

Abstract
Background
That ventilator-associated pneumonia (VAP) can be reduced by continuous and/or intermittent subglottic suction highlights the importance of clearance of oropharyngeal secretions. We prospectively evaluated the usefulness of intermittent suction of oral secretions before each positional change in reducing VAP.
Methods
A time-sequence nonrandomized intervention design was used. The study consisted of a 9-month observation phase (control group, 237 patients), a 6-month education phase, followed by a 7-month intervention phase (studied group, 227 patients). The occurrence of VAP, duration of mechanical ventilation, length of intensive care unit (ICU) stay, and mortality were recorded.
Results
VAP occurred less frequently in the studied group (6 of 227 patients, 2.6%) than in the control group (26 of 237 patients, 11.0%; P < 0.001). The incidence rate of VAP in control and studied groups was 6.51 and 2.04 per 1000 ventilator days, respectively (P = 0.002). For VAP patients, the ventilator days were 28.8 ± 17.2 days and 20.2 ± 4.0 days (P = 0.009), respectively, and the length of ICU stay was 27.6 ± 17.0 days and 20.3 ± 4.0 days (P = 0.012), respectively, in the control and studied groups. Intermittent suction of oral secretions before each positional change was the only independent factor responsible for a decrease of VAP in the studied group after stepwise logistic regression analysis (P = 0.003).
Conclusions
Intermittent suction of oral secretions before each positional change may reduce VAP occurrence in ICU patients.
KEY INDEXING TERMS: Critical care, Mechanical ventilation, Oral secretions, Pneumonia, Ventilator-associated pneumonia
Ventilator-associated pneumonia (VAP) is a common nosocomial infection. The data from the National Nosocomial Infection Surveillance System indicated that VAP was the second most nosocomial infection, after urinary tract infection, affecting approximately 27% of all critical patients.1 In Europe, VAP and low respiratory tract infection accounted for 65% of all infections in the European Prevalence of Infection in Intensive Care Study.2 With the advances of improved diagnosis, treatment and prevention, VAP remains a significant cause of mortality.3 In addition, VAP is associated with increased morbidity and prolongs the duration of mechanical ventilation and the length of intensive care unit (ICU) stay and hospitalization, all of which impact medical resources and finances.4., 5., 6. It is estimated that a single VAP episode prolongs the duration of hospital stay by 6 to 30 days or even longer, and incurs additional medical expenses ranging from 5,000 to 40,000 U.S. dollars per patient.6., 7. Accordingly, effective prevention of VAP can be a life-saving and cost-effective measure.
Bacterial colonization of the aerodigestive tract and aspiration of contaminated secretions into the lower airways seem to be the 2 essential processes in the pathogenesis of VAP.3., 4., 8. Continuous or intermittent subglottic suction proves useful in reducing VAP in particular in early-onset VAP.9., 10. Because pooled secretions above inflated endotracheal tube cuff is thought as a major source of aspiration.11 These findings highlight that adequate clearance of oral secretions may be of value in reducing the occurrence of VAP.
Our hypothesis is that intermittent suction of oral secretions before each positional change may decrease the oral secretions pooling above the endotracheal tube cuff and aspiration of contaminated secretions, and consequently reduce the occurrence of VAP. The study was conducted prospectively in a combined medical and surgical ICU.
Methods
Patients and Study Setting
From January 2004 to October 2005, consecutive patients with an age of 18 years or over admitted to the combined medical and surgical ICU were potentially eligible for this study at Taipei Veterans General Hospital. The patients who had pneumonia, tracheostomy or endotracheal intubation, and mechanical ventilation >72 hours before ICU admission, those with endotracheal intubation and mechanical ventilation or admission <48 hours in ICU, and those without endotracheal intubation and mechanical ventilation in ICU were excluded.
The study consisted of a 9-month observation phase, a 6-month education phase, followed by a 7-month intervention phase. From January to September 2004, 237 patients who fulfilled the patient selection criteria were classified into control group (Figure 1A ). From October 2004 to March 2005, all nursing staffs in ICU were informed why the study would be done, how the staffs would execute the intervention, and why the compliance of the intervention would be maintained high enough. Change of body position every 2 hours except for routine mouth care in the early morning was the routine nursing protocols in our ICU. The intervention was suction of oral secretions before each positional change. Other suction of oral secretions was allowed if clinically indicated. The suction of oral secretions was performed to clear the oral secretions as completely as possible and the suction tube was not extended into the oropharyngeal space. Accordingly, the patients in the studied group received additional 11 times of suction of oral secretions. The compliance of intermittent suction of oral secretions was monitored by self-report and checked randomly by senior staff during the education phase. The intervention phase of the study was started from April 2005, because the compliance of the intervention was >8/11 times in every staff. From April to October 2005, there were 227 patients who met the selection criteria were classified into studied group (Figure 1B). The institute review board of Taipei Veterans General Hospital approved this study, and a written informed consent was obtained from all patients or patients’ next of kin before the study.
Figure 1.
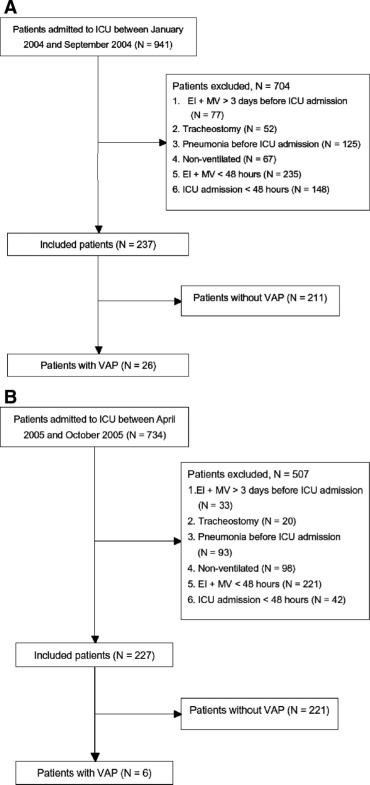
Flow diagram of patients in the control (A) and studied (B) groups. ICU, intensive care unit; EI, endotracheal intubation; MV, mechanical ventilation; VAP, ventilator-associated pneumonia.
During the period of intervention phase, the nursing staffs were reminded everyday to execute the intervention precisely and monitored closely by the senior staffs. The intervention was started when the patient admitted to the ICU, and was ended in case of 10 days after ICU admission, extubation, performance of tracheostomy or death in ICU, or discharged from ICU.
Semirecumbent position with head elevation of 30° or greater was part of nursing care protocols in our ICU except for those with contraindications. The only difference in nursing care protocols between control and studied groups was the intervention—suction of oral secretions before each positional change.
Data Collection and Definition
The following data were recorded: demographic data, primary reason for ICU admission, acute physiology and chronic health evaluation II score, occurrence of infection during hospitalization, use of antibiotics, and reported risk factors for VAP.3., 4. Outcome measures included occurrence and incidence rate of VAP, duration of mechanical ventilation, length of ICU stay, and mortality.
VAP was diagnosed based on the presence of new and/or progressive pulmonary infiltrates on chest radiographs plus 2 or more of the following criteria: fever (body temperature ≥38.3°C) or hypothermia (body temperature <36°C), leukocytosis (≥12 × 109/L), purulent tracheobronchial secretions, and Pao2/Fio2 ≤250 mm Hg in the last 48 hours in accordance with the definitions of the Centers for Disease Control and Prevention.12
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation. Statistical comparisons between 2 independent groups were performed by using Student t test or Mann–Whitney U test when appropriate. Comparisons of category data between the 2 groups were made using the χ2 test. All statistical tests were two-tailed. The independent factors for reducing VAP were assessed by stepwise logistic regression analysis. Significance was defined as P < 0.05. Statistical analysis was performed using SPSS version 13.0 (SPSS, Chicago, IL).
Results
In this study, there were 237 patients in the control group and 227 patients in the studied group. The demographic and clinical data between control and studied groups are summarized in Table 1 . There were no significant differences between the 2 groups except for more surgical patients were enrolled in the control group.
Table 1.
Demographic and Clinical Data between Control and Studied Groupsa
| Control Group, N = 237 | Studied Group, N = 227 | P | |
|---|---|---|---|
| Age, year | 68.1 ± 16.7 | 68.2 ± 16.2 | 0.913 |
| Gender, M/F | 170/67 | 153/74 | 0.311 |
| ICU ward, medical/surgical | 85/152 | 107/120 | 0.014 |
| Smoking, yes/no | 123/114 | 110/117 | 0.516 |
| Admission diagnosis Operation | |||
| Upper abdomen | 110 | 89 | 0.117 |
| Lower abdomen | 12 | 7 | 0.279 |
| Others | 13 | 13 | 0.910 |
| Acute respiratory failure | 14 | 17 | 0.495 |
| Cardiovascular diseases | 15 | 12 | 0.631 |
| Sepsis | 10 | 14 | 0.404 |
| Renal diseases | 8 | 12 | 0.310 |
| Liver diseases | 8 | 11 | 0.424 |
| UGI bleeding | 8 | 9 | 0.736 |
| CNS diseases | 15 | 16 | 0.756 |
| Others | 24 | 27 | 0.543 |
| Risk factors for VAP | |||
| COPD | 15 | 8 | 0.201 |
| DM | 32 | 40 | 0.249 |
| APACHE II score | 28.5 ± 5.9 | 28.1 ± 6.6 | 0.353 |
| Antacid/H2 blockers | 56 | 40 | 0.316 |
| Aerosol therapy | 43 | 24 | 0.372 |
| Corticosteroid | 43 | 51 | 0.251 |
| Sedation | 57 | 46 | 0.372 |
ICU indicates intensive care unit; UGI, upper gastrointestinal; CNS, central nervous system; VAP, ventilator-associated pneumonia; COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; APACHE, acute physiology and chronic health evaluation.
Data of mean ± SD or case number are given.
VAP occurred less frequently in the studied group (6 of 227, 2.6%) than in the control group (26 of 237, 11.0%; P < 0.001) (Table 2 ). Similarly, the incidence rate of VAP was significantly lower in the studied than in the control groups (2.04 versus 6.51 per 1000 ventilator days, P = 0.002). The onset of VAP ranged from 3 to 7 days with a median of 4 days in the control group and 4 to 7 days with a median of 5 days in the studied group. Of note, the duration of mechanical ventilator was significantly reduced in the studied group. The length of ICU stay also decreased in the studied group, however, the difference did not reach statistic significance.
Table 2.
Clinical Outcome between Control and Studied Groupsa
| Control Group, N = 237 | Studied Group, N = 227 | P | |
|---|---|---|---|
| Occurrence of VAP | 26 | 6 | <0.001 |
| Ventilator day | 19.0 ± 15.5 | 14.5 ± 11.8 | 0.004 |
| ICU stay, day | 18.2 ± 16.0 | 14.4 ± 11.8 | 0.057 |
| Hospital stay, day | 58.1 ± 58.8 | 58.7 ± 48.0 | 0.675 |
| Mortality | 51 | 40 | 0.290 |
VAP indicates ventilator-associated pneumonia; ICU, intensive care unit.
Data of mean ± SD or case number are given.
To determine the independent factors responsible for the reduction of VAP in the studied group, the variables with a P value ≤0.1 listed in Table 1 and the intervention, intermittent suction of oral secretions before each positional change were analyzed. After stepwise logistic regression analysis, intermittent suction of oral secretions before each positional change was the only independent factor for the reduction of VAP (OR = 0.250, 95% CI = 0.101–0.624, P = 0.003).
Comparisons of demographic and clinical data of VAP patients between the control and studied groups are shown in Table 3 . Compared with control group, the duration of mechanical ventilation and the length of ICU stay were significantly reduced in the studied group.
Table 3.
Comparisons of Patients with Ventilator-Associated Pneumonia between Control and Studied Groupsa
| Control Group, N = 26 | Studied Group, N = 6 | P | |
|---|---|---|---|
| Age, years | 73.2 ± 19.2 | 57.3 ± 26.5 | 0.337 |
| Gender, M/F | 21/5 | 5/1 | 0.883 |
| Ventilator day | 28.8 ± 17.2 | 20.2 ± 4.0 | 0.009 |
| ICU stay, day | 27.6 ± 17.0 | 20.3 ± 4.0 | 0.012 |
| Hospital stay, day | 51.0 ± 34.8 | 60.5 ± 42.5 | 0.558 |
| Mortality | 13 | 1 | 0.121 |
ICU indicates intensive care unit.
Data of mean ± SD or case number are given.
The potential pathogens of VAP yielded from cultures of endotracheal aspirates in control and studied groups are shown in Table 4 . No growth was found in 1 of 26 cases in the control group and in 2 of 6 in the studied group. The microorganisms yielded from the culture of endotracheal aspirates from VAP patients in this study were those appeared to be the pathogens of late-onset VAP, although none of VAP occurred 7 days after endotracheal intubation and mechanical ventilation.
Table 4.
Pathogens of Ventilator-Associated Pneumonia in Control and Studied Groupsa
| Potential Pathogen | Control Group, N = 26 | Studied Group, N = 6 |
|---|---|---|
| No growth | 1 (3.8) | 2 (33.3) |
| Stenotrophomonas maltophilia | 5 (19.2) | 1 (16.7) |
| Klebsiella pneumoniae | 3 (11.5) | 1 (16.7) |
| Pseudomonas aeruginosa | 2 (7.5) | |
| Acinetobacter species | 2 (7.5) | 2 (33.3) |
| Burkholderia cepacia | 2 (7.5) | |
| Escherichia coli | 1 (3.8) | |
| Enterobacter species | 1 (3.8) | |
| Serratia species | 1 (3.8) | |
| ORSA | 1 (3.8) | |
| PDRAB | 1 (3.8) | |
| MDRAB | 1 (3.8) | |
| Escherichia coli Klebsiella pneumoniae | 1 (3.8) | |
| MDRAB + Klebsiella pneumoniae | 1 (3.8) | |
| Pseudomonas aeruginosa + Burkholderia cepacia | 1 (3.8) | |
| ORSA + Pseudomonas aeruginosa | 1 (3.8) | |
| ORSA + MDRAB | 1 (3.8) |
Values given in parenthesis are percentage.
ORSA indicates oxacillin resistant Staphylococcus aureus; PDRAB, pan-drug resistant Acinetobacter species; MDRAB, multidrug-resistant Acinetobacter species.
The data of case number and (%) are given.
Discussion
The preliminary results indicated that intermittent suction of oral secretions before each positional change might significantly reduce VAP occurrence and incidence in ICU patients and the intervention was the only independent factor for the decrease of VAP. In addition, the duration of mechanical ventilation and the length of ICU stay of VAP patients were significantly reduced in the studied group. These findings suggest that intermittent suction of oral secretions before each positional change may be an attractive prevention measure of VAP.
There is a firm body of evidence that oropharyngeal colonization is pivotal in the pathogenesis of VAP. A link between increasing severity of illness, higher occurrence of oropharyngeal colonization and increased risk for the development of VAP was reported.13., 14. Subsequent studies confirmed that oropharyngeal colonization was a risk factor for VAP.15., 16. Further evidence was supported by the studies demonstrating a decrease in VAP occurrence and incidence by continuous and/or intermittent subglottic suction.9., 10., 17., 18. Accordingly, it is plausible that adequate clearance of oral secretions may be of value in reducing the oropharyngeal colonization and subsequent development of VAP.
In supporting this concept, our results showed that intermittent suction of oral secretions before each positional change could significantly reduce VAP occurrence (from 11.0% to 2.6%, P < 0.001) and incidence rate (from 6.51 to 2.04 episodes per 1000 ventilator days, P = 0.002) in ICU patients. For those with VAP, a significant decrease in the duration of mechanical ventilation and the length of ICU stay was found in the studied group (Table 2). The duration of mechanical ventilation and the length of ICU stay of VAP patients were decreased by 7 to 8 days, respectively, in the studied group. Taken together, intermittent suction of oral secretions before each positional change could reduce VAP occurrence and incidence and lessen the severity of VAP in ICU patients.
VAP remains a clinical challenge for the physicians involving in the critical care, despite an improved understanding and recent advances in the diagnosis, prevention and management strategies of the disease. VAP occurs in 9% to 27% of all intubated patients.3., 4., 6. In agreement with these reports, VAP occurred in 26 of 237 (11.0%) patients in our control group. The relatively low occurrence of VAP in this study may be explained in part by the following reasons. Hand hygiene and education for infection control were promoted more aggressively due to the impact of severe acute respiratory syndrome in Taiwan in 2003.19 Semirecumbent position with head elevation of 30° or greater, which proved useful in reducing VAP,4., 20. was part of routine care protocols in our ICU for years. Only early-onset VAP was found in this study.
There are some limitations in this study. First, this was not a randomized controlled study. The cases studied may not be large enough. The heterogeneity of the patients as the study conducted in a combined medical and surgical ICU may confound the results or the effect of intervention. The value of intermittent suction of oral secretions before each positional change in reducing late-onset VAP remains unknown because late-onset VAP was not found in this study. However, the results of the present study can be clinically relevant because all patients studied came from the same ICU and were treated with same protocol except for the intervention evaluated in the studied group. This may decrease or avoid inherent bias caused by different patient population, nursing protocols, and quality of medical and nursing staffs in particular in multicenter studies or in a study conducted simultaneously in different ICUs at a same hospital. Further prospective and randomized studies with larger population are needed to verify these issues.
In conclusion, intermittent suction of oral secretions before each positional change may significantly reduce VAP occurrence and incidence and decrease the duration of mechanical ventilation and the length of ICU stay in VAP patients. The clinical benefit of intermittent suction of oral secretions before each positional change needs further studies with larger population to verify.
Acknowledgments
The authors thank all medical and nursing staffs of ICU, Taipei Veterans General Hospital.
References
- 1.Richards M.J., Edwards J.R., Culver D.H. Nosocomial infections in medical intensive care units in the United States. National Nosocomial Infections Surveillance System. Crit Care Med. 1999;27:887–892. doi: 10.1097/00003246-199905000-00020. [DOI] [PubMed] [Google Scholar]
- 2.Vincent J.L., Bihari D.J., Suter P.M. The prevalence of nosocomial infection in intensive care units in Europe: results of the European Prevalence of Infection in Intensive Care (EPIC) Study. JAMA. 1995;274:639–644. [PubMed] [Google Scholar]
- 3.Chastre J., Fagon J.Y. Ventilator-associated pneumonia. Am J Respir Crit Care Med. 2002;165:867–903. doi: 10.1164/ajrccm.165.7.2105078. [DOI] [PubMed] [Google Scholar]
- 4.American Thoracic Society Guidelines for the management of adults with hospital-acquired, ventilator-associated pneumonia, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171:388–416. doi: 10.1164/rccm.200405-644ST. [DOI] [PubMed] [Google Scholar]
- 5.Papazian L., Bregeon F., Thirion X. Effect of ventilator-associated pneumonia on mortality and morbidity. Am J Respir Crit Care Med. 1996;154:91–97. doi: 10.1164/ajrccm.154.1.8680705. [DOI] [PubMed] [Google Scholar]
- 6.Rello J., Ollendorf D.A., Oster G. Epidemiology and outcomes of ventilator-associated pneumonia in a large US database. Chest. 2002;122:2115–2121. doi: 10.1378/chest.122.6.2115. [DOI] [PubMed] [Google Scholar]
- 7.Warren D.K., Shukla S.J., Olsen M.A. Outcome and attributable cost of ventilator-associated pneumonia among intensive care unit patients in a suburban medical center. Crit Care Med. 2003;31:1312–1317. doi: 10.1097/01.CCM.0000063087.93157.06. [DOI] [PubMed] [Google Scholar]
- 8.Estes R.J., Meduri G.U. The pathogenesis of ventilator-associated pneumonia. I. Mechanisms of bacterial transcolonization and airway inoculation. Intensive Care Med. 1995;21:365–383. doi: 10.1007/BF01705418. [DOI] [PubMed] [Google Scholar]
- 9.Vallés J., Artigas A., Rello J. Continuous aspiration of subglottic secretions in preventing ventilator-associated pneumonia. Ann Intern Med. 1995;122:179–186. doi: 10.7326/0003-4819-122-3-199502010-00004. [DOI] [PubMed] [Google Scholar]
- 10.Kollef M.H., Skubas N.J., Sundt T.M. A randomized clinical trial of continuous aspiration of subglottic secretions in cardiac surgery patients. Chest. 1999;116:1339–1346. doi: 10.1378/chest.116.5.1339. [DOI] [PubMed] [Google Scholar]
- 11.Oikkonen M., Aromaa U. Leakage of fluid around low-pressure tracheal tube cuffs. Anaesthesia. 1997;52:567–569. doi: 10.1111/j.1365-2044.1997.149-az0153.x. [DOI] [PubMed] [Google Scholar]
- 12.Garner J.S., Jarvis W.R., Emori T.G. CDC definitions for nosocomial infections. Am J Infect Control. 1988;16:128–140. doi: 10.1016/0196-6553(88)90053-3. [DOI] [PubMed] [Google Scholar]
- 13.Johanson W.G., Jr, Pierce A.K., Sanford J.P. Nosocomial respiratory infections with Gram-negative bacilli: the significance of colonization of the respiratory tract. Ann Intern Med. 1972;77:701–706. doi: 10.7326/0003-4819-77-5-701. [DOI] [PubMed] [Google Scholar]
- 14.Johanson W.G., Jr, Pierce A.K., Sanford J.P. Changing pharyngeal bacterial flora of hospitalized patients: emergence of gram-negative bacilli. N Engl J Med. 1969;281:1137–1140. doi: 10.1056/NEJM196911202812101. [DOI] [PubMed] [Google Scholar]
- 15.Bonten M.J.M., Bergmans D.C.J.J., Ambergen A.W. Risk factors for pneumonia, and colonization of respiratory tract and stomach in mechanically ventilated ICU patients. Am J Respir Crit Care Med. 1996;154:1339–1346. doi: 10.1164/ajrccm.154.5.8912745. [DOI] [PubMed] [Google Scholar]
- 16.Garrouste-Orgeas M., Chevret S., Arlet G. Oropharyngeal or gastric colonization and nosocomial pneumonia in adult intensive care unit patients: a prospective study based on genomic DNA analysis. Am J Respir Crit Care Med. 1997;156:1647–1655. doi: 10.1164/ajrccm.156.5.96-04076. [DOI] [PubMed] [Google Scholar]
- 17.Shorr A.F., O’Malley P.G. Continuous subglottic suctioning for the prevention of ventilator-associated pneumonia: potential economic implications. Chest. 2001;119:228–235. doi: 10.1378/chest.119.1.228. [DOI] [PubMed] [Google Scholar]
- 18.Smulders K., van der Hoeven H., Weers-Pothoff I. A randomized clinical trial of intermittent subglottic secretion drainage in patients receiving mechanical ventilation. Chest. 2002;121:858–862. doi: 10.1378/chest.121.3.858. [DOI] [PubMed] [Google Scholar]
- 19.Wang J.T., Sheng W.H., Fang C.T. Clinical manifestations, laboratory findings, and treatment outcomes of SARS patients. Emerg Infect Dis. 2004;10:818–824. doi: 10.3201/eid1005.030640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dodek P., Keenan S., Cook D. Evidence-based clinical practice guideline for the prevention of ventilator-associated pneumonia. Ann Intern Med. 2004;141:305–313. doi: 10.7326/0003-4819-141-4-200408170-00011. [DOI] [PubMed] [Google Scholar]