

Background: The coronavirus disease 2019 (COVID-19) epidemic began in Wuhan, China, in late 2019 and continues to spread globally (1), with exported cases confirmed in 109 countries at the time of writing (2). During the interval between 19 February and 23 February 2020, Iran reported its first 43 cases, with 8 deaths. Three exported cases originating in Iran were identified, suggesting an underlying burden of disease in that country greater than that indicated by reported cases. A large epidemic in Iran could further fuel global dissemination of COVID-19.
Objective: To quantify the COVID-19 outbreak size in Iran on the basis of known exported case counts and air travel links between Iran and other countries, and to anticipate where infections originating in Iran may spread next.
Methods: We assessed interconnectivity between Iran and other countries by using direct and total traveler volumes and final destination cities of travelers originating in Iran in February 2019, according to data from the International Air Transport Association (accounting for 90% of global air travel, with the other 10% modeled by using market intelligence). Because exported cases were identified in United Arab Emirates (UAE), Lebanon, and Canada, we used the methods of Fraser and colleagues (3) to estimate the size of the underlying epidemic in Iran that would be needed for these cases to be observed with a reasonable probability. To estimate the time at risk for COVID-19 exposure among travelers departing Iran, we obtained data from the United Nations World Tourism Organization for the proportion of international travelers who are residents of Iran (4) and the average length of stay of tourists to Iran (5), and assumed that the Iranian outbreak began in early January 2020. We evaluated the relationship between the strength of travel links with Iran and the ranking of destination countries on the Infectious Disease Vulnerability Index (IDVI), a validated metric that estimates the capacity of a country to respond to an infectious disease outbreak. Scores range from 0 to 1, with higher scores reflecting greater capacity to manage infectious outbreaks.
Findings: A total of 212 000 persons traveled from Iranian airports (Tehran, Rasht, and Arak) to international destinations in February 2019. Although Qom has reported COVID-19 cases, its international airport is still under construction. Global cities receiving the greatest number of total travelers from Iran during this period include Istanbul, Turkey (n = 46 550); Najaf, Iraq (n = 24 659); and Dubai, UAE (n = 16 340). Among the top 10 traveler-receiving cities, 4 (Najaf, Baghdad, Damascus, and Baku) are in countries with an IDVI score lower than 0.6, suggesting elevated vulnerability to infectious disease outbreaks as well as limited ability to detect cases (Figure 1).
Figure 1.
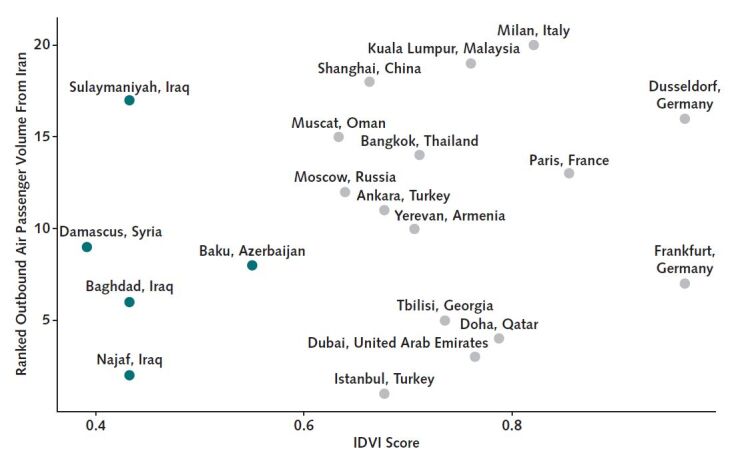
Top 20 international cities connected to Iran by commercial air travel and associated vulnerability to infectious disease outbreaks.
Vulnerability is measured at the country level by using the IDVI score, with a lower value indicating reduced capacity to respond to outbreaks. Countries with the lowest IDVI scores are indicated in green. The top 20 cities accounted for 70% of international outbound traveler volumes from Iran in February 2019. The first and 20th ranked cities, Istanbul and Milan, had 46 550 and 2500 outbound passengers, respectively, during this period. IDVI = Infectious Disease Vulnerability Index.
United Arab Emirates, Lebanon, and Canada ranked third, 21st, and 31st, respectively, for outbound air travel volume from Iran in February 2019. We estimated that 18 300 COVID-19 cases (95% CI, 3770 to 53 470 cases) would have had to occur in Iran, assuming an outbreak duration of 1.5 months in the country, in order to observe these 3 internationally exported cases reported at the time of writing.
Given the low rankings for Lebanon and Canada for outbound air travel, it is unlikely that cases would be identified in these countries and not in Iraq, Syria, or Azerbaijan (countries with higher travel volumes but low IDVI scores). Considering traveler volume alone, the odds of a single case being imported into Iraq rather than Canada or Lebanon would be 33.6 to 1 and 15.4 to 1 respectively; for Azerbaijan, the odds would be 3.8 to 1 and 1.7 to 1, respectively; and for Syria, the odds would be 3.7 to 1 and 1.7 to 1, respectively. As such, we performed exploratory analyses in which we assumed that an unidentified exported case of COVID-19 was present in Iraq, Syria, Azerbaijan, or all 3 countries, in addition to Lebanon, Canada, and UAE, and estimated the outbreak size in Iran that would produce these results (Figure 2). We also evaluated a scenario in which we assumed perfect case detection in travelers from Iran, such that disease is truly absent in countries not reporting cases. Under this “best-case” scenario, the estimated outbreak size in Iran was smaller but still substantial (1820 cases [CI, 380 to 5320 cases]).
Figure 2.
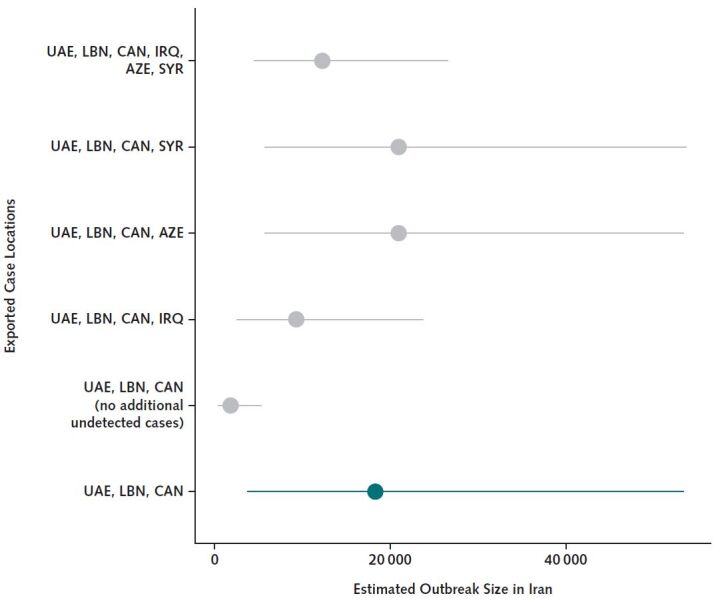
Estimated outbreak size in Iran required to observe exported cases internationally.
The estimated cumulative number of COVID-19 cases in Iran required to observe 3 cases exported to UAE, LBN, and CAN is shown in green. We also estimated the outbreak size required under alternate scenarios, including no additional exported cases to any other international destinations despite perfect case detection and 1 additional exported case to IRQ, AZE, or SYR (independently or to all 3 countries). Mean and 95% CIs are presented. The rate at which persons become infected while in Iran was assumed to be the same for residents and visitors. The rate of infection among air passengers (λ) was estimated as number of exported cases ÷ person-time at risk while in Iran. Person-time at risk was calculated as number of outbound air passengers × (average length of stay for visitors × proportion of air passengers who are visitors + outbreak duration × proportion of air passengers who are residents of Iran). Outbreak size in Iran was then estimated as λ × population size of Iran × outbreak duration. AZE = Azerbaijan; CAN = Canada; COVID-19 = coronavirus disease 2019; IRQ = Iraq; LBN = Lebanon; SYR = Syria; UAE = United Arab Emirates.
Discussion: Given the low volumes of air travel to countries with identified cases of COVID-19 originating in Iran (such as Canada), Iran probably is currently experiencing a COVID-19 epidemic of substantial size for such exportations to be occurring. Our analysis would be modified by travel restrictions from Iran due to the recent political situation and by variations in the R0 value. Further, the lack of identified COVID-19 cases in countries with far closer travel ties to Iran suggests that cases in these countries are probably being missed rather than being truly absent. This is concerning, both for public health in Iran itself and because of the high likelihood for outward dissemination of the disease to neighboring countries with lower capacity to respond to infectious disease epidemics. Supporting capacity for public health initiatives in the region is urgently needed.
Biography
Note: Drs. Tuite and Bogoch contributed equally to this work.
Grant Support: By grant 02179-000 from the Canadian Institutes of Health Research.
Disclosures: Disclosures can be viewed at www.acponline.org/authors/icmje/ConflictOfInterestForms.do?msNum=M20-0696.
Reproducible Research Statement: Study protocol: Not applicable. Statistical code: Available from Dr. Tuite (ashleigh.tuite@utoronto.ca). Data set: Available from Dr. Khan (kamran.khan@unityhealth.to).
Previous Posting: This manuscript was posted as a preprint on medRxiv on 25 February 2020. doi:10.1101/2020.02.24.20027375
Footnotes
This article was published at Annals.org on 16 March 2020.
References
- Bogoch II, Watts A, Thomas-Bachli A, et al. doi: 10.1093/jtm/taaa011. Bogoch II, Watts A, Thomas-Bachli A, et al. Potential for global spread of a novel coronavirus from China. J Travel Med. 2020. [PMID: 31985790] doi:10.1093/jtm/taaa011. [DOI] [PMC free article] [PubMed]
- World Health Organization. World Health Organization. Coronavirus disease 2019 (COVID-19) situation report – 33. Accessed at www.who.int/docs/default-source/coronaviruse/situation-reports/20200222-sitrep-33-covid-19.pdf?sfvrsn=c9585c8f_2. on 22 February 2020.
- Fraser C, Donnelly CA, Cauchemez S, et al; WHO Rapid Pandemic Assessment Collaboration. doi: 10.1126/science.1176062. Fraser C, Donnelly CA, Cauchemez S, et al; WHO Rapid Pandemic Assessment Collaboration. Pandemic potential of a strain of influenza A (H1N1): early findings. Science. 2009;324:1557-61. [PMID: 19433588] doi:10.1126/science.1176062. [DOI] [PMC free article] [PubMed]
- United Nations World Tourism Organization. United Nations World Tourism Organization. Tourism Statistics: Iran, Islamic Republic Of: Country-specific: Basic indicators (Compendium) 2014–2018. Accessed at www.e-unwto.org/doi/abs/10.5555/unwtotfb0364010020142018201912. on 22 February 2020.
- United Nations. United Nations. Encyclopedia of the Nations: Average length of stay of visitors - Tourism indicators - UNCTAD Handbook of Statistics - Country Comparison. Accessed at www.nationsencyclopedia.com/WorldStats/UNCTAD-average-length-stay-visitors.html. on 22 February 2020.