

Abstract
Background
The optimal nutritional support for critically ill septic patients remains unknown. This study evaluates the associations of macronutrient intake during the first week of intensive care unit (ICU) admission and long‐term clinical outcomes in septic and non‐septic patients.
Methods
Prolonged mechanically ventilated patients were retrospectively studied. The association of protein (low: <0.8 g/kg/d, medium: 0.8–1.2 g/kg/d, high >1.2 g/kg/d) and energy intake (<80%, 80%–110%, 110% of target) during days 1–3 and 4–7 after ICU admission and 6‐month mortality was analyzed for septic and non‐septic patients separately.
Results
A total of 423 patients were investigated. Of these, 297 had sepsis. In the sepsis group, medium protein intake at days 4–7 was associated with lower 6‐month mortality (hazard ratio [HR]: 0.646, 95% confidence interval [CI]: 0.418‐0.996, P=0.048) compared with high intake. In the non‐sepsis group, early high and late low protein intake were associated with higher 6‐month mortality (HR: 3.902, 95% CI: 1.505‐10.115, P=0.005; HR: 2.642, 95% CI: 1.128‐6.189, P=0.025) compared with low and high protein intake, respectively. For energy intake, late energy intake of >110% was associated with decreased mortality in septic patients (HR: 0.400, 95% CI: 0.222‐0.721, P=0.002), whereas in non‐septic patients, late medium energy intake (80%–110%) was associated with better survival (HR: 0.379, 95% CI: 0.175‐0.820, P=0.014), both compared with low energy intake.
Conclusion
Divergent associations of macronutrient intake were found; early high protein intake in non‐septic patients, but not in septic patients, was found to be associated with higher 6‐month mortality.
Keywords: autophagy, critical care nutrition, energy, mortality, protein, sepsis
Clinical Relevancy Statement
Our findings may indicate that septic and non‐septic patients have different nutritional needs in the first week of intensive care unit (ICU) admission. Moreover, divergent time‐dependent associations of protein intake were observed. However, current guidelines suggest similar nutrition needs during ICU admission, neglecting subgroups and time‐dependent effects. This hypothesis‐generating study underlines the need for large prospective trials to develop more tailor‐based approaches for nutrition in critically ill patients.
Introduction
Sepsis is a syndrome defined by life‐threatening organ dysfunction because of a dysregulated host response to infection.1 Sepsis accounts for 10% of all intensive care unit (ICU) admissions in the Netherlands and results in a marked in‐hospital mortality of 28% compared with 13% in general non‐septic ICU patients.2 Optimal nutrition support in critically ill patients is associated with lower mortality and long‐term outcome3; however, evidence in septic patients is scarce.4, 5 Although septic patients are considered a subgroup of critically ill patients and guidelines suggest similar nutrition needs, they may not experience the same level of inflammation, severity of illness, and metabolic changes (ie, changes in energy expenditure and protein catabolism) as compared with non‐septic patients.6
Protein Intake
Protein intake is essential to prevent muscle loss; however, muscle loss cannot be completely counteracted by nutrition support.7 It has been suggested that protein intake may be more important than energy intake.8 Most observational studies found that higher protein intake was associated with better outcomes in general ICU and septic patients.9, 10, 11, 12 However, this is not supported by few randomized controlled trials (RCTs) that have been performed in general ICU patients13, 14, 15 and other evidence from septic patients.16, 17 Presumably, timing of nutrition interventions18 might play an important role, and especially early (≤3 days) high protein intake may relate to negative effects.19 Suggestions have been made that early protein intake inhibits autophagy.20 Autophagy is essential to clear cell debris and intracellular bacteria in order to provide metabolic precursors.21 Moreover, it has been related to cell survival and adverse outcomes.22
However, the interplay of nutrition, catabolism, inflammation, and autophagy is not well understood. Furthermore, the clinical implications and the role of autophagy preservation by adjustment of protein provision in severely catabolic ICU patients remains debated.23
Energy Provision
For energy intake, recent RCTs do not report survival benefit of early provision of approximately 100% of energy expenditure compared with lower energy intakes.14, 24, 25 Furthermore, overfeeding (>110%) has been associated with increased morbidity and mortality.17, 26 Most observational studies have reported the lowest mortality rate associations with energy intakes of 70%–90% of calculated or measured energy expenditure.17, 27
Most of the aforementioned studies included general critically ill patients, and percentages of patients with sepsis are frequently unknown or relatively low. Subgroup analyses for septic patients were not performed. Therefore, the optimal amount and timing of nutrition intake in septic patients remains unknown. Our primary aim was to evaluate the effects of protein and energy intake and the timing of these interventions in critically ill septic patients during the first week of ICU admission on 6‐month mortality and to compare findings with non‐septic patients. We expected to find a stronger association of early high protein intake and higher 6‐month mortality in septic patients than in non‐septic patients, speculating that early high protein intake suppresses autophagy, which could play a more prominent role in septic patients.
Methods
Study Description
We performed a retrospective observational study among all consecutive, critically ill, mechanically ventilated patients in a mixed medical‐surgical ICU in a tertiary university‐affiliated teaching hospital between January 1, 2011, and April 1, 2016. Sepsis was defined as a suspected or proven infection within the first 24 hours of ICU admission, in combination with a Sequential Organ Failure Assessment (SOFA) score at admission of ≥2, concordant with the new sepsis‐3 definitions.1, 28 Outcomes of patients with and without sepsis were compared.
Patient Population
Patients were eligible for analysis if they were >18 years old and received invasive mechanical ventilation for ≥7 days, commenced within 48 hours after ICU admission. Patients were excluded from analysis when no nutrition data were available, when their condition affected their nutrition demand (ie, pregnancy, preexistent neuromuscular diseases, chronic hemodialysis and [protein] malabsorption syndromes), or when they were on noninvasive or chronic home ventilation. If patients were readmitted to the ICU within 6 months, only data of the first admission were analyzed.
Baseline characteristics such as age, gender, admission type and diagnosis, baseline blood tests, SOFA score,28 Acute Physiology and Chronic Health Evaluation II score,29 Charlson Comorbidity Index,30 Nutrition Risk in Critically Ill Patients score,31 need for vasopressor agents, and presence of shock were used to assess baseline differences.
Subgroup Analyses
Predefined subgroup analyses were performed addressing protein and energy intake in the first 7 days of ICU admission. Both were divided into 3 groups: protein intake <0.8 g/kg/d, 0.8–1.2 g/kg/d, and >1.2 g/kg/d17 and energy intake <80%, 80%–110%, and >110% of energy target.17, 26, 32 Energy intake, including energy from trisodium citrate, propofol, and glucose infusions, was monitored during complete ICU stay according to published methods.33, 34, 35
Target protein prescriptions were 1.5 g/kg/d for patients with body mass index (BMI) <27 kg/m2; in case of BMI 27–30, weight was corrected to BMI 27. In case of BMI >30, ideal weight was used and target protein administration was set to 2.0 g/kg/d (BMI 30–40) or 2.5 g/kg/d (BMI >40).5 Energy targets were calculated by our computerized nutrition protocol based on the Food and Agricultural Organization and World Health Organization (FAO/WHO) formula.36 In this study, 20% was added to resting energy expenditure to correct for disease activity.37 Additionally, energy targets were calculated using the ventilator‐derived carbon dioxide output (VCO2; L/min) using VCO2 × 8.19.38
Outcome
Primary outcome was 6‐month mortality. Dates of death were collected from the municipal administration on October 1, 2016. Secondary outcomes were ICU and in‐hospital mortality, length of stay (LOS), 6‐month all‐cause hospital readmission, ventilator‐free days, and presence of acute kidney injury according Risk, Injury, Failure, Loss of kidney function, and End‐stage kidney disease criteria.39
Data Collection and Protection
Data were automatically extracted using SAS Enterprise Guide queries from Metavision (Patient Data Management System, iMDsoft MetaVision, Tel Aviv, Israel) and other hospital electronic patient records. Verification was performed manually. Collected data were deidentified and stored on a secure hospital computer. There were no identifiable paper documents.
Ethics Approval
The Gelderse Vallei Hospital Institutional Review Board approved the study and waived informed consent for reasons of the retrospective design and anonymization of patient identifiers before analysis.
Statistical Analysis
Continuous data are reported as mean and standard deviation (SD) or as median and interquartile range [IQR], depending on data distribution. Differences in continuous variables were analyzed using independent t‐tests or Mann‐Whitney U tests where appropriate. Categorical variables are presented as frequencies and percentages. Differences were analyzed using χ2 or Fischer's exact tests. Six‐month mortality was assessed by χ2 test, Kaplan‐Meier survival functions, and Cox proportional hazards models. All baseline and nutrition variables (Tables 1 and 2) were included in unadjusted Cox regression analysis. For the primary outcome measure, when univariate analysis revealed P < 0.10, multivariate analysis was performed. Multicollinearity of variables included into multivariate analyses was assessed by calculation of the variance inflation factor (VIF). We considered a VIF >2 as an indicator of relevant collinearity. Results of multivariate Cox regression will only be included in supplementary material for illustrative reasons because of small sample sizes (Tables S1–S3). Leave‐1‐out cross‐validation of the univariate Cox regression was performed for admission year. Analyses were performed using IBM SPSS Statistics for Windows and for Macintosh, version 23.0 (IBM Corporation, released 2013, Armonk, New York, USA). A P value < 0.05 was considered statistically significant.
Table 1.
Baseline Characteristics
| Variable | Total, n = 423 | Sepsis, n = 297 | No Sepsis, n = 126 | P a |
|---|---|---|---|---|
| Gender, male, n (%) | 253 (59.8) | 166 (55.9) | 87 (69.0) | 0.013e |
| Age, years, median [IQR] | 71 [62–77] | 71 [61–77] | 71 [63.8–77.3] | 0.538 |
| BMI, kg/m2, median [IQR] | 26.6 [23.6–30.5] | 26.6 [23.5–29.9] | 26.7 [24.4–30.7] | 0.278 |
| <25, n (%) | 156 (36.9) | 111 (37.4) | 45 (35.7) | |
| 25–35, n (%) | 225 (53.2) | 159 (53.5) | 66 (52.4) | |
| >35, n (%) | 42 (9.9) | 27 (9.1) | 15 (11.9) | |
| APACHE II score on admission, mean (SD) | 23.4 (7.0) | 23.1 (5.72) | 24.2 (7.3) | 0.143 |
| SOFA score on admission, mean (SD) | 8.1 (3.0) | 8.1 (3.1) | 8.1 (2.9) | 0.858 |
| SOFA <2, n (%) | 2 (0.5) | 0 | 2 (1.6) | |
| SOFA ≥2, n (%) | 421 (99.5) | 297 (100) | 124 (98.4) | |
| Charlson Comorbidity Index, mean (SD)b | 4.2 (2.4) | 4.2 (2.5) | 4.1 (2.1) | 0.914 |
| Nutric score, mean (SD) | 5.1 (1.8) | 5.1 (1.8) | 5.2 (1.7) | 0.408 |
| Nutric score 0–4, n (%) | 154 (36.4) | 113 (38.0) | 41 (32.5) | |
| Nutric score ≥5, n (%) | 269 (63.6) | 184 (62.0) | 85 (67.5) | |
| Baseline creatinine, μmol/L, median [IQR] | 101 [73–147] | 101 [72–164] | 99 [74–124] | 0.171 |
| Admission type | 0.067 | |||
| Medical, n (%) | 282 (66.7) | 208 (70.0) | 74 (58.7) | |
| Elective surgical, n (%) | 61 (14.4) | 37 (12.5) | 24 (19.0) | |
| Emergency surgery, n (%) | 80 (18.9) | 52 (17.5) | 28 (22.2) | |
| Positive SIRS criteria on admissionc | <0.001e | |||
| <2, n (%) | 44 (10.4) | 21 (7.1) | 23 (18.3) | |
| ≥2, n (%) | 339 (80.1) | 255 (85.9) | 84 (66.7) | |
| Missing data, n (%) | 40 (9.5) | 21 (7.1) | 19 (15.1) | |
| Vasopressors first 24 hours of ICU admission | 0.327 | |||
| Yes, n (%) | 258 (61) | 186 (62.6) | 72 (57.1) | |
| No, n (%) | 165 (39) | 111 (37.4) | 54 (42.8) | |
| Shock first 24 hours of ICU admissiond | 0.338 | |||
| Yes, n (%) | 194 (45.9) | 141 (47.5) | 53 (42.1) | |
| No, n (%) | 229 (54.1) | 156 (52.5) | 73 (57.9) | |
| Site of initial infection | NA | NA | NA | |
| Lung, n (%) | 153 (51.5) | |||
| Abdomen, n (%) | 98 (33.0) | |||
| Urinary tract, n (%) | 19 (6.4) | |||
| Neurologic site, n (%) | 7 (2.4) | |||
| Primary bloodstream, n (%) | 2 (0.7) | |||
| Skin and soft tissue | 9 (3.0) | |||
| Other | 9 (3.0) |
APACHE II, Acute Physiology and Chronic Health Evaluation; BMI, body mass index; ICU, intensive care unit; IQR, interquartile range (1st–3rd quartile); NA, not applicable; NUTRIC, Nutritional Risk in Critically Ill; SIRS, systemic inflammatory response syndrome; SOFA, Sequential Organ Failure Assessment; SD, standard deviation.
Comparison of sepsis and non‐sepsis group, calculated by Pearson's χ2 test, independent t‐test or Mann‐Whitney U test as appropriate.
Charlson Comorbidity Index predicts 10‐year mortality from 22 comorbid conditions.
SIRS criteria: leucocytes <4 × 109/L or >12 × 109/L, respiratory rate >20 breaths/min, heart rate >90 beats/min, temperature <36.0°C or >38.3°C.
Shock was defined as the need for vasopressors the first 24 hours after ICU admission and lactate >2 mmol/L.
P < 0.05.
Table 2.
Feeding Parameters
| Variable | Total Population, n = 423 | Sepsis, n = 297 | No Sepsis, n = 126 | P a |
|---|---|---|---|---|
| Time to start feeding, hours, median [IQR] | 6.0 [3.2–15.5] | 6.1 [3.3–14.5] | 5.7 [2.9–17.2] | 0.844 |
| Patients parenterally fed, days 1–3, n (%) | 40 (9.5) | 33 (11.1) | 7 (5.6) | 0.074 |
| Patients parenterally fed, days 4–7, n (%) | 39 (9.2) | 29 (9.8) | 10 (7.9) | 0.552 |
| Protein intake | ||||
| Daily protein target, g, mean (SD) | 115.5 (20.9) | 113.8 (20.6) | 119.3 (21.2) | 0.013e |
| Total protein intake 7 days, g, mean (SD) | 522.19 (154.6) | 517.5 (148.0) | 532.8 (169.1) | 0.352 |
| Protein intake days 1–3, g/kg/d, median [IQR] | 0.72 [0.42–0.97] | 0.75 [0.44–0.99] | 0.59 [0.34–0.91] | 0.010e |
| <0.8, n (%) | 249 (58.9) | 166 (55.9) | 83 (65.9) | |
| 0.8–1.2, n (%) | 140 (33.1) | 103 (34.78) | 37 (29.4) | |
| >1.2, n (%) | 34 (8.0) | 28 (9.4) | 6 (4.8) | |
| Protein intake days 4–7, g/kg/d, mean (SD) | 1.21 (0.30) | 1.21 (0.31) | 1.21 (0.29) | 0.976 |
| <0.8, n (%) | 35 (8.3) | 24 (8.1) | 11 (8.7) | |
| 0.8–1.2, n (%) | 161 (38.1) | 116 (39.1) | 45 (35.7) | |
| >1.2, n (%) | 227 (53.7) | 157 (52.9) | 70 (55.6) | |
| Energy intake | ||||
| Daily energy target in kcalb, mean (SD) | 1704 (324) | 1694 (321) | 1727 (331) | 0.340 |
| Daily energy target in kcal, based on VCO2 c, mean (SD) | 1818 (366) | 1798 (376) | 1863 (340) | 0.234 |
| Total energy intake in kcald, mean (SD) | 9871 (2436) | 9877 (2419) | 9857 (2486) | 0.937 |
| Adequacy energy intake to targetb , d, days 1–3, mean % (SD) | 67.2 (28.6) | 69.4 (28.5) | 62.1 (28.3) | 0.016e |
| <80%, n (%) | 268 (63.4) | 178 (59.9) | 90 (71.4) | |
| 80%–110%, n (%) | 130 (30.7) | 102 (34.3) | 28 (22.2) | |
| >110%, n (%) | 25 (5.9) | 17 (5.7) | 8 (6.3) | |
| Adequacy energy intake to targetb , d, days 4–7, mean % (SD) | 107 (25) | 107 (24) | 107 (27) | 0.760 |
| <80%, n (%) | 49 (11.6) | 34 (11.4) | 15 (11.9) | |
| 80%–110%, n (%) | 233 (55.1) | 158 (53.2) | 75 (59.5) | |
| >110%, n (%) | 141 (33.3) | 105 (35.4) | 36 (28.6) | |
| Non‐nutrition energy as % of total energy intake, median [IQR] | 7.7 [3.6–15.7] | 7.6 [4.0–15.9] | 8.5 [3.0–15.0] | 0.886 |
IQR, interquartile range; SD, standard deviation.
Comparison of sepsis with non‐sepsis group, calculated with t‐test or Mann‐Whitney U test where appropriate.
Target based on World Health Organization formula for resting energy expenditure + 20%.
Target based on mean daily VCO2 × 8.19.
Nutritional + non‐nutritional energy.
P < 0.05.
Results
Patients
During the study period, 3839 patients were admitted, of which 552 received invasive mechanical ventilation for ≥7 days, and of these, 423 were eligible for analysis (Figure S1). Sepsis was present in 297 patients (70.2%).
Baseline characteristics of the studied patients are depicted in Table 1. Except for gender (sepsis group 56% men vs non‐sepsis 69% men, P = 0.013) and systemic inflammatory response syndrome, criteria baseline characteristics were comparable between groups. Regarding nutrition parameters (Table 2), protein intake in the first 3 days after admission was significantly higher in the sepsis group (0.75 vs 0.59 g/kg/d, P = 0.010), despite significantly lower targets (114 vs 119 g/d, respectively, both 1.5 g/kg/d according to real or corrected body weight, P = 0.013). In addition, a higher percentage of energy target was achieved in septic patients in the first 3 days (69.4% vs 62.1%, P = 0.016), even though targets were comparable.
Primary Outcome
Six‐month mortality did not significantly differ between the sepsis and the non‐sepsis group (104 [35.0%] vs 49 [38.9%], respectively, P = 0.448).
Subgroup Analysis: Proteins
The effects of protein intake during the early (days 1–3) and later phase (days 4–7) of the first week were evaluated separately. In septic patients, no association was found between protein intake at days 1–3 and 6‐month mortality (Table 3, Figure S2, Table S4). In the later phase, protein intake of 0.8–1.2 g/kg/d was significantly associated with a lower 6‐month mortality in univariate analysis (hazard ratio [HR]: 0.646, 95% confidence interval [CI]: 0.418–0.996, P = 0.048) compared with the high (>1.2) protein intake subgroup (Table 3, Figure S3).
Table 3.
Univariate Cox Proportional Hazards Model 6‐Month Mortality: Proteins‐Separated Early and Later Phase
| Protein Intake | Sepsis | No Sepsis | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intake Subgroups | n | Mean | β | HR | 95% CI | P | n | Mean | β | HR | 95% CI | P |
| Days 1–3, g/kg/d | ||||||||||||
| <0.8 | 166 | 0.47 | Reference | 83 | 0.41 | Reference | ||||||
| 0.8–1.2 | 103 | 0.98 | 0.146 | 1.157 | (0.764–1.752) | 0.491 | 37 | 0.99 | −0.116 | 0.891 | (0.466–1.702) | 0.726 |
| >1.2 | 28 | 1.34 | 0.367 | 1.444 | (0.772–2.699) | 0.250 | 6 | 1.25 | 1.362 | 3.902 | (1.505–10.115) | 0.005a |
| Days 4–7, g/kg/d | ||||||||||||
| <0.8 | 24 | 0.55 | 0.496 | 1.643 | (0.902–2.994) | 0.105 | 11 | 0.64 | 0.971 | 2.642 | (1.128–6.189) | 0.025a |
| 0.8–1.2 | 116 | 1.03 | −0.438 | 0.646 | (0.418–0.996) | 0.048a | 45 | 1.03 | 0.461 | 1.585 | (0.865–2.905) | 0.136 |
| >1.2 | 157 | 1.44 | Reference | 70 | 1.42 | Reference | ||||||
β, beta coefficient; CI, confidence interval; HR, hazard ratio.
P < 0.05 is considered statistically significant.
For non‐septic patients, early high protein intake was associated with significantly increased 6‐month mortality compared with low protein intake (HR: 3.902, 95% CI: 1.505‐10.115, P = 0.005; Table 3, Figure S2). Conversely, in the later phase, low protein intake was associated with higher 6‐month mortality in univariate analysis compared with high protein intake (HR: 2.642, 95% CI: 1.128‐6.189, P = 0.025).
Subsequently, protein intakes during days 1–3 and 4–7 were combined, and different feeding regimens were evaluated (Table 4). Four groups were assessed: patients who received <0.8 g/kg/d the whole week (group 1), <0.8 on days 1–3 and >0.8 g/kg/d on days 4–7 (group 2), 0.8–1.2 g/kg/d the whole week (group 3), and >1.2 g/kg/d the whole week (group 4). In septic patients, group 3 was significantly associated with a better survival in univariate analysis (HR: 0.315, 95% CI: 0.124‐0.798, P = 0.015) compared with an overall low protein intake. In non‐septic patients, group 2 showed a trend toward better survival (HR: 0.414, 95% CI: 0.162‐1.056, P = 0.065) compared with an overall low protein intake.
Table 4.
Univariate Cox Proportional Hazards Model 6‐Month Mortality: Proteins‐Combined Early and Later Phase
| Protein Intake | Sepsis | No Sepsis | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Days 1–3 to days 4–7, g/kg/d | n | Mean | β | HR | 95% CI | P | n | Mean | β | HR | 95% CI | P |
| <0.8 overall | 19 | 0.44 | Reference | 8 | 0.49 | Reference | ||||||
| <0.8 to >0.8 | 215 | 0.93 | −0.524 | 0.592 | (0.306–1.146) | 0.120 | 102 | 0.93 | −0.882 | 0.414 | (0.162–1.056) | 0.065 |
| 0.8–1.2 overall | 39 | 0.95 | −1.156 | 0.315 | (0.124–0.798) | 0.015a | 11 | 0.97 | −0.798 | 0.450 | (0.121–1.679) | 0.235 |
| >1.2 overall | 24 | 1.34 | −0.170 | 0.844 | (0.358–1.987) | 0.697 | 5 | 1.18 | 0.423 | 1.527 | (0.409–5.706) | 0.529 |
β, beta coefficient; CI, confidence interval; HR, hazard ratio.
P < 0.05 is considered statistically significant.
Secondary endpoints were evaluated for the different protein feeding regimens (Table 5). In septic patients, overall protein intake of 0.8–1.2 g/kg/d was associated with decreased ventilation duration, ICU, in‐hospital, 28‐day mortality, and 6‐month readmission rates. However, ICU LOS was significantly lower in the low to high (<0.8 to >0.8) intake group, all compared with an overall low protein intake. Other secondary end points were not significantly associated with protein intake (Table 5).
Table 5.
Outcome Measures to Protein Intake Group with Combined Early and Later Phase Feeding Regimen
| Sepsis | No Sepsis | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Outcome Measure | Overall <0.8 | <0.8 to >0.8 | Overall 0.8–1.2 | Overall >1.2 | P a | Overall <0.8 | <0.8 to >0.8 | Overall 0.8–1.2 | Overall >1.2 | P a |
| Mortality | ||||||||||
| ICU mortality, n of events/n total (%) | 7/19 (37)b | 39/215 (18) | 3/39 (8)b | 6/24 (25) | 0.010b | 5/8 (63)b | 13/102 (13)b | 3/11 (27) | 2/5 (40) | 0.003b |
| In‐hospital mortality, n of events/n total (%) | 9/19 (47)b | 55/215 (26) | 7/39 (18)b | 8/24 (33) | 0.029b | 5/8 (63)b | 26/102 (26)b | 3/11 (27) | 3/5 (60) | 0.039b |
| 28‐day mortality, n of events/n total (%) | 7/19 (37)b | 48/215 (22) | 4/39 (10)b | 7/24 (29) | 0.029b | 3/8 (38) | 20/102 (21) | 3/11 (27) | 3/5 (60) | 0.133 |
| 6‐month mortality, n of events/n total (%) | 10/19 (53)b | 75/215 (35) | 8/39 (21)b , c | 11/24 (46)c | 0.018b 0.048c | 5/8 (63) | 36/102 (35) | 4/11 (36) | 4/5 (80) | 0.111 |
| LOS | ||||||||||
| ICU LOS days, median [IQR] | 22 [14–30.5]b | 16 [11–25]b | 14 [11.5–26.5] | 13 [11–28.5] | 0.038b | 24.5 [7.5–52.5] | 14.5 [11–24] | 13 [10–19] | 13 [12–13] | 0.635 |
| Hospital LOS days, median [IQR] | 27 [19.5–43] | 29 [18.5–42] | 28 [21–41.5] | 25.5 [14.5–36.5] | 0.613 | 37.5 [10.5–57] | 26.5 [19–44] | 23 [18.5–53] | 26 [15–31] | 0.913 |
| Organ failure | ||||||||||
| Ventilation duration days, median [IQR] | 15 [11–24.5]b , c | 11 [8–17]b | 10 [8–15]c | 10.5 [8–19.5] | 0.031b 0.013c | 19 [7.5–35.5] | 10 [8–14] | 10 [8.5–12.5] | 10 [8–11] | 0.776 |
| Presence of AKId n of events/n total (%) | 1/19 (5) | 13/215 (6) | 4/39 (10) | 1/24 (4) | 0.740 | 0/8 (0) | 15/102 (15) | 0/11 (0) | 0/5 (0) | 0.261 |
| Need for CRRT, n of events/n total (%) | 6/19 (32) | 57/215 (27) | 6/39 (15) | 2/24 (8) | 0.103 | 6/8 (75)b , c | 26/102 (26)b | 4/11 (36) | 0/5 (0)c | 0.007b 0.021c |
| Number of days on CRRT, median [IQR] | 10 [9–16] | 7 [4–10] | 5 [4–11] | 16.5 [8–25] | 0.148 | 14 [6–28] | 7 [5–12] | 3.5 [2–6.5] | NA | 0.099 |
| Other | ||||||||||
| 6‐Month hospital readmissione, n of events/n total (%) | 3/19 (16)b | 69/215 (32) | 17/39 (44)b | 9/24 (38) | 0.044b | 1/8 (13) | 38/102 (37) | 3/11 (27) | 1/5 (20) | 0.426 |
AKI, acute kidney injury; CRRT, continuous renal replacement therapy; ICU, intensive care unit; IQR, interquartile range; LOS, length of stay; NA, not applicable.
All groups were compared for sepsis and no sepsis separately using χ2 tests or Fischer exact tests where appropriate.
Statistical differences between the groups with corresponding P‐value.
Statistical differences between the groups with corresponding P‐value.
AKI, positive Rifle criteria for AKI, acute kidney failure or loss of renal function.
6‐Month all‐cause hospital readmission.
For non‐septic patients, ICU and in‐hospital mortality and need for Continuous Renal Replacement Therapy (CRRT) was lower in group 2 (<0.8 to >0.8 g/kg/d; Table 5) compared with an overall low intake. Other secondary endpoints were not significantly different between the subgroups.
Subgroup Analysis: Energy
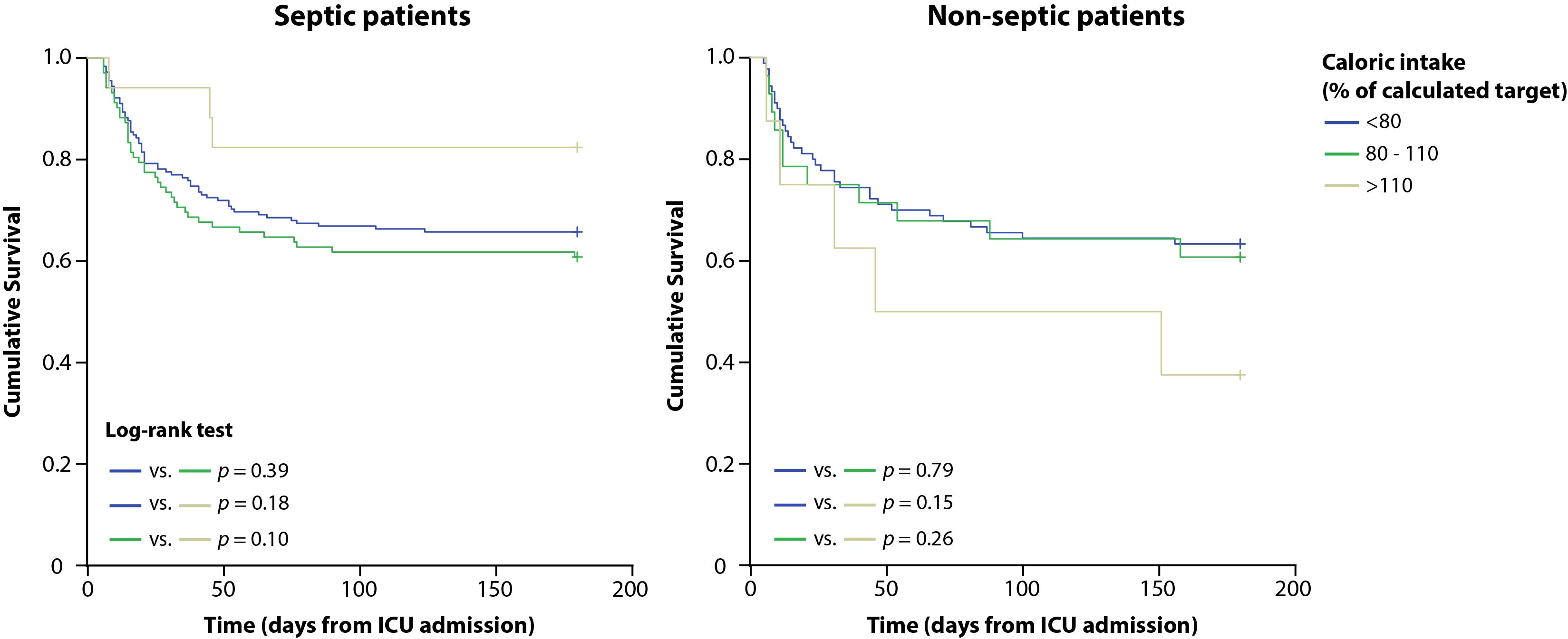
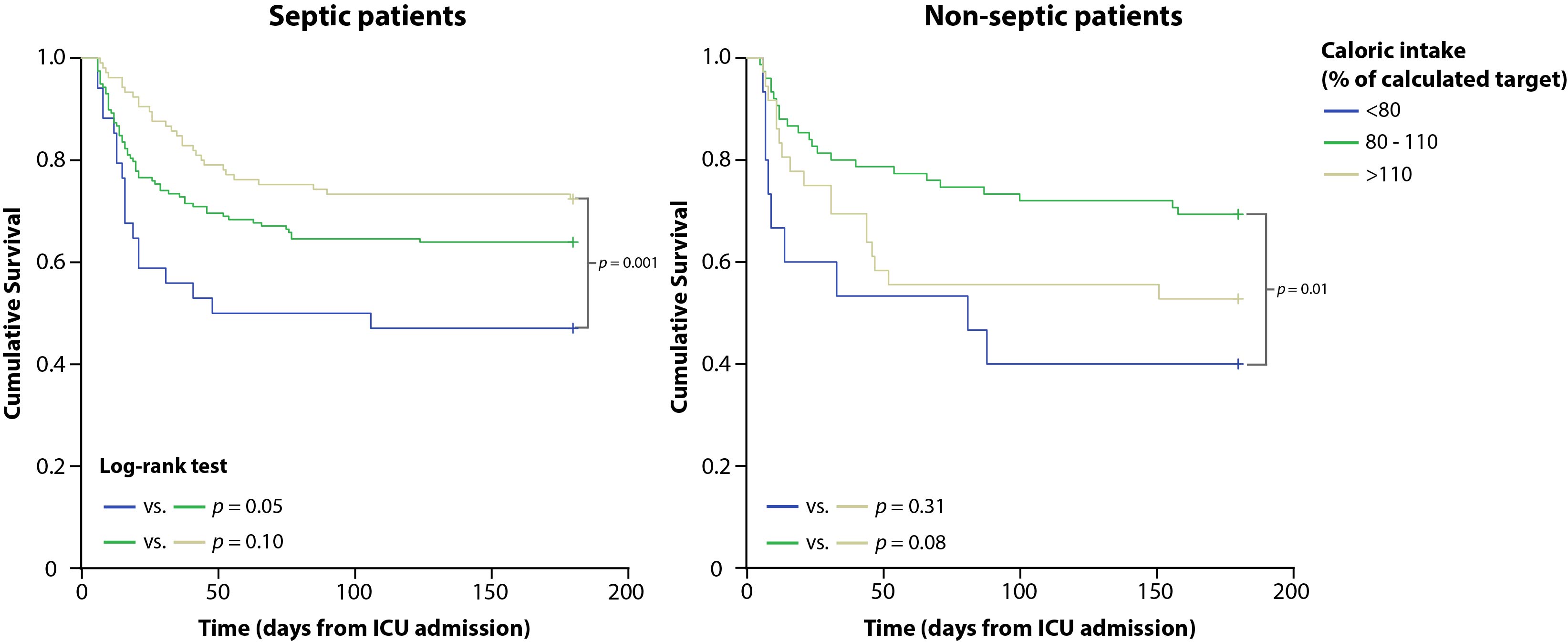
In septic patients, no significant associations were found between early energy intake and 6‐month mortality (Table 6, Figure S4, Table S5). In the later phase, medium (80%–110%) and high energy intake (>110%) were significantly better than low energy intake (<80%) (HR: 0.583, 95% CI: 0.343‐0.991, P = 0.046 for medium energy intake; HR: 0.400, 95% CI: 0.222‐0.721, P = 0.002 for high energy intake; Table 6, Figure S5).
Table 6.
Univariate Cox Proportional Hazards Model 6‐Month Mortality: Energy‐First Week Separated in Early and Later Phase
| Energy Intake | Sepsis | No Sepsis | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intake subgroups | n | Mean, % | β | HR | 95% CI | P | n | Mean, % | β | HR | 95% CI | P |
| Days 1–3 | ||||||||||||
| <80% of target | 178 | 51 | Reference | 90 | 48 | Reference | ||||||
| 80%–110% of target | 102 | 91 | 0.176 | 1.192 | (0.800–1.777) | 0.387 | 28 | 89 | 0.094 | 1.099 | (0.555–2.174) | 0.787 |
| >110% of target | 17 | 130 | −0.778 | 0.459 | (0.144–1.464) | 0.188 | 8 | 120 | 0.676 | 1.967 | (0.767–5.041) | 0.159 |
| Days 4–7 | ||||||||||||
| <80% of target | 34 | 65 | Reference | 15 | 69 | Reference | ||||||
| 80%–110% of target | 158 | 100 | −0.539 | 0.583 | (0.343–0.991) | 0.046a | 75 | 100 | −0.971 | 0.379 | (0.175–0.820) | 0.014a |
| >110% of target | 105 | 130 | −0.916 | 0.400 | (0.222–0.721) | 0.002a | 36 | 139 | −0.422 | 0.655 | (0.292–1.471) | 0.306 |
β, beta‐coefficient; CI, confidence interval; HR, hazard ratio.
P‐value < 0.05 is considered statistically significant.
In non‐septic patients also, no significant associations for early energy intake were found. An energy intake of 80%–110% at days 4–7 was associated with a significantly lower 6‐month mortality compared with low energy intake (HR: 0.379, 95% CI: 0.175‐0.820, P = 0.014; Table 6, Figure S4, Figure S5).
Associations between macronutrient intake and 6‐month mortality were not significantly influenced by any admission year. In case significance was lost in leave‐1‐out cross‐validation, direction of the observed associations (ie, β) did not change.
Discussion
We found divergent associations of protein and energy intake and 6‐month mortality during the first week of ICU admission among critically ill adult patients with sepsis compared with those without sepsis.
Septic Patients
A late protein intake of 0.8–1.2 g/kg/d was associated with the lowest 6‐month mortality. No strong time‐dependent effects were observed. A secondary analysis of an observational study in 2270 septic patients reported a decrease in 60‐day mortality when increasing protein intake by 30 g/d (odds ratio: 0.76, P < 0.001) from 0.7 g/kg/d.11 These results could be in line with our findings; however, no time‐dependent effects were taken into account. Contradictory findings with a significantly decreased mortality due to high protein intake (1.5 vs 1.1 vs 0.8 g/kg/d) in sepsis were reported by Allingstrup et al.12 In addition, Weijs et al reported no significant association of hospital mortality with protein intake at day 4 in sepsis.17
In our study, overfeeding, defined as an intake above 110% of the calculated energy target, was associated with better long‐term survival in septic patients; however, this is known to be harmful in general critically ill patients.26 Partially in line with our findings, Weijs et al reported no harmful effects nor beneficial effects from energy overfeeding in septic patients.17
Because of contradictory findings of different studies, large prospective studies in septic patients are warranted to develop proper clinical guidelines in this large subgroup of critically ill patients.
Non‐Sepsis Patients
A strong time‐dependent effect of protein intake was observed. Early high protein intake was associated with higher 6‐month mortality, whereas late high protein intake showed a trend toward lower mortality. These findings are concordant with those of Casaer et al40 and Weijs et al,17 who found an association with harm on day 340 but either no effect40 or a beneficial effect of high protein intake ≥day 4.17 Contradictory, Ferrie et al did not find an effect of early protein intake on mortality, comparing patients receiving parenteral nutrition at doses of 0.87 vs 1.17 g/kg/d (days 1–3).13 However, the differences in protein intake between these groups were relatively small, and both groups would relate to our medium protein intake category (0.8–1.2 g/kg/d).
As reported in multiple studies, we also found energy overfeeding to be associated with higher mortality in non‐sepsis patients.14, 17, 27 Furthermore, we did not find a survival benefit for early medium (80%–110%) energy intake compared with early low energy intake, in line with recent RCTs.24, 25
Based on our findings and those in other recent studies, we suggest to prospectively investigate build‐up regimens in protein intake (0.8 g/kg/d in days 1–3 followed by >1.2 g/kg/d from day 4) and energy intake at 70%–90% of target in non‐sepsis patients.17, 32
Pathophysiology
We hypothesized that early high protein intake would be more harmful to septic patients because early high protein intake is supposed to inhibit autophagy.20 However, we did not observe these associations in septic patients, contrary to non‐septic patients. These observations may indicate a difference between these 2 groups and underline the importance for prospective research within both groups to address this hypothesis. Our study was not designed to address the association between autophagy, sepsis, and protein intake, and conclusions regarding these associations therefore cannot be drawn.
In addition to prospective research, further basic research is warranted to obtain more insight in the process of autophagy. It is possible, and we speculate, that patients with sepsis have different or earlier activation of autophagy.41, 42 Furthermore, different levels of catabolism and absorption rates of macronutrients from the gut also might play a role in any potential differences between septic and non‐septic patients.43
Strengths and Weaknesses
Strict adherence to our feeding protocol (mean start of feeding 6 hours after admission) facilitated early evaluation and analysis of possible time‐dependent effects of nutrition support. The number of (sepsis) patients included, covariates taken into account, inclusion of non‐nutrition energy, and the long follow‐up period (6 months) are other strengths.
Limitations of our study and its single‐center retrospective design include potential selection of the sicker ICU patients due to including only prolonged mechanically ventilated patients. This may potentially lead to selection bias and residual confounding, limiting external validity. In addition, some subgroups in our analyses were very small, and energy targets were based on the FAO/WHO formulas and not on indirect calorimetry. Generalization of our study should be done with caution, and we strongly emphasize that large adequately powered RCTs are warranted to address causality of the observed associations.
Conclusions
We found divergent associations of protein and energy intake during the first week of ICU admission among critically ill adult patients with sepsis compared with those without sepsis. In septic patients, we observed that late medium protein and late high energy intake were associated with survival benefit. For non‐septic patients, a strong time‐dependent effect was observed; early high protein intake was associated with higher 6‐month mortality, whereas in the later phase an intake of >0.8 g/kg/d might be beneficial.
Supporting information
Figure S1. Flowchart of enrolled patients. ICU, intensive care unit; SOFA, Sequential Organ Failure Assessment.
{kind=link}
Figure S2. Kaplan‐Meier 6‐month survival curves for protein intake subgroups days 1–3, sepsis and no sepsis. ICU, intensive care unit.
{kind=link}
Figure S3. Kaplan‐Meier 6‐month survival curves for protein intake subgroups days 4–7, sepsis and no sepsis. ICU, intensive care unit.
{kind=link}
Figure S4. Kaplan‐Meier 6‐month survival curves for caloric intake subgroups days 1–3, sepsis and no sepsis. ICU, intensive care unit.
{kind=link}
Figure S5. Kaplan‐Meier 6‐month survival curves for caloric intake subgroups days 4–7, sepsis and no sepsis. ICU, intensive care unit.
{kind=link}
Table S1. Multivariate Cox Proportional‐Hazard Model 6‐Month Mortality: Proteins—Separated Early and Later Phase.
Table S2. Multivariate Cox Proportional‐Hazards Model 6‐Months Mortality: Proteins—Combined Early and Later Phase
Table S3. Multivariate Cox Proportional‐Hazards Model 6‐Month Mortality: Calories—Separated Early and Later Phase.
Table S4. Univariate Cox Proportional‐Hazards Model 6‐Month Mortality: Proteins—Separated Early and Later Phase, Continuous Data.
Table S5. Univariate Cox Proportional‐Hazards Model 6‐Month Mortality: Calories—Separated Early and Later Phase, Continuous Data.
Supporting Information
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are not publicly available due to privacy or other restrictions but are available from the corresponding author on reasonable request.
Acknowledgments
The authors thank research students Y. Menger and L. E. Olthof for support with screening for sepsis and data analyses.
Statement of Authorship
M. L. Y. de Koning and A. R. H. van Zanten equally contributed to the conception and design of the research; J. C. N. Kars and M. L. Y. de Koning contributed to the acquisition of the data; M. L. Y. de Koning and W. A. C. Koekkoek and A. R. H. van Zanten contributed to the analysis and interpretation of the data; M. L. Y. de Koning drafted the manuscript; W. A. C. Koekkoek and A. R. H. van Zanten critically revised the manuscript. All authors agree to be fully accountable for all aspects of the work, ensure integrity and accuracy, and read and approved the final manuscript.
Financial disclosure: None declared.
Conflicts of interest: None declared
References
- 1. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis‐3). JAMA. 2016;315(8):801‐810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Arbous S, Bakhshi‐Raiez F, Brinkman S, et al. Jaarboek 2015. stichting NICE; https://stichting-nice.nl/doc/jaarboek-2015-web.pdf. Updated 2016. Accessed October 20, 2016. [Google Scholar]
- 3. Preiser JC, van Zanten AR, Berger MM, et al. Metabolic and nutritional support of critically ill patients: consensus and controversies. Crit Care. 2015;19:35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Elke G, Kott M, Weiler N. When and how should sepsis patients be fed? Curr Opin Clin Nutr Metab Care. 2015;18(2):169‐178. [DOI] [PubMed] [Google Scholar]
- 5. McClave SA, Taylor BE, Martindale RG, et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of critical care medicine (SCCM) and american society for parenteral and enteral nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr. 2016;40(2):159‐211. [DOI] [PubMed] [Google Scholar]
- 6. Kreymann G, Grosser S, Buggisch P, Gottschall C, Matthaei S, Greten H. Oxygen consumption and resting metabolic rate in sepsis, sepsis syndrome, and septic shock. Crit Care Med. 1993;21(7):1012‐1019. [DOI] [PubMed] [Google Scholar]
- 7. Ishibashi N, Plank LD, Sando K, Hill GL. Optimal protein requirements during the first 2 weeks after the onset of critical illness. Crit Care Med. 1998;26(9):1529‐1535. [DOI] [PubMed] [Google Scholar]
- 8. Weijs PJ, Wischmeyer PE. Optimizing energy and protein balance in the ICU. Curr Opin Clin Nutr Metab Care. 2013;16(2):194‐201. [DOI] [PubMed] [Google Scholar]
- 9. Weijs PJ, Stapel SN, de Groot SD, et al. Optimal protein and energy nutrition decreases mortality in mechanically ventilated, critically ill patients: a prospective observational cohort study. JPEN J Parenter Enteral Nutr. 2012;36(1):60‐68. [DOI] [PubMed] [Google Scholar]
- 10. Alberda C, Gramlich L, Jones N, et al. The relationship between nutritional intake and clinical outcomes in critically ill patients: results of an international multicenter observational study. Intensive Care Med. 2009;35(10):1728‐1737. [DOI] [PubMed] [Google Scholar]
- 11. Elke G, Wang M, Weiler N, Day AG, Heyland DK. Close to recommended caloric and protein intake by enteral nutrition is associated with better clinical outcome of critically ill septic patients: secondary analysis of a large international nutrition database. Crit Care. 2014;18(1):R29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Allingstrup MJ, Esmailzadeh N, Wilkens KA, et al. Provision of protein and energy in relation to measured requirements in intensive care patients. Clin Nutr. 2012;31(4):462‐468. [DOI] [PubMed] [Google Scholar]
- 13. Ferrie S, Allman‐Farinelli M, Daley M, Smith K. Protein requirements in the critically ill: a randomized controlled trial using parenteral nutrition. JPEN J Parenter Enteral Nutr. 2016;40(6):795‐805. [DOI] [PubMed] [Google Scholar]
- 14. Allingstrup MJ, Kondrup J, Wiis J, et al. Early goal‐directed nutrition versus standard of care in adult intensive care patients: the single‐centre, randomised, outcome assessor‐blinded EAT‐ICU trial. Intensive Care Med. 2017;43(11):1637‐1647. [DOI] [PubMed] [Google Scholar]
- 15. Braunschweig CA, Sheean PM, Peterson SJ, et al. Intensive nutrition in acute lung injury: a clinical trial (INTACT). JPEN J Parenter Enteral Nutr. 2015;39(1):13‐20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Elke G, Kuhnt E, Ragaller M, et al. Enteral nutrition is associated with improved outcome in patients with severe sepsis. A secondary analysis of the VISEP trial. Med Klin Intensivmed Notfmed. 2013;108(3):223‐233. [DOI] [PubMed] [Google Scholar]
- 17. Weijs PJ, Looijaard WG, Beishuizen A, Girbes AR, Oudemans‐van Straaten HM. Early high protein intake is associated with low mortality and energy overfeeding with high mortality in non‐septic mechanically ventilated critically ill patients. Crit Care. 2014;18(6):701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Braunschweig CL, Freels S, Sheean PM, et al. Role of timing and dose of energy received in patients with acute lung injury on mortality in the intensive nutrition in acute lung injury trial (INTACT): a post hoc analysis. Am J Clin Nutr. 2017;105(2):411‐416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Koekkoek WACK, van Setten CHC, Olthof LE, Kars JCN, van Zanten ARH. Timing of PROTein INtake and clinical outcomes of adult critically ill patients on prolonged mechanical VENTilation: The PROTINVENT retrospective study. Clin Nutr. 2018;38(2):883‐890. [DOI] [PubMed] [Google Scholar]
- 20. Hermans G, Casaer MP, Clerckx B, et al. Effect of tolerating macronutrient deficit on the development of intensive‐care unit acquired weakness: a subanalysis of the EPaNIC trial. Lancet Respir Med. 2013;1(8):621‐629. [DOI] [PubMed] [Google Scholar]
- 21. Choi AJ, Ryter SW. Autophagy in inflammatory diseases. Int J Cell Biol. 2011;2011:732798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Gunst J, Derese I, Aertgeerts A, et al. Insufficient autophagy contributes to mitochondrial dysfunction, organ failure, and adverse outcome in an animal model of critical illness. Crit Care Med. 2013;41(1):182‐194. [DOI] [PubMed] [Google Scholar]
- 23. McClave SA, Weijs PJ. Preservation of autophagy should not direct nutritional therapy. Curr Opin Clin Nutr Metab Care. 2015;18(2):155‐161. [DOI] [PubMed] [Google Scholar]
- 24. Arabi YM, Aldawood AS, Haddad SH, et al. Permissive underfeeding or standard enteral feeding in critically ill adults. N Engl J Med. 2015;372(25):2398‐2408. [DOI] [PubMed] [Google Scholar]
- 25. TARGET Investigators, for the ANZICS Clinical Trials Group , Chapman M, Peake SL, Bellomo R, et al. Energy‐dense versus routine enteral nutrition in the critically ill. N Engl J Med. 2018;379(19):1823‐1834. [DOI] [PubMed] [Google Scholar]
- 26. Klein CJ, Stanek GS, Wiles CE, III. Overfeeding macronutrients to critically ill adults: metabolic complications. J Am Diet Assoc. 1998;98(7):795‐806. [DOI] [PubMed] [Google Scholar]
- 27. Zusman O, Theilla M, Cohen J, Kagan I, Bendavid I, Singer P. Resting energy expenditure, calorie and protein consumption in critically ill patients: a retrospective cohort study. Crit Care. 2016;20(1):367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Vincent JL, de Mendonça A, Cantraine F, et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working Group on “Sepsis‐Related Problems” of the European Society of Intensive Care Medicine. Crit Care Med. 1998;26(11):1793‐1800. [DOI] [PubMed] [Google Scholar]
- 29. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818‐829. [PubMed] [Google Scholar]
- 30. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373‐383. [DOI] [PubMed] [Google Scholar]
- 31. Heyland DK, Dhaliwal R, Jiang X, Day AG. Identifying critically ill patients who benefit the most from nutrition therapy: the development and initial validation of a novel risk assessment tool. Crit Care. 2011;15(6):R268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Heyland DK, Cahill N, Day AG. Optimal amount of calories for critically ill patients: depends on how you slice the cake! Crit Care Med. 2011;39(12):2619‐2626. [DOI] [PubMed] [Google Scholar]
- 33. Food energy‐methods of analysis and conversion factors. Food and Agriculture Organization of the United Nations; http://www.fao.org/docrep/006/Y5022E/y5022e00.htm. Updated 2003. Accessed October 4, 2016. [Google Scholar]
- 34. Bousie E, van Blokland D, van Zanten AR. Effects of implementation of a computerized nutritional protocol in mechanically ventilated critically ill patients: a single‐centre before and after study. Clin Nutr. 2016;11:e47‐e54. [DOI] [PubMed] [Google Scholar]
- 35. Greenwood J. ICU guideline: adjusting goal feed rates in the patients receiving propofol. Vancouver Coastal Health. http://www.criticalcarenutrition.com/docs/tools/Propofol.pdf. Updated 2009. Accessed October 4, 2016.
- 36. FAO . Human Energy Requirements. Report of a joint FAO/ WHO/ UNU Expert Consultation. FAO food and nutrition technical report series no 1. Food and Agricultural Organisation; http://www.fao.org/3/a-y5686e.pdf. Updated 2004. Accessed October 4, 2016. [Google Scholar]
- 37. Elia M. Insights into energy requirements in disease. Public Health Nutr. 2005;8(7A):1037‐1052. [DOI] [PubMed] [Google Scholar]
- 38. Stapel SN, de Grooth HJ, Alimohamad H, et al. Ventilator‐derived carbon dioxide production to assess energy expenditure in critically ill patients: proof of concept. Crit Care. 2015;19:370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P. Acute renal failure – definition, outcome measures, animal models, fluid therapy and information technology needs: the second international consensus conference of the acute dialysis quality initiative (ADQI) group. Crit Care. 2004;8(4):R204‐R212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Casaer MP, Mesotten D, Hermans G, et al. Early versus late parenteral nutrition in critically ill adults. N Engl J Med. 2011;365(6):506‐517. [DOI] [PubMed] [Google Scholar]
- 41. Delgado MA, Elmaoued RA, Davis AS, Kyei G, Deretic V. Toll‐like receptors control autophagy. EMBO J. 2008;27(7):1110‐1121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Chien WS, Chen YH, Chiang PC, et al. Suppression of autophagy in rat liver at late stage of polymicrobial sepsis. Shock. 2011;35(5):506‐511. [DOI] [PubMed] [Google Scholar]
- 43. Puthucheary ZA, Rawal J, McPhail M, et al. Acute skeletal muscle wasting in critical illness. JAMA. 2013;310(15):1591‐1600. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1. Flowchart of enrolled patients. ICU, intensive care unit; SOFA, Sequential Organ Failure Assessment.
Figure S2. Kaplan‐Meier 6‐month survival curves for protein intake subgroups days 1–3, sepsis and no sepsis. ICU, intensive care unit.
Figure S3. Kaplan‐Meier 6‐month survival curves for protein intake subgroups days 4–7, sepsis and no sepsis. ICU, intensive care unit.
Figure S4. Kaplan‐Meier 6‐month survival curves for caloric intake subgroups days 1–3, sepsis and no sepsis. ICU, intensive care unit.
Figure S5. Kaplan‐Meier 6‐month survival curves for caloric intake subgroups days 4–7, sepsis and no sepsis. ICU, intensive care unit.
Table S1. Multivariate Cox Proportional‐Hazard Model 6‐Month Mortality: Proteins—Separated Early and Later Phase.
Table S2. Multivariate Cox Proportional‐Hazards Model 6‐Months Mortality: Proteins—Combined Early and Later Phase
Table S3. Multivariate Cox Proportional‐Hazards Model 6‐Month Mortality: Calories—Separated Early and Later Phase.
Table S4. Univariate Cox Proportional‐Hazards Model 6‐Month Mortality: Proteins—Separated Early and Later Phase, Continuous Data.
Table S5. Univariate Cox Proportional‐Hazards Model 6‐Month Mortality: Calories—Separated Early and Later Phase, Continuous Data.
Supporting Information