

Abstract
Introducing appropriate complementary feeding at 6 months of age is crucial for the optimal growth and development of an infant. In Ethiopia, however, no previous national‐level studies have examined the trends and associated factors of complementary feeding practices. The aim of this study is to investigate the trends and determinants of complementary feeding practices in Ethiopia from 2005 to 2016. The study was conducted using the Ethiopia Demographic and Health Survey (EDHS) data for 2005 (N = 2,520), 2011 (N = 2,850), and 2016 (N = 2,864). Percentage point changes in complementary feeding indicators were estimated to examine the trends over the EDHS years. Multivariate logistic regression was used to examine the association between socioeconomic, demographic, health service, and community‐level factors and (a) the introduction of complementary foods, (b) minimum dietary diversity (MDD), (c) minimum meal frequency (MMF), and (d) minimum acceptable diet (MAD). The proportion of mothers who met MDD increased from 6.3% to 13.5% (p < .001), and MAD increased from 4.1% to 7.1% (p = .003) from 2005 to 2016. Improvements in the introduction of complementary foods (from 50.3% to 59.5%, p = .051) and MMF (from 41.3% to 43.6%, p = .288) were not statistically significant. Maternal education and occupation were associated with the introduction of complementary foods, MDD, MMF, and MAD. Higher partner education and frequent antenatal visits were associated with MDD and MAD. Children whose mothers listened to the radio had higher odds of MDD, MMF, and MAD. Our analysis of the EDHS suggests that the proportion of MDD and MAD were unacceptably low. Interventions aiming to improve complementary feeding practices in Ethiopia should also target mothers with low education, antenatal service usage, and media exposure.
Keywords: complementary feeding, infants and young children, minimum acceptable diet, minimum dietary diversity, minimum meal frequency; Ethiopia
Key messages.
The study showed that there were improvements in the proportion of children who met minimum dietary diversity (MDD) and minimum acceptable diet (MAD) in Ethiopia between 2005 and 2016.
Higher maternal and paternal education, mother's informal occupation, frequent antenatal care (ANC) visits, and listening to the radio were associated with MAD among children aged 6–23 months.
Efforts to improve complementary feeding practices should focus on mothers with lower education and employment, infrequent ANC visits, and less exposure to the media in Ethiopia.
Abbreviations
- ANC
antenatal care
- CI
confidence interval
- CSA
Central Statistics Agency
- DHS
Demographic and Health Survey
- EA
enumeration areas
- EDHS
Ethiopian Demographic and Health Survey
- ICF
Inner City Fund
- IYCF
infant and young child feeding
- MAD
minimum acceptable diet
- MDD
minimum dietary diversity
- MMF
minimum meal frequency
- SDG
Sustainable Development Goals
- SNNPR
Southern Nations Nationalities and Peoples Region
- WHO
World Health Organization.
1. INTRODUCTION
The introduction of appropriate complementary feeding around the age of 6 months following exclusive breastfeeding plays a crucial role in optimal growth and development of an infant (Black et al., 2008; Heidkamp, Ayoya, Teta, Stoltzfus, & Marhone, 2015). This is because the breast milk is no longer sufficient to meet the nutritional and developmental requirements of the infant (Arikpo, Edet, Chibuzor, Odey, & Caldwell, 2018; Black et al., 2008). In contrast, inappropriate complementary feeding (such as introducing complementary foods too early or too late, or providing a less diverse diet and/or infrequent feeding) in the early years can result in short‐ and long‐term adverse health outcomes (Abeshu, Lelisa, & Geleta, 2016; WHO, 2009). The short‐term adverse health outcomes may include stunted growth (Lassi, Das, Zahid, Imdad, & Bhutta, 2013), increased risk of diarrhoeal diseases (Ogbo et al., 2017; Ogbo, Page, Idoko, Claudio, & Agho, 2016), micronutrient deficiencies, and increased risk of mortality (Ahmed, Prendiville, & Narayan, 2016; Black et al., 2013). In the long‐term, inappropriate complementary feeding can negatively affect cognitive development (Dewey & Adu‐Afarwuah, 2008; Woldehanna, Behrman, & Araya, 2017), work capacity (Martins et al., 2011), childbirth outcomes (Victora et al., 2008), and social–emotional interactions (Metwally et al., 2016)
The World Health Organization (WHO) and the United Nations Children's Fund (UNICEF) recommend the introduction of adequate, safe, and appropriate complementary foods for infants aged 6–8 months to meet nutritional and developmental needs (WHO, 2009; WHO & UNICEF, 2003). However, reports from low‐ and middle‐income countries (LMICs) indicated that many infants and young children are not receiving appropriate complementary foods (Aguayo, 2017; Black et al., 2013). For example, a study conducted in 46 LMICs showed that the proportion of infants and young children who met the minimum acceptable diet (MAD) were 16% in Africa and 26% in Asia (Lutter et al., 2011). In Africa, previous studies from Nigeria (Ogbo, Page, Idoko, Claudio, & Agho, 2015), Tanzania (Ogbo, Ogeleka, & Awosemo, 2018; Victor, Baines, Agho, & Dibley, 2014), and Francophone and Anglophone Western African countries (Issaka et al., 2015a; Issaka et al., 2015b) have reported that complementary feeding practices were below expected levels.
In Ethiopia, inadequate complementary feeding practices are a major contributor to childhood malnutrition such as stunting (Abeway, Gebremichael, Murugan, Assefa, & Adinew, 2018; Tessema, Belachew, & Ersino, 2013). Despite the decreasing trends in stunting in the last two decades in Ethiopia (from 67% in 2000 to 38% in 2016), more than five million children remain stunted (Wirth et al., 2017). Studies conducted in Ethiopia indicated that homemade complementary foods were inadequate in calories and micronutrients, with limited animal protein and poor intake of fruits and vegetables (Abeshu et al., 2016; Asres, Nana, & Nega, 2018). This inappropriate feeding practice potentially has huge short‐ and long‐term implications for child growth and development in Ethiopia. A recent systematic review focused on the introduction of complementary foods suggested that maternal employment, improved knowledge on complementary feeding, frequent antenatal care (ANC) or postnatal care visits, and giving birth at the health facility were associated with the timely introduction of complementary foods (Habtewold et al., 2018).
No previous nationally representative studies from Ethiopia have investigated trends in WHO/UNICEF complementary feeding indicators, nor has there been a comprehensive assessment of determining factors that make Ethiopian mothers introduce complementary foods too early or too late and provide a less diverse food to and/or infrequently feed their infants and young children. Detailed information on trends and determinants of timely introduction of diverse, frequent, and acceptable diet complementary foods to infants and young children would be helpful to researchers, health practitioners, and policymakers and can inform policy interventions. Furthermore, context‐specific evidence from Ethiopia will be essential to international stakeholders given the promotion of appropriate complementary feeding in LMICs such as Ethiopia in the United Nations Decade of Action on Nutrition (2016–2025, reduce stunting by 40% in 2025; United Nations, 2015) and the Sustainable Development Goal (Sustainable Development Goal‐2, end all forms of malnutrition by 2030; Sustainable Development Goal‐United Nations, 2015). This study aimed to investigate the trends and factors associated with complementary feeding practices (i.e., the introduction of solid, semi‐solid, and soft foods, minimum dietary diversity [MDD], minimum meal frequency [MMF], and MAD) in Ethiopia from 2005 to 2016.
2. METHODS
2.1. Data sources
The study was conducted using the Ethiopia Demographic and Health Survey (EDHS) data for 2005 (N = 2,520), 2011 (N = 2,850), and 2016 (N = 2,864). The EDHS collected nationally representative data on maternal and child health indicators, including infant and young child feeding (IYCF) practices of children under 2 years of age. The EDHS used a two‐stage stratified cluster sampling technique to select households from each enumeration area (EA). In the first stage, clusters were selected from a list of EAs from the population and housing census in Ethiopia (Central Statistics Agency [CSA], 2008). In the second stage, households were randomly selected from each EA after the complete household listing was conducted. The response rate of the surveys for the women questionnaire (which were used to collect information on infant and child health and nutrition) ranged from 94.6% in 2016 to 95.6% in 2005. The detailed methodology of the surveys has been reported in the respective EDHS reports (CSA [Ethiopia] and ICF [Inner City Fund] International, 2012, 2016; CSA [Ethiopia] and ORC Macro, 2006).
2.2. Outcome variables
The study outcome variables included the introduction of solid, semi‐solid, and soft foods, MDD, MMF, and MAD, measured according to mother's recall of foods given to the child during the day and at night prior to the survey (WHO & UNICEF, 2008).
Introduction of solid, semi‐solid, and soft foods (complementary foods) was defined as the proportion of infants 6–8 months of age who received solid, semi‐solid, or soft foods in the 24‐hr period, during the day and at night prior to the survey.
MDD was defined as the proportion of children 6–23 months of age who received foods from four or more of the seven food groups. The seven food groups included grains, roots, and tubers; legumes and nuts; dairy products (milk, yoghurt, and cheese); flesh foods (meat, fish, poultry, and liver/organ meats); eggs; vitamin A‐rich fruits and vegetables; and other fruits and vegetables.
MMF: For breastfed children, MMF was defined as the proportion of children who received solid, semi‐solid, or soft foods two times or more for children aged 6–8 months and three times or more for children aged 9–23 months over the 24‐hr period. For non‐breastfed children, MMF was defined as the proportion of children who received solid, semi‐solid, and soft foods plus other milk or milk products four times or more for children aged 6–23 months in the previous day.
MAD: For breastfed children, MAD was defined as the proportion of children 6–23 months of age who received MDD and MMF in the previous day (apart from breast milk). For non‐breastfed children, MAD was defined as the proportion of children 6–23 months of age who had received other milk or milk products and met the MDD (not including milk feeds) and the MMF in the day before.
2.3. Study variables
The study factors were selected based on the availability of information in the respective EDHS reports (CSA [Ethiopia] and ICF International, 2012, 2016; CSA [Ethiopia] and ORC Macro, 2006). Previous research conducted in Tanzania (Ogbo et al., 2018), Nigeria (Ogbo et al., 2015), Nepal (Na et al., 2018), Bangladesh (Na, Aguayo, Arimond, Narayan, & Stewart, 2018), and Afghanistan (Na, Aguayo, Arimond, Mustaphi, & Stewart, 2018) have also documented the importance of socioeconomic, demographic, health service, and community‐level factors associated with the introduction of solid, semi‐solid, and soft foods, MDD, MMF, and MAD. These variables informed the present study, and the variable categorization was based on the EDHS (CSA [Ethiopia] and ICF International, 2012, 2016; CSA [Ethiopia] and ORC Macro, 2006) and past studies (Na, Aguayo, Arimond, Dahal, et al., 2018; Na, Aguayo, Arimond, Narayan, & Stewart, 2018; Ogbo et al., 2018).
Socioeconomic factors included mother/father education, maternal occupation, and household wealth. Educational status was grouped as no schooling, primary education, or secondary education and higher. Mothers who were working in professional, technical, managerial, clerical, and services areas were grouped under formal occupation; those who were working in agriculture and manual works were grouped under informal occupation, and those who were not working were grouped under no occupation (Ahmed, Page, Arora, & Ogbo, 2019). The EDHS used principal components analysis to calculate the household wealth index based on a series of variables relating to ownership of household assets such as cattle and bicycles, type of materials used for housing construction, and types of water source and sanitation facilities. The EDHS categorized household wealth index into five quintiles (poorest, poorer, poor, rich, or richest). In this study, the household wealth index was re‐classified as “poor,” “middle,” or “rich” based on previously published studies (Ahmed et al., 2019; Ogbo et al., 2018) to increase the sample within each category.
Demographic factors included maternal age (grouped as 15–24 years, 25–34 years, or 35–49 years), sex of the child (male or female), birth order (categorized as 1, 2–4, or 5 and above), family size (categorized as ≤3, 4–5, or 6 and above members), desire for the pregnancy (grouped as desired or not desired), and media exposure (dichotomized as yes or no).
Health service factors included frequency of ANC visit (grouped as none, 1–4 visits, or 4 and above visits), place of birth (grouped as home or health facility delivery), and postnatal check‐up (grouped as yes or no).
Community‐level factors included place of residence (grouped as urban or rural) and region of residence (grouped as large central, small peripheral, and metropolis regions) based on their geopolitical features (Abrha, Shiferaw, & Ahmed, 2016; Ahmed et al., 2019). The large central region included Tigray, Amhara, Southern Nations Nationalities and Peoples Region, and Oromia regions, and the small peripheral region included Afar, Somali, Benishangul, and Gambella regions. The metropolis region included Addis Ababa and Dire Dawa city administrations and Harari region.
2.4. Statistical analysis
Initial analyses involved the calculation of the prevalence of the introduction of solid, semi‐solid, and soft foods, MDD, MMF, and MAD by each of the study factors (socioeconomic, demographic, health service, and community‐level factors) for each year of the EDHS to assess the extent to which the prevalence decreased or increased over the study period (2005–2016). Then, the percentage point change of the outcome variables (the introduction of complementary foods, MDD, MMF, and MAD) by each of the study factors was estimated in examining the changes over the EDHS years (from 2005 to 2011, from 2011 to 2016, and from 2005 to 2016; Tables S2, S3, S4, and S5).
A series of multivariate logistic regression models were used to investigate the association between the socioeconomic, demographic, health service, and community‐level factors with the introduction of solid, semi‐solid, and soft foods, MDD, MMF, and MAD. In Stage 1, the association between socioeconomic factors and the outcome variables was examined, while adjusting for demographic, health service, and community‐level confounding factors based on previously published studies (Issaka, Agho, Page, Burns, et al., 2015; Na, Aguayo, Arimond, Narayan, et al., 2018; Ogbo et al., 2015). In Stage 2, demographic factors were entered to the model to examine their relationship with the outcome measures, while adjusting for socioeconomic, health service, and community‐level confounders. In subsequent models (Stages 3 and 4), similar analytical strategies were used in examining the association between health service and community‐level factors and the outcome variables.
In this study, we used the combined data set to increase the statistical power of the study in order to detect any association between the study factors and the outcomes, as well as to examine trends in the complementary feeding indicators over the study period. In models of the combined data, a similar four‐stage analytical approach was used, as well as adjustment for year of the survey. We also estimated p for trend in models of the combined data to determine changes within each study factors over time. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated as the measure of association between the study factors and outcome variables. All analyses were conducted using Stata Version 14.0 with “svy” command for counts and percentages to adjust for sampling weights, clustering, and stratification effects; “lincom” command for estimating percentage points changes; and “melogit” function for multivariate models (StataCorp, 2017).
2.5. Ethics approval and consent to participate
The Ethiopia Demographic Health Survey (EDHS) was conducted after ethical approval was obtained from the National Research Ethics Review Committee (NRERC) in Ethiopia. During the survey, permission from administrative offices and verbal consent from study participants were obtained before the commencement of data collection. For this study, the data set was obtained after online submission of the proposal to MEASURE DHS/ICF website.
2.6. Availability of data and materials
The analysis was based on the data sets collected Ethiopian Demographic Health Survey. Information on the data and content can be accessed at https://dhsprogram.com/data/available-datasets.cfm
3. RESULTS
3.1. Characteristics of the study participants
Among the study participants, the majority (68.5%) of mothers had no schooling, and more than half (59.1%) of them had no occupation. Nearly 45% of mothers were resided in poor‐level households, and more than half of them had no ANC visit (Table S1).
3.2. Prevalence of complementary feeding practices by study factors
Over the study period, the highest prevalence of the introduction of solid, semi‐solid, and soft foods at 6–8 months of age was found among children whose mothers attended secondary or higher education (79.5%), whereas the lowest prevalence was observed among children who resided in the small peripheral region of Ethiopia (46.5%; Table 1). The proportion of MDD was highest among children whose mothers attended secondary or higher education (26.8%), whereas those who resided in the small peripheral region had the lowest prevalence of MDD (5.1%; Table 2). The highest prevalence of MMF (60.9%;Table 3) and MAD (17.8%; Table 4) was observed among children whose mothers attended secondary or higher education, whereas the lowest prevalence of MMF (33.2%; Table 3) and MAD (3.0%; Table 4) was among those who resided in the small peripheral region.
Table 1.
Factors associated with the introduction of solid, semi‐solid, and soft foods in Ethiopia, 2005–2016
| Variable | 2005 | 2011 | 2016 | 2005–2016 | 2005–2016 | p for trend | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | OR (95% CI) | n (%) | OR (95% CI) | n (%) | OR (95% CI) | n (%) | OR (95% CI) |
% point change (95% CI) |
||
| Socioeconomic factorsa | ||||||||||
| Maternal education | ||||||||||
| No schooling | 227 (49.4) | 1.00 | 174 (41.8) | 1.00 | 187 (59.0) | 1.00 | 588 (49.3) | 1.00 | 9.6 [−2.4, 21.6] | .741 |
| Primary school | 53 (49.4) | 1.03 [0.54, 1.97] | 108 (61.4) | 2.18 [1.14, 4.15] | 114 (54.1) | 0.69 [0.41, 1.15] | 276 (55.7) | 1.17 [0.88, 1.57] | 4.7 [−11.9, 21.2] | .909 |
| Secondary and higher | 21 (67.6) | 2.28 [0.43, 11.94] | 12 (75.7) | 1.86 [0.48, 7.26] | 39 (89.6) | 2.76 [1.17, 6.49] | 72 (79.5) | 2.37 [1.34, 4.20] | 22.0 [−2.7, 46.7] | .712 |
| Maternal occupation | ||||||||||
| No occupation | 207 (47.5) | 1.00 | 158 (43.0) | 1.00 | 214 (60.2) | 1.00 | 579 (50.0) | 1.00 | 12.7 [1.6, 23.8] | .554 |
| Formal occupation | 24 (54.1) | 0.83 [0.30, 2.25] | 55 (74.4) | 2.97 [1.42, 6.24] | 42 (49.6) | 0.74 [0.37, 1.49] | 121 (59.6) | 1.18 [0.81, 1.73] | −4.5 [−30.5, 21.6] | .648 |
| Informal occupation | 67 (58.3) | 2.09 [1.00, 4.35] | 77 (48.9) | 1.78 [0.95, 3.35] | 84 (63.8) | 1.22 [0.71, 2.11] | 228 (56.4) | 1.45 [1.06, 1.99] | 5.6 [−12.8, 23.9] | .225 |
| Partner education | ||||||||||
| No schooling | 153 (52.4) | 1.00 | 123 (43.4) | 1.00 | 130 (55.7) | 1.00 | 405 (50.2) | 1.00 | 3.3 [−9.4, 15.9] | .900 |
| Primary school | 109 (46.5) | 0.81 [0.47, 1.38] | 135 (50.6) | 1.5 [0.89, 2.54] | 146 (59.9) | 0.97 [0.6, 1.54] | 389 (52.4) | 1.10 [0.86, 1.42] | 13.5 [0.4, 26.5] | .819 |
| Secondary and higher | 37 (56.7) | 0.75 [0.31, 1.80] | 37 (63.3) | 1.45 [0.6, 3.52] | 61 (67.5) | 0.77 [0.41, 1.45] | 135 (63.1) | 0.96 [0.66, 1.40] | 10.8 [−9.0, 30.7] | 0.975 |
| Household wealth status | ||||||||||
| Poor | 127 (51.7) | 1.00 | 125 (46.1) | 1.00 | 145 (56.5) | 1.00 | 396 (51.3) | 1.00 | 4.8 [−8.9, 18.5] | .889 |
| Middle | 70 (50.7) | 1.09 [0.58, 2.06] | 57 (47.9) | 1.06 [0.52, 2.18] | 91 (64.0) | 1.83 [0.92, 3.61] | 217 (54.6) | 1.12 [0.81, 1.55] | 13.3 [−2.6, 29.2] | .230 |
| Rich | 105 (48.5) | 1.04 [0.56, 1.94] | 112 (51.6) | 0.73 [0.38, 1.43] | 104 (60.3) | 0.58 [0.29, 1.19] | 322 (53.0) | 0.76 [0.55, 1.04] | 11.8 [−3.0, 26.5] | 0.754 |
| Demographic factorsb | ||||||||||
| Maternal age | ||||||||||
| 15–24 years | 90 (52.6) | 1.00 | 89 (47.5) | 1.00 | 134 (64.2) | 1.00 | 313 (55.2) | 1.00 | 11.5 [−3.7, 26.8] | .527 |
| 25–34 years | 138 (48.7) | 0.69 [0.37, 1.31] | 151 (52.5) | 1.45 [0.81, 2.6] | 152 (57.2) | 0.82 [0.48, 1.40] | 441 (52.7) | 0.96 [0.71, 1.29] | 8.6 [−3.0, 20.2] | .463 |
| 35–49 years | 72 (50.9) | 1.13 [0.45, 2.88] | 55 (41.0) | 1.32 [0.55, 3.15] | 53 (55.5) | 0.67 [0.28, 1.56] | 181 (48.5) | 1.05 [0.67, 1.65] | 4.7 [−15.4, 24.7] | .118 |
| Listening to radio | ||||||||||
| No | 192 (48.9) | 1.00 | 131 (42.9) | 1.00 | 231 (56.0) | 1.00 | 554 (49.9) | 1.00 | 71 [−3.7, 17.9] | .900 |
| Yes | 108 (53.1) | 1.65 [0.93, 2.91] | 164 (54.0) | 1.25 [0.75, 2.09] | 108 (68.6) | 1.16 [0.67, 1.99] | 380 (57.2) | 1.15 [0.88, 1.49] | 15.6 [1.7, 29.4] | .498 |
| Reading newspaper/magazine | ||||||||||
| No | 274 (49.9) | 1.00 | 264 (47.3) | 1.00 | 308 (57.9) | 1.00 | 845 (51.6) | 1.00 | 8.0 [−1.5, 17.5] | .981 |
| Yes | 27 (54.9) | 1.48 [0.52, 4.24] | 30 (63.0) | 1.97 [0.69, 5.63] | 32 (81.1) | 3.06 [1.11, 8.4] | 89 (65.2) | 1.50 [0.91, 2.49] | 26.2 [2.2, 50.2] | .823 |
| Watching TV | ||||||||||
| No | 269 (49.9) | 1.00 | 181 (42.6) | 1.00 | 263 (57.1) | 1.00 | 713 (50.0) | 1.00 | 7.3 [−2.4, 16.9] | .905 |
| Yes | 29 (52.6) | 1.09 [0.39, 3.09] | 111 (61.5) | 1.27 [0.72, 2.25] | 77 (69.1) | 1.43 [0.75, 2.72] | 217 (62.50) | 1.19 [0.85, 1.68] | 16.5 [−6.0, 39.0] | .377 |
| Desire for the pregnancy | ||||||||||
| Desired the pregnancy | 251 (51.3) | 1.00 | 266 (49.8) | 1.00 | 310 (59.4) | 1.00 | 827 (53.5) | 1.00 | 8.0 [−1.2, 17.3] | .577 |
| Not desired the pregnancy | 50 (45.8) | 0.67 [0.33, 1.35] | 29 (38.5) | 0.82 [0.35, 1.94] | 29 (60.7) | 0.75 [0.27, 2.11] | 108 (46.6) | 0.79 [0.53, 1.19] | 14.9 [−10.8, 40.6] | .232 |
| Health service factorsc | ||||||||||
| Antenatal visit | ||||||||||
| None | 202 (48.3) | 1.00 | 162 (46.8) | 1.00 | 99 (58.5) | 1.00 | 462 (49.6) | 1.00 | 10.2 [−4.6, 25.0] | .467 |
| 1–3 | 64 (57.9) | 1.38 [0.75, 2.54] | 69 (48.6) | 1.27 [0.69, 2.33] | 106 (58.7) | 0.80 [0.47, 1.36] | 238 (55.2) | 1.11 [0.84,1.47] | 0.8 [−16.8, 18.4] | .255 |
| 4+ | 35 (53.5) | 1.68 [0.63, 4.5] | 64 (53.7) | 0.89 [0.41, 1.94] | 125 (59.1) | 0.76 [0.40, 1.43] | 225 (56.6) | 1.03 [0.71, 1.49] | 5.7 [−13.2, 24.5] | .491 |
| Postnatal check‐up | ||||||||||
| No | 276 (49.2) | 1.00 | 286 (48.2) | 1.00 | 306 (58.0) | 1.00 | 868 (51.6) | 1.00 | 8.8 [−0.1, 19.7] | .965 |
| Yes | 25 (67.6) | 1.57 [0.55, 4.48] | 9 (57.2) | 2.07 [0.51, 1.67] | 33 (77.5) | 0.92 [0.39, 2.16] | 67 (70.4) | 1.36 [0.83, 2.22] | 9.9 [−15.9, 35.7] | .814 |
| Community‐level factorsd | ||||||||||
| Place of residence | ||||||||||
| Urban | 23 (56.1) | 1.00 | 50 (55.0) | 1.00 | 44 (70.7) | 1.00 | 118 (60.2) | 1.00 | 14.6 [−9.8, 39.0] | .855 |
| Rural | 277 (49.9) | 0.99 [0.33, 2.99] | 244 (47.3) | 0.96 [0.37, 2.45] | 296 (58.1) | 0.85 [0.36, 1.97] | 817 (51.7) | 0.85 [0.54, 1.33] | 8.2 [−1.2, 17.6] | .462 |
| Region of residence | ||||||||||
| Large central | 278 (50.1) | 1.00 | 271 (49.1) | 1.00 | 301 (59.0) | 1.00 | 850 (52.6) | 1.00 | 8.9 [−0.7, 18.5] | .961 |
| Small peripheral | 16 (50.0) | 1.01 [0.55, 1.86] | 10 (30.9) | 0.61 [0.35, 1.08] | 25 (57.4) | 0.93 [0.55, 1.6] | 51 (46.5) | 0.81 [0.61, 1.08] | 9.5 [−6.3, 25.2] | .507 |
| Metropolis | 8 (66.9) | 1.02 [0.43, 2.47] | 13 (57.2) | 1.07 [0.48, 2.38] | 13 (79.8) | 2.01 [0.9, 4.48] | 34 (66.7) | 1.08 [0.72, 1.63] | 12.9 [−6.0, 31.9] | .102 |
Note. n (%): weighted count and proportion for each outcome variable by study factors; % point change indicates percentage point changes from 2005 to 2016.
Abbreviations: CI, confidence; OR, odds ratio.
ORs of socioeconomic factors were adjusted for demographic, health service, and community‐level factors.
ORs of demographic factors were adjusted for socioeconomic, health service, and community‐level factors.
ORs of health service factors were adjusted for socioeconomic, demographic, and community‐level factors.
ORs of community‐level factors were adjusted for socioeconomic, demographic, and health service factors.
Table 2.
Factors associated with minimum dietary diversity in Ethiopia, 2005–2016
| Variable | 2005 | 2011 | 2016 | 2005–2016 | 2005–2016 | p for trend | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | OR (95% CI) | n (%) | OR (95% CI) | n (%) | OR (95% CI) | n (%) | OR (95% CI) |
% point change (95% CI) |
||
| Socioeconomic factors | ||||||||||
| Maternal education | ||||||||||
| No schooling | 96 (4.3) | 1.00 | 45 (2.2) | 1.00 | 189 (10.4) | 1.00 | 330 (5.5) | 1.00 | 6.1 [3.1, 9.1] | .078 |
| Primary school | 57 (11.3) | 1.48 [0.88, 2.49] | 69 (8.3) | 1.84 [1.16, 2.92] | 131 (14.1) | 1.06 [0.77, 1.46] | 256 (11.3) | 1.42 [1.14, 1.77] | 2.7 [−2.4, 7.9] | .320 |
| Secondary and higher | 27 (19.7) | 1.57 [0.76, 3.24] | 28 (21.7) | 1.91 [0.94, 3.87] | 82 (33.3) | 1.71 [1.03, 2.85] | 137 (26.8) | 1.77 [1.27, 2.49] | 13.7 [3.1, 24.3] | .002 |
| Maternal occupation | ||||||||||
| No occupation | 122 (6.1) | 1.00 | 59 (4.1) | 1.00 | 212 (12.1) | 1.00 | 393 (7.6) | 1.00 | 6.0 [2.8, 9.1] | .004 |
| Formal occupation | 29 (12.7) | 1.26 [0.74, 2.15] | 39 (7.4) | 1.47 [0.99, 2.20] | 112 (23.7) | 1.15 [0.79, 1.69] | 180 (14.7) | 1.23 [0.98, 1.56] | 11.0 [3.0, 18.9] | .176 |
| Informal occupation | 29 (4.5) | 1.01 [0.59, 1.75] | 43 (4.4) | 1.59 [0.97, 2.61] | 78 (10.3) | 1.36 [0.92, 2.01] | 150 (6.4) | 1.33 [1.03, 1.71] | 5.8 [12.9, 10.3] | .777 |
| Partner education | ||||||||||
| No schooling | 65 (4.1) | 1.00 | 32 (2.3) | 1.00 | 106 (8.6) | 1.00 | 233 (5.3) | 1.00 | 5.4 [2.2, 8.5] | .097 |
| Primary school | 58 (6.2) | 1.52 [0.93, 2.48] | 71 (5.7) | 1.09 [0.69, 1.72] | 172 (14.8) | 1.37 [0.95, 1.97] | 301 (9.0) | 1.29 [1.02, 1.64] | 8.6 [3.7, 13.4] | .151 |
| Secondary and higher | 56 (17.6) | 1.64 [0.88,3.04] | 35 (13.8) | 1.52 [0.84, 2.72] | 98 (24.1) | 1.83 [1.23, 2.73] | 189 (19.3) | 1.65 [1.24, 2.19] | 6.5 [−1.5, 14.5] | .002 |
| Household wealth status | ||||||||||
| Poor | 50 (4.0) | 1.00 | 40 (3.0) | 1.00 | 120 (9.1) | 1.00 | 211 (5.4) | 1.00 | 5.0 [1.8, 8.3] | .567 |
| Middle | 28 (4.4) | 1.06 [0.53, 2.12] | 16 (2.7) | 1.14 [0.57, 2.30] | 81 (12.3) | 1.73 [1.09, 2.77] | 124 (6.6) | 1.43 [1.03, 1.98] | 7.9 [3.3, 12.5] | .046 |
| Rich | 102 (10.3) | 1.46 [0.84, 2.52] | 85 (8.4) | 1.04 [0.54, 2.00] | 201 (20.0) | 1.78 [1.13, 2.79] | 388 (12.9) | 1.51 [1.11, 2.05] | 9.6 [4.4, 14.8] | .003 |
| Demographic factors | ||||||||||
| Maternal age | ||||||||||
| 15–24 years | 57 (6.9) | 1.00 | 49 (5.7) | 1.00 | 105 (12.5) | 1.00 | 210 (8.3) | 1.00 | 5.6 [1.4, 9.8] | .343 |
| 25–34 years | 94 (6.8) | 1.15 [0.72, 1.83] | 77 (5.1) | 1.20 [0.78, 1.84] | 232 (15.1) | 1.01 [0.69, 1.46] | 403 (9.1) | 1.12 [0.89, 1.41] | 8.3 [4.4, 12.3] | .035 |
| 35–49 years | 29 (4.5) | 0.77 [0.38, 1.60] | 15 (2.4) | 1.11 [0.53, 2.31] | 65 (10.7) | 0.97 [0.58, 1.62] | 109 (5.9) | 0.99 [0.70, 1.38] | 6.2 [1.6, 10.8] | .015 |
| Listening to radio | ||||||||||
| No | 73 (4.0) | 1.00 | 33 (2.2) | 1.00 | 220 (10.2) | 1.00 | 327 (5.9) | 1.00 | 6.2 [3.6, 8.8] | .346 |
| Yes | 107 (10.5) | 1.58 [0.96, 2.60] | 108 (7.5) | 1.37 [0.92, 2.03] | 182 (22.3) | 1.65 [1.18,2.29] | 396 (12.1) | 1.30 [1.05, 1.62] | 11.8 [6.4, 17.2] | .002 |
| Reading newspaper/magazine | ||||||||||
| No | 146 (5.5) | 1.00 | 104 (3.9) | 1.00 | 323 (11.6) | 1.00 | 573 (7.0) | 1.00 | 6.2 [3.5, 8.8] | .032 |
| Yes | 34 (18.5) | 1.52 [0.81, 2.83] | 37 (15.3) | 1.32 [0.79, 2.19] | 79 (36.9) | 1.35 [0.87, 2.11] | 150 (23.5) | 1.27 [0.97, 1.66] | 18.4 [6.3, 30.4] | .009 |
| Watching TV | ||||||||||
| No | 131 (5.1) | 1.00 | 39 (2.0) | 1.00 | 263 (10.8) | 1.00 | 433 (6.2) | 1.00 | 5.7 [3.1, 8.3] | .126 |
| Yes | 49 (18.0) | 2.00 [1.03, 3.88] | 101 (10.3) | 1.85 [1.17, 2.93] | 139 (25.5) | 0.97 [0.63, 1.50] | 290 (16.1) | 1.28 [0.98, 1.66] | 7.5 [−1.9, 16.9] | .002 |
| Desire for the pregnancy | ||||||||||
| Desired the pregnancy | 165 (7.0) | 1.00 | 135 (5.1) | 1.00 | 356 (13.0) | 1.00 | 656 (8.5) | 1.00 | 6.1 [3.2, 8.9] | .007 |
| Not desired the pregnancy | 15 (3.0) | 1.12 [0.68, 1.83] | 6 (2.0) | 0.36 [0.13, 1.00] | 46 (18.0) | 1.52 [0.82, 2.81] | 67 (6.4) | 0.96 [0.69, 1.34] | 14.9 [6.9, 23.0] | .163 |
| Health service factors | ||||||||||
| Antenatal visit | ||||||||||
| None | 110 (5.4) | 1.00 | 42 (2.5) | 1.00 | 125 (12.2) | 1.00 | 277 (5.8) | 1.00 | 6.8 [2.7, 10.9] | .569 |
| 1–3 | 18 (3.9) | 0.73 [0.39, 1.36] | 46 (6.4) | 1.64 [0.96, 2.78] | 101 (11.1) | 1.13 [0.73, 1.75] | 165 (7.9) | 1.29 [0.98, 1.68] | 7.1 [3.1, 11.2] | .002 |
| 4+ | 52 (14.3) | 1.34 [0.72, 2.47] | 53 (10.0) | 2.21 [1.24, 3.95] | 173 (16.8) | 1.11 [0.71, 1.75] | 278 (14.4) | 1.56 [1.18, 2.07] | 2.5 [−3.8, 8.7] | .057 |
| Postnatal check‐up | ||||||||||
| No | 149 (5.5) | 1.00 | 134 (4.7) | 1.00 | 360 (13.1) | 1.00 | 643 (7.7) | 1.00 | 7.6 [4.8, 10.4] | .005 |
| Yes | 31 (19.2) | 1.53 [0.81, 2.89] | 7 (7.6) | 1.86 [0.92, 3.77] | 42 (17.3) | 0.86 [0.55, 1.35] | 80 (16.1) | 1.12 [0.85, 1.48] | −1.9 [−12.1, 8.3] | .099 |
| Community‐level factors | ||||||||||
| Place of residence | ||||||||||
| Urban | 46 (21.2) | 1.00 | 48 (12.0) | 1.00 | 109 (30.1) | 1.00 | 204 (20.7) | 1.00 | 8.9 [−1.9, 19.7] | <.001 |
| Rural | 134 (50.1) | 1.11 [0.50, 2.47] | 92 (3.6) | 0.76 [0.42, 1.38] | 293 (11.2) | 0.73 [0.45, 1.20] | 519 (6.6) | 0.91 [0.65, 1.27] | 6.1 [3.4, 8.8] | .278 |
| Region of residence | ||||||||||
| Large central | 164 (6.2) | 1.00 | 124 (4.6) | 1.00 | 352 (13.0) | 1.00 | 639 (7.9) | 1.00 | 6.8 [3.8, 9.9] | .217 |
| Small peripheral | 5 (3.1) | 1.07 [0.60, 1.90] | 7 (4.7) | 1.54 [0.96, 2.46] | 13 (7.1) | 1.08 [0.72, 1.63] | 25 (5.1) | 1.13 [0.87, 1.47] | 3.9 [0.9, 7.0] | .583 |
| Metropolis | 11 (18.6) | 0.95 [0.51, 1.75] | 10 (12.1) | 1.09 [0.67, 1.76] | 37 (37.3) | 1.54 [1.03, 2.31] | 58 (23.9) | 1.10 [0.85, 1.42] | 18.6 [6.7, 30.6] | .001 |
Note. n (%): weighted count and proportion for each outcome variable by study factors; % point change indicates percentage point changes from 2005 to 2016.
Abbreviations: CI, confidence; OR, odds ratio.
ORs of socioeconomic factors were adjusted for demographic, health service, and community‐level factors.
ORs of demographic factors were adjusted for socioeconomic, health service, and community‐level factors.
ORs of health service factors were adjusted for socioeconomic, demographic, and community‐level factors.
ORs of community‐level factors were adjusted for socioeconomic, demographic, and health service factors.
Table 3.
Factors associated with minimum meal frequency in Ethiopia, 2005–2016
| Variable | 2005 | 2011 | 2016 | 2005–2016 | 2005–2016 | p for trend | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | OR (95% CI) | n (%) | OR (95% CI) | n (%) | OR (95% CI) | n (%) | OR (95% CI) | % point change (95% CI) | ||
| Socioeconomic factors | ||||||||||
| Maternal education | ||||||||||
| No schooling | 869 (39.0) | 1.00 | 875 (43.9) | 1.00 | 764 (42.2) | 1.00 | 2508 (41.6) | 1.00 | 3.2 [−2.0, 8.5] | .386 |
| Primary school | 235 (47.1) | 1.24 [0.94, 1.64] | 469 (56.6) | 1.31 [1.05, 1.65] | 391 (41.9) | 1.13 [0.89, 1.45] | 1094 (48.4) | 1.18 [1.04, 1.35] | −5.2 [−13.1, 2.7] | .191 |
| Secondary and higher | 80 (58.3) | 1.37 [0.81, 2.29] | 84 (66.3) | 1.20 [0.74, 1.95] | 147 (59.6) | 2.05 [1.37, 3.08] | 312 (60.9) | 1.57 [1.22, 2.01] | 1.3 [−12.5, 15.1] | .480 |
| Maternal occupation | ||||||||||
| No occupation | 777 (38.9) | 1.00 | 633 (44.2) | 1.00 | 709 (40.5) | 1.00 | 2119 (40.9) | 1.00 | 1.6 [−3.6, 6.7] | .824 |
| Formal occupation | 131 (56.7) | 1.23 [0.89, 1.68] | 308 (59.3) | 1.60 [1.26, 2.02] | 211 (44.6) | 1.11 [0.85, 1.46] | 650 (53.1) | 1.35 [1.16, 1.56] | −12.1[−23.9, −0.4] | .959 |
| Informal occupation | 274 (43.3) | 1.16 [0.89, 1.51] | 479 (49.2) | 1.41 [1.13, 1.75] | 381 (50.1) | 1.63 [1.28, 2.08] | 1134 (47.9) | 1.43 [1.26, 1.63] | 6.9 [−1.9, 15.7] | .147 |
| Partner education | ||||||||||
| No schooling | 614 (38.6) | 1.00 | 635 (44.9) | 1.00 | 518 (41.8) | 1.00 | 1841 (41.6) | 1.00 | 2.9 [−2.6, 8.4] | .237 |
| Primary school | 393 (41.9) | 1.11 [0.87, 1.41] | 626 (50.4) | 1.08 [0.89, 1.29] | 491 (42.2) | 0.82 [0.66, 1.02] | 1509 (45.2) | 1.03 [0.91, 1.15] | 0.3 [−6.3, 6.9] | .270 |
| Secondary and higher | 171 (53.1) | 1.18 [0.82, 1.71] | 147 (58.1) | 1.05 [0.76, 1.45] | 225 (55.2) | 0.99 [0.75, 1.31] | 542 (55.3) | 1.09 [0.91, 1.3] | 2.1 [−8.0, 12.1] | .491 |
| Household wealth status | ||||||||||
| Poor | 468 (37.3) | 1.00 | 601 (44.5) | 1.00 | 512 (38.7) | 1.00 | 1581 (40.2) | 1.00 | 1.4 [−4.4, 7.3] | .588 |
| Middle | 250 (40.1) | 0.99 [0.75, 1.29] | 305 (51.3) | 1.18 [0.93, 1.50] | 310 (47.3) | 1.34 [0.99, 1.80] | 865 (46.2) | 1.13 [0.97, 1.31] | 7.2 [−1.7, −16.2] | .216 |
| Rich | 467 (47.3) | 1.19 [0.92, 1.53] | 523 (52.0) | 1.06 [0.84, 1.33] | 479 (47.5) | 1.01 [0.76, 1.35] | 1468 (44.5) | 1.11 [0.96, 1.28] | 0.2 [−6.2, 6.6] | .731 |
| Demographic factors | ||||||||||
| Maternal age | ||||||||||
| 15–24 years | 335 (40.3) | 1.00 | 400 (46.7) | 1.00 | 343 (40.9) | 1.00 | 1078 (42.7) | 1.00 | 0.6 [−6.3, 7.4] | .377 |
| 25–34 years | 560 (40.2) | 1.00 [0.78, 1.29] | 752 (49.9) | 1.18 [0.93, 1.50] | 697 (45.4) | 1.26 [0.98, 1.63] | 2009 (45.3) | 1.13 [0.99, 1.29] | 5.2 [−0.01, 10.4] | .289 |
| 35–49 years | 290 (45.1) | 1.29 [0.91, 1.82] | 276 (47.2) | 1.08 [0.77, 1.52] | 262 (42.7) | 1.59 [1.11, 2.26] | 828 (45.0) | 1.27 [1.05, 1.53] | −2.5 [−10.4, 5.4] | .526 |
| Listening to radio | ||||||||||
| No | 692 (37.4) | 1.00 | 639 (42.6) | 1.00 | 909 (41.8) | 1.00 | 2240 (40.6) | 1.00 | 4.4 [−0.2, 9.0] | .929 |
| Yes | 493 (48.5) | 1.29 [1.04, 1.59] | 789 (54.6) | 1.36 [1.13, 1.65] | 393 (48.2) | 1.10 [0.87, 1.39] | 1674 (51.1) | 1.28 [1.14, 1.44] | −0.3 [−7.6, 7.0] | .719 |
| Reading newspaper/magazine | ||||||||||
| No | 1093 (40.8) | 1.00 | 1280 (47.3) | 1.00 | 1192 (43.0) | 1.00 | 3564 (43.7) | 1.00 | 2.2 [−2.1, 6.5] | .576 |
| Yes | 89 (49.0) | 1.89 [0.78, 1.80] | 149 (61.7) | 1.39 [0.95, 2.03] | 110 (51.1) | 0.87 [0.60, 1.28] | 348 (54.5) | 1.07 [0.87, 1.32] | 2.0 [−10.7, 14.8] | .971 |
| Watching TV | ||||||||||
| No | 1048 (40.5) | 1.00 | 885 (45.0) | 1.00 | 1010 (41.4) | 1.00 | 2942 (42.1) | 1.00 | 0.9 [−3.5, 5.3] | .660 |
| Yes | 134 (49.2) | 0.76 [0.53, 1.09] | 541 (55.1) | 1.02 [0.83, 1.26] | 291 (53.3) | 1.19 [0.88, 1.60] | 967 (53.7) | 1.06 [0.91, 1.23] | 4.1 [−6.3, 14.6] | .820 |
| Desire for the pregnancy | ||||||||||
| Desired the pregnancy | 959 (40.7) | 1.00 | 1316 (49.5) | 1.00 | 1186 (43.4) | 1.00 | 3461 (44.7) | 1.00 | 2.7 [−1.6, 7.0] | .414 |
| Not desired the pregnancy | 226 (44.6) | 1.24 [0.96, 1.59] | 113 (38.4) | 0.63 [0.45, 0.89] | 116 (45.3) | 1.08 [0.74, 1.60] | 454 (43.1) | 0.99 [0.83, 1.17] | 7.6 [−10.6, 12.1] | .546 |
| Health service factors | ||||||||||
| Antenatal visit | ||||||||||
| None | 809 (39.9) | 1.00 | 736 (43.6) | 1.00 | 410 (40.1) | 1.00 | 1956 (41.2) | 1.00 | −0.3 [−6.0, 6.6] | .280 |
| 1–3 | 181 (39.7) | 0.80 [0.62, 1.05] | 376 (52.2) | 1.19 [0.97, 1.46] | 403 (44.1) | 0.89 [0.69, 1.15] | 961 (45.9) | 1.03 [0.91, 1.17] | 4.5 [−3.4, 12.3] | .332 |
| 4+ | 187 (51.9) | 1.31 [0.95, 1.81] | 315 (59.1) | 1.25 [0.96, 1.64] | 477 (46.2) | 0.91 [0.69, 1.19] | 979 (50.8) | 1.11 [0.95, 1.30] | −5.7 [−14.1, 2.8] | .111 |
| Postnatal check‐up | ||||||||||
| No | 1095 (40.5) | 1.00 | 1378 (48.2) | 1.00 | 1189 (43.3) | 1.00 | 3662 (44.1) | 1.00 | 2.8 [−1.5, 7.1] | .662 |
| Yes | 89 (54.9) | 1.14 [0.80, 1.63] | 51 (54.7) | 1.75 [1.15, 2.67] | 113 (46.8) | 1.15 [0.83, 1.60] | 252 (50.9) | 1.17 [0.97, 1.42] | −8.2 [−20.9, 4.6] | .522 |
| Community‐level factors | ||||||||||
| Place of residence | ||||||||||
| Urban | 115 (52.6) | 1.00 | 210 (52.0) | 1.00 | 203 (56.0) | 1.00 | 529 (53.6) | 1.00 | 3.4 [−7.0, 13.8] | .789 |
| Rural | 1069 (40.4) | 1.00 [0.66, 1.52] | 1218 (47.9) | 1.16 [0.80, 1.66] | 1098 (41.9) | 0.82 [0.56, 1.21] | 3386 (43.3) | 0.95 [0.77, 1.18] | 1.4 [−2.9, 5.8] | .458 |
| Region of residence | ||||||||||
| Large central | 1101 (41.7) | 1.00 | 1340 (49.2) | 1.00 | 1165 (43.2) | 1.00 | 3606 (44.7) | 1.00 | 1.5 [−2.9, 6.0] | .305 |
| Small peripheral | 46 (28.1) | 0.72 [0.54, 0.95] | 42 (29.3) | 0.54 [0.43, 0.67] | 77 (40.5) | 0.92 [0.72, 1.19] | 165 (33.2) | 0.74 [0.64, 0.84] | 12.4 [4.9, 19.8] | .704 |
| Metropolis | 37 (61.8) | 1.11 [0.80, 1.54] | 47 (55.3) | 0.98 [0.72, 1.33] | 59 (59.3) | 1.08 [0.79, 1.47] | 143 (58.5) | 1.04 [0.88, 1.24] | 2.4 [−14.2, 9.3] | .915 |
Note. n (%): weighted count and proportion for each outcome variable by study factors; % point change indicates percentage point changes from 2005 to 2016.
Abbreviations: CI, confidence; OR, odds ratio.
ORs of socioeconomic factors were adjusted for demographic, health service, and community‐level factors.
ORs of demographic factors were adjusted for socioeconomic, health service, and community‐level factors.
ORs of health service factors were adjusted for socioeconomic, demographic, and community‐level factors.
ORs of community‐level factors were adjusted for socioeconomic, demographic, and health service factors.
Table 4.
Factors associated with minimum acceptable diet in Ethiopia, 2005–2016
| Variable | 2005 | 2011 | 2016 | 2005–2016 | 2005–2016 | p for trend | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | OR (95% CI) | n (%) | OR (95% CI) | n (%) | OR (95% CI) | n (%) | OR (95% CI) | % point change (95% CI) | ||
| Socioeconomic factors | ||||||||||
| Maternal education | ||||||||||
| No schooling | 60 (2.7) | 1.00 | 40 (2.0) | 1.00 | 94 (5.2) | 1.00 | 194 (3.2) | 1.00 | 2.6 [4.4, 4.7] | .053 |
| Primary school | 42 (8.4) | 1.89 [0.95, 3.73] | 58 (7.0) | 1.92 [1.12, 3.29] | 64 (6.8) | 0.92 [0.60, 1.41] | 164 (7.3) | 1.41 [1.04, 1.89] | −1.6 [−5.5, 2.3] | .852 |
| Secondary and higher | 15 (11.3) | 1.47 [0.62, 3.47] | 22 (17.5) | 1.99 [0.85, 4.66] | 53 (21.6) | 1.47 [0.77, 2.83] | 91 (17.8) | 1.68 [1.09, 2.59] | 10.3 [−0.5, 21.1] | .049 |
| Maternal occupation | ||||||||||
| No occupation | 74 (3.7) | 1.00 | 51 (3.5) | 1.00 | 106 (6.0) | 1.00 | 230 (4.4) | 1.00 | 2.3 [1.9, 4.5] | .034 |
| Formal occupation | 20 (8.8) | 1.31 [0.72, 2.38] | 31 (6.0) | 1.33 [0.81, 2.17] | 69 (14.5) | 1.10 [0.67, 1.79] | 120 (9.8) | 1.23 [0.94, 1.62] | 5.7 9 [−1.6, 13.1] | .427 |
| Informal occupation | 23 (3.7) | 1.10 [0.60, 2.01] | 38 (3.9) | 1.43 [0.85, 2.42] | 37 (4.9) | 1.66 [1.06, 2.58] | 99 (4.2) | 1.47 [1.11, 1.94] | 1.2 [−1.9, 4.4] | .488 |
| Partner education | ||||||||||
| No schooling | 41 (2.6) | 1.00 | 29 (2.1) | 1.00 | 50 (4.0) | 1.00 | 133 (3.0) | 1.00 | 1.7 [−0.6, 4.0] | .551 |
| Primary school | 41 (4.3) | 1.41 [0.79, 2.53] | 62 (5.0) | 1.09 [0.66, 1.82] | 82 (7.0) | 1.85 [1.15, 2.98] | 184 (5.5) | 1.46 [1.09, 1.96] | 2.7 [−0.4, 5.8] | .244 |
| Secondary and higher | 35 (11.0) | 1.83 [0.90, 3.73] | 26 (10.3) | 1.31 [0.68, 2.51] | 71 (17.3) | 2.87 [1.70, 4.85] | 132 (13.4) | 2.01 [1.42, 2.86] | 6.3 [−1.2, 13.8] | .005 |
| Household wealth status | ||||||||||
| Poor | 35 (2.8) | 1.00 | 33 (2.4) | 1.00 | 62 (4.7) | 1.00 | 129 (3.3) | 1.00 | 1.9 [−0.4, 4.2] | .971 |
| Middle | 17 (2.7) | 0.74 [0.31, 1.74] | 16 (2.7) | 1.39 [0.64, 3.01] | 54 (8.2) | 1.94 [1.07, 3.52] | 87 (4.6) | 1.43 [0.96, 2.14] | 5.5 [1.7, 9.3] | .021 |
| Rich | 66 (6.7) | 1.39 [0.70, 2.77] | 71 (7.1) | 1.16 [0.57, 2.38] | 96 (9.6) | 1.66 [0.93, 2.95] | 233 (7.8) | 1.52 [1.05, 2.19] | 2.9 [−0.1, 6.6] | .052 |
| Demographic factors | ||||||||||
| Maternal age | ||||||||||
| 15–24 years | 39 (4.7) | 1.00 | 46 (5.4) | 1.00 | 57 (6.9) | 1.00 | 142 (5.6) | 1.00 | 2.2 [−1.2, 5.6] | .438 |
| 25–34 years | 60 (4.3) | 1.30 [0.72, 2.33] | 61 (4.1) | 1.05 [0.66, 1.68] | 127 (8.3) | 1.04 [0.64, 1.69] | 248 (5.6) | 1.09 [0.82, 1.45] | 4.0 [1.1, 6.9] | .204 |
| 35–49 years | 18 (2.9) | 1.36 [0.53, 3.48] | 13 (2.2) | 0.94 [0.43, 2.04] | 27 (4.4) | 1.09 [0.58, 2.05] | 58 (3.2) | 1.11 [0.74, 1.68] | 1.5 [−1.5, 4.5] | .032 |
| Listening to radio | ||||||||||
| No | 47 (2.5) | 1.00 | 28 (1.9) | 1.00 | 124 (5.7) | 1.00 | 199 (3.6) | 1.00 | 3.2 [1.3, 5.1] | .349 |
| Yes | 71 (7.0) | 1.65 [0.92, 2.96] | 92 (6.3) | 2.02 [1.27, 3.20] | 89 (10.8) | 1.47 [0.96, 2.25] | 250 (7.6) | 1.45 [1.12, 1.89] | 3.8 [−0.4, 8.0] | .055 |
| Reading newspaper/magazine | ||||||||||
| No | 96 (3.6) | 1.00 | 92 (3.4) | 1.00 | 167 (6.0) | 1.00 | 355 (4.4) | 1.00 | 2.5 [0.6, 4.4] | .055 |
| Yes | 21 (11.8) | 1.77 [0.84, 3.71] | 28 (11.5) | 1.23 [0.71, 2.12] | 44 (20.6) | 1.14 [0.69, 1.88] | 93 (14.7) | 1.20 [0.87, 1.64] | 8.8 [−2.0, 19.7] | .082 |
| Watching TV | ||||||||||
| No | 93 (3.6) | 1.00 | 36 (1.8) | 1.00 | 135 (5.5) | 1.00 | 263 (3.8) | 1.00 | 1.9 [0.2, 3.7] | .296 |
| Yes | 24 (9.0) | 0.89 [0.40, 2.03] | 84 (8.6) | 1.63 [0.99, 2.70] | 76 (14.0) | 0.89 [0.54, 1.46] | 185 (10.3) | 1.13 [0.83, 1.54] | 5.0 [−2.1, 12.2] | .017 |
| Desire for the pregnancy | ||||||||||
| Desired the pregnancy | 104 (4.4) | 1.00 | 114 (4.3) | 1.00 | 187 (6.8) | 1.00 | 405 (5.2) | 1.00 | 2.4 [0.4, 4.4] | .015 |
| Not desired the pregnancy | 13 (2.6) | 1.27 [0.73, 2.18] | 6 (2.0) | 0.52 [0.19, 1.45] | 25 (9.8) | 1.10 [0.52, 2.35] | 44 (4.2) | 0.91 [0.61, 1.35] | 7.2 [1.3, 13.2] | .744 |
| Health service factors | ||||||||||
| Antenatal visit | ||||||||||
| None | 809 (39.9) | 1.00 | 37 (2.2) | 1.00 | 70 (6.8) | 1.00 | 174 (3.7) | 1.00 | 3.5 [0.5, 6.4] | .386 |
| 1–3 | 181 (39.7) | 0.66 [0.31, 1.42] | 41 (5.8) | 1.64 [0.88, 3.07] | 49 (5.3) | 0.95 [0.52, 1.73] | 104 (5.0) | 1.28 [0.92, 1.79] | 2.3 [−0.7, 5.3] | .046 |
| 4+ | 187 (51.9) | 1.64 [0.78, 3.43] | 42 (7.9) | 1.96 [1.00, 3.85] | 93 (9.0) | 0.91 [0.49, 1.69] | 170 (8.8) | 1.49 [1.03, 2.13] | −0.6 [−5.8, 4.6] | .209 |
| Postnatal check‐up | ||||||||||
| No | 98 (3.6) | 1.00 | 114 (4.0) | 1.00 | 189 (6.9) | 1.00 | 401 (4.8) | 1.00 | 3.3 [1.3, 5.2] | .018 |
| Yes | 19 (11.5) | 1.06 [1.09, 3.87] | 6 (6.8) | 1.47 [0.64, 3.40] | 22 (9.2) | 0.95 [0.57, 1.60] | 47 (9.5) | 1.14 [0.84, 1.56] | −2.4 [−10.4, 5.7] | .341 |
| Community‐level factors | ||||||||||
| Place of residence | ||||||||||
| Urban | 24 (11.0) | 1.00 | 37 (9.2) | 1.00 | 66 (18.2) | 1.00 | 128 (12.9) | 1.00 | 7.2 [−1.0, 15.5] | .007 |
| Rural | 93 (3.5) | 1.61 [0.57, 4.53] | 83 (3.3) | 0.76 [0.41, 1.41] | 145 (5.5) | 0.66 [0.36, 1.21] | 321 (4.1) | 0.92 [0.63, 1.35] | 2.0 [0.2, 3.9] | .536 |
| Region of residence | ||||||||||
| Large central | 109 (4.1) | 1.00 | 111 (4.1) | 1.00 | 181 (6.7) | 1.00 | 400 (5.0) | 1.00 | 2.6 [0.4, 4.7] | .961 |
| Small peripheral | 2 (1.1) | 0.66 [0.32, 1.37] | 4 (3.0) | 1.07 [0.63, 1.82] | 9 (4.7) | 1.51 [0.93, 2.46] | 15 (3.0) | 1.17 [0.87, 1.58] | 3.6 [1.7, 5.4] | .507 |
| Metropolis | 6 (10.7) | 1.05 [0.50, 2.17] | 5 (6.1) | 0.75 [0.45, 1.23] | 22 (22.1) | 1.33 [0.81, 2.19] | 33 (13.7) | 0.95 [0.70, 1.30] | 11.5 [1.1, 21.8] | .102 |
Note. n (%): weighted count and proportion for each outcome variable by study factors; % point change indicates percentage point changes from 2005 to 2016.
Abbreviations: CI, confidence; OR, odds ratio.
ORs of socioeconomic factors were adjusted for demographic, health service, and community‐level factors.
ORs of demographic factors were adjusted for socioeconomic, health service, and community‐level factors.
ORs of health service factors were adjusted for socioeconomic, demographic, and community‐level factors.
ORs of community‐level factors were adjusted for socioeconomic, demographic, and health service factors.
3.3. Trends in complementary feeding practices
The proportion of children who met MDD significantly increased from 6.3% (95% CI: 5.1, 7.8%) in 2005 to 13.5% (95% CI: 11.3, 16.0%) in 2016 (p trend < .001), and MAD also significantly increased from 4.1% (95% CI: 3.2, 5.3%) in 2005 to 7.1% (95% CI: 5.6, 8.9%) in 2016 (p trend = .003). Between 2005 to 2016, the highest increase in the prevalence of introduction of complementary foods was observed among children whose mothers read magazine/newspaper (percentage point change = 26.2%; 95% CI: 2.2, 50.2%; Table 1). The largest percentage point increase in MDD was found among those who resided in the metropolis region (percentage point change = 18.6%; 95% CI: 6.7, 30.6%; Table 2).
The prevalence of the introduction of complementary foods increased from 50.3% (95% CI: 44.3, 56.3%) in 2005 to 59.5% (95% CI: 53.1, 65.5%) in 2016 (p trend = .051), and MMF increased from 41.3% (95% CI: 38.7, 44.0%) in 2005 to 43.6% (95% CI: 40.5, 46.7%) in 2016 (p trend = 0.228), but the increases were not statistically significant (Figure 1). Between 2005 to 2016, children who resided in the small peripheral region showed the highest percentage increase change in MMF (percentage point change = 12.4%; 95% CI: 4.9, 19.8%; Table 3), and those who resided in the metropolis region had the highest percentage point increase in MAD (percentage point change = 11.5%; 95% CI: 1.1, 21.8%; Table 4).
Figure 1.
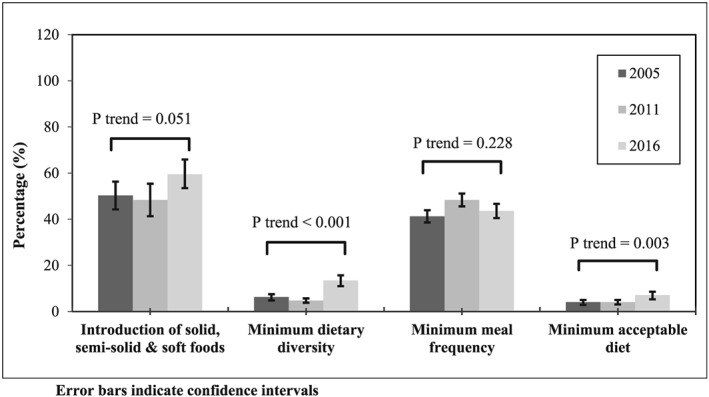
Prevalence and trends of complementary feeding practices in Ethiopia, 2005–2016
3.4. Factors associated with the introduction of complementary foods
From 2005 to 2016, infants whose mothers attended secondary or higher education were more likely to introduce solid, semi‐solid, and soft foods at 6–8 months of age compared with those who had no schooling (OR = 2.37; 95% CI [1.34, 4.40]; Table 1). The likelihood of the introduction of complementary foods was significantly higher among infants whose mothers who had informal occupations compared with those who had no occupation (OR = 1.45; 95% CI [1.07, 1.99]; Table 1).
3.5. Factors associated with MDD
Over the study period, the odds of MDD were significantly higher in children whose mothers or fathers attended secondary or higher education compared with those who did not attend formal schooling (OR = 1.77; 95% CI [1.27, 2.49] for mothers and OR = 1.65; 95% CI [1.24, 2.19] for fathers; Table 2). Children whose mothers resided in wealthy households had higher odds of MDD compared with those who were from poor households (OR = 1.51; 95% CI [1.11, 2.05]). Children whose mothers had four or more ANC visits were more likely to meet MDD compared with those who had no ANC visits (OR = 1.56; 95% CI [1.18, 2.07]). Children whose mothers listened to the radio had higher odds of MDD compared with those who did not listen to the radio (OR = 1.30; 95% CI [1.05, 1.62]; Table 2).
3.6. Factors associated with MMF
Over the study period, children whose mothers attended secondary or higher education (OR = 1.57; 95% CI: 1.22, 2.01), those employed in informal jobs (OR = 1.35; 95% CI: 1.16, 1.56) or formal jobs (OR = 1.43; 95% CI: 1.26, 1.63) and those who listened to the radio (OR = 1.28; 95% CI: 1.14, 1.44) had higher odds of MMF compared with their counterparts. The likelihood of MMF was lower among children who resided in the small peripheral region (i.e. Afar, Somali, Benishangul and Gambella regions) compared with children whose mothers who resided in the larger central region (OR = 0.74; 95% CI: 0.64, 0.84) [Table 3].
3.7. Factors associated with MAD
Over the study period, children who resided in wealthy households had a higher odds of MAD compared with those who were from poor households (OR = 1.47; 95% CI [1.11, 1.94]). Children whose fathers attended secondary or higher education were more likely to meet MAD compared with those whose fathers had no schooling (OR = 2.01; 95% CI [1.42, 2.86]). Children whose mothers had frequent ANC (≥4) visits had higher odds of MAD compared with those who had no ANC visits (OR = 1.49; 95% CI [1.04, 2.13]). The likelihood of MAD was higher among children whose mothers listened to the radio compared with their counterparts (OR = 1.45; 95% CI [1.12, 1.89] Table 4).
4. DISCUSSION
The present study showed improvements in the proportion of children who met MDD (from 6.3% to 13.5%) and MAD (from 4.1% to 7.1%) between 2005 and 2016. There were also improvements in the introduction of solid, semi‐solid, and soft foods (from 50.3% to 59.5%) and MMF (from 41.3% to 43.6%), but were not statistically significant. Improvements in the MDD and MAD may reflect the impact of the national IYCF strategy and any other nutrition initiative in Ethiopia (Ethiopian Federal Ministry of Health, 2004). However, the progress reported in some complementary feeding indicators has not kept pace with the overall economical growths reported in the last two decades in Ethiopia (The World Bank, 2019). Scaling up current national nutritional efforts on food adequacy and dietary diversity would possibly be helpful to Ethiopian mothers to increase IYCF practices.
Over the study period, higher maternal education and occupation were associated with the introduction of complementary foods, MDD, MMF, and MAD. Higher partner education, frequent ANC (≥4) visits, and those who resided in wealthy households were associated with MDD and MAD. Children whose mothers listened to the radio had higher odds of MDD, MMF, and MAD compared with those who did not listen to the radio. Children of mothers who resided in the small peripheral region (i.e., Afar, Somali, Benishangul, and Gambella regions) were less likely to meet MMF compared with those who resided in the large central region. Additionally, maternal occupation and listening to the radio were the most common factors associated with higher odds of MMF over the study period.
Research from many LMICs showed that parental education, particularly maternal education, has a significant impact on the nutritional status of infants and young children (Alderman & Headey, 2017; Iftikhar, Bari, Bano, & Masood, 2017; Smith‐Greenaway, 2013). The present study also indicated that higher maternal education was associated with the introduction of solid, semi‐solid, and soft foods, MDD, MMF, and MAD, consistent with national studies conducted in Tanzania (Ogbo et al., 2018), Nigeria (Ogbo et al., 2015), Sri Lanka (Senarath, Godakandage, Jayawickrama, Siriwardena, & Dibley, 2012), India (Patel et al., 2012), and Bangladesh (Kabir et al., 2012). A possible explanation for the observed relationship could be that education helps the mother to improve her knowledge on healthy eating behaviour for infant and young children such as attentive child feeding practices and providing an appropriately diversified diet (Alderman & Headey, 2017; Pan American Health Organization & WHO, 2001). Higher maternal education may also create the pathway for better access and benefit from child feeding programs (Alderman & Headey, 2017; Black et al., 2013; Guldan et al., 1993). In addition, available feeding programs (often delivered as written materials, pamphlets, or books) might not be suitable for mothers with no schooling (Fein, Labiner‐Wolfe, Scanlon, & Grummer‐Strawn, 2008).
The study also found that children with educated fathers were more likely to meet MDD and MAD, indicating the positive impact of fathers' education on complementary feeding practices. The relationship between mothers' and fathers' education with complementary feeding practices indicates that achieving universal primary education in adolescent girls (future mothers) would be helpful in improving the nutritional status of infant and young children in Ethiopia.
Our study showed that mothers who were in occupation were more likely to timely introduce solid, semi‐solid, and soft foods to their infants. Similarly, infants whose mothers were in occupation were more likely to meet MDD, MMF, and MAD. These findings are consistent with nationally representative studies conducted in Tanzania (Ogbo et al., 2018), Nigeria (Ogbo et al., 2015), Nepal (Joshi, Agho, Dibley, Senarath, & Tiwari, 2012), and India (Patel et al., 2012). According to previous studies, maternal occupation has two conflicting relationships with the feeding of infant and young children. First, maternal occupation may increase household income with subsequent empowerment of women and improvement in the dietary intake of children (Eshete, Abebe, Loha, Gebru, & Tesheme, 2017; Tucker & Sanjur, 1988). Second, maternal occupation may reduce the time a mother can spend in caring and feeding of their children (Eshete et al., 2017; Nair, Ariana, & Webster, 2014; Tucker & Sanjur, 1988). In Ethiopia, policymakers and programme planners would do well to consider interventions that acknowledge these conflicting relationships between maternal occupation and complementary feeding. For example, arranging child day‐care centres near the working area of mothers may be helpful for children to receive attention and time and for the provision of diversified complementary foods (Hirani & Karmaliani, 2013).
Child nutrition education and counselling during ANC and postnatal care visits are also among the effective and less expensive strategies to improve the complementary feeding practice of mothers (WHO, 2009). The present study found that a higher frequency of ANC (≥4) visits was associated with meeting MDD and MMF compared with no ANC visits. This finding is consistent with similar studies conducted in Nigeria (Ogbo et al., 2015), India (Patel et al., 2012), Nepal (Na, Aguayo, Arimond, Dahal, et al., 2018), and Pakistan (Na, Aguayo, Arimond, & Stewart, 2017). ANC visit is often the entry point for mothers to receive appropriate nutritional education and counselling, with subsequent improvement in the mother's knowledge on IYCF (Tariku et al., 2017; Wu et al., 2014). Improving the mother's knowledge is also associated with a positive attitude and a good practice of complementary feeding for children (Blaney, Februhartanty, & Sukotjo, 2015). Strengthening the maternal health care system with nutritional counselling and education during the antenatal and postnatal visits would be helpful in improving complementary feeding practices in Ethiopia.
Children whose mothers listened to the radio had higher odds of meeting MDD, MMF, and MAD than their counterparts, and this finding is consistent with studies conducted in India (Patel et al., 2012) and Nepal (Joshi et al., 2012). In Ethiopia, in recent years, IYCF practices have received significant mass media coverage, which may explain the reason for the observed relationship between a mother's listening to the radio and optimal complementary feeding practices. This finding is also supported by research conducted in Bangladesh, which indicated that intensive counselling combined with nationwide mass media campaign increased the prevalence of MAD from 16% to 50% (Menon et al., 2016). The relationship between listening to the radio and complementary feeding practices can also be explained by listening to the radio being a proxy marker for household wealth and education. Our result suggests that a nationwide mass media campaign may be needed as they remain strategically important in improving IYCF practices.
The present study showed that children who resided in the small peripheral region (i.e., Afar, Somali, Benishangul, and Gambella) were less likely to meet the MMF compared with those who resided in the large central region. This finding may be due to economic reason as the large central region are more developed, with higher socioeconomic status as a result of their fertile soil and rainfall throughout the year. On the other hand, the latter regions were among the areas that suffered from repeated drought, with adverse effects on food production and availability (Food and Agriculture Organization, 2017).
4.1. Study limitations and strengths
The following limitations should be considered while interpreting the findings of this study: (a) cross‐sectional nature of the data might not allow inferring casual direction.; (b) social desirability bias as a result of the tendency to respond to socially desirable answers for dietary diversity and meal frequency questions may have occurred, which may result in overestimation of the proportion of MDD and MMF; (c) overestimation or underestimation of the ORs could also be expected as a result of misclassification bias in the grouping of the variables such as frequency of ANC visit and birth order; and (d) unmeasured confounding factors such as parents' interactions with each other and with their children, communication between family members, and the influence of grandmothers can also be considered as the limitation of this study. Despite the above limitation, nationally representativeness of the data and the high response rate of the surveys are the strengths of this study. The study was also based on EDHS that used a standard questionnaire, which allows comparability of the findings across time and regions.
5. CONCLUSION
The study indicates that MDD and MAD improved between 2005 and 2016; however, their levels remain unacceptably low. Over the same period, the introduction of complementary foods and MMF increased but were not statistically significant. Maternal education and occupation were the common factors associated with timely introduction of complementary foods, MDD, MMF, and MAD. Higher partner education and frequent antenatal visits were associated with MDD and MAD. Listening to the radio increased the odds of MDD, MMF, and MAD. National IYCF policy interventions that aim to improve complementary feeding practices of Ethiopian mothers should also focus on those with limited education, antenatal service usage, and media exposure.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
CONTRIBUTIONS
KYA contributed to the conception of the study, obtained and analysed the data, drafted the manuscript, interpreted the results, and critically revised the manuscript. AP and AA contributed to the conception of the idea and critically revised the manuscript. All authors read and approved the final manuscript. FAO contributed to the conception of the idea, drafting, analysis, and interpretation of the data and critically revised the manuscript.
Supporting information
Table S1.
Characteristics of the study participants in Ethiopia, 2005–2016
Table S2.
Percentage point change in prevalence of solid, semi‐solid and soft foods by study factors, 2005–2016
Table S3.
Percentage point change in the prevalence of minimum dietary diversity by study factors, 2005–2016
Table S4.
Percentage point change in the prevalence of minimum meal frequency by study factors, 2005–2016
Table S5.
Percentage point change in the prevalence of minimum acceptable diet by study factors, 2005–2016
ACKNOWLEDGMENTS
The authors are grateful to Measure DHS, ICF International, Rockville, MD, USA, for providing the data for analysis. KYA and FAO appreciate the support and time of Global Maternal and Child Health Research collaboration (GloMACH) during the peer‐review process. GloMACH Members are Kingsley E. Agho, Felix A. Ogbo, Thierno Diallo, Osita E. Ezeh, Osuagwu L. Uchechukwu, Pramesh R. Ghimire, Blessing J. Akombi, Paschal Ogeleka, Tanvir Abir, Abukari I. Issaka, Kedir Yimam Ahmed, Rose Victor, Deborah Charwe, Abdon Gregory Rwabilimbo, Daarwin Subramanee, Mehak Mehak, Nilu Nagdev, and Mansi Dhami.
Ahmed KY, Page A, Arora A, Ogbo FA. Trends and factors associated with complementary feeding practices in Ethiopia from 2005 to 2016. Matern Child Nutr. 2020;16:e12926 10.1111/mcn.12926
REFERENCES
- Abeshu, M. A. , Lelisa, A. , & Geleta, B. (2016). Complementary feeding: Review of recommendations, feeding practices, and adequacy of homemade complementary food preparations in developing countries—Lessons from Ethiopia. Frontiers in Nutrition, 3, 41 10.3389/fnut.2016.00041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Abeway, S. , Gebremichael, B. , Murugan, R. , Assefa, M. , & Adinew, Y. M. (2018). Stunting and its determinants among children aged 6–59 months in Northern Ethiopia: A cross‐sectional study. Journal of Nutrition and Metabolism, 2018, 1078480 10.1155/2018/1078480 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Abrha, S. , Shiferaw, S. , & Ahmed, K. Y. (2016). Overweight and obesity and its socio‐demographic correlates among urban Ethiopian women: Evidence from the 2011 EDHS. BMC Public Health, 16, 636 10.1186/s12889-016-3315-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aguayo, V. M. (2017). Complementary feeding practices for infants and young children in South Asia. A review of evidence for action post‐2015. Maternal & Child Nutrition, 13(S2), e12439 10.1111/mcn.12439 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ahmed, F. , Prendiville, N. , & Narayan, A. (2016). Micronutrient deficiencies among children and women in Bangladesh: Progress and challenges. Journal of Nutritional Science, 5, e46 10.1017/jns.2016.39 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ahmed, K. Y. , Page, A. , Arora, A. , & Ogbo, F. A. (2019). Trends and determinants of early initiation of breastfeeding and exclusive breastfeeding in Ethiopia from 2000 to 2016. International Breastfeeding Journal, 14(1), 40 10.1186/s13006-019-0234-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alderman, H. , & Headey, D. D. (2017). How important is parental education for child nutrition? World Development, 94, 448–464. 10.1016/j.worlddev.2017.02.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arikpo, D. , Edet, E. S. , Chibuzor, M. T. , Odey, F. , & Caldwell, D. M. (2018). Educational interventions for improving primary caregiver complementary feeding practices for children aged 24 months and under. Cochrane Database of Systematic Reviews, 5 10.1002/14651858.CD011768.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Asres, D. T. , Nana, A. , & Nega, G. (2018). Complementary feeding and effect of spontaneous fermentation on anti‐nutritional factors of selected cereal‐based complementary foods. BMC Pediatrics, 18(1), 394 10.1186/s12887-018-1369-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Black, R. E. , Allen, L. H. , Bhutta, Z. A. , Caulfield, L. E. , de Onis, M. , Ezzati, M. , … Rivera, J. (2008). Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet, 371(9608), 243–260. 10.1016/s0140-6736(07)61690-0 [DOI] [PubMed] [Google Scholar]
- Black, R. E. , Victora, C. G. , Walker, S. P. , Bhutta, Z. A. , Christian, P. , de Onis, M. , … Uauy, R. (2013). Maternal and child undernutrition and overweight in low‐income and middle‐income countries. Lancet, 382(9890), 427–451. 10.1016/s0140-6736(13)60937-x [DOI] [PubMed] [Google Scholar]
- Blaney, S. , Februhartanty, J. , & Sukotjo, S. (2015). Feeding practices among Indonesian children above six months of age: A literature review on their potential determinants (part 2). Asia Pacific Journal of Clinical Nutrition, 24(1), 28–37. 10.6133/apjcn.2015.24.1.14 [DOI] [PubMed] [Google Scholar]
- Central Statistics Agency (CSA) . (2008). Summary and statistical report of the 2007: Population and housing census results. In. Retrieved from https://www.ethiopianreview.com/pdf/001/Cen2007_firstdraft(1).pdf
- Central Statistics Agency (CSA) [Ethiopia] and ICF International . (2012). Ethiopia demographic and health survey 2011. Addis Ababa, Ethiopia and Calverton, Maryland, USA: Central Statistical Agency and ICF International; Retrieved from https://dhsprogram.com/pubs/pdf/fr255/fr255.pdf [Google Scholar]
- Central Statistics Agency (CSA) [Ethiopia] and ICF International . (2016). Ethiopia demographic and health survey 2016. Addis Ababa, Ethiopia and Rockville, Maryland, USA: Central Statistical Agency (CSA) and ICF International; Retrieved from https://dhsprogram.com/pubs/pdf/FR328/FR328.pdf [Google Scholar]
- Central Statistics Agency (CSA) [Ethiopia] and ORC Macro . (2006). Ethiopia demographic and health survey 2005. Addis Ababa, Ethiopia and Calverton, Maryland, USA: CSA and ORC Macro; Retrieved from https://www.dhsprogram.com/pubs/pdf/fr179/fr179%5B23june2011%5D.pdf [Google Scholar]
- Dewey, K. G. , & Adu‐Afarwuah, S. (2008). Systematic review of the efficacy and effectiveness of complementary feeding interventions in developing countries. Maternal & Child Nutrition, 4(Suppl 1), 24–85. 10.1111/j.1740-8709.2007.00124.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eshete, H. , Abebe, Y. , Loha, E. , Gebru, T. , & Tesheme, T. (2017). Nutritional status and effect of maternal employment among children aged 6–59 months in Wolayta Sodo Town, Southern Ethiopia: A cross‐sectional study. Ethiopian Journal of Health Sciences, 27(2), 155–162. 10.4314/ejhs.v27i2.8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ethiopian Federal Ministry of Health (2004). National strategy for infant and young child feeding. Addis Ababa, Ethiopia: Ethiopian Federal Ministry of Health. [Google Scholar]
- Fein, S. B. , Labiner‐Wolfe, J. , Scanlon, K. S. , & Grummer‐Strawn, L. M. (2008). Selected complementary feeding practices and their association with maternal education. Pediatrics, 122(Suppl 2), S91–S97. 10.1542/peds.2008-1315l [DOI] [PubMed] [Google Scholar]
- Food and Agriculture Organization . (2017). Ethiopia drought response plan and priorities. Retrieved from https://reliefweb.int/report/ethiopia/fao-ethiopia-drought-response-plan-and-priorities-2017-revised-version-august-2017
- Guldan, G. S. , Zeitlin, M. F. , Beiser, A. S. , Super, C. M. , Gershoff, S. N. , & Datta, S. (1993). Maternal education and child feeding practices in rural Bangladesh. Social Science & Medicine, 36(7), 925–935. 10.1016/0277-9536(93)90084-H [DOI] [PubMed] [Google Scholar]
- Habtewold, T. D. , Mohammed, S. H. , Endalamaw, A. , Akibu, M. , Sharew, N. T. , Alemu, Y. M. , … Tegegne, B. S. (2018). Breast and complementary feeding in Ethiopia: New national evidence from systematic review and meta‐analyses of studies in the past 10 years. European Journal of Nutrition, 58, 2565–2595. 10.1007/s00394-018-1817-8 [DOI] [PubMed] [Google Scholar]
- Heidkamp, R. A. , Ayoya, M. A. , Teta, I. N. , Stoltzfus, R. J. , & Marhone, J. P. (2015). Complementary feeding practices and child growth outcomes in Haiti: An analysis of data from Demographic and Health Surveys. Maternal & Child Nutrition, 11(4), 815–828. 10.1111/mcn.12090 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hirani, S. A. , & Karmaliani, R. (2013). Evidence based workplace interventions to promote breastfeeding practices among Pakistani working mothers. Women and Birth, 26(1), 10–16. 10.1016/j.wombi.2011.12.005 [DOI] [PubMed] [Google Scholar]
- Iftikhar, A. , Bari, A. , Bano, I. , & Masood, Q. (2017). Impact of maternal education, employment and family size on nutritional status of children. Pakistan Journal of Medical Sciences, 33(6), 1401–1405. 10.12669/pjms.336.13689 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Issaka, A. I. , Agho, K. E. , Page, A. N. , Burns, L. P. , Stevens, G. J. , & Dibley, M. J. (2015b). Determinants of suboptimal complementary feeding practices among children aged 6–23 months in seven francophone West African countries. Maternal & Child Nutrition, 11(S1), 31–52. 10.1111/mcn.12193 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Issaka, A. I. , Agho, K. E. , Page, A. N. , Burns, P. L. , Stevens, G. J. , & Dibley, M. J. (2015a). Determinants of suboptimal complementary feeding practices among children aged 6–23 months in four anglophone West African countries. Maternal & Child Nutrition, 11(S1), 14–30. 10.1111/mcn.12194 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Joshi, N. , Agho, K. E. , Dibley, M. J. , Senarath, U. , & Tiwari, K. (2012). Determinants of inappropriate complementary feeding practices in young children in Nepal: Secondary data analysis of Demographic and Health Survey 2006. Maternal & Child Nutrition, 8(Suppl 1), 45–59. 10.1111/j.1740-8709.2011.00384.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kabir, I. , Khanam, M. , Agho, K. E. , Mihrshahi, S. , Dibley, M. J. , & Roy, S. K. (2012). Determinants of inappropriate complementary feeding practices in infant and young children in Bangladesh: Secondary data analysis of Demographic Health Survey 2007. Maternal & Child Nutrition, 8(Suppl 1), 11–27. 10.1111/j.1740-8709.2011.00379.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lassi, Z. S. , Das, J. K. , Zahid, G. , Imdad, A. , & Bhutta, Z. A. (2013). Impact of education and provision of complementary feeding on growth and morbidity in children less than 2 years of age in developing countries: A systematic review. BMC Public Health, 13(3), S13–S10. 10.1186/1471-2458-13-s3-s13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lutter, C. K. , Daelmans, B. M. , de Onis, M. , Kothari, M. T. , Ruel, M. T. , Arimond, M. , … Borghi, E. (2011). Undernutrition, poor feeding practices, and low coverage of key nutrition interventions. Pediatrics, 128(6), e1418–e1427. 10.1542/peds.2011-1392 [DOI] [PubMed] [Google Scholar]
- Martins, V. J. , Toledo Florencio, T. M. , Grillo, L. P. , do Carmo, P. F. M. , Martins, P. A. , Clemente, A. P. , … Sawaya, A. L. (2011). Long‐lasting effects of undernutrition. International Journal of Environmental Research and Public Health, 8(6), 1817–1846. 10.3390/ijerph8061817 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Menon, P. , Nguyen, P. H. , Saha, K. K. , Khaled, A. , Sanghvi, T. , Baker, J. , … Rawat, R. (2016). Combining intensive counseling by frontline workers with a nationwide mass media campaign has large differential impacts on complementary feeding practices but not on child growth: Results of a cluster‐randomized program evaluation in Bangladesh. The Journal of Nutrition, 146(10), 2075–2084. 10.3945/jn.116.232314 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Metwally, A. M. , El‐Din, E. M. , Shehata, M. A. , Shaalan, A. , El Etreby, L. A. , Kandeel, W. A. , … Rabah, T. M. (2016). Early life predictors of socio‐emotional development in a sample of Egyptian infants. PLoS ONE, 11(7), e0158086 10.1371/journal.pone.0158086 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Na, M. , Aguayo, V. M. , Arimond, M. , Dahal, P. , Lamichhane, B. , Pokharel, R. , … Stewart, C. P. (2018). Trends and predictors of appropriate complementary feeding practices in Nepal: An analysis of national household survey data collected between 2001 and 2014. Maternal & Child Nutrition, 14(Suppl 4), e12564 10.1111/mcn.12564 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Na, M. , Aguayo, V. M. , Arimond, M. , Mustaphi, P. , & Stewart, C. P. (2018). Predictors of complementary feeding practices in Afghanistan: Analysis of the 2015 Demographic and Health Survey. Maternal & Child Nutrition, 14(Suppl 4), e12696 10.1111/mcn.12696 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Na, M. , Aguayo, V. M. , Arimond, M. , Narayan, A. , & Stewart, C. P. (2018). Stagnating trends in complementary feeding practices in Bangladesh: An analysis of national surveys from 2004–2014. Maternal & Child Nutrition, 14(Suppl 4), e12624 10.1111/mcn.12624 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Na, M. , Aguayo, V. M. , Arimond, M. , & Stewart, C. P. (2017). Risk factors of poor complementary feeding practices in Pakistani children aged 6–23 months: A multilevel analysis of the Demographic and Health Survey 2012–2013. Maternal & Child Nutrition, 13(Suppl 2). 10.1111/mcn.12463 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nair, M. , Ariana, P. , & Webster, P. (2014). Impact of mothers' employment on infant feeding and care: A qualitative study of the experiences of mothers employed through the Mahatma Gandhi National Rural Employment Guarantee Act. BMJ Open, 4(4), e004434 10.1136/bmjopen-2013-004434 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ogbo, F. A. , Agho, K. , Ogeleka, P. , Woolfenden, S. , Page, A. , & Eastwood, J. (2017). Infant feeding practices and diarrhoea in sub‐Saharan African countries with high diarrhoea mortality. PLoS ONE, 12(2), e0171792 10.1371/journal.pone.0171792 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ogbo, F. A. , Ogeleka, P. , & Awosemo, A. O. (2018). Trends and determinants of complementary feeding practices in Tanzania, 2004–2016. Tropical Medicine and Health, 46, 40 10.1186/s41182-018-0121-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ogbo, F. A. , Page, A. , Idoko, J. , Claudio, F. , & Agho, K. E. (2015). Trends in complementary feeding indicators in Nigeria, 2003–2013. BMJ Open, 5(10), e008467 10.1136/bmjopen-2015-008467 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ogbo, F. A. , Page, A. , Idoko, J. , Claudio, F. , & Agho, K. E. (2016). Diarrhoea and suboptimal feeding practices in Nigeria: Evidence from the national household surveys. Paediatric and Perinatal Epidemiology, 30(4), 346–355. 10.1111/ppe.12293 [DOI] [PubMed] [Google Scholar]
- Pan American Health Organization , & WHO . (2001). Guiding principles for complementary feeding of the breastfed child. Retrieved from https://www.who.int/nutrition/.../guiding_principles_compfeeding_breastfed.pdf
- Patel, A. , Pusdekar, Y. , Badhoniya, N. , Borkar, J. , Agho, K. E. , & Dibley, M. J. (2012). Determinants of inappropriate complementary feeding practices in young children in India: Secondary analysis of National Family Health Survey 2005–2006. Maternal & Child Nutrition, 8(Suppl 1), 28–44. 10.1111/j.1740-8709.2011.00385.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Senarath, U. , Godakandage, S. S. , Jayawickrama, H. , Siriwardena, I. , & Dibley, M. J. (2012). Determinants of inappropriate complementary feeding practices in young children in Sri Lanka: Secondary data analysis of Demographic and Health Survey 2006–2007. Maternal & Child Nutrition, 8(Suppl 1), 60–77. 10.1111/j.1740-8709.2011.00375.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith‐Greenaway, E. (2013). Maternal reading skills and child mortality in Nigeria: A reassessment of why education matters. Demography, 50(5), 1551–1561. 10.1007/s13524-013-0209-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- StataCorp (2017). Stata survey data reference manual release 15. College Station: Texas A Stata Press Publication StataCorp LLC. [Google Scholar]
- Sustainable Development Goal‐United Nations . (2015). Transforming our world: The 2030 agenda for sustainable development. New York, USA: UN; Retrieved from https://sustainabledevelopment.un.org/content/documents/21252030%20Agenda%20for%20Sustainable%20Development%20web.pdf [Google Scholar]
- Tariku, A. , Alemu, K. , Gizaw, Z. , Muchie, K. F. , Derso, T. , Abebe, S. M. , … Biks, G. A. (2017). Mothers' education and ANC visit improved exclusive breastfeeding in Dabat Health and Demographic Surveillance System Site, northwest Ethiopia. PLoS ONE, 12(6), e0179056 10.1371/journal.pone.0179056 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tessema, M. , Belachew, T. , & Ersino, G. (2013). Feeding patterns and stunting during early childhood in rural communities of Sidama, South Ethiopia. The Pan African Medical Journal, 14, 75 10.11604/pamj.2013.14.75.1630 [DOI] [PMC free article] [PubMed] [Google Scholar]
- The World Bank . (2019). The world bank in Ethiopia. Retrieved from https://www.worldbank.org/en/country/ethiopia/overview
- Tucker, K. , & Sanjur, D. (1988). Maternal employment and child nutrition in Panama. Social Science & Medicine, 26(6), 605–612. 10.1016/0277-9536(88)90024-X [DOI] [PubMed] [Google Scholar]
- United Nations . (2015). United Nations global nutrition agenda: Delivering on the commitment to eradicate malnutrition in all its forms, the role of the un system. New York ,USA: UN; Retrieved from http://scalingupnutrition.org/wp-content/uploads/2015/06/UN-Global-Nutrition-Agenda-2015.pdf [Google Scholar]
- Victor, R. , Baines, S. K. , Agho, K. E. , & Dibley, M. J. (2014). Factors associated with inappropriate complementary feeding practices among children aged 6–23 months in Tanzania. Maternal & Child Nutrition, 10(4), 545–561. 10.1111/j.1740-8709.2012.00435.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Victora, C. G. , Adair, L. , Fall, C. , Hallal, P. C. , Martorell, R. , Richter, L. , & Sachdev, H. S. (2008). Maternal and child undernutrition: Consequences for adult health and human capital. The Lancet, 371(9609), 340–357. 10.1016/S0140-6736(07)61692-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- WHO . (2009). Infant and young child feeding: Model chapter for textbooks for medical students and allied health professionals. Geneva, Switzerland: WHO; Retrieved from https://apps.who.int/iris/bitstream/handle/10665/44117/9789241597494_eng.pdf?sequence=1&isAllowed=y [PubMed] [Google Scholar]
- WHO , & UNICEF . (2003). Global strategy for infant and young child feeding. In. Retrieved from https://apps.who.int/iris/bitstream/handle/10665/42590/9241562218.pdf?sequence=1
- WHO , & UNICEF . (2008). Indicators for assessing infant and young child feeding practices Part 1 Definitions. In.
- Wirth, J. P. , Rohner, F. , Petry, N. , Onyango, A. W. , Matji, J. , Bailes, A. , … Woodruff, B. A. (2017). Assessment of the WHO Stunting Framework using Ethiopia as a case study. Maternal & Child Nutrition, 13(2). 10.1111/mcn.12310 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woldehanna, T. , Behrman, J. R. , & Araya, M. W. (2017). The effect of early childhood stunting on children's cognitive achievements: Evidence from young lives Ethiopia. Ethiopian Journal of Health Development, 31(2), 75–84. [PMC free article] [PubMed] [Google Scholar]
- Wu, Q. , Scherpbier, R. W. , van Velthoven, M. H. , Chen, L. , Wang, W. , Li, Y. , … Car, J. (2014). Poor infant and young child feeding practices and sources of caregivers' feeding knowledge in rural Hebei Province, China: Findings from a cross‐sectional survey. BMJ Open, 4(7), e005108 10.1136/bmjopen-2014-005108 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1.
Characteristics of the study participants in Ethiopia, 2005–2016
Table S2.
Percentage point change in prevalence of solid, semi‐solid and soft foods by study factors, 2005–2016
Table S3.
Percentage point change in the prevalence of minimum dietary diversity by study factors, 2005–2016
Table S4.
Percentage point change in the prevalence of minimum meal frequency by study factors, 2005–2016
Table S5.
Percentage point change in the prevalence of minimum acceptable diet by study factors, 2005–2016
Data Availability Statement
The analysis was based on the data sets collected Ethiopian Demographic Health Survey. Information on the data and content can be accessed at https://dhsprogram.com/data/available-datasets.cfm