

Abstract
Aims
We aim to agree on a set of proposals to improve the current management of heart failure (HF) within the Spanish National Health System (SNHS) and apply the social return on investment (SROI) method to measure the social impact that these proposals would generate.
Methods and results
A multidisciplinary working team of 16 experts was set up, with representation from the main stakeholders regarding HF: medical specialists (cardiologists, internal medicine physicians, general practitioners, and geriatric physicians), nursing professionals, health management professionals, patients, and informal caregivers. This team established a set of proposals to improve the management of HF according to the main areas of HF care: emergency and hospitalization, primary care, cardiology, and internal medicine. A forecast‐type SROI method, with a 1‐year time frame, was applied to measure the social impact resulting from the implementation of these proposals. The required investment and social return were estimated and summarized into a ratio indicating how much social return could be generated for each euro invested. Intangible returns were included and quantified through financial proxies. The approach to improve the management of HF consisted of 28 proposals, including the implementation of a case management nurse network, standardization of operational protocols, psychological support, availability of echocardiography machines at emergency departments, stationary units and primary care, early specialist visits after hospital discharge, and cardiac rehabilitation units, among others. These proposals would benefit not only patients and their informal caregivers but also the SNHS. Regarding patients, proposals would increase their autonomy in everyday activities, decrease anxiety, increase psychological and physical well‐being, improve pharmacological adherence and self‐care, enhance understanding of the disease, delay disease progression, expedite medical assessment, and prevent the decrease in work productivity associated with HF management. Regarding informal caregivers, proposals would increase their quality of life; improve their social, economic, and emotional well‐being; and reduce their care burden. The SNHS would benefit from shorter stays of HF patients at intensive care units and reduction of hospitalizations and admissions to emergency departments. The investment needed to implement these proposals would amount to €548m and yield a social return of €1932m, that is, €3.52 for each euro invested.
Conclusions
The current management of HF could be improved by a set of proposals that resulted in an overall positive social return, varying between areas of analysis. This may guide the allocation of healthcare resources and improve the quality of life of patients with HF.
Keywords: Heart failure, Disease management, Spanish National Health System, Social return on investment (SROI)
Introduction
Heart failure (HF) is a clinical syndrome caused by structural and/or functional alterations of myocardium, which result in reduced cardiac output and/or raised intracardiac pressures at rest or during physical exertion.1 While characterized by impaired systolic and/or diastolic ventricular function, its clinical manifestations are related to haemodynamic effects on other organs.2 In Spain, HF prevalence is 4.7% for population ≥ 18 years old and 6.8% for population > 44 years old.3 This incidence has achieved a rate of 3.9/1000 inhabitants.4 In 2015, cardiovascular diseases were considered the second cause of death in Spain, with 22.3% of these deaths caused by HF, with an age‐adjusted mortality rate of 16.8/100 000 inhabitants.5
This syndrome is associated with an unfavourable prognosis, given that 50% to 65% of patients with HF die within 5 years of diagnosis.6, 7 Furthermore, the presence of co‐morbidities, such as arterial hypertension, diabetes mellitus, and hypercholesterolaemia, are considered detrimental factors for this syndrome.8 In addition, patients with HF usually require assistance in their everyday activities, as the disease significantly affects their work environment, as well as emotional, sexual, and social status. Similarly, informal caregivers also suffer from a negative impact primarily on emotional, physical, and economic levels. Thus, HF patients and their families experience a significant decline of physical and psychological health.9, 10, 11, 12, 13
Consequently, the management of HF should be addressed in a holistic manner. Therefore, an improvement of the current approach is necessary to provide an answer to the unmet needs that benefit the Spanish National Health System (SNHS), patients with HF, and their informal caregivers. Correspondingly, a comprehensive evaluation of improvements is deemed necessary.
Accordingly, the social return on investment (SROI) method, developed in 1996 by the Roberts Enterprise Development Fund, may account for the social value of the holistic management of HF. The main motivation for developing the SROI framework was to measure returns that do not have a market value but possess an intrinsic value (e.g. emotional well‐being of patients or doctor–patient relationship).14 The application of this method helped to improve the assessment of social value, as every intervention could create or destroy social and environmental values.15
In subsequent revisions of the original SROI method, new principles and processes normally used in evaluations of economic and financial return on investment were added to create a framework capable of capturing the total economic, social, and environmental impact of the interventions.16 This method has recently been used in the SNHS in the areas of dermatology, cardiology, and oncology,17, 18, 19 as well as for the management of viral infections, such as human immunodeficiency virus, childhood bronchial asthma, spinal cord injuries,20 arterial hypertension and obesity,21 and paediatric cancer22 in other countries. However, the SROI method has not been applied to the management of HF. Therefore, the objective of this study was twofold: first, to agree on a set of proposals that could potentially improve the current management of HF within the SNHS and, second, to apply the SROI method to measure the social impact that these proposals would generate, including the intangible aspects of the disease.
Methods
The six stages of the SROI analysis were used to achieve the goals of the present study: (i) to establish scope and identify stakeholders; (ii) to map outcomes; (iii) to evidence and give them a value; (iv) to establish the impact; (v) to calculate the SROI; and (vi) to report to the stakeholders, use the results, and embed the SROI process. The first four stages of the SROI analysis were based on the collection of relevant data from the following sources.
-
a
Literature review
We reviewed scientific articles, official data, and, to a lesser extent, grey literature. This helped design a survey to collect relevant data from patients with HF and their informal caregivers. Moreover, the evidence was gathered to obtain necessary information for the SROI analysis.
-
b
Surveys for patients with HF and their informal caregivers
A survey was administered from May to August 2016 among HF patients and their informal caregivers, of legal age and living in Spain, to analyse the impact of HF on each life domain. The patient survey, designed ad hoc for this study, contained a sub‐questionnaire addressed to the patients' primary informal caregiver.
In addition, a five‐level health‐related quality of life (EQ‐5D©) questionnaire was delivered to patients and caregivers; and a 12‐item General Health Questionnaire, a screening tool for minor psychiatric disorders, was administered to HF patients. In brief, the EQ‐5D© evaluates mobility, self‐care, usual activities, pain/discomfort, and anxiety/depression on a scale ranging from ‘no problems' to ‘extreme problems'.
Two data collection methods were used to obtain a larger sample size: paper‐based surveys and an online reproduction of the paper‐based format. Owing to the difficulty of obtaining a random sample of HF population across the country, patients were mainly recruited through cardiovascular disease associations grouped in the CardioAlianza association, following the inclusion criteria designed by expert cardiologists and internal medicine physicians. HF patients ≥18 years old, living in Spain, and who had at least one of the following symptoms in the past year, were included in the study population: shortness of breath during or after physical exercise, exertion, or while lying down; peripheral oedema and/or ascites; unexplained weight gain in the past week; feeling full or stomach bloating; nocturia; or fatigue. Overall, the study sample consisted of 558 patients with HF.
The exclusion criteria were underage subjects, patients living abroad, those who did not have any of the symptoms referred to in the inclusion criteria, or those with any limitation on responding to the questionnaire (no knowledge of Spanish, cognitive disability, etc.).
The calculated sample error (from HF prevalence in Spain23 and population data24) was 4.15% (level of confidence: 95%; distribution p = q = 0.5). This survey did not require the approval of an ethics committee yet conforms with the principles outlined in the Declaration of Helsinki.
-
c
Expert consultation
A multidisciplinary working team (MWT) consisting of 16 experts was set up, with representation from the main stakeholders regarding HF: medical specialists (cardiologists, internal medicine physicians, general practitioners, and geriatric physicians), nursing and health management professionals, patients, and informal caregivers. Four of the 16 experts formed the Project Advisory Committee to establish the current approach to HF (starting point) and, together with the rest of the experts, agreed on a set of proposals aimed to improve the management of HF patients (first objective).
During an extensive meeting, the MWT was organized into the three subgroups from the perspectives of medicine, nursing, and patients. Each group discussed the most relevant proposals. Thereafter, these were shared with the rest of the groups via a spokesperson and discussed and categorized into four blocks that were previously established according to the main areas of HF management: emergency and hospitalization (EH), primary care (PC), cardiology (C), and internal medicine (IM).
Subsequently, the members of the MWT were asked to rate the proposals according to their importance on a scale, ranging from 0 (‘not important') to 10 (‘maximum importance'). Finally, the technical team, on the basis of the basic principle of economy of resource scarcity, decided to select 25% of the proposals with the highest average score in each area. A new general (G) area was introduced to address HF patients treated by different specialists.
Social return on investment analysis
To measure the social impact of selected proposals, a forecast‐type SROI method, with a 1‐year time frame, was applied. The analysis combined both qualitative and quantitative methodologies, as indicated by the SROI guide.25 The investment was determined from the SNHS perspective, while the impact was determined from a social perspective. The relationship between investment and social return was presented by a ratio indicating how much social return could be generated for each euro invested (Figure 1 ). The SROI framework is based on seven principles: (i) involvement of stakeholders, (ii) understanding of changes, (iii) evaluation of significant factors, (iv) inclusion of material aspects, (v) assessment of changes associated with the activity independent of other factors, (vi) transparency, and (vii) verification of the result.25 Initially, the costs associated with the activities and resources required for implementation of each proposal were identified, and the latter were multiplied by their unit prices. These resources, be they medical or non‐medical, or material or human, they were quantified (in number and cost) from literature sources, official data, public prices of health services of the Spanish autonomous regions, and market prices. Following the current convention on SROI methodology, no financial value was given to the time spent on interventions by patients and caregivers (main beneficiaries).25
Figure 1.
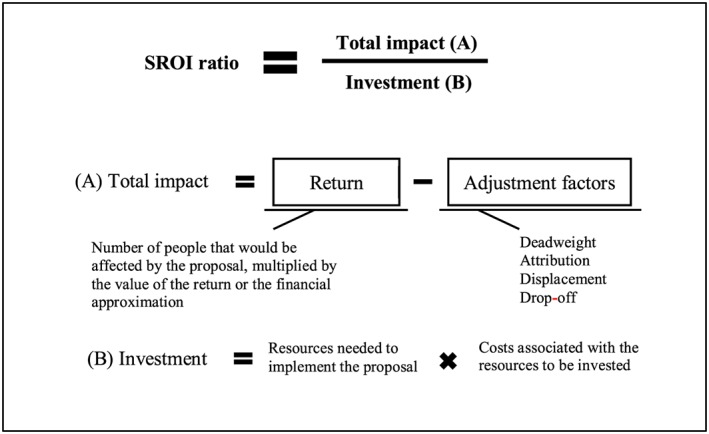
The association between investment, return, total impact, and SROI ratio. SROI, social return on investment.
To calculate returns, the potential consequences of each proposal from the clinical, welfare, economic, and social perspectives were identified. These returns, be they tangible or intangible, or positive or negative, were obtained from the MWT, literature review, official data, public prices of health services of the Spanish autonomous regions, and market prices. Finally, unit market prices and financial proxies (an approximate value when a return does not have a market price) were used to evaluate the tangible and intangible returns, respectively. The adjustment factors, including deadweight (percentage of return that would have been obtained without the proposal), attribution (percentage of the return resulting from activities independent from the proposal), displacement (percentage of the return that would have displaced another return), and drop‐off (percentage of return deterioration over time) were deducted from the return (Figure 1 ). All calculations were based on the prevalence of HF in Spain.4, 23, 24 In addition, the analyses were carried out with a conservative perspective, so that the highest costs were chosen among all the available ones, whereas for the returns, the lowest monetary impact was taken into account. Missing data points were added based on assumptions. Prices were updated to euros from 2015 according to the corresponding consumer price index.26
Finally, a sensitivity analysis was performed by comparing three scenarios that considered the different ways of amortizing the equipment acquisition investment27, 28:
the worst scenario, considering the total costs of the equipment;
an intermediate scenario, considering the minimum amortization of the equipment; and
the best scenario, considering the maximum amortization of the equipment.
Results
The MWT agreed on a total of 28 proposals to improve the current approach to HF management within the SNHS (Table 1). Proposal 17 has been used as an example of how outcomes were mapped and evaluated, and impact established, according to the stages of SROI analysis. The details on each proposal are presented in the Supporting Information.
Table 1.
The proposals to improve the current approach to heart failure in the Spanish National Health System
| Areas of HF management | Proposals |
|---|---|
| General | 1. Optimization of the electronic medical record use |
| 2. Enhancement of electronic prescription use | |
| 3. Implementation of a widespread hospital nurse case manager network | |
| 4. Realization of a widespread community nurse case manager network | |
| 5. Standardization of operational protocols between specialities attending the same patients | |
| 6. Application of a clinical pathway in each hospital | |
| 7. Psychological–emotional support of patients | |
| 8. Professional reorientation and insertion actions | |
| Emergency and hospitalization | 9. Monograph for palliative care patient identification |
| 10. Informative dissemination of the advance directives document | |
| 11. Profile definition of a patient with acute HF and initial comprehensive assessment | |
| 12. Availability of echocardiography division at hospital emergency departments | |
| 13. Awareness campaign for health professionals on the importance of good communication with patients at hospital discharge | |
| 14. Health education for patients and caregivers before hospital discharge | |
| 15. Telephone contact 48 hours after hospital discharge to home | |
| Primary care | 16. Quick access to the echocardiography in the primary care upon initial evaluation |
| 17. Health education for patients with HF | |
| 18. Home visit within 7 days from hospital discharge | |
| 19. Early visit to the corresponding specialist within 2 weeks from hospital discharge | |
| Cardiology | 20.Implementation of cardiac rehabilitation units at reference hospitals |
| 21. Nursing staff specialization at HF units | |
| 22. Approach for non‐invasive mechanical ventilation in the emergency department, cardiology, and acute care units | |
| 23. Early visit to the specialist indicated within 2 weeks from hospital discharge | |
| 24. Quick access to a clinical cardiologist | |
| Internal medicine | 25. Campaigns on the importance of good communication between healthcare professionals and patients followed at the IM department |
| 26. Social resource streamlining | |
| 27. Implementation of an optimal palliative care ratio | |
| 28. Early visit to the specialist indicated within 2 weeks from hospital discharge |
Regarding the mapping of outcomes, Proposal 17 aimed to improve physical and mental well‐being of patients, decrease hospital readmission, delay HF progression, increase labour productivity, and reduce informal care hours (Table 3S ). This further implied an investment on three nursing appointments per year for each patient (Table 2S ).
To monetize the reduction in hospital readmission, Proposal 17 used the number of readmissions due to HF, the percentage of reduction of readmissions due to pharmacological adherence training, and cost of hospitalization. On the other hand, to monetize the improvement of physical and mental well‐being, the average annual costs on leisure, entertainment, and culture were used, which could be equivalent to achieving well‐being of patients in an alternative way.
In Proposal 17, to establish return related to delaying HF progression includes an attribution correction of 50% (a conservative assumption), which means that half of the return may be due to other causes, so the amount of return is reduced to half (Table S5 ).
Once the required total investment and the net social return were estimated, the SROI ratio was calculated (Figure 1 ). The investment for the first year would amount to €548.1m, while the expected social return would amount to €1931.7m. The main investment would be made in areas G (€232.2m) and PC (€180.0m), followed by areas C, IM, and EH (€86.3m, €39.6m, and €10.0m, respectively) (Table 2). In addition, more than half of the total social return would be obtained from area G (€1164.2m), followed by PC (€515.5m) and to a lesser extent from areas C, EH, and IM (€115.0m, €90.6m, and €46.4m, respectively) (Table 2). The detailed evaluation of both the investment and the expected social return for each proposal is presented in the tables of the Supporting Information.
Table 2.
Investment and social return by areas of analysis
| Areas of HF management | Investment | Social return |
|---|---|---|
| General | €232.15 | €1164.17 |
| Emergency and hospitalization | €10.02 | €90.63 |
| Primary care | €180.01 | €515.49 |
| Cardiology | €86.29 | €115.00 |
| Internal medicine | €39.62 | €46.40 |
| Total | €548.08 | €1931.71 |
Therefore, the SROI ratio would yield a return of €3.52 for each euro invested. The highest SROI ratios would be achieved in the areas of EH and G (€9.05 and €5.01, respectively). For the rest of areas of HF management, lower but positive values for SROI ratios would be achieved (€2.86 in PC, €1.33 in C, and €1.17 in IM). These ratios could potentially be higher according to the results of the sensitivity analysis (Table 3).
Table 3.
Social return on investment ratio and sensitivity analysis
| Areas of HF management | Worst scenario (base case) | Intermediate scenario | Best scenario |
|---|---|---|---|
| General | €5.01 | €5.01 | €5.01 |
| Emergency and hospitalization | €9.05 | €16.50 | €18.39 |
| Primary care | €2.86 | €3.80 | €3.96 |
| Cardiology | €1.33 | €1.92 | €1.99 |
| Internal medicine | €1.17 | €1.17 | €1.17 |
| Total SROI | €3.52 | €4.09 | €4.16 |
Note: The SROI ratio is the social return in euros for each euro invested.
SROI, social return on investment.
The obtained results were reported to the Project Advisory Committee for validation. Subsequently, they were disclosed in 2017 at the congresses of the Spanish Society of Cardiology,29 the Spanish Society of Internal Medicine,30 and the Spanish Association of Health Economics,31 as well as via media and social networks.
Discussion
To our knowledge, this is the first study in Spain that has quantified the social value generated by the implementation of a set of proposals to improve the current HF approach in the SNHS. Until now, the expenses related to the management of HF have only been studied in terms of tangible costs,11, 13, 32, 33, 34 without showing a complete overview of their impact on patients' lives, their informal caregivers, and the society. There is no exact method to capture the social value, but the traditional ones leave out of the analysis its total impact. The SROI method, unlike other economic evaluation methods, allows measuring a broader concept of value,35, 36 as it quantifies the tangible and intangible social impact of an intervention, compares it to the investment needed, and gives an SROI ratio that expresses how much social return could be obtained for each euro invested. Furthermore, it includes internal adjustment mechanisms that provide a conservative perspective during the processes of calculation and analysis.
We have shown that the total investment for this approach to HF would imply a social return of €3.52 for each euro invested. Moreover, this amount could be greater because the base case analysis corresponds to the most unfavourable scenario of the sensitivity analysis, and it follows the principles on which the SROI method is based on, including a conservative character and trying not to overestimate the potential of the social return and not to underestimate the required expenses to achieve it. The involvement of stakeholders related to HF and the consensus of proposals may enable a response to the existing gaps in the current management of patients with HF.
The implementation of this new approach in the SNHS could substantially improve the quality of life of HF patients and their informal caregivers, as well as optimize the use of certain healthcare resources. This approach could prevent the decrease in labour productivity and contribute to the reduction of informal caregiving while minimizing unnecessary health expenses. The SROI ratio justifies addressing unmet needs of HF patients through interventions that provide positive results for all stakeholders.
This study has several limitations. A different configuration of MWT could have conducted a different set of proposals from the ones presented in this paper. Therefore, the SROI ratio would have been different. However, the proposals are in line with the latest consensus of scientific societies.37 Furthermore, the New York Heart Association functional class of the study patients with HF was not taken into account, an important parameter that could have altered the results.
In conclusion, based on the SROI method, the implementation of proposals agreed upon to improve HF management would result in a social return of €3.52 for each euro invested. More specifically, the analysis of EH area of HF management yielded the highest SROI ratio, followed by G, PC, C, and IM areas, respectively.
The present study provides valuable information that could guide the allocation of healthcare resources with respect to HF management and improve the quality of life of patients with HF. Having proposals developed by stakeholders involved in the management of different pathologies, knowing their cost, and their social return are of great importance at a time when the general budgets for healthcare are declining, and when the timing of investment is essential.
Conflict of interest
M. M., M. J., Y. I., and A. G. are employees of the consultancy firm that received funds from Novartis Farmacéutica, S.A. to develop this study. E. C., M. S., and N. M. worked as experts for the consultancy firm. However, the participation of Novartis Farmacéutica, S.A. was limited to sponsoring the project.
Funding
This work was supported by Novartis Farmacéutica, S.A..
Supporting information
Data S1. Supporting Information
Acknowledgements
The authors are grateful to patients with HF and their caregivers who participated in this study for their valuable time spent responding to the survey. All of them have significantly contributed to the improvement of knowledge about the impact of HF on the daily lives of patients.
We would also like to thank the patient associations involved in the data collection: Asociación de Cardiópatas y Anticoagulados de La Coruña, Corazones Atendidos, Associació gironina de prevenció i ajuda a les malalties del cor Maçanet Cor, Associació de Malalts Cardíacs i Anticoagulats d'Ontinyent, Asociación Valenciana de Pacientes Anticoagulados de la Comunidad Valenciana, Corazones sin Fronteras, Canarios con Corazón, Federación Andaluza de Asociaciones de Enfermos del Corazón, Asociación Española de Portadores de Válvulas Cardíacas y Anticoagulados, Asociación de Enfermos y Trasplantados de Corazón y Pulmón de Euskadi, Asociación de Trasplantados de Corazón—Castilla y León, Asociación de Trasplantados de Corazón de Gibraltar, and Asociación de Pacientes Cardiacos y Anticoagulados Portuenses.
Finally, the authors are also thankful to the following people for their valuable contribution to the project: Mercè Faraudo, Myriam Moralejo Martín, María Pumares Álvarez, Concepción Sánchez Gallego, Marta Cruz Lázaro, María Aroca Moreno, Dr. Carlos Palanco Vázquez, Alberto San Martín Prado, María José Pirla Buxó, Núria Mesado Batalla, Ana García Otero, José Andrés Peña Álvarez, and Dr. Pablo Díez Villanueva.
Merino, M. , Jiménez, M. , Manito, N. , Casariego, E. , Ivanova, Y. , González‐Domínguez, A. , San Saturnino, M. , Hidalgo‐Vega, Á. , and Blanch, C. (2020) The social return on investment of a new approach to heart failure in the Spanish National Health System . ESC Heart Failure, 7: 130–137. 10.1002/ehf2.12535.
References
- 1. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González‐Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2016; 37: 2129–2200.27206819 [Google Scholar]
- 2. Roig Minguell E. Cardiología: Insuficiencia cardíaca In Farreras‐Rozman, ed. Medicina Interna, 17th ed. Barcelona: Elsevier; 2012. p 414–423. [Google Scholar]
- 3. Sayago‐Silva I, García‐López F, Segovia‐Cubero J. Epidemiología de la insuficiencia cardiaca en España en los últimos 20 años. Rev Esp Cardiol 2013; 66: 649–656. [DOI] [PubMed] [Google Scholar]
- 4. Gomez‐Soto FM, Andrey JL, Garcia‐Egido AA, Escobar MA, Romero SP, Garcia‐Arjona R, Gutierrez J, Gomez F. Incidence and mortality of heart failure: a community‐based study. Int J Cardiol 2011; 151: 40–45. [DOI] [PubMed] [Google Scholar]
- 5. Ministerio de Sanidad, Servicios Sociales e Igualdad . Patrones de mortalidad en España. Madrid: Ministerio de Sanidad, Servicios Sociales e Igualdad; 2015. https://www.mscbs.gob.es/estadEstudios/estadisticas/estadisticas/estMinisterio/mortalidad/docs/PatronesMortalidad2015.pdf (22 October 2018). [Google Scholar]
- 6. Rodríguez‐Artalejo F, Banegas JR, Guallar‐Castillón P. Epidemiología de la insuficiencia cardíaca. Rev Esp Cardiol 2004; 57: 163–170. [PubMed] [Google Scholar]
- 7. Sarría‐Santamera A, Prado‐Galbarro FJ, Martín‐Martínez MA, Carmona R, Gamiño Arroyo AE, Sánchez‐Piedra C, Garrido Elustondo S, del Cura González I. Supervivencia de pacientes con insuficiencia cardiaca en atención primaria. Aten Primaria 2015; 47: 438–445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Ruiz‐Laiglesia F‐J, Sánchez‐Marteles M, Pérez‐Calvo J‐I, Formiga F, Bartolomé‐Satué JA, Armengou‐Arxé A, López‐Quirós R, Pérez‐Silvestre J, Serrado‐Iglesias A, Montero‐Pérez‐Barquero M. Comorbidity in heart failure. Results of the Spanish RICA Registry. Q J Med 2014; 107: 989–994. [DOI] [PubMed] [Google Scholar]
- 9. Naveiro‐Rilo JC, Diez‐Juárez MD, Flores‐Zurutuza L, Rodríguez‐García MÁ, Rebollo‐Gutiérrez F, Romero Blanco A. La calidad de vida en los enfermos con insuficiencia cardiaca: visión desde atención primaria de salud. Gac Sanit 2012; 26: 436–443. [DOI] [PubMed] [Google Scholar]
- 10. Aguirre Montoya JC, Carmona Heredia AM, Pinedo Iguíñez M, Rius Ferrús LIM, Salmerón Hernández M, de Castro Arizmendi R, Valdovinos Perdices P. Estudio de la calidad de vida en pacientes con insuficiencia cardiaca. Enfermería en Cardiología 2009; 26: 11–16. [Google Scholar]
- 11. Comín‐Colet J, Anguita M, Formiga F, Almenar L, Crespo‐Leiro MG, Manzano L, Muñiz J, Chaves J, de Frutos T, Enjuanes C. Calidad de vida relacionada con la salud de los pacientes con insuficiencia cardiaca crónica sistólica en España: resultados del estudio VIDA‐IC. Rev Esp Cardiol 2016; 69: 256–271.26725973 [Google Scholar]
- 12. Serrano‐Aguilar P, Ramallo Fariña Y, Trujillo‐Martín MM, Muñoz‐Navarro SR, Perestelo Pérez L, De las Cuevas‐Castresana C. The relationship among Mental Health Status (GHQ‐12), Health Related Quality of Life (EQ‐5D) and Health‐State Utilities in a general population. Epidemiol Psichiatr Soc 2009; 18: 229–239. [PubMed] [Google Scholar]
- 13. Delgado JF, Oliva J, Llano M, Pascual‐Figal D, Grillo JJ, Comín‐Colet J, Díaz B, Martínez de La Concha L, Martí B, Peña LM. Costes sanitarios y no sanitarios de personas que padecen insuficiencia cardiaca crónica sintomática en España. Revista Española de Cardiología (English Edition) 2014; 67: 643–650. [DOI] [PubMed] [Google Scholar]
- 14. Emerson J, Cabaj M. Social return on investment. Making Waves 2000; 11: 10–14. [Google Scholar]
- 15. Narrillos H. Economía Social. Valoración y medición de la inversión social (método SROI). Madrid: Ecobook; 2012. [Google Scholar]
- 16. Tuan MT. Measuring and/or Estimating Social Value Creation: Insights Into Eight Integrated Cost Approaches [Internet]. Bill & Melinda Gates Foundation—Impact Planning and Improvement; 2008 http://cmapspublic.ihmc.us/rid=1LHK87JH8-F72NL0-2R6P/WWL-report-measuring-estimating-social-value-creation%5B1%5D.pdf (08 February 2016).
- 17. González A, Ivanova Y, Jiménez M, Merino M, Hidalgo Á, Alfonso S, Carretero G, Ledesma A, Sarquella E, Blanch C, Costa A. Grupo de Expertos del Proyecto SROI‐PSORIASIS. Retorno Social de la Inversión de un abordaje ideal de la psoriasis. Madrid: Instituto Max Weber; 2016. [Google Scholar]
- 18. Durán Piñeiro G, del Sánchez Carreira M, Peña Gil C, Paredes Galán E, Gómez Ruíz R, Lado Sestayo R, Grande Sellera C, Lamas Díaz MJ. El retorno económico y social de la e‐interconsulta de cardiología en el área de Vigo. ICEDE Working Paper Series, ISSN 2254‐7487 2015; 11:1–28. [Google Scholar]
- 19. de Castro Carpeño J, Fírvida Pérez JL, Lianes Barragán P, Cobo Dols MÁ, Gil JM, Carrato Mena A, Fernández Puentes Á, García Palomo A, Muñoz Mateu M, Carreras Soler MJ, Peñuelas Saiz MÁ, Parrondo García J, Pinyol i Villena C. Cuantificando el beneficio de la sustitución por vinorelbina oral en los pacientes susceptibles de tratamiento con vinorelbina. Estudio del retorno social de la inversión. Revista Española de Economía de la Salud 2018; 13: 336–353. [Google Scholar]
- 20. Banke‐Thomas AO, Madaj B, Charles A, van den Broek N. Social Return on Investment (SROI) methodology to account for value for money of public health interventions: a systematic review. BMC Public Health 2015; 15: 582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Masters R, Anwar E, Collins B, Cookson R, Capewell S. Return on investment of public health interventions: a systematic review. J Epidemiol Community Health 2017; 71: 827–834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Laing CM, Moules NJ. “It's not just camp!”: understanding the meaning of children's cancer camps for children and families. J Pediatr Oncol Nurs 2016; 33: 33–44. [DOI] [PubMed] [Google Scholar]
- 23. Anguita Sánchez M, Crespo Leiro MG, de Teresa Galván E, Jiménez Navarro M, Alonso‐Pulpón L, Muñiz García J. Prevalencia de la insuficiencia cardiaca en la población general española mayor de 45 años. Estudio PRICE. Rev Esp Cardiol 2008; 61: 1041–1049.18817680 [Google Scholar]
- 24. Instituto Nacional de Estadística . Estadística del Padrón Continuo. Datos provisionales a 1 de enero de 2016. Población mayor o igual a 45 años. 2016. http://www.ine.es/jaxi/Datos.htm?path=/t20/e245/p04/provi/l0/&file=00000002.px (21 November 2016).
- 25. Nicholls J, Lawlor E, Neitzert E, Goodspeed T. A guide to Social Return on Investment [Internet]. UK: The SROI Network. Accounting for Value; 2012. http://www.socialvalueuk.org/app/uploads/2016/03/The%20Guide%20to%20Social%20Return%20on%20Investment%202015.pdf (27 March 2019) [Google Scholar]
- 26. Instituto Nacional de Estadística . Índice de Precios de Consumo. Base 2016. Índices nacionales: general y de grupos ECOICOP. http://www.ine.es/jaxiT3/Tabla.htm?t=22553&L=0 (26 July 2017).
- 27. ESPAÑA . Real Decreto 1777/2004, de 30 de julio, por el que se aprueba el Reglamento del Impuesto sobre Sociedades. BOE núm. 189, 6 agosto. 2004.
- 28. Pascual Pedreño E. Contabilidad: Iniciación práctica (e‐book), 4th ed. Lex Nova: Valladolid; 2010. [Google Scholar]
- 29. Merino Ventosa M, Jiménez Torres M, Manito Lorite N, Casariego Vales E, Ivanova Markova Y, González Domínguez A, San Saturnino Peciña M, Blanch Mur C. 4013‐4 – Retorno social de la inversión de un abordaje ideal en insuficiencia cardiaca en el sistema nacional de salud español. Rev Esp Cardiol 2017; 70: 500. [Google Scholar]
- 30. Merino Ventosa M, Jiménez Torres M, Manito Lorite N, Casariego Vales E, Ivanova Markova Y, González Domínguez A, San Saturnino Peciña M, Blanch Mur C. ICYFA‐023 – Retorno social de la inversión de un abordaje ideal en insuficiencia cardiaca en el sistema nacional de salud español. Rev Clin Esp 2017; 217: 85. [Google Scholar]
- 31. Merino M, Jiménez M, Ivanova Y, González A, Villoro R, Hidalgo A, Casariego E, Manito N, San Saturnino M, Fajardo T, Blanch C, Lloret J, Grupo de Trabajo Multidisciplinar del Proyecto SROI‐IC . P‐53. Valor social de un abordaje ideal de la insuficiencia cardiaca. Gac Sanit 2017; 31: 382.28545739 [Google Scholar]
- 32. Montes‐Santiago J, Rodil V, Formiga F, Cepeda JM, Urrutia A. Características y costes de los pacientes ingresados por arritmias cardiacas en España. Rev Clin Esp 2013; 213: 235–239. [DOI] [PubMed] [Google Scholar]
- 33. Cabo J, Herreros J, Trainini J. Análisis de costes (evaluación económica) en el tratamiento de la insuficiencia cardíaca. Cirugía Cardiovascular 2011; 18: 233–243. [Google Scholar]
- 34. Oliva J, Jorgensen N, Rodríguez JM. Carga socioeconómica de la insuficiencia cardiaca: revisión de los estudios de coste de la enfermedad. Pharmacoeconomics Spanish Res Art 2010; 7: 68–79. [Google Scholar]
- 35. Drummond MF, Sculpher MJ, Claxton K, Stoddart GL, Torrance GW. Methods for the Economic Evaluation of Health Care Programmes. Oxford: Oxford University Press; 2015. [Google Scholar]
- 36. Nicholls J. Social return on investment—development and convergence. Eval Program Plann 2017; 64: 127–135. [DOI] [PubMed] [Google Scholar]
- 37. Real J, Cowles E, Wierzbicki AS. Chronic heart failure in adults: summary of updated NICE guidance. BMJ 2018; 362: k3646. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1. Supporting Information