

Key Points
CAD causes complement-mediated hemolysis and anemia, which may necessitate blood transfusion therapy.
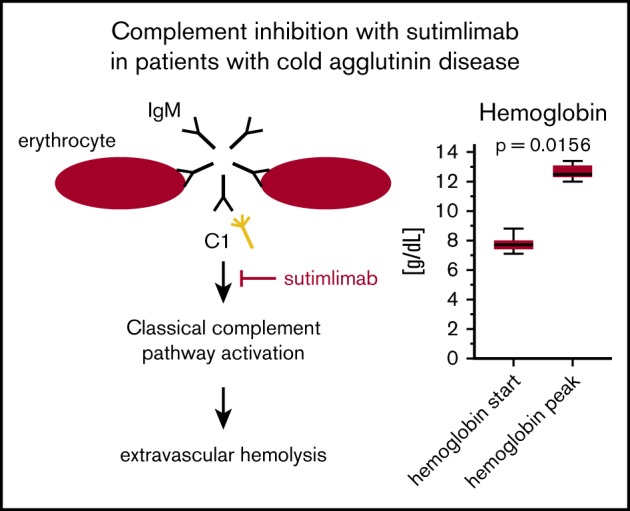
Sutimlimab precludes hemolysis and effectively increases hemoglobin levels in CAD patients without causing relevant adverse events.
Abstract
Cold agglutinin disease (CAD) causes predominantly extravascular hemolysis and anemia via complement activation. Sutimlimab is a novel humanized monoclonal antibody directed against classical pathway complement factor C1s. We aimed to evaluate the safety and efficacy of long-term maintenance treatment with sutimlimab in patients with CAD. Seven CAD patients treated with sutimlimab as part of a phase 1B study were transitioned to a named patient program. After a loading dose, patients received biweekly (once every 2 weeks) infusions of sutimlimab at various doses. When a patient’s laboratory data showed signs of breakthrough hemolysis, the dose of sutimlimab was increased. Three patients started with a dose of 45 mg/kg, another 3 with 60 mg/kg, and 1 with a fixed dose of 5.5 g every other week. All CAD patients responded to re-treatment, and sutimlimab increased hemoglobin from a median initial level of 7.7 g/dL to a median peak of 12.5 g/dL (P = .016). Patients maintained near normal hemoglobin levels except for a few breakthrough events that were related to underdosing and which resolved after the appropriate dose increase. Four of the patients included were eventually treated with a biweekly 5.5 g fixed-dose regimen of sutimlimab. None of them had any breakthrough hemolysis. All patients remained transfusion free while receiving sutimlimab. There were no treatment-related serious adverse events. Overlapping treatment with erythropoietin, rituximab, or ibrutinib in individual patients was safe and did not cause untoward drug interactions. Long-term maintenance treatment with sutimlimab was safe, effectively inhibited hemolysis, and significantly increased hemoglobin levels in re-exposed, previously transfusion-dependent CAD patients.
Visual Abstract
Introduction
Cold agglutinin disease (CAD) is a subtype of autoimmune hemolytic anemia (AIHA) in which cold-induced binding of antibodies directed against antigens on the erythrocyte surface causes hemolysis and anemia via complement activation.1 CAD is deemed a low-grade B-cell lymphoproliferative disorder (now termed “primary cold agglutinin-associated lymphoproliferative disorder”), bearing a vague morphologic resemblance to lymphoplasmacytic lymphoma (LPL)2,3 but with a distinct lack of the MYD88 L265P mutation.4 In secondary CAD, now referred to as cold agglutinin syndrome, the most common underlying conditions include overt malignancy, infection, and autoimmune diseases.5 Cold agglutinins are most often of the immunoglobulin M (IgM) antibody subtype2,6 and usually target the I-antigen on the surface of red blood cells.7 Clinical severity of CAD is primarily determined by the thermal amplitude of these cold agglutinins as opposed to their serum concentrations.8 Cardinal symptoms of patients with CAD are anemia (requiring transfusion therapy in severe cases), chronic fatigue, and acrocyanosis, caused by IgM-induced binding and agglutination of red blood cells, which leads to occlusion of arterioles and capillaries. Binding of cold agglutinins to the target antigen initiates the classical pathway of the complement system.9
C1 complexes with antigen-bound cold agglutinins lead to cleavage of C2 and C4. Together, C2b and C4b form the C3 convertase, which catalyzes the proteolysis of C3 into C3a, a potent anaphylatoxin,10 and C3b, an important factor of opsonization.11 Subsequently, C3b-coated red blood cells are sequestered by macrophages of the reticuloendothelial system in the liver, a process known as extravascular hemolysis,12-14 which is the main pathophysiological mechanism behind anemia in CAD.15,16 In addition, C5b-induced formation of the membrane attack complex can result in intravascular hemolysis, but it is tightly regulated by surface-bound, complement-inhibitory proteins CD55 and CD59.14,17 Inhibition of C5 with eculizumab attenuated hemolysis in patients with CAD (measured by lactate dehydrogenase [LDH] levels) but did not substantially increase hemoglobin levels.18 Other treatment approaches include rituximab monotherapy and fludarabine-rituximab and bendamustine-rituximab.19 However, these options offer only varying degrees of efficacy and differing response rates; in the case of immune chemotherapy, they can cause serious adverse events.20-23
In recent years, a new humanized monoclonal antibody, sutimlimab, has been introduced that is directed against C1s and results in upstream inhibition of the classical pathway of the complement cascade.24 Studies have evaluated the use of sutimlimab in both normal healthy volunteers and various patient groups.24-27
In the first-in-human trial, the effects of sutimlimab were tested in 10 CAD patients with promising results.25 A total of 4 once-per-week doses of sutimlimab 60 mg/kg effectively inhibited hemolysis. This was manifested by a rapid increase in hemoglobin levels by a median of 1.6 g/dL within the first week and 3.9 g/dL within 6 weeks, normalization of bilirubin levels within 24 hours in most patients, and normalization of haptoglobin levels in 4 patients within 1 week. In addition, sutimlimab treatment precluded the need for transfusions in all 6 previously transfusion-dependent patients. Infusions were administered over 1 hour and were well tolerated without a need for premedication. We hypothesized that the effects of sutimlimab could be maintained as a long-term treatment and that treatment at 2-week intervals between infusions would be feasible. CAD patients treated with sutimlimab as part of this phase 1B study25 were transitioned to a named-patient program (NPP) to allow continuous long-term maintenance treatment with this drug.
Methods
Patients who participated in the phase 1B trial of sutimlimab25 were given the chance to receive further CAD treatment with the study drug as part of an open-label, single-center NPP. The program was approved by the medical directorate of the Vienna General Hospital, and written informed consent was obtained from all patients. The initial phase 1B study was approved by the independent Ethics Committee of the Medical University of Vienna and the national competent authority (Austrian Agency for Health and Food Safety).25 The NPP was conducted at the Department of Clinical Pharmacology, Medical University of Vienna, between March 2016 and October 2017 and was performed in accordance with the Good Clinical Practice Guideline and the principles set forth in the Declaration of Helsinki. Data were collected only until the patients completed the NPP and were enrolled in an open label extension of the original sutimlimab trial. The primary aim was to evaluate the safety and efficacy of continuous long-term maintenance treatment with sutimlimab in patients with CAD.
Inclusion and exclusion criteria
Only CAD patients who participated in the phase 1B trial of sutimlimab and showed an appropriate response to treatment were eligible for enrollment in the NPP. Patients were excluded from the program if they showed persistent insufficient response to treatment with sutimlimab or experienced worsening of the underlying or concomitant condition.
Study design and treatment
All clinical procedures were conducted in the same manner and at the same investigational site as the phase 1B trial, but blood sampling for the purpose of monitoring efficacy and safety was reduced. Treatment was started with up to 4 once-per-week loading doses of sutimlimab, and patients received individually tailored biweekly (once every 2 weeks) maintenance doses starting with either 45 mg/kg, 60 mg/kg, or a fixed-dose regimen of 5.5 g. The weight-dependent dose regimens were chosen on the basis of the results of the first-in-human trial, in which once-per-week doses of 60 mg/kg completely suppressed the classical complement pathway activity for 2 weeks after the last dose, yet a dose of 30 mg/kg was insufficient.24 Because the minimally effective dose for a biweekly infusion regimen was not defined, we chose 45 mg/kg (and later on, 60 mg/kg) as the initial doses. Blood samples were taken before the study drug was administered to measure both hemoglobin levels and parameters indicative of hemolysis such as LDH, bilirubin, and haptoglobin. When a patient experienced drug washout or showed laboratory signs of breakthrough hemolysis, the dose of sutimlimab was increased. Sutimlimab was infused via an infusion pump over a period of 60 minutes without premedications. More information about the investigational drug can be found in the supplemental Data.
Two patients (002 and 004) received concomitant treatment with sutimlimab and rituximab. In patient 002, treatment with rituximab was initiated after pretreatment with sutimlimab for several months. In contrast, patient 004 received treatment with rituximab during a prolonged period of breakthrough hemolysis and drug washout under continuously increased bilirubin levels. When sutimlimab and rituximab were administered on the same day, the latter was given first with sutimlimab being administered shortly after.
Laboratory analysis
All laboratory assessments were performed by the central laboratory of the Medical University of Vienna. A complete blood count was performed to monitor hemoglobin changes. Complement activity was assessed by measurement of C4 and the surrogate parameter CH50 (quantitatively).28 The CH50 test is a global test to determine the functional complement activity. Haptoglobin, LDH, and bilirubin were measured to detect hemolysis. Blood samples were obtained either by fresh venipuncture or by using existing central lines (ports), and blood was immediately stored in prewarmed steel blocks to prevent ex vivo agglutination and hemolysis.
Safety and statistical analysis
Safety was assessed by regular physical examinations, measurement of vital signs, electrocardiogram, laboratory tests, and recording of adverse events, which were further classified as mild, moderate, or severe. Routine laboratory tests included hematologic tests, blood chemistry, coagulation tests, and urinalysis. Descriptive statistics (median and quartiles) were primarily used to analyze the data. Start hemoglobin and peak hemoglobin levels were compared by using a Wilcoxon signed-rank test.
Results
Seven patients (age 55 to 76 years) were included, all of whom suffered from cold-induced acrocyanosis and who tested positive for C3d in the direct antiglobulin test (Coombs test). The duration of sutimlimab treatment ranged from 2 to 20 months, and doses were tailored to the individual patient’s clinical and laboratory responses. Accordingly, the number of sutimlimab infusions varied between 6 and 43. Additional patient information is provided in Tables 1 and 2 (to further de-identify patients, the patient number does not reflect the number assigned during the trial). Three patients started with a dose of 45 mg/kg. This was infused once per week for a period of 4 weeks, which was then changed to biweekly infusions. An additional 3 patients were treated with 60 mg/kg; they received once-per-week sutimlimab for 2 weeks and were then switched to a biweekly treatment regimen. One patient received a fixed dose of 5.5 g of sutimlimab every other week throughout the NPP.
Table 1.
Patient characteristics and treatment information
| Patient | Weight at NPP start, kg | Additional hematologic diagnosis | Concomitant treatment | No. of infusions | Duration of NPP participation, mo | Highest dose received | Breakthrough on highest dose |
|---|---|---|---|---|---|---|---|
| 001 | 57 | LPL with CAS, active NHL | Ibrutinib | 6 | 2 | 3420 mg (60 mg/kg) | Yes |
| 002 | 75 | CAD/cancer | EPO (5000 IU 3 times per wk), rituximab | 11 | 5 | 4500 mg (60 mg/kg) | No |
| 003 | 63 | NA | NA | 9 | 3.5 | 3960 mg (60 mg/kg) | Yes |
| 004 | 75 | NA | Rituximab | 13 | 5.5 | 5.5 g | No |
| 005 | 60 | CAD after LPL | NA | 43 | 20 | 5.5 g | No |
| 006 | 75 | Mixed AIHA | NA | 43 | 20 | 5.5 g | No |
| 007 | 78 | CAD after LPL | EPO (10 000 IU 3 times per wk) | 20 | 9.5 | 5.5 g | No |
CAS, cold agglutinin syndrome; EPO, erythropoietin; NA, not applicable; NHL, non-Hodgkin lymphoma.
Table 2.
Characteristics of patients included in NPP
| Patient | Initial IgM level, mg/dL | IgM subtype | Monospecific Coombs test (at NPP start) | Cold agglutinin titer (at NPP start) |
|---|---|---|---|---|
| 001 | 1720 | κ and suspected λ | Anti-IgG–, anti-IgM++, anti-C3c+, anti-C3d+++ | 1:>1024 |
| 002 | 163 | Suspected κ | Anti-IgG–, anti-IgM–, anti-C3d++ | 1:32 |
| 003 | 229 | κ | Anti-IgG–, anti-IgM–, anti-C3d++ | 1:>1024 |
| 004 | 121 | Suspected κ | Anti-IgG–, anti-IgM–, anti-C3d++ | 1:>1024 |
| 005 | 93 | Paraprotein not excludable | Anti-IgG+, anti-IgM++, anti-C3d+++ | 1:256 |
| 006 | 22.5 | No signs of paraprotein | Anti-IgG–, anti-IgM+, anti-C3d+++ | 1:256 |
| 007 | NA | NA | Anti-IgG–, anti-IgM–, anti-C3d++ | 1:>1024 |
IgM level normal range, 40-230 mg/dL.
NA, not available.
Sutimlimab rapidly increased hemoglobin to near normal levels in all patients: hemoglobin levels rose from a median initial level of 7.7 g/dL to a median peak of 12.5 g/dL (P = .0156; Figure 1; supplemental Table 1). Patients maintained near normal hemoglobin levels and inhibition of hemolysis for the duration of the study, except for a few breakthrough events that were related to underdosing that resolved after the appropriate dose increase. Four of the patients were eventually treated with a 5.5-g fixed-dose regimen of sutimlimab once every other week. None of them experienced breakthrough hemolysis. Despite increasing hemoglobin and hematocrit levels, neither improvement nor worsening of acrocyanosis was detected.
Figure 1.

Response to sutimlimab. Start and peak/nadir levels of hemoglobin, bilirubin, LDH and haptoglobin. Box plots depict min-max (whiskers), quartiles (boxes), and median (horizontal lines).
Accordingly, sutimlimab decreased bilirubin levels from a median baseline level of 1.75 mg/dL to a median nadir of 0.4 mg/dL (Figure 1; supplemental Table 1). Furthermore, sutimlimab reduced LDH levels from a median initial level of 336 U/L to a median nadir of 177 U/L (Figure 1; supplemental Table 1). The median initial haptoglobin level of <12 mg/dL increased to a median peak level of 80 mg/dL under treatment with sutimlimab (Figure 1; supplemental Table 1). None of the patients required transfusions because of CAD.
Patient 006 was classified as having mixed AIHA because she intermittently tested positive for both IgM and IgG auto-antibodies in the Coombs test. She responded well to sutimlimab with her initial hemoglobin level of 7.1 g/dL, which increased to a peak of 12 g/dL, although her steady state level was ∼11 g/dL (Figure 2; supplemental Table 1).
Figure 2.

Laboratory course of patient 006. Patient 006 initially received 45 mg/kg (3.4 g once per week, then once every other week) of sutimlimab, and hemoglobin levels increased from 7.1 g/dL to 11.2 g/dL after 6 doses, when she experienced laboratory evidence of biochemical breakthrough. This prompted a subsequent dose increase to 60 mg/kg (4.3 g), which stopped hemolysis and stabilized hemoglobin levels. However, after 8 additional doses, breakthrough hemolysis re-occurred (increased bilirubin and LDH and decreased haptoglobin and C4), which led to a slight dose increase to 65 mg/kg preventing additional breakthrough events. Hemoglobin levels decreased significantly during repeated long washout periods (lengthy holiday and health treatment vacation). She was eventually assigned to a 5.5-g fixed-dose regimen, and after re-commencement of regular infusion therapy, the patient’s hemoglobin improved to a peak level of 11.4 g/dL. In week 75, her hemoglobin dropped to 6.1 g/dL which was a result of gastrointestinal bleeding after the re-operation of a diaphragmatic hernia. At that time, laboratory results revealed a sufficiently inhibited complement system (CH50, 30.8%; C4, 36 mg/dL) but no signs of hemolysis (bilirubin, 0.46 mg/dL; LDH, 213 U/L; and haptoglobin, 80 mg/dL). After transfusion of 4 erythrocyte concentrates, her hemoglobin rose to 10.2 g/dL and remained stable throughout her hospital stay. She continued with regular biweekly infusions of sutimlimab 5.5 g and her hemoglobin levels remained stable (blue arrows denote sutimlimab infusions).
Concomitant or overlapping treatments of interest
Two patients concomitantly received erythropoietin to enhance or accelerate the hemoglobin response while receiving treatment with sutimlimab (patient 002, Figure 3; patient 007, supplemental Figure 1). Patient 002 had a baseline erythropoietin level of 34.4 mU/mL and a corresponding hematocrit level of 27.9%. Patient 007 had a baseline erythropoietin level between 18.7 and 28.6 mU/mL and a corresponding hematocrit level of 22.4%. Doses of erythropoietin ranged between 4000 and 10 000 IU and were administered 3 times per week (the exact doses used are shown in Table 1, Figure 3, and supplemental Figure 1).
Figure 3.

Laboratory course of patient 002. Because of renal insufficiency, patient 002 was treated with erythropoietin 5000 IU 3 times per week in addition to sutimlimab. This increased the speed with which her hemoglobin rose when compared with the phase 1 trial. She received 10 infusions of sutimlimab 60 mg/kg (4.5 g) over the course of 5 months. Her hemoglobin increased from 7.9 to 9.0 g/dL within 1 week and reached 13.4 g/dL after 9 weeks. Her participation in the NPP was terminated because of the diagnosis of a massive inoperable uterine cancer with unilateral hydronephrosis which required radiotherapy. After exclusion from the NPP, the patient received regular transfusions every 1 to 2 weeks. As part of a different study, the patient began treatment with rituximab 2 weeks before the last administered dose of sutimlimab. Although CD20+ cells decreased immediately and remained low over the course of treatment, she was not able to achieve an adequate clinical response. Approximately 1 year later, the patient developed sepsis after a stroke and subsequently died.
In 2 rituximab-naïve patients, the principle investigator decided to switch from sutimlimab to rituximab treatment because of unrelated severe health conditions with a high likelihood for future serious (but unrelated) adverse events, making early concurrent use of any investigational agent undesirable. One of these patients (002; Figure 3) was diagnosed with uterine cancer and required radiation therapy; the other patient (004; Figure 4) suffered from preexisting hydrocephalus and underwent surgical shunt implantation. Despite ongoing sutimlimab treatment, rituximab was able to deplete B cells from the circulation (Figure 4), but rituximab did not result in a sustained partial hematologic response (as defined by a >2 g/dL hemoglobin increase over baseline).
Figure 4.

Laboratory course of patient 004. At treatment initiation, patient 004 had a hemoglobin level of 7.4 g/dL. She was started on 45 mg/kg (3.4 g) sutimlimab which rapidly abrogated hemolysis and increased her hemoglobin level by 5.8 g/dL over the course of 4 weeks. Patient 004 experienced laboratory evidence of breakthrough hemolysis after the sixth and seventh doses of sutimlimab. However, when blood sampling was performed 1 week after the seventh dose of sutimlimab, the hemoglobin level was slightly increased and the bilirubin level normalized, suggesting that the treatment effect of sutimlimab was sufficient for at least 7 days but not sufficient for an interval of 14 days. This indicates that either the dose needed to be increased or the dosing interval needed to be decreased to achieve a sustained treatment effect. Despite underdosing, patient 004 was deliberately continued on 45 mg/kg of sutimlimab to allow for the detection of a putative beneficial effect of concomitantly started treatment with rituximab. The patient was eventually switched to a 5.5-g fixed-dose regimen, resulting in a rapid increase of hemoglobin and a decrease of bilirubin. Patient 004 experienced a washout of sutimlimab after the second fixed dose and her hemoglobin dropped to 9.2 g/dL. However, after 2 infusion cycles of sutimlimab, her hemoglobin promptly increased again to a level of 11.5 g/dL. During a scheduled checkup 2 weeks later, her hemoglobin level had further increased by 2.2 g/dL to a peak level of 13.7 g/dL, concluding the NPP. The investigator decided to discontinue treating this patient because she had repeated falls as a result of unrelated hydrocephalus, which required a shunt operation. In spite of a fifth dose of rituximab administered after the NPP, patient 004 could not maintain normal hemoglobin levels. Her hemoglobin levels decreased by more than 4 g/dL within 3 weeks to a level of 9.5 g/dL and then ranged from 7.7 to 10.2 g/dL over the following months, eventually reaching a nadir of 7.3 g/dL 8 months later.
After participating in the phase 1B sutimlimab trial, patient 001 started ibrutinib treatment for LPL. While receiving ibrutinib monotherapy, this patient developed a urinary tract infection, which triggered a hemolytic crisis; thus, the patient was temporarily restarted on concomitant sutimlimab (Figure 5). Patient 001 was the only patient who suffered from active underlying cancer (non-Hodgkin lymphoma) and consistently showed increased IgM levels. The remaining 6 patients showed normal IgM levels throughout the duration of the NPP. Further information (ie, duration of therapy) about concomitant treatments can be found in Figures 2-5 and supplemental Figures 1-3.
Figure 5.

Laboratory course of patient 001. To target the underlying lymphoplasmacytic lymphoma, patient 001 had been treated with ibrutinib since her participation in the phase 1B trial. Her initial hemoglobin level was 7.7 g/dL accompanied by distinct laboratory markers of hemolysis. After initiation of ibrutinib, her IgM levels started to decrease, and her bilirubin levels steadily increased. Hemoglobin levels continued to improve until the patient suffered a urinary tract infection, which triggered a hemolytic crisis and caused a sudden drop in hemoglobin level and a peak in bilirubin level. She was subsequently re-treated with sutimlimab 60 mg/kg (3.4 g) on top of antibiotic therapy and responded with normalization of bilirubin within 3 days, a 1.6 g/dL increase in hemoglobin within 6 days, and a complete normalization of anemia within 5 weeks. The patient’s haptoglobin levels remained below measurable limits, indicating fully compensated residual hemolysis. *In week 9, the patient presented with increased levels of bilirubin (1.49 mg/dL) and LDH (566 U/L), while still retaining a normal level of hemoglobin, which we therefore classified as early breakthrough hemolysis.
Safety
A total of 62 adverse events were reported throughout the duration of the NPP, most of which were of mild or moderate severity and which eventually resolved. Adverse events included gastrointestinal symptoms (10%), palpitations (6%), common cold (6%), sore throat (6%), and night sweats (5%). All adverse events but 1 were deemed unrelated or unlikely to be related to the investigational drug. One serious adverse event occurred (postoperative gastrointestinal bleeding described in Figure 2), but it was attributed to the re-operation of a diaphragmatic hernia and was therefore not considered related to the study drug.
Sutimlimab infusions were well tolerated without the need for premedication. There was no occurrence of any infusion-related symptoms. A detailed list of adverse events is provided in supplemental Table 2. The effects of sutimlimab in the other patients are depicted in supplemental Figures 2 and 3 showing laboratory evidence of breakthrough hemolysis in patients in whom sutimlimab was either underdosed or for whom the interval between infusions was too long to maintain adequate inhibition of the complement system (eg, after extended washout periods resulting from prolonged vacation).
Because there is an increased incidence of thromboembolic events in patients with CAD29 and a known interaction between complement and coagulation,30 we sought to depict the changes in D-dimer over time for all patients (supplemental Figure 4). Two of the patients had increased D-dimer levels at baseline. D-dimer levels decreased under continued long-term sutimlimab treatment in 1 of these patients (006), whereas D-dimer levels decreased after start of ibrutinib therapy in the patient with high tumor load (001). Although no clinical thromboembolic events occurred, spikes of D-dimer were associated with gastrointestinal bleeding (006), and breakthrough hemolysis (004).
Discussion
The NPP showed that biweekly infusion therapy with sutimlimab was safe, effectively abrogated complement-mediated hemolysis (Figure 3), and increased and maintained hemoglobin at near normal levels in all patients upon re-exposure. However, underdosing or prolonged washout periods invariably resulted in disease recurrence in all patients.
Pharmacokinetic and pharmacodynamic modeling (not shown) suggests a low but present risk of insufficient drug levels with the 5.5-g fixed-dose regimen in certain patients at the end of a 14-day treatment interval. To further reduce the risk of breakthrough hemolysis, higher doses of sutimlimab have been chosen for the 2 phase 3 trials (NCT03347396, NCT03347422).
Different biomarkers may be used to detect early breakthrough hemolysis: bilirubin was proven to be reliable, even at times when there was no notable drop in hemoglobin values. However, bilirubin may not be useful in patients with Gilbert’s disease or liver disease. LDH could be used in CAD patients; however, it is not a specific parameter of hemolysis, and LDH can be increased by underlying lymphomas. Haptoglobin presents the most sensitive marker of hemolysis, but some patients may have undetectable haptoglobin levels despite normal hemoglobin and bilirubin levels as part of ongoing residual hemolysis (eg, as a result of mechanical forces in the microcirculation caused by erythrocyte agglutination during acrocyanosis). Alternatively, serial measurements of C4 levels seem to be a relevant marker for breakthrough hemolysis (Figure 3) and may be useful when bilirubin cannot be interpreted. However, C4 levels must be read with caution, particularly in patients with paradoxical hemolysis, in which infection or trauma-induced hemolysis is caused by increased synthesis of classical complement pathway components, which result in false-normal C4 levels.31
Free hemoglobin was not used as a marker for hemolysis because we frequently observe falsely elevated levels (false positives) when a blood draw is complicated or prolonged, even in healthy volunteers. Conversely, physicians should be aware of reticulocytopenia in up to 20% of autoimmune hemolytic anemias.32 Normal reticulocyte counts were seen initially in 1 of our transfusion-dependent patients, and sutimlimab therapy unmasked the true degree of reticulocytosis, which increased by 75% within 24 hours. This indicates that C3b-positive reticulocytes are readily consumed until complement deposition is blocked.
Although sutimlimab substantially ameliorated anemia, two patients (002 and 007) required concomitant treatment with erythropoietin to optimize their hemoglobin response. Both suffered from renal insufficiency with inadequate erythropoietin levels relative to the degree of anemia (patient 002 suffered from uterine cancer, which obstructed the ureter and caused postrenal kidney failure; patient 007 suffered from renal insufficiency as a consequence of multiple previous chemotherapies). Thus, some patients might benefit from erythropoietin as an add-on therapy, which is currently being investigated.33
For 4 consecutive months, patient 004 received overlapping treatment with sutimlimab and the anti-CD20 antibody rituximab. Rituximab was infused once every 4 weeks and immediately depleted CD20+ cells (Figure 4). Interestingly, sutimlimab does not seem to impair the CD20-cell-killing ability of rituximab. Therefore, rituximab-induced complement attack on B cells may not be its driving mechanism of action in humans, as has previously been suggested.34 Hence, there may not be a negative drug-drug interaction apart from enhanced immunosuppression, although more data are needed.
Before ibrutinib treatment was initiated, patient 001 received 4 doses of sutimlimab as part of the previous phase 1B trial; however, hemoglobin levels did not improve. We speculate that this was a result of the patient not having an underlying extravascular hemolysis process, as indicated by normal bilirubin levels at baseline. This may be secondary to tumor-associated complement deficiency, because this patient had an active LPL (70% bone marrow infiltration before treatment with ibrutinib).34,35 Tumor-associated anemia improved after the start of ibrutinib treatment and hemoglobin levels steadily increased (Figure 5). Interestingly, bilirubin levels concomitantly increased, which could indicate resurgent complement-mediated hemolysis and/or liver toxicity by ibrutinib. Along with other tyrosine kinase inhibitors, ibrutinib treatment has been associated with hepatotoxicity.36,37 After ibrutinib treatment was initiated, our patient showed a slight increase in transaminase levels. However, there was a surge in bilirubin levels after a hemolytic crisis that was triggered by a urinary tract infection. To control the hemolysis, sutimlimab was re-started along with standard antibiotic therapy for the underlying infection. After treatment with sutimlimab was initiated, bilirubin normalized and hemoglobin increased. Although no definitive conclusions on cause and effect can be made solely on the basis of 1 patient, several lessons can be learned from this illustrative case.
First, some patients with CAD secondary to an underlying malignancy may experience tumor-associated hypocomplementemia that attenuates CAD-induced hemolysis. Clinicians should be aware of the potential replenishment of complement factors with a resurgence of hemolysis in patients who are receiving treatment for underlying lymphomas. Second, infections can cause hemolytic crises as a consequence of increased complement synthesis,31 and such hemolytic crises may not be prevented by tyrosine kinase inhibitors such as ibrutinib. Apart from the treatment of the underlying infection, the addition of sutimlimab might be a treatment option to counteract exacerbated hemolysis in such cases. Third, we demonstrate the first successful use of ibrutinib in a patient with LPL (MYD88: ENST00000396334:c.794T>C p.L265P.) and CAD. So far, there are no systematic studies examining the effect of ibrutinib in AIHA. Three recent case reports have described treatment success with ibrutinib in AIHA secondary to other hematologic malignancies (chronic lymphocytic leukemia and mantle cell lymphoma).38-40 However, the effect of ibrutinib in patients with primary CAD without a hematologic malignancy remains unknown.
Patient 006 was the only patient classified as having mixed AIHA. However, some uncertainty remains regarding the subtype of her diagnosis, because there are several definitions of mixed AIHA in the current literature.41 Of note, this patient tested positive only intermittently for IgG auto-antibodies in the Coombs test, which could mean that the IgG antibodies are not always or necessarily contributing to hemolysis in this patient.
Over an extended treatment period, sutimlimab up to 5.5 g continued to demonstrate a good safety and tolerability profile. Only mild or moderate adverse events were observed, most of them unrelated or not likely related to the investigational drug. Concomitant administration of erythropoietin was safe, and overlapping treatment with ibrutinib or rituximab did not render patients susceptible to infections or cause any apparent drug interactions.
A clear limitation of these findings is the small sample size, so that the eventual evaluation of the safety of sutimlimab and interactions of concomitant treatments for patients with such a rare condition as CAD will be a real-world postmarketing exercise. Another limitation is the uncertain efficacy of sutimlimab in patients with warm or mixed AIHA. Of the 3 patients from the initial phase 1B trial who did not adequately respond to study treatment, 1 had mixed AIHA and 2 suffered from active lymphoma. Complement inhibition may not be a suitable treatment strategy in such patients. Furthermore, because sutimlimab does not affect the production of cold agglutinins or their binding to erythrocyte antigens, CAD patients might still experience acrocyanosis. Another shortcoming of this NPP is the lack of measurement of pharmacokinetics and antidrug antibodies, which could have added to the understanding of breakthrough hemolysis events and explained the need for dose increases. To successfully undergo treatment with sutimlimab, regular venous access is required for infusion therapy. This may be difficult in some patients whose peripheral venous access is suboptimal, or it may necessitate implantation of a central venous access line. Definitive conclusions about the safety and drug interactions of sutimlimab are not possible because of limited exposure and sample size.
In conclusion, during this extended treatment period with the anti-C1s antibody sutimlimab, all CAD patients responded to re-treatment, and all patients reached normal hemoglobin levels at least once. Sutimlimab showed a good safety profile without the occurrence of infusion-related symptoms or drug-related serious adverse events. Overlapping treatment with erythropoietin, rituximab, or ibrutinib in individual patients was safe, caused no apparent drug interactions, and did not manifest an increased susceptibility to infections. C1s inhibition by sutimlimab seems to be an effective therapeutic strategy for long-term treatment of CAD patients.
Supplementary Material
The full-text version of this article contains a data supplement.
Acknowledgments
The authors thank Sabine Schranz and Sarah Ely for organizational support and Christa Drucker and Karin Petroczi for their technical assistance.
This work was supported by grant SFB54-P04 from the Austrian Science Funds (G.G.). The study drug and financial reimbursement for laboratory costs were provided by Sanofi.
The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Footnotes
Requests for data may be made by contacting Bernd Jilma by e-mail (bernd.jilma@meduniwien.ac.at).
Authorship
Contribution: B.J. and J.C.G. designed the trial; T.S., M.F., S.D., R.C., U.J., and C. Sillaber helped recruit patients; G.G., C. Schoergenhofer, N.B., and U.D. performed the research; G.G. and B.J. performed statistical analysis and interpreted the data; G.G. drafted the manuscript; and all authors helped critically revise the manuscript and approved the final version for publication.
Conflict-of-interest disclosure: U.G. received personal fees from True North Therapeutics, Amgen, Takeda, and AbbVie and grants and personal fees from Roche, Celgene, Gilead, Novartis, and True North Therapeutics. J.C.G. was an employee and stockholder of True North Therapeutics. B.J. received reimbursement for travel costs and scientific advice from True North Therapeutics. The remaining authors declare no competing financial interests.
Correspondence: Bernd Jilma, Department of Clinical Pharmacology, Medical University of Vienna, Währinger Gürtel 18-20, 1090 Vienna, Austria; e-mail: bernd.jilma@meduniwien.ac.at.
References
- 1.Pruzanski W, Shumak KH. Biologic activity of cold-reacting autoantibodies (first of two parts). N Engl J Med. 1977;297(10):538-542. [DOI] [PubMed] [Google Scholar]
- 2.Berentsen S, Ulvestad E, Langholm R, et al. Primary chronic cold agglutinin disease: a population based clinical study of 86 patients. Haematologica. 2006;91(4):460-466. [PubMed] [Google Scholar]
- 3.Swiecicki PL, Hegerova LT, Gertz MA. Cold agglutinin disease. Blood. 2013;122(7):1114-1121. [DOI] [PubMed] [Google Scholar]
- 4.Randen U, Trøen G, Tierens A, et al. Primary cold agglutinin-associated lymphoproliferative disease: a B-cell lymphoma of the bone marrow distinct from lymphoplasmacytic lymphoma. Haematologica. 2014;99(3):497-504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lechner K, Jäger U. How I treat autoimmune hemolytic anemias in adults. Blood. 2010;116(11):1831-1838. [DOI] [PubMed] [Google Scholar]
- 6.Gertz MA. Cold agglutinin disease. Haematologica. 2006;91(4):439-441. [PubMed] [Google Scholar]
- 7.Ulvestad E, Berentsen S, Bø K, Shammas FV. Clinical immunology of chronic cold agglutinin disease. Eur J Haematol. 1999;63(4):259-266. [DOI] [PubMed] [Google Scholar]
- 8.Rosse WF, Adams JP. The variability of hemolysis in the cold agglutinin syndrome. Blood. 1980;56(3):409-416. [PubMed] [Google Scholar]
- 9.Baines AC, Brodsky RA. Complementopathies. Blood Rev. 2017;31(4):213-223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Coulthard LG, Woodruff TM. Is the complement activation product C3a a proinflammatory molecule? Re-evaluating the evidence and the myth. J Immunol. 2015;194(8):3542-3548. [DOI] [PubMed] [Google Scholar]
- 11.Merle NS, Church SE, Fremeaux-Bacchi V, Roumenina LT. Complement System Part I - Molecular Mechanisms of Activation and Regulation. Front Immunol. 2015;6:262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Brodsky RA. Complement in hemolytic anemia. Blood. 2015;126(22):2459-2465. [DOI] [PubMed] [Google Scholar]
- 13.Berentsen S. Cold agglutinin disease. Hematology Am Soc Hematol Educ Program. 2016;2016:226-231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Berentsen S. Role of complement in autoimmune hemolytic anemia. Transfus Med Hemother. 2015;42(5):303-310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Jaffe CJ, Atkinson JP, Frank MM. The role of complement in the clearance of cold agglutinin-sensitized erythrocytes in man. J Clin Invest. 1976;58(4):942-949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Shi J, Rose EL, Singh A, et al. TNT003, an inhibitor of the serine protease C1s, prevents complement activation induced by cold agglutinins. Blood. 2014;123(26):4015-4022. [DOI] [PubMed] [Google Scholar]
- 17.Ruiz-Argüelles A, Llorente L. The role of complement regulatory proteins (CD55 and CD59) in the pathogenesis of autoimmune hemocytopenias. Autoimmun Rev. 2007;6(3):155-161. [DOI] [PubMed] [Google Scholar]
- 18.Röth A, Bommer M, Hüttmann A, et al. Eculizumab in cold agglutinin disease (DECADE): an open-label, prospective, bicentric, nonrandomized phase 2 trial. Blood Adv. 2018;2(19):2543-2549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Jäger U, Barcellini W, Broome CM, et al. Diagnosis and treatment of autoimmune hemolytic anemia in adults: Recommendations from the First International Consensus Meeting [published online ahead of print 5 December 2019]. Blood Rev. doi:10.1016/j.blre.2019.100648. [DOI] [PubMed] [Google Scholar]
- 20.Berentsen S, Ulvestad E, Gjertsen BT, et al. Rituximab for primary chronic cold agglutinin disease: a prospective study of 37 courses of therapy in 27 patients. Blood. 2004;103(8):2925-2928. [DOI] [PubMed] [Google Scholar]
- 21.Berentsen S, Randen U, Vågan AM, et al. High response rate and durable remissions following fludarabine and rituximab combination therapy for chronic cold agglutinin disease. Blood. 2010;116(17):3180-3184. [DOI] [PubMed] [Google Scholar]
- 22.Berentsen S, Randen U, Oksman M, et al. Bendamustine plus rituximab for chronic cold agglutinin disease: results of a Nordic prospective multicenter trial. Blood. 2017;130(4):537-541. [DOI] [PubMed] [Google Scholar]
- 23.Berentsen S. How I manage patients with cold agglutinin disease. Br J Haematol. 2018;181(3):320-330. [DOI] [PubMed] [Google Scholar]
- 24.Bartko J, Schörgenhofer C, Schwameis M, et al. A randomized, first-in-human, healthy volunteer trial of sutimlimab, a humanized antibody for the specific inhibition of the classical complement pathway. Clin Pharmacol Ther. 2018;104(4):655-663. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Jäger U, D’Sa S, Schörgenhofer C, et al. Inhibition of complement C1s improves severe hemolytic anemia in cold agglutinin disease: a first-in-human trial. Blood. 2019;133(9):893-901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Freire PC, Muñoz CH, Derhaschnig U, et al. Specific inhibition of the classical complement pathway prevents C3 deposition along the dermal-epidermal junction in bullous pemphigoid. J Invest Dermatol. 2019;139(12):2417-2424.e2. [DOI] [PubMed] [Google Scholar]
- 27.Eskandary F, Jilma B, Mühlbacher J, et al. Anti-C1s monoclonal antibody BIVV009 in late antibody-mediated kidney allograft rejection-results from a first-in-patient phase 1 trial. Am J Transplant. 2018;18(4):916-926. [DOI] [PubMed] [Google Scholar]
- 28.Costabile M. Measuring the 50% haemolytic complement (CH50) activity of serum. J Vis Exp. 2010;(37): [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Broome C, Cunningham JM, Mullins M, et al. Incidence of thromboembolic events is increased in a retrospective analysis of a large cold agglutinin disease (CAD) cohort [abstract]. Blood; 2017;130 Abstract 928. [Google Scholar]
- 30.Foley JH. Examining coagulation-complement crosstalk: complement activation and thrombosis. Thromb Res. 2016;141(suppl 2):S50-S54. [DOI] [PubMed] [Google Scholar]
- 31.Ulvestad E, Berentsen S, Mollnes TE. Acute phase haemolysis in chronic cold agglutinin disease. Scand J Immunol. 2001;54(1-2):239-242. [DOI] [PubMed] [Google Scholar]
- 32.Liesveld JL, Rowe JM, Lichtman MA. Variability of the erythropoietic response in autoimmune hemolytic anemia: analysis of 109 cases. Blood. 1987;69(3):820-826. [PubMed] [Google Scholar]
- 33.Fattizzo B, Languille L, Levati G, et al. Evidence based use of erythropoietin in patients with autoimmune hemolytic anemia: a multicenter international study [abstract]. Presented at the 24th European Hematology Association Congress; 13-16 June 2019; Amsterdam, The Netherlands. Abstract S900. Available at: https://library.ehaweb.org/eha/2019/24th/267483/bruno.fattizzo.evidence.based.use.of.erytrhopoietin.in.patients.with.html?f=menu%3D6%2Abrowseby%3D8%2Asortby%3D2%2Amedia%3D3%2Ace_id%3D1550%2Aot_id%3D20974%2Afeatured%3D16435. Accessed 1 September 2019.
- 34.Afshar-Kharghan V. The role of the complement system in cancer. J Clin Invest. 2017;127(3):780-789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Hebert LA, Cosio FG, Neff JC. Diagnostic significance of hypocomplementemia. Kidney Int. 1991;39(5):811-821. [DOI] [PubMed] [Google Scholar]
- 36.Nandikolla AG, Derman O, Nautsch D, et al. Ibrutinib-induced severe liver injury. Clin Case Rep. 2017;5(6):735-738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Shah RR, Morganroth J, Shah DR. Hepatotoxicity of tyrosine kinase inhibitors: clinical and regulatory perspectives. Drug Saf. 2013;36(7):491-503. [DOI] [PubMed] [Google Scholar]
- 38.Cavazzini F, Lista E, Quaglia FM, et al. Response to ibrutinib of refractory life-threatening autoimmune hemolytic anemia occurring in a relapsed chronic lymphocytic leukemia patient with 17p deletion. Leuk Lymphoma. 2016;57(11):2685-2688. [DOI] [PubMed] [Google Scholar]
- 39.Galinier A, Delwail V, Puyade M. Ibrutinib is effective in the treatment of autoimmune haemolytic anaemia in mantle cell lymphoma. Case Rep Oncol. 2017;10(1):127-129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Manda S, Dunbar N, Marx-Wood CR, Danilov AV. Ibrutinib is an effective treatment of autoimmune haemolytic anaemia in chronic lymphocytic leukaemia. Br J Haematol. 2015;170(5):734-736. [DOI] [PubMed] [Google Scholar]
- 41.Hill QA, Hill A, Berentsen S. Defining autoimmune hemolytic anemia: a systematic review of the terminology used for diagnosis and treatment. Blood Adv. 2019;3(12):1897-1906. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.