

Abstract
In this paper, we formulated a mathematical model that studies the dynamics of HIV/AIDS in Turkey from 1985 to 2016. We find two equilibrium points, disease free equilibrium and endemic equilibrium. Global stability analysis of the equilibria was conducted using Lyapunov function which depends on the basic reproduction ratio R 0. If R 0 < 1, the disease free equilibrium point is globally asymptotically stable, and if R 0 ≥ 1 the endemic equilibrium point is globally asymptotically stable. We computed and predicted the basic reproduction ratios across all the years. It was found out that there were flaws in the exact values of R 0 which is related to the poor registration system of HIV/AIDS in Turkey. Hence, there is need for the government to improve the system in order to cover the actual cases of the disease. The increase of the basic reproduction ratio over the years also shows the need for the relevant authorities to adopt appropriate control measures in combating the disease.
Keywords: Dynamics, HIV/AIDS, Basic reproduction ratio, Turkey, Equilibrium points, Stability
Introduction
Human immunodeficiency virus (HIV) aims at destroying and weakening the human defense mechanisms viz., immune systems, against fighting infections and any other disease. The progression of the virus impairs, destruct and worsen the role of the immune cells in protecting the human body against infection, this leads to the reduction of the CD4 cell count and advancement of the disease. The CD4 cell count mainly measures how active and functioning the immune systems is. When it is at most 200 cell/mm3, then the individual is immunodeficient and considered to be in the “AIDS phase”. Therefore, the most advanced stage of HIV infection is acquired immunodeficiency syndrome (AIDS) (Hove-Musekwaa and Nyabadza 2009; Duffin and Tullis 2002).
HIV/AIDS is the leading disease threatening the human population. It is the biggest health problem that is hunting every part of the world which is likely to persist for a very long time. It was discovered in the early 1980’s in two homosexual men in the United States of America. They were discovered with Candidiasis (a fungal infection) and a tumor called Kaposi’s sarcoma respectively. The virus responsible for these infections was found out to be the human immunodeficiency virus (HIV) (Diekmann and Heesterbeek 2000). The virus is transmitted through unprotected sexual intercourse, homosexual and bisexual sex, contaminated blood transfusion, intravenous drug use, interaction with contaminated sharp objects and other unidentified ways. Symptoms of the disease include Influenza-like sickness, fever, headache, rashes and sore throat. However, some individuals may not be aware of the illness until their situation start becoming critical (Kockaya et al. 2016).
In 2009, around 33.3 million HIV infected individuals were recorded worldwide (Sayan et al. 2013). Also, according to a report in 2010, almost 2 million people died of HIV/AIDS, around 3 million newly infected individuals, and about 34 million individuals were living with HIV/AIDS across the globe. In 2011, China reported that 2.8 million patients died of HIV/AIDS and 7.8 million new cases were recorded by December (Li et al. 2012). The World Health Organization (WHO) stated in 2013 that, 2.1 million people were newly infected, and about 1.5 million people died of AIDS-related disease. Moreover, in 2014, the total number of people living with HIV was 35 million (Al-Sheikh et al. 2011).
HIV/AIDS was first discovered in Turkey in 1985. At the beginning, the number of people infected with the disease in Turkey was very small; therefore, enough attention was not given to gather the actual number of people living with it. As a result, from 1985 to 1996 it was considered to be a single time period with a total of 617 patients, in which 57% of such patients got infected through heterosexual sex, 16.1% via intravenous drug use, 14.8% through homosexual/bisexual courtship, 10% through blood transfusion, and 1.4% was from mother to child. The National AIDS Commission was established in 1996 due to the rapid spread of the disease (Erbaydar and Eybaydar 2012). There were 708 people living with HIV/AIDS from 1997 to 2001; of which 119 newly infected individuals were recorded in 1999.
The Ministry of Health (Ankara, Turkey) in 2004 reported 210 new cases, and 1802 HIV infected individuals; where 800 were AIDS patients (Ayranci 2005). Some researchers reported that 946 new cases were detected in the period 2007–2011 with heterosexual relationships contributing more to the increase of the disease. More so, in 2011, the number of new cases (which is the highest) and the total number of people living with HIV/AIDS was 699 and 5224 respectively.
In 2013, the Ministry also published that, at least 6000 individuals were infected with HIV/AIDS. Additionally, 1767 were newly infected in 2014, and about 9379 people were living with HIV/AIDS by the end of the year. This registered about 38% increase in the number of patients in Turkey (Sayan et al. 2016).
Conclusively over the last decade, infection with STDs has risen due to the rise of ‘mobile prostitution’ with illegal workers from abroad, especially from Eastern Europe. In addition, an increasing number of workers from African countries, which is also one of the most infected continents in the globally (Altan 2007), enter Turkey illegally.
New infections start with someone who is already infected. This new infection occurs because the infected persons do not take necessary precaution measures or because of poor protective services. This can be possible if patients are not being well educated on their responsibility to prevent the spread of the disease and/or are not being included in protective service studies (Morin et al. 2004). In general, HIV diagnosis is a traumatic experience that changes HIV+ person’s life. This is why patients don’t reveal their diagnosis at all or only reveal it to a limited number of people. It is among the strategic goal of HIV prevention to understand how and why patients hide their diagnosis and to determine possible solution to it (Miller and Rubin 2007; Anderson et al. 2009; Wolf et al. 2004). Previous studies indicated that the most common reason patients hide their diagnosis is fear of stigma and exclusion (Anderson and Walker 2010). It has also been indicated that having a family member diagnosed with HIV can affect family members in different ways (Vithayachockitikhun 2006).
Another study performed in Turkey shows that in addition to problems faced by HIV+ people with regard to employment, health and education, the biggest problem is stigma. Many more studies carried out in different countries and in different cultures and religions have reported the same threat faced by the patients and their families as those in Turkey (Ramchandani et al. 2007). Due to these problems HIV/AIDS positive people normally do not register themselves in the various registration centers. However, there is need for government and other relevant authorities to know the exact cases of HIV in the country in order to know the exact threat posed by the disease and consequently adopt possible measures in combating it.
Mathematical models can be used in studying the dynamics of HIV/AIDS (Korenromp et al. 2002; White et al. 2004). Primary purpose of any mathematical model of HIV transmission lies in using individual level inputs to project population level outcomes. Some of the important outcomes that can be examined with a model are; the incidence of infection, the prevalence of infection, or the doubling time of the epidemic. More important than these however, is simply the likelihood of an epidemic to occur that is whether there is sufficient transmission potential for a chain of infection to be sustained. This outcome is termed by a simple summary statistic: the reproduction number of the infectious process, R0. In a susceptible population, R0 represents the expected number of secondary infections generated by the first infected individual. If R0 is equal or greater than 1 an epidemic is expected. If R0 is less than 1, the infection is expected to die out.
The magnitude of R 0 is used to measure the risk of an epidemic or pandemic in any emerging infectious disease. It was used for understanding the outbreak and danger of SARS (Choi and Pak 2003). R 0 was also used to characterize bovine spongiform encephalitis (BSE), foot and mouth disease (FMD), strains of influenza, and West Nile Virus (Woolhouse and Anderson 1997; Ferguson et al. 2001; Mills et al. 2004; Wonham et al. 2004). The incidence and spread of dengue, Ebola, and scrapie have also been assessed by R 0 (Luz et al. 2003; Hagmann et al. 2003; Chowell et al. 2004). Tropical issues such as the risks of indoor airborne infection, bioterrorism, and computer viruses also depend on this important parameter (Gravenor et al. 2004; Rudnick and Milton 2003; Kaplan et al. 2002).
The aim of this study is to determine the actual threats posed by HIV/AIDS using mathematical modeling, and to indicate the possible flaws in the existing registration exercise in Turkey. We intend to achieve this by comparing the magnitude of this important threshold quantity (basic reproduction ratio) for the official data obtained from Federal Ministry of Health Turkey and the results obtained from the simulation of our model.
The organization of the paper is as follows: In Sect. 2, the model is presented and the basic reproduction number is obtained. In Sect. 3, stability of the equilibria is investigated. In Sect. 4, results are obtained and compared using the official data and by numerically simulating our model. Finally Sect. 5 is the discussion and conclusion of the research.
Construction of the model
The model is a system of differential equations as follows; where the meaning of parameters/variables is given by Table 1.
Table 1.
Meaning of parameters and variables of the model (1)
| Parameters/variables | Meaning |
|---|---|
| S(t) | Population of susceptibles |
| H(t) | Infectives with HIV that have not yet developed AIDS symptoms |
| A(t) | Infectives with AIDS symptoms |
| Λ | Recruitment rate (birth rate of Turkish people) |
| Duration spent in the HIV stage before developing AIDS symptoms | |
| Life expectancy of Turkish people | |
| Average duration spent in the AIDS stage | |
| α | Incidence rate |
| 1 |
Assumptions
-
(i)
S(0) is considered to be the whole population in a specific year
-
(ii)
We considered homogeneous mixing in the population
It follows from (1) that,
Then
Thus the feasible region for (1) is
Existence of equilibrium points
Equating the equations in (1) to zero and solving simultaneously we find two equilibrium points. Disease free and endemic equilibrium points.
E 0 always exists
and
E 1 exists (is biologically meaningful) when are both positive.
S 1 > 0, H 1, A 1 > 0 if Λα − μv − μ 2 > 0, which implies .
In Sect. 2.3, we will come to realize the meaning of .
Basic reproduction ratio
This is the number of secondary infections caused by a single infective individual in a completely susceptible population. It is denoted by R 0. Using the next generation of matrix (NGM) method we have,
The spectral radius, which is the dominant eigenvalue, is
Hence the basic reproduction ration is;
Global stability analysis of the equilibria
In this section stability analysis of the two equilibrium points is obtained by the use of Lyapunov function. The conditions for the global stability of the equilibria in each case depends on the magnitude of the basic reproduction ratio R 0. Hence we have the following theorems and their proofs.
Theorem 1
The disease free equilibrium is globally asymptotically stable when R 0 ≤ 1.
Proof
We construct the following Lyapunov function
where C = S 0 lnS 0 − S 0 − H 0
< 0 by the relation between geometric and arithmetic means and if αS 0 ≤ (v + μ).
This implies R 0 ≤ 1.
Theorem 2
The endemic equilibrium E 1 is globally asymptotically stable when R 0 > 1.
Proof
We construct the following Lyapunov function
where
< 0 by the relation between arithmetic and geometric mean and if αΛ − μv − μ 2 > 0
This implies R 0 > 1.
Results
In this section, results are calculated by simulating the model using the formal data obtained in Turkey. Table 2 and Fig. 1 show the comparison of the official data obtained from Federal Ministry of Health Turkey with the predicted value from the model. It shows the years, number of HIV cases, number of AIDS cases and the total number of HIV and AIDS from 1985 to 2016.
Table 2.
HIV/AIDS cases in Turkey from 1985 to 2016 as obtained from Ministry of Health Turkey compared with predicted values from the model
| Year | HIV exact (predicted) | AIDS exact (predicted) | Total exact (predicted) |
|---|---|---|---|
| 1985 | 0 (0) | 3 (3) | 3 (3) |
| 1986 | 1 (2.31014) | 1 (1) | 2 (3.3101) |
| 1987 | 32 (2.31014) | 8 (1) | 40 (3.3101) |
| 1988 | 21 (4.066481) | 11 (1.000001) | 32 (5.0665) |
| 1989 | 22 (7.66129) | 11 (1.000004) | 33 (8.6613) |
| 1990 | 23 (13.80698) | 13 (1.000002) | 36 (14.8070) |
| 1991 | 27 (23.19329) | 24 (1.000088) | 51 (24.1834) |
| 1992 | 37 (36.96717) | 28 (1.00035) | 65 (37.9675) |
| 1993 | 49 (57.09593) | 34 (1.00128) | 83 (38.0972) |
| 1994 | 49 (87.09992) | 36 (1.004533) | 85 (88.1045) |
| 1995 | 60 (132.403) | 29 (1.015914) | 89 (133.4189) |
| 1996 | 93 (201.0708) | 35 (1.055754) | 128 (202.1266) |
| 1997 | 96 (305.2835) | 38 (1.195321) | 134 (306.4789) |
| 1998 | 83 (443.7849) | 42 (1.600894) | 125 (445.3858) |
| 1999 | 89 (623.8392) | 29 (2.67366) | 118 (626.5128) |
| 2000 | 115 (859.6329) | 47 (5.400612) | 162 (865.0335) |
| 2001 | 139 (1170.991) | 44 (12.22252) | 183 (1183.2138) |
| 2002 | 139 (1581.795) | 41 (29.11121) | 180 (1610.9060) |
| 2003 | 136 (2116.389) | 50 (70.31996) | 186 (2186.7093) |
| 2004 | 177 (2790.633) | 59 (168.3727) | 236 (2959.0055) |
| 2005 | 253 (3592.832) | 46 (391.6827) | 299 (3984.5147) |
| 2006 | 257 (4455.529) | 43 (864.6296) | 300 (5320.1588) |
| 2007 | 352 (5180.24) | 23 (1661.795) | 375 (6842.0349) |
| 2008 | 393 (5613.643) | 55 (2586.58) | 448 (8200.2232) |
| 2009 | 441 (5852.257) | 66 (3529.285) | 507 (9381.5420) |
| 2010 | 519 (5976.791) | 71 (4461.45) | 590 (10438.2413) |
| 2011 | 642 (6031.311) | 84 (5366.967) | 726 (11398.2777) |
| 2012 | 982 (6041.799) | 95 (6236.744) | 1077 (12278.5434) |
| 2013 | 1311 (6024.255) | 101 (7065.889) | 1412 (13090.1448) |
| 2014 | 1892 (5988.786) | 131 (7852.095) | 2023 (13840.8810) |
| 2015 | 2072 (5966.372) | 112 (8230.182) | 2184 (14196.5535) |
| 2016 | 3302 (6012.41) | 80 (8520.12) | 3382 (14532.5300) |
| Total | 5227 (77196.55) | 1483 (57072.39) | 13646 (134268.9442) |
Fig. 1.
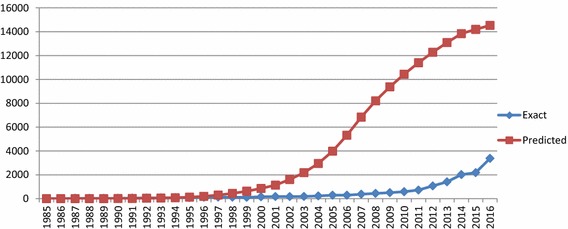
Exact and predicted cumulative HIV+ cases from 1985 to 2016
We computed the basic reproduction ration (R 0) in each year to show number of secondary infections caused by a single infectious individual in the population for that year. In epidemiology if this threshold quantity is equal or greater than one there is going to be epidemics, as such it’s magnitude is used to measure the threat posed by certain disease in a given population. Table 3 and Fig. 2 give the comparison between these basic reproduction ratios as calculated using the official data and the corresponding predicted values as calculated using the model.
Table 3.
Exact and predicted R 0 values from 1985 to 2015
| Year | Exact values | Predicted values |
|---|---|---|
| 1985 | 0.045401 | 0.045401 |
| 1986 | 0.029659 | 0.049087 |
| 1987 | 0.58178 | 0.049087 |
| 1988 | 0.456853 | 0.075133 |
| 1989 | 0.462785 | 0.128441 |
| 1990 | 0.353095 | 0.160276 |
| 1991 | 0.563757 | 0.295019 |
| 1992 | 0.679453 | 0.463176 |
| 1993 | 0.867609 | 0.708746 |
| 1994 | 0.882049 | 1.07482 |
| 1995 | 0.796116 | 1.40781 |
| 1996 | 1.124347 | 2.102394 |
| 1997 | 1.154649 | 3.14182 |
| 1998 | 1.05553 | 4.48248 |
| 1999 | 0.938591 | 6.18886 |
| 2000 | 1.338066 | 8.90877 |
| 2001 | 1.443639 | 11.95852 |
| 2002 | 1.36609 | 15.91767 |
| 2003 | 1.37469 | 21.4029 |
| 2004 | 1.706281 | 28.86696 |
| 2005 | 1.859081 | 34.17056 |
| 2006 | 1.842382 | 46.31508 |
| 2007 | 2.262939 | 61.45404 |
| 2008 | 2.643101 | 74.6881 |
| 2009 | 3.138635 | 93.12544 |
| 2010 | 4.677689 | 138.0197 |
| 2011 | 5.650843 | 153.5268 |
| 2012 | 8.712188 | 178.081 |
| 2013 | 11.62473 | 200.521 |
| 2014 | 16.26865 | 214.8543 |
| 2015 | 16.73746 | 215.3541 |
Fig. 2.
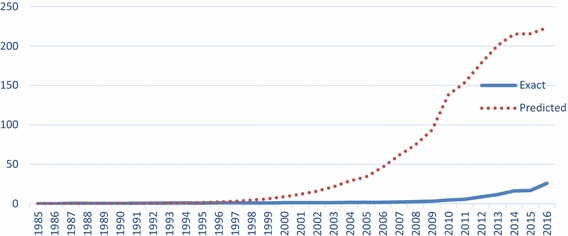
Exact and predicted basic reproduction ratios from 1985 to 2015
To show the significance of the data obtained by the model in predicting HIV epidemics in Turkey over the official data obtained from the Ministry of Health Turkey, we obtained HIV drug data from intercontinental marketing service (IMS). The IMS data composed of IMS Health Turkey Pharmaceutical Index Data view and Turkey Hospital Index Data view. Table 4 and Fig. 3 shows the relationships of these three sets of data (exact, predicted, and IMS) from 2000 to 2016. This is because the only available IMS data for Turkey started from the year 2000.
Table 4.
Comparison of number of HIV cases in Turkey from 2000 to 2016 using the official data obtained from Ministry of Health Turkey (exact), model data (predicted) and IMS drug data
| Years | Exact | Predicted | IMS drug data |
|---|---|---|---|
| 2000 | 115 | 859.6329 | 17 |
| 2001 | 139 | 1170.991 | 25 |
| 2002 | 139 | 1581.795 | 42 |
| 2003 | 136 | 2116.389 | 84 |
| 2004 | 177 | 2790.633 | 109 |
| 2005 | 253 | 3592.832 | 273 |
| 2006 | 257 | 4455.529 | 383 |
| 2007 | 352 | 5180.24 | 490 |
| 2008 | 393 | 5613.643 | 659 |
| 2009 | 441 | 5852.257 | 1087 |
| 2010 | 519 | 5976.791 | 1942 |
| 2011 | 642 | 6031.311 | 1734 |
| 2012 | 982 | 6041.799 | 2411 |
| 2013 | 1311 | 6024.255 | 2959 |
| 2014 | 1892 | 5988.786 | 3841 |
| 2015 | 2072 | 5966.372 | 5434 |
| 2016 | 3302 | 6012.41 | 7835 |
| Total | 13,122 | 75255.67 | 29,325 |
Fig. 3.
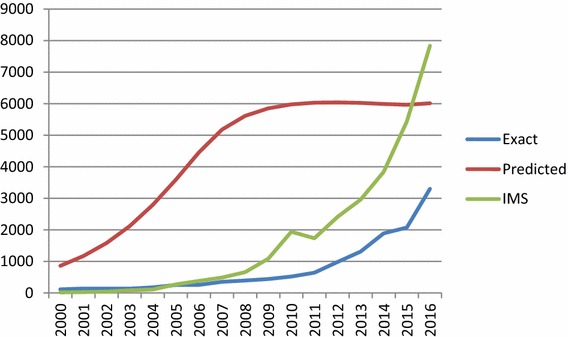
Exact, predicted, and IMS HIV+ cases from 2000 to 2016
Discussions and conclusions
In this paper, we constructed a mathematical model that describes the dynamics of HIV/AIDS in Turkey from 1985 to 2015. We found two equilibrium points, disease free and endemic equilibrium point. Global stability analysis of the equilibria was carried out by the use of Lyapunov function. Conditions of stability of both the equilibrium points were shown to depend on a threshold quantity, the basic reproduction ratio (R 0). It was shown that if the basic reproduction ratio is less than one, the disease free equilibrium is globally asymptotically stable and the disease dies out. Also, if the basic reproduction ratio is greater than one, the endemic equilibrium point is globally asymptotically stable, and epidemics occur.
We used official data collected from the Ministry of Health in Turkey from 1985 to 2016 to study and predict the dynamics of HIV/AIDS in Turkey. Basic reproduction ratios were found over the years, and their magnitudes were compared. We also predicted the basic reproduction ratios over the years using our model. From Table 2 and Fig. 1, it can be observed that the predicted cases of both HIV and AIDS are below or almost equal to the exact values from 1985 to 1993. Starting from 1994 the predicted cases continue to increase rapidly and are far greater than the exact cases. This can be attributed to poor registration exercise in the country.
From Table 3, it can be seen that from 1985 to 1995 the exact values for the basic reproduction ratios are less than one, hence no epidemics. It is also less than one in 1999. Starting from 1996, with the exception of 1999, all the basic reproduction ratios are greater than one, implying epidemics.
From the predicted values R 0 values are less than one from 1985 to 1993, which almost agrees with the exact values. After 1993 the epidemics start to occur with the value of R 0 greater than one in each year. In the exact values of R 0, we noticed a fluctuation from 1985 up to 2005 and then a steady increase from 2006 to 2016. This can also be attributed to poor registration system to cover the exact HIV/AIDS cases in Turkey. However, there is stable increase in the predicted values of R 0 over the years. Hence our model shows the flaws in the registration systems of the disease in Turkey. This can also be clearly observed from Figs. 1 and 2.
To show the significance of the data obtained by the model in predicting HIV epidemics in Turkey over the official data obtained from the Ministry of Health Turkey, we obtained HIV drug data from intercontinental marketing service (IMS). Comparing these three sets of data, which can be seen from Fig. 3, shows the flaws in the official data. The result of the analysis in this paper shows the urgent need of intervention by the relevant authorities in controlling the spread of the disease. Since in recent years, the education sector has come to play an increasingly important role in preventing HIV. Our proposal here is the use of interventions through the education sector to curtail the spread of the disease in Turkey. This is particularly because many studies in literature show that the school-based HIV/AIDS education programs provide significant changes in knowledge and attitudes that affect sexual behavior of young people. This leads to significant progress in the use of condoms and decrease in most of the sexual health problems. (Thomson et al. 1999; Kinsler 2004; Fawole et al. 1999; Kirby et al. 2007; James-Traore et al. 2004). Two element are covered by effective school-based education: training of teachers and curriculum development. A review by Kirki et al. evaluates multiple studies of such interventions and found that successful curriculum-based programs have 17 characteristics (Thomson et al. 1999). Some of these characteristics were about development of the curriculum; Some were about the curriculum itself; and the remaining were about the implementation of the curriculum (Thomson et al. 1999). After developing a curriculum, there is need for teachers to be well trained to enable them to improve students’ knowledge about HIV prevention and transmission, attitudes toward HIV prevention, and behaviours relating to HIV/AIDS.
In conclusion, the basic reproduction ratio is increasing in Turkey over the years. This shows the need of intervention from the relevant authorities in controlling the spread of this disease. Also there is need for the government to enhance the registration system of HIV/AIDS, so as to know the exact threat posed by the disease and consequently adopt possible measures in combating it.
Compliance with ethical standards
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Contributor Information
Murat Sayan, Email: sayanmurat@hotmail.com.
Evren Hınçal, Email: evren.hincal@neu.edu.tr.
Tamer Şanlıdağ, Email: trsanlidag@yahoo.com.
Bilgen Kaymakamzade, Email: bilgen.kaymakamzade@neu.edu.tr.
Farouk Tijjani Sa’ad, Email: farouksaaad@yahoo.co.uk.
Isa Abdullahi Baba, Email: isababa7@yahoo.com.
References
- Al-Sheikh S, Musali F, Alsolami M. Stability analysis of an HIV/AIDS epidemic model with screening. Int. Math. Forum. 2011;6(66):3251–3273. [Google Scholar]
- Altan P. Surveillance of the sexually transmitted diseases and HIVAIDS in Turkey: situation analysis. Ankara: Ministry of Health; 2007. [Google Scholar]
- Anderson GL, Walker L. My biggest fear was that people would reject me once they knew my status: stigma as experienced by patients in an HIV/AIDS clinic in Johannesburg, South Africa. Health Soc. Care Community. 2010;18:139–146. doi: 10.1111/j.1365-2524.2010.00921.x. [DOI] [PubMed] [Google Scholar]
- Anderson M, Elam G, Solarin I, Gerver S, Fenton K, Easterbrook P. Coping with HIV: caribbean people in the United Kingdom. Qual. Health Res. 2009;19:1060–1075. doi: 10.1177/1049732309341191. [DOI] [PubMed] [Google Scholar]
- Ayranci U. Aids knowledge and attitudes in a Turkish population. An epidemiology study. BMC Public Health. 2005;5:95. doi: 10.1186/1471-2458-5-95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Choi BCK, Pak AWP. A simple approximate mathematical model to predict the number of severe acute respiratory syndrome cases and deaths. J. Epidemiol. Community Health. 2003;57:831–835. doi: 10.1136/jech.57.10.831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chowell G, Hengartner NW, Castillo-Chavez C, Fenimore PW, Hyman JM. The basic ratio number of ebola and the effects of public health measures: the cases of Congo and Uganda. J. Theor. Biol. 2004;229:119–126. doi: 10.1016/j.jtbi.2004.03.006. [DOI] [PubMed] [Google Scholar]
- Diekmann O, Heesterbeek JAP. Mathematical Epidemiology of Infectious Diseases: Model Building, Analysis and Interpretation. Chichester: Wiley; 2000. [Google Scholar]
- Duffin RP, Tullis RH. Mathematical models of the complete course of HIV infection and AIDS. J. Theor. Med. 2002;4(4):215–221. doi: 10.1080/1027366021000051772. [DOI] [Google Scholar]
- Erbaydar T, Eybaydar NP. Status HIV/AIDS epidemic in Turkey. Acta Medica. 2012;1:19–24. [Google Scholar]
- Fawole IO, Asuzu MC, Oduntan SO, Brieger WR. A school-based AIDS education programme for secondary school students in Nigeria: a review of effectiveness. Health Educ. Res. 1999;14:675–683. doi: 10.1093/her/14.5.675. [DOI] [PubMed] [Google Scholar]
- Ferguson NM, Donnelly CA, Anderson RM. The foot-and-mouth epidemic in Great Britain: pattern of spread and impact of interventions. Science. 2001;292:1155–1160. doi: 10.1126/science.1061020. [DOI] [PubMed] [Google Scholar]
- Gravenor MB, Papasozomenos P, McLean AR, Neophytou GA. Scrapie epidemic in Cyprus. Epidemiol. Infect. 2004;132:751–760. doi: 10.1017/S0950268804002110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hagmann R, Charlwood JD, Gil V, Conceicao F, do Rosario V, Smith TA. Malaria and its possible control on the island of Principe. Malar. J. 2003;2:15. doi: 10.1186/1475-2875-2-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hove-Musekwaa SD, Nyabadza F. The dynamics of an HIV/AIDS model with screened disease carriers. Comput. Math. Methods Med. 2009;10:287–305. doi: 10.1080/17486700802653917. [DOI] [Google Scholar]
- James-Traore, T.A., Finger, W., Ruland, C.D., Savariaud, S.: Teacher training: essential for school-based reproductive health and HIV/AIDS education; focus on sub-Saharan Africa, p. 36. Family Health International, Durham. (Technical report; youth issues paper no. 3) (2004)
- Kaplan EH, Craft DL, Wein LM. Emergence response to small pox attack: the case for mass vaccination. Proc. Natl. Acad. Sci. U.S.A. 2002;99:10935–10940. doi: 10.1073/pnas.162282799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kinsler J. Evaluation of a school-based intervention for HIV/AIDS prevention among Belizean adolescents. Health Educ. Res. 2004;19(6):730–738. doi: 10.1093/her/cyg091. [DOI] [PubMed] [Google Scholar]
- Kirby DB, Laris BA, Rolleri LA. Sex and HIV education programs: their impact on sexual behaviors of young people throughout the world. J. Adolesc. Health. 2007;40(3):206–217. doi: 10.1016/j.jadohealth.2006.11.143. [DOI] [PubMed] [Google Scholar]
- Kockaya G, et al. Analysis of the treatment costs of HIV/AIDS in Turkey. Farmeconomia Health Econ. Ther. Pathw. 2016;17(1):13–17. doi: 10.7175/fe.V17i1.1219. [DOI] [Google Scholar]
- Korenromp EL, Bakker R, de Vlas SJ, et al. HIV dynamics and behaviour change as determinants of the impact of sexually transmitted disease treatment on HIV transmission in the context of the Rakai trial. AIDS. 2002;16:2209–2218. doi: 10.1097/00002030-200211080-00014. [DOI] [PubMed] [Google Scholar]
- Li Q, et al. Stability analysis of an HIV/AIDS dynamics model with drug resistance. Discrete Dyn. Nat. Soc. 2012 doi: 10.1155/2012/162527. [DOI] [Google Scholar]
- Luz PM, Cadeco CT, Massad E, Struchiner CJ. Uncertainties regarding dengue modeling in Rio de Janeiro, Brazil. Mem. Inst. Oswaldo Cruz. 2003;98:871–878. doi: 10.1590/S0074-02762003000700002. [DOI] [PubMed] [Google Scholar]
- Miller AN, Rubin DL. Factors leading to self-disclosure of a positive HIV diagnosis in Nairobi, Kenya: people living with HIV/AIDS in the Sub-Sahara. Qual. Health Res. 2007;17:586–598. doi: 10.1177/1049732307301498. [DOI] [PubMed] [Google Scholar]
- Mills CE, Robins JM, Lipsitch M. Transmissibility of 1918 pandemic influenza. Nature. 2004;432:904–906. doi: 10.1038/nature03063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morin SF, Koester KA, Steward WT, et al. Missed opportunities: prevention with HIV-infected patients in clinical care settings. J. Acquir. Immune Defic. Syndr. 2004;36:960–966. doi: 10.1097/00126334-200408010-00010. [DOI] [PubMed] [Google Scholar]
- Ramchandani SR, Mefta SH, Saple DG, Vaidya SB, Pandey VP, Vadrevu R, et al. Knowledge, attitudes, and practices of antiretroviral therapy among HIV-infected adults attending private and public clinics in India. AIDS Patient Care STDS. 2007;21:129–142. doi: 10.1089/apc.2006.0045. [DOI] [PubMed] [Google Scholar]
- Rudnick SN, Milton DK. Risk of indoor airborne infection transmission estimated from carbon dioxide concentration. Indoor Air. 2003;13:237–245. doi: 10.1034/j.1600-0668.2003.00189.x. [DOI] [PubMed] [Google Scholar]
- Sayan M, Willke A, Ozgunes N, Sargin F. HIV-1 subtypes and primary antiretroviral resistance mutations in antiretroviral therapy naïve HIV-1 infected individuals in Turkey. Jpn. J. Infect. Dis. 2013;66:306–311. doi: 10.7883/yoken.66.306. [DOI] [PubMed] [Google Scholar]
- Sayan M, et al. HIV-1 transmitted drug resistance mutations in newly diagnosed antiretroviral-naïve patients in Turkey. AIDS Res. Human Retrovir. 2016 doi: 10.1089/aid.2015.0110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomson C, Currie C, Todd J, Elton R. Changes in HIV/AIDS education, knowledge and attitudes among Scottish 15–16 year olds, 1990–1994: findings from the WHO: Health Behaviour in school-aged Children Study (HBSC) Health Educ. Res. 1999;14:357–370. doi: 10.1093/her/14.3.357. [DOI] [PubMed] [Google Scholar]
- Vithayachockitikhun N. Family caregiving of persons living with HIV/AIDS in Thailand: caregiver burden, an outcome measure. Int. J. Nurs. Pract. 2006;12:123–128. doi: 10.1111/j.1440-172X.2006.00560.x. [DOI] [PubMed] [Google Scholar]
- White RG, Orroth KK, Korenromp EL, et al. Can population differences explain the contrasting results of the Mwanza, Rakai, and Masaka HIV/sexually transmitted disease intervention trials: a modeling study. J. Acquir. Immune. Defic. Syndr. 2004;37:1500–1513. doi: 10.1097/01.qai.0000127062.94627.31. [DOI] [PubMed] [Google Scholar]
- Wolf MS, Davis TC, Cross JT, Marin E, Green K, Bennett CL. Health literacy and patient knowledge in a Southern US HIV clinic. Int. J. STD AIDS. 2004;15:747–752. doi: 10.1258/0956462042395131. [DOI] [PubMed] [Google Scholar]
- Wonham MJ, de-Camino-Beek T, Lewis MA. An epidemiological model for West Nile Virus: invasion analysis and control applications. Proc. R. Soc. Lond. B. 2004;271:501–507. doi: 10.1098/rspb.2003.2608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woolhouse MEJ, Anderson RM. Understanding the epidemiology of BSE. Trends Microbiol. 1997;5:421–424. doi: 10.1016/S0966-842X(97)01146-3. [DOI] [PubMed] [Google Scholar]