

Abstract
Background
Cardiovascular disease (CVD) remains the leading cause of death in the United Arab Emirates (UAE). One of the common CVDs is hypertrophic cardiomyopathy (HCM). Recent studies conducted in heart cells of mice have shown that this condition involves a chemical modification called hydroxymethylation of the DNA of heart cells.
Objective
Objectives of the proposed research are to profile the distribution of 5-hydroxymethylation in the cardiomyocyte (CMC) genome of cadaveric cardiac tissue and cardiac biopsy specimens; to compare the hydroxymethylome of cadaveric CMCs with that of cardiac biopsy specimens from HCM patients and/or cardiac transplant patients (control) undergoing cardiac catheterization; to histologically appraise sarcomere distribution and mitochondrial morphology of CMCs in the presence of HCM; to correlate the mitochondrial genome with the HCM phenotype; and to integrate anatomy with biochemistry and genetics into the instructional design of HCM in the core medical curriculum at Mohammed Bin Rashid University of Medicine and Health Sciences (MBRU).
Methods
Normal and hypertrophic heart specimens will be obtained from 8 whole-body cadavers (2/8, 25% control and 6/8, 75% HCM). Myocardial biopsy specimens will be obtained from cardiothoracic and transplant units at the Cleveland Clinic in Abu Dhabi, UAE. As this is a proof-of-concept study, we plan to recruit 5 patients with HCM, where HCM has been diagnosed according to the guidelines of the 2014 European Society of Cardiology Guidelines. Patients with valvular heart disease, history of myocarditis, regular alcohol consumption, or cardiotoxic chemotherapy will be excluded. The control biopsy specimens will be obtained from patients who had received heart transplants. Three investigational approaches will then be employed: (1) gross anatomical evaluation, (2) histological analysis, and (3) profiling and analysis of the hydroxymethylome. These investigations will be pursued with minor modifications, if required, to the standard protocols and in accordance with institutional policy. The objective associated with the education of health professionals will be addressed through a strategy based on Graham’s knowledge translation model.
Results
This study is at the protocol-development stage. The validated questionnaires have been identified in relation to the objectives. The MBRU and the Cleveland Clinic Abu Dhabi Institutional Review Board (IRB) are reviewing this study. Further clarification and information can be obtained from the MBRU IRB. There is funding in place for this study (MBRU-CM-RG2019-08). Currently, we are in the process of standardizing the protocols with respect to the various molecular techniques to be employed during the course of the study. The total duration of the proposed research is 24 months, with a provision for 6 months of a no-cost extension.
Conclusions
The spectrum of CVDs has recently received significant focus from the public health sector in the UAE. HCM is a common familial heart disease, contributing to the sudden increase in the mortality rate of young Emiratis in the UAE. Incorporating artificial intelligence into the identification of epigenetic risk factors associated with HCM will promote accurate diagnosis and lead to the development of improved management plans, hence, positive patient outcomes. Furthermore, integration of these findings into the instructional design of undergraduate, postgraduate, and continuous professional development medical curricula will further contribute to the body of knowledge regarding HCM.
International Registered Report Identifier (IRRID)
PRR1-10.2196/17241
Keywords: epigenomics, mitochondrial genome, hypertrophic cardiomyopathy, undergraduate medical education
Introduction
Background
Geographically, the Arab world is comprised of 22 countries from North Africa to Western Asia—Algeria, Egypt, Bahrain, Comoros, Djibouti, Iraq, Jordan, Saudi Arabia, Kuwait, Lebanon, Libya, Mauritania, Morocco, Oman, occupied Palestinian territory, Qatar, Yemen, Somalia, Sudan (including South Sudan), Syria, Tunisia, and the United Arab Emirates (UAE). These countries comprise the members of the League of Arab States. Each country has an inimitable set of historical, geopolitical, social, cultural, and economic characteristics, which define its public health systems and the burden of disease and injury. In 2014, Mokdad et al assessed the burden of disease and injuries in the 22 Arab countries in 1990, 2005, and 2010, employing data and methods from the Global Burden of Diseases, Injuries, and Risk Factors Study 2010 [1,2]. Interestingly, the study showed that since 1990, premature death and disability caused by communicable, newborn, nutritional, and maternal disorders, with the exception of HIV/AIDS, has decreased in the Arab world with a stark increase in ischemic heart disease, which contributed to 14.3% of deaths (see Figure 1) [1-3]. In addition, if one compares age-standardized mortality rates registered by the World Health Organization for specific countries in the region [4], a marked augmentation of cardiovascular deaths in most countries from the Middle East is observed, including in the UAE, when compared with data from comparator western countries (ie, the United Kingdom, Germany, and the United States); these deaths are predominantly from ischemic heart disease and hypertensive heart disease (see Figure 2).
Figure 1.

Top 25 causes of death in the Arab population in 1990 and 2010 (mean rank). A comparative analysis is provided. Solid blue lines indicate the elevation in rank for a condition or factor responsible for causing death in the Arab population from 1990 to 2010. Green dotted lines indicate a fall in rank of a condition or factor responsible causing death in the Arab population from 1990 to 2010. Red solid lines indicate the elevation or fall in rank of the factors contributing to cardiometabolic syndrome (CMS) in causing death from 1990 to 2010 (note: all the factors contributing to CMS are elevated in rank when compared between 1990 and 2010). Redrawn with modifications from Mokdad et al, 2014. COPD: chronic obstructive pulmonary disease; CV: cardiovascular.
Figure 2.
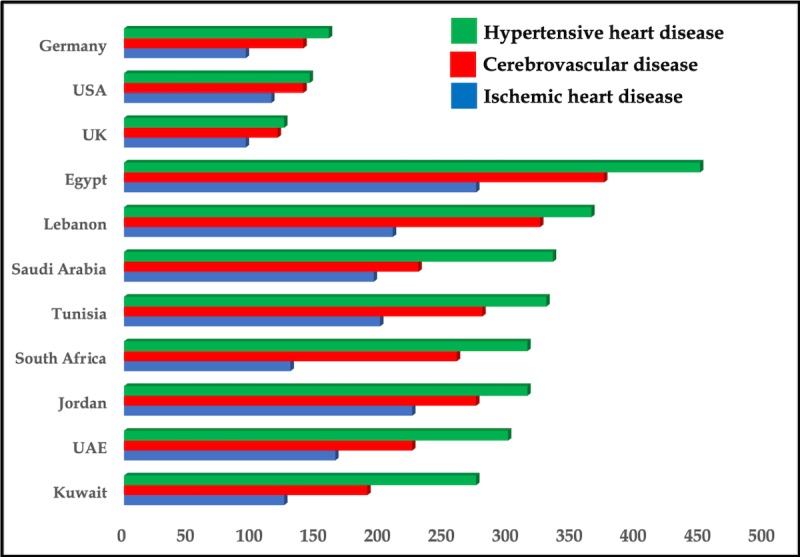
Death rates (ie, number of deaths per 100,000 people) from vascular diseases in selected countries in Africa and the Middle East compared to western countries. Drawn from data presented by the World Health Organization. UAE: United Arab Emirates.
Hence, with recent public health concerns focused on the high prevalence of cardiovascular diseases (CVDs) in the UAE, and with the sudden increase in deaths of relatively young Emiratis from CVD and associated disorders, the UAE National Service has implemented routine screening of all recruits for heart disease [5]. Interestingly, hypertrophic cardiomyopathy (HCM) has been identified as one of the four maladies contributing to the escalation in the mortality rate of young Emiratis, although the detailed statistics are still pending [5].
This necessitates that the molecular mechanism underlying HCM be elucidated, such that novel management and treatment strategies targeting the disorder can be identified and designed. Additionally, it is imperative that the concept of genomics education of physicians be integrated into the medical curriculum in the UAE, such that Emirati medical students can present findings based on correlation with known clinical information about the patients’ diseases and traits.
This is pivotal in light of the revelation that HCM is the most common familial heart disease with vast genetic heterogeneity. Two decades of rigorous investigation have described the vast and intimidating heterogeneity of the HCM substrate. Early reports of seven mutations in one gene—the myosin heavy chain beta isoform (MYH7) [6,7]—have now expanded to 11 or more causative genes with over 1400 mutations, expressed primarily or exclusively in the heart. These genes encode thick and thin myofilament proteins of the sarcomere or contiguous Z-disc. Mutations in several additional sarcomere, or calcium-handling, genes have been proposed, but with less evidence supporting pathogenicity [8]. Also, HCMs show remarkable variability in their age of onset, phenotypic presentation, and clinical course [9], alluding to the fact that disease mechanisms must exist that modify the occurrence and progression of HCM, either by genetic or epigenetic factors that may interact with environmental stimuli and external influences. According to Frey et al [10], HCM develops in response to external influences—ischemia, valvular insufficiency and stenosis, fibrillation, and hypertension—and may eventually progress to heart failure [10]. Further, in the cardiovascular system, histone modifications and chromatin remodeling are believed to modulate adaptive, as well as maladaptive, molecular pathways in HCM and heart failure [11]; as well, methylation of DNA has been responsible for the hypermutability of specific cardiac genes [12]. Additionally, investigations by Jirtle and Skinner [13] as well as Herceg and Vaissiere [14] allude to the potential interplay between environmental factors and the disease phenotype by epigenetic mechanisms. This has been successfully demonstrated in HCM in animal model studies, especially those originating from the Condorelli group [15-17]. Also, studies from the Hein group indicate strict epigenetic regulation during prenatal development and postnatal maturation, as well as in diseased human cardiomyocytes (CMCs) [18-20]. However, the knowledge about the impact of epigenetic alterations on the disease phenotype, specifically in HCM in human patients, is still very limited. This can be attributed to the limited availability of study specimens, because cardiac biopsy is a delicate procedure requiring cardiac catheterization.
Thanatology, which prioritizes the scientific study of death in the context of other fields of interest (ie, medicine, education, psychology, etc), has paved the way for genomic investigation of the pathological state; this is possible as formalin-fixed paraffin embedding of embalmed human cadavers preserves DNA, reduces the rate of decay, and promotes expansion of the available resource bank [21]. In fact, with the improvement in DNA isolation techniques, amplifiable DNA of high quality and quantity has been isolated from nonparaffin-embedded embalmed cadaver tissue [21].
This proposal is founded on the working hypothesis that the hydroxymethylome of cadaveric CMCs with HCM will exhibit epigenetic modification in the form of 5-hydroxymethylation of cytosine (5-hmC) in the genes, in line with observations from animal studies [19].
Study Aims
In line with our working hypothesis, the primary objective of this study involves profiling the distribution of 5-hmC in the CMC genome in cardiac tissue obtained from cadavers and comparing them with the hydroxymethylome of biopsy specimens obtained from the apical part of the free left ventricle (LV); these were collected during left ventricular assist device surgery from HCM patients or cardiac transplant patients (control) undergoing cardiac catheterization using a standardized protocol. Additionally, as HCM is attributable to mutations in the mitochondrial DNA [22], we will compare the mitochondrial genome of cadaveric CMCs with that of biopsy specimens from HCM patients or cardiac transplant patients (control) undergoing cardiac catheterization. A summary of the study is shown in Figure 3.
Figure 3.
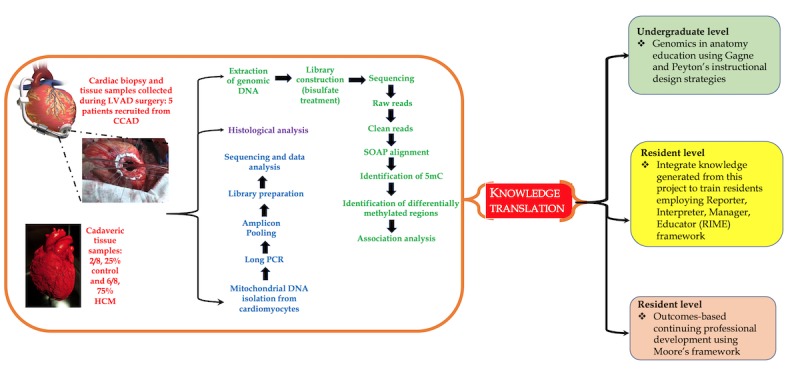
Summary of the proposed study; important steps are indicated (note: the results from this study will be used for competency-based medical education at different levels of training). 5mC: 5-methylation of cytosine; CCAD: Cleveland Clinic Abu Dhabi; HCM: hypertrophic cardiomyopathy; LVAD: left ventricular assist device; SOAP: short oligonucleotide alignment program.
The secondary objective of this study aims to integrate genomics education into medical education, specifically anatomy education, whereby we will blend Graham’s knowledge translation (KT) process [23] with instructional design models from Gagne and Peyton [24]. By doing so, we will strategize a lesson plan using the epigenetics of HCM as a case study to integrate anatomy with genetics and biochemistry into the core medical curriculum at Mohammed Bin Rashid University of Medicine and Health Sciences (MBRU).
In summary, this proposal aims to augment knowledge with regard to epigenetic regulation of HCM—one of the key cardiovascular concerns in the UAE—concomitantly strengthening medical education by integrating genomics education into anatomy. This will stimulate scientific inquiry among medical students, thereby providing KT, such that medical students can present new biomedical findings, correlating them with known clinical information about the patients’ diseases and traits.
Methods
In order to address the primary objective, the following methodology will be implemented.
Sample Collection
The total sample series will be obtained from two different types of tissue specimens, as follows: (1) cadaveric tissue and (2) biopsy specimens.
Cadaveric Series
Normal and hypertrophic heart specimens will be obtained from 8 whole-body cadavers (2/8, 25% control and 6/8, 75% HCM), which have been donated for the promotion of teaching and research to MBRU. As indicated in the cadaver records, 6 cadavers presented with a previous history of pathological conditions causing HCM. All cadavers were commercially embalmed according to standard protocols [25].
Dissection Protocol and Gross Anatomical Evaluation
The thickest heart slice will be selected and subjected to morphometric assessment. A digital caliper—Mitutoyo Digimatic Caliper, Model No. CD-8“ C (Mitutoyo Corporation)—will be used to measure the following parameters:
Thickness of the anterior, lateral, and posterior LV walls (ALV, LLV, and PLV, respectively).
Thickness of the anterior, lateral, and posterior right ventricle (RV) walls (ARV, LRV, and PRV, respectively).
Endocardial trabeculations, papillary muscles, and epicardial fat will be excluded from morphometric assessment.
In an effort to reduce intraobserver error, each parameter will be measured three times, from which a mean value will be determined. Clinical history with associated findings and demographic data (ie, age, race, sex, and nutritional status) pertaining to each cadaver will be documented. Ventricular wall thicknesses that exceeds 1.5 cm and 0.5 cm in the LV and RV, respectively, will be indicative of hypertrophy. These values will also be correlated with the weight of the heart and histological attributes of the CMCs to account for the effects of embalming, duration and method of storage, position of cadaver during storage, and rigor mortis. Heart specimens weighing more than 400 g will be described as hypertrophic.
Recruitment Criteria: Myocardial Biopsy Series
Myocardial biopsy specimens will be obtained from the cardiothoracic and transplant units at the Cleveland Clinic in Abu Dhabi, UAE. Collection will be in accordance with the principles of the Declaration of Helsinki. All participants of the study must provide written informed consent, and the study will be appraised and approved by the relevant ethics committees. HCM will be diagnosed according to the 2014 European Society of Cardiology Guidelines [26]. Patients with valvular heart disease, history of myocarditis, regular alcohol consumption, or cardiotoxic chemotherapy will be excluded. The control biopsy specimens will be obtained from patients who had received heart transplants. To be included in the control cohort, patients would have received successful cardiac transplants more than 6 months previously, with normal systolic and diastolic function and no evidence of relevant vasculopathy as judged by coronary angiography. Furthermore, all control patients will have to exhibit freedom from relevant acute or chronic organ rejection. Details regarding processing of ventricular biopsy specimens are described below.
Processing of Left Ventricle Biopsies
Tissue samples, measuring approximately 2 mm in length, will be extracted from the apical region of the LLV wall of 5 patients diagnosed with HCM and 3 cardiac transplant patients (control) undergoing cardiac catheterization, utilizing a standardized protocol used at the Cleveland Clinic in Abu Dhabi. Biopsies will be washed with NaCl (0.9%) and immediately transferred and stored in liquid nitrogen until DNA or RNA are extracted and histological analysis is pursued.
Histological Analysis
Tissue Preparation
Cadaveric and biopsy specimens will be fixed in an embedding medium. Each specimen will then be dehydrated in a series of alcohol solutions of increasing concentration up to 100% alcohol. Washing will occur for 6-18 hours to remove water. Alcohol will be removed by infiltration of xylene. The specimen will then be placed in a cassette containing liquid paraffin. Once the melted paraffin has cooled and hardened into a mold, it will be trimmed into a suitably sized block. The block will be mounted in a specimen holder of the microtome sectioning machine. By careful rotary movement of the hand wheel, the block will cut thin sections in the form of a ribbon. Individual sections will be partitioned from the ribbon and placed in a water bath of 40°C. They will then be mounted on glass slides with albumin and allowed to dry.
Staining
The glass slide will be placed in xylene before it is passed through a series of solutions of decreasing alcohol concentration. Each glass slide will undergo routine staining with hematoxylin and eosin. Lee’s stain (ie, methylene blue and basic fuchsin) will then be employed to further highlight cytoplasmic organelles and enhance the contrast of the tissue.
The following connective tissue elements will be depicted: (1) nuclei in blue and (2) cytoplasm, mitochondria, and cilia in reddish-pink. The slide will then be passed through xylene to a nonaqueous mounting medium. A coverslip will be placed over the specimen on the slide to attain permanent preparation.
Semiquantitative Analysis
A total of three field areas per slide will be examined. Cross-sectional area, length, and width of CMCs will be quantified. In addition, organization of sarcomeres, mitochondrial size, and arrangement of cristae will be described.
Level of Significance
Statistical analysis will be performed using SPSS Statistics for Windows, version 24.0 (IBM Corp). The means and frequencies of the continuous and categorical variables, respectively, will be compared for difference or equivalence between parameters and demographically relevant factors.PP s of less than .05 will be considered statistically significant.
Profiling, Sequencing, and Analysis of the Hydroxymethylome
Extraction of DNA
DNA will be collected from cadaveric tissues according to the method of Gielda and Rigg, which involves modification of existing techniques of tissue disruption, combined with phenol-chloroform treatment [21]. For biopsy samples, we will use the protocol of Haas et al [27].
Total DNA will be extracted from CMCs from 6 cadaveric hearts diagnosed with HCM, 2 normal cadaveric hearts (control), and biopsy specimens obtained from the apical part of the free LV wall from 5 HCM patients. In addition, DNA will be extracted from the CMCs of 3 cardiac transplant patients (control) undergoing cardiac catheterization. DNA will be enriched for 5-hmC using a biotin-based streptavidin pull-down technique—Hydroxymethyl Collector, Active Motif (Epigenie)—originally described by Song et al [28,29]. The rationale behind employing Song’s technique is that it has been successfully used in other studies [30,31].
Sequencing and Analysis of the Hydroxymethylome
Libraries will be prepared using 500 ng of 5-hmC-enriched DNA using the NEBNext Kit (New England Biolabs) and will be sequenced on the BGISEQ-500 platform (Beijing Genomics Institute, BGI), carried out by the BGI epigenetic sequencing service [32], where the corresponding author has collaborative projects.
The BGISEQ-500 generates approximately 500 Gb of sequence data per flow cell, or about 62 Gb per lane. Therefore, a single human genome library can be run across two lanes of the eight-lane flow cell to generate approximately 120 Gb of data per sample. Additional sequencing will be pursued for higher coverage.
Hydroxymethylation analysis will be performed using the Bismark online module for reading bisulfite sequence maps. In summary, FASTQ files will be quality filtered and adapter sequences will be trimmed using the Trimmomatic tool [33]. A bisulfite-converted human genome (HG19) reference genome file will be generated using Bowtie [34], and the EpiGnome (Epicentre) library sequence data will be aligned to the reference genome.
Hydroxymethylation information will be extracted from the output *.sam file, and genome tracks will be the output for visualization and reporting of downstream differential methylation calculations.
The hydroxymethylation extraction report should show minimal bias. A perfectly unbiased sequencing run would be a horizontal line. Visualization of hydroxymethylated sites of the genome will be performed using the Integrative Genomics Viewer (Broad Institute) [35].
To identify regions that gained or lost 5-hmC at specific differentially hydroxymethylated regions (DhMRs), the normal samples will be set as the control group and the HCM samples as the treated group, and the diffReps program [36] will be used with default settings. The diffReps program normalizes each sample by removing regions of low read counts and then calculates a normalization ratio for each sample based on the remaining reads. The medians of the ratios will then be used as normalization factors. To assess differential sites, diffReps uses a negative binomial test on sliding windows and the significant windows will be selected by a predefined cutoff (P<.001). The significant windows that overlap with each other will then be merged, and the differential sites will be used to perform the statistical tests again. ThePP for each differential site and the bestPP for the sliding window within each differential site will be documented and reported. Subsequently, DhMRs will be classified by diffReps into genomic locations and annotated using the human (HG19) reference genome.
Mitochondrial DNA Isolation
Mitochondrial DNA will be isolated from cadaveric and biopsy samples, for both HCM and control groups, employing the method of Quispe-Tintaya et al, as this technique exhibits an approximately 2000-fold enrichment of mitochondrial DNA in comparison to commercial kits and is also relatively cheaper [37]. Briefly, the process has two steps: (1) extraction of a mitochondrial DNA-enriched fraction employing a common plasmid miniprep kit and (2) additional purification of mitochondrial DNA using the Agencourt AMPure XP system (Beckman Coulter).
Library Preparation and Sequence Analysis of the Mitochondrial Genome
The CMC mitochondrial DNA will be amplified in two fragments using high-fidelity, long-distance polymerase chain reaction (PCR) with a proofreading polymerase—LA Taq DNA polymerase (TaKaRa)—as described by Tang et al [38]. The primers that will be used to amplify cardiac CMC mitochondrial DNA fragment 1 (9289 bp in length) and fragment 2 (7626 bp in length) are shown in Figure 4. The amplified fragments will be used for preparation and sequencing.
Figure 4.
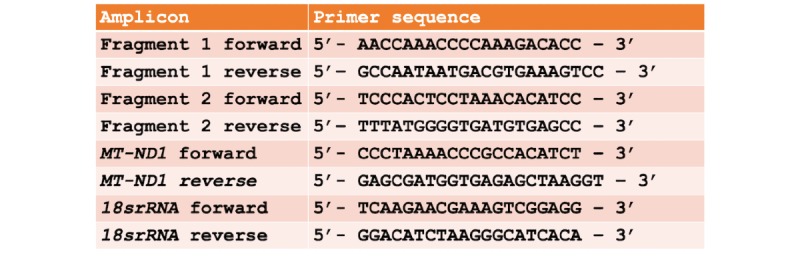
Sequence of primers that will be used to amplify cardiomyocyte (CMC) mitochondrial DNA fragment 1 (9289 bp in length) and fragment 2 (7626 bp in length). 18srRNA: 18S ribosomal RNA; MT-ND1: mitochondrial NADH-ubiquinone oxidoreductase chain 1.
Complementary DNA (cDNA) libraries will be prepared with Nextera sample preparation kits (Illumina). These libraries will be quantified using a PicoGreen assay (Invitrogen) and a Kapa quantitative PCR (qPCR) library quantification kit (Kapa Biosystems). Size and quality of cDNA libraries will be confirmed using an Agilent Bioanalyzer 2100 DNA high-sensitivity chip. The cDNA libraries will then be pooled based on qPCR values. cDNA products will be sequenced in rapid mode using the BGISEQ-500 platform.
Paired-sequence reads will be demultiplexed using bcl2fastq, version 1.8.4 (Illumina). Reads will then be mapped to the reference mitochondrial genome—NC_012920.1 (version GI: 251831106)—and will undergo variant calling using the CLC Genomics Workbench, version 8.0.1 (QIAGEN), alignment tool. This will require a minimum coverage of 1000× and a minimum frequency of 1.00 × 10-6. An average of 7.50 million reads will be mapped per sample. Sequencing data will then be compiled into Microsoft Excel spreadsheet form for analysis. Data in the form of mitochondrial DNA alterations—mutations in specific genes and single-nucleotide polymorphisms (SNPs) at specific loci—between the control and HCM samples will be analyzed using the chi-square test and the Fisher exact test.PP s of less than .05 will be considered statistically significant.
Knowledge Translation
In order to address the secondary objective, we will employ Graham’s KT process (see Figure 5). KT is a dynamic and iterative process that includes synthesis, dissemination, exchange, and ethically sound application of knowledge to improve the health of Emiratis, provide more effective health services and products, and strengthen the health care system [23].
Figure 5.
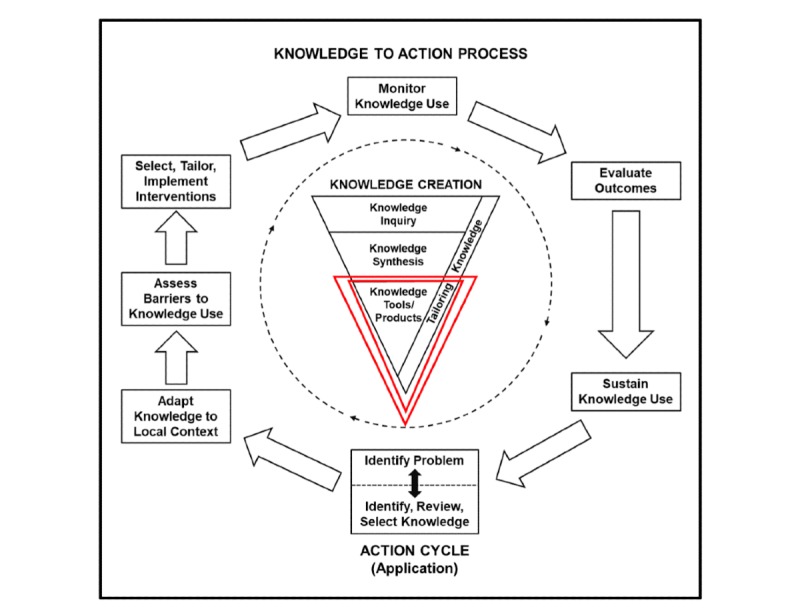
Graham's knowledge translation process (Straus et al, 2011). The central idea of this process is to create knowledge through diverse knowledge tools, which may be in the form of research, that could create new knowledge.
In order to integrate genomics into anatomy education, we will use a blended approach where we will blend Gagne’s approach with Peyton’s approach [24]. A successful implementation of such KT using these approaches is explained using a scenario of familial hypercholesterolemia [39-41], which is the key research interest of the corresponding author. Here, data obtained from a project on familial hypercholesterolemia is used to augment knowledge regarding bioinformatics in undergraduate medical education. Data shown here are from an article by Tambi et al, published in JMIR Medical Education (see Figure 6) [24].
Figure 6.
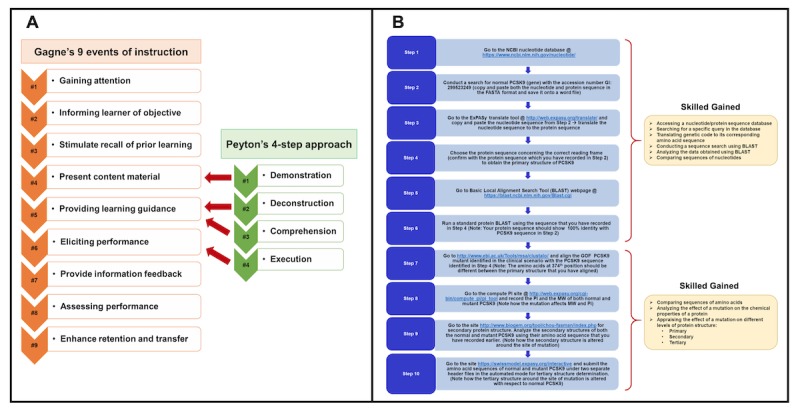
The framework for knowledge translation to be implemented in this study, elaborated using a vignette of autosomal dominant familial hypercholesterolemia. A. Description of the blended lesson plan: Gagne's events of instruction and Peyton's approach. B. The sequential steps of the lesson plan and skills gained. ExPASy: Expert Protein-Analysis System of the Swiss Institute of Bioinformatics; GOF: gain of function; NCBI: National Center for Biotechnology Information; PCSK9: proprotein convertase subtilisin/kexin type 9; PI: isoelectric point; MW: molecular weight.
The proposed research will generate new knowledge with regard to HCM. We aim to add this to the existing knowledge available in the literature and adapt it to suit the needs of medical education in the UAE by assessing barriers to knowledge use (see Figure 5). We will do this via the following proposed KT strategies:
At the undergraduate medical student level, integration of genomics into anatomy education will be pursued by the implementation of instructional design strategies, specifically by blending Gagne’s and Peyton’s approaches (see Figure 6) [24].
At the resident level, KT will involve Pangaro’s Reporter, Interpreter, Manager, Educator (RIME) framework [42], as this model has particular merit for providing feedback to residents.
At the practicing physician level (noncardiologists), KT will be facilitated through outcomes-based continuing professional development devised by Moore (see Figure 7) [43,44].
Figure 7.
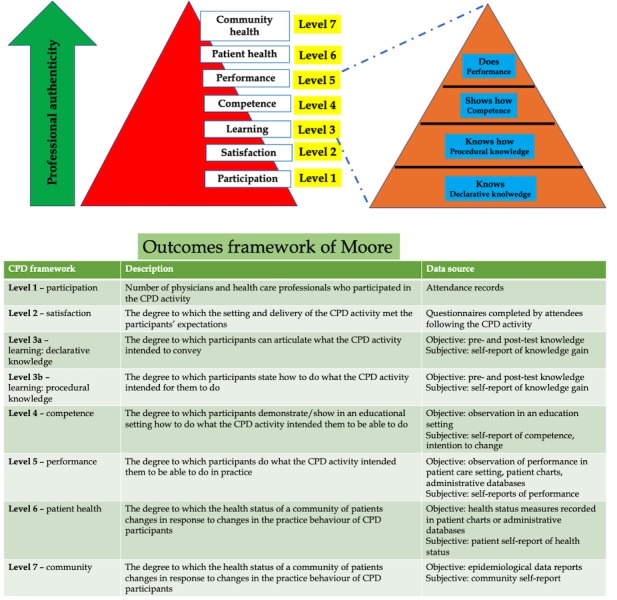
Framework for outcomes-based continuing professional development (CPD) to be used in the proposed research.
Results
This study is at the protocol-development stage. The validated questionnaires have been identified in relation to the objectives. The MBRU and the Cleveland Clinic Abu Dhabi Institutional Review Boards (IRB) are reviewing this study. Further clarification and information can be obtained from the MBRU IRB. There is funding in place for this study (MBRU-CM-RG2019-08). Currently, we are in the process of standardizing the protocols with respect to the various molecular techniques to be employed during the course of the study. The total duration of the proposed research is 24 months, with a provision for 6 months of a no-cost extension. Key project milestones and the timeline are shown in Figure 8.
Figure 8.
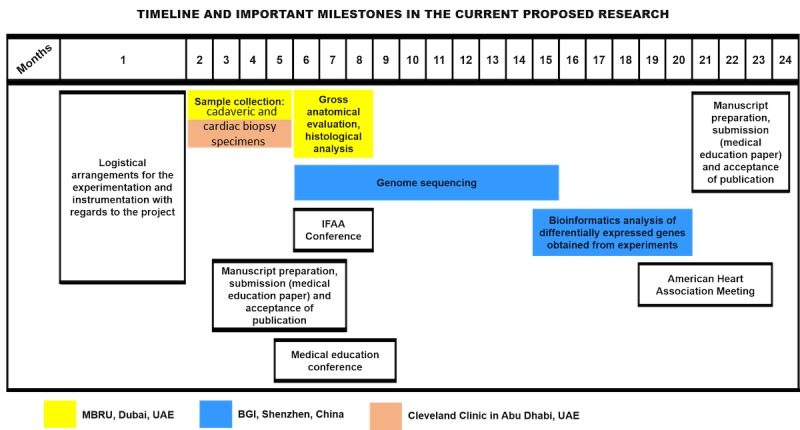
Timeline and key milestones for the study; the sites where the research will be conducted are also indicated. BGI: Beijing Genomics Institute; IFAA: International Federation of Associations of Anatomists; MBRU: Mohammed Bin Rashid University of Medicine and Health Sciences; UAE: United Arab Emirates.
Discussion
Overview
To the best of our knowledge, this is the first study exploring the correlation between the HCM phenotype and alterations in mitochondrial DNA. If a correlation is observed, then a study in a larger HCM cohort is warranted.
Additionally, we believe that specific adjustments will be required in the protocol by Quispe-Tintaya et al [37] when isolating mitochondrial DNA from cadaveric samples. This will provide a standardized protocol for such a procedure, benefitting medicine as well as forensic research.
The problem of nuclear copies of mitochondrial DNA (NUMTs) is often encountered while sequencing mitochondrial DNA. Double bands in PCR results or double peaks in mitochondrial DNA sequences indicate NUMTs, however, the case of mitochondrial DNA heteroplasmy has to be ruled out first. In order to avoid NUMTs, we are using mitochondrial DNA-specific primers and a rigorous mitochondrial DNA purification process. Furthermore, this work will be pursued at BGI [45], where the protocol for the required experimentation is standardized [38].
For the secondary objective, data will be collected through semistructured interviews regarding participants’ use of genomics in their understanding of HCM, as well as the ability of different frameworks to raise awareness regarding the importance of HCM with regard to the Emirati population.
We believe that successful implementation of KT frameworks will support the primary objective, as increased participation in these frameworks will ensure successful dissemination of sequence analysis—in the form of undergraduate students participating in the process—and obtainment of specimens—in the form of resident and physician participation.
Conclusions
The spectrum of CVDs has recently received significant focus from the public health sector in the UAE. While HCM is a common familial heart disease, it is now considered to be one of four CVDs contributing to the sudden increase in the mortality rate of young Emiratis in the UAE. Incorporating artificial intelligence to identify the epigenetic risk factors associated with HCM will promote accurate diagnosis and lead to the development of improved management plans, hence, positive patient outcomes. Furthermore, integration of these findings into the instructional design of undergraduate, postgraduate, and continuous professional development medical curricula will further contribute to the body of knowledge regarding HCM. In summary, this proposal aims to augment knowledge with regard to epigenetic regulation of HCM. This concomitantly strengthens medical education by integrating genomics education into anatomy to stimulate scientific inquiry among medical students. KT is thereby provided, such that medical students can present new biomedical findings, correlating them with known clinical information about patients’ diseases and traits.
Firstly, while this study will include a small cohort of specimens due to tissue accessibility, it will begin to answer the question, “Is there a correlation between epigenetic modification of the genome and HCM phenotype?” and will allude to whether mitochondrial DNA alterations have detrimental consequences with regard to CMC structure and function. If the investigational approaches employed in this study hint toward a positive correlation, future study of the hydroxymethylome in a larger cohort of HCM patients will be warranted.
Secondly, as cadaver and patient records will provide information regarding other comorbidities (eg, diabetes, metabolic syndrome, and dyslipidemia), the underlying effect of these conditions on the severity of HCM may be elucidated, which, like above, will require confirmation in a larger cohort of patients with HCM. This study will also pave the way to design the strategy of integrating genomics education into anatomy teaching, as well as KT through different frameworks at different levels and competence of medical training. The success of this integration may be evaluated via different models of feedback, such as that of Pendleton [46], and structured questionnaires.
Abbreviations
- 5-hmC
5-hydroxymethylation of cytosine
- ALV
anterior left ventricle
- ARV
anterior right ventricle
- BGI
Beijing Genomics Institute
- cDNA
complementary DNA
- CMC
cardiomyocyte
- CVD
cardiovascular disease
- DhMR
differentially hydroxymethylated region
- HCM
hypertrophic cardiomyopathy
- IRB
Institutional Review Board
- KT
knowledge translation
- LLV
lateral left ventricle
- LRV
lateral right ventricle
- LV
left ventricle
- MBRU
Mohammed Bin Rashid University of Medicine and Health Sciences
- MYH7
myosin heavy chain beta isoform
- NUMT
nuclear copy of mitochondrial DNA
- PCR
polymerase chain reaction
- PLV
posterior left ventricle
- PRV
posterior right ventricle
- qPCR
quantitative polymerase chain reaction
- RIME
Reporter, Interpreter, Manager, Educator
- RV
right ventricle
- SNP
single-nucleotide polymorphism
- UAE
United Arab Emirates
Appendix
Peer-reviewer report from MBRU College of Medicine.
Footnotes
Conflicts of Interest: None declared.
References
- 1.Mokdad AH, Forouzanfar MH, Daoud F, El Bcheraoui C, Moradi-Lakeh M, Khalil I, Afshin A, Tuffaha M, Charara R, Barber RM, Wagner J, Cercy K, Kravitz H, Coates MM, Robinson M, Estep K, Steiner C, Jaber S, Mokdad AA, O'Rourke KF, Chew A, Kim P, El Razek MM, Abdalla Sa, Abd-Allah F, Abraham JP, Abu-Raddad LJ, Abu-Rmeileh NM, Al-Nehmi AA, Akanda AS, Al Ahmadi H, Al Khabouri MJ, Al Lami FH, Al Rayess ZA, Alasfoor D, AlBuhairan FS, Aldhahri SF, Alghnam S, Alhabib S, Al-Hamad N, Ali R, Ali SD, Alkhateeb M, AlMazroa MA, Alomari MA, Al-Raddadi R, Alsharif U, Al-Sheyab N, Alsowaidi S, Al-Thani M, Altirkawi KA, Amare AT, Amini H, Ammar W, Anwari P, Asayesh H, Asghar R, Assabri AM, Assadi R, Bacha U, Badawi A, Bakfalouni T, Basulaiman MO, Bazargan-Hejazi S, Bedi N, Bhakta AR, Bhutta ZA, Bin Abdulhak AA, Boufous S, Bourne RR, Danawi H, Das J, Deribew A, Ding EL, Durrani AM, Elshrek Y, Ibrahim ME, Eshrati B, Esteghamati A, Faghmous IA, Farzadfar F, Feigl AB, Fereshtehnejad SM, Filip I, Fischer F, Gankpé FG, Ginawi I, Gishu MD, Gupta R, Habash RM, Hafezi-Nejad N, Hamadeh RR, Hamdouni H, Hamidi S, Harb HL, Hassanvand MS, Hedayati MT, Heydarpour P, Hsairi M, Husseini A, Jahanmehr N, Jha V, Jonas JB, Karam NE, Kasaeian A, Kassa NA, Kaul A, Khader Y, Khalifa SE, Khan EA, Khan G, Khoja T, Khosravi A, Kinfu Y, Defo BK, Balaji AL, Lunevicius R, Obermeyer CM, Malekzadeh R, Mansourian M, Marcenes W, Farid HM, Mehari A, Mehio-Sibai A, Memish ZA, Mensah GA, Mohammad KA, Nahas Z, Nasher JT, Nawaz H, Nejjari C, Nisar MI, Omer SB, Parsaeian M, Peprah EK, Pervaiz A, Pourmalek F, Qato DM, Qorbani M, Radfar A, Rafay A, Rahimi K, Rahimi-Movaghar V, Rahman SU, Rai RK, Rana SM, Rao SR, Refaat AH, Resnikoff S, Roshandel G, Saade G, Saeedi MY, Sahraian MA, Saleh S, Sanchez-Riera L, Satpathy M, Sepanlou SG, Setegn T, Shaheen A, Shahraz S, Sheikhbahaei S, Shishani K, Sliwa K, Tavakkoli M, Terkawi AS, Uthman OA, Westerman R, Younis MZ, El Sayed Zaki M, Zannad F, Roth GA, Wang H, Naghavi M, Vos T, Al Rabeeah AA, Lopez AD, Murray CJ. Health in times of uncertainty in the eastern Mediterranean region, 1990-2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet Glob Health. 2016 Oct;4(10):e704–e713. doi: 10.1016/S2214-109X(16)30168-1. https://linkinghub.elsevier.com/retrieve/pii/S2214-109X(16)30168-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mokdad AH, Jaber S, Aziz MI, AlBuhairan F, AlGhaithi A, AlHamad NM, Al-Hooti SN, Al-Jasari A, AlMazroa MA, AlQasmi AM, Alsowaidi S, Asad M, Atkinson C, Badawi A, Bakfalouni T, Barkia A, Biryukov S, El Bcheraoui C, Daoud F, Forouzanfar MH, Gonzalez-Medina D, Hamadeh RR, Hsairi M, Hussein SS, Karam N, Khalifa SE, Khoja TA, Lami F, Leach-Kemon K, Memish ZA, Mokdad AA, Naghavi M, Nasher J, Qasem MB, Shuaib M, Al Thani AA, Al Thani MH, Zamakhshary M, Lopez AD, Murray CJ. The state of health in the Arab world, 1990-2010: An analysis of the burden of diseases, injuries, and risk factors. Lancet. 2014 Jan 25;383(9914):309–320. doi: 10.1016/S0140-6736(13)62189-3. [DOI] [PubMed] [Google Scholar]
- 3.Al-Ashwal A, Alnouri F, Sabbour H, Al-Mahfouz A, Al-Sayed N, Razzaghy-Azar M, Al-Allaf F, Al-Waili K, Banerjee Y, Genest J, Santos R, Al-Rasadi K. Identification and treatment of patients with homozygous familial hypercholesterolaemia: Information and recommendations from a Middle East advisory panel. Curr Vasc Pharmacol. 2015;13(6):759–770. doi: 10.2174/1570161113666150827125040. http://europepmc.org/abstract/MED/26311574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Blair I, Sharif AA. Population structure and the burden of disease in the United Arab Emirates. J Epidemiol Glob Health. 2012 Jun;2(2):61–71. doi: 10.1016/j.jegh.2012.04.002. https://linkinghub.elsevier.com/retrieve/pii/S2210-6006(12)00021-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Al Nowais S. The National. 2018. Mar 11, [2019-09-07]. UAE National Service recruits screened for heart conditions in drive to save lives https://www.thenational.ae/uae/uae-national-service-recruits-screened-for-heart-conditions-in-drive-to-save-lives-1.712202.
- 6.Clarke A, Harper P. Genetic testing for hypertrophic cardiomyopathy. N Engl J Med. 1992 Oct 15;327(16):1175–1176. doi: 10.1056/NEJM199210153271616. [DOI] [PubMed] [Google Scholar]
- 7.Watkins H, Rosenzweig A, Hwang D, Levi T, McKenna W, Seidman CE, Seidman J. Characteristics and prognostic implications of myosin missense mutations in familial hypertrophic cardiomyopathy. N Engl J Med. 1992 Apr 23;326(17):1108–1114. doi: 10.1056/NEJM199204233261703. [DOI] [PubMed] [Google Scholar]
- 8.Maron BJ, Maron MS, Semsarian C. Genetics of hypertrophic cardiomyopathy after 20 years: Clinical perspectives. J Am Coll Cardiol. 2012 Aug 21;60(8):705–715. doi: 10.1016/j.jacc.2012.02.068. https://linkinghub.elsevier.com/retrieve/pii/S0735-1097(12)01586-0. [DOI] [PubMed] [Google Scholar]
- 9.Friedrichs F, Zugck C, Rauch G, Ivandic B, Weichenhan D, Müller-Bardorff M, Meder B, El Mokhtari NE, Regitz-Zagrosek V, Hetzer R, Schäfer A, Schreiber S, Chen J, Neuhaus I, Ji R, Siemers NO, Frey N, Rottbauer W, Katus HA, Stoll M. HBEGF, SRA1, and IK: Three cosegregating genes as determinants of cardiomyopathy. Genome Res. 2009 Mar;19(3):395–403. doi: 10.1101/gr.076653.108. http://genome.cshlp.org/cgi/pmidlookup?view=long&pmid=19064678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Frey N, Luedde M, Katus HA. Mechanisms of disease: Hypertrophic cardiomyopathy. Nat Rev Cardiol. 2011 Oct 25;9(2):91–100. doi: 10.1038/nrcardio.2011.159. [DOI] [PubMed] [Google Scholar]
- 11.Montgomery RL, Davis CA, Potthoff MJ, Haberland M, Fielitz J, Qi X, Hill JA, Richardson JA, Olson EN. Histone deacetylases 1 and 2 redundantly regulate cardiac morphogenesis, growth, and contractility. Genes Dev. 2007 Jul 15;21(14):1790–1802. doi: 10.1101/gad.1563807. http://www.genesdev.org/cgi/pmidlookup?view=long&pmid=17639084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Meurs KM, Kuan M. Differential methylation of CpG sites in two isoforms of myosin binding protein C, an important hypertrophic cardiomyopathy gene. Environ Mol Mutagen. 2011 Mar;52(2):161–164. doi: 10.1002/em.20596. [DOI] [PubMed] [Google Scholar]
- 13.Jirtle RL, Skinner MK. Environmental epigenomics and disease susceptibility. Nat Rev Genet. 2007 Apr;8(4):253–262. doi: 10.1038/nrg2045. http://europepmc.org/abstract/MED/17363974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Herceg Z, Vaissière T. Epigenetic mechanisms and cancer: An interface between the environment and the genome. Epigenetics. 2011 Jul;6(7):804–819. doi: 10.4161/epi.6.7.16262. [DOI] [PubMed] [Google Scholar]
- 15.Greco CM, Kunderfranco P, Rubino M, Larcher V, Carullo P, Anselmo A, Kurz K, Carell T, Angius A, Latronico MV, Papait R, Condorelli G. DNA hydroxymethylation controls cardiomyocyte gene expression in development and hypertrophy. Nat Commun. 2016 Aug 04;7:12418. doi: 10.1038/ncomms12418. http://europepmc.org/abstract/MED/27489048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Papait R, Cattaneo P, Kunderfranco P, Greco C, Carullo P, Guffanti A, Viganò V, Stirparo GG, Latronico MV, Hasenfuss G, Chen J, Condorelli G. Genome-wide analysis of histone marks identifying an epigenetic signature of promoters and enhancers underlying cardiac hypertrophy. Proc Natl Acad Sci U S A. 2013 Dec 10;110(50):20164–20169. doi: 10.1073/pnas.1315155110. http://www.pnas.org/cgi/pmidlookup?view=long&pmid=24284169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Papait R, Serio S, Pagiatakis C, Rusconi F, Carullo P, Mazzola M, Salvarani N, Miragoli M, Condorelli G. Histone methyltransferase G9a is required for cardiomyocyte homeostasis and hypertrophy. Circulation. 2017 Sep 26;136(13):1233–1246. doi: 10.1161/CIRCULATIONAHA.117.028561. [DOI] [PubMed] [Google Scholar]
- 18.Gilsbach R, Preissl S, Grüning BA, Schnick T, Burger L, Benes V, Würch A, Bönisch U, Günther S, Backofen R, Fleischmann BK, Schübeler D, Hein L. Dynamic DNA methylation orchestrates cardiomyocyte development, maturation and disease. Nat Commun. 2014 Oct 22;5:5288. doi: 10.1038/ncomms6288. http://europepmc.org/abstract/MED/25335909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Gilsbach R, Schwaderer M, Preissl S, Grüning BA, Kranzhöfer D, Schneider P, Nührenberg TG, Mulero-Navarro S, Weichenhan D, Braun C, Dreßen M, Jacobs AR, Lahm H, Doenst T, Backofen R, Krane M, Gelb BD, Hein L. Distinct epigenetic programs regulate cardiac myocyte development and disease in the human heart in vivo. Nat Commun. 2018 Jan 26;9(1):391. doi: 10.1038/s41467-017-02762-z. http://europepmc.org/abstract/MED/29374152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Preissl S, Schwaderer M, Raulf A, Hesse M, Grüning BA, Köbele C, Backofen R, Fleischmann BK, Hein L, Gilsbach R. Deciphering the epigenetic code of cardiac myocyte transcription. Circ Res. 2015 Aug 14;117(5):413–423. doi: 10.1161/CIRCRESAHA.115.306337. [DOI] [PubMed] [Google Scholar]
- 21.Gielda L, Rigg S. Extraction of amplifiable DNA from embalmed human cadaver tissue. BMC Res Notes. 2017 Dec 13;10(1):737. doi: 10.1186/s13104-017-3066-y. https://bmcresnotes.biomedcentral.com/articles/10.1186/s13104-017-3066-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Choi Y, Lee JH, Cui MN, Lee YS, Jung MH, Yi JE, Jung HO, Youn HJ. Hypertrophic cardiomyopathy attributable to mitochondrial DNA mutation diagnosed by pathology and gene sequencing. Circulation. 2016 Mar 29;133(13):1297–1299. doi: 10.1161/CIRCULATIONAHA.115.020463. [DOI] [PubMed] [Google Scholar]
- 23.Straus SE, Tetroe JM, Graham ID. Knowledge translation is the use of knowledge in health care decision making. J Clin Epidemiol. 2011 Jan;64(1):6–10. doi: 10.1016/j.jclinepi.2009.08.016. [DOI] [PubMed] [Google Scholar]
- 24.Tambi R, Bayoumi R, Lansberg P, Banerjee Y. Blending Gagne's instructional model with Peyton's approach to design an introductory bioinformatics lesson plan for medical students: Proof-of-concept study. JMIR Med Educ. 2018 Oct 25;4(2):e11122. doi: 10.2196/11122. https://mededu.jmir.org/2018/2/e11122/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Coleman R, Kogan I. An improved low-formaldehyde embalming fluid to preserve cadavers for anatomy teaching. J Anat. 1998 Apr;192 ( Pt 3):443–446. doi: 10.1046/j.1469-7580.1998.19230443.x. https://onlinelibrary.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=0021-8782&date=1998&volume=192&issue=&spage=443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Authors/Task Force Members. Elliott PM, Anastasakis A, Borger MA, Borggrefe M, Cecchi F, Charron P, Hagege AA, Lafont A, Limongelli G, Mahrholdt H, McKenna WJ, Mogensen J, Nihoyannopoulos P, Nistri S, Pieper PG, Pieske B, Rapezzi C, Rutten FH, Tillmanns C, Watkins H. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC) Eur Heart J. 2014 Oct 14;35(39):2733–2779. doi: 10.1093/eurheartj/ehu284. [DOI] [PubMed] [Google Scholar]
- 27.Haas J, Frese KS, Park YJ, Keller A, Vogel B, Lindroth AM, Weichenhan D, Franke J, Fischer S, Bauer A, Marquart S, Sedaghat-Hamedani F, Kayvanpour E, Köhler D, Wolf NM, Hassel S, Nietsch R, Wieland T, Ehlermann P, Schultz J, Dösch A, Mereles D, Hardt S, Backs J, Hoheisel JD, Plass C, Katus HA, Meder B. Alterations in cardiac DNA methylation in human dilated cardiomyopathy. EMBO Mol Med. 2013 Mar;5(3):413–429. doi: 10.1002/emmm.201201553. doi: 10.1002/emmm.201201553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rusk N. Profiling the sixth base. Nat Methods. 2011 Jul;8(7):532–533. doi: 10.1038/nmeth0711-532b. [DOI] [PubMed] [Google Scholar]
- 29.Song CX, Szulwach KE, Fu Y, Dai Q, Yi C, Li X, Li Y, Chen CH, Zhang W, Jian X, Wang J, Zhang L, Looney TJ, Zhang B, Godley LA, Hicks LM, Lahn BT, Jin P, He C. Selective chemical labeling reveals the genome-wide distribution of 5-hydroxymethylcytosine. Nat Biotechnol. 2011 Jan;29(1):68–72. doi: 10.1038/nbt.1732. http://europepmc.org/abstract/MED/21151123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hahn M, Qiu R, Wu X, Li A, Zhang H, Wang J, Jui J, Jin S, Jiang Y, Pfeifer G, Lu Q. Dynamics of 5-hydroxymethylcytosine and chromatin marks in mammalian neurogenesis. Cell Rep. 2013 Feb 21;3(2):291–300. doi: 10.1016/j.celrep.2013.01.011. https://linkinghub.elsevier.com/retrieve/pii/S2211-1247(13)00018-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ivanov M, Kals M, Kacevska M, Barragan I, Kasuga K, Rane A, Metspalu A, Milani L, Ingelman-Sundberg M. Ontogeny, distribution and potential roles of 5-hydroxymethylcytosine in human liver function. Genome Biol. 2013 Aug 19;14(8):R83. doi: 10.1186/gb-2013-14-8-r83. https://genomebiology.biomedcentral.com/articles/10.1186/gb-2013-14-8-r83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.BGI. [2020-01-04]. Whole genome bisulfite sequencing https://www.bgi.com/us/sequencing-services/epigenetics/whole-genome-bisulfite-sequencing/
- 33.Bolger AM, Lohse M, Usadel B. Trimmomatic: A flexible trimmer for Illumina sequence data. Bioinformatics. 2014 Aug 01;30(15):2114–2120. doi: 10.1093/bioinformatics/btu170. http://europepmc.org/abstract/MED/24695404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Langmead B, Trapnell C, Pop M, Salzberg SL. Ultrafast and memory-efficient alignment of short DNA sequences to the human genome. Genome Biol. 2009;10(3):R25. doi: 10.1186/gb-2009-10-3-r25. https://genomebiology.biomedcentral.com/articles/10.1186/gb-2009-10-3-r25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Robinson JT, Thorvaldsdóttir H, Winckler W, Guttman M, Lander ES, Getz G, Mesirov JP. Integrative genomics viewer. Nat Biotechnol. 2011 Jan;29(1):24–26. doi: 10.1038/nbt.1754. http://europepmc.org/abstract/MED/21221095. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Shen L, Shao NY, Liu X, Maze I, Feng J, Nestler EJ. diffReps: Detecting differential chromatin modification sites from ChIP-seq data with biological replicates. PLoS One. 2013;8(6):e65598. doi: 10.1371/journal.pone.0065598. http://dx.plos.org/10.1371/journal.pone.0065598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Quispe-Tintaya W, White RR, Popov VN, Vijg J, Maslov AY. Fast mitochondrial DNA isolation from mammalian cells for next-generation sequencing. Biotechniques. 2013 Sep;55(3):133–136. doi: 10.2144/000114077. http://europepmc.org/abstract/MED/24003945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Tang M, Tan M, Meng G, Yang S, Su X, Liu S, Song W, Li Y, Wu Q, Zhang A, Zhou X. Multiplex sequencing of pooled mitochondrial genomes: A crucial step toward biodiversity analysis using mito-metagenomics. Nucleic Acids Res. 2014 Dec 16;42(22):e166. doi: 10.1093/nar/gku917. http://europepmc.org/abstract/MED/25294837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Al-Rasadi K, Al-Waili K, Al-Zidi WA, Al-Abri AR, Al-Hinai AT, Al-Sabti HA, Al-Tobi S, Al-Zakwani I, Al-Zadjali F, Al-Hashmi K, Banerjee Y. Low-density lipoprotein receptor gene mutation analysis and structure-function correlation in an Omani Arab family with familial hypercholesterolemia. Angiology. 2014 Nov;65(10):911–918. doi: 10.1177/0003319713510059. [DOI] [PubMed] [Google Scholar]
- 40.Bamimore MA, Zaid A, Banerjee Y, Al-Sarraf A, Abifadel M, Seidah NG, Al-Waili K, Al-Rasadi K, Awan Z. Familial hypercholesterolemia mutations in the Middle Eastern and North African region: A need for a national registry. J Clin Lipidol. 2015;9(2):187–194. doi: 10.1016/j.jacl.2014.11.008. [DOI] [PubMed] [Google Scholar]
- 41.Lansberg PJ, Banerjee Y. A highly durable RNAi therapeutic inhibitor of PCSK9. N Engl J Med. 2017 May 04;376(18):e38. doi: 10.1056/NEJMc1703361. [DOI] [PubMed] [Google Scholar]
- 42.Meyer EG, Kelly WF, Hemmer PA, Pangaro LN. The RIME model provides a context for entrustable professional activities across undergraduate medical education. Acad Med. 2018 Jun;93(6):954. doi: 10.1097/ACM.0000000000002211. [DOI] [PubMed] [Google Scholar]
- 43.Banerjee Yajnavalka, Tuffnell Christopher, Alkhadragy Rania. Mento's change model in teaching competency-based medical education. BMC Med Educ. 2019 Dec 27;19(1):472. doi: 10.1186/s12909-019-1896-0. https://bmcmededuc.biomedcentral.com/articles/10.1186/s12909-019-1896-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Wallace S, May SA. Assessing and enhancing quality through outcomes-based continuing professional development (CPD): A review of current practice. Vet Rec. 2016 Nov 19;179(20):515–520. doi: 10.1136/vr.103862. http://europepmc.org/abstract/MED/27856985. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.BGI. [2020-02-17]. https://www.bgi.com/global/
- 46.Burgess A, Mellis C. Feedback and assessment for clinical placements: Achieving the right balance. Adv Med Educ Pract. 2015;6:373–381. doi: 10.2147/AMEP.S77890. doi: 10.2147/AMEP.S77890. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Peer-reviewer report from MBRU College of Medicine.