

Abstract
Intimate partner violence (IPV) victimization is a strong predictor of women’s sexual risk behavior. Social disconnection may be central to understanding this association. In a sample of 204 IPV victims, we (a) evaluated the extent to which social disconnection underlies the association between IPV severity and sexual risk behavior, and (b) tested the idea that the association between social disconnection and sexual risk behavior is stronger among women without alternative means to social connection (i.e., lack close friendships). The indirect effect of physical and sexual IPV, respectively, on sexual risk behavior via social disconnection was significant. The number of close friends women had moderated the association between social disconnection and sexual risk behavior, such that having multiple close friendships buffered the effects of social disconnection.
Keywords: intimate partner violence, sexual risk behavior, social disconnection, friends
Women’s intimate partner violence (IPV) victimization is one of the strongest predictors of their engagement in sexual risk behavior, including having unprotected sex with partners of unknown or positive HIV/STI status (Golder & Logan, 2011; Mittal, Senn, & Carey, 2011; Seth, Raiford, Robinson, Wingood, & DiClemente, 2010). Women with (vs. without) a history of victimization are more likely to engage in sexual risk behavior even when accounting for demographic characteristics and other unhealthy behaviors (e.g., smoking, heavy drinking; Breiding, Black, & Ryan, 2008; Centers for Disease Control and Prevention, 2014). Although both cross-sectional and longitudinal research provide support for the IPV sexual risk association (Campbell & Soeken, 1999; Gidycz, Orchowski, King, & Rich, 2008; Lang et al., 2011), the underlying mechanisms are not fully understood. One mechanism that may be central is women’s social disconnection, defined by a perception of loneliness or lack of social connection, which is often unrelated to the actual size of one’s social network (Cacioppo & Patrick, 2008; Lee & Robbins, 1995). In the current study, we posit that victimization has the potential to disrupt interpersonal functioning (Arriaga & Schkeryantz, 2015; Macmillan, 2001) leading to experiences of social disconnection. Under certain circumstances, sexual risk behavior may fulfill women’s goals to achieve social connection (Cooper, Shapiro, & Powers, 1998; Rawn & Vohs, 2011). Thus, we test a model rooted in social psychological theory to (a) evaluate the extent to which social disconnection mediates the association between IPV severity and sexual risk behavior, and (b) test the idea that the association between social disconnection and sexual risk behavior is stronger among women without alternative means to social connection (i.e., lack close friendships).
There are several limitations of previous research linking women’s IPV victimization to sexual risk behavior that impede understanding of the underlying social processes. The association between IPV victimization and sexual risk behavior is often reported as an empirical finding without extensive theoretical explanation of the underlying processes, therefore necessitating additional research that provides further insight into the mechanisms underlying this phenomenon. First, the research often considers the mechanisms for different risk behaviors (e.g., substance use, sexual risk behavior) jointly rather than evaluating mechanisms that are specific to sexual risk behavior. Further, most research has focused on understanding the role of only one type of victimization (e.g., distortion of sex-related cognitions subsequent to sexual victimization; Noll, Trickett, & Putnam, 2003; Zurbriggen & Freyd, 2004). Although the association between sexual victimization and sexual risk behavior is robust (Gidycz et al., 2008; Lang et al., 2011), research has shown that physical and psychological IPV are also relevant to sexual risk behavior (Davis, Combs-Lane, & Jackson, 2002; Golder & Logan, 2011). This suggests that various types of victimization, not just solely sexual victimization, impacts the way women approach interpersonal and sexual relationships.
Although there are a multitude of well-known psychological and physical health consequences of IPV (Campbell et al., 2002; Coker, Davis, et al., 2002), there are also noteworthy social health consequences that are comparatively less understood (Arriaga & Schkeryantz, 2015; Macmillan, 2001). Specific to intimate relationships, individuals expect for their partners to fulfill important needs such as connection, intimacy, and support (Cox, Buhr, Owen, & Davidson, 2016; Feeney & Collins, 2015; Mikulincer & Shaver, 2007). However, IPV may not fulfill these important expectations and result in unanticipated harm (Arriaga & Schkeryantz, 2015), which may manifest as feelings of rejection, loneliness, and social disconnection (Cullerton-Sen & Crick, 2005; Macmillan, 2001).
Social disconnection, in turn, may lead to engagement in risky behaviors, including sexual risk behavior (Twenge, Catanese, & Baumeister, 2002; Woerner, Kopetz, Lechner, & Lejuez, 2016). Research suggests that sexual behavior is best understood in terms of the goals that it fulfills (Cooper et al., 1998; Kopetz & Orehek, 2015). Given that people have a fundamental need to belong (Baumeister & Leary, 1995), women who feel socially disconnected may be particularly motivated to engage in behaviors that facilitate social connection (Maner, DeWall, Baumeister, & Schaller, 2007)—even at the expense of health and safety (Cooper et al., 1998; Kopetz & Orehek, 2015; Rawn & Vohs, 2011). Specifically, women who have experienced IPV may attempt to fill their needs for social connection through sexual relationships. This could include sex with casual partners, which may be important for women who desire social connection without the component of emotional intimacy (Cooper et al., 1998). It is important to note that although these social connection goals may be conscious and explicit, this is not requisite; extensive research has shown that both consciously and nonconsciously activated goals can guide behavior (Aarts & Dijksterhuis, 2000; Gollwitzer & Bargh, 2005; Webb & Sheeran, 2006).
Sexual risk behavior also might occur within one’s intimate relationship, with the partner who perpetrated the IPV. This includes situations in which a woman’s partner is engaging in sexual behavior with other partners outside the relationship, or his HIV/STI status is positive or unknown. In this context, social connection goals still may be central to understanding sexual risk behavior. Research suggests that IPV occurs, on average, during one-third of days in abusive relationships (Sullivan, McPartland, Armeli, Jaquier, & Tennen, 2012), and victims report many positive aspects of the relationship when IPV is not occurring (Enander, 2011; Rhatigan & Axsom, 2006). Thus, sexual risk behavior with one’s partner may often reflect an attempt to maintain or restore these positive aspects of the relationship, including feelings of social connection (Cooper et al., 1998; Jacques-Tiura et al., 2015; Purdie & Downey, 2000; Rawn & Vohs, 2011). It is important to note that women may also engage in sexual risk behavior with their partner in order to avoid further violence and harm to the relationship (El-Bassel, Gilbertl, Rajah, Foleno, & Frye, 2000; Maman, Campbell, Sweat, & Gielen, 2000)—although addressing this potential pathway is beyond the scope of the current study. For example, fear of physical IPV in particular may prevent women from asking partners to wear a condom (El-Bassel et al., 2000; Maman et al., 2000).
Although sexual behavior is one possible way to facilitate social connection, there are alternative ways to attain social connection goals. Specifically, women who feel disconnected as a result of IPV might seek out social interactions and comfort from friends and other support figures. Consistent with this notion, a multitude of studies have indicated that social support buffers the detrimental effects of IPV on psychological, physical, and social well-being (e.g., Beeble, Bybee, Sullivan, & Adams, 2009; Coker, Smith et al., 2002; Coker, Watkins, Smith, & Brandt, 2003). However, many women lack such a support network, or this network may become increasingly difficult to maintain as they remain in an abusive relationship for an extended duration (Goodman & Smyth, 2011; Levendosky et al., 2004). Thus, sexual risk behavior should be more likely to occur when women do not have other means to socially connect (i.e., they lack close friends for social support).
In the current study, the ideas outlined above are assessed in a sample of women who have experienced IPV in their current relationship. We first test the hypothesis that social disconnection mediates the association between IPV severity and sexual risk behavior. Next, we assess the extent to which women’s number of close friends moderates the relationship between social disconnection and sexual risk behavior. We hypothesize that having alternative means to social connection (i.e., having close friends) will buffer the effects of social disconnection on engagement in sexual risk behavior. The full hypothesized model is depicted in Figure 1.
FIGURE 1.
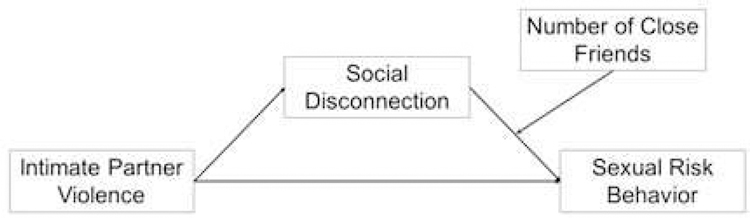
Conceptual model.
METHOD
Participants
Women (N = 240) were recruited from an urban community to participate in a “Women’s Relationship Study” and complete a 2-hour interview about their relationship with their boyfriend or husband. To be eligible to participate, women must have experienced physical victimization perpetrated by their current male partner in the past 6 months, which was determined by responses to items from the Conflict Tactics Scale-2 (CTS-2; Straus, Hamby, & Warren, 2003) during a phone screening. Eligible participants were also 18 years of age or older, currently in their relationship for at least 6 months, in contact with their partner multiple times per week without spending more than 2 full weeks apart, and had an annual household income no greater than $50,000. Data from 28 participants were removed due to failure to meet the study criteria at the time of the interview though they met the criteria during the phone screening. An additional eight participants had missing data for sexual risk behavior, the primary outcome of interest, and thus were excluded from analyses. The final sample consisted of 204 women between the ages of 18 and 58 years (M = 36.46, SD = 10.42). More than half of the participants (60.8%) were married or cohabitating, and their average relationship duration was 6.4 years (SD = 6.3). Most participants were unemployed (65.2%), with a median annual income of $9,600 and mean education level of 12.09 years (SD = 1.56). Participants’ mean number of children was 2.34 (SD = 2.07). Self-reported race/ethnicity was as follows: 135 (66.2%) African American, 43 (21.1%) White, 16 (7.8%) Latina, 10 (4.9%) multiracial.
Procedures
Participants were recruited from the community through flyers posted in establishments such as grocery stores, libraries, pizza and sandwich shops, convenience stores, primary care clinics, agencies such as the Departments of Adult Education and Employment, and nail and hair salons. Women who were interested in participating called to complete a phone screen to determine their eligibility. Eligible women were invited to participate in a 2-hour semi-structured interview. All interviews were conducted face-to-face using computer-assisted interviewing (NOVA Research Company, 2003) by female post baccalaureate, master’s or doctoral level research associates who had undergone more than 20 hours of structured training. After the interview, participants were debriefed, compensated with $50, and provided with a list of community resources for domestic violence, unemployment, benefits assistance, and mental health and substance abuse treatment.
Measures
IPV Severity.
IPV, namely physical, sexual, and psychological IPV victimization, was assessed with three separate measures. All measures used a referent period of 6 months and referred to IPV victimization perpetrated by their current partner.
Physical IPV.
The 12-item physical assault subscale of the CTS-2 (Straus et al., 2003) was administered to assess physical IPV. Participants self-reported how many times each victimization act had occurred (e.g., “My partner pushed or shoved me”), with seven response options: never, once, twice, 3–5 times, 6–10 times, 10–20 times, more than 20 times in the past 6 months. Response categories presented as ranges were recoded according to the procedures suggested by Straus et al. (2003; i.e., 4 = 3–5; 8 = 6–10; 15 = 10–20; 25 = >20), and responses across the 12 items were summed and log-transformed due to significant skew, with higher scores representing great physical IPV severity (α = .90).
Sexual IPV.
To assess sexual IPV victimization, participants responded to the 10-item Sexual Experiences Survey (SES; Koss & Oros, 1982). The SES was modified to improve comprehension among participants due to the high required reading level. Response options were the same as those for the CTS-2. Due to significant skew that could not be corrected with standard transformations, scores were recoded using procedures from Gidycz et al. (2007) such that 0 = no sexual IPV, 1 = moderate sexual IPV (ranging from unwanted sexual contact to attempted rape), and 2 = rape (vaginal, oral, or anal penetration through the use of force or threats of force).
Psychological IPV.
Psychological IPV was assessed with the 48-item Psychological Maltreatment of Women Inventory (PMWI; Tolman, 1989) assessing domains of dominance and emotional abuse (e.g., “My partner called me names,” “My partner did not let me talk about my feelings”). This measure has been widely used to assess coercive control and has demonstrated good reliability and discriminant validity (Bell, Goodman, & Dutton, 2007). Response options ranged from 1 never to 5 very frequently, and responses were summed to create a total score (following original scoring procedures; Tolman, 1989), with higher scores indicating greater IPV severity (α = .96).
Social Disconnection.
Social disconnection over the previous 6 months was assessed with four items: “I felt lonely,” “I felt that people disliked me,” “People were unfriendly,” and “I felt distant or cut off from people.” Items were sourced from multiple measures included in the study (Center for Epidemiologic Studies Depression Scale, Posttraumatic Stress Diagnostic Scale; Foa, 1995; Radloff, 1977) and were chosen based on face validity, consistency with theoretical notions of social disconnection and loneliness (Cacioppo & Patrick, 2008; Hewitt, Flett, Sherry, & Caelian, 2006), and item similarity to existing measures of social connectedness (e.g., “I feel distant from people”; Lee & Robbins, 1995). Participants reported the frequency of each statement on a scale from 0 (none of the time) to 4 (all of the time) and were averaged such that higher scores indicate greater social disconnection (α = .76).
Number of Close Friends.
The number of participants’ close friendships (i.e., high quality friendships) was assessed with a single item in which participants reported how many close friends they have. Responses were coded such that 0 = zero close friends, 1 = one close friend, and 2 = multiple (two or more) close friends.
Sexual Risk Behavior.
Participants’ sexual risk behavior over the prior 6 months was assessed with a 25-item questionnaire about women’s sexual behavior and health designed for this study (adapted from Sikkema et al., 2008; Sikkema, Hansen, Meade, Kochman, & Fox, 2009). Questions also assessed the number of times that women had unprotected anal or vaginal sex with (a) their primary partner and/or (b) other partners who were either HIV-positive or whose HIV status was unknown. Participants also reported whether they had traded sex for money, drugs, or shelter in the prior 6 months. Responses of “don’t know” were coded as “No,” to be conservative. For example, participants were asked to report: “Is your partner HIV-positive,” “Has your partner used intravenous drugs (or needles) in the past 6 months,” and “Does your partner have oral, anal, or vaginal sex with other people.” Due to relatively low endorsement of individual items, a dichotomous variable was formed to reflect women’s sexual risk behavior based on an affirmative response to one or more of the following items (Cavanaugh, Hansen, & Sullivan, 2010): (a) unprotected anal or vaginal sex with a primary partner who was HIV-seropositive, (b) unprotected anal or vaginal sex with a primary partner who had used IV drugs during the previous 6 months, (c) unprotected anal or vaginal sex with a primary partner who had multiple sex partners during the previous 6 months, (d) unprotected anal or vaginal sex with a nonprimary partner whose HIV status was either positive or unknown, and/or (e) woman has been involved in sex trade. Thus, this variable reflects the presence or absence of sexual risk behavior over the prior 6 months (0 = no sexual risk behavior, 1 = sexual risk behavior).
Analytic Approach
The PROCESS macro for SPSS (Hayes, 2012) was used to test the conceptual model depicted in Figure 1 in a series stages for each type of IPV (i.e., physical, sexual, psychological). The indirect effects and moderation components of the model were tested separately before evaluating the full, combined model. First, the indirect effects component of the model was assessed by examining the effect of each type of IPV severity on social disconnection, and in turn, sexual risk behavior. Second, the moderation component of the model was assessed by evaluating the interaction between social disconnection and number of close friends on sexual risk behavior. Finally, the full moderated mediation model was assessed. Significance was determined through 95% confidence intervals; intervals that do not contain zero are statistically significant at p < .05.
RESULTS
Prior to conducting the primary analyses, bivariate correlations were assessed (see Table 1). In line with what was expected, all three forms of IPV (physical, sexual, psychological) were significantly positively correlated with both social disconnection and sexual risk behavior. Approximately 20% reported engagement in sexual risk behavior. Next, analyses were conducted in model building stages. First, the indirect effects of each type of IPV on sexual risk behavior via social disconnection were assessed.
TABLE 1.
Correlations (N = 204)
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| 1. Physical IPV | − | |||||
| 2. Sexual IPV | .22* | − | ||||
| 3. Psychological IPV | .50* | .26* | − | |||
| 4. Social disconnection | .31* | .21* | .44* | − | ||
| 5. Number of close friends | −.07 | .06 | −.14** | −.12 | − | |
| 6. Sexual risk behavior | .14** | .18** | .25* | .23* | −.16** | − |
Note. IPV = intimate partner violence.
p < .05.
p < .01.
As predicted, physical IPV severity was associated with increased social disconnection, B (SE) = 0.17 (0.04), p < .001, 95% CI [0.10, 0.24], and in turn, social disconnection was associated with sexual risk behavior, B (SE) = 0.63 (0.24), p = .009, 95% CI [0.16, 1.10]. The indirect effect of physical IPV on sexual risk behavior through social disconnection was significant, B (SE) = 0.11 (0.05), 95% CI [0.03, 0.22].
Next, sexual IPV severity was associated with increased social disconnection, B (SE) = 0.18 (0.06), p = .003, 95% CI [0.06, 0.29], and in turn, social disconnection was associated with sexual risk behavior, B (SE) = 0.62 (0.23), p = .007, 95% CI [0.17, 1.07]. Again, the indirect effect was significant, B (SE) = 0.13 (0.06), 95% CI [0.04, 0.29].
Finally, psychological IPV severity was associated with increased social disconnection, B (SE) = 0.01 (0.001), p < .001, 95% CI [0.01, 0.013]; however, social disconnection did not predict sexual risk behavior in this model, B (SE) = 0.45 (0.25), p = .075, 95% CI [−0.05, 0.94]. Thus, the indirect effect of psychological IPV on sexual risk behavior was nonsignificant, B (SE) = 0.004 (0.003), 95% CI [−0.0002, 0.01].
Next, a moderation analysis was conducted to assess the extent to which participants’ number of close friends moderates the relationship between social disconnection and sexual risk behavior. The interaction between social disconnection and number of close friends was significant, B(SE) = −0.67 (0.33), p = .038, bootstrapped 95% CI: [0.56, 2.59]. Specifically, the link between social disconnection and sexual risk behavior was positive and significant for individuals with zero close friends, B(SE) = 1.58 (0.52), p = .002, bootstrapped 95% CI: [0.56, 2.59], and with one close friend, B(SE) = 0.90 (0.28), p = .001, 95% CI: [0.36, 1.44]. However, as shown in Figure 2, this link was nonsignificant for individuals with two or more close friends, B(SE) = 0.23 (0.31), p = .465, 95% CI: [−0.38, 0.83], indicating that social disconnection was not associated with their sexual risk behavior; risk behavior was unlikely regardless of feelings of social disconnection among individuals with multiple close friends.
FIGURE 2.
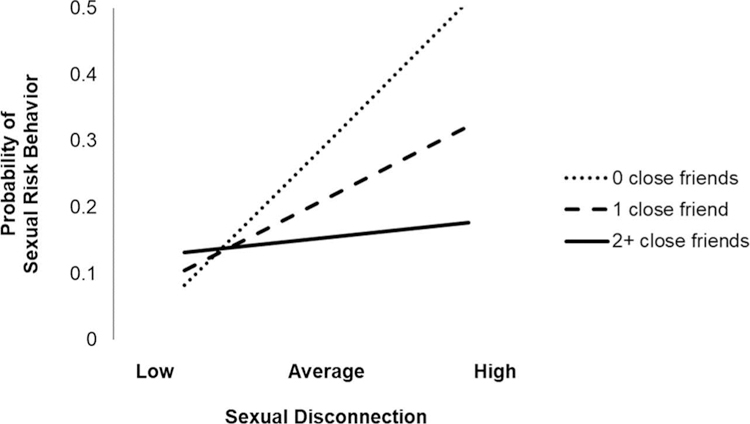
Moderating effect of number of close friends on the association between social disconnection and sexual risk behavior.
The full model (Figure 1) was then assessed separately with physical IPV and sexual IPV as the predictor. The model was not tested with psychological IPV as a predictor given that the indirect effects model for psychological IPV in the first model building step was nonsignificant. As hypothesized, the index of moderated mediation was significant for physical IPV, B (SE) = −0.11 (0.07), 95% CI [−0.26, −0.01], and sexual IPV, B (SE) = −0.13 (0.08), 95% CI [−0.32, −0.02]. The pattern of results was consistent with the results described in the previous model building stages, such that physical and sexual IPV severity was associated with increased social disconnection, and social disconnection was only associated with sexual risk behavior among women with 0 or 1 close friends. Full model results are presented in Table 2.
TABLE 2.
Results for Conditional Process Analyses (N = 204)
| B (SE) | p | 95% CI: [LL, UL] | |
|---|---|---|---|
| Physical IPV Model | |||
| Outcome: Social disconnection | |||
| Intercept | .63 (.11) | < .001* | [.41, .84] |
| Physical IPV | .17 (.04) | < .001* | [.10, .24] |
| Outcome: Sexual risk behavior | |||
| Intercept | −3.10 (.88) | < .001* | [−4.83, −1.38] |
| Physical IPV | .12 (.12) | .383 | [−.15, .39] |
| Social disconnection | .51 (.26) | .047** | [.01, 1.02] |
| No. close friends | −.27 (.26) | .309 | [−.78, .25] |
| Social disconnection × No. close friends | −.68 (.33) | .038** | [−1.31, −.04] |
| Sexual IPV Model | |||
| Outcome: Social disconnection | |||
| Intercept | .90 (.08) | < .001* | [.75, 1.05] |
| Sexual IPV | .18 (.06) | .003* | [.06, .29] |
| Outcome: Sexual risk behavior | |||
| Intercept | −3.32 (.87) | < .001* | [−5.03, −1.61] |
| Sexual IPV | .53 (.22) | .017** | [.10, .97] |
| Social disconnection | 1.55 (.52) | .003* | [.53, 1.57] |
| No. close friends | .45 (.49) | .364 | [−.52, 1.41] |
| Social disconnection × No. close friends | −.74 (.33) | .024** | [−1.38, −.10] |
Note. IPV = intimate partner violence.
p < .05.
p < .01.
DISCUSSION
The current study was aimed at investigating a specific social process that may underlie the association between women’s IPV victimization and their engagement in sexual risk behavior. We tested the idea that women’s IPV victimization severity would be associated with meaningful increases in feelings of social disconnection, and that feelings of social disconnection would, in turn, be associated with seeking out behaviors that facilitate social connection. We expected that women would engage in sexual risk behavior to socially connect, but only if they lacked alternative (and arguably less risky) social opportunities to fulfill this goal. As hypothesized, social disconnection mediated the relationships between both physical and sexual IPV severity and sexual risk behavior. Although psychological IPV severity was significantly, positively correlated with social disconnection and sexual risk behavior, this indirect effect was nonsignificant. In general, these results support the notion that multiple forms of IPV predict sexual risk behavior via social disconnection. Overall, these findings were consistent with past research that has shown positive associations between IPV and sexual risk behavior (Campbell & Soeken, 1999; Gidycz et al., 2008; Lang et al., 2011), and provide empirical support for the idea that sexual behavior may fulfill interpersonal goals (Cooper et al., 1998; Rawn & Vohs, 2011). Further, these findings extend past research, which has primarily focused only on one form of victimization, and provides greater insight into the mechanisms underlying the association between IPV and sexual risk behavior by examining social disconnection in general, and close friendships in particular. Past research has shown that social connection is crucial for women’s recovery and well-being following IPV (e.g., Beeble et al., 2009; Coker, Smith et al., 2002; Coker et al., 2003), and the current research extends these findings by identifying one specific outcome (i.e., sexual risk behavior) that results from a lack of connection. Additionally, we evaluated these pathways in a sample of women who are still with the partner that perpetrated IPV, which extends previous research that has largely focused on behavior and well-being after the relationship has ended.
In line with expectations, the effect of social disconnection on sexual risk behavior was only significant when women lacked close friends (i.e., potentially lacked alternative means to social connection). It is likely that women who have sufficient social support resources can more readily and easily attain their social connection goals through their existing networks. However, when such resources are not available, individuals become increasingly likely to engage in behaviors that quickly facilitate social connection (e.g., sexual risk behavior), even if it compromises other goals women might have such as health and safety. This finding is important for the development and implementation of interventions, given that one way to reduce engagement in undesirable/risky behavior (e.g., sexual risk behavior) is to introduce alternative behavioral means that target the same goal (Conrod, Castellanos-Ryan, & Mackie, 2011; Kruglanski et al., 2002). The reason for the nonsignificant indirect effect through psychological IPV is unclear. Interestingly, psychological IPV was more strongly related to both social disconnection and sexual risk behavior than either of the other forms of IPV, and the direct effect on sexual risk behavior remained significant in the mediation model. Because sexual risk behavior is a complex and multidetermined behavior, it is likely that there are multiple psychological pathways (e.g., coping, regulating affect) operating in parallel—and future research should seek to identify the set of circumstances under which the social processes described in the current study are most relevant.
Strengths, Limitations, and Future Directions
In addition to the novel theoretical lens through which this study was framed, strengths included the consideration of multiple types of IPV predicting social disconnection and sexual risk behavior, and the inclusion of a community sample of IPV victims. However, there were limitations that should be addressed in future studies that aim to replicate and extend these findings. First, all the women in this sample were still with their partner that perpetrated the IPV, which limits generalizability to women who are no longer with their abusive partners. Because women were currently involved with their abusive partner, only a small subset of women were engaging in sexual risk behavior, reducing variability in the types and frequency of sexual risk behavior women reported. Future research that includes samples with a higher prevalence of these behaviors would allow for greater variation and analysis of different types (e.g., inconsistent condom use, multiple casual partners), and frequency of sexual risk behavior. Women of low socioeconomic status were also overrepresented in this sample, again limiting generalizability. Additionally, although this study aimed to understand the circumstances under which sexual risk behavior reflects victims’ attempts at fulfilling social connection goals following interpersonal harm and disconnection, motives for sex were not explicitly evaluated. It is important for future research to more directly measure goals and motives, though this may prove difficult given that individuals are not always consciously aware of what drives their own behavior. Relatedly, future research should collect more specific information regarding participants’ actual and perceived social support in order to better disentangle these associations. It also would be useful to evaluate multiple sources of social support including social support in the workplace, which may be lacking in the current sample in particular due to the high rate of unemployment. The items used in the current study to represent social disconnection were face valid, mapped onto theoretical conceptualizations of social disconnection, and were similar to existing social connectedness measures—however, it is important for future research to incorporate a well-validated measure for this construct. Although the design of this study was cross-sectional, the results provide preliminary insight into the social pathways that underlie sexual risk behavior among IPV victims that may inform future research that allows for causal conclusions to be made.
Implications
This research provides critical insight into a social process that may lead IPV victims to engage in sexual risk behavior. Researchers and clinicians should focus primary efforts on preventing IPV from occurring; however, if IPV already has occurred, then it is imperative to mitigate its effects on engagement in unhealthy behaviors. For instance, given that this study suggests that having alternative means to social connection buffers the effect of social disconnection on sexual risk behavior among IPV victims, it is important for researchers and practitioners to implement interventions that target belongingness and social connection such as enhancing peer connections and promoting community engagement (Coker, Smith, et al., 2002; Constantino, Kim, & Crane, 2005). Additionally, because many IPV victims stay in their relationships (either by choice or due to fear of their partner’s retribution if they leave; Bell et al., 2007), it is important to increase the accessibility of resources that promote healthy coping strategies that may ameliorate feelings of social disconnection. Strategies specific to reducing the impact of sexual risk behavior include increasing communication with one’s partner to encourage regular STI/HIV screening (if safe for the victim), or increasing access to pre-exposure prophylaxis (PrEP) for HIV specifically if the aforementioned approach is not safe for the victim. In the current study, we found that simply the presence of multiple friendships—not necessarily the utilization of social support—buffered the effects of social disconnection. Thus, simply the availability of the resources described above may offer a small, but positive benefit for victims.
CONCLUSION
Results of this study highlight the importance of social connection for women’s well-being and risk behavior. It is important for researchers to continue to consider the social processes that are important to IPV victims’ healing and recovery in order to promote global increases in health. Doing so would both complement approaches that largely emphasize psychological and individual-level processes, as well as inform more effective prevention and intervention strategies for women who have experienced IPV.
Acknowledgments.
The research described here was supported, in part, by grants from the National Institute on Drug Abuse (R03 DA17668, T32 DA019426).
Footnotes
Disclosure. The authors have no relevant financial interest or affiliations with any commercial interests related to the subjects discussed within this article.
REFERENCES
- Aarts H, & Dijksterhuis A (2000). Habits as knowledge structures: Automaticity in goal-directed behavior. Journal of Personality and Social Psychology, 78(1), 53–63. doi: 10.1037/0022-3514.78.1.53 [DOI] [PubMed] [Google Scholar]
- Arriaga XB, & Schkeryantz EL (2015). Intimate relationships and personal distress: The invisible harm of psychological aggression. Personality and Social Psychology Bulletin, 41(10), 1332–1344. doi: 10.1177/0146167215594123 [DOI] [PubMed] [Google Scholar]
- Baumeister RF, & Leary MR (1995). The need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychological Bulletin, 117(3), 497–529. doi: 10.1037/0033-2909.117.3.497 [DOI] [PubMed] [Google Scholar]
- Beeble ML, Bybee D, Sullivan CM, & Adams AE (2009). Main, mediating, and moderating effects of social support on the well-being of survivors of intimate partner violence across 2 years. Journal of Consulting and Clinical Psychology, 77(4), 718–729. doi: 10.1037/a0016140 [DOI] [PubMed] [Google Scholar]
- Bell ME, Goodman LA, & Dutton MA (2007). The dynamics of staying and leaving: Implications for battered women’s emotional well-being and experiences of violence at the end of a year. Journal of Family Violence, 22(6), 413–428. doi: 10.1007/s10896-007-9096-9 [DOI] [Google Scholar]
- Breiding MJ, Black MC, & Ryan GW (2008). Chronic disease and health risk behaviors associated with intimate partner violence—18 US states/territories, 2005. Annals of Epidemiology, 18(7), 538–544. doi: 10.1016/j.annepidem.2008.02.005 [DOI] [PubMed] [Google Scholar]
- Cacioppo JT, & Patrick W (2008). Loneliness: Human nature and the need for social connection. New York, NY: WW Norton. [Google Scholar]
- Campbell J, Jones AS, Dienemann J, Kub J, Schollenberger J, O’campo P, … Wynne C (2002). Intimate partner violence and physical health consequences. Archives of Internal Medicine, 162(10), 1157–1163. doi: 10.1001/archinte.162.10.1157 [DOI] [PubMed] [Google Scholar]
- Campbell JC, & Soeken KL (1999). Forced sex and intimate partner violence: Effects on women’s risk and women’s health. Violence Against Women, 5(9), 1017–1035. doi: 10.1177/1077801299005009003 [DOI] [Google Scholar]
- Cavanaugh CE, Hansen NB, & Sullivan TP (2010). HIV sexual risk behavior among low-income women experiencing intimate partner violence: The role of posttraumatic stress disorder. AIDS and Behavior, 14(2), 318–327. doi: 10.1007/s10461-009-9623-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (2014). Intersection of intimate partner violence and HIV in women. Atlanta, GA: Author; Retrieved from http://www.CDC.gov/violenceprevention/pdf/ipv/13_243567_green_aag-a.pdf [Google Scholar]
- Coker AL, Davis KE, Arias I, Desai S, Sanderson M, Brandt HM, … Smith PH (2002). Physical and mental health effects of intimate partner violence for men and women. American Journal of Preventive Medicine, 23(4), 260–268. doi: 10.1016/S0749-3797(02)00514-7 [DOI] [PubMed] [Google Scholar]
- Coker AL, Smith PH, Thompson MP, McKeown RE, Bethea L, & Davis KE (2002). Social support protects against the negative effects of partner violence on mental health. Journal of Women’s Health & Gender-Based Medicine, 11(5), 465–476. doi: 10.1089/15246090260137644 [DOI] [PubMed] [Google Scholar]
- Coker AL, Watkins KW, Smith PH, & Brandt HM (2003). Social support reduces the impact of partner violence on health: Application of structural equation models. Preventive Medicine, 37(3), 259–267. doi: 10.1016/S0091-7435(03)00122-1 [DOI] [PubMed] [Google Scholar]
- Conrod PJ, Castellanos-Ryan N, & Mackie C (2011). Long-term effects of a personality-targeted intervention to reduce alcohol use in adolescents. Journal of Consulting and Clinical Psychology, 79(3), 296–306. doi: 10.1037/a0022997 [DOI] [PubMed] [Google Scholar]
- Constantino R, Kim Y, & Crane PA (2005). Effects of a social support intervention on health outcomes in residents of a domestic violence shelter: A pilot study. Issues in Mental Health Nursing, 26(6), 575–590. doi: 10.1080/01612840590959416 [DOI] [PubMed] [Google Scholar]
- Cooper ML, Shapiro CM, & Powers AM (1998). Motivations for sex and risky sexual behavior among adolescents and young adults: A functional perspective. Journal of Personality and Social Psychology, 75(6), 1528–1558. doi: 10.1037/0022-3514.75.6.1528 [DOI] [PubMed] [Google Scholar]
- Cox DW, Buhr EE, Owen JJ, & Davidson E (2016). Linking partner emotional support, partner negative interaction, and trauma with psychological distress: Direct and moderating effects. Journal of Social and Personal Relationships, 33(3), 303–319. doi: 10.1177/0265407515574467 [DOI] [Google Scholar]
- Cullerton-Sen C, & Crick NR (2005). Understanding the effects of physical and relational victimization: The utility of multiple perspectives in predicting social-emotional adjustment. School Psychology Review, 34(2), 147–160. [Google Scholar]
- Davis JL, Combs-Lane AM, & Jackson TL (2002). Risky behaviors associated with interpersonal victimization: Comparisons based on type, number, and characteristics of assault incidents. Journal of Interpersonal Violence, 17(6), 611–629. doi: 10.1177/0886260502017006002 [DOI] [Google Scholar]
- El-Bassel N, Gilbertl L, Rajah V, Foleno A, & Frye V (2000). Fear and violence: Raising the HIV stakes. AIDS Education and Prevention, 12(2), 154–170. [PubMed] [Google Scholar]
- Enander V (2011). Leaving Jekyll and Hyde: Emotion work in the context of intimate partner violence. Feminism & Psychology, 21(1), 29–48. doi: 10.1177/0959353510384831 [DOI] [Google Scholar]
- Feeney BC, & Collins NL (2015). A new look at social support: A theoretical perspective on thriving through relationships. Personality and Social Psychology Review, 19(2), 113–147. doi: 10.1177/1088868314544222 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foa E (1995). The posttraumatic diagnostic scale (PDS) manual. Minneapolis, MN: National Computer Systems. [Google Scholar]
- Gidycz CA, Loh C, Lobo T, Rich C, Lynn SJ, & Pashdag J (2007). Reciprocal relationships among alcohol use, risk perception, and sexual victimization: A prospective analysis. Journal of American College Health, 56(1), 5–14. doi: 10.3200/JACH.56.1.5-14 [DOI] [PubMed] [Google Scholar]
- Gidycz CA, Orchowski LM, King CR, & Rich CL (2008). Sexual victimization and health-risk behaviors: A prospective analysis of college women. Journal of Interpersonal Violence, 23(6), 744–763. doi: 10.1177/0886260507313944 [DOI] [PubMed] [Google Scholar]
- Golder S, & Logan T (2011). Cumulative victimization, psychological distress, and high-risk behavior among substance-involved women. Violence and Victims, 26(4), 477–495. doi: 10.1891/0886-6708.26.4.477 [DOI] [PubMed] [Google Scholar]
- Gollwitzer PM, & Bargh JA (2005). Automaticity in goal pursuit In Elliot A & Dweck C (Eds.), Handbook of competence and motivation. New York, NY: Guilford Press. [Google Scholar]
- Goodman LA, & Smyth KF (2011). A call for a social network-oriented approach to services for survivors of intimate partner violence. Psychology of Violence, 1(2), 79–92. doi: 10.1037/a0022977 [DOI] [Google Scholar]
- Hayes AF (2012). Process: A versatile computational tool for observed variable mediation, moderation, and conditional process modeling. University of Kansas, KS; Retrieved from http://imaging.mrc-cbu.cam.ac.uk/statswiki/FAQ/SobelTest?action=AttachFile&do=get&target=process.pdf [Google Scholar]
- Hewitt PL, Flett GL, Sherry SB, & Caelian C (2006). Trait perfectionism dimensions and suicidal behavior In Ellis TE (Ed.), Cognition and suicide: Theory, research, and practice (pp. 215–235). Washington, DC: American Psychological Association. [Google Scholar]
- Jacques-Tiura AJ, Norris J, Kiekel PA, Davis KC, Zawacki T, Morrison DM, … Abdallah DA (2015). Influences of acute alcohol consumption, sexual precedence, and relationship motivation on women’s relationship and sex appraisals and unprotected sex intentions. Journal of Social and Personal Relationships, 32(2), 197–221. doi: 10.1177/0265407514528101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kopetz C, & Orehek E (2015). When the end justifies the means: Self-defeating behaviors as “rational” and “successful” self-regulation. Current Directions in Psychological Science, 24(5), 386–391. doi: 10.1177/0963721415589329 [DOI] [Google Scholar]
- Koss MP, & Oros CJ (1982). Sexual experiences survey: A research instrument investigating sexual aggression and victimization. Journal of Consulting and Clinical Psychology, 50(3), 455–457. doi: 10.1037/0022-006X.50.3.455 [DOI] [PubMed] [Google Scholar]
- Kruglanski AW, Shah JY, Fishbach A, Friedman R, Chun WY, & Sleeth-Keppler D (2002). A theory of goal systems. Advances in Experimental Social Psychology, 34, 215–258. doi: 10.1016/S0065-2601(02)80008-9 [DOI] [Google Scholar]
- Lang DL, Sales JM, Salazar LF, Hardin JW, DiClemente RJ, Wingood GM, … Rose E (2011). Rape victimization and high risk sexual behaviors: Longitudinal study of African-American adolescent females. Western Journal of Emergency Medicine, 12(3), 333–342. [PMC free article] [PubMed] [Google Scholar]
- Lee RM, & Robbins SB (1995). Measuring belongingness: The social connectedness and the social assurance scales. Journal of Counseling Psychology, 42(2), 232. doi: 10.1037/0022-0167.42.2.232 [DOI] [Google Scholar]
- Levendosky AA, Bogat GA, Theran SA, Trotter JS, von Eye A, & Davidson WS (2004). The social networks of women experiencing domestic violence. American Journal of Community Psychology, 34(1–2), 95–109. doi: 10.1023/B:AJCP.0000040149.58847.10 [DOI] [PubMed] [Google Scholar]
- Macmillan R (2001). Violence and the life course: The consequences of victimization for personal and social development. Annual Review of Sociology, 27(1), 1–22. doi: 10.1146/annurev.soc.27.1.1 [DOI] [Google Scholar]
- Maman S, Campbell J, Sweat MD, & Gielen AC (2000). The intersections of HIV and violence: Directions for future research and interventions. Social Science & Medicine, 50(4), 459–478. doi: 10.1016/S0277-9536(99)00270-1 [DOI] [PubMed] [Google Scholar]
- Maner JK, DeWall CN, Baumeister RF, & Schaller M (2007). Does social exclusion motivate interpersonal reconnection? Resolving the “porcupine problem.” Journal of Personality and Social Psychology, 92(1), 42–55. doi: 10.1037/0022-3514.92.1.42 [DOI] [PubMed] [Google Scholar]
- Mikulincer M, & Shaver PR (2007). Attachment in adulthood: Structure, dynamics, and change. New York: Guilford Press. [Google Scholar]
- Mittal M, Senn TE, & Carey MP (2011). Mediators of the relation between partner violence and sexual risk behavior among women attending a sexually transmitted disease clinic. Sexually Transmitted Diseases, 38(6), 510–515. doi: 10.1097/OLQ.0b013e318207f59b [DOI] [PMC free article] [PubMed] [Google Scholar]
- Noll JG, Trickett PK, & Putnam FW (2003). A prospective investigation of the impact of childhood sexual abuse on the development of sexuality. Journal of Consulting and Clinical Psychology, 71(3), 575–586. doi: 10.1037/0022-006X.71.3.575 [DOI] [PMC free article] [PubMed] [Google Scholar]
- NOVA Research Company. (2003). Questionnaire Development System user’s manual. Bethesda, MD: Author. [Google Scholar]
- Purdie V, & Downey G (2000).Rejection sensitivity and adolescent girls’ vulnerability to relationship-centered difficulties. Child Maltreatment, 5(4), 338–349. doi: 10.1177/1077559500005004005 [DOI] [PubMed] [Google Scholar]
- Radloff LS (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1(3), 385–401. doi: 10.1177/014662167700100306 [DOI] [Google Scholar]
- Rawn CD, & Vohs KD (2011). People use self-control to risk personal harm: An intra-interpersonal dilemma. Personality and Social Psychology Review, 15(3), 267–289. doi: 10.1177/1088868310381084 [DOI] [PubMed] [Google Scholar]
- Rhatigan DL, & Axsom DK (2006). Using the investment model to understand battered women’s commitment to abusive relationships. Journal of Family Violence, 21(2), 153–162. doi: 10.1007/s10896-005-9013-z [DOI] [Google Scholar]
- Seth P, Raiford JL, Robinson LS, Wingood GM, & DiClemente RJ (2010). Intimate partner violence and other partner-related factors: Correlates of sexually transmissible infections and risky sexual behaviours among young adult African American women. Sexual Health, 7(1), 25–30. doi: 10.1071/SH08075 [DOI] [PubMed] [Google Scholar]
- Sikkema KJ, Hansen NB, Meade CS, Kochman A, & Fox AM (2009). Psychosocial predictors of sexual HIV transmission risk behavior among HIV-positive adults with a sexual abuse history in childhood. Archives of Sexual Behavior, 38(1), 121–134. doi: 10.1007/s10508-007-9238-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sikkema KJ, Wilson PA, Hansen NB, Kochman A, Neufeld S, Ghebremichael MS, … Kershaw T (2008). Effects of a coping intervention on transmission risk behavior among people living with HIV/AIDS and a history of childhood sexual abuse. Journal of Acquired Immune Deficiency Syndromes, 47(4), 506–513. doi: 10.1097/QAI.0b013e318160d727 [DOI] [PubMed] [Google Scholar]
- Straus MA, Hamby SL, & Warren WL (2003). Conflict tactics scale handbook (CTS). Los Angeles, CA: Western Psychological Services. [Google Scholar]
- Sullivan TP, McPartland TS, Armeli S, Jaquier V, & Tennen H (2012). Is it the exception or the rule? Daily co-occurrence of physical, sexual, and psychological partner violence in a 90-day study of substance-using, community women. Psychology of Violence, 2(2), 154–164. doi: 10.1037/a0027106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tolman RM (1989). The development of a measure of psychological maltreatment of women by their male partners. Violence and Victims, 4(3), 159–177. doi: 10.1891/0886-6708.4.3.159 [DOI] [PubMed] [Google Scholar]
- Twenge JM, Catanese KR, & Baumeister RF (2002). Social exclusion causes self-defeating behavior. Journal of Personality and Social Psychology, 83(3), 606–615. doi: 10.1037/0022-3514.83.3.606 [DOI] [PubMed] [Google Scholar]
- Webb TL, & Sheeran P (2006). Does changing behavioral intentions engender behavior change? A meta-analysis of the experimental evidence. Psychological Bulletin, 132(2), 249. doi: 10.1037/0033-2909.132.2.249 [DOI] [PubMed] [Google Scholar]
- Woerner J, Kopetz C, Lechner WV, & Lejuez C (2016). History of abuse and risky sex among substance users: The role of rejection sensitivity and the need to belong. Addictive Behaviors, 62, 73–78. doi: 10.1016/j.addbeh.2016.06.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zurbriggen EL, & Freyd JJ (2004). The link between child sexual abuse and risky sexual behavior: The role of dissociative tendencies, information-processing effects, and consensual sex decision mechanisms In Koenig LJ and Doll LS (Eds.), From child sexual abuse to adult sexual risk: Trauma, revictimization, and intervention (pp. 135–157). Washington, DC: American Psychological Association. [Google Scholar]