

Abstract
OBJECTIVES:
To examine the association between potential inappropriate prescribing practices of opioids and deaths among opioid users in the Georgia Medicaid population.
STUDY DESIGN:
A retrospective analysis of individual pharmacy claims data from Georgia Medicaid from 2009 through 2014.
METHODS:
The sample was restricted to patients without cancer aged 18 to 64 years with an opioid prescription and included 3,562,227 observations representing 401,488 individuals. A descriptive analysis and a multivariate logistic regression analysis were conducted.
RESULTS:
Results indicate a total of 14,516 deaths among opioid users in the study sample, of whom approximately 42% experienced at least 1 incidence of potential inappropriate prescribing practices. Regression results indicate that the odds of opioid users experiencing death were 1.76 times higher for those who experienced at least 1 incidence of potential inappropriate prescribing practices of opioids compared with those who did not experience any incidence, even after controlling for other covariates (P <.001). Moreover, opioid users in managed care Medicaid were less likely to experience death compared with fee-for-service (FFS) enrollees.
CONCLUSIONS:
The results indicate a positive and statistically significant association between potential inappropriate opioid prescribing practices and deaths among opioid users in Georgia Medicaid, with FFS enrollees experiencing higher rates of death compared with managed care enrollees. Appropriate policies and interventions targeted at reducing potential inappropriate prescribing practices may help reduce the risk factors associated with mortality among opioid users in this population.
Deaths related to opioid overdose continue to rise at an alarming rate in the United States. Drug overdose mortality is now the leading cause of death for Americans younger than 50 years and has been largely attributed to deaths associated with prescription opioids.1 The Medicaid population in particular has been significantly affected by the opioid crisis, experiencing high rates of opioid prescribing, opioid-related overdose deaths, and opioid use disorder (OUD).1–3 Prior studies have examined opioid prescribing among Medicaid enrollees2,4–9 and the relationship between opioid prescribing and mortality in this population.3,10–17
Several studies have identified risk factors associated with risk of opioid overdose and mortality, including some indicators of potential inappropriate use and prescription of opioids.3,11,14–16 One such study, by Ray et al,14 used data from the Tennessee Medicaid program (1999-2012) to examine the risk of mortality associated with prescription of long-acting opioid therapy compared with a set of control medications. Results showed that the risk of all-cause mortality was greater for patients receiving prescriptions for long-acting opioids for chronic noncancer conditions compared with patients in the control medication group.14
In a study by Yang et al,11 multistate Medicaid claims data were used to examine the relationships between pharmacy shopping and overlapping prescriptions of opioids and opioid-related overdose events using data from 2008 to 2010. This study defined overlapping prescriptions of opioids as 2 prescriptions for the same opioid drug type that overlapped by at least 25% of the days prescribed, with the initial dispensed prescription having at least 5 days of supply. Results indicated that the adjusted risks of an overdose event were higher for patients with overlapping opioid prescriptions and for patients engaging in pharmacy shopping.11
Another study, by Cochran et al, examined the association between nonmedical use of prescription opioids and opioid medication overdose using data from the Pennsylvania Medicaid program (2007-2012).16 Opioid overdose was higher among patients with opioid abuse, probable misuse, and possible misuse compared with patients with no misuse. The study used a 3-category measure of misuse based on the number of opioid prescribers, number of pharmacies used for medication filling, days’ supply of short-acting opioids, and days’ supply of long-acting opioids over a 6-month period (no misuse, 0-1; possible misuse, 2-4; and probable misuse, ≥5). The results indicated that doses of 100 morphine milligram equivalents (MME) per day or greater were associated with a higher rate of overdose compared with doses below 20 MME per day. Further, any use of benzodiazepines or muscle relaxants was associated with overdose.16
Two additional studies3,15 found support for the relationship between potential inappropriate use or prescription of opioids and prescription opioid overdose mortality. Using data from the Colorado Medicaid program (2009-2014), Dilokthornsakul and colleagues found in 2016 that mean morphine equivalent dose of more than 50 mg per day, methadone use, benzodiazepine use, and number of pharmacies used by the beneficiary (≥4 vs 1) were associated with an increased risk of prescription opioid overdose.15 In 2017, Garg and colleagues3 found that risk of opioid overdose death increased at doses of 50 mg to 89 mg, 120 mg to 199 mg, and 200 mg or greater compared with 1 mg to 19 mg per day among Medicaid patients in the state of Washington. Risk of opioid overdose death was also greater for patients using both long-acting and short-acting Schedule II opioids compared with non–Schedule II opioids alone. Finally, patients receiving overlapping prescriptions of opioids and benzodiazepines, or opioids and skeletal muscle relaxants, had a higher risk of opioid overdose.3
To date, studies investigating mortality associated with opioid prescribing have focused primarily on identifying risk factors associated with opioid overdose mortality. However, most of these studies rely on older data that predate the sharp increase in prescription opioid mortality. Further, there is some question as to how accurately death due to opioid overdose is captured in death certificates.18 In addition, to our knowledge, no single study has examined a comprehensive set of indicators of inappropriate opioid prescribing and how these indicators are related to mortality. Finally, most prior studies examined the Medicaid fee-for-service (FFS) population. However, a majority of Medicaid patients are enrolled in managed care plans; therefore, the results of these studies may not extend to Medicaid managed care. To better understand how potential inappropriate prescribing of opioids is associated with all-cause mortality in the Medicaid population, we used the Georgia Medicaid pharmacy claims database (2009-2014) to examine the impact of 5 indicators of potential inappropriate opioid prescribing practices on all-cause mortality among patients in both FFS and managed care plans.
METHODS
Data
Individual pharmacy claims data from the Georgia Medicaid pharmacy claims database from 2009 to 2014 were used in the study. If any individual in the study sample during the 2009 to 2014 period died in 2015, that information was included in the data sample. Following extant research, individuals with cancer diagnoses were identified using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes (including 140-172.9, 174-215.9, 217-229.10, 235-239.9, and 338.3) and were excluded from the study sample.2,19,20 The study sample was restricted to individuals who received an opioid prescription (short-acting or long-acting extended-release [LA/ER] opioids) and were aged 18 to 64 years during the study period.
The final study sample included 3,562,227 patient-prescription observations representing 401,488 individuals over the study period. It should be noted that about 8.6% of the sample did not include race/ethnicity information for the study period, although other demographic characteristics, such as age, gender, and insurance type, were included. Therefore, a missing-race category was created to include the individuals with missing race/ethnicity information in the analysis.9
Measures
The key dependent variable of interest was individual deaths among opioid users in the study sample, which was coded as a dichotomous measure (1/0). The key independent variable of interest was whether an individual experienced any incidences of potential inappropriate prescribing practices, which was also coded as a dichotomous measure (1/0). The indicators of potential inappropriate prescribing practices by providers were adapted following previous expert panels and clinical guidelines, and they were measured using the following 5 indicators: (1) overlapping opioid prescriptions, defined as opioid prescriptions that overlap by 7 days or more; (2) overlapping opioid and benzodiazepine prescriptions, defined as opioid and benzodiazepine prescriptions that overlap by 7 days or more; (3) overlapping opioid and buprenorphine-naloxone (BUP-NX; Suboxone) prescriptions, defined as opioid and BUP-NX prescriptions that overlap by 1 day or more; (4) LA/ER opioid prescriptions for acute pain; and (5) high daily doses of opioid prescriptions, defined as receiving more than 100 MME.21–25 The other confounding variables in the analysis included sociodemographic variables of age (continuous), gender (female, male [reference]), race/ethnicity (Hispanic, non-Hispanic black, non-Hispanic other, missing race, non-Hispanic white [reference]), and type of insurance (managed care, FFS [reference]). Because the severity of an individual’s health conditions (comorbidities) could have an impact on their death, we controlled for the severity of their comorbidities using Charlson Comorbidity Index (CCI) scores.26 CCI scores were calculated using ICD-9-CM diagnosis codes in the data. Additional confounding variables, such as number of prescriptions received (opioids, LA/ER opioids, benzodiazepines, and BUP-NX) and whether an individual experienced a diagnosis of acute pain, chronic pain, or OUD, were included in the analysis.
Statistical Analysis
Descriptive statistics of the sample were calculated for all study variables by whether an individual experienced any incidences of potentially inappropriate prescribing practices during the study period. Significance tests were conducted using the t test to examine statistical significance for continuous variables and the χ2 test for categorical variables. To show the variation in number of deaths among opioid users in the sample, the number of deaths was graphed by demographic characteristics age, gender, race/ethnicity, and type of insurance over time. A multivariate logistic regression model was used to examine the association between incidences of potentially inappropriate prescribing practices and deaths among the Medicaid population receiving opioid prescriptions. All statistical analyses were conducted in Stata version 14.2 (StataCorp LP; College Station, Texas).
RESULTS
Results indicate a total of 14,516 all-cause deaths among opioid users in the study sample. About 42% of these deaths were among opioid users who experienced at least 1 incidence of potential inappropriate prescribing practices of opioids. Descriptive statistics of the study sample are presented in Table 1 by whether an individual experienced any incidences of potential inappropriate prescribing practices of opioids. Individuals who experienced any incidences of potential inappropriate opioid prescriptions were more likely to be male, older, non-Hispanic white, and FFS enrollees. They also had higher average CCI scores (2.36), indicating higher severity of health conditions, compared with individuals who did not experience any incidences of potential inappropriate prescriptions (0.96). Individuals who experienced any incidences of potential inappropriate opioid prescriptions received higher numbers of prescriptions of opioids, LA/ER opioids, benzodiazepines, and BUP-NX compared with individuals who did not experience any incidences. Higher proportions of individuals with potential inappropriate opioid prescriptions were diagnosed with chronic pain, acute pain, and OUD. Additionally, a higher proportion of these individuals experienced death (8.65%) compared with those who did not experience any incidences of inappropriate opioid prescriptions (2.56%).
TABLE 1.
Characteristics of the Study Sample by Whether Individuals Experienced Any Incidences of Potential Inappropriate Opioid Prescribing (N = 401,488)
| Variable | Any Inappropriate Incidences | No Inappropriate Incidences | P |
|---|---|---|---|
| Observations (n) | 69,668 | 331,820 | |
| Died (1/0), % | 8.65 | 2.56 | <.001 |
| Female, % | 72.43 | 80.71 | <.001 |
| Managed care Medicaid, % | 45.43 | 69.02 | <.001 |
| Age in years, % | |||
| 18-34 | 30.66 | 66.37 | <.001 |
| 35-44 | 23.26 | 15.86 | <.001 |
| 45-54 | 24.32 | 9.45 | <.001 |
| 55-64 | 21.77 | 8.31 | <.001 |
| Age in years, mean (SD) | 42.39 (12.31) | 32.20 (12.17) | <.001 |
| Race/ethnicity, % | |||
| Hispanic | 0.43 | 0.48 | .11 |
| Non-Hispanic white | 57.71 | 39.52 | <.001 |
| Non-Hispanic black | 28.37 | 50.92 | <.001 |
| Non-Hispanic other | 0.70 | 1.42 | <.001 |
| Missing race | 12.79 | 7.67 | <.001 |
| CCI score, mean (SD) | 2.36 (2.75) | 0.96 (1.92) | <.001 |
| Diagnoses,a % | |||
| Chronic pain (1/0) | 90.06 | 42.88 | <.001 |
| Acute pain (1/0) | 68.22 | 34.91 | <.001 |
| OUD (1/0) | 9.11 | 0.73 | <.001 |
| Number of prescriptions, mean (SD) | |||
| Opioids | 17.77 (18.15) | 3.42 (4.66) | <.001 |
| LA/ER opioids | 1.66 (6.93) | 0.01 (0.27) | <.001 |
| Benzodiazepines | 12.85 (17.42) | 0.51 (2.44) | <.001 |
| BUP/NX | 0.10 (1.22) | 0.01 (0.22) | <.001 |
BUP/NX indicates buprenorphine-naloxone (Suboxone); CCI, Charlson Comorbidity Index; LA/ER, long-acting/extended-release; OUD, opioid use disorder.
Diagnoses were identified using International Classification of Diseases, Ninth Revision, Clinical Modification codes as appropriate.
The number of deaths among individuals who experienced any incidences of potential inappropriate opioid prescriptions increased over time (2009-2014), with a slight drop in 2015 (Figure 1). Although the number of deaths was higher among women than men, the rate of death was higher among men (Figure 2). In addition, the rate of death was higher among FFS enrollees compared with managed care enrollees (Figure 3). Moreover, the rate of death was higher among older individuals (aged 55-64 years) compared with other age groups (eAppendix Figure 1 [eAppendix available at ajmc.com]). However, the rate of death was not higher among a specific race/ethnic group throughout all years (eAppendix Figure 2).
FIGURE 1.
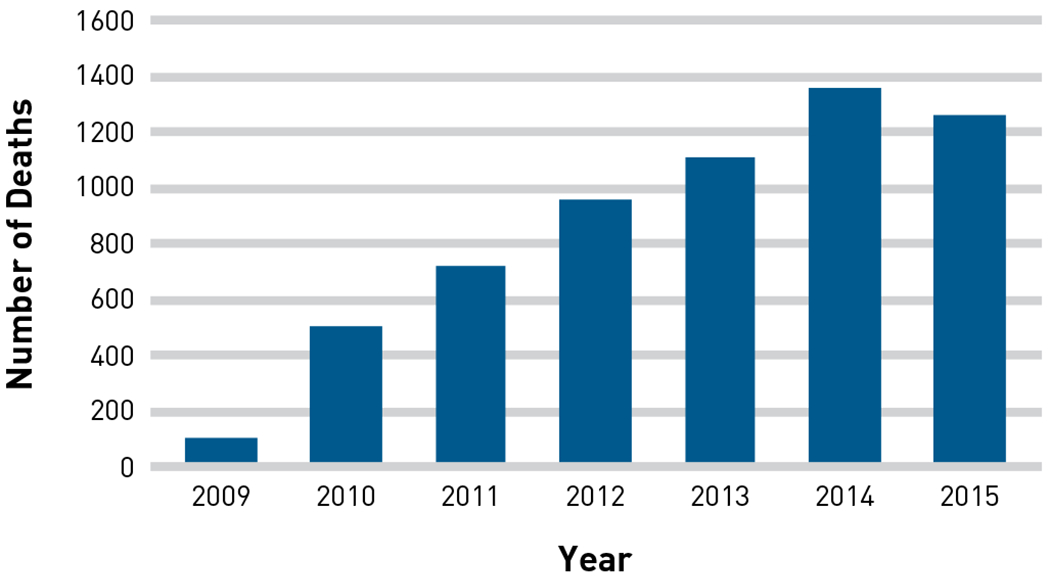
Number of Deaths When 1 or More Incidences of Potential Inappropriate Prescribing of Opioids Occurred
FIGURE 2.

Number and Rate of Deaths by Gender When 1 or More Incidences of Potential Inappropriate Prescribing of Opioids Occurred
FIGURE 3.
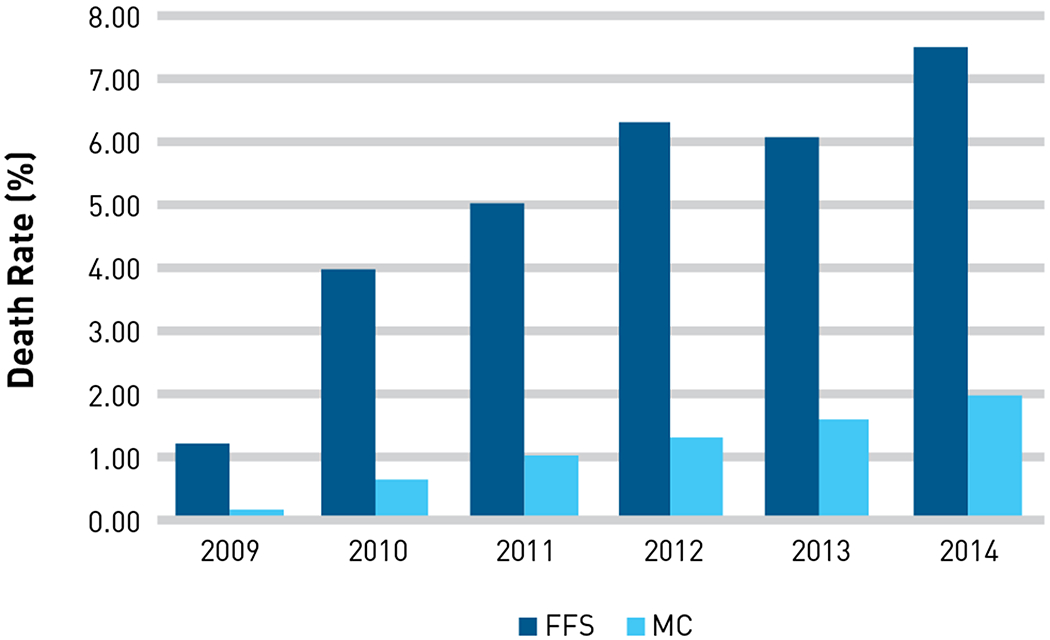
Rate of Deaths by Type of Medicaid Insurance When 1 or More Incidences of Potential Inappropriate Prescribing of Opioids Occurred
FFS indicates fee-for-service; MC, managed care.
Table 2 presents the results from the multivariate logistic regression analysis. The odds of opioid users experiencing death were 1.76 times higher for those who experienced 1 or more incidences of inappropriate opioid prescribing practices compared with those who did not have this experience during the study period (P <.001). In addition, the odds of experiencing death were higher among opioid users who were older, were diagnosed with acute pain or OUD, and had a higher severity of health conditions; meanwhile, the odds were lower among opioid users who were female and managed care enrollees. Moreover, the odds of experiencing death were lower among opioid users who belonged to all other races (Hispanic, non-Hispanic black, non-Hispanic other, missing race) compared with non-Hispanic white opioid users.
TABLE 2.
Multivariate Logistic Regression Results (N = 401,488]
| Died (1/0) | Odds Ratio | SE | z Score | P >|z| |
|---|---|---|---|---|
| Experienced incidences (1/0) | 1.76 | 0.04 | 23.11 | <.001 |
| Age | 1.04 | 0.00 | 42.31 | <.001 |
| Female | 0.63 | 0.01 | −23.84 | <.001 |
| Hispanic | 0.51 | 0.06 | −5.46 | <.001 |
| Non-Hispanic black | 0.60 | 0.01 | −23.99 | <.001 |
| Non-Hispanic other | 0.57 | 0.06 | −5.52 | <.001 |
| Missing race | 0.47 | 0.01 | −24.94 | <.001 |
| Managed care Medicaid | 0.31 | 0.01 | −39.42 | <.001 |
| CCI score | 1.31 | 0.00 | 93.94 | <.001 |
| Opioid prescriptions | 0.98 | 0.00 | −21.54 | <.001 |
| LA/ER opioid prescriptions | 1.00 | 0.00 | −1.47 | .14 |
| Benzodiazepine prescriptions | 1.00 | 0.00 | 1.55 | .12 |
| BUP/NX prescriptions | 0.98 | 0.02 | −1.24 | .22 |
| Chronic pain diagnosis (1/0) | 0.95 | 0.02 | −2.20 | .03 |
| Acute pain diagnosis (1/0) | 1.08 | 0.02 | 3.51 | <.001 |
| OUD diagnosis (1/0) | 1.30 | 0.06 | 5.38 | <.001 |
| Constant | 0.01 | 0.00 | −92.71 | <.001 |
BUP/NX indicates buprenorphine-naloxone (Suboxone); CCI, Charlson Comorbidity Index; LA/ER, long-acting/extended-release; OUD, opioid use disorder; SE, standard error.
DISCUSSION
The number of deaths caused by opioid overdoses is increasing in the United States,27 and prescribers, dispensers, and other stakeholders are aware of the wide range of implications associated with the use of these medications—from their impact on relief of pain to morbidity and mortality (usually caused by respiratory depression). Because patients with legitimate prescriptions for opioids are also at risk of opioid overdose and death,28 we sought to examine (1) if the appropriateness of the prescribing practices for opioids presents another risk factor for death from all causes within the population of opioid users and (2) differences between traditional FFS Medicaid and managed care Medicaid.
With more than 14,500 opioid deaths over the study period, we found that 42% of these deaths occurred in patients with 1 or more incidences of inappropriate prescribing. Using 5 established criteria for identifying potential inappropriate prescriptions for opioids, we identified an increasing trend in the death rate for patients who used opioids between 2009 and 2014, with male, white, and older patients dying at higher rates. In fact, patients had a 76% greater chance of dying during the study period if they had 1 or more incidences of inappropriate opioid prescriptions. Comparatively, severity of health conditions increased the odds of dying during the study period by 31%, whereas being in managed care Medicaid decreased the odds of death by 69%. Our results also showed that regarding insurance type, death rates among FFS Medicaid enrollees were significantly higher than among managed care enrollees who experienced at least 1 incidence of potential inappropriate prescribing of opioids.
Although these trends are generally consistent with those found in other descriptive studies that have identified risk factors for opioid overdose deaths,3,14,15 the finding that insurance type affects death rates was concerning. This is of interest because it is possible that structural differences in the payment system (FFS vs managed care) could be affecting opioid use. In particular, FFS may be imposing fiscal controls (eg, formulary status, limits on the numbers of prescriptions or quantity per prescription) at the point of payment to curb opioid use. In contrast, managed care plans may use these same methods but employ additional strategies for patient education and shared decision making.
In this study, FFS enrollees had a 27.00% rate of inappropriate incidences of opioid prescribing whereas managed care enrollees had a rate of 12.14%. The comparative effectiveness of FFS versus managed care strategies needs further evaluation to determine if safety measures, fiscal control, or clinical patient management are the source of differences between FFS and managed care. This question presents many opportunities for future research, including further policy analyses to determine if these trends also exist in private insurance plan populations. Using commercially available databases, such as IMS (now part of IQVIA) Health LifeLink, would be a reasonable approach. Better ways to link medical and pharmacy claims are also needed to be able to move from measuring all-cause death to measuring death from opioid causes. Although this variable is much harder to assess because of coding in the medical record, it is worth pursuing.
The finding that potential inappropriate prescribing increased the odds of death is significant in that it adds another risk factor to those previously identified. This means that policies aimed at controlling potential inappropriate medication use may be effective in reducing risk factors associated with opioid prescribing. This is certainly supported by the finding that patients in managed care Medicaid had a significantly lower chance of experiencing death in this population. These results provide impetus to more closely examine FFS versus managed care Medicaid, as we now have preliminary evidence that type of insurance plan is associated with health outcomes.
Although patient age and health status (comorbidities) are important determinants of their odds of death, we found violation of basic prescribing principles to be the most important predictor of death. Patients with 1 or more indicators of potential inappropriate prescribing of opioids died at a greater rate than those without these indicators when controlling for other factors. Further, participation in a managed care Medicaid insurance program also reduced the odds of death. This may also represent selection bias in type of insurance, as patients who do not make a plan selection at enrollment are assigned to FFS. It may represent a deeper problem with the provision of FFS Medicaid.
Limitations
There are several limitations in this study that should be considered when interpreting the results. First, it uses pharmacy claims data in the analysis, which show only filled prescriptions, not actual consumption. In addition, the data do not include information on nonprescription opioids, such as heroin and illicit fentanyl. Second, this study focuses only on the adult population (aged 18-64 years) in Georgia Medicaid during 2009 to 2014; thus, results may not be generalizable to other states, other populations, or other time periods. This time period was chosen for this study because it had the most recent data that were available to us. Third, similar to other studies, this study uses ICD-9-CM codes to identify diagnoses, which have their own limitations given that certain diagnoses, such as type of pain, may not be classified or reported accurately. Fourth, this study examines the association between potential inappropriate prescribing practices of opioids and deaths among opioid users. Therefore, additional analyses are needed to draw any causal effects of potential inappropriate prescribing of opioids on health outcomes, including death.
Like all cross-sectional studies, there is a serious risk of confounding from unobserved factors. We found major differences in observable traits between individuals with and without inappropriate prescriptions, which suggests that unobserved factors may also be important; interpretation of these results must be made with caution. That said, when we compare a more parsimonious model with the one reported (eAppendix Table 1), we find that the fuller model yields an even stronger association. Moreover, a longitudinal model with cluster-robust standard errors at the individual level reveals similar results to the fuller model in Table 2 (eAppendix Table 2).
CONCLUSIONS
The findings of this study indicate that incidences of potential inappropriate prescribing practices of opioids are significantly and positively associated with deaths among opioid users in the Georgia Medicaid population when controlling for other factors. In addition, results show that managed care Medicaid enrollees were less likely to experience death than FFS enrollees, indicating possible selection bias in the type of insurance among Medicaid enrollees, variations in prescribing and management practices within FFS and managed care plans, or a combination of both. The findings of this study are also consistent with previous findings in identifying usual risk factors, such as being male, white, and older, that are positively and significantly associated with mortality among opioid users. Although our results do not represent a causal effect, they are consistent with the notion that appropriate interventions targeted at reducing inappropriate prescribing practices of opioids could help lessen risk factors for mortality among opioid users in this population. Moreover, policies aiming to curb potential inappropriate prescribing practices of opioids within FFS insurance plans may be vital to decrease mortality rates in this population.
Supplementary Material
TAKEAWAY POINTS.
This study indicates that incidences of potential inappropriate prescribing practices of opioids are significantly and positively associated with deaths among opioid users in the Georgia Medicaid population.
The odds of experiencing death were 76% higher for opioid users with incidences of potential inappropriate opioid prescribing practices compared with those without any incidences.
Being in managed care Medicaid decreased the odds of experiencing death by 69% for opioid users compared with being in fee-for-service (FFS) Medicaid.
Policies and interventions targeted at reducing inappropriate opioid prescribing practices, especially among FFS enrollees, could help curb the risk factors associated with prescribing opioids.
Acknowledgments
Source of Funding: This research was supported by the National Institute on Drug Abuse of the National Institutes of Health under award number R01DA039930 and the Georgia Department of Community Health, contract number 2015012. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Georgia Department of Community Health.
Footnotes
Prior Presentation: A previous version of this paper was presented at the 2017 International Health Economics Association Congress (Boston, MA; July 8-11, 2017) and the 2017 Addiction Health Services Research Conference (Madison, WI; October 18-20, 2017).
Author Disclosures: The authors report no relationship or financial interest with any entity that would pose a conflict of interest with the subject matter of this article.
REFERENCES
- 1.Prescription opioids: risk factors for prescription opioid abuse and overdose. CDC website; cdc.gov/drugoverdose/opioids/prescribed.html. Updated August 29, 2017. Accessed December 1, 2017. [Google Scholar]
- 2.Mack KA, Zhang K, Paulozzi L, Jones C. Prescription practices involving opioid analgesics among Americans with Medicaid, 2010. J Health Care Poor Underserved. 2015;26(1):182–198.doi: 10.1353/hpu.2015.0009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Garg RK, Fulton-Kehoe D, Franklin GM. Patterns of opioid use and risk of opioid overdose death among Medicaid patients. Med Care. 2017;55(7):661–668. doi: 10.1097/MLR.0000000000000738. [DOI] [PubMed] [Google Scholar]
- 4.Braden JB, Fan MY, Edlund MJ, Martin BC, DeVries A, Sullivan MD. Trends in use of opioids by noncancer pain type 2000-2005 among Arkansas Medicaid and HealthCore enrollees: results from the TROUP study.J Pain. 2008;9(11):1026–1035. doi: 10.1016/j.jpain.2008.06.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sullivan MD, Edlund MJ, Fan MY, DeVries A, Brennan Braden J, Martin BC. Trends in use of opioids for non-cancer pain conditions 2000-2005 in commercial and Medicaid insurance plans: the TROUP study. Pain. 2008;138(2):440–449. doi: 10.1016/j.pain.2008.04.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Zerzan JT, Morden NE, Soumerai S, et al. Trends and geographic variation of opiate medication use in state Medicaid fee-for-service programs, 1996-2002. Med Care. 2006;44(11):1005–1010. doi: 10.1097/01.mlr.0000228025.04535.25. [DOI] [PubMed] [Google Scholar]
- 7.Morden NE, Zerzan JT, Rue TC, et al. Medicaid prior authorization and controlled-release oxycodone. Med Care. 2008;46(6):573–580. doi: 10.1097/MLR.0b013e31816493fb. [DOI] [PubMed] [Google Scholar]
- 8.Ringwalt C, Roberts AW, Gugelmann H, Skinner AC. Racial disparities across provider specialties in opioid prescriptions dispensed to Medicaid beneficiaries with chronic noncancer pain. Pain Med. 2015:16(4):633–640. doi: 10.1111/pme.12555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jayawardhana J, Abraham AJ, Perri M. Opioid analgesics in Georgia Medicaid: trends in potential inappropriate prescribing practices by demographic characteristics, 2009-2014. J Manag Care Spec Pharm. 2018:24(9):886–894. doi: 10.18553/jmcp.2018.24.9.886. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Coolen P, Best S, Lima A, Sabel J, Paulozzi L. Overdose deaths involving prescription opioids among Medicaid enrollees–Washington, 2004-2007. MMWR Morb Mortal Wkly Rep. 2009:58(42):1171–1175. [PubMed] [Google Scholar]
- 11.Yang Z, Wilsey B, Bohm M, et al. Defining risk of prescription opioid overdose: pharmacy shopping and overlapping prescriptions among long-term opioid users in Medicaid .J Pain. 2015:16(5):445–453. doi: 10.1016/j.jpain.2015.01.475. [DOI] [PubMed] [Google Scholar]
- 12.Hartung DM, Middleton L, Haxby DG, Koder M, Ketchum KL, Chou R. Rates of adverse events of long-acting opioids in a state Medicaid program [erratum in Ann Pharmacother. 2007:41(9):1552. doi: 10.1345/aph.1K066a] Ann Pharmacother. 2007;41(6):921–928. doi: 10.1345/aph.1K066. [DOI] [PubMed] [Google Scholar]
- 13.Ray WA, Chung CP, Murray KT, Cooper WO, Hall K, Stein CM. Out-of-hospital mortality among patients receiving methadone for noncancer pain. JAMA Intern Med. 2015:175(3):420–427. doi: 10.1001/jamainternmed.2014.6294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ray WA Chung CP, Murray KT, Hall K, Stein CM Prescription of long-acting opioids and mortality in patients with chronic noncancer pain. JAMA. 2016:315(22):2415–2423. doi: 10.1001/jama.2016.7789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Dilokthornsakul P, Moore G, Campbell JD, et al. Risk factors of prescription opioid overdose among Colorado Medicaid beneficiaries. J Pain. 2016:17(4):436–443. doi: 10.1016/j.jpain.2015.12.006. [DOI] [PubMed] [Google Scholar]
- 16.Cochran G, Gordon AJ, Lo-Ciganic WH, et al. An examination of claims-based predictors of overdose from a large Medicaid program. Med Care. 2017;55(3):291–298. doi: 10.1097/MLR.0000000000000676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fulton-Kehoe D, Sullivan MD, Turner JA, et al. Opioid poisonings in Washington State Medicaid: trends, dosing, and guidelines. Med Care. 2015:53(8):679–685. doi: 10.1097/MLR.0000000000000384. [DOI] [PubMed] [Google Scholar]
- 18.Ruhm CJ Drug poisoning deaths in the United States, 1999-2012: a statistical adjustment analysis. Popul Health Metr. 2016:14:2. doi: 10.1186/s12963-016-0071-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Liu Y, Logan JE, Paulozzi LJ, Zhang K, Jones CM. Potential misuse and inappropriate prescription practices involving opioid analgesics. Am J Manag Care. 2013:19(8):648–658. [PubMed] [Google Scholar]
- 20.Jayawardhana J, Abraham AJ, Young HN, Perri M 3rd. Opioids in Georgia Medicaid: gender and insurance disparities in utilization and potential inappropriate prescribing practices.J Pharm Health Serv Res. 2018:9(2):101–108. doi: 10.1111/jphs.12215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.White AG, Birnbaum HG, Rothman DB, Katz N. Development of a budget-impact model to quantify potential cost savings from prescription opioids designed to deter abuse or ease of extraction. Appl Health Econ Health Policy. 2009:7(1):61–70. doi: 10.2165/00148365-200907010-00006. [DOI] [PubMed] [Google Scholar]
- 22.Goldberg GA, Kim SS, Seifeldin R, Haberman M, Robinson D Jr. Identifying suboptimal management of persistent pain from integrated claims data: a feasibility study. Manag Care. 2003:12(suppl 8):8–13. [PubMed] [Google Scholar]
- 23.Parente ST, Kim SS, Finch MD, et al. Identifying controlled substance patterns of utilization requiring evaluation using administrative claims data. Am J Manag Care. 2004:10(11, pt 1):783–790. [PubMed] [Google Scholar]
- 24.Sundwall DN, Rolfs RT, Johnson E. Utah Clinical Guidelines on Prescribing Opioids for Treatment of Pain. Salt Lake City, UT: Utah Department of Health: 2009. health.utah.gov/prescription/pdf/guidelines/final.04.09opioidGuidlines.pdf. Accessed December 1, 2016. [DOI] [PubMed] [Google Scholar]
- 25.Interagency guideline on opioid dosing for chronic non-cancer pain: an educational aid to improve care and safety with opioid therapy [2010 update]. Washington State Agency Medical Directors’ Group website; agencymeddirectors.wa.gov/files/opioidgdline.pdf. Published 2010. Accessed May 14, 2018. [Google Scholar]
- 26.Charlson ME, Pompei P, Ales KL, Mackenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987:40(5):373–383. [DOI] [PubMed] [Google Scholar]
- 27.Understanding the epidemic. CDC website, cdc.gov/drugoverdose/epidemic. Updated December 19, 2018. Accessed May 18, 2018. [Google Scholar]
- 28.Lanier WA, Johnson EM, Rolfs RT, Friedrichs MD, Grey TC. Risk factors for prescription opioid-related death, Utah, 2008-2009. Pain Med. 2012:13(12):1580–1589. doi: 10.1111/j.1526-4637.2012.01518.x. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.