

Abstract
Noninvasive body shaping is becoming a growing demand. The aim of this study was to investigate the efficacy and safety of the combined treatments of 1064 nm Nd:YAG and 2940 nm Er:YAG in noninvasive lipolysis and skin tightening. Ten females were enrolled, and all women's side of the waist or the lower part of the abdomen were treated. In the first step, the 1064 nm Nd:YAG was used. As a second step, the 2940 nm Er:YAG laser was applied. Each woman was treated four times, once every 2 weeks. The effects were determined by comparative photo documentation, waist circumference measurement, two‐dimensional B‐mode ultrasonography and low‐dose native computer tomography (CT), whereas body fat was monitored with bioelectric impedance. The tissue firmness was measured by ultrasound shear wave elastography. Combined laser treatment significantly reduced waist circumference and total body fat. Ultrasonography has revealed that the treatment considerably decreased fat thickness and improved skin stiffness in the treated region. Subcutaneous fat volume, measured by low‐dose CT, displayed a moderate decrease in the waist region. The combined 1064 nm Nd:YAG and 2940 nm Er:YAG laser treatment results in the reduction of fat tissue and tightens the skin as confirmed by objective measurements.
Keywords: Er:YAG laser, fat reduction, Nd:YAG laser, skin stiffness
Noninvasive body shaping is a growing demand. Our goal was to test the efficacy of the combined treatments of 1064 nm Nd:YAG and 2940 nm Er:YAG in noninvasive lipolysis and skin tightening. Four treatments were performed in 10 subjects. Waist circumference, fat thickness, fat volume and tissue firmness were determined. The combined 1064 nm Nd:YAG and 2940 nm Er:YAG laser treatment resulted in the reduction of fat tissue and tightened the skin.
1. INTRODUCTION
According to a recent survey, obesity in the United States affects almost 40% of adults and nearly 20% of youth 1. Obesity is known to be accompanied by the elevated risk of cardiovascular diseases (eg, heart failure) and metabolic disorders (eg, type 2 diabetes mellitus) 2, 3. Furthermore, it is a risk factor for some cancers and may influence the cancer outcome 4. Obesity significantly increases the risk of developing an arthritic condition, as well 5. Thus, many people are seeking to shed weight. In addition to health related factors, cosmetic purposes, greater social integration, higher self‐worth and self‐esteem can also be motivations for weight loss. For this aim, several body contouring techniques are available at present. Nonsurgical procedures are preferred due to fewer side effects and shorter recovery times. There are four prominent non‐invasive techniques for reduction of subcutaneous adipose tissue: cryolipolysis, high‐intensity focused ultrasound (HIFU), radio frequency (RF) and low‐level laser therapy (LLLT) 6. Cryolipolysis utilizes cold temperature which triggers apoptosis of adipocytes and initiates inflammatory response leading to slow digestion of fat tissue by surrounding macrophages 7, 8 while HIFU quickly raises local temperature leading to immediate death of fat cells via coagulative necrosis 9, 10, 11. The use of RF is based on an oscillating electrical current which generates heat 12. As concerns LLLT, the mechanism of its action on fat is controversial and probably affects several intracellular targets 13. For noninvasive body contouring, the efficacy of red lasers of 635 nm was reported 14, 15. However, combination of red lasers with infrared 16, 17 and blue 18 wavelengths was also found to be effective. In addition to fat reduction, skin tightening is also an important issue in order to achieve a good cosmetic outcome. Different laser systems were reported to be able to tighten skin while diminishing the quantity of fat and combination of different wavelengths seems to be useful in terms of skin tightening, as well 19, 20. The efficiency of combined Er:YAG and Nd:YAG laser treatment for noninvasive body contouring has already been described in a case report 21; however, clinical trials with detailed and objective measurements are still missing. Thus, the goal of our study was to examine the safety and efficacy of combined 1064 nm Nd:YAG and 2940 nm Er:YAG laser treatment on body shaping and skin tightening.
2. MATERIALS AND METHODS
2.1. Subjects and study protocol
The study involved 10 females with visible and measurable excess fat on waist and abdomen. Their age was between 27 and 50 years. The mean body mass index was 26.84 (range: 19.4‐38.1). Participant data are summarized in Table 1.
Table 1.
Age and body mass index of the participants
| ID number | Age (years) | Body mass index |
|---|---|---|
| 1 | 37 | 22.9 |
| 2 | 41 | 24.2 |
| 3 | 27 | 38.1 |
| 4 | 46 | 28.4 |
| 5 | 43 | 31.5 |
| 6 | 31 | 23.9 |
| 7 | 34 | 23.8 |
| 8 | 42 | 19.4 |
| 9 | 44 | 27.1 |
| 10 | 50 | 29.1 |
The study protocol was approved in advance by the local institutional ethics committee for human biomedical trials at the University of Szeged (license number: 175/2017‐SZTE). All involved participant had otherwise healthy skin and did not suffer from any major disease. Exclusion criteria were pregnancy, anticoagulant medication, a history of malignancy and acute dermatitis on the treated site. All subject participated only after receiving detailed oral and written information and signing an informed consent agreement. Figure 1 demonstrates the study protocol. Briefly, photo documentation, measurement of waist circumference, body fat monitoring (BFM), subcutaneous fat tissue thickness measurement by two‐dimensional (2D) B‐mode ultrasonography, elastography and low‐dose computer tomography (CT) were performed in each subject at the beginning (week 0) then they received the first combined laser treatment. Further treatments were given on weeks 2, 4 and 6. These treatments were preceded by photo documentation, waist circumference measurement and BFM. On week 8, all above‐mentioned examinations were performed again.
Figure 1.
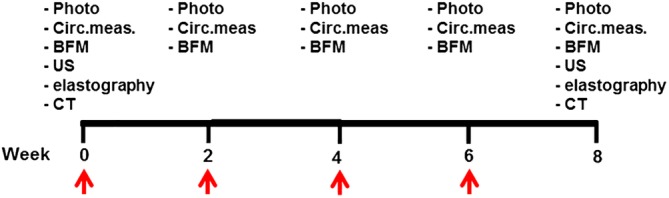
Study protocol. The red arrows indicate the times of combined laser treatments. Photo, photo documentation; Circ. meas., measurement of waist circumference; BFM, body fat monitoring; US, ultrasound; CT, low‐dose computed tomography
2.2. Laser treatment
The females were treated with the combined 1064 nm Nd:YAG and 2940 nm Er:YAG laser (FOTONA SP Dynamis, TightSculpting PIANO and SMOOTH mode). Laser treatments were applied four times during the study. The first step was to use the PIANO mode, the 1064 nm Nd:YAG was applied with S11‐L‐Runner scanning hand piece, the scanning surface was 78 mm × 84 mm and power flux density (fluence/treatment time) was 1.2 W/cm2, at a fluence of 108 J/cm2. All participants' treated skin areas were treated in nine fields, 5 (upper part of abdomen) +2 (right side of waist) +2 (left side of waist). The temperature of the skin surface was 42°C for 8 minutes. The skin's temperature was checked by special MatrixView temperature monitor. During treatment, neither skin cooling nor local anesthesia was applied. The second step was to apply the SMOOTH mode, the 2940 nm Er:YAG laser with R11 handpiece and with a spot size of 7 mm at a fluence of 2 J/cm2 and 2 Hz frequency. We passed four times over the treated area with Er: YAG laser. Specific safety eyeglasses were worn during the treatment for both the operator and the patient. The participants reported only minimal sense of warmth. Total laser application lasted about 60 minutes, this time consisted of two consecutive steps. Treatment time was shorter, as we used the scanning handpiece, because this way multiple fields can be heated up to 42°C at the same time.
2.3. Photo documentation
Photographs were taken before the first laser treatment (baseline, week 0), before the further laser treatments (week 2, 4 and 6) and at the final assessment (week 8) (Figure 1). All photographs were taken by one photographer with a Nikon D200 camera, under identical conditions of illumination and patient positioning.
2.4. Measurement of waist circumference and BFM
Waist circumference was determined in three different locations: 4, 8 and 12 cm above the anterior superior iliac spine. Measurements were performed at the same locations (Figure 1). Body fat was monitored by measuring bioelectric impedance with Omron BF 306 device (Omron Healthcare, UK).
2.5. Subcutaneous fat tissue thickness measurement by 2D B‐mode ultrasonography
The ultrasound (US) imaging was performed by an experienced radiologist. Image acquisition was performed in a standardized patient position (supine, relaxed, hands above head). A GE Logiq E9 US system was used, with the linear probe ML‐RS operated at 12 to 15 MHz (General Electric, GE Healthcare). Subcutaneous fat thickness measurements were performed on B‐mode scan in six standardized points. Thickness value was given in mm.
Each measurement was repeated five times and the average of the five values was used during comparison analysis. To avoid fat compression errors, the US probe was placed above a given site without any pressure and by using a thick layer of US gel between the probe and the skin.
2.6. Subcutaneous fat tissue stiffness measurement by shear wave elastography
The examination was performed by the same radiologist described above. The same US equipment with a L9 9 MHz probe was used to quantify tissue stiffness by measuring the speed of shear waves in tissues. As before, compression artifacts were avoided by using a thick layer of US gel between the probe and the skin. Fat tissue treated in the waist of the patient was visualized by US. Elasticity boxes were established in the center of the field of view. Shear‐wave elastography images were saved after a few seconds of immobilization to allow the shear‐wave elastography image to stabilize. The size of elasticity box was a minimum depth of 6 mm. For measurement, circular region of interest was generated inside of the elasticity box, and the stiffness was calculated in kPa. Elastographic measurements were repeated in 12 different points on both side of the patient treated waist. Data were displayed on an absolute scale. In order to reduce the variability of the repeated measurements, interquartile range (IQR) based outlier detection was performed in each case. The measurement values between Q1–1.5 IQR and Q3 + 1.5 IQR were considered as valid measurements and all the other values were treated as outliers. For before and after treatment comparison, the average of the valid measurements was calculated.
2.7. Subcutaneous tissue fat volume measurement by low‐dose CT
Low‐dose CT scan was performed using MEDISO ANYSCAN TRIO (Mediso Medical Imaging Systems, Hungary). The scanned region was from the anterior superior iliac spine to the hepatic dome. Field of view 500 × 500 mm, matrix 512 × 512, slice thickness of 2.5 mm, 120 keV, 46.67 mAs, 0.98 pixel per mm resolution. For quantitative assessment, the before and after treatment performed CTs were registered in each patients. The subcutaneous fat tissue was segmented on the reconstructed CT data automatically using an in‐house developed software and validated by visual inspection. The volume of the interest (VOI) was set manually in each case defining a 12‐cm wide region from the top of iliac bone. The volume of difference of the adipose tissue was calculated in ml inside the defined VOIs.
2.8. Statistical analysis
Statistical analysis was performed with the SigmaStat for Windows statistical software package (Jandel Scientific, Erkrath, Germany). The Shapiro‐Wilk test was used to check normality. In case of few parameters, the values obtained varied significantly from the pattern expected if the data were drawn from a population with normal distribution. Thus, non‐parametric method was chosen. The Wilcoxon signed‐rank test was applied to compare data obtained before and after the treatments and P < .05 was considered statistically significant.
3. RESULTS
3.1. Combined Nd: YAG/Er: YAG laser treatment significantly reduced waist circumference and total body fat
Photo documentation revealed a considerable improvement in visual appearance of the treated region (Figure 2).
Figure 2.
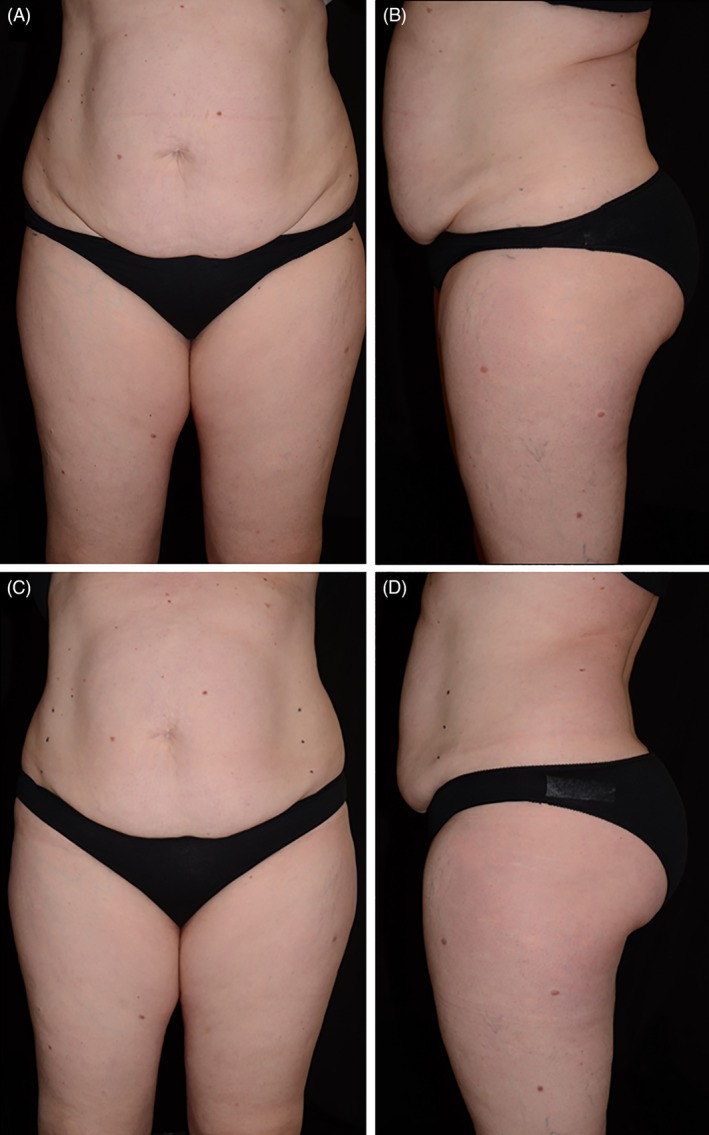
Comparative photographs of participant ID 4 before and after the treatments. A, The participant before the 1st combined laser treatment from frontwise. B, The participant before the 1st combined laser treatment from side view. C, The participant 2 weeks after the 4th treatment from frontwise. D, The participant 2 weeks after the 4th treatment from side view
The waist‐measurement confirmed this finding: after four laser treatments, the waist circumference showed a significant reduction as compared to the baseline values in all points of measurements (4, 8 and 12 cm above the spina iliaca anterior superior) (Figure 3).
Figure 3.
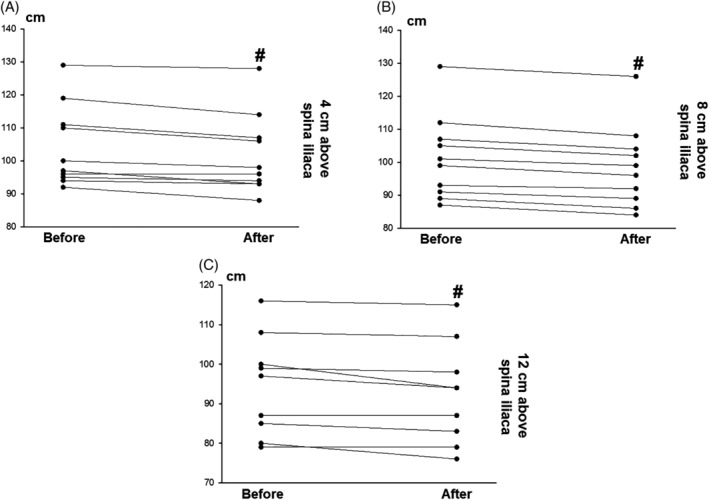
Findings of waist circumference measurements. “Before” values represent the status before the 1st laser treatment while “after” values were determined 2 weeks after the last treatment. Data of participants are depicted separately. Circumference values are given in cm. A, B and C demonstrate measurement points 4, 8 and 12 cm above the spina iliaca anterior superior, respectively. #, difference between “before” and “after” values is statistically significant
Furthermore, laser treatments resulted in a significant decrease of total body fat. Lower total body fat levels were measured in nine of the 10 participants after laser treatments than before them (Figure 4).
Figure 4.
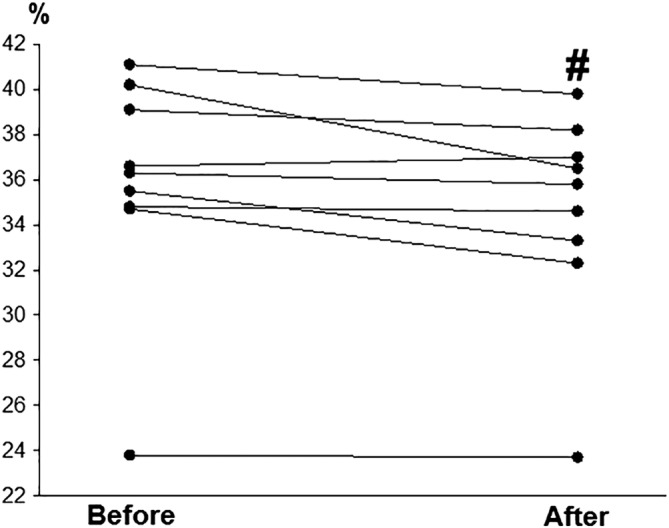
Total body fat. “Before” and “after” values demonstrate baseline values and the values measured 2 weeks after the 4th laser treatment, respectively. Data of participants are depicted separately. Total body fat values are given in percentage. #, difference between “before” and “after” values is statistically significant
3.2. According to the US measurements, combined Nd: YAG/Er: YAG laser treatment considerably decreased fat thickness and improved skin stiffness in the treated region
The fat tissue thickness, which was determined by means of US on B‐mode, decreased in each participant after the final combined laser therapy. The statistical analysis found a significant difference between “before” and “after” values (Figure 5). The elastography revealed tightening of the waist and the abdomen in all participants without exception. Two weeks after the fourth laser treatment, the affected area became smooth and tight. As compared with the baseline values, the difference was statistically significant. (Figure 6).
Figure 5.
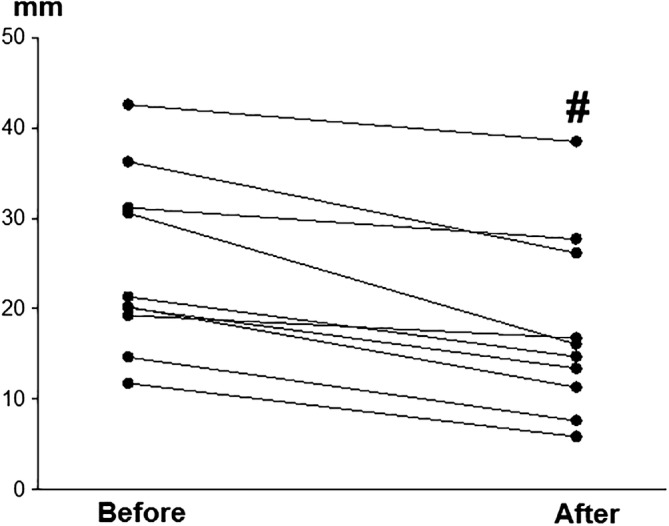
Mean subcutaneous fat measured with two‐dimensional B‐mode ultrasonography. “Before” values were determined before the 1st laser treatment while “after” values demonstrate the fat thickness 2 weeks after the 4th laser treatment. Data of participants are depicted separately. Fat thickness values are given in mm. #, difference between “before” and “after” values is significant
Figure 6.
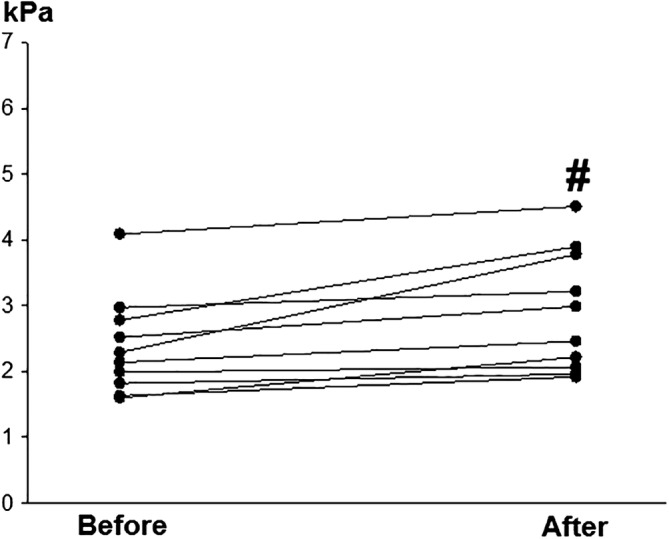
Subcutaneous fat tissue stiffness determined by means of shear wave elastography. “Before” values represent the status before the 1st laser treatment while “after” values were determined 2 weeks after the last treatment. Data of participants are depicted separately. Stiffness values are given in kPa. #, difference between “before” and “after” values is statistically significant
3.3. Subcutaneous fat volume, measured by low‐dose CT, displayed a moderate but not significant decrease in the waist region
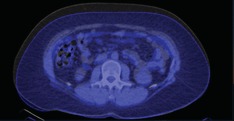
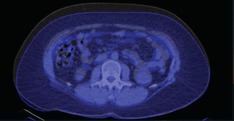
The volume of the subcutaneous fat in the treated region was determined by means of low‐dose CT before the first combined laser treatment and 2 weeks after the last one. In six participants, the treatments reduced the fat volume but in case of the remaining four participants, some increase was detected (Table 2). The statistical analysis did not reveal significant difference between the values before and after the treatments. However, [Link], [Link] demonstrates the changes in the adipose tissue of participant ID 5 who was found to be the most responsive participant.
Table 2.
Fat tissue volume before the first and 2 weeks after the last treatment (measured with low‐dose computer tomography)
| ID number | Fat tissue volume before treatment (mL) | Fat tissue volume after treatment (mL) | Results |
|---|---|---|---|
| 1 | 3078 | 3016 | ↓ |
| 2 | 1858 | 1971 | ↑ |
| 3 | 7419 | 7673 | ↑ |
| 4 | 3433 | 3272 | ↓ |
| 5 | 6114 | 5385 | ↓ |
| 6 | 2672 | 2753 | ↑ |
| 7 | 2150 | 2177 | ↑ |
| 8 | 1818 | 1777 | ↓ |
| 9 | 3041 | 3015 | ↓ |
| 10 | 3855 | 3159 | ↓ |
4. DISCUSSION
Non‐invasive body contouring procedures mean a quickly growing area of cosmetic interventions. Lasers play a prominent role in these techniques. The application area of LLLT is wide: it can be used to relieve pain, inflammation and edema and it may contribute to wound healing. Furthermore, it can be utilized to enhance the efficacy of liposuction and to diminish its complications but the technique alone is also useful for fat reduction 13, 18. Fat removal by LLLT may be performed via different mechanisms. It was suggested that LLLT leads to formation of transitory micropores which allow the release of intracellular lipids from adipocytes 17. It is also possible that production of reactive oxygen species 22 and complement activation 23 contribute to the process, as well. Moreover, LLLT can elevate the level of cAMP (via absorption laser light by mitochondrial chromophores) then cAMP stimulates cytoplasmic lipase resulting in transformation of triglycerides into fatty acids and glycerol 24, 25, 26. Application of lasers also increases the local temperature which reduces adipocyte viability 27.
The wavelengths utilized in our study have already been applied separately. It has been reported that use of 1060 nm diode laser leads to hyperthermic temperatures within the adipose tissue with subsequent lipolysis 28. Laser of 1064 nm generates thermal effect appropriate for lipolysis, as well 29. A pilot study has also described that treatment with 2940 nm Er:YAG laser results in effective reduction of perioral wrinkles and tightens the skin 30. Moreover, SMOOTH mode Er:YAG laser is an effective and safe method for the treatment of vaginal laxity 31. Thus, the benefit of combined use is that fat reduction and skin tightening may be achieved by the same treatment while other methods result in lipolysis only.
A case report has already been published on the efficacy of combined Er:YAG and Nd:YAG laser treatment for noninvasive body contouring. Superficial tightening of the skin was performed using 2940 nm Er:YAG pulse, combined with deep bulk heating of the skin to temperatures above 40°C, using few seconds long pulse 1064 nm Nd: YAG laser 21. This modality may be of benefit also when considering treatments that combine non‐ablative Nd:YAG laser skin remodeling with Er:YAG laser fractional skin resurfacing. Laser treatment is the safest when a laser pulse width can be chosen that is longer than the thermal relaxation time (TRT), TRTepi of the epidermis, but shorter than the TRTtarget of the treated skin target. New skin treatment possibilities with the Nd: YAG Laser allows selective heat treatment of the target without overheating the epidermis 32, 33. The 1064 nm wavelength has many advantages including its minimal absorption in the epidermis so it can be used on all skin types. This wavelength penetrates into the subcutaneous fat layers and provides bulk heating needed to destroy adipocytes.
Our results have confirmed these findings: the combined 1064 nm Nd:YAG and 2940 nm Er:YAG laser therapy is effective in reducing the circumference measurements, fat tissue volume of specifically treated regions, including the waist and lower part of abdomen. The effect of treatment improved the skin tightening for each participant. It is important to highlight the fact that we have not detected any complications. The participants tolerated the treatments well and did not report pain or any other symptoms of adverse effects.
Previously, the safety and efficacy of the various non‐invasive body shaping procedures were determined with comparative pre‐ and post‐treatment photography, circumferential measurements and ultrasonography. An important new aspect in our study is that we used the elastography to the representation of compactness of the fat tissue. Shear wave technique estimates tissue stiffness in real time and is quantitative and user independent. This technique provides useful information, for example, on liver diseases 34 and musculoskeletal disorders 35.
In our clinical study, we applied FOTONA device with TightSculpting method. This is a unique dual‐wavelength (1064 nm Nd,YAG, 2940 nm Er:YAG), nonablative laser treatment for sculpting and skin tightening which can be utilized on all body areas. The first step is deep tissue heating with the objective of skin tightening and fat reduction with PIANO pulse duration of the 1064 nm laser. The super long 1064 nm Nd:YAG pulse mode is designed for homogenous tissue heating comfortably, safely and rapidly without injury to the epidermis. Adipocyte destruction and collagen remodeling with exceptional results were found. The duration of the PIANO mode is much longer than the TRT of the epidermis. This is therefore the safest way for reaching deeper tissues, with minimal thermal effect on the epidermis. The PIANO mode pulse durations are also longer than the relaxation times of any other skin structures, such as hair follicles or blood vessels. The PIANO modality is thus indicated for overall homogeneous, bulk heating of the dermis and subcutaneous tissue.
The second step of treatment comprises a nonablative 2940 nm Er:YAG SMOOTH mode, appropriate for skin tightening. The intense and monitored surface tissue heating stimulates collagen remodeling and the Er:YAG laser treatment supports collagen production, therefore improves laxity and elasticity on the treated areas. The MatrixView temperature monitor ensures effective and controlled treatments with ultimate patient comfort and safety.
Owing to the described technical features, the treatment is almost painless and there appears to be no adverse events associated with combined Nd:YAG/Er:YAG laser. The treatment protocols determined for this study seem to be appropriate for future treatments and investigations.
In conclusion, the combined 1064 nm Nd:YAG and 2940 nm Er:YAG laser treatment for body shaping has proven to be a comfortable, safe and effective therapy for transdermal skin tightening and reduction of fat tissue. In combination with a healthy lifesytle, this TightSculpting method in body shaping represents a very promising non‐invasive alternative to laser lipolysis.
CONFLICT OF INTEREST
The equipment was loaned by FOTONA to the Department.
AUTHOR BIOGRAPHIES
Please see Supporting Information online.
Supporting information
Author Biographies
Video S1. Three‐dimensional (3D) computer tomography (CT) images of the waist. Registered 3D CT images of segmented subcutaneous adipose tissue of the waist. Yellow: before treatment, red: after treatment.
Video S2. Axial three‐dimensional computer tomography (CT) images. Axial images obtained by means of low‐dose CT from the abdominal region of participant ID 5. Registered CT slices in LII vertebral level. The baseline scan is gray, the repeated scan is blue.
Video S3. Coronal three‐dimensional computer tomography (CT) images. Coronal images obtained by means of low‐dose CT from the abdominal region of participant ID 5. The baseline scan is gray, the repeated scan is blue.
ACKNOWLEDGMENTS
The authors express their thanks to Dr. Anita Altmayer and Dr. Réka Németh for their useful suggestions, to Andrea Gyimesi, Szilvia László and Zsolt Hunyadi for the technical assistance and to Éva Dósa‐Rácz for her valuable contribution to the statistical analysis. This work was supported by EFOP 3.6.2.‐16‐2017‐00005 research grant.
Vas K, Besenyi Z, Urbán S, et al. Efficacy and safety of long pulse 1064 and 2940 nm lasers in noninvasive lipolysis and skin tightening. J. Biophotonics. 2019;12:e201900083 10.1002/jbio.201900083
REFERENCES
- 1. Hales C. M., Carrol M. D., Fryar C. D., Ogden C. L., NCHS Data Brief 2017, 288, 1. [PubMed] [Google Scholar]
- 2. Carbone S., Lavie C. J., Arena R., Mayo Clin. Proc. 2017, 92, 266. [DOI] [PubMed] [Google Scholar]
- 3. Alpert M. A., Lavie C. J., Agrawal H., Aggarwal K. B., Kumar S. A., Transl. Res. 2014, 164, 345. [DOI] [PubMed] [Google Scholar]
- 4. Klil‐Drori A. J., Azoulay L., Pollak M. N., Nat. Rev. Clin. Oncol. 2017, 14, 85. [DOI] [PubMed] [Google Scholar]
- 5. Duclos M., Ann. Phys. Rehabil. Med. 2016, 59, 157. [DOI] [PubMed] [Google Scholar]
- 6. Kennedy J., Verne S., Griffith R., Falto‐Aizpurua L., Nouri K., J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1679. [DOI] [PubMed] [Google Scholar]
- 7. Krueger N., Mai S. V., Luebberding S., Sadick N. S., Clin. Cosmet. Investig. Dermatol. 2014, 7, 201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Manstein D., Laubach H., Watanabe K., Farinelli W., Zurakowski D., Anderson R. R., Lasers Surg. Med. 2008, 40, 595. [DOI] [PubMed] [Google Scholar]
- 9. Moreno‐Moraga J., Valero‐Altés T., Riquelme A. M., Isarria‐Marcosi M. I., de la Torre J. R., Lasers Surg. Med. 2007, 39, 315. [DOI] [PubMed] [Google Scholar]
- 10. Fatemi A., Kane M. A., Aesthetic Plast. Surg. 2010, 34, 577. [DOI] [PubMed] [Google Scholar]
- 11. Fatemi A., Semin. Cutan. Med. Surg. 2009, 28, 257. [DOI] [PubMed] [Google Scholar]
- 12. Weiss R. A., Semin. Cutan. Med. Surg. 2013, 32, 9. [PubMed] [Google Scholar]
- 13. Avci P., Nyame T. T., Gupta G. K., Sadasivam M., Hamblin M. R., Lasers Surg. Med. 2013, 45, 349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Nestor M. S., Zarraga M. B., Park H., J. Clin. Aesthet. Dermatol. 2012, 5, 42. [PMC free article] [PubMed] [Google Scholar]
- 15. McRae E., Boris J., Lasers Surg. Med. 2013, 45, 1. [DOI] [PubMed] [Google Scholar]
- 16. Lach E., Pap S., Lasers Surg. Med. 2004, 34, S16. [Google Scholar]
- 17. Neira R., Arroyave J., Ramirez H., Ortiz C. L., Solarte E., Sequeda F., Gutierrez M. I., Plast. Reconstr. Surg. 2002, 110, 912. [DOI] [PubMed] [Google Scholar]
- 18. Montazeri K., Mokmeli S., Barat M., J. Lasers Med. Sci. 2017, 8, S22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Ali Y. H., Plast. Reconstr. Surg. Glob. Open 2018, 6, e1934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Wolfenson M., Hochman B., Ferreira L. M., Plast. Reconstr. Surg. 2015, 135, 1369. [DOI] [PubMed] [Google Scholar]
- 21. Gaspar A., J LA&HA 2015, 1, 48. [Google Scholar]
- 22. Chen A. C., Arany P. R., Huang Y. Y., Tomkinson E. M., Sharma S. K., Kharkwal G. B., Saleem T., Mooney D., Yull F. E., Blackwell T. S., Hamblin M. R., PLoS ONE 2011, 6, e22453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Caruso‐Davis M. K., Guillot T. S., Podichetty V. K., Mashtalir N., Dhurandhar N. V., Dubuisson O., Yu Y., Greenway F. L., Obes. Surg. 2011, 21, 722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Karu T. I., Photochem. Photobiol. 2008, 84, 1091. [DOI] [PubMed] [Google Scholar]
- 25. Karu T., Health Phys. 1989, 56, 691. [DOI] [PubMed] [Google Scholar]
- 26. Karu T. I., Afanas'eva N. I., Dokl. Akad. Nauk 1995, 342, 693. [PubMed] [Google Scholar]
- 27. Franco W., Kothare A., Ronan S. J., Grekin R. C., McCalmont T. H., Lasers Surg. Med. 2010, 42, 361. [DOI] [PubMed] [Google Scholar]
- 28. Schilling L., Saedi N., Weiss R., J. Drugs Dermatol. 2017, 16, 48. [PubMed] [Google Scholar]
- 29. DiBernardo B. E., Reyes J., Chen B., J. Cosmet. Laser Ther. 2009, 11, 62. [DOI] [PubMed] [Google Scholar]
- 30. Gaspar A., Gasti G. A., J LA&HA 2013, 2, 17. [Google Scholar]
- 31. Vizintin Z., Lukac M., Kazic M., Tettamanti M., Climacteric 2015, 18, 4. [DOI] [PubMed] [Google Scholar]
- 32. Lukac M., Vizintin Z., Pirnat S., Nemes K., J LA&HA 2011, 1, 22. [Google Scholar]
- 33. Marini L., J. Cosmet. Laser Ther. 2009, 11, 202. [DOI] [PubMed] [Google Scholar]
- 34. Kim J. R., Suh C. H., Yoon H. M., Lee J. S., Cho Y. A., Jung A. Y., Eur. Radiol. 2018, 28, 1175. [DOI] [PubMed] [Google Scholar]
- 35. Taljanovic M. S., Gimber L. H., Becker G. W., Latt L. D., Klauser A. S., Melville D. M., Gao L., Witte R. S., Radiographics 2017, 37, 855. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Author Biographies
Video S1. Three‐dimensional (3D) computer tomography (CT) images of the waist. Registered 3D CT images of segmented subcutaneous adipose tissue of the waist. Yellow: before treatment, red: after treatment.
Video S2. Axial three‐dimensional computer tomography (CT) images. Axial images obtained by means of low‐dose CT from the abdominal region of participant ID 5. Registered CT slices in LII vertebral level. The baseline scan is gray, the repeated scan is blue.
Video S3. Coronal three‐dimensional computer tomography (CT) images. Coronal images obtained by means of low‐dose CT from the abdominal region of participant ID 5. The baseline scan is gray, the repeated scan is blue.