

Abstract
Purpose
Patients with severe acute respiratory distress syndrome (ARDS) are candidates for extracorporeal membrane oxygenation (ECMO) therapy. The evaluation of organ severity is difficult in patients considered for cannulation in a distant hospital. This study was designed to identify early factors associated with hospital mortality in ARDS patients treated with ECMO and retrieved from referring hospitals.
Methods
Data from 85 consecutive ARDS patients equipped with ECMO by our mobile team and consequently admitted to our ICU were prospectively collected and analyzed.
Results
The main ARDS etiologies were community-acquired bacterial pneumonia (35 %), influenza pneumonia (23 %) (with 12 patients having been treated during the first half of the study period), and nosocomial pneumonia (14 %). The median (interquartile range) time between contact from the referring hospital and patient cannulation was 3 (1–4) h. ECMO was venovenous in 77 (91 %) patients. No complications occurred during transport by our mobile unit. Forty-eight patients died at the hospital (56 %). Based on a multivariate logistic regression, a score including age, SOFA score, and a diagnosis of influenza pneumonia was constructed. The probability of hospital mortality following ECMO initiation was 40 % in the 0–2 score class (n = 58) and 93 % in the 3–4 score class (n = 27). Patients with an influenza pneumonia diagnosis and a SOFA score before ECMO of less than 12 had a mortality rate of 22 %.
Conclusions
Age, SOFA score, and a diagnosis of influenza may be used to accurately evaluate the risk of death in ARDS patients considered for retrieval under ECMO from distant hospitals.
Keywords: Acute respiratory distress syndrome, Extracorporeal membrane oxygenation, Mortality, Outcome, Mobile unit
Introduction
The technique of extracorporeal membrane oxygenation (ECMO) for patients with severe acute respiratory distress syndrome (ARDS) involves placing them on a venovenous or venoarterial life-support circuit with a membrane oxygenator to temporarily take over the gas exchange and, sometimes, cardiac function [1]. Over the last two decades, the technique has progressed significantly, and several studies have reported encouraging survival rates using mainly venovenous ECMO in adults with ARDS [2–8]. Recently, an ECMO-based management protocol for selected ARDS patients transferred to a referral center was shown to improve 6-month disability-free survival [9, 10]. However, owing to recent advances in the management of ARDS [11, 12], ECMO remains a salvage therapy in a limited number of patients with life-threatening hypoxemia or respiratory acidosis [13]. Moreover, because of its additional costs and the need for trained expertise [14, 15], a rational allocation of this limited resource is critical, and indications must be further explored. ECMO centers have developed and have long been associated with mobile units that retrieve patients from distant hospitals immediately after cannulation [16, 17]. Approximately half of the patients treated with ECMO for ARDS are cannulated in distant hospitals and transported on ECMO [4, 18, 19]. For these patients, the decision to initiate ECMO is often made by phone and is based on the severity of respiratory failure, which is often evaluated by blood gas results or the lung injury score [20, 21]. Although some patients do not present with other organ failures, most of them present with septic shock and associated organ dysfunction. Because they may contribute significantly to ECMO outcomes, an understanding of the impact of preexisting organ dysfunction on ECMO-associated mortality is helpful in modifying the current strategies of ECMO in the resuscitation of these high-risk patients [5]. In the present study, we evaluated early prognostic factors in ARDS patients treated with ECMO in distant hospitals by our mobile team and brought to our center during a 3-year period. The goal was to establish simple decision rules that could aid the clinician in the decision regarding whether to treat patients with ECMO.
Methods
Patients and ECMO indications
Marseille North Hospital is a general acute-care, university hospital. It is a regional referral center for the treatment of severe respiratory infections. We established an ECMO-based protocol in autumn 2009 that included a mobile unit that could initiate ECMO in referring hospitals of our region before transfer to our center [4, 22]. We prospectively included all consecutive adult patients treated with ECMO in distant hospitals (a 31,400-km2 region) by our mobile team and immediately brought to our center between October 2009 and March 2013. Only patients with ARDS were included. Patients treated with ECMO as a bridge to or following lung transplantation or any surgery were not included. The protocol was approved by the local research ethics committee, who waived the need for informed consent, according to French legislation.
Referring hospitals were informed twice a year of ECMO criteria. The indication was discussed with one of three referees from our center who were contactable 24/7 through a hotline. A standardized form including ventilatory and blood gas parameters and sequential organ failure assessment (SOFA) score parameters was prospectively completed. Before consideration for ECMO, patients were all sedated using continuous neuromuscular blockade [11] and ventilated with volume-controlled ventilation using a tidal volume (Vt) of 5–7 ml/kg of predicted body weight. ECMO therapy was indicated if patients presented a PaO2 to FiO2 ratio of less than 70 mmHg for at least 6 h under an FiO2 of 1 and a PEEP level adjusted to obtain a plateau pressure (Pplat) of 30 cmH2O, a PaO2 to FiO2 ratio of less than 100 mmHg associated with a Pplat value greater than 35 cmH2O, or respiratory acidosis with pH less than 7.15 despite a respiratory rate greater than 35/min. Absolute contraindications included the following: any contraindication to heparin treatment, a chronic disease expected to be fatal within 5 years, a SOFA score greater than 18, and age over 70 years. The SOFA score [23] was always precisely calculated before ECMO consideration. When feasible in the referring hospital, prone positioning was systematically performed before considering ECMO. Relative contraindications were body mass index (BMI) greater than 40 kg/m2 and duration of ARDS greater than 7 days.
ECMO protocol
Venovenous ECMO was instituted using surgical cannulation, usually in a femoral–jugular configuration. Echocardiography was performed in all patients before cannulation and each day under ECMO. This procedure enabled venoarterial cannulation to be performed initially or later in patients presenting with left heart failure on the basis of echocardiography, defined as a less than 30 % left ventricular ejection fraction. We used centrifugal pumps (Bio-console 560; Medtronic Perfusion Systems, Minneapolis, MN, USA) with a flow of 3–5 l/min in all patients. Circuits were heparin-coated and composed of Quadrox D with Bioline Coating oxygenators (Maquet, Hirrlingen, Germany), 20–25 Fr cannulae (Edwards Lifesciences, Irvine, CA, USA), and intersept polyvinyl chloride (PVC) class VI tubing (Medtronic). Initial ventilator settings were as follows: Pplat, 20–30 cmH2O; PEEP, 15–20 cmH2O; respiratory rate, 5–10 breaths/min; and FiO2 adjusted to obtain an arterial O2 saturation of 90–95 %, whereas the FiO2 was set at 1 on the oxygenator. The patients were transferred to our ICU immediately after ECMO initiation by a team comprising one physician from our ICU, the cardiac surgeon who cannulated the patient, and a perfusionist. Continuous heparin infusion maintained the activated partial thromboplastin time (APTT) at 40–50 s. The triggering limits for transfusion were 50 × 103/ml for platelets and 10 g/dl for hemoglobin. ECMO was continued until lung recovery or until irreversible multiorgan failure leading to death. Patients were weaned from venovenous ECMO when the following criteria were met: PaO2 to FiO2 ratio greater than 150 mmHg with PEEP less than 12 cmH2O, Pplat less than 32 cmH2O with a Vt of 5–7 ml/kg, FiO2 of 0.21 on ECMO, blood flow of 1 l/min, and gas flow of 1 l/min.
Collected data
Prospectively collected data included demographic data; presence of identified risk factors for ARDS and major co-morbidities; respiratory and hemodynamic parameters at admission, before ECMO initiation, and throughout ARDS evolution; duration of ECMO and of mechanical ventilation; complications; and outcome. ICU and hospital mortality were recorded. The severity of the illness was assessed based on the simplified acute physiology score (SAPS) II [24] at ICU admission and the SOFA [23] score before ECMO initiation and at days 1, 3, and 7 of ECMO. The neurological score was calculated on the basis of the Glasgow coma scale just before intubation. Biological parameters were obtained in the 3 h preceding cannulation for all patients. The number of ECMO-free days at day 28 was defined as the number of days alive and free from ECMO at this time point.
Statistical analysis
Descriptive statistics included percentages for categorical variables and medians and interquartile ranges (IQRs) for continuous variables. Comparisons were made using either the Chi-square test or the Fisher exact test for categorical variables and the Student’s t test or Mann–Whitney U test for continuous variables, according to their distribution. Parameters significantly associated with hospital mortality on the basis of univariate analysis (p < 0.05) were introduced into a logistic regression analysis. The final model expressed the odds ratios (OR) and 95 % confidence intervals (CI).
To derive a simple and practical score to predict hospital mortality, we combined the logistic regression and the recursive partitioning analysis (RPA) [25, 26] conducted using the RPART routine in R software [27]. Briefly, RPA accepts predictor and response values as the inputs. As the output, this function generates a decision tree using a recursive partitioning algorithm. Each partitioning step selects the tree-branching criterion based on the predictor variables that will split the parent data set into two daughter data sets, with the daughter sets being as “pure” (homogeneous) as possible as approximated according to a heuristic. Here, purity is measured with the Gini statistic with respect to the response variable, such that the more homogeneous a daughter set, the higher the purity. Partition steps are repeated, adding branches to the tree, until the subgroups reach a minimum size or until no improvement can be obtained. Firstly, the significant variables in the multivariate logistic regression were selected into an RPA to build a decision tree. Then the optimal cutoff in the tree associated with each variable was used to transform the continuous variables into categorical variables (named partial score). With the aim to be as intuitive as possible, the score was constructed to give a result between 0 and 4 where 0 is a lower risk of hospital mortality and 4 a higher risk. The score can be calculated with the following formula: score = , where is the partial score assigned to each categorical variable. The discriminative performance of the score was evaluated with a receiver operating characteristics (ROC) curve and quantified by calculating the area under the curve and 95 % CI. The best cutoff value was identified as the point with the highest sensitivity and specificity (Youden index: SE + SP − 1). Lastly, Kaplan–Meier survival analysis was used to estimate the probability of survival after ECMO initiation for groups under and over the best cutoff value of the score. The log-rank test was used. Statistical analysis was performed using the SPSS statistics 20 software.
Results
During the study period, the referee from our center was contacted for consideration for ECMO by a referring hospital for 142 patients with ARDS (Fig. 1). Among them, 57 patients did not meet criteria for ECMO and were not referred and 85 consecutive patients treated with ECMO were included. Six of them had been included in a previous cohort study [4]. Patients’ demographic characteristics are provided in Table 1. No patient had a history of chronic heart, renal, or respiratory insufficiency. The main cause of ARDS was documented as community-acquired bacterial pneumonia (n = 30). Twenty patients presented with influenza pneumonia, 12 of whom had been treated in the first half of the study period. The median (interquartile range) time between contact from the referring hospital and patient cannulation was 3 (1–4) h; transfer to our center occurred within 6 (3–7) h. No serious complications (including vascular or chest tube displacement, ECMO malfunction, cardiac arrest, or death) occurred during transport by our mobile unit. For venovenous ECMO, femoral–jugular vein cannulation was performed in 62 patients, and femoral–femoral cannulation was performed in 15 patients. Femoral–femoral cannulation was performed in the eight patients treated with venoarterial ECMO. In all cases, venoarterial ECMO was used for left heart failure and severe shock complicating ARDS-associated disease. Prior to ECMO, all patients had refractory hypoxemia, 20 had a PaCO2 greater than 70 mmHg, and 29 had an arterial pH less than 7.2.
Fig. 1.
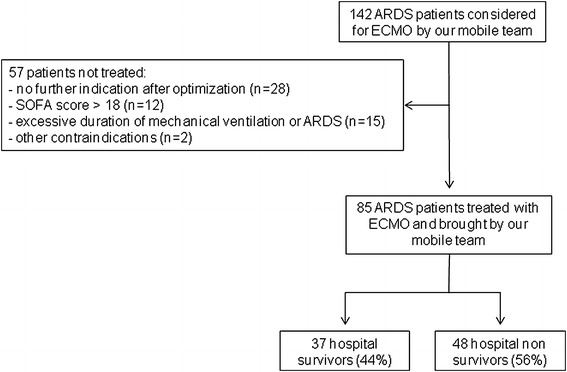
Study flowchart. ARDS acute respiratory disease syndrome, ECMO extracorporeal membrane oxygenation
Table 1.
Patient demographic characteristics according to hospital survival
| Total (n = 85) | Survivors (n = 37) | Nonsurvivors (n = 48) | p | |
|---|---|---|---|---|
| Age (years) | 47 ± 15 | 42 ± 12 | 51 ± 15 | 0.002 |
| Male (gender) | 52 (61) | 22 (59) | 30 (62) | 0.8 |
| BMI (kg/m2) | 28 ± 6 | 29 ± 7 | 27 ± 7 | 0.8 |
| BMI > 30 (kg/m2) | 22 (26) | 11 (30) | 11 (23) | 0.5 |
| SAPS II at ICU admission, mean ± SD | 57 ± 15 | 52 ± 13 | 60 ± 16 | 0.034 |
| ECMO period | ||||
| Oldest | 42 (49) | 25 (59) | 17 (40) | 0.5 |
| Latest | 43 (51) | 23 (53) | 20 (47) | |
| Comorbidities | ||||
| Chronic lung disease | 2 (2) | 0 | 2 (4) | 0.5 |
| Diabetes | 5 (6) | 1 (3) | 4 (8) | 0.4 |
| Transplantation | 2 (2) | 0 | 2 (4) | 1 |
| Malignancy | 7 (8) | 1 (1) | 6 (12) | 0.13 |
| Immunocompromised | 13 (15) | 3 (8) | 10 (20) | 0.13 |
| HIV | 1 (1) | 1 (3) | 0 | 0.4 |
| Drug addiction | 2 (2) | 1 (3) | 1 (2) | 1 |
| Cause of ARDS | ||||
| CAP | 56 (66) | 24 (65) | 32 (67) | 0.9 |
| Influenza A(H1N1) pneumonia | 20 (23) | 14 (38) | 6 (12) | 0.006 |
| Influenza pneumonia | 15 (18) | 9 (25) | 6 (12) | 0.2 |
| Legionella pneumonia | 7 (8) | 3 (8) | 4 (8) | 1 |
| S. pneumoniae pneumonia | 6 (7) | 2 (5) | 4 (8) | 0.7 |
| Acute pancreatitis | 5 (6) | 3 (8) | 2 (4) | 0.6 |
| Nosocomial pneumonia | 12 (14) | 5 (13) | 7 (15) | 0.9 |
| Burns | 3 (3) | 2 (5) | 1 (2) | 0.6 |
| Trauma | 3 (3) | 1 (3) | 2 (4) | 1 |
| Aspiration pneumonia | 5 (6) | 2 (5) | 3 (6) | 1 |
| Other | 2 (2) | 1 (3) | 1 (2) | 1 |
Data are provided as n (%) unless otherwise specified; p survivors vs. nonsurvivors
SD standard deviation, BMI body mass index SAPS II simplified acute physiology score II, HIV human immunodeficiency virus, AIDS acquired immunodeficiency syndrome, COPD chronic obstructive pulmonary disease, CAP community-acquired pneumonia
Forty-eight patients died in the ICU or at the hospital (56 %). Causes of death were multiorgan failure frequently associated with refractory hypoxemia (n = 44); hemorrhagic complications secondary to cannulation (n = 2); and intracerebral hemorrhage (n = 2). Forty-two nonsurvivors died during therapy after a median (range) of 9 (1–53) days of ECMO, and 6 of them died after successful ECMO weaning after a median (range) of 8 (5–10) days of ECMO. Survivors had a median (range) duration of ECMO therapy of 10 (3–25) days and were mechanically ventilated for a median (interquartile range) duration of 28 (24–35) days. After univariate analysis, factors potentially collected before ECMO that were associated with hospital mortality were age, SOFA score, lactate level, and a diagnosis of influenza pneumonia (Table 2). SAPS II was not considered for multivariate analysis because it could not constantly be obtained at this time and because SOFA score is easier to use at the bedside. Age, SOFA score, and a diagnosis of influenza pneumonia were introduced into the logistic regression analysis, which showed that these three parameters were independently associated with hospital mortality. Mortality increased with age [OR 1.045, CI (1.008; 1.083), p = 0.017] and SOFA score [OR 1.267, CI (1.053; 1.525), p = 0.01] whereas a diagnosis of influenza pneumonia was associated with a lower risk of death [OR 0.202, CI (0.061; 0.67), p = 0.009]. Lactate level was not introduced into the multivariate analysis because it was not available for all patients in the 3 h before considering ECMO. The distribution of SOFA subscores just before ECMO is presented in Fig. 2. Hemodynamic and liver scores were higher in nonsurvivors (p = 0.03 and p = 0.04, respectively).
Table 2.
Clinical characteristics and support in the 3 h before ECMO and during ECMO according to hospital survival
| Total (n = 85) | Survivors (n = 37) | Nonsurvivors (n = 48) | p | |
|---|---|---|---|---|
| In the 3 h before ECMO | ||||
| MV duration before ECMO (days) | 2 [1–8] | 2 [1–8] | 2 [1–7] | 0.9 |
| MV duration >7 days | 22 (26) | 7 (19) | 15 (31) | 0.4 |
| Interval call–cannulation (h) | 3 [2–4] | 3 [2.5–4] | 3 [2–4] | 0.8 |
| ARDS criteria (days) | 2 [1–7] | 1.5 [1–7.5] | 2 [1–7] | 0.8 |
| Prone positioning | 38 (45) | 16 (43) | 22 (46) | 0.8 |
| Nitric oxide | 51 (60) | 18 (49) | 33 (69) | 0.06 |
| HFOV | 4 (5) | 2 (6) | 2 (4) | 1 |
| RRT | 9 (11) | 6 (16) | 3 (6) | 0.2 |
| Corticosteroids for ARDS | 12 (14) | 4 (11) | 8 (17) | 0.4 |
| Vasopressive agents | 62 (74) | 25 (68) | 37 (79) | 0.2 |
| Pplat (cmH2O) | 32 [29–35] | 32 [29–35] | 32 [29–35] | 0.5 |
| pH | 7.1 ± 0.2 | 7.1 ± 0.1 | 7.1 ± 0.2 | 0.5 |
| PaCO2 (mmHg) | 59 [50–73] | 62 [50–75] | 57 [51–70] | 0.5 |
| PaO2 to FiO2 ratio (mmHg) | 60 [50–70] | 60 [52–70] | 60 [50–71] | 0.6 |
| Lactate (mmol/l)a | 3.8 [2–5.9] | 2.3 [1.5–3.6] | 4.2 [2.7–8.1] | 0.01 |
| SOFA score | 9 [7–11] | 8 [6–9] | 10 [7–12] | 0.003 |
| LIS | 3.5 [3.3–3.7] | 3.4 [3.2–3.6] | 3.6 [3.5–3.7] | 0.5 |
| Under ECMO | ||||
| Venovenous ECMO | 77 (91) | 33 (89) | 44 (92) | 0.7 |
| SOFA score at day 1 | 10 [7–12] | 8 [7–10] | 11 [8–15] | 0.007 |
| SOFA score at day 3 | 11 [8–13] | 9 [7–12] | 12 [9–15] | 0.004 |
| SOFA score at day 7 | 9 [7–12] | 8 [5–9] | 12 [9–14 | 0.001 |
| Lactate level at day 1 (mmol/l) | 2.7 [1–5] | 3.1 [1.7–5.3] | 2.5 [1.6–4.3] | |
| Lactate level at day 3 (mmol/l) | 2 [1.6–2.5] | 2.2 [1.7–3.4] | 1.9 [1.6–2.2] | 0.3 |
| Prone positioning | 17 (20) | 10 (27) | 7 (15) | 0.2 |
| Corticosteroids for ARDS | 17 (20 | 7 (19) | 10 (21) | 0.8 |
| RRT | 41 (48) | 11 (30) | 30 (62) | 0.003 |
| ECMO duration | 9 [7–13] | 10 [8–13] | 8 [6–15] | 0.3 |
| ECMO-free days at day 28 | 0 [0–18] | 18 [15–20] | 0 [0–0] | 0.001 |
Data are provided as n (%), median [interquartile range], or mean ± SD; p survivors vs. nonsurvivors
MV mechanical ventilation, HFOV high-frequency oscillatory ventilation, RRT renal replacement therapy, Pplat plateau airway pressure, SOFA sequential organ failure assessment, LIS lung injury score
aThe lactate level in the 3 h before consideration for ECMO was available in 48 patients
Fig. 2.
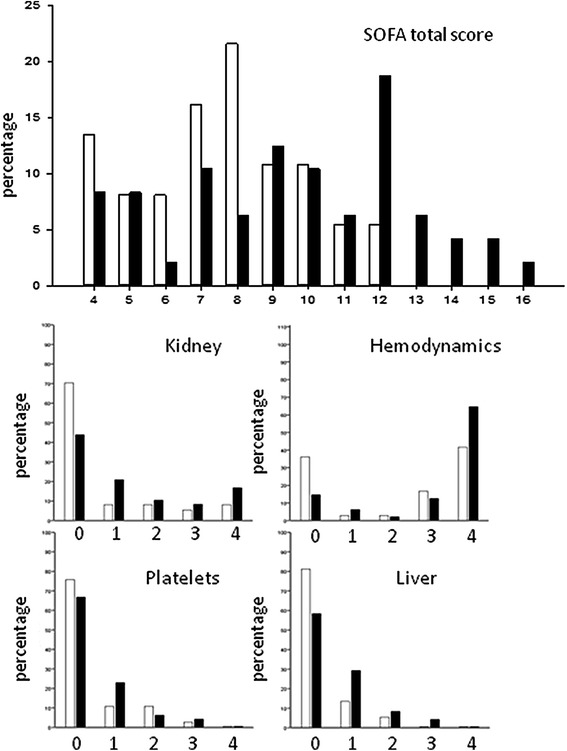
Distribution of SOFA score and subscores before ECMO in survivors (white bars) and in nonsurvivors (black bars). The neurological score was 0 and the respiratory score was 4 in all patients
The score developed after transforming continuous into categorical variables is displayed in Table 3. The optimal cutoff for the score was identified as 2.5. Finally, the probability of hospital mortality following ECMO initiation was 40 % in the 0–2 score class (n = 58) and 93 % in the 3–4 score class (n = 27) (Fig. 3; p < 0.001). The area under the ROC curve of the performance of this scoring system was 0.802, IC [0.710; 0.894], p < 0.001.
Table 3.
Hospital mortality score calculated with parameters available just before ECMO initiation
| Parameter | Partial score |
|---|---|
| SOFA | |
| <9 | 0 |
| 9–11 | 1 |
| ≥12 | 2 |
| Age | |
| <45 years | 0 |
| ≥45 years | 1 |
| Influenza pneumonia | |
| Yes | 0 |
| No | 1 |
| Total score | 0–4 |
A higher score was associated with higher hospital mortality
SOFA sequential organ failure assessment
Fig. 3.

Kaplan–Meier estimates of cumulative probabilities of survival for patients with pre-ECMO score classes 0–2 (n = 58), and 3–4 (n = 27). ECMO extracorporeal membrane oxygenation
During ECMO therapy, 10 patients were treated with high-frequency oscillatory ventilation, 17 with prone positioning, and 17 with corticosteroids for ARDS (Table 2). SOFA scores at day 1, 3, or 7 of ECMO were higher in hospital nonsurvivors than in survivors. Renal replacement therapy during ECMO was used more frequently in nonsurvivors than in survivors. Hemorrhagic complications occurred in 25 patients (29 %) under ECMO. Major hemorrhagic complications were retroperitoneal hematoma secondary to cannulation (n = 2), intracerebral hemorrhage (n = 2), and hemothorax due to fibrinolysis requiring ECMO weaning (n = 1). Other hemorrhagic complications were limited or moderate respiratory tract hemorrhage (n = 10), epistaxis requiring nasal packing (n = 2), and limited hemorrhage at cannulation sites (n = 8). While under ECMO, patients were transfused with a median (IQR) of 7 (4–15) units of red blood cells [1 (1–1) U/day], 3 (2–4) units of frozen plasma, and 1 (0–1) unit of platelets. In eight cases, membrane exchange was required during ECMO therapy because of acute hemolysis.
Discussion
The results of the present study show that age, SOFA score calculated in the 3 h before ECMO, and a diagnosis of influenza pneumonia are independently associated with hospital mortality in ARDS patients retrieved under ECMO from distant hospitals and brought to our ECMO center. These simple criteria can be included in a simple score to help clinicians make decisions regarding whether to treat patients with ECMO.
Our study is the first to analyze prognostic factors prior to ECMO in patients who have all been cannulated in distant hospitals. This population is likely to represent the majority of patients considered for ECMO in the future. Those patients are often considered for ECMO under rescue conditions, and the decision to initiate ECMO is often difficult. Our results show that simple criteria can be useful in predicting the prognosis in those patients despite the rapid evolution of their organ dysfunctions. Another strength of the present study is that it only includes patients with ARDS. Previous studies have frequently mixed patients with ARDS and cardiogenic shock [3, 5, 28–30], whereas these diseases are likely to affect different populations and to have different prognostic factors.
Most studies have shown that ECMO can be applied with encouraging survival rates [2–8]. Although the 56 % mortality rate found in the present study is in agreement with most other studies, some studies have reported lower rates. In the CESAR trial [9], 63 % of patients treated with ECMO survived. Of note, most of our patients had pneumonia with severe septic shock requiring vasopressors, and half of them required renal replacement therapy during the ICU stay, which has been shown to have an important prognostic impact in ECMO patients [31, 32]. Moreover, mortality rate is most likely largely influenced by indications and contraindications defined by each center. In the present study, indications were quite liberal regarding the evolution of organ dysfunctions, making it possible to accurately evaluate their prognostic impact. To date, decision criteria given for ECMO initiation in guidelines and studies are still undefined. Nevertheless, a recent study [18] showed that the application of new criteria based on Extracorporeal Life Support Organization (ELSO) guidelines [33] resulted in a higher mortality compared with previous criteria used at the same center, suggesting a strong influence of these criteria on the reported outcomes.
Studies, some with large numbers of patients, have identified early prognostic factors in patients treated with ECMO [3, 5, 18, 29, 31, 32, 34, 35]. The analysis of the ELSO multicenter database has notably identified age as a pre-ECMO factor associated with prognosis in patients with acute respiratory failure [5]. For this reason, only a few patients over 60 years of age are treated with ECMO [5, 9, 18]. Recently, Schmidt et al. [35] reported that age over 45 years was associated with a higher mortality. In the present study, we also observed that patients less than 45 years old had a markedly better prognosis and that outcome was independent of other organ dysfunctions in those very young patients. This important finding suggests that ECMO should not be contraindicated on the basis of organ dysfunction in young patients.
We found that the SOFA score before ECMO was associated with mortality. The SOFA score is simple to calculate and has been validated as a marker of organ dysfunction and of mortality in large multicenter studies in different patient populations [36]. In a cohort of 45 patients treated with ECMO for respiratory or heart failure, Wu et al. [29] suggested the prognostic value of SOFA calculated before ECMO. Recently, Lindskov et al. [18] showed that the SOFA score calculated at day 1 after ECMO initiation was predictive of death. In this latter study, a SOFA score of 10 or less was associated with 90 % survival. In the study by Wu et al. [29], the mean SOFA score before ECMO was 14 ± 4 in ARDS patients, whereas it was 10 ± 3 in our study. However, as in the study by Lindskov et al. [18], SOFA was not calculated in the same way as in the present study. Notably, the Glasgow coma scale score was set arbitrarily to 2 points. No patient presented with impaired consciousness at the time of sedation in our study, resulting in a 0-point neurological score in all patients. Pappalardo et al. [19] proposed a prognostic score in patients with H1N1-associated ARDS treated with ECMO that was based on biological and clinical data similar to the data used to determine the SOFA score. More recently, Schmidt et al. [35] proposed a prognostic score in ARDS patients treated with ECMO in which SOFA had a quite similar weight to that in the present study.
We found that a diagnosis of influenza-associated ARDS was associated with a better prognosis. Our 30 % mortality rate is in agreement with recent studies in patients with influenza H1N1-associated ARDS treated with ECMO [19, 37]. Our results also confirm those of previous observational studies suggesting that patients treated with ECMO for influenza pneumonia have a lower risk of death than patients presenting with other causes of ARDS [2]. However, no study had previously clearly shown a protective effect of influenza in ECMO patients. Unfortunately, the diagnosis of influenza is inconsistently confirmed but rather suspected at the time the ECMO decision is made. Therefore, this parameter cannot be taken into account in all patients when making ECMO decisions. Of note, all patients in our study who had confirmed influenza had been suspected of having influenza at ECMO initiation, and only three patients with suspected influenza were not confirmed.
Some studies have shown that the duration of mechanical ventilation before ECMO is associated with mortality [5, 7, 34, 35]. In our study, the duration of mechanical ventilation prior to ECMO was not longer in nonsurvivors. However, it is notable that our duration of ventilation before ECMO was short. The analysis of the ELSO database showed that the duration of mechanical ventilation was no longer associated with mortality in the most recently treated patients [5], whereas the number of patients treated after 7 days of mechanical ventilation decreased with time. Further studies are necessary to clearly address this question.
The present study is a single-center study, which could limit the translation of our results to other centers. However, our population has been stringently selected on the basis of predefined criteria and has benefited from protocolized treatments, including medical and technical maintenance of ECMO support. It is notable that the predefined indications that we used for ECMO based on gas exchange and ventilator pressure are not universally standardized and remain an important topic of discussion.
Conclusions
In ARDS patients treated mainly with venovenous ECMO and retrieved after cannulation from referring hospitals, age, SOFA score just before considering ECMO, and a diagnosis of influenza pneumonia can be used to aid the clinician in the decision about whether to initiate ECMO. Prognosis is much less dependent on organ dysfunction in young patients. A diagnosis of influenza-associated ARDS is associated with a lower mortality rate.
Conflicts of interest
The author(s) declare that they have no competing interests.
Footnotes
Take-home message: Our results suggest that, in patients considered for retrieval under ECMO to a referral center: (1) the use of age, SOFA score and a diagnosis of influenza can accurately categorize the risk of death; (2) the hospital mortality rate is lower in patients with a diagnosis of influenza-associated ARDS.
References
- 1.Combes A, Bacchetta M, Brodie D, Muller T, Pellegrino V. Extracorporeal membrane oxygenation for respiratory failure in adults. Curr Opin Crit Care. 2012;18:99–104. doi: 10.1097/MCC.0b013e32834ef412. [DOI] [PubMed] [Google Scholar]
- 2.Davies A, Jones D, Bailey M, Beca J, Bellomo R, Blackwell N, Forrest P, Gattas D, Granger E, Herkes R, Jackson A, McGuinness S, Nair P, Pellegrino V, Pettila V, Plunkett B, Pye R, Torzillo P, Webb S, Wilson M, Ziegenfuss M. Extracorporeal membrane oxygenation for 2009 influenza A(H1N1) acute respiratory distress syndrome. JAMA. 2009;302:1888–1895. doi: 10.1001/jama.2009.1535. [DOI] [PubMed] [Google Scholar]
- 3.Hemmila MR, Rowe SA, Boules TN, Miskulin J, McGillicuddy JW, Schuerer DJ, Haft JW, Swaniker F, Arbabi S, Hirschl RB, Bartlett RH. Extracorporeal life support for severe acute respiratory distress syndrome in adults. Ann Surg. 2004;240:595–605. doi: 10.1097/01.sla.0000141159.90676.2d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Roch A, Lepaul-Ercole R, Grisoli D, Bessereau J, Brissy O, Castanier M, Dizier S, Forel JM, Guervilly C, Gariboldi V, Collart F, Michelet P, Perrin G, Charrel R, Papazian L. Extracorporeal membrane oxygenation for severe influenza A (H1N1) acute respiratory distress syndrome: a prospective observational comparative study. Intensive Care Med. 2010;36:1899–1905. doi: 10.1007/s00134-010-2021-3. [DOI] [PubMed] [Google Scholar]
- 5.Brogan TV, Thiagarajan RR, Rycus PT, Bartlett RH, Bratton SL. Extracorporeal membrane oxygenation in adults with severe respiratory failure: a multi-centre database. Intensive Care Med. 2009;35:2105–2114. doi: 10.1007/s00134-009-1661-7. [DOI] [PubMed] [Google Scholar]
- 6.Lindén V, Palmér K, Reinhard J, Westman R, Ehrén H, Granholm T, Frenckner B. High survival in adult patients with acute respiratory distress syndrome treated by extracorporeal membrane oxygenation, minimal sedation, and pressure supported ventilation. Intensive Care Med. 2000;26:1630–1637. doi: 10.1007/s001340000697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Beiderlinden M, Eikermann M, Boes T, Breitfeld C, Peters J. Treatment of severe acute respiratory distress syndrome: role of extracorporeal gas exchange. Intensive Care Med. 2006;32:1627–1631. doi: 10.1007/s00134-006-0262-y. [DOI] [PubMed] [Google Scholar]
- 8.Camboni D, Philipp A, Lubnow M, Bein T, Haneya A, Diez C, Schmid C, Müller T. Support time-dependent outcome analysis for veno-venous extracorporeal membrane oxygenation. Eur J Cardiothorac Surg. 2011;40:1341–1346. doi: 10.1016/j.ejcts.2011.03.062. [DOI] [PubMed] [Google Scholar]
- 9.Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, Hibbert CL, Truesdale A, Clemens F, Cooper N, Firmin RK, Elbourne D. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009;374:1351–1363. doi: 10.1016/S0140-6736(09)61069-2. [DOI] [PubMed] [Google Scholar]
- 10.Noah MA, Peek GJ, Finney SJ, Griffiths MJ, Harrison DA, Grieve R, Sadique MZ, Sekhon JS, McAuley DF, Firmin RK, Harvey C, Cordingley JJ, Price S, Vuylsteke A, Jenkins DP, Noble DW, Bloomfield R, Walsh TS, Perkins GD, Menon D, Taylor BL, Rowan KM. Referral to an extracorporeal membrane oxygenation center and mortality among patients with severe 2009 influenza A(H1N1) JAMA. 2011;306:1659–1668. doi: 10.1001/jama.2011.1471. [DOI] [PubMed] [Google Scholar]
- 11.Papazian L, Forel JM, Gacouin A, Penot-Ragon C, Perrin G, Loundou A, Jaber S, Arnal JM, Perez D, Seghboyan JM, Constantin JM, Courant P, Lefrant JY, Guérin C, Prat G, Morange S, Roch A, ACURASYS Study Investigators Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med. 2010;363:1107–1116. doi: 10.1056/NEJMoa1005372. [DOI] [PubMed] [Google Scholar]
- 12.Guérin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, Mercier E, Badet M, Mercat A, Baudin O, Clavel M, Chatellier D, Jaber S, Rosselli S, Mancebo J, Sirodot M, Hilbert G, Bengler C, Richecoeur J, Gainnier M, Bayle F, Bourdin G, Leray V, Girard R, Baboi L, Ayzac L, PROSEVA Study Group Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368:2159–2168. doi: 10.1056/NEJMoa1214103. [DOI] [PubMed] [Google Scholar]
- 13.Combes A, Brechot N, Luyt CE, Schmidt M. What is the niche for extracorporeal membrane oxygenation in severe acute respiratory distress syndrome? Curr Opin Crit Care. 2012;18:527–532. doi: 10.1097/MCC.0b013e328357f090. [DOI] [PubMed] [Google Scholar]
- 14.Extracorporeal Life Support Organization (2010) ELSO guidelines for ECMO centers. http://www.elso.med.umich.edu/WordForms/ELSO%20Guidelines%20For%20ECMO%20Centers.pdf. Accessed 3 Dec 2010
- 15.Karamlou T, Vafaeezadeh M, Parrish AM, Cohen GA, Welke KF, Permut L, McMullan DM. Increased extracorporeal membrane oxygenation center case volume is associated with improved extracorporeal membrane oxygenation survival among pediatric patients. J Thorac Cardiovasc Surg. 2013;145:470–475. doi: 10.1016/j.jtcvs.2012.11.037. [DOI] [PubMed] [Google Scholar]
- 16.Bennett JB, Hill JG, Long WB, 3rd, Bruhn PS, Haun MM, Parsons JA. Interhospital transport of the patient on extracorporeal cardiopulmonary support. Ann Thorac Surg. 1994;57:107–111. doi: 10.1016/0003-4975(94)90375-1. [DOI] [PubMed] [Google Scholar]
- 17.Lindén V, Palmér K, Reinhard J, Westman R, Ehrén H, Granholm T, Frenckner B. Inter-hospital transportation of patients with severe acute respiratory failure on extracorporeal membrane oxygenation—national and international experience. Intensive Care Med. 2001;27:1643–1648. doi: 10.1007/s001340101060. [DOI] [PubMed] [Google Scholar]
- 18.Lindskov C, Jensen RH, Sprogoe P, Klaaborg KE, Kirkegaard H, Severinsen IK, Lorentsen AG, Folkersen L, Ilkjaer S, Pedersen CM. Extracorporeal membrane oxygenation in adult patients with severe acute respiratory failure. Acta Anaesthesiol Scand. 2013;57:303–311. doi: 10.1111/aas.12050. [DOI] [PubMed] [Google Scholar]
- 19.Pappalardo F, Pieri M, Greco T, Patroniti N, Pesenti A, Arcadipane A, Ranieri VM, Gattinoni L, Landoni G, Holzgraefe B, Beutel G, Zangrillo A, Italian ECMOnet Predicting mortality risk in patients undergoing venovenous ECMO for ARDS due to influenza A (H1N1) pneumonia: the ECMOnet score. Intensive Care Med. 2013;39:275–281. doi: 10.1007/s00134-012-2747-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.MacLaren G, Combes A, Bartlett RH. Contemporary extracorporeal membrane oxygenation for adult respiratory failure: life support in the new era. Intensive Care Med. 2012;38:210–220. doi: 10.1007/s00134-011-2439-2. [DOI] [PubMed] [Google Scholar]
- 21.Murray JF, Matthay MA, Luce JM, Flick MR. An expanded definition of the adult respiratory distress syndrome. Am Rev Respir Dis. 1988;138:720–723. doi: 10.1164/ajrccm/138.3.720. [DOI] [PubMed] [Google Scholar]
- 22.Bessereau J, Chenaitia H, Michelet P, Roch A, Gariboldi V. Acute respiratory distress syndrome following 2009 H1N1 virus pandemic: when ECMO come to the patient bedside. Ann Fr Anesth Reanim. 2010;29:165–166. doi: 10.1016/j.annfar.2010.01.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, Reinhart CK, Suter PM, Thijs LG. The SOFA (sepsis-related organ failure assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22:707–710. doi: 10.1007/BF01709751. [DOI] [PubMed] [Google Scholar]
- 24.Le Gall JR, Lemeshow S, Saulnier F. A new simplified acute physiology score (SAPS II) based on a European/North American multicenter study. JAMA. 1993;270:2957–2963. doi: 10.1001/jama.1993.03510240069035. [DOI] [PubMed] [Google Scholar]
- 25.Atkinson EJ, Therneau TM. An introduction to recursive partitioning using the Rpart routines. Rochester: Mayo Foundation; 1997. [Google Scholar]
- 26.Venables WN, Ripley BD. Modern applied statistics with S. New York: Springer; 2002. [Google Scholar]
- 27.Team RDC. R: a language, environment for statistical computing. Vienna: The R Foundation for Statistical Computing; 2008. [Google Scholar]
- 28.Lin CY, Tsai FC, Tian YC, Jenq CC, Chen YC, Fang JT, Yang CW. Evaluation of outcome scoring systems for patients on extracorporeal membrane oxygenation. Ann Thorac Surg. 2007;84:1256–1262. doi: 10.1016/j.athoracsur.2007.05.045. [DOI] [PubMed] [Google Scholar]
- 29.Wu MY, Lin PJ, Tsai FC, Haung YK, Liu KS, Tsai FC. Impact of preexisting organ dysfunction on extracorporeal life support for non-postcardiotomy cardiopulmonary failure. Resuscitation. 2008;79:54–60. doi: 10.1016/j.resuscitation.2008.05.002. [DOI] [PubMed] [Google Scholar]
- 30.Chang WW, Tsai FC, Tsai TY, Chang CH, Jenq CC, Chang MY, Tian YC, Hung CC, Fang JT, Yang CW, Chen YC. Predictors of mortality in patients successfully weaned from extracorporeal membrane oxygenation. PLoS ONE. 2012;7:e42687. doi: 10.1371/journal.pone.0042687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Chen YC, Tsai FC, Chang CH, Lin CY, Jenq CC, Juan KC, Hsu HH, Chang MY, Tian YC, Hung CC, Fang JT, Yang CW. Prognosis of patients on extracorporeal membrane oxygenation: the impact of acute kidney injury on mortality. Ann Thorac Surg. 2011;91:137–142. doi: 10.1016/j.athoracsur.2010.08.063. [DOI] [PubMed] [Google Scholar]
- 32.Wagner K, Risnes I, Abdelnoor M, Karlsen HM, Svennevig JL. Is it possible to predict outcome in pulmonary ECMO? Analysis of pre-operative risk factors. Perfusion. 2008;23:95–99. doi: 10.1177/0267659108096260. [DOI] [PubMed] [Google Scholar]
- 33.Park PK, Napolitano LM, Bartlett RH. Extracorporeal membrane oxygenation in acute adult respiratory distress syndrome. Crit Care Clin. 2011;27:627–646. doi: 10.1016/j.ccc.2011.05.009. [DOI] [PubMed] [Google Scholar]
- 34.Pranikoff T, Hirschl RB, Steimle CN, Anderson HL, 3rd, Bartlett RH. Mortality is directly related to the duration of mechanical ventilation before the initiation of extracorporeal life support for severe respiratory failure. Crit Care Med. 1997;25:28–32. doi: 10.1097/00003246-199701000-00008. [DOI] [PubMed] [Google Scholar]
- 35.Schmidt M, Zogheib E, Rozé H, Repesse X, Lebreton G, Luyt CE, Trouillet JL, Bréchot N, Nieszkowska A, Dupont H, Ouattara A, Leprince P, Chastre J, Combes A. The PRESERVE mortality risk score and analysis of long-term outcomes after extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. Intensive Care Med. 2013;39:1704–1713. doi: 10.1007/s00134-013-3037-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ferreira FL, Bota DP, Bross A, Melot C, Vincent JL. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA. 2001;286:1754–1758. doi: 10.1001/jama.286.14.1754. [DOI] [PubMed] [Google Scholar]
- 37.Zangrillo A, Biondi-Zoccai G, Landoni G, Frati G, Patroniti N, Pesenti A, Pappalardo F. Extracorporeal membrane oxygenation (ECMO) in patients with H1N1 influenza infection: a systematic review and meta-analysis including 8 studies and 266 patients receiving ECMO. Crit Care. 2013;17(1):R30. doi: 10.1186/cc12512. [DOI] [PMC free article] [PubMed] [Google Scholar]