

Abstract
Objective:
This study examined the association between transnational death and psychological distress among undocumented Mexican immigrants. The Minority Stress Model and a disenfranchised grief perspective were used as frameworks for this study.
Method:
Respondent driven sampling (RDS) was used to collect data from clinical interviews with 248 undocumented Mexican immigrants residing near the US–Mexico border.
Results:
After controlling for relevant covariates, experiencing transnational death was a significant predictor of clinically significant distress in this at-risk population.
Conclusions:
Our findings underscore the need to contextualize transnational death among undocumented immigrants from a perspective of disenfranchised grief that requires the development of contextually and culturally sensitive interventions aimed at addressing the high prevalence of transnational death and its associated distress in this marginalized population.
Introduction
The United States (US) received 23 million immigrants between 1990 and 2015, the largest increase of immigration in any country. Among these, immigrants of Mexican origin account for the largest share of immigration in the US, with a considerable proportion being undocumented (Krogstad, Passel, & Cohn, 2017). As of 2015, there were 11 million undocumented Mexican immigrants in the US, with nearly half of these immigrants having lived in the country for over a decade (Krogstad et al., 2017). As these immigrants establish residence in the US, they are often torn between longing for family members left in their home country and focusing on their new families in the US. (Krogstad et al., 2017). Given that undocumented Mexican immigrants make up a considerable proportion of the US population, research is needed to inform the depth of immigration-related distress and potential protective factors.
The minority stress model emphasizes that individuals from stigmatized groups, such as undocumented immigrants, face chronic stressors imposed by social and cultural structures that require greater effort to cope with stress, increasing their vulnerability for psychological distress (Meyer, 2003). A growing body of literature shows that undocumented immigrants often face multiple, complex, chronic stressors that increase the risk for psychological distress over time (Garcini et al., 2016, 2017). A salient stressor among undocumented immigrants is separation from family and friends, which is associated with increased psychological distress (Cervantes, Padilla, & Salgado, 1991; Hovey, 2000). As immigrants separate from their friends and families, they often lose contact with social, emotional, and cultural resources that are essential for coping (Solheim, Zaid, & Ballard, 2016). Separation from family and friends may become particularly difficult when undocumented immigrants experience transnational death, that is, the death of a loved one in their home country while the immigrant is living in the US. Given that undocumented immigrants are usually unable to travel internationally, they are often faced with having to mourn the death of their loved ones from afar and with limited support and resources (Bravo, 2017; Solheim et al., 2016).
The loss of a loved one is one of the most distressing events a person may face, which is often characterized by intense psychological reactions soon after the loss (Byrne & Raphael, 1997; Stroebe, Stroebe, & Abakomkin, 2005). The death of a loved one may be particularly distressing when the loss is experienced as disenfranchised grief, such that an individual’s ability to grieve is limited by stigma or not acknowledged by society (Doka, 2002). For instance, among documented immigrants, the ability to return home for funerals is a critical component for the emotional experience of grief, partly because lacking social support is a risk factor for negative health outcomes following bereavement (Bravo, 2017; Stroebe & Schut, 2001). Undocumented immigrants typically do not have the option to return home. Factors that often impede these immigrants from traveling when a loved one dies in their country of origin include the cost of payments to “coyotes” or smugglers, dangers involved in border crossing, and increased possibility of capture or deportation (Bravo, 2017). Salient stereotypes that portray undocumented immigrants as an economic and social burden to society may contribute to distancing the general population from the immigrant’s predicament to return to their home country in the face of loss, as this could be perceived by others as self-inflicted. Stigmatized grief occurs when there is a lack of sympathy due to the circumstances of the loss; thus, people generally express less empathy and less support for the person in need (Tarrant, Dazeley, & Cottom, 2009). In this way, the losses that undocumented immigrants experience may often go unacknowledged or may be dismissed by others, which likely increases the risk of psychological distress beyond that normally associated with the bereavement process (Doka, 2002). Documenting the distress associated with transnational bereavement among undocumented immigrants from a disenfranchised perspective is essential to inform much-needed research, intervention, and advocacy efforts.
Identifying protective factors that could ameliorate distress associated with experiencing transnational bereavement or the death of a loved one from afar is critical to develop intervention efforts. One important factor to consider is religiosity, defined as the compliance, belongingness, and commitment to an organized tradition with a specific belief system (Thoresen, Harris, & Oman, 2001). Among undocumented Mexican immigrants, religiosity is frequently used to cope with distressing events and daily life stressors associated with the undocumented experience; furthermore, religiosity is often seen as fundamental to wellbeing (Cobb, Sanders, & Xie, 2016; Ransford, Carrillo, & Rivera, 2010). However, little is known about the effect of religiosity on transnational bereavement in this population. Using the Minority Stress Model (Meyer, 2003) and Doka’s perspective on disenfranchised grief (Doka, 2002) as frameworks for our research, this study aims to: (1) identify the association between history of transnational death and clinically significant psychological distress among undocumented Mexican immigrants and (2) assess the role of religiosity in the aforementioned association.
Method
Design and sample
This cross-sectional study used respondent driven sampling (RDS) as sampling and data analysis method. RDS is currently the most effective method to study hard-to-reach populations and has previously been used in the study of undocumented immigrants (Heckathorn, 1997; Montealegre, Risser, Selwyn, Sabin, & McCurdy, 2012; Tyldum & Johnston, 2014, Zhang, 2012;). Briefly, RDS uses a structured referral system in which successive waves of participants are recruited until diversity in the sample is achieved. In this study, diversity of the sample was achieved at the 11th wave of the referral process. Further details about the RDS methodology used are described in previous research (San Diego State University and University of California San Diego Institutional Review Board). Participants were adults 18 years or older, of Mexican-origin, and undocumented. Other inclusion criteria were being Spanish-speaking and not having acute psychotic symptoms. Participants provided verbal consent prior to the interviews, and the study was approved by the San Diego State University and University of California San Diego Institutional Review Board Institutional Review Board.
Data collection
Data were collected from 2014 to 2015. Recruitment began with three previously selected undocumented Mexican immigrants or seeds carefully identified during formative research. Seeds were selected to represent the diversity of the community, including gender, age, place of residence, and relevant immigration characteristics. Each seed was provided with three referral coupons to recruit other undocumented immigrants for participation. The next waves of recruited participants were provided with another set of three referral coupons to recruit additional participants. Sampling continued until the desired sample size was reached and equilibrium was achieved. Equilibrium was verified empirically through RDS Analyst (Handcock, Fellows, & Gile, 2014), which showed that the final subjects recruited no longer had identical characteristics to the initial seeds. In accordance with RDS methodology, participants were provided a dual monetary incentive; one for completing their clinical interview ($30) and another of less monetary value ($10) for each referral that completed an interview, with a maximum of three referrals. Participants redeemed their coupons prior to completing the clinical interview, and each coupon was carefully numbered to ensure that participants would only complete the interview once (Figure 1).
Figure 1.
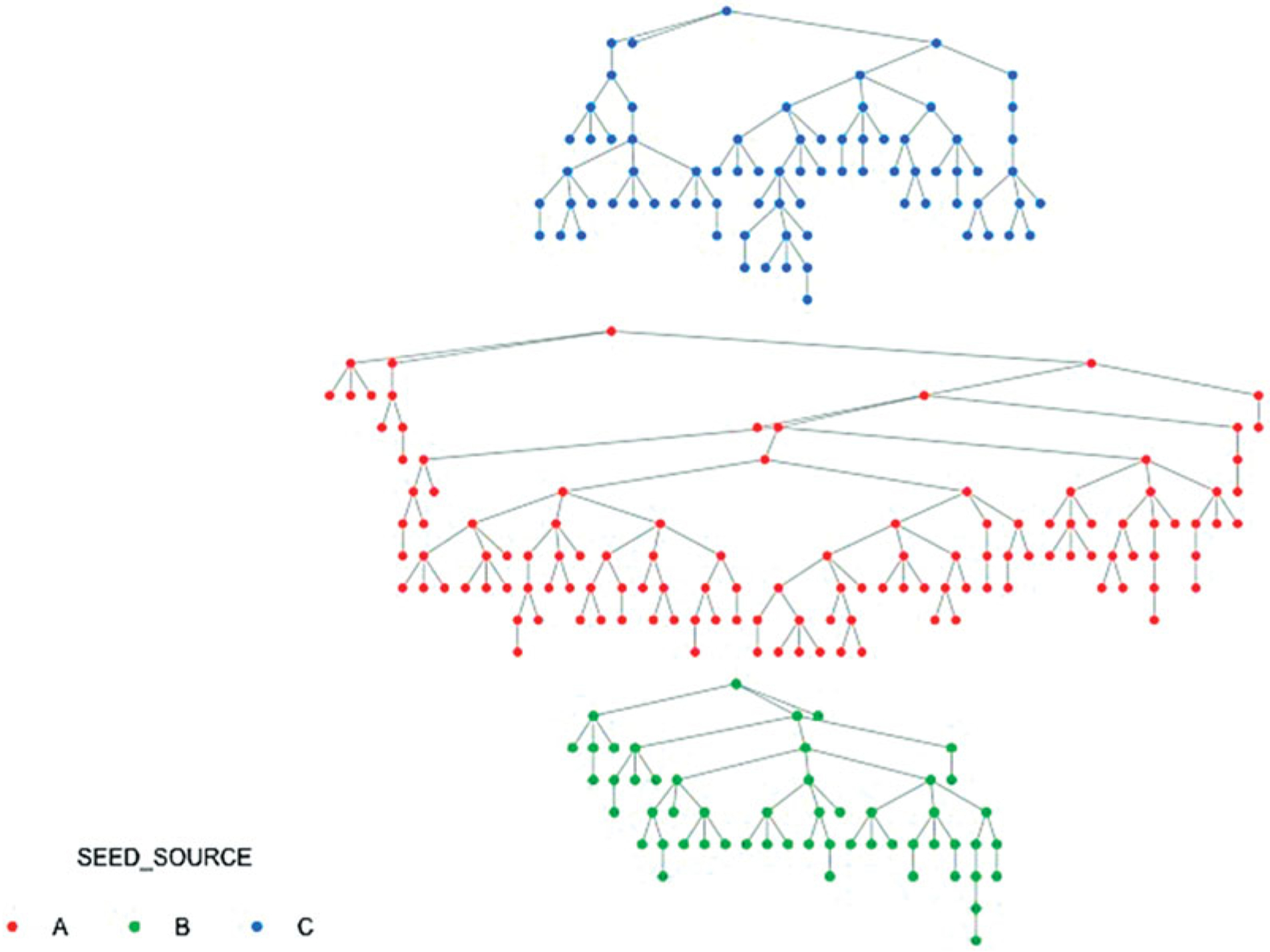
Recruitment tree.
Face-to-face semi-structured clinical interviews were conducted by psychology trainees under direct supervision of mental health clinicians. Interviews ranged from 1 to 3 hr. All interviews were conducted in Spanish by native Spanish speakers. Participants included 257 undocumented immigrants; however, six participants were not of Mexican origin and were excluded. Additionally, three participants had missing data on the outcome of interest and were also excluded. The analytical sample is based on data from 248 undocumented Mexican immigrants residing in a medium size city, relatively near the US–Mexico border. To provide the most conservative estimates, analyses in this study were conducted using the 15% population estimate in the target location as reference (N = 22,000).
Measures
History of transnational death.
This was assessed using two questions from the Multidimensional Loss Scale (MLS), which assesses different types of losses experienced among immigrant populations (Vromans, Schweitzer, & Brough, 2012). The first question asked participants if they had experienced the death of a family member in their country of origin while living in the US; the second question asked if the participant had experienced the death of a friend in their country of origin while living in the US Responses were dichotomous (yes/no). For the regression analyses, a dichotomous variable was calculated to denote history of transnational death if the participant had experienced the loss of a family member and/or friend (yes) versus no death from afar (no).
Psychological distress.
This was assessed using the Spanish version of the Brief Symptom Inventory (BSI; Derogatis, 1993), which was pre-tested and adapted with members of the target population (Peña, Garcini, Gutierrez, Ulibarri, & Klonoff, 2016). The BSI assesses psychological distress using symptom patterns along nine dimensions and a global severity index (GSI) to provide an overall assessment of distress. Each item was rated on a five-point scale to denote distress from 0=not at all to 4=extremely. Using gender-specific community non-patient norms, raw scores for each scale and the GSI were converted to standardized T-scores (M = 50, SD = 10). Clinically significant psychological distress or a “case for positive diagnosis” was denoted with a T score of 63 or above on the GSI or on any two subscale dimension scores. The choice for using a dichotomous score versus a continuous score was made to denote clinical significance, which identifies subject’s scores that are elevated to the point of functional impairment and clinical concern in need of treatment. The BSI is widely used, has well-established psychometric properties and has been previously used with Mexican immigrants (Cervantes, Fisher, Padilla, & Napper, 2015). The Cronbach’s alpha for the BSI was 0.95.
Religiosity.
Three aspects of religiosity were assessed including perceptions of religiosity, influence of religion, and church attendance (Hovey, 2000). Perceptions of religiosity were measured with the question “how religious are you?” whereas influence of religion was measured with the question “how much influence does religion have upon your life?” Church attendance was measured using the question “how often do you attend church?” and responses were given using a six-point scale from 1=never to 6=once a week or more. Each of these questions has been previously used to assess religiosity among Mexican immigrants (Hovey, 2000; Hovey & Magana, 2002).
Demographics, immigration characteristics, and history of trauma.
Demographic and immigration questions were modeled from the 2009 San Diego Prevention Research Center (SDPRC) and the San Diego Labor Trafficking Survey Questionnaire (Zhang, 2012). Demographic questions included sex, age, education, and monthly household income. Immigration history included length of time in the US. History of trauma was assessed with the Traumatic Events Inventory of the Harvard Trauma Questionnaire (HTQ), which assesses traumatic experiences among at-risk immigrants (Mollica, Mcdonald, Massagli, & Silove, 2004). This inventory assessed participants’ experience and/or witnessing of 25 common forms of human rights violations (Mollica et al., 2004). Responses to the HTQ inventory were dichotomous (yes/no).
All measures were adapted for content and language based on results from pilot testing with recently deported undocumented immigrants (Peña et al., 2016). The established methodology was used in the adaptation of all measures (Beaton, Bombardier, Guillemin, & Ferraz, 2002).
Analyses
RDS analyst was used for the testing of RDS assumptions, generation of RDS weights, and analysis of population estimates and 95% confidence intervals (Gile, 2011; Handcock et al., 2014). To estimate the sample size needed, a priori power analysis was conducted using OpenEpi version 3.01 (Dean, Sullivan, & Soe (MIT License), 2013). For all analyses, inferential statistics accounted for design effects and sample weights to produce weighted population estimates. Logistic regression was used to assess the association between history of transnational death and clinically significant psychological distress. Also, three different logistic regression models evaluated the moderating effect of different aspects of religiosity on the association between history of transnational death and clinically significant psychological distress. In these models, each of the religiosity variables was centered to reduce multicollinearity, and an interaction term of the history of death while abroad by the specific aspect of religiosity assessed were created (Aiken & West, 1991). In all three models, we controlled for sex, age, education, monthly household income, and years in the US.
Results
Descriptive statistics
Participants’ average age was 38 years (SD = 11.2). The majority was female, married, had low educational attainment, and lived on a monthly household income of less than $2000 USD. Length of time residing in the US ranged from less than one year to 54 years, with the majority of participants residing in the US for more than 10 years (M = 16 years; SD = 7.9). (See Table 1). Also, 86% of the participants were parents and had, on average, three children. Among those who were parents, most had at least one of their children born in the US. (83%), with more than half of these parents having had all of their children born in the U.S (53%). Furthermore, the majority of participants reported having a history of trauma (83%), and approximately, 42% of participants met criteria for clinically significant psychological distress.
Table 1.
Demographic and immigration characteristics by history of a death while abroad.
| Sample (n = 248) | Population (N = 22,000) | History of a death whileabroad (n = 247) | ||||||
|---|---|---|---|---|---|---|---|---|
| Factor | n | % | % | 95% CI | Any death (%) | Death of family (%) | Death of friend (%) | Death of family and friends (%) |
| Total | 84.6 | 73.8 | 57.3 | 46.8 | ||||
| Sex | ||||||||
| Women | 172 | 69.4 | 69.4 | [63.2, 75.5] | 86.8 | 85.3 | 82.8 | 80.0 |
| Men | 76 | 30.6 | 30.6 | [24.5, 36.8] | 83.6 | 81.7 | 77.0 | 3.1 |
| Age (years) | ||||||||
| 18–25 | 35 | 14.1 | 14.1 | [8.9, 19.3] | 57.1*** | 51.6*** | 44.4*** | 34.8*** |
| 26–35 | 61 | 24.6 | 25.5 | [19.3, 31.8] | 85.0 | 83.6 | 76.9 | 73.5 |
| 36–45 | 103 | 41.5 | 40.2 | [31.9,48.2] | 89.3 | 88.2 | 85.5 | 83.3 |
| ≥46 | 49 | 19.8 | 20.3 | [14.6, 26.0] | 93.9 | 92.9 | 92.1 | 90.3 |
| Education | ||||||||
| <High school | 161 | 64.9 | 63.3 | [56.1, 70.6] | 87.6 | 85.9 | 82.9 | 79.6 |
| ≥High school | 87 | 35.1 | 36.7 | [29.4, 43.9] | 79.1 | 77.2 | 71.4 | 67.9 |
| Monthly income | ||||||||
| <$ 20,000 | 164 | 66.1 | 67.0 | [59.3, 74.8] | 84.1 | 82.6 | 77.8 | 74.5 |
| ≥$ 20,000 | 84 | 33.9 | 33.0 | [25.2, 40.7] | 85.5 | 83.3 | 81.0 | 76.9 |
| Marital status | ||||||||
| Married | 169 | 68.1 | 68.0 | [61.1, 74.8] | 83.5 | 80.9 | 77.6 | 72.3 |
| Single | 79 | 31.9 | 32.0 | [25.2, 38.9] | 85.1 | 83.7 | 79.5 | 76.6 |
| Years in US | ||||||||
| ≤10 years | 55 | 22.4 | 21.8 | [16.1,27.4] | 74.5* | 70.2** | 67.4* | 60.0* |
| 11–20 years | 125 | 50.8 | 50.8 | [44.7, 57.0] | 84.0 | 82.5 | 78.0 | 75.0 |
| >20 years | 66 | 26.8 | 27.5 | [20.5, 34.3] | 93.9 | 93.2 | 91.1 | 89.5 |
| Trauma | ||||||||
| No | 43 | 82.7 | 73.8* | 72.5* | 59.3** | 56.0** | ||
| Yes | 205 | 17.3 | 86.8 | 85.1 | 82.4 | 79.1 | ||
| Psychological distress | ||||||||
| Yes | 103 | 41.5 | 41.0 | [38.3, 48.6] | 43.5 | 40.4 | 48.6 | 44.8 |
p < .05.
p < .01.
p < .001.
Most participants reported having a history of transnational death (85%). Among those with a history of transnational death, the most prevalent death experienced pertained to the loss of family members (88%). Also, 63% of participants experienced the death of one or more friends from afar in addition to that of family members. Significant differences in the history of transnational death were observed across age groups, years living in the US, and history of trauma. Specifically, older undocumented Mexican immigrants were significantly more likely to experience a greater prevalence of having experienced any death from afar when compared to their younger counterparts (χ2 (3, N = 247) = 25.28, p < .001). Moreover, undocumented Mexican immigrants with longer time living in in the US were significantly more likely to have a history of a death from afar when compared to those with less time living in the US (χ2 (2, N = 247) = 8.70, p = .013). Participants with a history of trauma were significantly more likely to have a history of death from afar when compared to those without a history (χ2 (1, N= 247) = 4.54, p = .033). No significant differences in history of transnational death were observed across sex, education, or monthly household income (see Table 1).
Transnational death and psychological distress
After controlling for sex, age, education, monthly household income, years in the US, and history of trauma, the full model to assess for the association of history of transnational death (yes/no) and psychological distress was statistically significant, χ2 (10, N = 247) = 43.84, p < .001. The model fit using Cox and Snell R square was 0.16 and 0.22 when using Nagelkerke R squared. The model correctly classified 58.1% of cases. In this model, having a history of transnational death was a significant predictor of clinically significant psychological distress (OR = 2.47, 95% CI [0.97, 6.31], p = .053). Specifically, participants with a history of transnational death were 2.47 times more likely to meet criteria for clinically significant psychological distress when compared to those without a history (p = .030), even after controlling for history of trauma. In this model, sex, age, and history of trauma were also significantly associated with psychological distress in that men, participants who were older, and those with a history of trauma were more likely to meet criteria for clinically significant distress when compared to their women, younger, and no history of trauma counterparts (see Table 2).
Table 2.
Adjusted regression analyses for the association of death while abroad and clinically significant psychological distress.
| Variable | OR | 95% CI | p |
|---|---|---|---|
| Sex | |||
| Woman (Ref) | |||
| Men | 1.90 | [1.04,3.47] | .037 |
| Age | .003 | ||
| 18–25 (Ref) | |||
| 26–35 | 0.14 | [0.05, 0.42] | .000 |
| 36–45 | 0.19 | [0.07, 0.56] | .002 |
| ≥46 | 0.32 | [0.10, 1.01] | .053 |
| Education | |||
| <High school (Ref) | |||
| ≥High school | 1.21 | [0.63, 2.32] | .570 |
| Monthly income | |||
| <$ 20,000 (Ref) | |||
| ≥$ 20,000 | 0.57 | [0.31, 1.06] | .076 |
| Years in US | .083 | ||
| ≤10 years (Ref) | |||
| 11–20 years | 2.39 | [1.11, 5.18] | .027 |
| >20 years | 1.80 | [0.74, 4.37] | .197 |
| Trauma | |||
| No (Ref) | |||
| Yes | 4.06 | [1.62, 10.21] | .003 |
| Death while abroad | |||
| None (Ref) | |||
| Yes | 2.47 | [0.97,6.31] | .053 |
Transnational death, religiosity, and clinically significant psychological distress
In the models to assess for the effect of religiosity on psychological distress associated with experiencing transnational death, none of the interactions between religiosity (i.e., perceptions of religiosity, influence of religion, and church attendance) and experiencing a transnational death were significant in predicting psychological distress. Also, there was no main effect of religiosity on clinically significant psychological distress. Nonetheless, history of transnational death remained significantly associated with psychological distress in the model testing for the effect of church attendance on distress (OR = 2.56, 95% CI [0.98, 6.69], p = .054) (Table 3).
Table 3.
Summary of regression analysis for the moderating effect of religiosity on the association between death while abroad and psychological distress.
| Perceptions of religiosity | Influence of religion | Church attendance | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p |
| Sex | |||||||||
| Woman (Ref) | |||||||||
| Men | 1.83 | [0.99, 3.36] | .053 | 1.84 | [1.00,3.40] | .050 | 1.83 | [0.99, 3.37] | .053 |
| Age | .005 | .003 | .005 | ||||||
| 18–25 (Ref) | |||||||||
| 26–35 | 0.16 | [0.05, 0.46] | .001 | 0.14 | [0.05, 0.43] | .001 | 0.15 | [0.05, 0.46] | .001 |
| 36–45 | 0.22 | [0.12, 0.66] | .007 | 0.20 | [0.07, 0.60] | .004 | 0.22 | [0.07, 0.64] | .005 |
| ≥46 | 0.38 | [0.69, 1.25] | .111 | 0.35 | [0.11, 1.13] | .079 | 0.37 | [0.11, 1.20] | .097 |
| Education | |||||||||
| <High school (Ref) | |||||||||
| ≥High school | 1.35 | [0.69, 2.62] | .384 | 1.33 | [0.68, 2.59] | .409 | 1.23 | [0.64, 2.37] | .540 |
| Monthly income | |||||||||
| <$ 20,000 (Ref) | |||||||||
| ≥$ 20,000 | 0.58 | [0.58, 0.31] | .095 | 0.55 | [0.29, 1.03] | .062 | 0.59 | [0.31, 1.11] | .099 |
| Years in US | .097 | .106 | .085 | ||||||
| ≤10 years (Ref) | |||||||||
| 11–20 years | 2.31 | [1.06,5.03] | .035 | 2.32 | [1.06, 5.06] | .035 | 2.38 | [1.09, 5.18] | .029 |
| >20 years | 1.64 | [0.66, 4.05] | .283 | 1.79 | [0.73, 4.39] | .206 | 1.69 | [0.69, | .255 |
| Trauma | |||||||||
| No (Ref) | |||||||||
| Yes | 4.12 | [1.63,10.43] | .003 | 4.03 | [1.59,10.17] | .003 | [1.61, 10.43] | .003 | |
| Death while abroad | 4.10 | ||||||||
| None (Ref) | |||||||||
| Yes | 2.36 | [0.91, 6.14] | .077 | 2.50 | [0.97, 6.47] | .059 | 2.56 | [0.98, 6.69] | .054 |
| Religiosity | 0.75 | [0.18, 3.38] | .746 | 1.28 | [0.37, 4.43] | .694 | 0.79 | [0.49, 1.27] | .332 |
| Death while abroad × religiosity | 0.89 | [0.20, 4.05] | .879 | 0.50 | [0.14, 1.86] | .303 | 1.09 | [0.65, 1.82] | .749 |
Discussion
The first aim of our study was to identify the association between history of transnational death and clinically significant psychological distress among undocumented Mexican immigrants. Having experienced the death of a loved one from afar is highly prevalent in this population, with the most common loss being that of a family member. Also, having a history of transnational death was associated with clinically significant distress after controlling for relevant covariates. Experiencing transnational death can be distressing for any immigrant due to the cost of traveling home and is particularly stressful for the undocumented considering the pros and cons of traveling back to their country of origin. Consistent with the concept of disenfranchised grief, losing a loved one from afar can be particularly distressing for immigrants who either have to stay home or risk capture and deportation to be with their family. Research shows that the distress suffered by these immigrants as a result of transnational death is often accompanied by sadness and guilt, which often remains long after the loss (Bravo, 2017). Little is known about the experience of transnational death in this marginalized population. To our knowledge, this is the first study to capture the magnitude of the problem, including how distressing this experience may be from a clinical perspective. Consistent with our approach, future studies should continue to focus on addressing translational death in this population from the perspective of disenfranchised grief to increase awareness of the contextual barriers that these immigrants face while also challenging existing stereotypes (e.g., blaming the immigrant for being away and abandoning the family). This information is essential to protect their human rights and those of their US-born family members.
Additionally, our study identified several vulnerabilities associated with the history of transnational death. For instance, particularly at the risk of transnational death were undocumented immigrants who were older, those who have lived longer in the US, and those with a history of trauma. The aforementioned findings highlight the heterogeneity of this immigrant population, which is often overlooked and mistaken as a one-size-fits-all. These findings are particularly important because of the marginalization and stigmatization of immigrant populations. The need for advocacy, policy, and intervention efforts that address the mental health needs of undocumented immigrants most at-risk of transnational death is a must, and of particular importance is to focus on those who have made the US their home after residing in this country for so long while also enduring hardship and trauma. Given that disenfranchised grief involves the stigma or lack of acknowledgment of grief that limits an individual’s ability to grieve, interventions are especially necessary to provide services that protect undocumented immigrants from the stigma associated with disenfranchised grief.
Another aim of our study was to examine the effect of different aspects of religiosity on the association between history of transnational death and clinically significant psychological distress among undocumented Mexican immigrants. Although religiosity has been previously identified as being frequently used for coping with distressing events among undocumented Mexican immigrants (Cobb et al., 2016), our results did not support an effect of religiosity on psychological distress in our population. It is possible that our inconsistent finding may be due to limited statistical power to detect a significant effect given that the majority of our sample had experienced transnational death. Another tentative hypothesis is that religiosity is a complex construct to assess given variations in its operational definition, its components, and its measurement (Becker, Xander, Blum, & Higginson, 2007). It is likely that other aspects of religiosity not assessed in this study (e.g., locus of control, beliefs in the afterlife, and religious rituals) may help diminish distress associated with transnational death. Future studies are needed that can incorporate the use of mixed-methods to identify specific facets religiosity that may diminish distress in this at-risk population during this difficult grieving time.
Our findings have important public health and clinical implications. The high prevalence of transnational death and its association with psychological distress among undocumented Mexican immigrants underscore the importance of facilitating access to contextually and culturally sensitive interventions and mental health services aimed at assisting this population when facing bereavement from afar. Undocumented immigrants are a marginalized population with limited access to healthcare, including mental health and counseling services. Our findings support that experiencing transnational death while having an undocumented status is significantly associated with clinical levels of psychological distress that may often require psychological intervention, which is not available to this population. Identifying nontraditional sources of service delivery for these at-risk immigrants, such as through faith-based organizations or advocacy agencies, could facilitate access to much needed educational and counseling resources. Our hope is that the aforementioned findings will motivate awareness, advocacy, and intervention efforts across disciplines that are aimed at addressing the mental health needs of marginalized immigrants, particularly in the face of adversity. Moreover, clinical recommendations for the development of bereavement interventions for this population include sensitivity to emotions that may stem from the immigrant’s inability to travel home when a loved one dies (e.g., anger and guilt), validation of emotions, facilitation of problem solving and decision making that could prevent making risky and impulsive decisions (e.g., engaging in dangerous border crossing, abruptly leaving the US without considering consequences), assistance in the development of culturally and contextually-sensitive skills to facilitate the bereavement process (e.g., using communication technology and social media to keep contact with family/friends abroad, reliance on existing support networks, goal setting), use of techniques that facilitate the integration of context in therapy (e.g., life narrative), and awareness of family dynamics in the expression of distress so as to facilitate the healing process. Undocumented immigrants are a highly resilient population despite the many challenges that they face (Garcini et al., 2017); nevertheless, to maintain their resilient spirit, it is important to provide these immigrants with the necessary contextually and culturally-appropriate resources to facilitate healing in the face of hardship.
Limitations
Our study makes a timely and significant contribution to identifying transnational death as a relevant stressor among undocumented immigrants, which is associated with clinically significant distress. Nevertheless, this study has some limitations. First, RDS is an effective method to study hidden populations (Heckathorn, 1997), yet it is not free from methodological limitations (Goel & Salganik, 2010). Nonetheless, steps were taken in this study to collect data from a representative sample (i.e., formative research, pre-selection of diverse seeds, long recruitment chains, use of weighted estimates based on the size of social network, accurate assessment of social network size). Also, psychological distress in this border community may be different from that experienced by undocumented immigrants in other parts of the US or from immigrants from other countries of origin. Moreover, our sample was predominantly female and on average, participants had lived in the US. for more than 10 years. Thus, our data is most representative of established undocumented Mexican women most of whom are living in mixed status families. Furthermore, given the lack of information on the prevalence of transnational bereavement and its associated distress in this immigrant population, this study was exploratory; thus, it is limited by the scope of the bereavement questions asked. Also, we did not include a grief measure as not everyone in the study had experienced death, as well as to minimize the distress experienced given that access to counseling services is limited for these immigrants. Future studies should include a more in-depth study of the many factors that influence transnational bereavement (e.g., closeness with the deceased, type of death) along with the use of open-ended questions to better understand the grieving experience among different subgroups of undocumented immigrants. Moreover, assessments were based on retrospective reporting, which may result in lower estimates of events and distress than contemporaneous reporting (Brewin, Andrews, & Gotlib, 1993). Finally, this study was cross-sectional; thus, causation cannot be inferred.
Conclusion
Overall, our findings underscore the need to address transnational bereavement among undocumented immigrants from a framework of disenfranchised grief, which is often associated with psychological distress that requires treatment. The high prevalence of transnational death associated with psychological distress in this population requires interdisciplinary collaboration and nontraditional sources of service delivery for the provision of culturally and contextually-sensitive interventions that can best address the complex needs of this marginalized group about which little is known. Despite being a highly resilient population that faces many challenges and daily stressors, it is necessary to provide undocumented immigrants with tools and avenues to facilitate healing in the face of transnational death within the context of marginalization and stigmatization so as to protect their wellbeing and preserve their resilient spirit.
Funding
Data collection and preparation of the manuscript was supported by the Ford Foundation Fellowship Program and a grant and diversity supplement from the National Heart, Lung and Blood Institute (1R01HL127260-01) and National Institutes of Health.
Footnotes
Disclosure statement
The authors of this manuscript have no conflict of interests to disclose.
References
- Aiken LS, & West SG (1991). Multiple regression: Testing and interpreting interactions. Newbury Park, CA: Sage Publications. [Google Scholar]
- Beaton D, Bombardier C, Guillemin F, & Ferraz MB (2002). Recommendations for the cross-cultural adaptation of health status measures (pp. 1–9). New York, NY: American Academy of Orthopaedic Surgeons. [Google Scholar]
- Becker G, Xander CJ, Blum HE, Lutterbach J, Momm F, Gysels M, & Higginson IJ (2007). Do religious or spiritual beliefs influence bereavement? A systematic review. Palliative Medicine, 21(3), 207–217. doi: 10.1177/0269216307077327 [DOI] [PubMed] [Google Scholar]
- Bravo V (2017). Coping with dying and deaths at home: How undocumented migrants in the United States experience to process of transnational grief. Mortality, 22(1), 33–44. doi: 10.1080/13576275.2016.1192590 [DOI] [Google Scholar]
- Brewin CR, Andrews B, & Gotlib IH (1993). Psychopathology and early experience: A reappraisal of retrospective reports. Psychology Bulletin, 113(1), 82–98. doi: 10.1037/0033-2909.113.1.82 [DOI] [PubMed] [Google Scholar]
- Byrne GJ, & Raphael B (1997). The psychological symptoms of conjugal bereavement in elderly men over the first 13 months. International Journal of Geriatric Psychiatry, 12(2), 241–251. doi: [DOI] [PubMed] [Google Scholar]
- Cervantes RC, Fisher DG, Padilla AM, & Napper LE (2015). The Hispanic stress inventory version 2: Improving the assessment of acculturation stress. Psychological Assessment, 28, 509–522. doi: 10.1037/pas0000200 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cervantes RC, Padilla AM, & Salgado de Snyder N (1991). The Hispanic stress inventory: A culturally relevant approach to psychosocial assessment. Psychosocial Assessment, 3(3), 438–447. doi: 10.1037/1040-3590.3.3.438 [DOI] [Google Scholar]
- Cobb CL, Sanders GL, & Xie DP (2016). Coping styles and depression among undocumented Hispanic immigrants. Journal of Immigrant and Minority Health, 18(4), 864–870. doi: 10.1007/s10903-015-0270-5 [DOI] [PubMed] [Google Scholar]
- Dean AG, Sullivan KM, & Soe MM (2013). OpenEpi: Open source epidemiologic statistics for public health, version. 3.01. Retrieved from www.OpenEpi.com [Google Scholar]
- Derogatis LR (1993). BSI brief symptom inventory: Administration, scoring, and procedure manual (4th ed). Minneapolis, MN: National Computer Systems. [Google Scholar]
- Doka K (2002). Disenfranchised grief In Doka Kenneth J (Ed.), Living with grief: Loss in later life (pp. 159–168). Washington, DC: The Hospice Foundation of America. [Google Scholar]
- Garcini LM, Murray KE, Zhou A, Klonoff EA, Myers MG, & Elder JP (2016). Mental health of undocumented immigrants in the United States: A systematic review of methodology and findings. Journal of Immigrant and Refugee Studies, 14(1), 1–25. doi: 10.1080/15562948.2014.998849 [DOI] [Google Scholar]
- Garcini LM, Peña JM, Gutierrez AP, Fagundes CP, Lemus H, Lindsay S, & Klonoff EA (2017). “One scar too many:” The associations between traumatic events and psychological distress among undocumented Mexican immigrants. Journal of Traumatic Stress, 30(5), 453–462. doi: 10.1002/jts.22216 [DOI] [PubMed] [Google Scholar]
- Gile KJ (2011). Improved inference for respondent-driven sampling data with application to HIV prevalence estimation. Journal of the American Statistical Association, 106(493), 135–146. doi: 10.1198/jasa.2011.ap09475 [DOI] [Google Scholar]
- Goel S, & Salganik MJ (2010). Assessing respondent-driven sampling. Proceedings of the National Academy of Sciences, 107(15), 6743–6747. doi: 10.1073/pnas.1000261107 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Handcock MS, Fellows IE, & Gile KJ (2014). RDS analyst: Software for the analysis of respondent-driven sampling data. Version 0.42. Retrieved from http://wiki.stat.ucla.edu/hpmrg/index.php/RDS_Analyst_Install
- Heckathorn DD (1997). Respondent driven sampling: A new approach to the study of hidden populations. Social Problems, 44 (2), 174–199. doi: 10.2307/3096941 [DOI] [Google Scholar]
- Hovey JD (2000). Psychosocial predictors of acculturative stress in Mexican immigrants. Journal of Psychology, 134, 480–502. doi: 10.1080/00223980009598231 [DOI] [PubMed] [Google Scholar]
- Hovey JD, & Magana CG (2002). Psychosocial predictors of anxiety among immigrant Mexican farmworkers: Implications for prevention and treatment. Cultural Diversity and Ethnic Minority Psychology, 8(3), 274–289. doi: 10.1037/1099-9809.8.3.274 [DOI] [PubMed] [Google Scholar]
- Krogstad JM, Passel JS, & Cohn D (2017). 5 facts about illegal immigration in the U.S Retrieved from http://www.pewresearch.org/fact-tank/2017/04/27/5-facts-about-illegal-immigration-in-the-u-s/ [Google Scholar]
- Mollica RF, Mcdonald LS, Masagli MP, & Silove DM (2004). Measuring Trauma Measuring Torture: Instructions and Guidance on the Utilization of the Harvard Program in Refugee Trauma’s Versions of the Hopkins Symptom Checklist-25 (HSCL-25), The Harvard Trauma Questionnaire (HTQ). Cambridge: Harvard Program in Refugee Trauma. [Google Scholar]
- Montealegre JR, Risser JM, Selwyn BJ, Sabin K, & McCurdy SA (2012). HIV testing behaviors among undocumented Central American immigrant women in Houston, Texas. Journal of Immigrant and Minority Health, 14(1), 116–123. doi: 10.1007/s10903-011-9534-x [DOI] [PubMed] [Google Scholar]
- Meyer IH (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychological Bulletin, 129(5), 674. doi: 10.1037/0033-2909.129.5.674 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peña JM, Garcini LM, Gutierrez AP, Ulibarri MD, & Klonoff EA (2016). Traumatic events and symptoms among Mexican deportees in a border community. Journal of Immigrant & Refugee Studies, 15, 36–52. doi: 10.1080/15562948.2016.1158341 [DOI] [Google Scholar]
- Ransford HE, Carillo FR, & Rivera Y (2010). Health care-seeking among Latino immigrants: Blocked access, use of traditional medicine, and the role of religion. Journal of Health Care for the Poor and Underserved, 21(3), 862–878. doi: 10.1353/hpu.0.0348 [DOI] [PubMed] [Google Scholar]
- Solheim C, Zaid S, & Ballard J (2016). Ambiguous loss experienced by transnational Mexican immigrant families. Family Process, 55(2), 338–353. doi: 10.1111/famp.12130 [DOI] [PubMed] [Google Scholar]
- Stroebe W, & Schut H (2001). Risk factors in bereavement outcome: A methodological and empirical review In Stroebe MS, Hansson RO, Stroebe W, Schut H, Stroebe MS, Hansson RO, … Schut H(Eds.), Handbook of bereavement research: Consequences, coping, and care (pp. 349–371). Washington, DC: American Psychological Association. doi: 10.1037/10436-015 [DOI] [Google Scholar]
- Stroebe M, Stroebe W, & Abakoumkin G (2005). The broken heart: Suicidal ideation in bereavement. The American Journal of Psychiatry, 162(11), 2178–2180. doi: 10.1176/appi.ajp.162.11.2178 [DOI] [PubMed] [Google Scholar]
- Tarrant M, Dazeley S, & Cottom T (2009). Social categorization and empathy for outgroup members. British Journal of Social Psychology, 48, 427–446. doi: 10.1348/014466608X373589 [DOI] [PubMed] [Google Scholar]
- Thoresen CE, Harris AHS, & Oman D (2001). Spirituality, religion, and health: Evidence, issues, and concerns In Plante TG & Sherman AC (Eds.), Faith and health (pp. 15–52). New York, NY: Guilford. [Google Scholar]
- Tyldum G, & Johnston LG (2014). Applying respondent driven sampling to migrant populations: Lessons from the field. Basingstoke, UK: Palgrave MacMillan. [Google Scholar]
- Vromans L, Schweitzer RD, & Brough M (2012). The multidimensional loss scale: Validating across-cultural instrument for measuring loss. The Journal of Nervous and Mental Disease, 200(4), 349–357. [DOI] [PubMed] [Google Scholar]
- Zhang SX (2012). Trafficking of migrant laborers in San Diego County: Looking for a hidden population. San Diego, CA: San Diego State University. [Google Scholar]