remnant pancreatic volume and body composition. Ann Surg. 2013;257:512–9. [DOI] [PubMed] [Google Scholar]
- 14.Copeland GP, Jones D, Walters M. POSSUM: a scoring system for surgical audit. Br J Surg. 1991;78:355–60. [DOI] [PubMed] [Google Scholar]
- 15.Haga Y, Ikei S, Ogawa M. Estimation of physiologic ability and surgical stress (E-PASS) as a new prediction scoring system for postoperative morbidity and mortality following elective gastrointestinal surgery. Surg Today. 1999;29:219–25. [DOI] [PubMed] [Google Scholar]
- 16.Deyle S, Banz Martine V, Wagner M, Becker K, Inderbitzin D, Gloor B, et al. Estimation of physiologic ability and surgical stress score does not predict immediate outcome after pancreatic surgery. Pancreas. 2011;40:723. [DOI] [PubMed] [Google Scholar]
- 17.Hashimoto D, Takamori H, Sakamoto Y, Tanaka H, Hirota M, Baba H. Can the physiologic ability and surgical stress (E-PASS) scoring system predict operative morbidity after distal pancreatectomy? Surg Today. 2010;40:632–7. [DOI] [PubMed] [Google Scholar]
- 18.Hashimoto D, Takamori H, Sakamoto Y, Ikuta Y, Nakahara O, Furuhashi S, et al. Is an estimation of physiologic ability and surgical stress able to predict operative morbidity after pancreaticoduodenectomy? J Hepatobil Pancreat Sci. 2010;17:132–8. [DOI] [PubMed] [Google Scholar]
- 19.Khan AW, Shah SR, Agarwal AK, Davidson BR. Evaluation of the POSSUM scoring system for comparative audit in pancreatic surgery. Dig Surg. 2003;20:539–45. [DOI] [PubMed] [Google Scholar]
- 20.Wagner D, DeMarco MM, Amini N, Buttner S, Segev D, Gani F, et al. Role of frailty and sarcopenia in predicting outcomes among patients undergoing gastrointestinal surgery. World J Gastrointest Surg. 2016;8:27–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56:M146–56. [DOI] [PubMed] [Google Scholar]
- 22.Ahmed N, Mandel R, Fain MJ. Frailty: an emerging geriatric syndrome. Am J Med. 2007;120:748–53. [DOI] [PubMed] [Google Scholar]
- 23.Makary MA, Segev DL, Pronovost PJ, Syin D, Bandeen-Roche K, Patel P, et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg. 2010;210:901–8. [DOI] [PubMed] [Google Scholar]
- 24.Saxton A, Velanovich V. Preoperative frailty and quality of life as predictors of postoperative complications. Ann Surg. 2011;253:1223–9. [DOI] [PubMed] [Google Scholar]
- 25.Handforth C, Clegg A, Young C, Simpkins S, Seymour MT, Selby PJ, et al. The prevalence and outcomes of frailty in older cancer patients: a systematic review. Ann Oncol. 2014;26:1–11. [DOI] [PubMed] [Google Scholar]
- 26.Schuurmans H, Steverink N, Lindenberg S, Frieswijk N, Slaets JPJ. Old or frail: what tells us more? J Gerontol A Biol Sci Med Sci. 2004;59:M962–5. [DOI] [PubMed] [Google Scholar]
- 27.Voudris V, Skoularigis JS, Malakos JS, Kourgianides GC, Pavlides GS, Manginas AN, et al. Long-term clinical outcome of coronary artery stenting in elderly patients. Coron Artery Dis 2002;13:323–9. [DOI] [PubMed] [Google Scholar]
- 28.Weinmann M, Jeremic B, Bamberg M, Bokemeyer C. Treatment of lung cancer in elderly part II: Small cell lung cancer. Lung Cancer. 2003;40:1–16. [DOI] [PubMed] [Google Scholar]
- 29.Mitnitski AB, Mogilner AJ, Rockwood K. Accumulation of deficits as a proxy measure of aging. Sci World J. 2001;1:323–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Rockwood K, Song X, MacKnight C, Bergman H, Hogan DB, McDowell I, et al. Frailty in the elderly: a concept analysis. J Nurs. 2013;60:105–10. [Google Scholar]
- 31.Karam J, Tsiouris A, Shepard A, Velanovich V, Rubinfeld I. Simplified frailty index to predict adverse outcomes and mortality in vascular surgery patients. Ann Vasc Surg. 2013;27:904–8. [DOI] [PubMed] [Google Scholar]
- 32.Tsiouris A, Hammoud ZT, Velanovich V, Hodari A, Borgi J, Rubinfeld I. A modified frailty index to assess morbidity and mortality after lobectomy. J Surg Res. 2013;183:40–6. [DOI] [PubMed] [Google Scholar]
- 33.Velanovich V, Antoine H, Swartz A, Peters D, Rubinfeld I. Accumulating deficits model of frailty and postoperative mortality and morbidity: its application to a national database. J Surg Res. 2013;183:104–10. [DOI] [PubMed] [Google Scholar]
- 34.Obeid NM, Azuh O, Reddy S, Webb S, Reickert C, Velanovich V, et al. Predictors of critical care-related complications in colectomy patients using the National Surgical Quality Improvement Program: exploring frailty and aggressive laparoscopic approaches. J Trauma Acute Care Surg. 2012;72:878–83. [DOI] [PubMed] [Google Scholar]
- 35.Cloney M, D’Amico R, Lebovic J, Nazarian M, Sonabend AM, Zacharia BE, et al. Frailty in geriatric glioblastoma patients: a predictor of operative morbidity and outcome. 2016 AANS Annu Sci Meet. 2016;89:362–7. [DOI] [PubMed] [Google Scholar]
- 36.ACS NSQIP Participant Use Data File 2005–2012. https://www.facs.org/quality-programs/acs-nsqip/program-specifics/participant-use Accessed 22 December 2016.
- 37.Rockwood K, Andrew M, Mitnitski A. A comparison of two approaches to measuring frailty in elderly people. J Gerontol A Biol Sci Med Sci. 2007;62:738–43. [DOI] [PubMed] [Google Scholar]
- 38.Ali R, Schwalb JM, Nerenz DR, Antoine HJ, Rubinfeld I. Use of the modified frailty index to predict 30-day morbidity and mortality from spine surgery. J Neurosurg Spine. 2016. doi: 10.3171/2015.10.SPINE14582. [DOI] [PubMed] [Google Scholar]
- 39.Silber JH, Romano PS, Rosen AK, Wang Y, Even-Shoshan O, Volpp KG. Failure-to-rescue: comparing definitions to measure quality of care. Med Care. 2007;45:918–25. [DOI] [PubMed] [Google Scholar]
- 40.Silber JH, Williams SV, Krakauer H, Schwartz JS. Hospital and patient characteristics associated with death after surgery: a study of adverse occurrence and failure to rescue. Med Care. 1992;30:615–29. [DOI] [PubMed] [Google Scholar]
- 41.Rockwood K, Mitnitski A. Frailty defined by deficit accumulation and geriatric medicine defined by frailty. Clin Geriatr Med. 2011;27:17–26. [DOI] [PubMed] [Google Scholar]
- 42.Audisio RA, van Leeuwen BL. Beyond ‘‘age’’: frailty assessment strategies improve care of older patients with cancer. Ann Surg Oncol. 2015;22:3774–5. [DOI] [PubMed] [Google Scholar]
- 43.Revenig LM, Canter DJ, Henderson MA, Ogan K, Kooby DA, Maithel SK, et al. Preoperative quantification of perceptions of surgical frailty. J Surg Res. 2015;193:583–9. [DOI] [PubMed] [Google Scholar]
- 44.Buigues C, Juarros-Folgado P, Fernandez-Garrido J, Navarro-Martinez R, Cauli O. Frailty syndrome and preoperative risk evaluation: a systematic review. Arch Gerontol Geriatr. 2015;61:309–21. [DOI] [PubMed] [Google Scholar]
- 45.Robinson TN, Walston JD, Brummel NE, Deiner S, Brown CH, Kennedy M, et al. Frailty for surgeons: review of a national institute on aging conference on frailty for specialists. J Am Coll Surg. 2015;221:1083–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Audisio RA. Preoperative evaluation of the older patient with cancer. J Geriatr Oncol. 2016. doi: 10.1016/j.jgo.2016.04.003. [DOI] [PubMed] [Google Scholar]
- 47.Extermann M, Aapro M, Bernabei R, Cohen HJ, Droz JP, Lichtman S, et al. Use of comprehensive geriatric assessment in older cancer patients: recommendations from the task force on CGA of the International Society of Geriatric Oncology (SIOG). Crit Rev Oncol Hematol. 2005;55:241–52. [DOI] [PubMed] [Google Scholar]
- 48.Ellis G, Whitehead MA, O’Neill D, Langhorne P, Robinson D. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst Rev. CD006211;2011. [DOI] [PMC free article] [PubMed]
- 49.Kothari A, Phillips S, Bretl T, Block K, Weigel, T. Components of geriatric assessments predict thoracic surgery outcomes. J Surg Res. 2011;166:5–13. [DOI] [PubMed] [Google Scholar]
- 50.Horgan AM, Leighl NB, Coate L, Liu G, Palepu P, Knox JJ, et al. Impact and feasibility of a comprehensive geriatric assessment in the oncology setting: a pilot study. Am J Clin Oncol. 2012;35:322–8. [DOI] [PubMed] [Google Scholar]
- 51.Ghignone F, van Leeuwen BL, Montroni I, Huisman MG, Somasundar P, Cheung KL, et al. The assessment and management of older cancer patients: a SIOG surgical task force survey on surgeons’ attitudes. Eur J Surg Oncol. 2015;42:297–302. [DOI] [PubMed] [Google Scholar]
- 52.Lascano D, Pak JS, Kates M, Finkelstein JB, Silva M, Hagen E, et al. Validation of a frailty index in patients undergoing curative surgery for urologic malignancy and comparison with other risk stratification tools. Urol Oncol Semin Orig Investig. 2015;33:426.e1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Uppal S, Igwe E, Rice LW, Spencer RJ, Rose SL. Frailty index predicts severe complications in gynecologic oncology patients. Gynecol Oncol. 2015;137:98–101. [DOI] [PubMed] [Google Scholar]
- 54.Chappidi MR, Kates M, Patel HD, Tosoian JJ, Kaye DR, Sopko NA, et al. Frailty as a marker of adverse outcomes in patients with bladder cancer undergoing radical cystectomy. Urol Oncol Semin Orig Investig. 2016. doi: 10.1016/j.urolonc.2015.12.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Wagner D, DeMarco MM, Amini N, Buttner S, Segev D, Gani F, et al. Wagner 2016, Sarcopenia outomes GI surgery cancer. World J Gastrointest Surg. 2016;8:27–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Gill TM, Gahbauer EA, Allore HG, Han L. Transitions between frailty states among community-living older persons. Arch Intern Med. 2006;166:418–23. [DOI] [PubMed] [Google Scholar]
- 57.McCorkle R, Strumpf NE, Nuamah IF, Adler DC, Cooley ME, Jepson C, et al. A specialized home care intervention improves survival among older post-surgical cancer patients. J Am Geriatr Soc. 2000;48:1707–13. [DOI] [PubMed] [Google Scholar]
- 58.Fiatarone MA, O’Neill EF, Ryan ND, Clements KM, Solares GR, Nelson ME, et al. Exercise training and nutritional supplementation for physical frailty in very elderly people. N Engl J Med. 1994;330:1769–75. [DOI] [PubMed] [Google Scholar]
- 59.Morley JE, Vellas B, Abellan van Kan G, Anker SD, Bauer JM, Bernabei R, et al. Frailty consensus: a call to action. J Am Med Dir Assoc. 2013;14:392–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Orlando Frailty Conference Group. Raising awareness on the urgent need to implement frailty into clinical practice. J Frailty Aging. 2013;2:121–4. [PMC free article] [PubMed] [Google Scholar]
- 61.Rockwood K, Mitnitski A, Song X, Steen B, Skoog I. Long-term risks of death and institutionalization of elderly people in relation to deficit accumulation at age 70. J Am Geriatr Soc. 2006;54:975–9. [DOI] [PubMed] [Google Scholar]