

Abstract
Research has established a strong association between asbestos exposure and malignant mesothelioma, a deadly form of cancer. Since the early 1980’s many countries have restricted or banned the production of asbestos, leading to a decline of occupational asbestos exposure in many industrialized countries. However, some countries continue to use asbestos, and worldwide rates of mesothelioma are still increasing. Because of the long latency between exposure and mesothelioma occurrence and the persistence of environmental exposure, incidence rates (IR) may decrease very slowly for several years ahead. In this review, we examine estimates of asbestos consumption before widespread asbestos regulations and the trends in incidence and mortality rates, as well as changes over time for the United States and Europe. In some countries with earlier asbestos restrictions, mesothelioma incidence has been in a modest decline over time. However, asbestos exposure is still a burden worldwide and legislative action is needed to obtain a full ban. The pattern of mesothelioma is shifting from a mostly male disease to a disease that affects females as well in substantial numbers. Studies on unknown sources of asbestos exposure, of other sources of natural exposure to asbestos and asbestos-like fibers, as well as of individual genetic susceptibility to asbestos fibers are needed.
Keywords: Carcinogen regulation, environmental exposure, incidence trends, mortality
Introduction
Mesothelioma is a rare, but deadly form of cancer, arising in the mesothelial surfaces (1) in the pleura, peritoneal, and pericardial cavities; the most common form of mesothelioma, accounting for 65–70% of all cases, is malignant pleural mesothelioma followed by peritoneal (30%) and pericardial mesothelioma (1–2%) (2). There are three subtypes, according to the histological morphology: epithelial, sarcomatoid, and biphasic (1).
Mesothelioma has a very poor prognosis with a median survival from the time of presentation of approximately 9–12 months (3). Despite the introduction of modern therapeutic interventions, only modest changes in survival are observed over time (1). There is a well-established causal relationship between asbestos exposure and malignant mesothelioma, although the latency period can be long. Research suggests that the average latency period is approximately 40 years, although in some cases, it may be as long as 60–70 years (4-9). The association with asbestos exposure is especially strong for the pleural site, where 80% of patients report a history of asbestos exposure (2). Among asbestos highly exposed individuals, the lifetime risk of mesothelioma can vary from 5–10% to 25% (3,4,10). Increased knowledge and better regulations since the early 1980’s, with restrictions or bans on production and use of asbestos in many developed countries has led to abatement of exposure, particularly in the occupational setting. Four subsequent bans on asbestos between 1973 and 1989 in the United States (US) resulted in decreased asbestos consumption and production, followed by a decline of mesothelioma incidence and mortality rates 20 years later (11). However, despite bans, people may still be exposed to asbestos, due to its presence in several structures such as schools or public buildings, and the construction of residential areas in close proximity to former asbestos mines, factories, or soil containing natural asbestos. Thus the disease burden associated with environmental asbestos exposure remains difficult to quantify and is understudied (6,7,12). Furthermore, a ban on the use and production of asbestos has not been implemented globally; countries that have a ban instituted it at different points in time (5), making the estimate of the future mesothelioma risk in the general population uncertain.
The goal of this report is to provide an overview of asbestos use, and mesothelioma incidence and mortality in the US and Europe [defined as the 53 countries in the European region of the World Health Organization (WHO)] (13), within the context of changes in asbestos policies around the world.
Data sources and methods
This report used several publicly available data sources. Asbestos consumption (calculated as production plus imports minus exports) was assessed per capita, in 1980 and 2007, using reports from the United States Geological Survey (USGS) (14,15), with population estimates compiled by the World Bank (16). Negative values of asbestos consumption (reflecting export of storage from previous years) were treated as zero. Overall and age specific mesothelioma incidence rates (IR) [2008–2012] were extracted from the Cancer Incidence in Five Continents Volume XI (CI5 Vol. XI) data made available by the WHO and the International Agency for Research on Cancer (IARC) (17). IR over time were calculated using Surveillance, Epidemiology, and End Results (SEER) data (18) (US) and WHO C15plus data (Europe) (17,19), which includes annual incidence of selected cancers for the longest possible period. For this analysis, only registries with continuous information from 1980–2012 were included (SEER-9 Registries for the US; Denmark, France Calvados, France-Doubs, France-Isere, Germany-Saarland, Iceland, Israel, Italy-Parma, Norway, Switzerland-Geneva and UK-Scotland for Europe). Mortality rates were queried from the IARC WHO Cancer Mortality Database (20). All incident and mortality rates are age-adjusted to the world standard population (21).
Results
Worldwide bans on asbestos and asbestos consumption
Since the 1970’s, countries have banned asbestos to varying degrees, with 67 countries worldwide having a total ban, as of July 15, 2019 (22). Although the US banned some forms of asbestos in 1973, and attempted to ban most asbestos-containing products in 1989 through the Toxic Substances Control Act, the ban was overturned in 1991 (23). To this day, the US does not have a full nationwide ban on asbestos. However there are many laws regulating the use of asbestos at the federal, state, and local level (24). In Europe, individual regulations banning asbestos were passed from the 1980’s through the early 2000’s in many countries (13,22,25,26). Member states of the European Union (EU) banned five of the six types of asbestos in 1991 (amosite, crocidolite, anthophyllite, tremolite, and actinolite) and a ban prohibiting the new use of chrysotile went into effect on January 1, 2005 (27). Details of asbestos bans, by country are shown in Table 1 (13,22,25,26).
Table 1. Asbestos bans and regulations in the United States and Europe.
| Country | Year | Description |
|---|---|---|
| United States | 1973 | Ban on spray-applied surfacing asbestos-containing material for fireproofing and insulation |
| 1989 | Toxic Substances Control Act bans most asbestos-containing products | |
| 1991 | Ban overturned, no current nationwide ban | |
| European Union | ||
| Austria† | 1990 | Ban on chrysotile asbestos |
| Belgium† | 1998 | Ban on chrysotile asbestos is introduced |
| Bulgaria | 2005 | Ban on import, production, and use of all asbestos |
| Croatia | 1993 | Ban on crocidolite and amosite |
| 2006 | Asbestos added to list of prohibited substances, in line with EU regulations, but ban is not thought to be well enforced | |
| Cyprus† | 2005 | Prohibits new use of chrysotile, other forms of asbestos previously banned under EU regulations |
| Czech Republic† | 1998 | Ban on the import of asbestos |
| 2005 | Prohibits new use of chrysotile, other forms of asbestos previously banned under EU regulations | |
| Denmark† | 1980 | Ban on uses of asbestos, with exceptions |
| 1985 | Extends ban to include asbestos cement products, further restrictions in 1986–1988 | |
| Estonia† | 2005 | Prohibits new use of chrysotile, other forms of asbestos previously banned under EU regulations |
| Finland† | 1992 | Phase-out ban on chrysotile |
| France† | 1996 | Ban on chrysotile |
| Germany† | 1993 | Ban on chrysotile asbestos (minor exemptions), amosite and crocidolite were banned previously |
| Greece† | 2005 | Prohibits new use of chrysotile, other forms of asbestos previously banned under EU regulations |
| Hungary† | 1988 | Ban on amphibole asbestos, with further bans on non-chrysotile asbestos in 1992, 2001, and 2003 |
| 2005 | Prohibits new use of chrysotile, other forms of asbestos previously banned under EU regulations | |
| Ireland† | 2000 | Ban on chrysotile asbestos |
| Italy† | 1992 | Ban on all types of asbestos (with some exceptions until 1994) |
| Latvia† | 2001 | Ban on asbestos (some exemptions) |
| Lithuania† | 1998 | First law restricting asbestos use |
| 2005 | Prohibits new use of chrysotile, other forms of asbestos previously banned under EU regulations | |
| Luxembourg† | 2002 | Phase out ban on asbestos |
| Malta† | 2005 | Prohibits new use of chrysotile, other forms of asbestos previously banned under EU regulations |
| Netherlands† | 1991 | First in a series of bans on chrysotile |
| Poland† | 1997 | Ban on all asbestos |
| Portugal† | 2005 | Prohibits new use of chrysotile, other forms of asbestos previously banned under EU regulations |
| Romania | 2005 | Prohibits new use of chrysotile, other forms of asbestos previously banned under EU regulations |
| Slovakia† | 2005 | Prohibits new use of chrysotile, other forms of asbestos previously banned under EU regulations |
| Slovenia† | 1996 | Ban on production of asbestos cement products |
| Spain† | 2002 | Phase out ban on asbestos |
| Sweden† | 1982 | First in a series of bans on various uses of asbestos |
| 1986 | Ban on use of all asbestos products | |
| United Kingdom† | 1999 | Ban on chrysotile asbestos, with minor exceptions |
| Other European nations | ||
| Albania | – | No ban |
| Andorra | – | No ban |
| Armenia | – | No ban |
| Azerbaijan | – | No ban |
| Belarus | – | No ban |
| Bosnia and Herzegovina | – | No ban |
| Georgia | – | No ban |
| Iceland | 1983 | Ban on all types of asbestos (with exceptions); bans updated in 1996 |
| Israel | 1980 | Series of restrictions on asbestos, which eventually became a de facto ban |
| Kazakhstan | – | No ban |
| Kyrgyzstan | – | No ban |
| Monaco | 2016 | Total ban on all forms of asbestos |
| Montenegro | – | No ban |
| North Macedonia | 2014 | Total ban on all forms of asbestos |
| Norway | 1984 | Ban on all asbestos |
| Republic of Moldova | – | No ban |
| Russian Federation | – | No ban |
| San Marino | – | No ban |
| Serbia | 2011 | Ban on all asbestos |
| Switzerland | 1989 | Ban on crocidolite, amosite, and chrysotile |
| Tajikistan | – | No ban |
| Turkey | 2010 | National regulation banning use of all types of asbestos |
| Turkmenistan | – | No ban |
| Ukraine | 2017 | Complete ban on asbestos announced, implementation may be delayed |
| Uzbekistan | – | No ban |
†, members of the European Union as of 2005, subject to the directive mandating all member states ban new uses of chrysotile. Other forms of asbestos were banned in 1991 for EU member states. All member states of the EU, Iceland, Israel, Macedonia, Monaco, Norway, Serbia, Switzerland, and Turkey have banned the use of all types of asbestos, as of July 15, 2019. EU, European Union.
Previous research (5,13) has defined asbestos consumption >1 kg/capita/year as “high”, as it corresponded to a 2.4- and 1.6-fold increase in mesothelioma deaths among men and women, respectively. Consumption >2 kg/capita/year was considered “very high”. Data from 1980 (14), before asbestos bans were widely implemented, show that asbestos consumption was very high in some parts of Europe, exceeding 5 kg/capita in the former Soviet Union (estimates for Russian Federation and Kazakhstan: 9.6 kg/capita), Cyprus (7.4 kg/capita), Germany (5.6 kg/capita), and former Yugoslavian states (combined estimates for all former Yugoslav nations: 5.2 kg/capita). Asbestos consumption for Belgium and Luxembourg (4.7 kg/capita), Hungary (4.0 kg/capita), Switzerland (3.3 kg/capita), Italy (3.2 kg/capita), Czech Republic and Slovakia combined (3.1 kg/capita), Austria (2.7 kg/capita), Denmark (2.7 kg/capita), Ireland (2.5 kg/capita), Poland (2.3 kg/capita), France (2.3 kg/capita), and Portugal (2.04 kg/capita) all exceeded 2 kg/capita, while it exceeded 1 kg/capita in Spain, Greece, United Kingdom, Netherlands, and Finland. Consumption in the US was also high at 1.6 kg/capita (Figure 1A), although it was already in decline from its peak in the early 1970’s (28).
Figure 1.
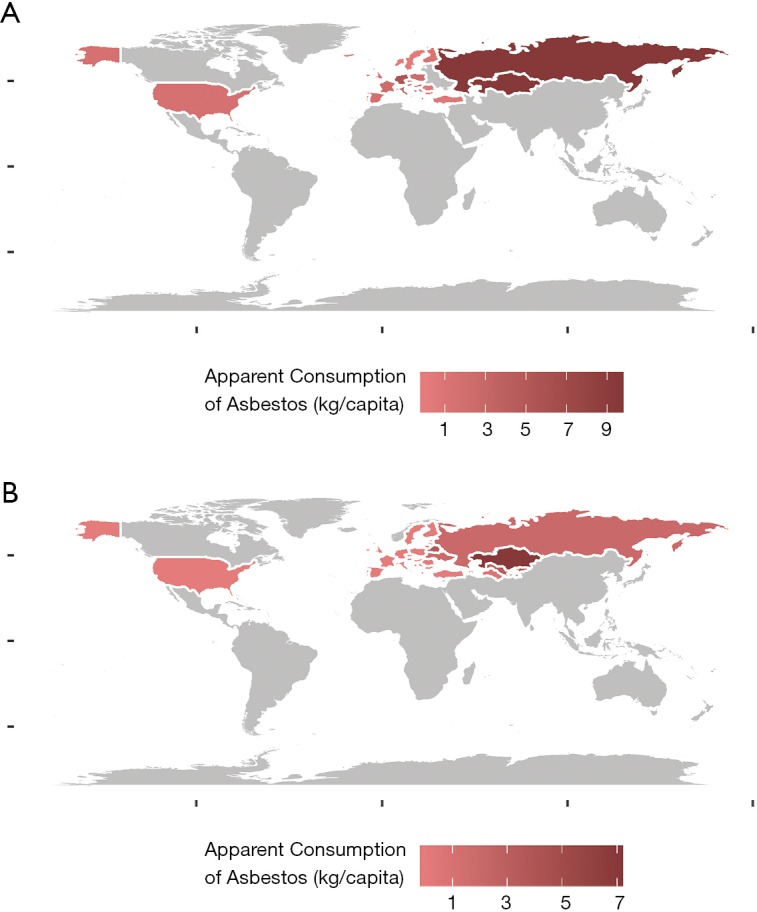
Apparent consumption (kg/capita) of asbestos in (A) 1980 and (B) 2007 in the United States and Europe.
The most recent available data refer to 2007 (15), and indicates that asbestos consumption has declined considerably in most countries in the years since bans were enacted (or attempted) (Figure 1B). US consumption was 0.003 kg/capita in 2007, while most of the countries in the EU had decreased to 0 (or nearly 0) kg/capita. Asbestos consumption remained high or very high in Kazakhstan (7.0 kg/capita), Kyrgyzstan (4.0 kg/capita), Belarus (3.5 kg/capita), Uzbekistan (3.2 kg/capita), Russian Federation (2.0 kg/capita), and Ukraine (1.8 kg/capita).
An advance report from the USGS for 2016 (29) indicates that consumption has started to decline in Ukraine (0.4 kg/capita) and Belarus (0.6 kg/capita), although it remains high or very high in the Russian Federation (1.6 kg/capita), Kazakhstan (1.4 kg/capita), Kyrgyzstan (1.1 kg/capita), and Uzbekistan (2.2 kg/capita).
Mesothelioma IR
Research has shown that IR of mesothelioma are lower in women than in men, and this difference has been attributed to historical differences in occupational asbestos exposure (30,31). From 2008 to 2012, the world standardized IR (WSIR), per 100,000 persons in the US was 0.9 for males and 0.3 for females. Overall in Europe, the WSIR per 100,000 was 1.7 for males and 0.4 for females. Data is limited for nations of the former Soviet Union, Russian Federation and former Yugoslavia, but for those with data, reported WSIR for males and females were 0.5 and 0.3 (Russian Federation), 1.5 and 0.3 (Croatia), and 1.5 and 0.5 (Slovenia) per 100,000 persons. In some of the other countries with very high asbestos consumption, WSIR remain high, particularly for males versus females: 2.0 and 0.4 (Belgium), 2.0 and 0.3 (Switzerland), 1.9 and 0.3 (Denmark), 1.8 and 0.6 (Italy), and 1.6 and 0.3 (Germany) per 100,000 persons. WSIR are also very high in the Netherlands (2.8 in males and 0.4 in females), and United Kingdom (3.4 and 0.6) (Figure 2). As women generally are less likely to be occupationally exposed, the high WSIR in females observed in certain countries, such as Italy, United Kingdom, and Turkey may indicate other sources of exposure that are difficult to detect, such as higher levels of environmental exposure. The classification of environmental, non-occupational exposure to asbestos is very heterogeneous in the literature and often includes (I) areas with naturally occurring asbestos, (II) neighborhood exposure based on residence in close proximity to industrial/mining sources of asbestos, and (III) household exposure for family members of occupationally exposed people, of which the latter two are more specific exposure risk factors for females (6). Furthermore, a caveat when comparing data collected in different countries is that there may be differences in patterns of reporting for mesothelioma, misclassification in diagnosis, or lack of the medical resources required to accurately diagnose the disease.
Figure 2.
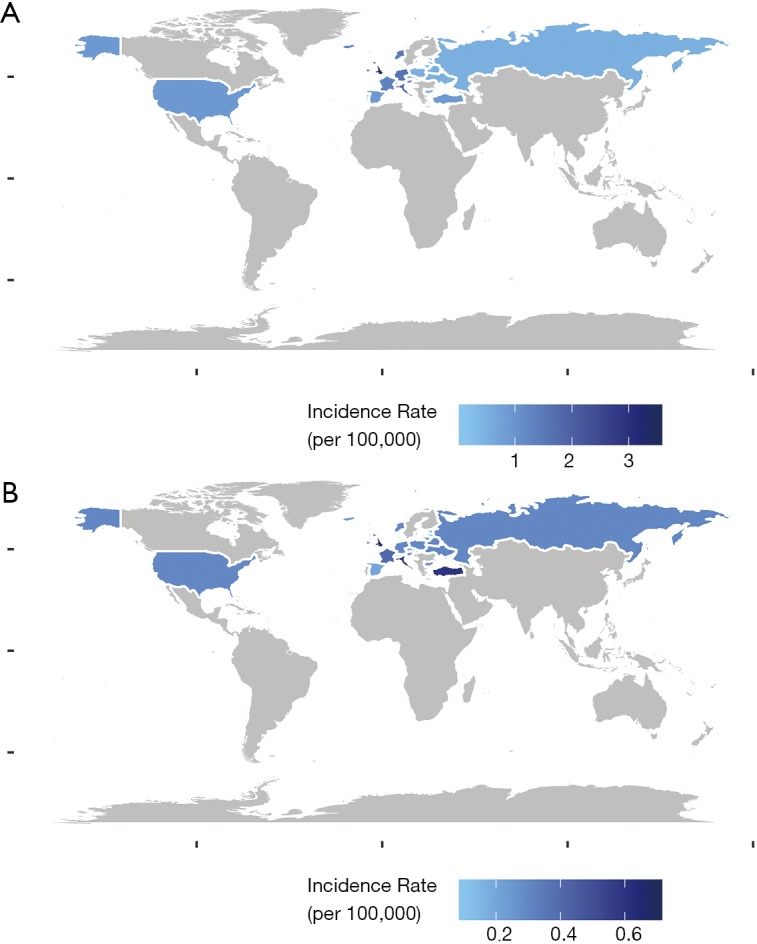
World standardized incidence rates of mesothelioma in the United States and Europe for (A) men and (B) women, 2008–2012.
Age related patterns
Mesothelioma is extremely rare in younger subjects, with a sharp uptick in IR starting between 50–60 years of age (4). Prior to age 50, the annual WSIR in the US for males is ≤0.3 per 100,000 persons, while for females it is ≤0.2. In Europe, the rates are ≤0.6 per 100,000 for males and ≤0.4 per 100,000 for females for the same age group. In the US, the IR for males aged 50–54 years is 0.6 per 100,000, while for females it is 0.4 per 100,000. The rate starts climbing faster in Europe, with an IR of 1.4 per 100,000 for males, and 0.6 per 100,000 for females at age 50–54 years. As people age, this gap across the US and Europe continues to widen, particularly for males. For those ≥80 years, the IRs for males in the US and Europe are 18.9 and 22.8 per 100,000, respectively; for females, it is 3.0 and 3.4 per 100,000 (Figure 3).
Figure 3.

Age specific annual incidence rates [2008–2012], for (A) United States and (B) Europe, by gender.
Time trends
Given the long latency period of mesothelioma (approximately 40 years, on average) (4), we may now just be beginning to see the effects of asbestos bans. In the US there is no official ban in place, however attempts were made to ban asbestos as far back as 1973, and as a result general consumption was lower in 1980 in the US as compared to Europe. Over time, the IR has started to decline in the US from 1980–2016, mostly driven by a decline in the IR for males, while females have mostly held steady (Figure 4A). In Europe, rates of mesothelioma were rising sharply in the early 2000’s, and may just now be beginning to level off (Figure 4B). This may be partly due to the later introduction of asbestos bans in parts of Europe, and the higher consumption observed at least 40 years ago in many geographic areas. As overall rates have slowly fallen in the US, and risen in Europe, with steady rates for females, females now make up a larger portion of those with mesothelioma in the US than in Europe (Figure 4C).
Figure 4.

World standardized incidence rates (per 100,000) over time, overall and by gender in the (A) United States, and (B) Europe. (C) Ratio of world standardized incidence rates for females vs. males, over time in the United States and Europe.
Mesothelioma mortality
Survival rates for mesothelioma are low, with estimated median survival of 9–12 months (3). Research has shown that females have significantly better overall survival (32-34), and speculated reasons include less amount and duration of exposure (35), more favorable clinical characteristics (36,37), and protective effects of estrogen (38,39). For countries in which IR and mortality rates were available, the ratio of the mortality rate to the IR was calculated. In almost all cases, this ratio exceeds 0.5, and in many cases exceeds 0.75, indicating high mortality rates among those with mesothelioma. Generally, the ratio was lower for females (Table 2), reflecting the better survival reported by individual studies for females with all forms of mesothelioma.
Table 2. Ratio of annual world standardized mortality rates to incidence rates [2008–2012], by country, for males and females.
| Country | Mortality rate to incidence rate ratio [2008–2012]† | |
|---|---|---|
| Male | Female | |
| United States | 0.89 | 0.67 |
| Austria | 0.82 | 1.00 |
| Belgium | 0.80 | 0.75 |
| Bulgaria | 0.20 | 0.00 |
| Croatia | 0.87 | 1.00 |
| Cyprus | 0.62 | 0.33 |
| Czech Republic | 0.75 | 0.50 |
| Denmark | 0.68 | 1.00 |
| Estonia | 1.00 | 0.50 |
| France | 0.85 | 0.75 |
| Germany | 0.69 | 0.67 |
| Iceland† | 0.42 | 1.00 |
| Ireland | 0.90 | 0.50 |
| Israel | 0.86 | 0.50 |
| Italy | 0.83 | 0.67 |
| Latvia | 1.00 | 1.00 |
| Lithuania | 1.00 | 1.00 |
| Malta | 0.74 | 1.00‡ |
| Netherlands | 0.89 | 0.75 |
| Norway | 0.80 | 0.67 |
| Poland | 0.80 | 0.67 |
| Portugal | 0.60 | – |
| Slovakia | 0.29 | 0.50 |
| Slovenia† | 0.60 | 0.80 |
| Spain | 0.67 | 1.00 |
| Switzerland | 0.90 | 0.67 |
| United Kingdom | 0.88 | 0.83 |
†, combined incidence rates are available from 2008–2012. Combined mortality rates are queried from all years available from 2008–2012 for each country. For some countries, not all years from 2008–2012 were available. ‡, due to data from difference sources, some mortality rates exceed incidence rates for the same time frame. Those ratios are recorded as 1. Russian Federation, Turkey, Ukraine, and Belarus reported incidence rates, but no mortality information. Armenia, Finland, Georgia, Hungary, Kazakhstan, Kyrgyzstan, Luxembourg, Republic of Moldova, Romania, Serbia, and Sweden, reported mortality rates, but not incidence information. Albania, Andorra, Azerbaijan, Bosnia and Herzegovina, Greece, Macedonia, Monaco, Montenegro, San Marino, Tajikistan, Turkmenistan, and Uzbekistan reported no mesothelioma information.
Comment
Although the US recognized the dangers of asbestos exposure early and in 1973 produced the first asbestos regulation followed by a complete ban in 1989, the country currently has no nationwide ban. Many countries in Europe independently implemented partial or total asbestos bans in the 1980’s and 1990’s, while member states of the EU banned most types of asbestos in 1991, with a complete ban on all remaining types of asbestos in effect starting in 2005. However, many non-EU states implemented bans later, while some still have no ban in place. The difference in the timeframe for asbestos ban legislation in the US and Europe, combined with a latency period of decades between exposure and mesothelioma partly explains why a slight decrease in mesothelioma standardized IR is seen in the US, consistent with previous research (11), while the incidence has just started to level off in Europe. There is speculation that the observed decrease in mesothelioma incidence is slower than projected (40), and that other factors, including individual genetic susceptibility, could play a role (41).
However, observational data from cancer registries prove that legislation on asbestos use and production is an effective way to decrease occupational exposure to asbestos, and therefore, mesothelioma rates in the general population, especially in males. Current legislation is insufficient to address neighborhood asbestos exposure based on residence in close proximity to industrial/mining sources of asbestos and household asbestos exposure for family members of occupationally exposed people, as well as other sources of environmental exposure. To further decrease risk from environmental asbestos exposure, legislation for building in regions with naturally occurring asbestos should be explored. These results stress the need for a global forum to urge countries that currently don’t have an asbestos ban to start implementing appropriate legislation.
One interesting observation is that any change in IR is mainly caused by a decrease in mesothelioma occurrence among males, while the IR of mesothelioma for females remains more stable. This may reflect the fact that asbestos exposure has shifted from occupational, mostly present in males, to environmental exposure, and indicates that current asbestos regulations do not sufficiently consider all sources of environmental exposure. The male/female (M/F) ratio has been used as a relatively reliable surrogate to distinguish environmental from occupational exposure (6,7), with a M/F ratio approaching one as a sign that environmental exposure plays a more important role. The identification of current sources of environmental exposure to asbestos and the associated health effects in the general population remains an important area of future research, including the identification of geographic areas where asbestos is naturally present in the environment (42). The difference in incidence with gender is of special importance because females with malignant mesothelioma have a significantly better survival than males, although the precise reasons for this observation are still uncertain (32,33). Given the positive effects of legislation on occupational exposure to asbestos, the next step will be to shift the focus of research and legislation to environmental sources of asbestos exposure, in order to target all potential avenues of asbestos exposure. Because mesothelioma is a rare but deadly disease, and combined with the changing landscape of asbestos exposure, mesothelioma registries capturing mesothelioma cases in real-time are of utmost importance to investigate the many unanswered scientific questions. Countries with mesothelioma registries are able to research and respond to the current scientific and legislative needs associated with mesothelioma incidence and mortality.
In conclusion, we report here the status of mesothelioma epidemiology in the recent years, and observe that asbestos exposure is still a burden worldwide, and legislative action is needed to obtain a complete ban. The pattern of mesothelioma is shifting from a mostly male disease to a disease that affects females as well in substantial numbers. Studies on unknown sources of asbestos exposure, of other sources of natural exposure to asbestos and asbestos-like fibers, as well as of individual genetic susceptibility to asbestos fibers are needed.
Acknowledgments
Funding: None.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Footnotes
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- 1.Yang H, Testa JR, Carbone M. Mesothelioma Epidemiology, Carcinogenesis and Pathogenesis. Curr Treat Options Oncol 2008;9:147-57. 10.1007/s11864-008-0067-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bridda A, Padoan I, Mencarelli R, et al. Peritoneal Mesothelioma: A Review. MedGenMed 2007;9:32. [PMC free article] [PubMed] [Google Scholar]
- 3.Robinson BW, Musk AW, Lake RA. Malignant mesothelioma. Lancet 2005;366:397-408. 10.1016/S0140-6736(05)67025-0 [DOI] [PubMed] [Google Scholar]
- 4.Mott FE. Mesothelioma: A Review. Ochsner J 2012;12:70-9. [PMC free article] [PubMed] [Google Scholar]
- 5.Lin RT, Takahashi K, Karjalainen A, et al. Ecological association between asbestos-related diseases and historical asbestos consumption: an international analysis. Lancet 2007;369:844-9. 10.1016/S0140-6736(07)60412-7 [DOI] [PubMed] [Google Scholar]
- 6.Liu B, van Gerwen M, Bonassi S, et al. Epidemiology of Environmental Exposure and Malignant Mesothelioma. J Thorac Oncol 2017;12:1031-45. 10.1016/j.jtho.2017.04.002 [DOI] [PubMed] [Google Scholar]
- 7.Selikoff IJ, Churg J, Hammond EC. Asbestos Exposure and Neoplasia. JAMA 1964;188:22-6. 10.1001/jama.1964.03060270028006 [DOI] [PubMed] [Google Scholar]
- 8.McDonald JC, McDonald AD. The epidemiology of mesothelioma in historical context. Eur Respir J 1996;9:1932-42. 10.1183/09031936.96.09091932 [DOI] [PubMed] [Google Scholar]
- 9.Bianchi C, Giarelli L, Grandi G, et al. Latency periods in asbestos-related mesothelioma of the pleura. Eur J Cancer Prev 1997;6:162-6. [PubMed] [Google Scholar]
- 10.Saba R, Aronu GN, Bhatti RP, et al. Malignant mesothelioma after household exposure to asbestos. Case Rep Oncol Med 2013;2013:570487. 10.1155/2013/570487 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sun H. North-south gradient of mesothelioma and asbestos consumption-production in the United States- Progresses since the 1st asbestos partial ban in 1973. Am J Ind Med 2019;62:337-46. 10.1002/ajim.22955 [DOI] [PubMed] [Google Scholar]
- 12.Noonan CW. Environmental asbestos exposure and risk of mesothelioma. Ann Transl Med 2017;5:234. 10.21037/atm.2017.03.74 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kameda T, Takahashi K, Kim R, et al. Asbestos: use, bans and disease burden in Europe. Bull World Health Organ 2014;92:790-7. 10.2471/BLT.13.132118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Virta RL. Worldwide asbestos supply and consumption trends from 1900 through 2003: United States Geological Survey. Circular 1298, 2006;80. [Google Scholar]
- 15.Mineral Industry Surveys. World Asbestos Consumption From 2003 Through 2007. United States Geological Survey, 2009.
- 16.The World Bank. DataBank: Population estimates and projections [Internet]. [cited 2019 Jul 11]. Available online: https://databank.worldbank.org/reports.aspx?source=Health%20Nutrition%20and%20Population%20Statistics:%20Population%20estimates%20and%20projections#
- 17.Bray F, Colombet M, Mery L, et al. Cancer Incidence in Five Continents, Vol. XI (electronic version). [Internet]. Lyon: International Agency for Research on Cancer; 2017 [cited 2019 May 24]. Available online: http://ci5.iarc.fr/CI5-XI/Default.aspx [Google Scholar]
- 18.National Cancer Institute, DCCPS, Surveillance Research Program. Surveillance, Epidemiology, and End Results (SEER) Program SEER*Stat Database: Incidence-SEER 9 Regs Research Data, Nov 2018 Sub (1975-2016) 2019 Apr.
- 19.Ferlay J, Colombet M, Bray F. Cancer Incidence in Five Continents, CI5plus: IARC CancerBase No. 9 [Internet]. Lyon, France: International Agency for Research on Cancer; 2018 [cited 2019 May 24]. Available online: http://ci5.iarc.fr/CI5plus/Default.aspx [Google Scholar]
- 20.World Health Organization, Department of Information, Evidence, and Research. Cancer Mortality Database [Internet]. [cited 2019 May 24]. Available online: http://www-dep.iarc.fr/WHOdb/WHOdb.htm
- 21.International Agency for Research on Cancer, World Health Organization. Age distribution of the world standard population used for age standardization in CI5. [cited 2019 May 24]. Available online: http://ci5.iarc.fr/CI5plus/Pages/glossary.aspx
- 22.London: International Ban Asbestos Secretariat. Current Asbestos Bans 2019 [cited 2019 Jul 22]. Available online: http://www.ibasecretariat.org/alpha_ban_list.php
- 23.University of Montana. International Bans on Asbestos Use. [cited 2019 Jul 2]. Available online: http://www.umt.edu/bioethics/libbyhealth/Resources/Legal%20Resources/international_ban_asbestos.aspx
- 24.Farquhar D, Hendrick D. State Asbestos Enforcement. National Conference of State Legislatures, 2009 Oct 7. [Google Scholar]
- 25.London: International Ban Asbestos Secretariat. Chronology of Asbestos Bans and Restrictions 2019 [cited 2019 Jul 2]. Available online: http://www.ibasecretariat.org/chron_ban_list.php
- 26.Haynes RC. A Worn-Out Welcome. Environ Health Perspect 2010;118:A298-303. 10.1289/ehp.118-a298 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.European Commission. The European Commission bans White Asbestos. [cited 2019 Sept 12]. Available online: https://europa.eu/rapid/press-release_IP-99-572_en.htm
- 28.Allen LP, Baez J, Stern MEC, et al. Trends and the Economic Effect of Asbestos Bans and Decline in Asbestos Consumption and Production Worldwide. Int J Environ Res Public Health 2018;15:531. 10.3390/ijerph15030531 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Flanagan D. Asbestos [Advance Release]: U.S. Geological Survey Minerals Yearbook 2016 2018 [cited 2019 Jul 1]; Available online: https://s3-us-west-2.amazonaws.com/prd-wret/assets/palladium/production/mineral-pubs/asbestos/myb1-2016-asbes.pdf
- 30.Hyland RA, Ware S, Johnson AR, et al. Incidence trends and gender differences in malignant mesothelioma in New South Wales, Australia. Scand J Work Environ Health 2007;33:286-92. 10.5271/sjweh.1145 [DOI] [PubMed] [Google Scholar]
- 31.Marinaccio A, Corfiati M, Binazzi A, et al. The epidemiology of malignant mesothelioma in women: gender differences and modalities of asbestos exposure. Occup Environ Med 2018;75:254-62. 10.1136/oemed-2016-104119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Taioli E, Wolf AS, Camacho-Rivera M, et al. Women With Malignant Pleural Mesothelioma Have a Threefold Better Survival Rate Than Men. Ann Thorac Surg 2014;98:1020-4. 10.1016/j.athoracsur.2014.04.040 [DOI] [PubMed] [Google Scholar]
- 33.Van Gerwen M, Alpert N, Wolf A, et al. Prognostic factors of survival in patients with malignant pleural mesothelioma: an analysis of the National Cancer Database. Carcinogenesis 2019;40:529-36. 10.1093/carcin/bgz004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Soeberg MJ, Leigh J, Driscoll T, et al. Incidence and survival trends for malignant pleural and peritoneal mesothelioma, Australia, 1982-2009. Occup Environ Med 2016;73:187-94. 10.1136/oemed-2015-103309 [DOI] [PubMed] [Google Scholar]
- 35.Hillerdal G. Mesothelioma: cases associated with non-occupational and low dose exposures. Occup Environ Med 1999;56:505-13. 10.1136/oem.56.8.505 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Yan TD, Popa E, Brun EA, et al. Sex difference in diffuse malignant peritoneal mesothelioma. Br J Surg 2006;93:1536-42. 10.1002/bjs.5377 [DOI] [PubMed] [Google Scholar]
- 37.Milano MT, Zhang H. Malignant pleural mesothelioma: a population-based study of survival. J Thorac Oncol 2010;5:1841-8. 10.1097/JTO.0b013e3181f1cf2b [DOI] [PubMed] [Google Scholar]
- 38.Wolf AS, Richards WG, Tilleman TR, et al. Characteristics of malignant pleural mesothelioma in women. Ann Thorac Surg 2010;90:949-56; discussion 956. 10.1016/j.athoracsur.2010.04.110 [DOI] [PubMed] [Google Scholar]
- 39.Pinton G, Brunelli E, Murer B, et al. Estrogen receptor-beta affects the prognosis of human malignant mesothelioma. Cancer Res 2009;69:4598-604. 10.1158/0008-5472.CAN-08-4523 [DOI] [PubMed] [Google Scholar]
- 40.Price B, Ware A. Time trend of mesothelioma incidence in the United States and projection of future cases: an update based on SEER data for 1973 through 2005. Crit Rev Toxicol 2009;39:576-88. 10.1080/10408440903044928 [DOI] [PubMed] [Google Scholar]
- 41.Testa JR, Cheung M, Pei J, et al. Germline BAP1 mutations predispose to malignant mesothelioma. Nat Genet 2011;43:1022-5. 10.1038/ng.912 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Pan XL, Day HW, Wang W, et al. Residential Proximity to Naturally Occurring Asbestos and Mesothelioma Risk in California. Am J Respir Crit Care Med 2005;172:1019-25. 10.1164/rccm.200412-1731OC [DOI] [PMC free article] [PubMed] [Google Scholar]