

Abstract
Groundwater through hand-operated tubewell (a type of water well) tapping is the main source of drinking water in Bangladesh. This study investigated iron and manganese concentration in groundwater across Jashore district–one of the worst arsenic contaminated area in Bangladesh. One working tubewell that had been tested previously for arsenic and marked safe (green) was selected from each unions of the district. Results revealed that approximately 73% and 87% of groundwater samples exceeded the limits for iron and manganese in Bangladesh drinking water, respectively. Additionally, spatial distribution of iron and manganese indicate that only 5% of the total surface area of groundwater is covered by safe level of iron and manganese. Human health risk due to ingestion of iron and manganese through drinking water was evaluated using hazard quotients (HQ) for adults and children. The result of the health risk assessment revealed that the non-carcinogenic health risks due to ingestion of iron (HQ up to 1.446 for adults and 0.590 for children) and manganese (HQ up to 2.459 for adults and 1.004 for children) contaminated groundwater are much higher among adults than children. On the basis of occurrences, spatial distribution and health risk assessment results, the area can be categorized as a high-risk zone for iron and manganese-related problems and needs special attention in order to protect public health of local residents.
Subject terms: Environmental chemistry, Environmental impact
Introduction
Groundwater is the main source of drinking water in Bangladesh and over 90% of the country’s drinking water source is groundwater. Now, it is estimated that close to 98% of the population of Bangladesh have access to ‘technologically improved water source’ but this level is likely lower than 39% when considering Sustainable Development Goal water target (SDG goal 6.1)1 of ‘safely managed water’2. Safely managed water services ensure access to a technologically improved water source which is available when needed, located on premises and free of fecal and priority chemical contamination.
In Bangladesh, access to technologically improve water source came mainly due to installation of tubewells–a type of water well, a low-cost technology used to withdraw groundwater by hand powered. Since their large scale installation in the 1970s and 1980s for obtaining microbiologically safe water, tubewells have become popular in Bangladesh, with close to 95% of rural people and 70% of urban people using them today3. Even though groundwater can be a safe and reliable source of drinking water, it can also be affected by geogenic contaminants, such as arsenic, iron and manganese. Therefore, increased consumption of groundwater in some area has led to long-term exposures to arsenic4, iron5 and manganese6,7 that are associated with adverse health effects.
Iron and manganese are naturally occurring metals, and coexist in groundwater as they have many common chemical properties including similar valence charge in physiological conditions, ionic radius and absorptive mechanisms for individuals8,9. Iron and manganese are essential elements required for proper body function. The World Health Organization (WHO) has established secondary or aesthetic based water guideline of iron as 0.3 mg/L, and derived a health-based drinking water guideline value of manganese as 0.4 mg/L10. Similarly, for aesthetic, economic, and health-related reasons, Bangladesh has established standards of 0.3 to 1.0 mg/L for iron and 0.1 mg/L for manganese. Manganese is ubiquitous in common foods, and its deficiency is rare in humans. Generally, dietary manganese intake greatly exceeds that from drinking water. In rural Bangladesh, it was speculated that high body iron stores were due to high levels of iron in the groundwater11. However, overexposure to these metals can cause adverse health risks including, parkinson disease, huntington disease, cardiovascular disease, hyperkeratosis, diabetes mellitus, pigmentation changes, alzheimer disease, kidney, liver, respiratory and neurological disorders6,12–14. According to the National Drinking Water Quality Survey (NDWQS) in 200915, approximately 70% and 61% of drinking water sources in Bangladesh(n = 2896), mainly groundwater, have been found to contain elevated level of iron (>0.3 mg/L) and manganese (>0.1 mg/L), respectively. However, the same survey results revealed that arsenic in only 8% of the samples exceeded the Bangladesh standard (0.05 mg/L)16, while 18% exceeded the WHO guideline value (0.01 mg/L)10. As a result, tubewell water contain safe level of arsenic may contain elevated level of iron and manganese. The British Geological Survey (BGS) of Groundwater Studies of Arsenic Contamination in Bangladesh— a systematic survey of 61 of the 64 districts of Bangladesh, also identified elevated and variable level of iron and manganese in tubewells water4. The survey results revealed that average (minimum, maximum) iron and manganese concentration (mg/L) were 2.81(0.027, 10.5) and 0.38(0.39, 2.6), respectively in Jashore district4. According to the NDWQS survey of 200915, 42% and 80% of tubewells (n = 43) in Jashore district contain iron and manganese, respectively, above Bangladesh drinking water standards. In Bangladesh, testing of tubewell water is not mandated by regulations; therefore, tubewell water is not monitored consistently. Since 1993, the first detection of arsenic in groundwater in Bangladesh, the Government with help from international and national organizations, has tried to inform people about the presence of arsenic in drinking water and associated health risk. Several actions have already been taken to provide access to safe (As < 0.05 mg/L) drinking water in arsenic contaminated areas mainly through the installation of tubewells at targeted deeper depth aquifer2. However, iron and manganese issues have attracted relatively less attention so far for safe water supply2.
The objectives of this study are to investigate the level of iron and manganese in tubewells water which contain safe level of arsenic in Jashore district of Bangladesh, and assess the health risk of the exposure of the local residents to iron and manganese. This study also uses geographic information system (GIS) for the identification of risk areas. Groundwater through tubewell tapping is the main source of drinking and cooking water in the study area. Therefore, this study has great importance for the identification of options for groundwater remedy and management to protect public health.
Materials and Methods
Study area, tubewells selection and sample collection
This study was performed in Jashore district with an area of ~2,606 km2 and an estimated population of 2,764,547 located in the rural southwestern part of Bangladesh (Fig. 1). Similar to other area of Bangladesh, groundwater is the main source of drinking water in this district. The arsenic contamination in this district’s groundwater is among the worst in the country. One working tubewell that had been tested previously for arsenic and found safe level of arsenic (As < 0.05 mg/L) was selected for water sampling from each unions (the smallest rural administrative and local government units in Bangladesh) of the district. Some other specific criteria to select the tubewells were: operating full year round, installed in public place, heavily used (more than 20 households depends on it), and mainly used for drinking purposes. Finally, a total of 85 out of 93 unions of the district were selected for water sampling (Fig. 1). A majority of the tubewells (n = 48, 56%) were installed within 10 years of the survey (median (interquartile range, IQR) year of installation: 2008 (2001, 2012)). Median (IQR) depth (feet) was 180 (160, 200). The samples were collected from January through March 2017. Eight unions were excluded in this study due to water logging in those unions during sampling time; the selected tubewells not function and people of those unions used drinking water from nearby unions. Geographical positions were recorded during the sampling by using GPS. Tubewells water samples were collected directly from the tubewell water flow in high density polyethylene (HDPE) bottles (1 L) after 5 or 8 min pumping, depending on depth, in a steady stream of water to reach the aquifer water source. The samples were acidified to pH <2.0 at sampling location using 2 mL of nitric acid (69% pure, ACS reagent grade, Sigma-Aldrich) and transferred to the laboratory for analysis.
Figure 1.

Location map of the study area (Jashore District) and distribution of sampling points.
Sample analysis
All the samples for laboratory analysis were filtered through Whatman® glass microfiber filters (Grade GF/B: 1.0 μm) before analysis. Iron and manganese were measured by the FerroVer® (HACH method 8008) and PAN (HACH method 8149) method, respectively, using a HACH DR/3900 Spectrophotometer (HACH, USA).The detection limit of the method is 0.02 to 3.0 mg/L for iron, and 0.01 to 0.7 mg/L for manganese. All glassware used in the experiments was thoroughly cleaned with 1% HNO3 (ACS reagent grade, Sigma-Aldrich). Double distilled water was used for standard preparation and sample dilution. Reagent blanks and replicate samples were performed during analysis.
Statistical analysis and GIS
Statistical analysis, including box and whisker plots, and frequency distribution were performed using R Studio (with R version 3.5.1, www.rstudio.com), and figures were generated using ggplot2 (version 3.1.0). In order to process geographical data and make related calculations, the software QGIS version 2.2.0-Valmiera was used. The inverse distance weighting (IDW) method was chosen for interpolation.
To explore the distribution of iron and manganese concentration in the study area, three scale categories defined as ‘minimal’, ‘elevated’ and ‘high’ were used based on established recommendations for iron and manganese in water and daily dietary intake (Table 1). Tubewells were defined as having ‘minimal’ iron and manganese if they were below the WHO aesthetic limit for iron (0.3 mg/L) and Bangladesh standard for manganese (0.1 mg/L) in drinking water, respectively. Tubewells with iron and manganese concentration above Bangladesh drinking water standard but bellow the Joint FAO/WHO Expert Committee on Food Additives (JECFA) defined limit (2.0 mg/L for iron and 0.4 mg/L for manganese) are defined as ‘elevated’17,18. The JECFA limit was established by allocating 10% and 20% of the intake to drinking water for iron and manganese, respectively, defined as 0.8 mg iron/kg and 0.2 mg manganese/kg of body weight assuming average body weight of 60 kg and daily water consumption of 2 L17,18. Tubewells were defined ‘high’ levels of iron and manganese if the iron and manganese concentrations were greater than 2.0 mg/L and 0.4 mg/L, respectively.
Table 1.
Distribution of 85 tubewells manganese and iron concentration categories based on Bangladesh, WHO and JECFA drinking water quality guideline.
| Category | N (%) | Mean | Min | Max | Median | IQR | |
|---|---|---|---|---|---|---|---|
| Manganese (mg/L) | Minimal (0–<0.1a) | 11 (13%) | 0.05 | 0.02 | 0.08 | 0.04 | 0.03, 0.06 |
| Elevated (0.1–0.4b) | 36 (42%) | 0.22 | 0.11 | 0.36 | 0.21 | 0.16, 0.27 | |
| High (>0.4) | 38 (45%) | 0.93 | 0.40 | 2.11 | 0.78 | 0.55, 1.07 | |
| Iron (mg/L) | Minimal (0–<0.3c) | 23 (27%) | 0.14 | 0.02 | 0.29 | 0.15 | 0.08, 0.20 |
| Elevated (0.3–2.0d) | 38 (45%) | 0.75 | 0.31 | 1.94 | 0.65 | 0.39, 0.98 | |
| High (>2.0) | 24 (28%) | 3.72 | 2.10 | 6.20 | 3.56 | 2.97, 4.40 |
Health risk assessment
In this study, health risk assessment method proposed by United States Environmental Protection Agency (US EPA)19 was used and population exposed to iron and manganese contaminated groundwater by ingestion via drinking tubewells water was considered. Iron and manganese are both non-carcinogens according to the division of toxicants, as suggested by US EPA. Non-carcinogenic human health risk associated with ingesting iron or manganese was assessed according to a hazard quotient (HQ)19 as Eq. (1):
| 1 |
where RfD (mg/kg/day) is the reference dose of iron or manganese as suggested by US EPA (0.7 mg/kg/day for iron20 and 0.14 mg/kg/day for manganese18, respectively). CDI is the chronic daily intake19 of iron or manganese (mg/kg/day), and calculated using Eq. (2):
| 2 |
where C is the iron or manganese concentration in groundwater (mg/L); IR is the human water ingestion rate in L/day (3.53 L/day for adults21 and 1.0 L/day for children19); ED is the exposure duration in years (70 years for adults and 6 years for children19); EF is the exposure frequency in days/year (365 days for adults and children); BW is the average body weight in kg (50 kg for adults22 and 15 kg for children19), and AT is the averaging time (AT = 365 × ED(d)).
Based on the HQ values, no significant health risk of non-carcinogenic effects is anticipated if the value is less than one (HQ < 1). However, in the case of HQ value that exceeds one (HQ > 1), residents are exposed to non-carcinogenic health risk. For the risk assessment of iron and manganese in combination in the drinking water, a hazard index (HI) was employed by summing the calculated HQ values of iron and manganese.
A HI of less than one (HI < 1) means iron and manganese are unlikely to cause adverse non-cancer health effects over a lifetime of exposure. However, HI greater than one (HI > 1) mean adverse non-cancer health effects are likely.
Results and Discussion
Iron and manganese in groundwater
As mentioned above, this study focused on iron and manganese concentration in 85 tubewells water with safe level of arsenic (As < 0.05 mg/L) across Jashore district (Fig. 1). The tubewells iron concentrations showed a wide range (0.02 to 6.2 mg/L) with a median iron concentration of 0.69 mg/L and inter quartile range 0.27 to 2.47 mg/L (Fig. 2). Approximately 73% of the tubewell water exceeded the limit for iron of which 45% were defined as ‘elevated’ and 24% were defined as ‘high’ —JECFA provisional maximum tolerable daily intake for iron in water (Table 1; Fig. 3). The maximum value of iron and manganese were nearly 20 and 21 times higher than the lower limit of Bangladesh standard of iron (0.3 to 1.0 mg/L) and manganese (0.1 mg/L), respectively. The mean value of iron was 1.4 mg/L, which was 4.6 times that of iron limit. The results are in agreement with elevated and variable levels of iron in tubewells water in Bangladesh15,17. Merrill et al. (2010)5 found iron concentration in a northeastern Bangladesh to be higher (median = 7.6 mg/L, inter quartile range = 1.6 to 17.6 mg/L) than this study. Elevated level of iron (3.9 to 10.5 mg/L) was previously reported from a small village in Jashore district23.
Figure 2.
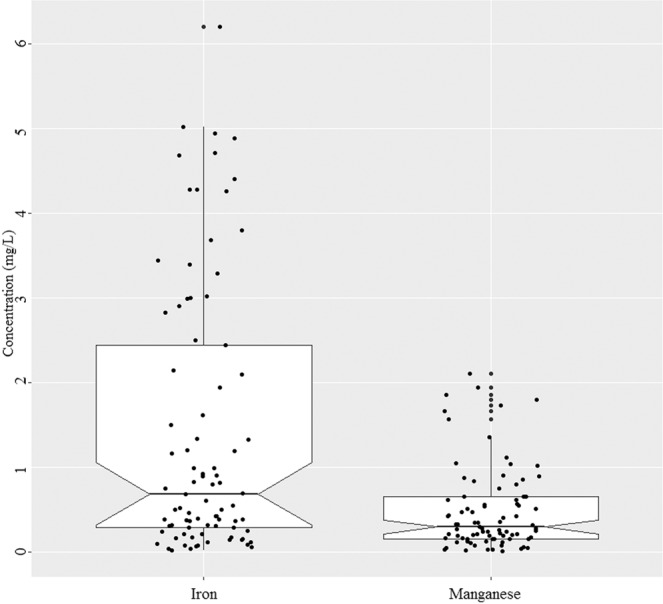
Notched box plot of iron and manganese concentration in the tubewells water (n = 85). The box bounds the interquartile range (IQR) divided by the median and whiskers extend to 1.5 × IQR beyond the box. The notch top and bottom indicate a 95% confidence interval (CI) for the median. Small disks represent the individual data points.
Figure 3.
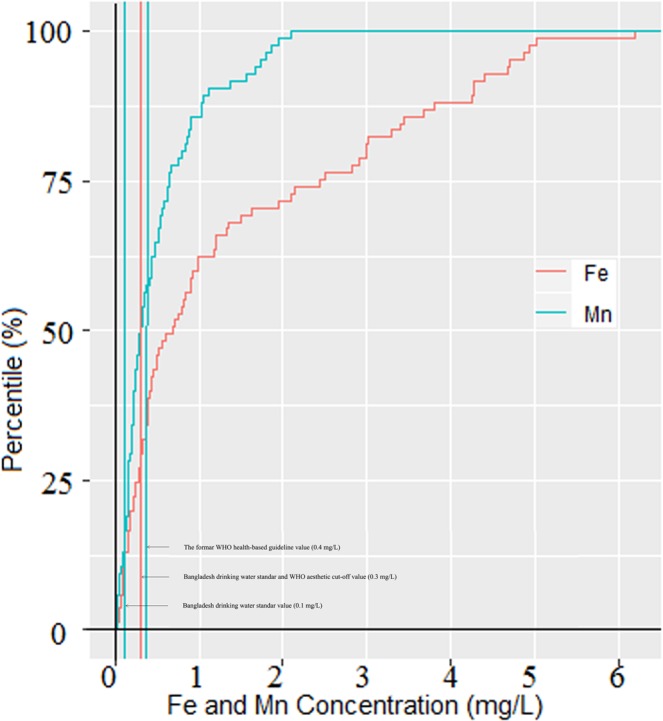
Cumulative frequency plot for tubewells iron and manganese concentration (n = 85).
The tubewells manganese concentrations also showed a wide range (0.016 to 2.108 mg/L) with a median concentration of 0.298 mg/L and inter quartile range 0.162 to 0.654 mg/L (Fig. 2). The mean value of manganese was 4.7 times higher than the Bangladesh standard of 0.1 mg/L, but remained slightly high to the former WHO health guideline of 0.4 mg/L. Similar to iron, a majority of the tubewells (87%) had manganese concentrations higher than the Bangladesh standard (0.1 mg/L) and only 13% of tubewells had ‘minimal’ (Table 1; Fig. 3). Many tubewells water have low iron levels but high manganese (Fig. 4). Other tubewells show the opposite relation: low manganese and high iron concentrations. However, there were no strong correlation between iron and manganese in the tubewells water (Fig. 4). A nationwide less densely sampled by British Geological Survey are in agreement with this result, where 74% of the wells water manganese concentration exceeded the limit4. Elevated levels of manganese were also reported in portions of Araihazar, Bangladesh24.
Figure 4.
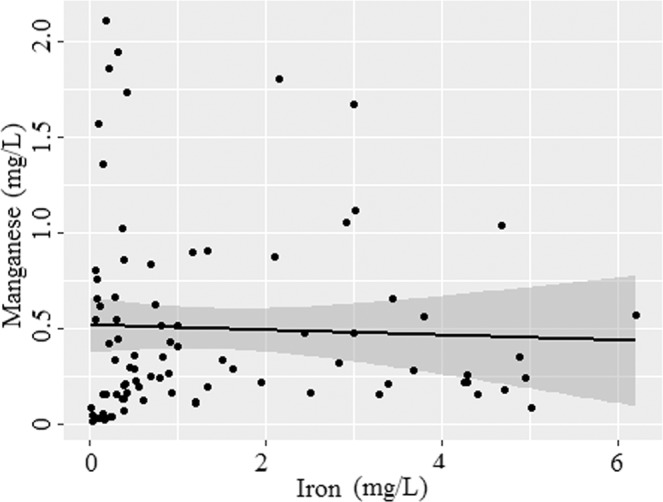
Manganese versus iron concentration in the tubewells water (n = 85). Solid line depicts the predicted relationship between iron and manganese; and shaded regions are the 95% confidence intervals.
Spatial distribution of iron and manganese
Figure 5 showed the spatial distribution of iron and manganese in the groundwater of Jashore district based on health related class boundaries. For iron, more than 75% of the total surface area of groundwater were covered by ‘elevated’ level of iron (0.3 to 2.0 mg/L) followed by ‘high’ level of iron (>0.2 mg/L) that covered 20% of the total surface, and only 5% covered by ‘minimal’ level of iron (<0.3 mg/L) (Fig. 5a). The ‘high’ levels of iron are distributed mostly in the southwestern and northeastern part of Jashore district. On the other hand, high level of manganese (>0.4 mg/L) covered 60% of the total surface area of the groundwater and distributed in the central and eastern part of the district (Fig. 5a). The ‘elevated’ level of manganese (0.1 to 0.4 mg/L) is distributed in the western and southern part of Jashore district and covered more than 35% of the total surface area of groundwater, and only less than 5% of the total surface is covered by ‘minimal’ level of manganese (<0.1 mg/L) that are distributed scatteredly in the southern part of the district (Fig. 5b). Moreover, only less than 5% of the total surface area is covered by ‘minimal’ level of both iron and manganese.
Figure 5.

Spatial distribution maps of (a) iron and (b) manganese in the groundwater of Jashore district.
Assessment of human health risks
In this study, only oral ingestion of iron and manganese through drinking tubewells water was taken into consideration for adults and children health risk assessment. The results of the risk assessment (HQ) are presented in Fig. 6. For adult, the HQ values for iron showed a wide range (0.004 to 1.446) with a median value of 0.161 and inter quartile range of 0.063 and 0.576. As show in Fig. 6, HQ values of iron for adults were higher than 1 in around 8% tubewells (n = 7), which indicated adverse health effect, although iron in 28% of the tubewells exceeded the JECFA provisional maximum tolerable daily intake for iron in water (Table 1). The HQ values of iron for children also showed a wide range (0.002 to 0.590) with lower median value (0.066) and inter quartile range (0.026 to 0.235) than adults.
Figure 6.
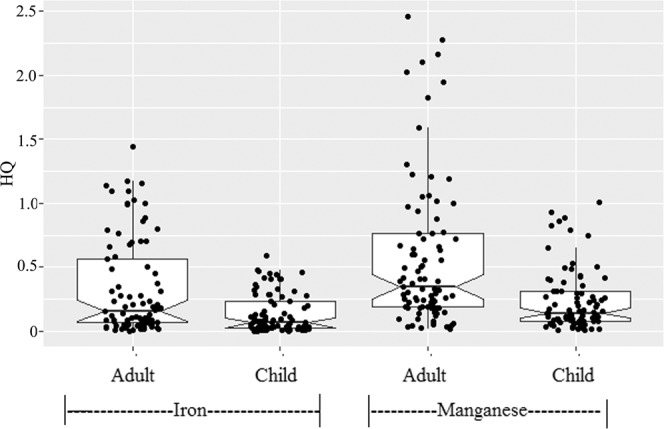
Notched box plot for non-carcinogenic hazard quotient (HQ) of iron and Manganese for different individuals. Boxplot details as in Fig. 2.
All HQ values of iron for children were less than 1 (Fig. 6), suggesting no potential non-carcinogenic health concerns among children. Iron in available form in drinking may provide nutritional benefit. Studies have shown that iron in drinking water that is highly bioavailable could be absorbed as high as 40%25–27. A study in Bangladesh suggested that a positive association between groundwater iron contents (between above or below 1 mg /L) and linear growth of children with iron deficiency28. However, excessive body iron may be an issue of concern because of a possible association with several chronic diseases, such as heart disease29–31 and diabetes32,33.
For adults, the HQ values for manganese showed a wide range (0.019 to 2.459) with a median value of 0.348 and inter quartile range of 0.186 and 0.764. As for manganese, the HQ values for children are lower than adults, and the maximum value for children is 1.004. The HQ of manganese for child was more than 1 at only one tubewell but HQ values of manganese for adults were higher than 1 at sixteen tubewells, which indicated relatively high health risk. In the studied tubewells, manganese concentration exceeded the limit (0.1 mg/L) for Bangladesh drinking water in around 83% tubewells, whereas 45% of the tubewells exceeded the WHO guideline value (0.4 mg/L). Wasserman et al.6 showed a positive association between manganese concentrations higher than 0.4 mg/L and reduced intellectual function of children aged 10 years in Bangladesh. A cross-sectional study in Bangladesh also suggested infants exposed to drinking water manganese concentrations higher than 0.4 mg/L had increased mortality risk during the first year of life when compared with unexposed infants34. A recent study also showed a positive association between manganese concentrations in drinking water and reduced intellectual function of children ages 5.9–13.7 years in Canada7. As shown in Fig. 7, the HI values for children showed a wide range (0.165 to 1.650) with a median value of 0.407 and inter quartile range of 0.223 and 0.894. HI values for children were found higher than 1 (HI > 1) at three points, indicating possible health hazards in Jashore district with respect to the use of groundwater with elevated level of iron and manganese for children drinking purpose. For adults, around 39% of the tubewells (n = 33) showed HI values higher than 1, which indicate relatively high health threat (Fig. 6).
Figure 7.
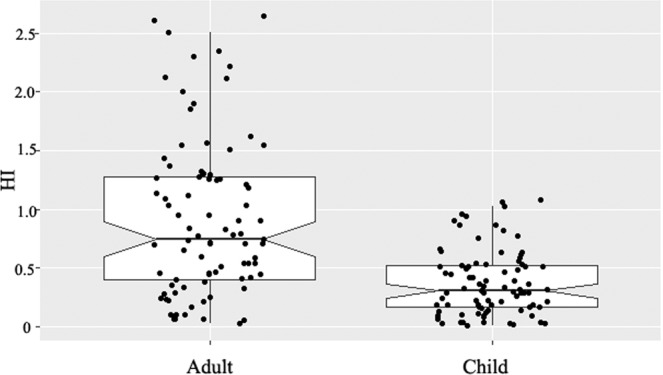
Hazard indexes of different individuals for iron and manganese. Boxplot details as in Fig. 2.
Limitations
In this study, tubewells which had been tested previously and marked safe (green; As <0.005 mg/L) was selected for water sampling to measure iron and manganese. We did not measure As concentration. The samples were collected only in dry season and no temporal variability was studied, which is a limitation of this study. Eight water logged unions were excluded and no attempt was made to go back at different times to collect sample as those areas experiencing seasonal water logging. Additionally, bioaccessibility of iron and manganese in groundwater was not measured and thus could not estimate actual iron and manganese exposure. Moreover, applying the risk assessment on these measurements are therefore even more compelling. We expressed non-carcinogenic risk of iron and manganese in terms of a hazard quotient (HQ), and hazard index (HI) for iron in combination with manganese. Elevated and variable level of iron and manganese in groundwater in Jashore, Bangladesh could represent a potential risk, but there is no way to establish that risk with any certainty. This study finding, associated with the absence of reports of iron and manganese deficiency in human, led us to conclude that the possible consequences of excess exposure to iron and manganese from groundwater deserve further attention.
Conclusions and recommendations
In this study, a total of 85 tubewells water samples were investigated to assess the iron and manganese concentrations in the groundwater of Jashore district, which is located in arsenic-polluted southwestern part of Bangladesh. Approximately 73% and 87% of the samples exceeded Bangladesh limits for iron and manganese in drinking water, respectively. The result of the health risk assessment revealed that the non-carcinogenic health risks due to ingestion of iron and manganese contaminated groundwater are much higher among adults than children. Additionally, other inorganic and organic contaminants in the groundwater may pose a threat to human health. Furthermore, it is necessary to consider the iron and manganese bioavailability in drinking water and in the rest of the human diet to integrate this value into a risk assessment. Therefore, it is important to communicate with people who intake these elements in the region to limit their consumption. Finally, special attention should be paid to reduce iron and manganese concentration in tubewells water with safe level of arsenic, and special measures need to be taken to protect children, the most vulnerable population, from iron and manganese toxicity. To improve this situation, several steps including periodical testing of tubewells water quality, increased awareness, entrepreneurial development and incentive to allow business to supply safe water at low cost, development of low cost household water treatment systems, appropriate water safety planning and strategies at the household level need to be taken to reduce the risk. Further research is needed to acquire a better understanding of the individual health risks associated with iron and manganese in drinking water sources.
Acknowledgements
This study was supported by Jashore University of Science and Technology. The authors would like to extend thanks to The World Academy of Science (TWAS) for instrumental facility under the COMSTECH-TWAS Joint Research Grants Programme (TWAS Ref: 13-371 RG/ENG/AS_C; UNISCO FR: 3240279207).
Author contributions
G.C.G. organized this study, conducted study design, performed the statistical analysis, drafted and revised the manuscript. J.H.K. contributed to laboratory analysis, prepared datasets, performed the statistical analysis and drafted the manuscript. T.K.C., S.Z. and A.H.M.E.K. contributed to prepared datasets and drafted the manuscript, H.T. provided input on the technical statements. All listed authors have read and approved the final manuscript. All authors contributed equally to this work.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Statistical Commission. Report of the Inter-Agency and Expert Group on Sustainable Development Goal Indicators, E/CN.3/2016/2/Rev.1, http://unstats.un.org/unsd/statcom/47th-session/documents/2016-2-SDGs-Rev1-E.pdf [accessed on 10 February 2020] (2016).
- 2.George, J. et al. Promising progress: a diagnostic of water supply, sanitation, hygiene, and poverty in Bangladesh: Main report. WASH Poverty Diagnostic. World Bank Group, Washington, DC, USA Available at: http://documents.worldbank.org/curated/en/152341520607754248/Main-report [accessed on 20 August 2019] (2018).
- 3.WHO. & UNICEF. Progress on drinking water, sanitation and hygiene: 2017 update and SDG baselines. World Health Organization (WHO), Geneva and the United Nations Children’s Fund (UNICEF), New York Available at: https://www.unicef.org/publications/index_96611.html [accessed on 10 August 2019] (2017).
- 4.BGS & DPHE. Arsenic contamination of groundwater in Bangladesh. Kinniburgh, D G and Smedley, P L (Editors). British Geological Survey Technical Report WC/00/19. British Geological Survey: Keyworth (2001).
- 5.Merrill RD, et al. Elevated and variable groundwater iron in rural northwestern Bangladesh. J. Water Health. 2010;8:818–825. doi: 10.2166/wh.2010.144. [DOI] [PubMed] [Google Scholar]
- 6.Wasserman GA, et al. Water manganese exposure and children’s intellectual function in Araihazar, Bangladesh. Environ. Health Perspect. 2006;114:124–129. doi: 10.1289/ehp.8030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kullar SS, et al. A benchmark concentration analysis for manganese in drinking water and IQ deficits in children. Environ. Int. 2019;130:104889. doi: 10.1016/j.envint.2019.05.083. [DOI] [PubMed] [Google Scholar]
- 8.Hem JD. Chemical factors that influence the availability of iron and manganese in aqueous systems. Geol. Soc. Am. Bull. 1972;83:443–450. doi: 10.1130/0016-7606(1972)83[443:CFTITA]2.0.CO;2. [DOI] [Google Scholar]
- 9.Davidson W. Iron and manganese in lakes. Earth-Sci. Rev. 1993;34:119–163. doi: 10.1016/0012-8252(93)90029-7. [DOI] [Google Scholar]
- 10.WHO. Guidelines for drinking-water quality. 4th edition. WHO, Geneva, Switzerland. Available at: https://apps.who.int/iris/bitstream/handle/10665/44584/9789241548151_eng.pdf?sequence=1 [accessed on 14 September 2019] (2011).
- 11.Merrill RD, et al. High prevalence of anemia with lack of iron deficiency among women in rural Bangladesh: a role for thalassemia and iron in groundwater. Asia Pac. J. Clin. Nutr. 2012;21:416–24. [PubMed] [Google Scholar]
- 12.Powers KM, et al. Parkinson’s disease risks associated with dietary iron, manganese, and other nutrient intakes. Neurology. 2003;60:1761–1766. doi: 10.1212/01.WNL.0000068021.13945.7F. [DOI] [PubMed] [Google Scholar]
- 13.Kell DB. Towards a unifying, systems biology understanding of large-scale cellular death and destruction caused by poorly liganded iron: Parkinson’s, Huntington’s, Alzheimer’s, prions, bactericides, chemical toxicology and others as examples. Arch. Toxicol. 2010;84:825–889. doi: 10.1007/s00204-010-0577-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Farina M, Avila DS, Da Rocha JBT, Aschner M. Metals, oxidative stress and neurodegeneration: a focus on iron, manganese and mercury. Neurochem. Int. 2013;62:575–594. doi: 10.1016/j.neuint.2012.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.UNICEF Bangladesh. Bangladesh national drinking water quality survey of 2009. Bangladesh Bureau of Statistics, Dhaka, Bangladesh Available at: https://washdata.org/sites/default/files/documents/reports/2019-06/Bangladesh-2009-MICS-water-quality-report.pdf. [accessed on 12 August 2019] (2011).
- 16.DPHE. Department of Public Health Engineering, Government of Bangladesh, http://old.dphe.gov.bd/index.php?option=com_content&view=article&id=125&Itemid=133. [accessed on 14 February 2020] (2018).
- 17.WHO. Guidelines for Drinking-Water Quality. WHO, Geneva, Switzerland (2004).
- 18.WHO. Guidelines for Drinking-Water Quality. WHO, Geneva, Switzerland (1984).
- 19.US EPA. Superfund Public Health Evaluation Manual. Washington, DC (1989).
- 20.US EPA 2006. Provisional Peer Reviewed Toxicity Values for Iron and Compounds (CASRN 7439-89-6): Derivation of Subchronic and Chronic Oral RfDs, EPA/690/R-06/020F. Superfund Health Risk Technical Support Center, U.S. Environmental Protection Agency, Cincinnati, OH (2006).
- 21.Milton AH, Rahman H, Smith W, Shrestha R, Dear K. Water consumption patterns in rural Bangladesh: are we underestimating total arsenic load? J Water Health. 2006;4:431–436. doi: 10.2166/wh.2006.0027. [DOI] [PubMed] [Google Scholar]
- 22.National Institute of Population Research and Training (NIPORT), Mitra and Associates & ICF International. Bangladesh Demographic and Health Survey 2011. Dhaka, Bangladesh and Calverton, Maryland, USA (2013).
- 23.Tanabe K, Yokota H, Hironaka H, Tsushima S, Kubota Y. Arsenic pollution of groundwater in Bangladesh. Appl. Organomet. Chem. 2001;15:241–251. doi: 10.1002/aoc.134. [DOI] [Google Scholar]
- 24.Cheng Z, Zheng Y, Mortlock R, Van Geen A. Rapid multi-element analysis of groundwater by high-resolution inductively coupled plasma mass spectrometry. Anal. Bioanal. Chem. 2004;379:512–518. doi: 10.1007/s00216-004-2618-x. [DOI] [PubMed] [Google Scholar]
- 25.Worwood M, Evans WD, Villis RJ, Burnett AK. Iron absorption from a natural mineral water (Spatone Iron-Plus) Clin. Lab. Haematol. 1996;18:23–27. doi: 10.1111/j.1365-2257.1996.tb00732.x. [DOI] [PubMed] [Google Scholar]
- 26.Halksworth G, Moseley L, Carter K, Worwood M. Iron absorption from Spatone (a natural mineral water) for prevention of iron deficiency in pregnancy. Clin. Lab. Haematol. 2003;25:227–231. doi: 10.1046/j.1365-2257.2003.00525.x. [DOI] [PubMed] [Google Scholar]
- 27.McKenna D, et al. A randomized trial investigating an iron-rich natural mineral water as a prophylaxis against iron deficiency in pregnancy. Clin. Lab. Haematol. 2003;25:99–103. doi: 10.1046/j.1365-2257.2003.00501.x. [DOI] [PubMed] [Google Scholar]
- 28.Briend A, Hoque BA, Aziz KM. Iron in tubewell water and linear growth in rural Bangladesh. Arch. Dis. Child. 1990;65:224–225. doi: 10.1136/adc.65.2.224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Salonen JT, et al. High stored iron levels are associated with excess risk of myocardial infarction in eastern Finnish men. Circulation. 1992;86:803–811. doi: 10.1161/01.CIR.86.3.803. [DOI] [PubMed] [Google Scholar]
- 30.Tuomainen TP, Punnonen K, Nyyssönen K, Salonen JT. Association between body iron stores and the risk of acute myocardial infarction in men. Circulation. 1998;97:1461–1466. doi: 10.1161/01.CIR.97.15.1461. [DOI] [PubMed] [Google Scholar]
- 31.Klipstein-Grobusch K, et al. Serum ferritin and risk of myocardial infarction in the elderly: the Rotterdam Study. Am. J. Clin. Nutr. 1999;69:1231–1236. doi: 10.1093/ajcn/69.6.1231. [DOI] [PubMed] [Google Scholar]
- 32.Tuomainen TP, et al. Body iron stores are associated with serum insulin and blood glucose concentrations: population study in 1,013 eastern Finnish men. Diabetes care. 1997;20:426–428. doi: 10.2337/diacare.20.3.426. [DOI] [PubMed] [Google Scholar]
- 33.Salonen JT, Tuomainen TP, Nyyssönen K, Lakka HM, Punnonen K. Relation between iron stores and non-insulin dependent diabetes in men: case-control study. BMJ. 1998;317:727–730. doi: 10.1136/bmj.317.7160.727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hafeman D, Factor-Litvak P, Cheng Z, van Geen A, Ahsan H. Association between manganese exposure through drinking water and infant mortality in Bangladesh. Environ. Health Perspect. 2007;115:1107–1112. doi: 10.1289/ehp.10051. [DOI] [PMC free article] [PubMed] [Google Scholar]