

Abstract
Objective:
This study aimed to evaluate blood volatile organic compound (VOC) levels as biomarkers of occupational jet propulsion fuel 8 (JP-8) exposure while controlling for smoking.
Methods:
Among 69 Air Force personnel, post-shift blood samples were analyzed for components of JP-8, including ethylbenzene, toluene, o-xylene, and m/p-xylene, and for the smoking biomarker, 2,5-dimethylfuran. JP-8 exposure was characterized based on self-report and measured work shift levels of total hydrocarbons in personal air. Multivariate regression was used to evaluate the relationship between JP-8 exposure and post-shift blood VOCs while controlling for potential confounding from smoking.
Results:
Blood VOC concentrations were higher among US Air Force personnel who reported JP-8 exposure and work shift smoking. Breathing zone total hydrocarbons was a significant predictor of VOC blood levels, after controlling for smoking.
Conclusions:
These findings support the use of blood VOCs as a biomarker of occupational JP-8 exposure.
Jet propulsion fuel 8 (JP-8) is a complex, kerosene-based chemical mixture composed of more than 200 aliphatic and aromatic hydrocarbons.1 More than 5 billion gallons of JP-8 are used every year by US and North Atlantic Treaty Organization militaries for fueling aircraft, ground vehicles, and support equipment, making it potentially the single largest source of chemical exposure for military personnel. Personal exposure assessment has proved challenging because of the complex composition of JP-8, and has focused on using surrogate measures of exposure including self-reported exposure2,3 and biomarkers of exposure.2–12 These studies have shown a wide range in the levels of exposure to JP-8 among US Air Force (USAF) personnel, with the highest occurring among those who report routine occupational exposure to jet fuel.
Self-reported exposure to JP-8 was found to be associated with total hydrocarbons (THCs) in personal breathing zone air samples.2,3 Similarly, previous studies have demonstrated that THCs in personal air samples were associated with other biomarkers of JP-8 exposure, including levels of volatile organic compounds (VOCs) in exhaled breath4,7,9 and 1- and 2-napthols in urine.6,9–12 Although these exposure assessment methods are noninvasive, certain methods only monitor a single route of exposure, and differences among individuals and dynamic environmental factors only permit approximating body burden of VOCs and their metabolites.
The National Health and Nutrition Examination Survey monitors levels of VOCs in blood collected from a representative sample of the US population.13,14 Measuring VOC exposure levels in blood is important because it provides an estimate of total absorbed dose from multiple routes of exposure (ie, dermal, inhalation) and a biologically relevant measure of VOCs that potentially can reach target organs such as the brain, liver, and kidneys.13 Most half-lives for VOCs in blood are bi-phasic and on the time course of hours; however, half-life increases in repeated exposure scenarios such as occupational exposure.15 To date, no studies have characterized blood VOCs in USAF personnel with occupational exposure to jet fuel or assessed their relationship with personal measures of JP-8 exposure (eg, THC in personal air samples).
Certain VOCs that make up fuel such as JP-8 are also abundant in cigarette smoke,14,16 gasoline,17 and other organic solvents,18 which also can affect levels of VOCs in blood. In a US Department of Defense health behavior study, approximately one third of US service members reported any cigarette use in the last month.19 In many of the studies examining USAF personnel JP-8 exposure, smoking also has been significantly associated with measured levels of JP-8 constituents in personal air2 and urine biomarkers,6,9–12 confounding the association between JP-8 exposure and blood VOC levels in active duty military personnel exposed to JP-8.
The overall goal of this study was to evaluate VOCs in blood as a biomarker for characterizing exposure to JP-8. Specifically, the objectives were to characterize VOCs in blood among a population of USAF personnel exposed to JP-8, and evaluate self-reported work shift JP-8 exposure and measured personal exposure to THC as predictors of VOCs in blood, while for controlling for the effect of smoking on VOC levels in blood.
METHODS
We recruited 74 active duty personnel who served at least 6 months in the USAF from three bases according to their Air Force Specialty Code and current job tasks (ie, administrative, aircraft structural maintenance, fuel systems maintenance) such that some participants were expected to have higher exposure to JP-8 and other participants were expected to have lower exposure to JP-8. Persons with a self-reported history of loss of consciousness for more than 20 minutes or known neurological or psychological disorder(s) were excluded from the study. The parent study included a 6-day protocol designed to assess JP-8 exposure and central nervous system functioning in active duty USAF personnel.20 Blood samples were only collected at the end of shift on day 5 (Thursday) of the week-long sampling investigation and were available for 69 of the 74 participants. Accordingly, this investigation focuses on the 69 workers who provided a blood sample on day 5. The study protocol was approved by institutional review boards at the US Army Research Institute of Environmental Medicine, USAF Research Laboratory at Wright Patterson Air Force Base and Boston University, and was in compliance with human subjects review procedure at the Centers for Disease Control and Prevention. Written informed consent was obtained from all participants.
Personal Air Samples
Personal air samples were collected and extracted in accordance with National Institute for Occupational Safety and Health Method 1550 (Cincinnati, OH) for THC.21 Methods for personal air sampling and laboratory analysis are described in detail by Merchant-Borna et al2 and Smith et al.3 In brief, participants wore a battery-operated personal air sampling pump (Casella Apex Pro IS; Casella USA, Amherst, NH) that was attached to a two-section (100/50 mg) coconut shell charcoal tube (Anasorb; SKC Inc, Eight Four, PA) clipped to the lapel of each subject near their breathing zone (flow rate = 0.2 L/min). The personal air-sampling pump was turned off and sealed during breaks from job tasks when the participant left the work area (eg, during lunch and cigarette breaks), and when participants were required to put on respirators to perform certain job tasks. Samples were analyzed for THC at the Organic Chemistry Analytical Laboratory (Harvard School of Public Health, Boston, MA) using gas chromatography with flame ionization detection.21 THC concentrations determined to be below the limit of detection (LOD), calculated as three times the standard deviation of the field blanks, and were replaced with a value of half the LOD. Air concentrations of THC are reported as 8-hour time-weighted averages (TWAs) in mg/m3 to account for difference in work shift length.
A data logger (HOBO; Onset Computer Corporation, Bourne, MA) was attached to each worker to obtain air temperature and relative humidity measurements in 15-minute intervals through the duration of each work shift. Air temperature and relative humidity measurements were averaged across an 8-hour work shift.
Blood VOCs
After the same work shift in which air samples were collected, a trained phlebotomist obtained a blood sample (20 mL total or less) from each worker. Samples were collected in specially prepared BD Vacutainer tubes (Becton, Dickinson and Company, Franklin Lakes, NJ) and sent to the Centers for Disease Control and Prevention laboratory for analysis. Using automated solid-phase microextraction coupled with capillary gas chromatography and quadrupole mass spectrometry, blood samples were analyzed for trace level amounts of the following 11 VOCs: n-hexane, n-heptane, n-octane, benzene, 1,4-dicholorobenzene, ethylbenzene, methyl tert-butyl ether, styrene, toluene, o-xylene, and m/p-xylene.17,22 Blood samples were also analyzed for 2,5-dimethylfuran, a highly specific combustion biomarker of cigarette smoke exposure for daily smokers or nonsmokers exposed to environmental tobacco smoke, using the same method.14,23 Concentrations of blood analytes are reported in μg/L.
Questionnaires
Participants completed a baseline questionnaire providing information about demographics and smoking, as well as occupational, military, and health history. Before starting the work shift, participants completed a brief questionnaire asking about chemical exposures from the previous evening and the morning. The pre-shift survey asked “Since we last saw you have you been to the gas station and filled up your car (self-service)?” (yes/no).
At the end of the work shift, participants completed another brief questionnaire that included a section for participants whose “job involved direct exposure to JP-8 during the work shift.” If participants completed this section, this was considered self-reported work shift JP-8 exposure. The post-shift questionnaire also asked about contact with other solvents and chemicals, use of protective equipment, and tobacco use during the work shift. On this survey, participants were asked to report whether they had worked with gasoline, cutting or lubricating oils, coolants or anti-freeze, degreasers or other cleaners, organic solvents, mineral spirits, and/or epoxy or adhesives (yes/no). The questionnaire also asked, “How many cigarettes have you had during today’s work shift?” Response options included “none,” “quarter-pack,” “half-pack,” “1 pack,” “1+ to 2 packs,” and “2+ packs.” Because of the lack of diversity in responses and the small number who smoked a half pack or more, we lacked statistical power for an analysis of the influence of fractional pack. Of the 23 persons who reported smoking during their work shift, 20 indicated that they had smoked a quarter-pack and three indicated they had smoked a half-pack of cigarettes during the work shift. Responses were dichotomized according to yes/no responses for smoking during the work shift for the data analysis.
Data Analysis
Statistical analyses focused on five VOCs that were detected above the LOD in at least 50% of the blood samples for both self-reported exposure groups: 2,5-dimethylfuran, ethylbenzene, toluene, o-xylene, and m/p-xylene. Blood VOC concentrations below the analytical LOD were replaced with a calculated value of the LOD/SQRT(2). Distribution of personal air and blood concentrations were right-skewed, so the data were transformed with the natural log function before statistical analyses. THCs in personal air and VOCs in blood were analyzed using descriptive statistics, and t test compared mean concentrations between workers who reported JP-8 exposure and those who reported no exposure. Blood VOCs also were compared between USAF personnel who smoked during the work shift and those who did not using the same method.
Air concentrations were natural log-transformed to reduce skewness for the correlation analysis and blood concentrations were natural log-transformed for both correlation and regression analyses. Pearson correlations were used to estimate the strength of the relationship between THC concentrations in air and VOC concentrations in blood. Multiple linear regression models examined the association between blood VOC levels and two surrogate measures of JP-8 exposure: categorical self-reported work shift jet fuel exposure (yes/no) and 8-hour TWA THC (mg/m3). To control for cigarette smoking, two variables were considered in separate models: categorical self-reported cigarette smoking during the work shift (yes/no) and 2,5-dimethylfuran in blood (μg/L). USAF base and relative humidity were included as covariates in all models. A model was fit for each of the VOCs measured in blood.
Mean air temperature, self-service at a gas station, age, and body mass index of participant were also considered as possible covariates. These covariates were not significant predictors of blood VOCs in either regression model and were not included in the final models. We considered conducting a post-hoc analysis to include exposure to other chemicals endorsed on the post-shift survey as possible covariates in our regression models; however, the sample size was small for those reporting the additional exposures (n = 5 or less), and therefore not performed. All statistical analyses were conducted using SAS statistical software version 9.2 (SAS Institute, Cary, NC).
RESULTS
Table 1 shows demographics for the 69 study participants. On average, the USAF personnel participating in this study were 25.3 years old and had spent 5.3 years in the USAF. The majority of participants were white males in the lower enlisted ranks. Significantly, more men than women reported work shift JP-8 exposure. Significantly, more JP-8 exposed individuals reported smoking during the work shift (χ2 = 5.71 (1 df), P = 0.02). Work shift exposure to JP-8 did not differ by other demographic factors.
TABLE 1.
Demographics of Participating USAF Personnel Tested for Volatile Organic Compounds in Blood (n = 69)
| Continuous Variables | Mean (Standard Deviation) | Range |
|---|---|---|
| Age, yrs | 25.3 (6.0) | 18.6–43.0 |
| Body mass index | 26.1 (3.4) | 17.8–34.4 |
| Years active USAF service | 5.31 (5.2) | 0.5–20.0 |
| Categorical variables | No. | (%) |
| Cigarette(s) smoked during shift | ||
| Yes | 23 | (33.3) |
| No | 46 | (66.7) |
| Day 5 work shift jet fuel exposure | ||
| Yes | 37 | (53.6) |
| No | 32 | (46.4) |
| USAF base | ||
| Base A | 20 | (29.0) |
| Base B | 17 | (24.6) |
| Base C | 32 | (46.4) |
| Rank | ||
| Airmen (lower enlisted ranks) | 45 | (65.2) |
| Non-commissioned officers (higher enlisted ranks) | 24 | (34.8) |
| Sex | ||
| Men | 58 | (84.1) |
| Women | 11 | (15.9) |
| Ethnicity | ||
| White | 49 | (71.0) |
| Non-white | 20 | (29.0) |
USAF, US Air Force.
Table 2 shows post-shift VOC concentrations in blood by self-reported JP-8 exposure and shift cigarette smoking. 2,5-dime-thylfuran, a biomarker for cigarette smoking, was detected in 91% of the samples for persons who reported smoking during the work shift. The geometric mean (GM) concentrations of 2,5-dimethylfuran (P < 0.0001), toluene (P = 0.0001), o-xylene (P = 0.005), and m/p-xylene (P = 0.0006) in blood were significantly higher among participants who reported smoking during the work shift. Similarly, the GM concentrations of toluene (P = 0.003), o-xylene (P = 0.0003), and m/p-xylene (P < 0.0001) in blood were significantly higher among participants who reported exposure to JP-8.
TABLE 2.
VOC Blood Concentrations for Sampled US Air Force Personnel (n=69)
| Cigarette(s) Smoked During Shift | Day 5 Work Shift JP-8 Exposure | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes (n = 23) | No (n = 46) | Yes (n = 37) | No(n = 32) | ||||||||||
| Analyte (μg/L) | LOD | % Detect | GM (GSD) | Range | % Detect | GM (GSD) | Range | % Detect | GM (GSD) | Range | % Detect | GM (GSD) | Range |
| 2,5-dimethylfuran | 0.0112 | 91 | 0.04 (2.6) | <LOD-0.2 | 7 | 0.01 (1.6) | <LOD-0.06 | 46 | 0.02 (2.8) | <LOD-0.26 | 22 | 0.01 (2.5) | <LOD-0.15 |
| Octane | 0.1 | 30 | 0.11 (2.1) | <LOD-0.55 | 11 | 0.08 (1.5) | <LOD-0.44 | 30 | 0.10 (2.0) | <LOD-0.55 | 3 | 0.10(1.1) | <LOD-0.15 |
| Isopropylbenzene | 0.04 | 30 | 0.04 (1.8) | <LOD-0.22 | 11 | 0.03 (1.5) | <LOD-0.13 | 30 | 0.04 (1.8) | <LOD-0.22 | 3 | 0.03(1.2) | <LOD-0.08 |
| Benzene | 0.024 | 96 | 0.11 (2.1) | <LOD-0.41 | 22 | 0.02(1.9) | <LOD-0.12 | 65 | 0.05 (2.7) | <LOD-0.41 | 25 | 0.03 (2.3) | <LOD-0.25 |
| Ethylbenzene | 0.024 | 96 | 0.19 (3.8) | <LOD-1.65 | 70 | 0.11 (5.1) | <LOD-1.81 | 86 | 0.17 (4.8) | <LOD-1.81 | 69 | 0.10 (4.4) | <LOD-1.21 |
| Toluene | 0.025 | 96 | 0.33 (2.6) | 0.02–1.15 | 91 | 0.09 (3.6) | <LOD-2.76 | 97 | 0.22 (3.4) | <LOD-2.76 | 88 | 0.09 (3.4) | <LOD-0.68 |
| o-xylene | 0.024 | 96 | 0.11 (3.0) | <LOD-1.16 | 80 | 0.05 (2.7) | <LOD-0.63 | 92 | 0.10 (3.4) | <LOD-1.16 | 78 | 0.04 (2.0) | <LOD-0.30 |
| m-/p-xylene | 0.0335 | 96 | 0.35 (3.0) | 0.02–3.1 | 94 | 0.13 (3.0) | <LOD-1.62 | 100 | 0.30 (3.3) | 0.05–3.11 | 88 | 0.10 (2.4) | <LOD-0.80 |
GM, geometric mean; GSD, geometric standard deviation; JP-8, jet propulsion fuel 8; LOD, limit of detection; ND, not detected; VOC, volatile organic compounds.
Concentrations of THC in personal air samples were significantly higher among participants who self-reported jet fuel exposure (GM = 4.40 mg/m3) than among those who did not (GM = 0.46 mg/m3) (P < 0.0001). In this sample of workers, personal air THC concentrations were strongly correlated with blood levels of o-xylene (r = 0.7) and m/p-xylene (r = 0.7), moderately correlated with blood concentrations of toluene (r = 0.5), and weakly correlated with ethylbenzene (r = 0.3) (Fig. 1). When participants smoked, they removed their personal air-sampling pumps. Consequently, the correlations between 8-hour TWA THC levels and blood levels of 2,5-dimethylfuran were negligible (r = 0.2).
FIGURE 1.
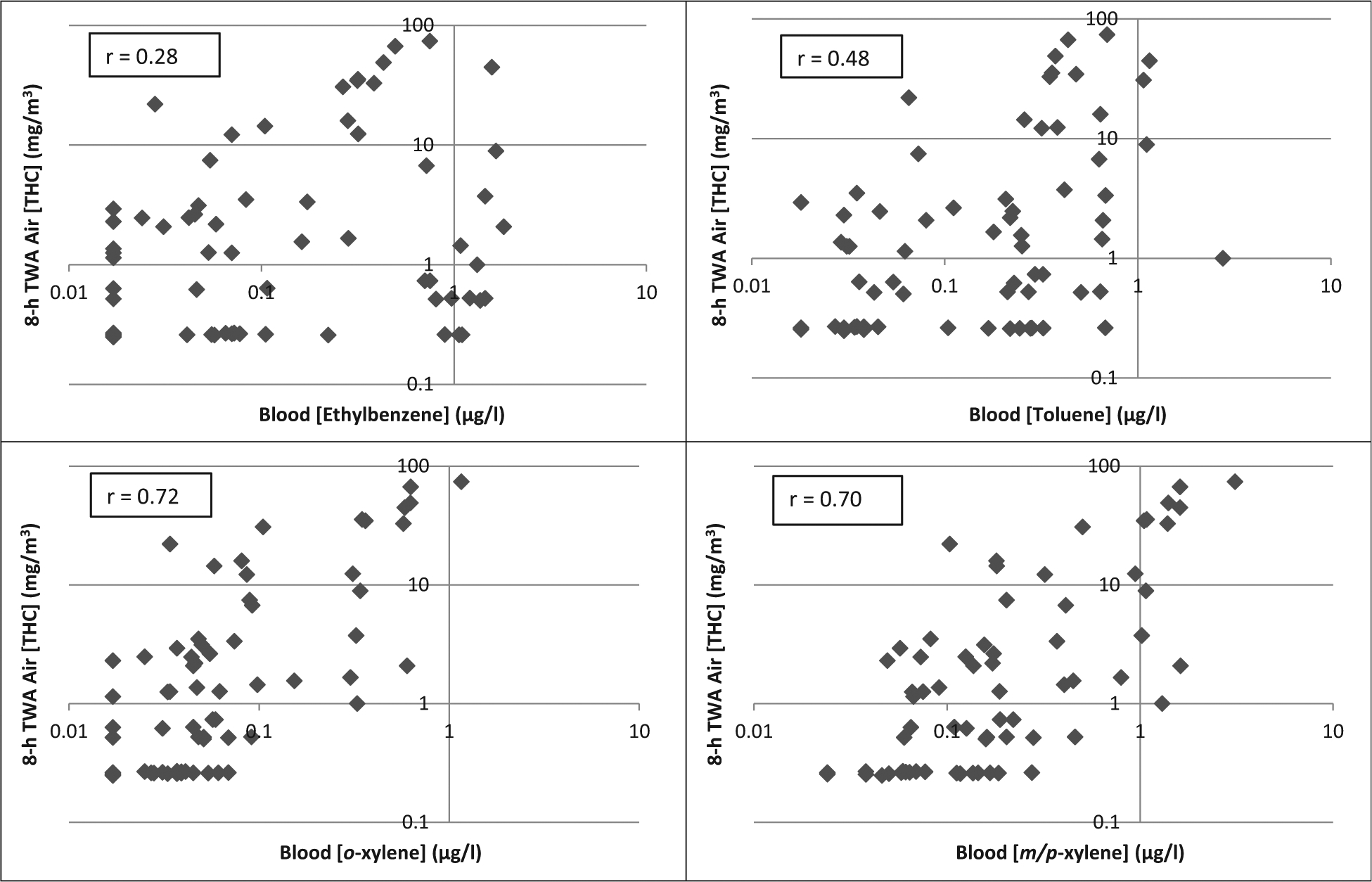
Correlation on log-scale between concentrations of personal air total hydrocarbons and blood volatile organic compounds in sampled US Air Force personnel (n = 69).
Definitions: r = Pearson correlation coefficient; THC = total hydrocarbons; TWA = time-weighted average.
Table 3 presents regression models evaluating predictors of ethylbenzene, toluene, o-xylene, and m/p-xylene in blood. Model 1 examined self-reported work shift exposure to JP-8 as a predictor of the individual blood VOCs, while controlling for self-reported shift cigarette smoking, USAF base (Base A [reference], Base B, or Base C), and mean relative humidity. Work shift jet fuel exposure was a significant predictor for o-xylene and m/p-xylene in blood. There was a positive association between work shift JP-8 exposure and ethylbenzene and toluene, but the association did not reach statistical significance. Smoking during the shift was a significant predictor for all analyzed blood VOCs, and participants at USAF Base B had significantly higher blood VOC concentrations compared with participants from the other USAF bases (Table 3, Model 1).
TABLE 3.
Models* Evaluating Predictors of VOC Blood Levels in Sampled USAF Personnel (n = 69)
| Ethylbenzene (μg/L)† | Toluene (μg/L)† | o-xylene (μg/L)† | m-/p-xylene (μg/L)† | |||||
|---|---|---|---|---|---|---|---|---|
| Model/Variables | β (SE) | P Value | β (SE) | P Value | β (SE) | P Value | β (SE) | P Value |
| Model 1 | ||||||||
| Intercept | −4.28 (0.42) | <0.0001 | −3.83 (0.49) | <0.0001 | −5.18 (0.41) | <0.0001 | −4.40 (0.42) | <0.0001 |
| JP-8 exposure (yes/no) | 0.31 (0.22) | 0.16 | 0.43 (0.26) | 0.10 | 0.52 (0.22) | 0.02 | 0.58 (0.22) | 0.01 |
| Shift cigarette smoking (yes/no) | 0.43 (0.21) | 0.05 | 1.13 (0.25) | <0.0001 | 0.48 (0.21) | 0.03 | 0.73 (0.21) | 0.001 |
| USAF base A | Ref | Ref | Ref | Ref | ||||
| USAF base B | 3.44 (0.26) | <0.0001 | 1.65 (0.31) | <0.0001 | 1.45 (0.25) | <0.0001 | 1.59 (0.26) | <0.0001 |
| USAF base C | −0.05 (0.58) | 0.93 | −0.97 (0.68) | 0.16 | −0.41 (0.57) | 0.47 | −1.04 (0.59) | 0.08 |
| Mean relative humidity | 0.03 (0.02) | 0.09 | 0.03 (0.02) | 0.09 | 0.04 (0.02) | 0.006 | 0.05 (0.02) | 0.001 |
| Summary Adjusted R2 | 0.74 | 0.50 | 0.5/ | 0.55 | ||||
| Model 2 | ||||||||
| Intercept | −3.57 (0.37 | <0.0001 | −3.24 (0.45) | <0.0001 | −4.26 (0.34) | <0.0001 | −3.54 (0.38) | <0.0001 |
| 8-h TWA THC (mg/m3) | 0.04 (0.01) | <0.0001 | 0.03 (0.01) | <0.0001 | 0.04 (0.01) | <0.0001 | 0.04 (0.01) | <0.0001 |
| 2,5-dimethylfuran (μg/L) | 3.76 (1.78) | 0.04 | 13.32 (2.17) | <0.0001 | 0.45 (1.67) | 0.79 | 4.65 (1.86) | 0.02 |
| USAF base A | Ref | Ref | Ref | Ref | ||||
| USAF base B | 3.36 (0.22) | <0.0001 | 1.55 (0.26) | <0.0001 | 1.38 (0.20) | <0.0001 | 1.50 (0.23) | <0.0001 |
| USAF base C | 0.44 (0.46) | 0.34 | −0.77 (0.56) | 0.17 | 0.12 (0.43) | 0.79 | −0.64 (0.48) | 0.19 |
| Mean relative humidity | 0.003 (0.01) | 0.81 | 0.02 (0.02) | 0.13 | 0.02 (0.01) | 0.13 | 0.03 (0.01) | 0.03 |
| Summary Adjusted R2 | 0.82 | 0.63 | 0.69 | 0.67 | ||||
JP-8, jet propulsion fuel 8; Ref, referent; SE, standard error; THC, total hydrocarbons; TWA, time-weighted average; USAF, US Air Force; VOC, volatile organic compounds.
Model 1: with self-reported cigarette use (shift cigarette smoking [yes/no]) and day 5 JP-8 exposure (yes/no).
Model 2: with measured JP-8 (8-h TWA THC [mg/m3]) and cigarette smoke exposure (2,5-dimethylfuran [μg/L]).
Multiple linear regression.
Natural log-transformed.
Model 2 was used to evaluate THC in personal air samples as a predictor of individual blood VOCs, while controlling for cigarette smoking using the blood biomarker 2,5-dimethylfuran, USAF base, and mean relative humidity (Table 3). THC in personal air was a significant predictor for ethylbenzene, toluene, o-xylene, and m/p-xylene in blood. The measure of cigarette smoking, blood levels of 2,5-dimethylfuran, remained significant in all models, with the exception of o-xylene. Model 2 explained a larger portion of the variance in the blood VOCs than did Model 1, with adjusted R2 values ranging from 63% (toluene) to 82% (ethylbenzene).
To further evaluate confounding from cigarette smoking, Model 2 was re-run only among USAF personnel who did not smoke during the work shift (n = 46), and 2,5-dimethylfuran was excluded as a covariate (data not shown). For each of the JP-8 components, parameter estimates for 8-h TWATHC and adjusted R2 were consistent with results in Table 3.
DISCUSSION
VOCs in blood can serve as biomarkers of JP-8 exposure over a work shift in USAF personnel. Specifically, of the VOCs measured, o-xylene and m/p-xylene appear to be the most appropriate blood biomarkers of JP-8 exposure. This is based on their strong correlations with THC in personal air, and results of the regression model that indicated that THC concentration was a significant predictor of o-xylene and m/p-xylene. Also, results showed that self-reported work shift jet fuel exposure was a good predictor of o-xylene and m/p-xylene. Because the half-life of VOCs in blood is on the time course of several hours, we used an exposure measure self-reported during the same work shift as the collection of the blood sample. THC concentration in the personal breathing zone measured over a work shift was a better predictor of ethylbenzene and toluene than self-reported exposure, potentially indicating another source of VOC exposure other than jet fuel.
We explored the role of several potential confounders, particularly cigarette smoke. Significantly, more individuals exposed to JP-8 during the day 5 work shift also smoked during that shift. We used two different variables to control for the effect of smoking on VOC levels in blood: self-reported smoking during the work shift and concentration of 2,5-dimethylfuran in blood. Self-reported smoking during the work shift corresponded well with smoking biomarker 2,5-dimethylfuran. Among the 23 participants who smoked during their work shift, 21 (91%) had detectable levels of 2,5-dimethylfuran and 20 (87%) had a blood concentration of 2,5-dimethylfuran 0.014 μg/L or more, the CDC cutoff for classifying a daily smoker smoking the equivalent of one cigarette per day.14 Blood levels of 2,5-dimethylfuran can be affected by several factors not captured by our questionnaires, including environmental tobacco smoke, brand style of cigarette, time since last cigarette, and cigarettes smoked per day. In our study, cigarette usage was categorized to the nearest fractional pack, rather than cigarettes per day, to simplify the estimation of cigarettes smoked during shift by participants and to utilize an inherent categorization established by smokers. Information regarding brand and style of cigarette smoked or exact time since the previous cigarette was not obtained.
The USAF base at which personnel worked was also a significant predictor of VOCs in blood. Participating personnel at USAF Base B had significantly higher levels of all the analyzed blood VOCs compared with those at other USAF base locations. There could be multiple factors contributing to the differences in VOC exposure by location. First, JP-8 composition can vary based on batch and can also be altered based on performance needs and type of aircraft maintained at a particular location.24 Second, exposure could be affected by specific job task being performed and differences in use of personal protective equipment (PPE) (eg, tasks requiring respirators). Certain tasks may require the use of other solvents and chemicals. We could not analyze exposure to other chemicals because of small sample size endorsing their use during the work shift (n = 5 or less). Lastly, personal air levels of THC capture occupational exposure to VOCs via inhalation; however, air sampling pumps were turned off while respirators were in use. Respirator use decreases inhalation exposure, but past studies have found that dermal exposure can also be an important route of VOC exposure.8,25 Blood biomarkers can provide a measure for both inhalation and dermal exposure.
CONCLUSIONS
This study demonstrates that VOCs in blood reflect occupational exposure to JP-8 during a work shift. USAF personnel who reported occupational exposure to JP-8 had higher concentrations of blood VOCs than did personnel who did not report occupational contact with JP-8. Higher concentrations of THC in personal air samples were significantly associated with higher levels of VOCs in blood, even after controlling for smoking and other potential confounders. Although more invasive, detection of VOCs in blood offers an estimate of absorbed dose from multiple routes of exposure and a direct measure of body burden compared with detection of these compounds in personal breathing zone samples. These observations support the use of blood VOCs as a biomarker of occupational exposure to fuels such as JP-8.
ACKNOWLEDGMENT
The authors thank the USAF personnel for their support and generous participation in the project. They thank the additional Boston area study team personnel (Kristin J. Heaton, Kristen W. Smith, Ema Rodrigues, Nichole Longcore, Elisa Kryskow, and Kian Merchant-Borna) and other personnel from local universities for their assistance in data collection at the respective USAF base locations.
This work was supported by the US Army Medical Research and Materiel Command through a grant award (W81XWH-06-1-0105; principal investigator: SPP) to the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc.
The views expressed are those of the authors and do not reflect the official policy of the US Department of the Army or the US Department of Defense. The findings and conclusions of this paper are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
Footnotes
The authors report no conflicts of interest.
REFERENCES
- 1.National Research Council. Toxicologic Assessment of Jet-Propulsion Fuel 8. Washington, DC: National Academy of Sciences; 2003. [PubMed] [Google Scholar]
- 2.Merchant-Borna K, Rodrigues EG, Smith KW, Proctor SP, McClean MD. Characterization of inhalation exposure to jet fuel among US Air Force personnel. Ann Occup Hyg. 2012;56:736–745. [DOI] [PubMed] [Google Scholar]
- 3.Smith KW, Proctor SP, Ozonoff A, McClean MD. Inhalation exposure to jet fuel (JP8) among US Air Force personnel. J Occup Environ Hyg. 2010;7:563–572. [DOI] [PubMed] [Google Scholar]
- 4.Pleil JD, Smith LB, Zelnick SD. Personal exposure to JP-8 jet fuel vapors and exhaust at Air Force bases. Environ Health Perspect. 2000;108:183–192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Puhala E, Lemasters G, Smith L, et al. Jet fuel exposure in the United States Air Force. Appl Occup Environ Hyg. 1997;12:606–610. [Google Scholar]
- 6.Smith KW, Proctor SP, Ozonoff A, McClean MD. Urinary biomarkers of occupational jet fuel exposure among air force personnel. J Expo Sci Environ Epidemiol. 2012;22:35–45. [DOI] [PubMed] [Google Scholar]
- 7.Tu RH, Mitchell CS, Kay GG, Risby TH. Human exposure to the jet fuel, JP-8. Aviat Space Environ Med. 2004;75:49–59. [PubMed] [Google Scholar]
- 8.Chao YE, Gibson RL, Nylander-French LA. Dermal exposure to jet fuel (JP-8) in US Air Force personnel. Ann Occup Hyg. 2005;49:639–645. [DOI] [PubMed] [Google Scholar]
- 9.Chao YE, Kupper LL, Serdar B, Egeghy PP, Rappaport SM, Nylander-French LA. Dermal exposure to jet fuel JP-8 significantly contributes to the production of urinary naphthols in fuel-cell maintenance workers. Environ Health Perspect. 2006;114:182–185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Serdar B, Egeghy PP, Waidyanatha S, Rappaport SM. Urinary biomarkers of exposure to jet fuel (JP-8). Environ Health Perspect. 2003;111:1760–1764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Serdar B, Egeghy PP, Gibson R, Rappaport SM. Dose-dependent production of urinary naphthols among workers exposed to jet fuel (JP-8). Am J Ind Med. 2004;46:234–244. [DOI] [PubMed] [Google Scholar]
- 12.Rodrigues EG, Smith K, Maule AL, et al. Urinary polycyclic aromatic hydrocarbon (OH-PAH) metabolite concentrations and the effect of GST polymorphisms among US Air Force personnel exposed to jet fuel. J Occup Environ Med. 2014;56:465–471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kirman CR, Aylward LL, Blount BC, Pyatt DW, Hays SM. Evaluation of NHANES biomonitoring data for volatile organic chemicals in blood: application of chemical-specific screening criteria. J Exp Sci Environ Epidemiol. 2012;22:24–34. [DOI] [PubMed] [Google Scholar]
- 14.Chambers DM, Ocariz JM, McGuirk MR, Blount BC. Impact of cigarette smoking on volatile organic compound (VOC) blood levels in the US population: NHANES 2003–2004. Environ Int. 2011;37:1321–1328. [DOI] [PubMed] [Google Scholar]
- 15.Ashely DL, Bonin MA, Cardinali FL, McCraw JM, Wooten JV. Measurements of volatile organic compounds in human blood. Environ Health Perspect. 1996;104(suppl 5):871–877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Polzin GM, Kosa-Maines RE, Ashley DL, Watson CH. Analysis of volatile organic compounds in mainstream cigarette smoke. Environ Sci Technol. 2007;41:1297–1302. [DOI] [PubMed] [Google Scholar]
- 17.Chambers DM, Blount BC, McElprang DO, Waterhouse MG, Morrow JC. Picogram measurement of volatile n-alkanes (n-hexane through n-dodecane) in blood using solid-phase microextraction to assess nonoccupational petroleum-based fuel exposure. Anal Chem. 2008;80: 4666–4674. [DOI] [PubMed] [Google Scholar]
- 18.Ashley DL, Bonin MA, Cardinali FL, McCraw JM, Wooten JV. Blood concentrations of volatile organic compounds in a nonoccupationally exposed US population and in groups with suspected exposure. Clin Chem. 1994;40:1401–1404. [PubMed] [Google Scholar]
- 19.Bray RM, Pemberton MR, Lane ME, Hourani LL, Mattiko MJ, Babeu LA. Substance use and mental health trends among US military active duty personnel: key findings from the 2008 DoD Health Behavior Survey. Mil Med. 2010;175:390–399. [DOI] [PubMed] [Google Scholar]
- 20.Proctor SP, Heaton KJ, Smith KW, et al. The Occupational JP8 Exposure Neuroepidemiology Study (OJENES): repeated workday exposure and central nervous system functioning among Air Force personnel. Neurotoxicology. 2011;32:799–808. [DOI] [PubMed] [Google Scholar]
- 21.National Institute for Occupational Safety and Health (NIOSH). Naphthas: method 1550 In: NIOSH Manual of Analytical Methods. 4th ed. Cincinnati, OH: National Institute for Occupational Safety and Health; 1994. [Google Scholar]
- 22.Chambers DM, McElprang DO, Waterhouse MG, Blount BC. An improved approach for accurate quantitation of benzene, toluene, ethylbenzene, xylene, and styrene in blood. Anal Chem. 2006;78:5375–5383. [DOI] [PubMed] [Google Scholar]
- 23.Ashley DL, Bonin MA, Hamar B, McGeehin M. Using the blood concentration of 2,5-dimethylfuran as a marker for smoking. Int Arch Occup Environ Health. 1996;68:183–187. [DOI] [PubMed] [Google Scholar]
- 24.Ritchie G, Still K, Rossi J III, Bekkedal M, Bobb A, Arfsten D. Biological and health effects of exposure to kerosene-based jet fuels and performance additives. J Toxicol Environ Health B Crit Rev. 2003;6:357–451. [DOI] [PubMed] [Google Scholar]
- 25.Kim D, Andersen ME, Nylander-French LA. Dermal absorption and penetration of jet fuel components in humans. Toxicol Lett. 2006;165:11–12. [DOI] [PubMed] [Google Scholar]