

Abstract
The biological mechanisms through which physical activity reduces metastatic disease recurrence and mortality in cancer patients are not known. This review offers the hypothesis that physical activity reduces the risk of recurrence and mortality in cancer patients through two synergistic processes: 1) indirect (systemic) effects related to the host tumor microenvironment and; 2) direct (physical) effects on cancer cells.
Keywords: Disease Progression, Exercise, Microfluidics, Neoplastic Cells, Prognosis, Tumor Microenvironment
Summary
Physical activity may reduce the risk of metastatic disease recurrence and mortality in cancer patients through two synergistic processes.
INTRODUCTION
Despite having no evidence of distant metastases at diagnosis, a substantial proportion of patients with cancer will develop metastatic disease recurrence within five years of tumor resection (1). Metastatic (e.g., systemic) disease recurrence marks the transition from localized, potentially curable to disseminated, often incurable disease that accounts for 90% cancer deaths (2). An unmet clinical need exists to identify additional therapeutic strategies that can reduce the risk of systemic recurrence and mortality in this population.
The prescription of physical activity is a potential therapeutic strategy to reduce the risk of systemic recurrence and mortality in this population. Physical activity is defined as any bodily movement produced by skeletal muscle that requires energy expenditure (3). Observational prospective cohort studies report that physical activity is associated with a lower risk of systemic recurrence and mortality in patients diagnosed with several types of cancer. For example, among 2,987 women with stage I-III breast cancer, participation in physical activity after diagnosis was associated with a 24% reduction in disease recurrence and 45% reduction in mortality (4). Among 832 men and women with stage III colon cancer, participation in physical activity was associated with a 40% reduction in disease recurrence and 63% reduction in mortality (5). Importantly, these associations were independent of various demographic, clinical, pathological, and treatment related prognostic or confounding factors.
Despite the strength and consistency of these observational data, the biological mechanisms through which physical activity (or exercise) reduces the risk of systemic recurrence and mortality are not yet known. Prevailing hypotheses contend that the benefits of physical activity are attributable to systemic adaptations that occur within the host microenvironment, such as favorable changes in metabolic growth factors, inflammation, and immune function (6). These changes create a host tumor microenvironment that is insufficient for metastatic initiation and progression. However, mechanical forces are also implicated in metastatic initiation and progression (7). Microfluidic studies demonstrate that fluid shear stress, similar to that of vascular blood flood, directly affect cell viability, alter intracellular characteristics, retard growth rates, and attenuate the metastatic potential of circulating tumor cells (8, 9). Recently, a proof-of-concept study demonstrated that physical activity reduced circulating tumor cells in patients with resected stage I-III colon cancer (10). Collectively, these findings offer the rationale that physical activity may also have an effect on cancer cells through a direct physical mechanism, such as shear stress in the vasculature.
In this review, we propose a hypothesis that unifies historic research with contemporary discoveries. We explore the hypothesis that physical activity reduces the risk of systemic recurrence and mortality in cancer patients through two synergistic processes: 1) indirect (systemic) effects in the host tumor microenvironment and; 2) direct (physical) effects on cancer cells. The majority of research conducted in this area has included patients with breast and colorectal cancer, however we describe how this hypothesis may be applicable to other solid tumors. Elucidating the mechanisms through which physical activity reduces the risk of systemic recurrence and mortality is one of the most provocative unanswered questions in oncology. This review provides a rationale that will expand our thinking, foster constructive dialogue, and offer a stimulating premise on which to design future research to elucidate the biological mechanisms that link physical activity with cancer outcomes.
PHYSICAL ACTIVITY IS ASSOCIATED WITH CANCER RECURRENCE AND MORTALITY
One in ten cancer deaths is attributed to insufficient physical activity (11). Nearly two dozen observational prospective cohort studies have reported on the inverse association between participation in physical activity after diagnosis with cancer recurrence and mortality in patients with early stage malignancies of the breast, colorectum, and prostate. It is important to recognize that despite statistical adjustment for prognostic or confounding variables, a conservative interpretation of these data is essential since causality cannot be presumed. These data have been integrated into systematic reviews and meta-analyses (12, 13). Briefly, an analysis of eight studies that included 15,298 patients with breast, colorectal, and prostate cancer demonstrated that higher self-reported volumes of post-diagnosis physical activity was associated with a 45% reduction in the risk of cancer recurrence (Hazard Ratio (HR): 0.65, 95% Confidence Interval (CI): 0.56−0.75) (13). Furthermore, among 21 studies that included 38,560 patients, higher self-reported volumes of post-diagnosis physical activity was associated with a 37% reduction in cancer mortality (HR: 0.63, 95% CI: 0.54−0.73) (13). The patients who derive the largest clinical benefits from physical activity are those individuals who were physically inactive prior to diagnosis and increase their volume of physical activity after diagnosis (12). In a nationally-representative sample of cancer patients, 8% engaged in ≥150 minutes per week of objectively-measured moderate- to vigorous-intensity physical activity (14). Accordingly there is a potential opportunity to utilize the promotion of physical activity as a therapeutic strategy to improve outcomes after a diagnosis of cancer.
THE METASTATIC CASCADE AND PROGNOSTIC IMPLICATIONS
The dissemination of cancer cells from a primary tumor to distant organs is a complex process with sequential and concurrent events occurring throughout the metastatic cascade. Key steps include the shedding of cancer cells from the primary tumor, intravasation into the circulation, migration to distant organs, extravasation into the surrounding tissue, and initiation of growth and proliferation (15). Intravasation can occur in the form of single tumor cells or tumor clusters that are bound to other cells such as leukocytes, platelets, and proteins. The vasculature is an inhospitable environment because cancer cells become vulnerable to natural killer cell surveillance and destruction from the physical stress of the circulation. While in the circulation, tumor cells acquire immune protection though platelet coating and neutrophil clustering (16). Tumor cells must possess plasticity to adapt to a new microenvironment and may halt cell division to persist in a quiescent state until new mutations are acquired or the environmental conditions permit the re-initiation of proliferation (17). Detailed mechanistic descriptions of these complex processes are described (18).
As precursors to clinically detected and potentially lethal metastases, circulating tumor cell detection and quantification provides unique mechanistic insight for translational research. More than three-dozen platforms exist for the detection of tumor cells (19). The presence of circulating tumor cells is associated with systemic recurrence and mortality in a variety of types of solid tumors. For example, among 735 men and women with stage II and III colorectal cancer, the presence of ≥1 circulating tumor cell was associated with a three-fold higher risk of recurrence (HR: 3.02, 95% CI: 1.83−5.00) and nearly four-fold higher risk of mortality (HR: 3.84, 95% CI: 2.41−6.22) compared to individuals without a detectable circulating tumor cell (20). In a meta-analysis of 19 studies of 2,993 women with stage I-III breast cancer, the presence of ≥1 circulating tumor cell was associated with a nearly three-fold higher risk of recurrence (HR: 2.86, 95% CI: 2.19−3.75) and mortality (HR: 2.78, 95% CI: 2.22−3.48) compared to women without a detectable circulating tumor cell, and the timing of blood sampling (e.g., prior to, during, or after cancer therapy) did not substantively influence these results (21). Circulating tumor cells often decrease after treatment initiation and increase with disease progression and treatment resistance (22). Therefore circulating tumor cells are uniquely situated as a potential pharmacodynamic biomarker for clinical trials (23). The analysis of circulating tumor cells in peripheral blood—a liquid biopsy—may offer unique insights into the biological mechanisms through which physical activity reduces risk of systemic recurrence and mortality in cancer patients.
THE BIOLOGICAL MECHANISMS THAT LINK PHYSICAL ACTIVITY WITH CANCER REUCRRENCE AND MORTALITY
Overview
The biological mechanisms through which physical activity may reduce risk of systemic recurrence and mortality in cancer patients are a complex interaction of multiple theorized pathways(Figure 1). This interplay may be due, in part, to the poly-pharmacologic or pleiotropic effects of physical activity. To date most studies have focused on mechanisms related to the host tumor microenvironment, including metabolic growth factors, inflammation, and immunity, that are implicated in cancer cell growth and proliferation. Several of these mechanisms may be mediated by body composition, such as adiposity and muscle, which can also secrete their own factors, adipokines and myokines, respectively. Here, we briefly describe the data that support the importance of these mechanisms as they relate to physical activity and systemic recurrence and mortality.
Figure 1.
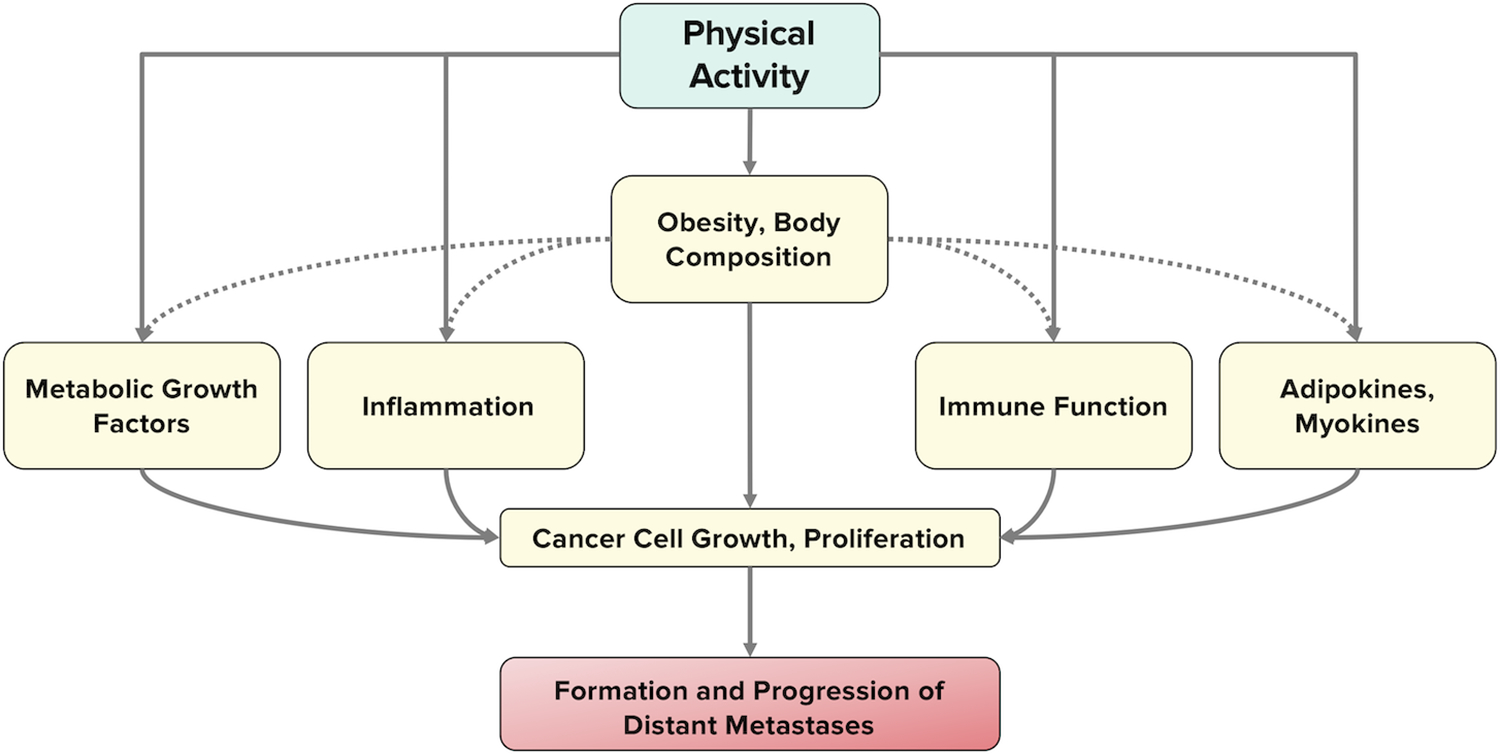
Hypothesized mechanisms underlying the association between physical activity and the development of systemic recurrence and mortality. The effects of physical activity may be mediated, in part, by body composition.
Metabolic Growth Factors
One of the most commonly studied mechanisms includes metabolic growth factors and insulin signaling. Cancer cells often overexpress the insulin receptor, which may explain why tumor cells have increased mitogenic sensitivity to hyperinsulinemia via activation of the PI3K-Akt-mTOR pathway (24). In a cohort of 512 women without known diabetes who had stage I-III breast cancer, independent of tumor and treatment-related factors, higher concentrations of fasting plasma insulin were associated with two-fold higher risk of distant recurrence (HR: 2.0, 95% CI: 1.2−3.3) and three-fold higher risk of mortality (HR: 3.1, 95% CI: 1.7−5.7) compared to the lowest concentrations of fasting plasma insulin (25). Among 373 men and women with stage I-III colorectal cancer, higher concentrations of C-peptide, a measure of insulin secretion, were independently associated with an increased risk of death (HR: 2.11, 95% CI: 1.06−4.21) compared to the lower concentrations of C-peptide (26). A meta-analysis of seven randomized controlled trials that included 369 women with stage I-III breast cancer demonstrated that physical activity reduced concentrations of fasting plasma insulin (−24.0 pmol/L, 95% CI: −41.5, −6.6) and these effects may be mediated by weight loss (27). A similar magnitude of reduction in fasting plasma insulin concentrations has been reported in a randomized controlled trial of men and women with stage I-III colon cancer (−28.0±31.2 pmol/L) and changes in insulin concentrations were correlated with changes in visceral adipose tissue area (r=0.37) (28).
Inflammation
Chronic low-grade systemic inflammation is considered a promoter of tumor progression, resulting from tumor associated macrophages that release cytokines and activate various pathways including PI3K-Akt-mTOR, JAK-STAT, and NF-kB to promote cell proliferation and survival (29). Circulating concentrations of acute-phase proteins of systemic inflammation, such as C-reactive protein, are associated with an increased risk of systemic recurrence and mortality in many solid tumors (30). Among 2,919 women with stage I-IIIA breast cancer, higher concentrations of C-reactive protein were associated with linearly proportional increases in breast cancer recurrence (HR: 1.13, 95% CI: 1.03−1.24) and mortality (HR: 1.19, 95% CI: 1.05−1.34) (31). The evaluation of the anti-inflammatory effects of physical activity is complicated by the observation that a single bout of activity often acutely increases inflammation, whereas chronic (e.g., long-term) physical activity causes a decrease in inflammation (32). Other measures of inflammation, such as GlycA, a biomarker of circulating N-linked glycoprotein acetyls have been linked with cancer risk and prognosis (33), and may offer complementary mechanistic insight into these complex pathways and their interactions with exercise. A pooled analysis of three randomized trials demonstrated that chronic muscle strengthening activity reduced C-reactive protein in 215 women with stage I-III breast cancer compared to control (34), and an ongoing randomized trial is evaluating the anti-inflammatory effects of 12 weeks of moderate-intensity aerobic activity in patients with stage III colon cancer ( NCT03975491).
Immune Function
In healthy adults, chronic moderate-intensity aerobic activity is associated with a variety of favorable changes to the innate immune and adaptive system, and an acute bout of moderate intensity aerobic exercise increases mobilization of natural killer cells, T cells, and B cells (35). The role of innate and adaptive immunity in cancer metabolism has long been appreciated, and the integration of the first generation of immune checkpoint inhibitors has rapidly transformed the landscape of oncology care (36). There is growing evidence that the peripheral and tumoral composition of immune cells is associated with both cancer risk and prognosis (37). In a cohort of 3,625 men and women, higher cytotoxic activity of peripheral blood lymphocytes was independently associated with a 36% lower risk of developing invasive cancer during 11 years of follow up (HR: 0.64, 95% CI: 0.44−0.94) (38). It is important to note that the cytotoxicity assay in this study was completed against a cell line from hematologic malignancy (chronic myeloid leukemia), whereas the majority of observed malignancies (n=154) were solid tumors (e.g., gastrointestinal and lung). A randomized trial in 53 patients with postmenopausal breast cancer demonstrated that moderate-intensity aerobic activity increased natural killer cell cytotoxic activity (6.8%, 95% CI: 0.4−13.3) (39), however other immune parameters were unchanged in this study and other clinical trials have not observed changes in lytic activity following exercise, which highlights the complexities of studying immune function and underscores the need for further studies.
Body Composition
Various measures of body composition have been associated with recurrence and mortality in patients with a several types of cancer. Among 3,262 men and women with stage I-III colorectal cancer, the combination of excess total adiposity and low muscle mass was associated with a 40% higher risk of mortality as compared to individuals without excess adiposity and sufficient muscle mass (HR: 1.40, 95% CI: 1.03−1.90) (40). Similar findings have been reported in stage II-III breast cancer (41). Randomized controlled trials have demonstrated that moderate-intensity aerobic activity reduces visceral (intra-abdominal) adiposity among patients with colon cancer, such that each 60 minute per week increase in aerobic activity reduces visceral adiposity by 2.7 cm2 (95% CI: −5.1, −0.1) (42) and muscle strengthening activity prevents the loss of appendicular lean mass among women with stage I-III breast cancer (0.07 kg/m2, 95% CI: 0.01−0.14) (43). It remains unclear if body composition serves as an intermediary to the above-described metabolic, inflammatory, and immune biological pathways or has a direct effect on cancer cells through secreted factors, such as adipokines and myokines.
Cancer Cell Response to Fluid Shear Stress
Experimental preclinical models of shear stress on circulating tumor cells demonstrate that mechanical forces influence the cancer cell viability. For example, in a colorectal adenocarcinoma cell line (COLO 225) using a cone-and-plate viscometer to provide a uniform and controlled shear rate, increasing fluid shear stress sensitized cancer cells to apoptosis (44). At a fixed duration of 120 minutes, shear stresses of 0.4, 1.0, and 2.0 dyn/cm2 induced cancer cell apoptosis, whereas shear stresses of 0.05 and 0.1 dyn/cm2 did not impact cell viability (44). At a fixed shear stress of 2.0 dyn/cm2, durations of shear stress exposure of 60, 90, and 120 minutes increased cell apoptosis, whereas durations of 10 and 30 minutes did not impact cell viability (44). These initial observations have been replicated in breast, ovarian, and lung cancer cell lines, however leukemia cells were more resistant to shear forces (45). The specific processes through which shear stress induces cancer cell apoptosis is under study, however hypotheses suggest that mechanosensitive receptors on cancer cell surface may induce cell cycle arrest (8).
Aerobic activity induces substantial increases in vascular shear stress (5.0−6.5 dyn/cm2) (46), and hypothesis-generating human studies have begun to document the potential importance of circulating tumor cells in the field of cancer metabolism. A randomized controlled trial explored the hypothesis that physical activity may reduce circulating tumor cells in 23 patients with resected stage I-III colon cancer who finished cancer treatment 9.0±6.1 months prior to trial enrollment (10). Patients were randomized to one of three groups: usual-care control, 150 minutes per week of aerobic activity (low-dose), and 300 minutes per week of aerobic activity (high-dose) for six months. Over six months, statistically significant decreases in circulating tumor cells were observed in the low-dose (−1.34±0.34 cells/mL) and high-dose (−1.18±0.40 cells/mL) groups, whereas no statistically significant change was observed in the control group (−0.59±0.56 cells/mL). Additional analyses demonstrated that reductions in body mass index, fasting plasma insulin, and Intercellular Adhesion Molecule 1 (ICAM-1) concentrations may partially mediate the association between exercise and circulating tumor cell count. ICAM-1 is an endothelial cell molecule that is expressed on immune cells and tumor cells, and that along with its ligand LFA-1 (CD11a/CD18) is also implicated with cell adhesion and extravasation (47). A confirmatory study is underway to replicate the novel observation that exercise reduces circulating tumor cells ( NCT03975491) in patients with stage III colon cancer.
THE NEXT FRONTIER OF A UNIFIED HYPOTHESIS
On the basis of the above-described data, we hypothesize that physical activity reduces the risk of systemic recurrence and mortality in cancer patients through two synergistic processes: 1) indirect (systemic) effects related to the host tumor microenvironment and; 2) direct (physical) effects on cancer cells (Figure 2). For cancer cells that have intravasated into the circulation, physical activity may reduce the proportion of cancer cells available to extravasate into distant organs. This may occur by inducing apoptosis via exercise-induced shear stress that is sensed by mechanoreceptors on the cancer cell surface. For cancer cells that have not succumb to shear stress or have already extravasated into distant organs, physical activity may reduce the abundance of growth factors (e.g., insulin) and increase immunosurveillance within the host tumor microenvironment to prevent or slow the formation or progression of metastatic foci. If physical activity favorably impacts both of the major phases of metastasis—physical translocation of a cancer cell and distant colonization—such a therapy may be poised to offer durable clinical benefits to patients.
Figure 2.
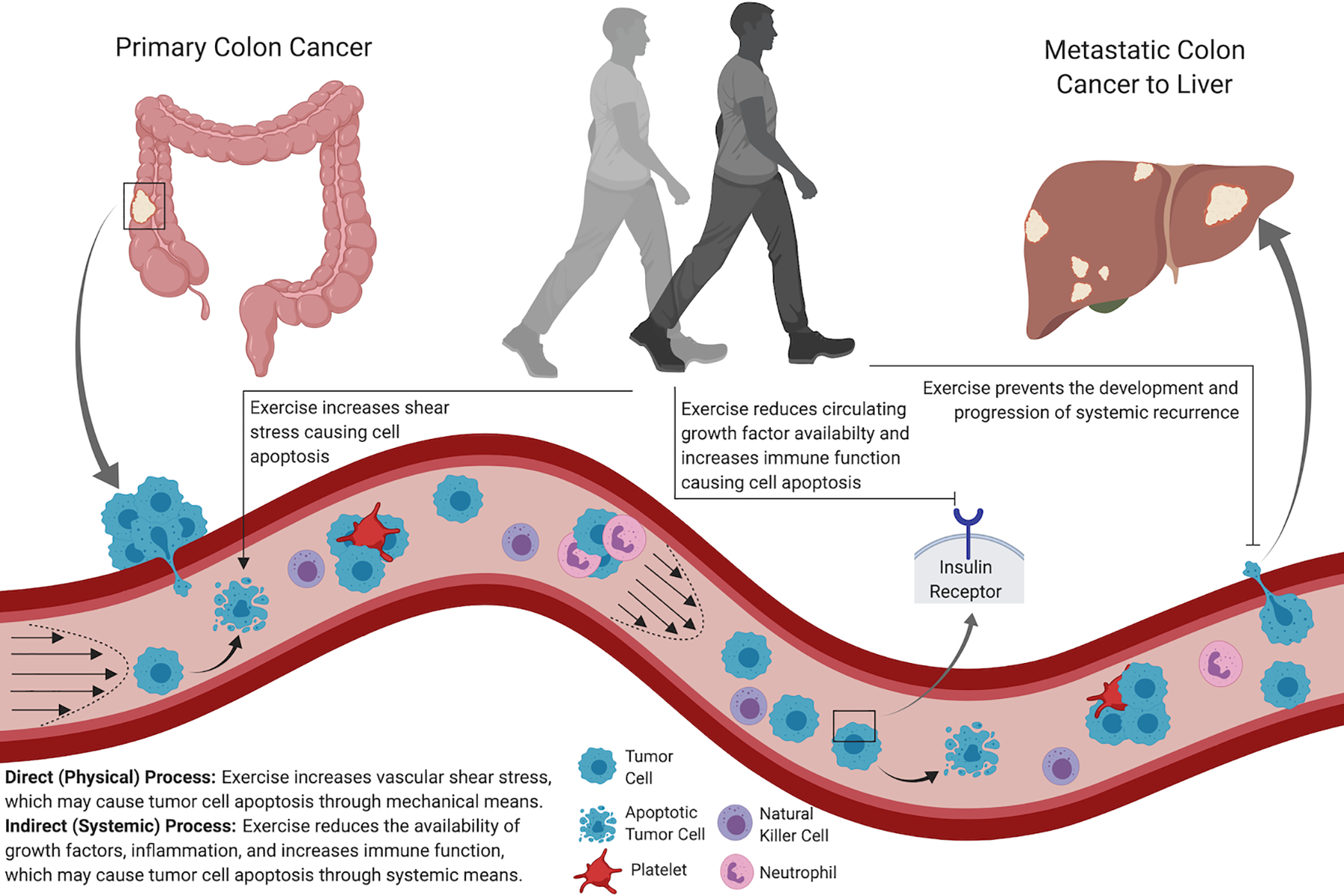
Hypothesis that physical activity reduces the risk of recurrence and mortality in cancer patients through two synergistic processes: 1) indirect (systemic) effects related to the host tumor microenvironment and; 2) direct (physical) effects on cancer cells.
Additional research is needed to empirically evaluate this hypothesis. First, identifying the source of tumor cells in patients who have completed treatment for early stage cancer is a critical next step to bolster the evidence to support this hypothesis. In patients with early stage cancer, it is unknown if tumor cells were shed from the primary tumor prior to surgical resection or are from established distant micro-metastatic foci that are not yet clinically identified. Second, the field has mostly focused on the chronic (e.g., long-term or longitudinally accrued) benefits of physical activity; a dearth of research has examined the acute effects of physical activity on mechanisms that are hypothesized to be related to systemic recurrence and mortality. Moreover, few randomized studies have systematically evaluated the comparative efficacy of different exercise modes, volumes, and frequencies on endpoints that are unique to cancer patients. Studies of exercise in this population should build upon the robust foundation of exercise science in healthy populations, not simply seek to replicate what is known and considered generalizable across health conditions. Third, given the poly-pharmacologic or pleiotropic effects of physical activity, systems biology approaches may accelerate the rate of discovery in this area. Fourth, examining the comparative effects of reducing tumor cells through mechanical forces using physical activity versus altering the tumor microenvironment exclusively, for example using weight loss, would provide evidence to evaluate this hypothesis. Exercise and weight loss may possess synergistic effects to reduce tumor cells through the combined effects of mechanical forces from exercise and changes in the host tumor microenvironment from weight loss. Similar hypothesis can be tested with pharmacological therapies, such as aspirin to reduce platelet and tumor cell aggregation to diminish the mechanical efficiency of extravasation, or metformin to reduce fasting plasma insulin to restrict growth factor availability. When circulating tumor cells undergo apoptosis, circulating tumor DNA is released (48), and understanding the effects of exercise on circulating tumor DNA may offer additional mechanistic insight.
The Food and Drug Administration (FDA) recently approved pembrolizumab, a programmed cell death ligand 1 inhibitor, for the treatment of adult and pediatric patients with unresectable or metastatic, microsatellite-instability-high or mismatch-repair-deficient solid tumors, regardless of tumor site or histology (49). This is the first time the FDA has approved a tissue- and site-agnostic anti-cancer therapy. With a continued understanding of tumor biology, the field of exercise science may soon be poised to conduct studies that target specific signaling pathways that are implicated across multiple tumor sites (e.g., tissue- and site-agnostic exercise clinical trials). If feasible in exercise science, such a transformative paradigm would accelerate our understanding of the cancer specific benefits of exercise in a time- and cost-efficient manner.
Randomized Trials with Clinical Disease Endpoints
Despite observational data and enthusiasm from translational scientists to elucidate potential biological mechanisms, the causality of the relationship between physical activity and systemic recurrence and mortality in cancer patients has not yet been proven. Several ongoing multicenter randomized trials will determine if physical activity improves clinical outcomes in patients with several types and stages of cancer. The Colon Health and Life-Long Exercise Change (CHALLENGE) trial will examine the effects of a 36-month aerobic exercise program on disease-free survival in 962 patients with high risk stage II or stage III colon cancer ( NCT00819208). The Intense Exercise for Survival among Men with Metastatic Castrate-Resistant Prostate Cancer (INTERVAL-GAP4) trial will examine the effects of a 24-month resistance and combinations of high-intensity interval training and moderate-intensity continuous aerobic exercise program on overall survival in 866 men with stage IV prostate cancer ( NCT02730338). The Lifestyle Intervention for Ovarian Cancer Enhanced Survival (LIVES) trial will examine the effects of a 24-month low-fat diet and ambulatory activity goal of 10,000 steps per day on progression-free survival in 1,024 women with stage II-IV ovarian cancer ( NCT00719303). In addition to offering a definitive test of causality of physical activity on clinical outcome, all of these studies include robust correlative studies that will provide additional mechanistic insight to the underlying biological processes that explain the beneficial effects of physical activity. It is critical that these phase III trial aim to validate surrogate biomarker endpoints and quantify the minimally clinically important differences for the above-described biomarkers.
LIMITATIONS
There are potential limitations to this hypothesis. The primary consideration relates to the timing of the development of systemic recurrence in cancer. It is probable that for some patients at the time of diagnosis of early stage cancer some tumor cells have already extravasated into distant organs but are not yet clinically detectable. Although it is often assumed that individual metastases are seeded exactly once by a single cancer cell or a small cluster of cancer cells, recent studies have demonstrated that under typical conditions, 10−150 cancer cells seed each metastasis (50). Therefore even if several tumor cells have seeded a metastatic site at the time of diagnosis, engaging in physical activity after initial diagnosis may prevent, delay, or interrupt continued seeding of tumor cells to the distant metastatic site. Moreover, even among patients with overt metastatic cancer (e.g., measurable lung and liver lesions), longitudinal declines in the number of circulating tumor cells are associated with improved prognosis when compared to patients with stable but persistently elevated or longitudinally increasing numbers of circulating tumor cells (22).
CONCLUSIONS
This review outlines the evidence to propose the hypothesis that the biological mechanisms through which physical activity prevents systemic cancer recurrence and modulates mortality rates occurs through two synergistic processes: 1) indirect (systemic) effects related to the host tumor microenvironment and; 2) direct (physical) effects on cancer cells. It is envisioned that this review: 1) provides a rationale to expand our thinking; 2) fosters constructive and transdisciplinary dialogue; and 3) offers a stimulating premise on which to design future research to elucidate the biological mechanisms that link physical activity with cancer outcomes, towards the goal of developing therapeutic strategies that are proven to reduce the morbidity and mortality associated with cancer.
Key Points.
Many cancer patients will develop metastatic disease recurrence. Metastatic disease accounts for 90% of all cancer deaths. Additional therapeutic strategies are needed to improve outcomes in this population.
Observational studies report that participation in physical activity after diagnosis of early stage cancer is associated with a reduction in the risk of metastatic disease recurrence and mortality. However, the biological mechanisms that underpin this association are not yet known.
To date, research has focused on how physical activity can favorably alter the host tumor microenvironment to reduce cancer cell growth and proliferation. However, mechanical forces are also implicated in metastatic initiation and progression. Physical activity may have an effect on cancer cells though mechanical forces.
This review provides a rationale that will expand our thinking, foster constructive dialogue, and offer a stimulating premise on which to design future research to elucidate the biological mechanisms that link physical activity with cancer outcomes.
Acknowledgements
Figure 2 was created by the authors using Biorender.com software.
Footnotes
Conflicts of Interest: Justin Brown reports grants from the American College of Sports Medicine, American Institute for Cancer Research, and the National Institutes of Health that were paid to his institution. Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under Award Number R00CA218603 (JCB) and R25CA203650 (JCB), the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number KL2TR003097 (LAG), and the National Institute of General Medicine Sciences of the National Institutes of Health under Award Number U54GM104940 (JCB and LAG). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The funding agency had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; and decision to submit the manuscript for publication.
References
- 1.Pantel K, Alix-Panabieres C. Liquid biopsy and minimal residual disease - latest advances and implications for cure. Nat Rev Clin Oncol. 2019;16(7):409–24. [DOI] [PubMed] [Google Scholar]
- 2.Chaffer CL, Weinberg RA. A perspective on cancer cell metastasis. Science. 2011;331(6024):1559–64. [DOI] [PubMed] [Google Scholar]
- 3.Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100(2):126–31. [PMC free article] [PubMed] [Google Scholar]
- 4.Holmes MD, Chen WY, Feskanich D, Kroenke CH, Colditz GA. Physical activity and survival after breast cancer diagnosis. JAMA. 2005;293(20):2479–86. [DOI] [PubMed] [Google Scholar]
- 5.Meyerhardt JA, Heseltine D, Niedzwiecki D et al. Impact of physical activity on cancer recurrence and survival in patients with stage III colon cancer: findings from CALGB 89803. J Clin Oncol. 2006;24(22):3535–41. [DOI] [PubMed] [Google Scholar]
- 6.Ballard-Barbash R, Friedenreich CM, Courneya KS, Siddiqi SM, McTiernan A, Alfano CM. Physical activity, biomarkers, and disease outcomes in cancer survivors: a systematic review. J Natl Cancer Inst. 2012;104(11):815–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mierke CT. The fundamental role of mechanical properties in the progression of cancer disease and inflammation. Rep Prog Phys. 2014;77(7):076602. [DOI] [PubMed] [Google Scholar]
- 8.Mitchell MJ, King MR. Computational and experimental models of cancer cell response to fluid shear stress. Front Oncol. 2013;3:44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jain RK, Martin JD, Stylianopoulos T. The role of mechanical forces in tumor growth and therapy. Annu Rev Biomed Eng. 2014;16:321–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Brown JC, Rhim AD, Manning SL et al. Effects of exercise on circulating tumor cells among patients with resected stage I-III colon cancer. PLoS One. 2018;13(10):e0204875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.van Dam RM, Li T, Spiegelman D, Franco OH, Hu FB. Combined impact of lifestyle factors on mortality: prospective cohort study in US women. BMJ. 2008;337:a1440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Schmid D, Leitzmann MF. Association between physical activity and mortality among breast cancer and colorectal cancer survivors: a systematic review and meta-analysis. Ann Oncol. 2014;25(7):1293–311. [DOI] [PubMed] [Google Scholar]
- 13.Friedenreich CM, Neilson HK, Farris MS, Courneya KS. Physical Activity and Cancer Outcomes: A Precision Medicine Approach. Clin Cancer Res. 2016;22(19):4766–75. [DOI] [PubMed] [Google Scholar]
- 14.Thraen-Borowski KM, Gennuso KP, Cadmus-Bertram L. Accelerometer-derived physical activity and sedentary time by cancer type in the United States. PLoS One. 2017;12(8):e0182554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chambers AF, Groom AC, MacDonald IC. Dissemination and growth of cancer cells in metastatic sites. Nat Rev Cancer. 2002;2(8):563–72. [DOI] [PubMed] [Google Scholar]
- 16.Szczerba BM, Castro-Giner F, Vetter M et al. Neutrophils escort circulating tumour cells to enable cell cycle progression. Nature. 2019;566(7745):553–7. [DOI] [PubMed] [Google Scholar]
- 17.Joosse SA, Gorges TM, Pantel K. Biology, detection, and clinical implications of circulating tumor cells. EMBO Mol Med. 2015;7(1):1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lambert AW, Pattabiraman DR, Weinberg RA. Emerging Biological Principles of Metastasis. Cell. 2017;168(4):670–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ferreira MM, Ramani VC, Jeffrey SS. Circulating tumor cell technologies. Mol. Oncol 2016;10(3):374–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Iinuma H, Watanabe T, Mimori K et al. Clinical significance of circulating tumor cells, including cancer stem-like cells, in peripheral blood for recurrence and prognosis in patients with Dukes’ stage B and C colorectal cancer. J Clin Oncol. 2011;29(12):1547–55. [DOI] [PubMed] [Google Scholar]
- 21.Zhang L, Riethdorf S, Wu G et al. Meta-analysis of the prognostic value of circulating tumor cells in breast cancer. Clin Cancer Res. 2012;18(20):5701–10. [DOI] [PubMed] [Google Scholar]
- 22.Hayes DF, Cristofanilli M, Budd GT et al. Circulating tumor cells at each follow-up time point during therapy of metastatic breast cancer patients predict progression-free and overall survival. Clin Cancer Res. 2006;12(14 Pt 1):4218–24. [DOI] [PubMed] [Google Scholar]
- 23.Devriese LA, Voest EE, Beijnen JH, Schellens JH. Circulating tumor cells as pharmacodynamic biomarker in early clinical oncological trials. Cancer Treat Rev. 2011;37(8):579–89. [DOI] [PubMed] [Google Scholar]
- 24.Belfiore A, Malaguarnera R. Insulin receptor and cancer. Endocr Relat Cancer. 2011;18(4):R125–47. [DOI] [PubMed] [Google Scholar]
- 25.Goodwin PJ, Ennis M, Pritchard KI et al. Fasting insulin and outcome in early-stage breast cancer: results of a prospective cohort study. J Clin Oncol. 2002;20(1):42–51. [DOI] [PubMed] [Google Scholar]
- 26.Wolpin BM, Meyerhardt JA, Chan AT et al. Insulin, the insulin-like growth factor axis, and mortality in patients with nonmetastatic colorectal cancer. J Clin Oncol. 2009;27(2):176–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kang DW, Lee J, Suh SH, Ligibel J, Courneya KS, Jeon JY. Effects of Exercise on Insulin, IGF Axis, Adipocytokines, and Inflammatory Markers in Breast Cancer Survivors: A Systematic Review and Meta-analysis. Cancer Epidemiol Biomarkers Prev. 2017;26(3):355–65. [DOI] [PubMed] [Google Scholar]
- 28.Brown JC, Rickels MR, Troxel AB et al. Dose-response effects of exercise on insulin among colon cancer survivors. Endocr Relat Cancer. 2018;25(1):11–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Coussens LM, Werb Z. Inflammation and cancer. Nature. 2002;420(6917):860–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Shrotriya S, Walsh D, Bennani-Baiti N, Thomas S, Lorton C. C-Reactive Protein Is an Important Biomarker for Prognosis Tumor Recurrence and Treatment Response in Adult Solid Tumors: A Systematic Review. PLoS One. 2015;10(12):e0143080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Villasenor A, Flatt SW, Marinac C, Natarajan L, Pierce JP, Patterson RE. Postdiagnosis C-reactive protein and breast cancer survivorship: findings from the WHEL study. Cancer Epidemiol Biomarkers Prev. 2014;23(1):189–99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ploeger HE, Takken T, de Greef MH, Timmons BW. The effects of acute and chronic exercise on inflammatory markers in children and adults with a chronic inflammatory disease: a systematic review. Exerc. Immunol. Rev 2009;15:6–41. [PubMed] [Google Scholar]
- 33.Chandler PD, Akinkuolie AO, Tobias DK et al. Association of N-Linked Glycoprotein Acetyls and Colorectal Cancer Incidence and Mortality. PLoS One. 2016;11(11):e0165615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Winters-Stone KM, Wood LJ, Stoyles S, Dieckmann NF. The Effects of Resistance Exercise on Biomarkers of Breast Cancer Prognosis: A Pooled Analysis of Three Randomized Trials. Cancer Epidemiol Biomarkers Prev. 2018;27(2):146–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Duggal NA, Niemiro G, Harridge SDR, Simpson RJ, Lord JM. Can physical activity ameliorate immunosenescence and thereby reduce age-related multi-morbidity? Nat Rev Immunol. 2019;19(9):563–72. [DOI] [PubMed] [Google Scholar]
- 36.Ribas A, Wolchok JD. Cancer immunotherapy using checkpoint blockade. Science. 2018;359(6382):1350–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Idorn M, Hojman P. Exercise-Dependent Regulation of NK Cells in Cancer Protection. Trends Mol. Med 2016;22(7):565–77. [DOI] [PubMed] [Google Scholar]
- 38.Imai K, Matsuyama S, Miyake S, Suga K, Nakachi K. Natural cytotoxic activity of peripheral-blood lymphocytes and cancer incidence: an 11-year follow-up study of a general population. Lancet. 2000;356(9244):1795–9. [DOI] [PubMed] [Google Scholar]
- 39.Fairey AS, Courneya KS, Field CJ, Bell GJ, Jones LW, Mackey JR. Randomized controlled trial of exercise and blood immune function in postmenopausal breast cancer survivors. J Appl Physiol (1985). 2005;98(4):1534–40. [DOI] [PubMed] [Google Scholar]
- 40.Caan BJ, Meyerhardt JA, Kroenke CH et al. Explaining the Obesity Paradox: The Association between Body Composition and Colorectal Cancer Survival (C-SCANS Study). Cancer Epidemiol Biomarkers Prev. 2017;26(7):1008–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Caan BJ, Cespedes Feliciano EM, Prado CM et al. Association of Muscle and Adiposity Measured by Computed Tomography With Survival in Patients With Nonmetastatic Breast Cancer. JAMA Oncol. 2018;4(6):798–804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Brown JC, Zemel BS, Troxel AB et al. Dose-response effects of aerobic exercise on body composition among colon cancer survivors: a randomised controlled trial. Br J Cancer. 2017;117(11):1614–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Brown JC, Schmitz KH. Weight lifting and appendicular skeletal muscle mass among breast cancer survivors: a randomized controlled trial. Breast Cancer Res Treat. 2015;151(2):385–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Mitchell MJ, King MR. Fluid Shear Stress Sensitizes Cancer Cells to Receptor-Mediated Apoptosis via Trimeric Death Receptors. New J Phys. 2013;15(1):015008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Regmi S, Fu A, Luo KQ. High Shear Stresses under Exercise Condition Destroy Circulating Tumor Cells in a Microfluidic System. Sci Rep. 2017;7:39975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Taylor CA, Cheng CP, Espinosa LA, Tang BT, Parker D, Herfkens RJ. In vivo quantification of blood flow and wall shear stress in the human abdominal aorta during lower limb exercise. Ann Biomed Eng. 2002;30(3):402–8. [DOI] [PubMed] [Google Scholar]
- 47.Reina M, Espel E. Role of LFA-1 and ICAM-1 in Cancer. Cancers (Basel). 2017;9(11). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Corcoran RB, Chabner BA. Application of Cell-free DNA Analysis to Cancer Treatment. N Engl J Med. 2018;379(18):1754–65. [DOI] [PubMed] [Google Scholar]
- 49.Lemery S, Keegan P, Pazdur R. First FDA Approval Agnostic of Cancer Site - When a Biomarker Defines the Indication. N Engl J Med. 2017;377(15):1409–12. [DOI] [PubMed] [Google Scholar]
- 50.Heyde A, Reiter JG, Naxerova K, Nowak MA. Consecutive seeding and transfer of genetic diversity in metastasis. Proc. Natl. Acad. Sci. U. S. A 2019;116(28):14129–37. [DOI] [PMC free article] [PubMed] [Google Scholar]