

Abstract
Therapist turnover is a major problem in community mental health. Financial strain, which is composed of cognitive, emotional, and behavioral responses to the experience of economic hardship, is an understudied antecedent of therapist turnover given the tumultuous financial environment in community mental health. We prospectively examined the relationship between therapist financial strain and turnover in 247 therapists in 28 community mental health agencies. We expected greater therapist financial strain to predict higher turnover and participation in a system-funded evidence-based practice (EBP) training initiative to alleviate this effect. Controlling for covariates, financial strain predicted therapist turnover (OR 1.12, p = .045), but not for therapists who participated in an EBP training initiative. Reducing financial strain and/or promoting EBP implementation may be levers to reduce turnover.
Keywords: Financial strain, Turnover, Implementation, Behavioral health services, Evidence-based practice, System transformation
Therapist turnover, or when a therapist voluntarily or involuntarily ends their tenure in their place of employment, is a major challenge in behavioral health services; between 30 and 60% of therapists leave their organization annually (Beidas et al. 2016a; Mor Barak et al. 2001). High rates of therapist turnover threaten the quality and consistency of mental health services (Babbar et al. 2018; Mor Barak et al. 2001) and contribute to poor staff morale, reduced productivity, weaker work teams, and increased costs of training new employees (Bingley and Westergaard-Nielsen 2004). Turnover also poses a specific threat to organizations implementing evidence-based practices (EBPs). To improve the well-being of vulnerable populations, the Institute of Medicine and other health organizations have called for increased efforts to improve the adoption, implementation, and sustainment of EBPs in community settings (Committee on Developing Evidence-Based Standards for Psychosocial Interventions for Mental Disorders 2015; Williams and Beidas 2018a). For organizations implementing new practices, turnover leads to a reduction in their highly trained work-force, leading to reduced fidelity to and penetration of EBPs overall (Beidas et al. 2016a; Droege and Hoobler 2003; Rollins et al. 2010; Woltmann et al. 2008). Thus, retaining staff during EBP implementation is critical given the resources that agencies and systems invest in training, maintaining the skills necessary to adhere to intervention protocols, and the ancillary support necessary for therapists to gain mastery in the model (Aarons et al. 2009). Given the importance of building a stable workforce within behavioral health agencies to support EBP implementation and sustainment, identifying mutable antecedents of therapist turnover is important to inform future turnover reduction strategies.
Previously identified antecedents of turnover generally fall into two categories: environmental factors, such as lack of support and high stress environments (Aarons et al. 2009), and psychological factors, such as employee burnout (Evans et al. 2006). Burnout is characterized as a combination of emotional exhaustion, depersonalization, and feelings of limited personal achievement (Evans et al. 2006; Maslach et al. 1996). These predictors of turnover are prevalent in the behavioral health field, especially given the tumultuous financial environments that these agencies reside in (Evans et al. 2006; Paris and Hoge 2010; Stewart et al. 2016). While there is a robust literature on the psychological and environmental factors that may lead to therapist turnover listed above, one psychological variable that has received surprisingly little attention is financial strain.
Financial strain, which is comprised of one’s cognitive, emotional, and behavioral responses to the experience of economic hardship, is a potential sequela of low wages. It occurs when an individual perceives that their real expenses exceed their income, leading to difficulty in meeting financial responsibilities (Aldana and Liljenquist 1998). Perceived measures of financial strain provide a richness that objective measures (e.g., yearly income) do not, for they support the examination of not only how financial conditions affect individuals and family’s needs and wants, but also how individuals perceive their financial status in relation to others (Prawitz et al. 2006). Further, measuring perceived financial strain rather than actual income allows for regional comparisons, alleviating statistical concerns which arise when comparing salaries in localities where cost of living varies. Outside of the behavioral health literature, financial strain has been cited as a critical source of stress for employees (Jacobson et al. 1996), resulting in productivity losses and increased absenteeism in the workplace (Bagwell and Kim 2003; Garman et al. 1996; Joo and Garman 1998).
There is little understanding of how therapists employed in the behavioral health sector experience financial strain and the potential sequelae of this stress. Further research into this construct is warranted given the historically low wages that therapists earn and the poor fiscal climate in behavioral health agencies (Golberstein and Busch 2017; Stewart et al. 2016). With a few exceptions, the majority of services provided in the public mental health system are funded by Medicaid, which reimburses on a fee-for-service basis at rates lower than those in the private market place (Stewart et al. 2016). Further, substantial cuts in state aid to behavioral health programs and threats to the Affordable Care Act have increased concerns about behavioral health budgets (Hoagwood et al. 2017). The effect of this tumultuous financial environment that agencies and therapists are faced with is highlighted by one qualitative study which found that 41% of therapists reported leaving their agency in the past year due to financial reasons, such as inadequate compensation (Beidas et al. 2016a).
Given the low wages that therapists earn and the poor fiscal climate in behavioral health agencies (Golberstein and Busch 2017; Stewart et al. 2016), addressing financial strain has been suggested as an intervention target to reduce turnover (e.g., offering competitive salaries and financial incentives; Paris and Hoge 2010). However, no studies have empirically examined the link between perceived financial strain and turnover in mental health. Establishing this link is necessary to inform the development of such turnover interventions.
Additionally, there are reasons to believe that participation in an EBP implementation effort may mitigate the potential negative sequelae of perceived financial strain on turnover. Studies have suggested that participation in an EBP training initiative with supportive components (e.g., fidelity monitoring, supervision) reduces the likelihood of turnover (Aarons et al. 2009). Being trained in an EBP, along with added supportive components such as consultation, technical assistance, and/or fidelity monitoring, may increase therapist competence, reduce burnout, and increase therapist self-efficacy to treat their clients (Beidas and Kendall 2010; Ouellette et al. 2018), all of which may translate to reduced turnover. Therapists may also become more invested in their organization and more connected to the cohort of therapists they were trained with, increasing job embeddedness (Beidas et al. 2016a).
While to our knowledge, no work has specifically examined perceived financial strain and turnover, there are a few studies that have examined the impact of a therapist’s objective economic status on turnover in the context of the implementation of EBPs. For example, Sheidow et al. (2007) found that organizations that paid lower salaries had greater odds of therapist turnover relative to organizations that paid higher salaries in the context of the implementation of Multisystemic Therapy. Another study examined the implementation of behavioral couples’ therapy (BCT) 3–5 years after initial training and found that the only agency still offering BCT had a low therapist turnover rate, “perhaps due to substantially higher pay compared to therapists in the programs no longer using BCT” (Fals-Stewart et al. 2004, p. 180). However, neither study addressed therapist perceptions of their financial status, which may be more salient than actual wages (Prawitz et al. 2006), or directly examined whether wages impacted turnover. More work is needed to parse apart the roles that perceived financial strain and participation in an EBP training initiative play in influencing turnover to inform future efforts to reduce turnover rates in community mental health.
To address this, we prospectively examined the relationship between therapist perceived financial strain and turnover in a large public mental health system. We also examined whether participation in an EBP training initiative moderated the relationship between financial strain and turnover. Given prior work theorizing that financial strain is associated with turnover, we hypothesized that higher rates of perceived financial strain would increase the likelihood that a therapist would leave their agency (Hypothesis 1). Consistent with prior work (Aarons et al. 2009), we also expected that therapist participation in an EBP training initiative would reduce the likelihood that a therapist would turnover (Hypothesis 2). Finally, we expected that participation in an EBP training initiative would moderate the effect of perceived financial strain on turnover, such that increased financial strain will not predict increased turnover for therapists who participated in an EBP training initiative (i.e., that participation in an EBP training initiative would serve as a protective factor and buffer the relationship between financial strain and turnover; Hypothesis 3).
Materials and Methods
Setting
The Department of Behavioral Health and Intellectual disAbility Services (DBHIDS) is the primary funder and policymaker for behavioral health services in the City of Philadelphia. In partnership with Community Behavioral Health, a not-for-profit 501(c) (3) corporation contracted by the City of Philadelphia, they provide behavioral health coverage for over 600,000 Medicaid-enrolled individuals (Powell et al. 2016). Since 2007, DBHIDS has committed to a system-wide transformation to ensure services are based upon the principles of recovery, resilience, and self-determination to optimize outcomes for the most vulnerable populations (Abrahams et al. 2013).
EBP Training Initiatives
At the time of data collection, DBHIDS supported four specific EBP training initiatives across a variety of care settings (i.e., outpatient, inpatient, residential): cognitive therapy, prolonged exposure, trauma-focused cognitive behavioral therapy, and dialectical behavior therapy. A full-time city employee coordinated the implementation, training, and ongoing consultation of each initiative. The initiatives have collectively supported and financed training, expert consultation, and ongoing technical assistance for more than 500 therapists in over 50 organizations and 10 levels of care in the Philadelphia system (Powell et al. 2016). Therapists were trained in EBP training initiatives on a rolling basis in cohorts starting with the cognitive therapy initiative in 2007, prolonged exposure and trauma-focused cognitive behavioral therapy in 2011, and dialectical behavioral therapy in 2012 (Powell et al. 2016).
Agencies and Participants
In 2015, as part of the second wave of a larger three wave study (Beidas et al. 2013), we used purposive sampling to recruit therapists working within 31 of the 100 behavioral health agencies that serve the largest proportion of youth in Philadelphia. Of these 31 agencies, 22 (71%) agreed to participate. Several agencies had multiple locations, resulting in 28 sites. Consistent with prior studies (Skriner et al. 2018; Aarons et al. 2009) each site rather than agency was treated as a distinct organization because of different leadership structures, locations, and staff. Approximately 58% of therapists employed by the 28 organizations participated in the study, resulting in a final sample of 247 therapists. There were no exclusion criteria for participation.
Procedure
Therapists were recruited during a one-time meeting at their agency, during which the research team provided lunch, gave an overview of the study, obtained written informed consent, and collected all measures. Therapists completed questionnaires on-site during work hours without supervisors present to reduce demand characteristics and assure confidentiality. Participants were compensated $50 for participation in the study. Organizational leadership (e.g., clinical director, executive director) reported on organization size. One year later, organizational leadership was contacted to gather data on therapist rates of turnover. All study procedures were approved by the City of Philadelphia and the University of Pennsylvania Institutional Review Boards.
Measures
Predictor Variable
Financial Strain
The InCharge Financial Distress/Financial Well-Being Scale (IFDFW; Prawitz et al. 2006) is an 8-item self-reported measure that evaluates an individual’s perceived financial strain on a continuum. Items are rated on a 1 (No financial distress/highest level of financial well-being) to 10 (Overwhelming financial distress/lowest level of financial well-being) scale. An example item is: “How frequently do you find yourself just getting by financially and living paycheck to paycheck?” See Appendix for all scale items. Total scores represent the average of the eight items. Prior work indicates that internal consistency/reliability of the scale is good (α = 0.96; Prawitz et al. 2006). The IFDFW has national norms, has demonstrated strong internal consistency, and has evidence of criterion validity and factorial validity (Prawitz et al. 2006). Internal consistency in this sample was excellent (α = 0.94).
Moderator Variable
Participation in EBP Training Initiative
Therapists indicated whether they had formally participated in any of the four DBHIDS EBP initiatives; we specifically double-checked with each participant to make sure they understood we were referring to the formal one-year training and ongoing consultation provided through DBHIDS.
Dependent Variable
Turnover
Approximately 1 year following the initial meeting where we gathered data from therapists, we contacted organization leadership, who identified therapists who had left their agencies since the initial meeting. Internal transitions (e.g., promotions to supervisory positions) were not considered turnover events. Reasons for turnover (i.e., voluntary or involuntary) were not obtained.
Control Variables
Therapist Characteristics
Therapists completed a brief demographics questionnaire that assessed age, educational background, job tenure in current organization, part-time or full-time status, and employment status (salaried, independent contractor, or other). Examples of “other” employment status include being a practicum student or an unpaid intern at the agency. Employment status was included given that behavioral health agencies are increasingly reliant on independent contractors (Beidas et al. 2016b).
Organizational Characteristics
Organization size was measured as the number of therapists working in the organization.
Burnout
The Maslach Burnout Inventory Human Services Survey (MBI-HSS; Maslach et al. 1996) is a 22-item measure that assesses emotional exhaustion, depersonalization, and reduced personal accomplishment. Items are rated on a 0 (Never) to 6 (Every day) scale. Higher scores on emotional exhaustion and depersonalization and lower scores on personal accomplishment (reverse scored for the total score) indicate higher levels of burnout. The MBI is the gold standard measure for assessing burnout and has shown satisfactory internal consistency and discriminant and factorial validity (Maslach et al. 2001; Schaufeli et al. 2001; Glass and Mcknight 1996). All three subscales showed acceptable to excellent internal consistency in this sample (α range = 0.76–0.93).
Data Analytic Plan
Given the hierarchical structure of the data (i.e., therapists nested within organizations), study hypotheses were tested using two-level mixed effects logistic regression models (Raudenbush and Bryk 2002) with random intercepts to account for the clustering of therapists within organizations. All models controlled for variables that have been related to therapist turnover in prior studies including: organizational size, therapist employment status (salaried, independent contractor, or other [e.g., unpaid intern]), job tenure, gender, and burnout (emotional exhaustion, depersonalization, and personal accomplishment). Covariates were grand-mean centered to facilitate model interpretation, including financial strain which was centered prior to calculating the interaction term (Enders and Tofighi 2007; Preacher et al. 2006). Missing data were minimal on all control variables (i.e., < 5%) and were imputed using the serial mean. Analyses were run using the TWOLEVEL command in Mplus, Version 7 which incorporates maximum likelihood estimation with robust standard errors (Muthén and Muthén 2012).
Model 1 tested Hypothesis 1, which stated that higher levels of perceived financial strain would predict increased likelihood of therapist turnover, controlling for covariates. Model 2 tested Hypothesis 2, which stated that therapist participation in an EBP training initiative would predict reduced likelihood of therapist turnover, controlling for financial strain and the other covariates. Model 3 tested Hypothesis 3, which stated that therapist participation in an EBP training initiative will moderate the effect of financial strain on turnover such that increased financial strain will not predict increased turnover for therapists who participate in initiatives.
Results
See Table 1 for descriptive statistics for all therapists in the sample. Thirty-nine percent of therapists (n = 97) left their organizations 1 year following the initial data collection meeting. The sample was predominantly female and ethnically diverse. The majority of therapists had master’s degrees, were independent contractors, and on average had worked approximately 3 years at their organization. Forty-seven percent of therapists (n = 114; data missing for four) had participated in an EBP training initiative. Therapists worked an average of 25 paid hours per week (SD = 15.879). The average score on the IFDFW scale for therapists in our sample was 6.32 (SD = 2.11) with higher scores indicating higher perceived financial strain, which indicated that, on average, therapists in this sample had greater financial distress than two-thirds of the U.S. population (derived from national norms, Prawitz et al. 2006).
Table 1.
Therapist characteristics
| Variable | Total N and frequency (%) (N = 247) |
N and frequency (%) of therapists who left agency after 1 year (N = 97) |
N and frequency (%) of therapists who stayed at their agency after 1 year (N = 150) |
|---|---|---|---|
| Gendera | |||
| Male | 51 (20.6%) | 15 (15.5%) | 36 (24.0%) |
| Female | 192 (77.7%) | 81 (83.5%) | 111 (74.0%) |
| Hispanic/Latinoa | |||
| Yes | 52 (21.1%) | 11 (11.3%) | 41 (27.3%) |
| No | 190 (76.9%) | 84 (86.6%) | 106 (70.7%) |
| Ethnicitya | |||
| Asian | 11 (4.5%) | 2 (2.1%) | 9 (6.0%) |
| Black or African-American | 74 (30.0%) | 35 (36.1%) | 39 (26%) |
| White | 101 (40.9%) | 46 (47.4%) | 55 (36.7%) |
| Hispanic/Latino | 40 (16.2%) | 5 (5.2%) | 35 (23.3%) |
| Multiracial | 10 (4.0%) | 5 (5.2%) | 5 (3.3%) |
| Other | 5 (2.0%) | 3 (3.1%) | 2 (1.3%) |
| Academic backgrounda | |||
| Bachelor’s degree | 16 (6.5%) | 9 (9.3%) | 7 (4.7%) |
| Master’s degree | 192 (77.7%) | 81 (83.5%) | 111 (74.0%) |
| Doctoral degree | 34 (13.8%) | 5 (5.2%) | 29 (19.3%) |
| Employment statusa | |||
| Salaried | 51 (20.6%) | 23 (23.7%) | 28 (18.7%) |
| Independent contractor | 167 (67.6%) | 57 (58.8%) | 110 (73.3%) |
| Other (e.g., unpaid intern) | 24 (9.7%) | 16 (16.5%) | 8 (5.3%) |
| Hours worked | |||
| Part time (≤ 29) | 138 (55.9%) | 60 (61.9%) | 78 (52%) |
| Full time (≥ 30) | 109 (44.1%) | 37 (38.1%) | 72 (48%) |
Does not add up to 100% because of missing responses
Table 2 presents results of the mixed effects regression models. Results of Model 1 supported Hypothesis 1; controlling for covariates, increased financial strain was associated with increased logged odds of therapist turnover (B = .111, SE = .055, p = .045, OR 1.12). The expected probability of turnover, denoted ŷ, for a therapist one standard deviation above the mean on perceived financial strain (ŷ = .42) was 1.3 times more than a therapist one standard deviation below the mean (ŷ = .32). This indicates that therapists with greater perceived financial strain were more likely to leave their agency a year later.
Table 2.
Two-level mixed effects logistic regression models predicting therapist turnover
| Predictor | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| B | SE | B | SE | B | SE | |
| Intercept | − .530* | .251 | − .528* | .250 | − .526* | .249 |
| Organization size (# therapists) | − .009 | .017 | − .009 | .016 | − .010 | .016 |
| Independent contractor employee (ref = salaried) | − .855 | .524 | − .865 | .518 | − .911 | .522 |
| Other employee (e.g., intern) (ref = salaried) | .574 | .745 | .573 | .751 | .534 | .720 |
| Full-time employee (ref = part-time) | − .512 | .413 | − .520 | .407 | − .559 | .376 |
| Emotional exhaustion | .012 | .013 | .012 | .013 | .011 | .013 |
| Depersonalization | − .049 | .028 | − .049 | .028 | − .058 | .030 |
| Personal accomplishment | − .038 | .023 | − .039 | .023 | − .039 | .024 |
| Tenure with organization | − .081 | .062 | − .081 | .063 | − .081 | .059 |
| Gender (referent = female) | − .258 | .416 | − .268 | .415 | − .321 | .419 |
| Financial strain (higher score = higher strain) | .110* | .055 | .111* | .055 | .111* | .054 |
| EBP initiative participation | − .094 | .267 | − .065 | .256 | ||
| Financial strain × EBP initiative participation | − .276* | .136 | ||||
N = 247, k = 28
p < .05
Model 2 tested whether therapist participation in an EBP initiative would reduce therapists’ overall likelihood of turnover. Participation in an EBP initiative was unrelated to therapist turnover, controlling for all covariates and therapist financial strain (B = − .094, SE = .267, p = .724, OR .91). Financial strain remained a significant predictor of therapist turnover after controlling for participation in an EBP training initiative (B = .111, SE = .055, p = .045, OR 1.12).
Hypothesis 3 predicted that therapist participation in an EBP initiative would moderate the relationship between financial strain and therapist turnover, such that increased financial strain would not predict increased turnover for therapists who participated in an EBP initiative but would predict increased turnover for therapists who did not participate in an EBP initiative. Results of Model 3 supported Hypothesis 3. Controlling for covariates, this interaction was significant (B = − .276, SE = .136, p = .043; see Fig. 1). Among therapists who had participated in an EBP initiative (n = 115) there was no relationship between financial strain and turnover (B = .006, p = .959, OR 1.01); however, among therapists who had not participated in an EBP initiative (n = 132), increased financial strain was a predictor of increased turnover (B = .199, p = .014, OR 1.22). This also provides partial support for Hypothesis 2, which hypothesized a protective effect of EBP initiative participation on turnover.
Fig. 1.
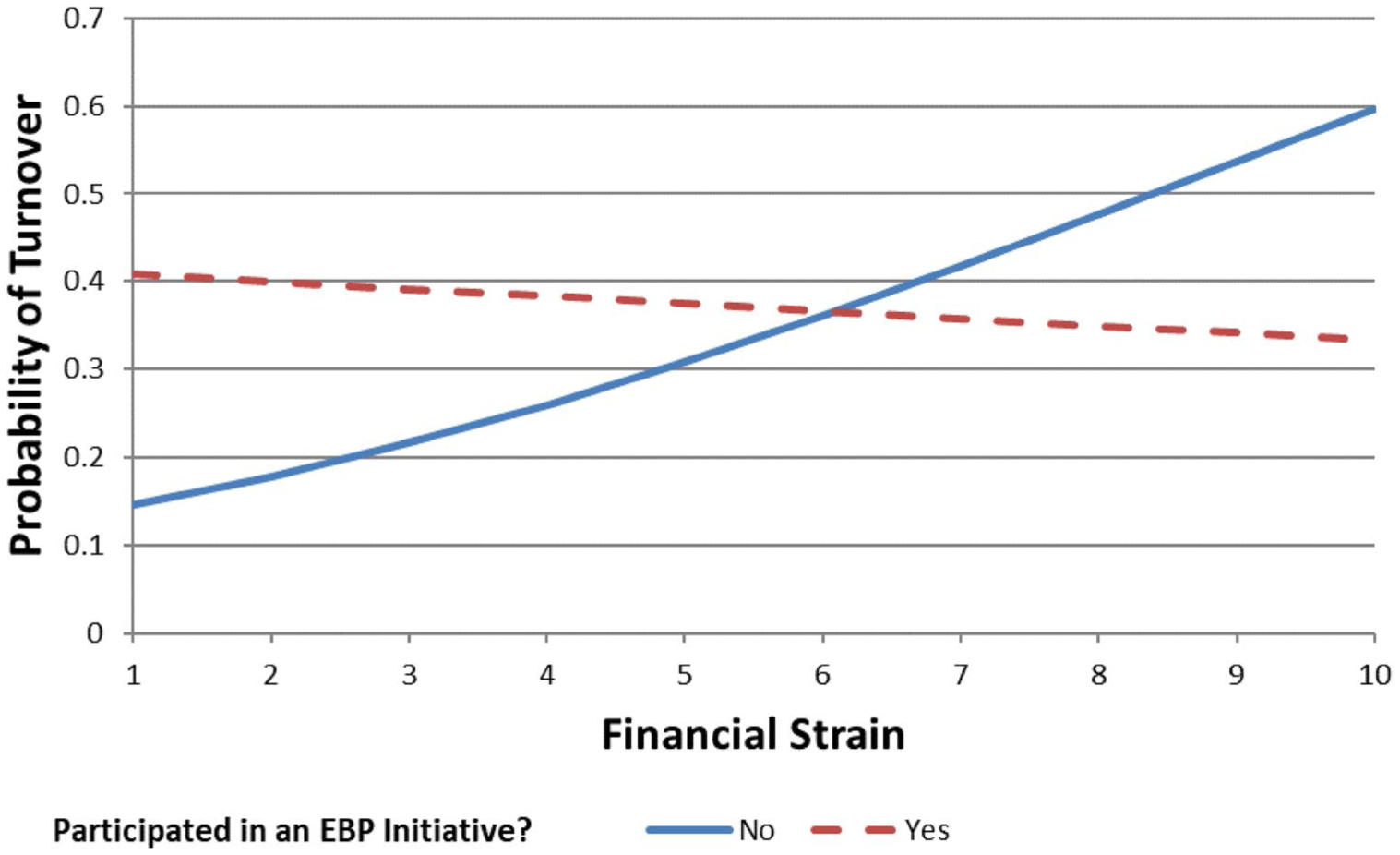
Moderating effect of EBP initiative participation on the relationship between financial strain and probability of turnover. Higher scores indicated higher financial strain. Figure shows that the expected probability of turnover was nearly identical among therapists who had participated in an EBP initiative regardless of whether they experienced low (one standard deviation below the mean) or high (one standard deviation above the mean) financial strain (i.e., ŷ = .39 vs. ŷ = .34, respectively). In contrast, among therapists who did not participate in an EBP initiative, the expected probability of turnover was much higher among those who experienced high financial strain (ŷ = .48) compared to those who experienced low financial strain (ŷ = .27)
Discussion
This study provides insight on the role of financial strain and participation in an EBP training initiative in predicting turnover in a sample of therapists working in an urban publicly-funded mental health system engaged in a large-scale effort to increase the use of EBP. The turnover rate for this sample was 39%, consistent with other studies which have found rates between 30 and 60% (Beidas et al. 2016a; Mor Barak et al. 2001). Further, therapists in this sample had greater financial distress than two-thirds of the U.S. population. Findings highlight that, overall, therapists who perceive greater financial strain are 1.3 times more likely to leave their agency in the following year. However, results further suggest that participating in an EBP training initiative exerted a protective effect on the likelihood of turnover among therapists who are experiencing financial strain. Results suggest that enacting policies to reduce financial strain and encourage therapist participation in EBP training initiatives may reduce turnover.
Our study is the first to quantitatively examine perceived financial strain as a predictor of turnover. Findings are consistent with prior qualitative work suggesting that higher levels of perceived financial strain increased the likelihood of turnover (Beidas et al. 2016a). This finding underscores the importance of attending to factors which affect perceived financial strain, such as wages for staff employed in behavioral health settings. Addressing financial strain within the context of interventions that aim to reduce turnover (e.g., Paris and Hoge 2010) may be a promising avenue for future research. System leaders and payers could take steps at reducing perceived financial strain by increasing the salaries or hourly wages of their employees. Further economic work should estimate the costs of therapists leaving their agency relative to increasing wages for staff to see if wage increases could in fact be cost-effective. However, given the tenuous financial conditions of the behavioral health sector, this may not be a possibility. An alternative may be for behavioral health agencies to implement strategies which aim to decrease administrative financial pressures therapists face. For example, agencies could offer free opportunities for therapists to participate in continuing education (CE) credits for maintenance of licensure in-house, alleviating therapists from having to seek costly CE credits elsewhere.
Results from our third hypothesis indicate that participating in an EBP initiative may reduce the effect of increased perceived financial strain on turnover. The highest level of turnover occurred among therapists who experienced high financial strain and did not participate in an EBP initiative. This finding is consistent with previous studies, which showed that the use of an EBP supports retention of therapists when it is paired with supportive components such as fidelity monitoring (Sheidow et al. 2007; Aarons et al. 2009). We expand upon this work by including financial strain, a phenomenon that was previously understudied, in the model. The EBP training initiatives in Philadelphia emphasized supporting therapists not only through training, but also through expert consultation, ongoing technical assistance, and supervision. These additional components facilitate sustained therapist knowledge and mastery, and increase the number of skills and tools they can use to treat their clients more effectively (Beidas and Kendall 2010). One hypothesis for this finding is that EBP training initiatives may have strengthened therapist connection to one another (e.g., through their cohort of trained therapists and their supervisors) and increased job embeddedness, improving the fit between an employee’s personal values, career goals, and plans for the future and the larger organizational culture and the demands of his or her immediate job (Holtom and Inderrieden 2006).
Another possibility for this finding is that therapists who participated in the EBP training initiatives may have been more willing to bear the brunt of low-wages in order to do the work which brought them into the field to begin with and that aligns well with their values and goals, that is, improving their ability to treat their clients more effectively. We hypothesize that rather than entering a profession to achieve the goal of personal wealth, many therapists enter the behavioral health profession based on personal values of health and well-being for all. In turn, they create goals and strategies to realize these values, such as improving the well-being of individuals with behavioral health disorders. Aligned with image violation theory, or when individual goals are inconsistent with organizational goals, job satisfaction may decrease when therapists feel they do not have the right tools or support to effectively improve their client’s outcomes, and are unable to achieve the values which brought them into the field (Lee et al. 1999; Williams and Beidas 2018b). This, in combination with the low wages and tumultuous financial environments that are prevalent in behavioral health, may send therapists down a decision path to leave their agency (Holt et al. 2007). However, providing therapists with training and support in an EBP may be an antidote to these image violations. To the extent that being trained in an EBP provides therapists the tools and support they need to provide more effective treatment to their clients, thereby satisfying the values and goals which brought them into the profession to begin with, therapists may be more willing to bear the burden of financial strain. Future work should assess these hypotheses through mixed-methods to further understand this moderation finding.
A majority (68%) of our sample reported independent contractor status. Prior preliminary research suggests that ramifications of employing independent contractors include independent contractors feeling less connected to their agency, employment instability, and higher staff turnover, potentially due to the tumultuous financial environment and lack of investment in their training (Beidas et al. 2016b). Interestingly, our sample did not reflect these findings, with independent contractor employees being less likely to leave their agency than salaried employees. One potential reason for this may be that independent contractors were more likely to hold additional jobs at other mental health agencies in Philadelphia compared to (22%, n = 28) salaried employees (8%, n = 4), indicating that independent contractors are more likely to piece together their income from multiple sources. Anecdotally, independent contractors have reported to us that they prefer the contractor status as it gives them more flexibility to choose when they want to see their clients. Further research should explore what incentives encouraged independent contractors in this system to stay at their agencies (Williams and Beidas 2018b).
Our study holds implications for agency and system leaders and policy makers. Specifically, when a system invests in EBP training initiatives they may be receiving a twofold benefit of improving the quality of services being provided and reducing the likelihood of trained therapists leaving their agencies, particularly those experiencing financial strain. To encourage organizations to send their therapists to EBP training initiatives, system leaders could offer incentives to therapists, such as an enhanced rate for therapists who bill for the EBP after being trained in it (Beidas et al. 2016c), or providing a bonus for becoming certified in the model. Further, agencies may also be wise to incentivize their therapist’s participation in EBP initiatives. Agencies could incentivize this by paying for therapist’s time to participate at an enhanced hourly rate, or have agency leadership provide recognition to therapists who participate in initiatives. Importantly, our study indicates that by specifically identifying therapists who perceive high levels of financial strain and encouraging them to participate in an EBP training initiative, agencies may get most “bang for their buck” in their efforts to reduce turnover. The context of Philadelphia is unique, given that the city paid for all components of the EBP initiatives (e.g., trainings, consultations, and other start-up costs). Future system leaders who wish to prioritize EBPs should follow this model, supporting the implementation in both value and dollars (Stewart et al. 2016).
While participating in an EBP training initiative provided a buffering effect for financially strained therapists who may have been on the path toward leaving their agency, it is ultimately not a panacea for low wages and the subsequent strain that therapists and agencies experience. Our sample experienced higher levels of financial strain than the national average, indicating this is a likely problem at the system-level. Behavioral health agency leaders, system leaders, and policy makers must come together to develop sustainable solutions to address the financial strain that therapists are facing, and work to build a more stable workforce that has the capacity to provide high quality services to the most vulnerable populations.
Some study limitations should be noted. First, results are specific to one publicly-funded mental health system, albeit a large system serving over 100,000 consumers annually, potentially reducing the external validity and generalizability. Second, the independent variables are based on therapists’ self-report, which can be limited by recall and social desirability biases. However, characteristics of our data suggest the self-reports were not biased. For example, scores on the IFDFW, the primary independent variable of interest, were normally distributed with a good range of responses, suggesting that therapists were willing to report both high and low levels of financial strain. Third, selection of both individuals and organizations for participation in the city EBP training initiatives was not randomized. Therapist self-selection into the trainings could have created selection issues, that is, certain therapists (e.g., highly motivated, have other sources of support to sustain their income during training if they are not reimbursed for that time) may have been more likely to participate in the initiative than other therapists. Fourth, temporality of measurement is an issue. Financial strain was measured 1 year prior to turnover; whereas therapists may have participated in an EBP initiative at any point between 2007 and 2015. Finally, our study cannot identify the mechanisms underpinning the observed moderation effect. Future research should aim to identify which elements of EBP training initiatives are most salient in the relationship between financial strain and turnover.
This study also had several notable strengths. We collected prospective data on turnover 1 year following the initial data collection meeting, allowing us to gain a better understanding of the actual effect of financial strain on turnover. Additionally, we had a relatively large sample size (N = 247), reducing our margin of error and increasing the accuracy of our model. Future work in this area should identify mutable therapist- and organizational-level characteristics of therapists who report the highest levels of financial strain and develop solutions that can attenuate those characteristics. Additionally, future work should expand the fields understanding of financial strain and its effect on outcomes at various levels both quantitatively and qualitatively. Finally, interventions to reduce therapist turnover should incorporate strategies to diminish the effect of perceived financial strain and incentivize participation in EBP trainings.
Conclusion
Given that between 30 and 60% of therapist’s turnover annually, identifying mutable antecedents of therapist turnover is a critical task. Our study demonstrated that financial strain predicted increased likelihood of therapist turnover, but only among therapists who had not participated in system-funded EBP training initiatives. When therapists feel they are able to more effectively treat their clients using EBP to achieve better clinical outcomes, they may be more willing to bear the brunt of low-wages to do the work that brought them into the field to begin with (i.e., improving well-being of families). At a system level, incentivizing participation in EBP training initiatives through financial rewards such as a bonus or an enhanced rate for being certified in the model are both potential intervention points in reducing turnover in therapists experiencing high levels of perceived financial strain.
Acknowledgements
We are especially grateful for the support that the Department of Behavioral Health and Intellectual disAbility Services has provided for this project and for the Evidence Based Practice and Innovation (EPIC) group. We would also like to thank the following experts who provided their consultation on this project: Dr. Steven Marcus and Dr. David Mandell.
Funding Funding for this research project was supported by NIMH K23 MH099179 (Beidas). Additionally, this paper was supported by the Agency for Healthcare Research and Quality under Grant Award T32 HS000084 (Adams; PI: Kathleen Cagney, PhD). Its contents are solely the responsibility of the author(s) and do not necessarily represent the official views of the AHRQ.
Appendix. InCharge Financial Distress/Financial Well‑Being Scale items

Footnotes
Earlier versions of this paper were presented at the annual meeting for the Association of Behavioral and Cognitive Therapies (ABCT) in October, 2016 and the biannual Society for Implementation Research Collaboration (SIRC) Conference in September, 2017.
Conflict of interest Dr. Beidas receives royalties from Oxford University Press. All other authors have no conflicts of interest to report.
Ethical Approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent Informed consent was obtained from all individual participants included in the study.
References
- Aarons GA, Sommerfeld DH, Hecht DB, Silovsky JF, & Chaffin MJ (2009). The impact of evidence-based practice implementation and fidelity monitoring on staff turnover: Evidence for a protective effect. Journal of Consulting and Clinical Psychology, 77(2), 270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Abrahams IA, Ali O, Davidson L, Evans AC, King JK, Poplawski P, White WL (2013). Philadelphia behavioral health services transformation: Practice guidelines for recovery and resilience oriented treatment. Philadelphia, Pennsylvania: Philadelphia Department of Behavioral Health and Intellectual disAbility Services; Retrieved from https://www.bhten.com/sites/default/files/PracticeGuidelines.pdf. [Google Scholar]
- Aldana SG, & Liljenquist W (1998). Validity and reliability of a financial strain survey. Journal of Financial Counseling and Planning, 9(2), 11. [Google Scholar]
- Babbar S, Adams DR, Becker-Haimes EM, Skriner LC, Kratz HE, Cliggitt L,… & Beidas RS (2018). Therapist turnover and client non-attendance. Children and Youth Services Review, 93, 12–16. [Google Scholar]
- Bagwell DC, & Kim J (2003). Financial stress, health status, and absenteeism in credit counseling clients. Journal of Consumer Education, 20, 50–58. [Google Scholar]
- Beidas RS, Aarons G, Barg F, Evans A, Hadley T, Hoagwood K,… & Mandell DS (2013). Policy to implementation: Evidence-based practice in community mental health–study protocol. Implementation Science, 8(1), 38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beidas RS, Adams DR, Kratz HE, Jackson K, Berkowitz S, Zinny A,… & Evans A Jr (2016c). Lessons learned while building a trauma-informed public behavioral health system in the City of Philadelphia. Evaluation and Program Planning, 59, 21–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beidas RS, & Kendall PC (2010). Training therapists in evidence-based practice: A critical review of studies from a systems-contextual perspective. Clinical Psychology: Science and Practice, 17(1), 1–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beidas RS, Marcus S, Wolk CB, Powell B, Aarons GA, Evans AC,… & Babbar S (2016a). A prospective examination of therapist and supervisor turnover within the context of implementation of evidence-based practices in a publicly-funded mental health system. Administration and Policy in Mental Health and Mental Health Services Research, 43(5), 640–649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beidas RS, Stewart RE, Benjamin Wolk C, Adams DR, Marcus SC, Evans AC Jr,… & Rubin R (2016b). Independent contractors in public mental health clinics: Implications for use of evidence-based practices. Psychiatric Services, 67(7), 710–717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bingley P, & Westergaard-Nielsen N (2004). Personnel policy and profit. Journal of Business Research, 57(5), 557–563. [Google Scholar]
- Committee on Developing Evidence-Based Standards for Psychosocial Interventions for Mental Disorders. (2015). Quality measurement In England MJ, Butler AS, & Gonzalez ML (Eds.), Psychosocial interventions for mental and substance use disorders: A framework for establishing evidence-based standards (pp. 1–20). Washington, DC: National Academies Press. [PubMed] [Google Scholar]
- Droege SB, & Hoobler JM (2003). Employee turnover and tacit knowledge diffusion: A network perspective. Journal of Managerial Issues, 15, 50–64. [Google Scholar]
- Enders CK, & Tofighi D (2007). Centering predictor variables in cross-sectional multilevel models: A new look at an old issue. Psychological Methods, 12(2), 121. [DOI] [PubMed] [Google Scholar]
- Evans S, Huxley P, Gately C, Webber M, Mears A, Pajak S,… & Katona C (2006). Mental health, burnout and job satisfaction among mental health social workers in England and Wales. The British Journal of Psychiatry, 188(1), 75–80. [DOI] [PubMed] [Google Scholar]
- Fals-Stewart W, Logsdon T, & Birchler GR (2004). Diffusion of an empirically supported treatment for substance abuse: An organizational autopsy of technology transfer success and failure. Clinical Psychology: Science and Practice, 11(2), 177–182. [Google Scholar]
- Garman ET, Leech IE, & Grable JE (1996). The negative impact of employee poor personal financial behaviors on employers. Financial Counseling and Planning, 7, 157–168. [Google Scholar]
- Glass DC, & McKnight JD (1996). Perceived control, depressive symptomatology, and professional burnout: A review of the evidence. Psychology and Health, 11(1), 23–48. [Google Scholar]
- Golberstein E, & Busch SH (2017). Mental health insurance parity and provider wages. The Journal of Mental Health Policy and Economics, 20(2), 75–82. [PubMed] [Google Scholar]
- Hoagwood KE, Atkins M, Horwitz S, Kutash K, Olin SS, Burns B,… & Kelleher KJ (2017). A response to proposed budget cuts affecting children’s mental health: Protecting policies and programs that promote collective efficacy. Psychiatric Services, 69(3), 268–273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holt DT, Rehg MT, Lin JH, & Miller J (2007). An application of the unfolding model to explain turnover in a sample of military officers. Human Resource Management, 46(1), 35–49. [Google Scholar]
- Holtom BC, & Inderrieden EJ (2006). Integrating the unfolding model and job embeddedness model to better understand voluntary turnover. Journal of Managerial Issues, 18(4), 435–452. [Google Scholar]
- Jacobson BH, Aldana SG, Goetzel RZ, Vardell KD, Adams TB, & Pietras RJ (1996). The relationship between perceived stress and self-reported illness-related absenteeism. American Journal of Health Promotion, 11(1), 54–61. [DOI] [PubMed] [Google Scholar]
- Joo S, & Garman ET (1998). The relationship between personal financial wellness and employee productivity: A conceptual model. Personal Finances and Worker Productivity, 2(2), 162–171. [Google Scholar]
- Lee TW, Mitchell TR, Holtom BC, McDaneil LS, & Hill JW (1999). The unfolding model of voluntary turnover: A replication and extension. Academy of Management Journal, 42(4), 450–462. [Google Scholar]
- Maslach C, Jackson SE, & Leiter MP (1996). Maslach burnout inventory manual In Zalaquett CP & Wood RJ (Eds.), Evaluating stress: A book of resources (pp. 191–218). Palo Alto, CA: Consulting Psychologists Press. [Google Scholar]
- Maslach C, Schaufeli WB, & Leiter MP (2001). Job burnout. Annual Review of Psychology, 52(1), 397–422. [DOI] [PubMed] [Google Scholar]
- Mor Barak ME, Nissly JA, & Levin A (2001). Antecedents to retention and turnover among child welfare, social work, and other human service employees: What can we learn from past research? A review and meta-analysis. Social Service Review, 75(4), 625–661. [Google Scholar]
- Muthén LK, & Muthén BO (2012). Mplus user’s guide (7th ed). Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Ouellette RR, Pellecchia M, Beidas RS, Wideman R, Xie M, & Mandell DS (2018). Boon or burden: The effect of implementing evidence-based practices on teachers’ emotional exhaustion. Administration and Policy in Mental Health and Mental Health Services Research, 46(1), 62–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paris M, & Hoge MA (2010). Burnout in the mental health work-force: A review. The Journal of Behavioral Health Services & Research, 37(4), 519–528. [DOI] [PubMed] [Google Scholar]
- Powell BJ, Beidas RS, Rubin RM, Stewart RE, Wolk CB, Matlin SL,… & Mandell DS (2016). Applying the policy ecology framework to Philadelphia’s behavioral health transformation efforts. Administration and Policy in Mental Health and Mental Health Services Research, 43(6), 909–926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prawitz A, Garman ET, Sorhaindo B, O’Neill B, Kim J, & Drentea P (2006). InCharge financial distress/financial well-being scale: Development, administration, and score interpretation. Financial Counseling and Planning, 17, 34–50. [Google Scholar]
- Preacher KJ, Curran PJ, & Bauer DJ (2006). Computational tools for probing interactions in multiple linear regression, multilevel modeling, and latent curve analysis. Journal of Educational and Behavioral Statistics, 31(4), 437–448. [Google Scholar]
- Raudenbush SW, & Bryk AS (2002). Hierarchical linear models: Applications and data analysis (2nd ed). Thousand Oaks, CA: Sage Publications. [Google Scholar]
- Rollins AL, Salyers MP, Tsai J, & Lydick JM (2010). Staff turnover in statewide implementation of ACT: Relationship with ACT fidelity and other team characteristics. Administration and Policy in Mental Health and Mental Health Services Research, 37(5), 417–426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schaufeli WB, Bakker AB, Hoogduin K, Schaap C, & Kladler A (2001). On the clinical validity of the Maslach burnout inventory and the burnout measure. Psychology & Health, 16(5), 565–582. [DOI] [PubMed] [Google Scholar]
- Sheidow AJ, Schoenwald SK, Wagner HR, Allred CA, & Burns BJ (2007). Predictors of workforce turnover in a trans-ported treatment program. Administration and Policy in Mental Health and Mental Health Services Research, 34(1), 45–56. [DOI] [PubMed] [Google Scholar]
- Skriner LC, Wolk CB, Stewart RE, Adams DR, Rubin RM, Evans AC, et al. (2018). Therapist and organizational factors associated with participation in evidence-based practice initiatives in a large urban publicly-funded mental health system. The Journal of Behavioral Health Services & Research, 45(2), 174–186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stewart RE, Adams DR, Mandell DS, Hadley TR, Evans AC, Rubin R,… & Beidas RS (2016). The perfect storm: Collision of the business of mental health and the implementation of evidence-based practices. Psychiatric Services, 67(2), 159–161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams NJ, & Beidas RS (2018a). Annual research review: The state of implementation science in child psychology and psychiatry: A review and suggestions to advance the field. Journal of Child Psychology and Psychiatry, 60(4), 430–450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams NJ, & Beidas RS (2018b). Navigating the storm: How proficient organizational culture promotes clinician retention in the shift to evidence-based practice. PLoS ONE, 13(12), e0209745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woltmann EM, Whitley R, McHugo GJ, Brunette M, Torrey WC, Coots L,… & Drake RE (2008). The role of staff turnover in the implementation of evidence-based practices in mental health care. Psychiatric Services, 59(7), 732–737. [DOI] [PubMed] [Google Scholar]