

Abstract
Background
Molecular targeted therapy increased overall and disease-free survival in a wide range of malignancies. Although generally well tolerated compared to chemotherapy, molecular targeted therapy may be associated with adverse events requiring ICU admission. Informing clinicians about clinical features of these toxic events might maintain awareness and favor early recognition, prompt diagnosis and treatment.
Methods
We performed a systematic review of published case reports of molecular targeted therapy-related life-threatening toxicity that led to ICU admission. The search used the Pubmed database using medical subject heading (Mesh) terms, including all FDA-approved molecular targeted therapy (TT), up to March 2019. No language restriction was applied. All cases reports of patients admitted to the ICU for molecular targeted therapy-related toxicity were included. Non-FDA-approved combinations of treatments or hormonal therapy were not included.
Results
Two hundred and fifty-three cases were identified. Nearly half of them (n = 102; 40.3%) were related to anti-angiogenic agents, mostly for gastrointestinal and cardiovascular complications. Other molecules responsible for adverse events were chiefly immune checkpoint inhibitors (n = 85, 33.6%), EGFR inhibitors (n = 33; 13.0%), and anti-HER2 (n = 10; 4.0%). They were associated with adverse events such as respiratory or hypersensitivity events. Management and outcomes associated with these life-threatening complications are reported.
Conclusions
Based on the vast number of treated patients, only 253 cases of molecular therapy-related severe toxicity are reported in cancer patients. Symptoms and biomarkers that depict these events need to be better identified as to allow appropriate reporting and improving dose and schedule of the treatment adapted to each patient.
Electronic supplementary material
The online version of this article (10.1007/s00134-019-05650-w) contains supplementary material, which is available to authorized users.
Keywords: Molecular targeted therapy, Malignancies, Critical care, Pneumonitis, Digestive perforation
Take-home message
| In cancer patients, molecular therapy-related severe toxicity can be life-threatening and require ICU management. Half the cases were reported to angiogenic agents, mostly for severe gastrointestinal and cardiovascular complications. Immune checkpoint inhibitors, EGFR inhibitors, and anti-HER2 were associated to respiratory or hypersensitivity events. |
Introduction
Survival of patients with solid tumors has markedly improved over the last decade with the advent of molecular targeted therapies [1]. Compared with conventional cytotoxic chemotherapy, these targeted agents offer a more tolerable toxicity profile, thereby promising both optimized dose intensity and better quality of life. Given the rise of an effective cancer screening throughout the world, the ageing population, the improvement of overall survival of patients with solid tumors, and the better understanding of molecular and cellular pathways involved in tumor progression, an ever-increasing number of patients will be receiving single or combined molecular treatments [2, 3]. These new therapeutic drugs significantly improve progression-free survival in several types of cancer, but also generate adverse events (AEs), which vary widely in nature and severity.
The majority of these AEs are of low to moderate severity, classified as grade 1 to 2 toxicities according to the Common Terminology Criteria of Adverse Events defined by the National Cancer Institute. Broadly reported in the literature, including in pivotal phase II and III clinical trials, they involve multiple organ systems, including the skin, gastrointestinal tract, peripheral nervous system, liver and endocrine system. These AEs are typically foreseeable and expected, as they correspond to a so-called on-target toxicity, as a result of inhibition of the targeted cellular pathway [4]. Although most AEs are well-managed in an outpatient setting, some AEs occasionally lead to severe morbidity or can even be fatal. Life-threatening, drug-related toxicities remain rarely described in clinical trials, which involve only carefully selected patients with middle-term clinical follow-up. Thus, few data are available regarding serious drug-related AEs in real-world patients who would not have been eligible for clinical trials. Recently, the development of immune checkpoint inhibitors in different settings and for different types of cancer has led to the rise of a new spectrum of immunotherapy-related adverse events (irAEs) [5–7], as a consequence of self-tolerance impairment through reduced cytotoxic T cell inhibition; however, the risk of life-threatening or fatal autoimmune-like AEs is unclear at this point, given the novelty of this class [8]. Therefore, data are needed on type, clinical presentation, management and outcomes of potential life-threatening AEs related to molecular targeted therapies, particularly those requiring an admission to an intensive care unit (ICU). In the years to come, intensivists will be managing an increasing number of patients treated with new single or combined targeted therapies. Consequently, clinicians should not overlook potential harmful effects of these new drugs, to allow for prompt diagnosis and initiation of specific treatments. Furthermore, identifying reliable predictive biomarkers of efficacy and toxicity is an urgent need to improve patient selection and help oncologists in treatment decision-making.
In this systematic review, we aimed to identify published cases of life-threatening AEs leading to an ICU admission following a targeted anticancer therapy in patients with solid tumors.
Search strategy
A systematic research on PubMed was performed, using the medical subject headings (MeSH) terms “drug-related adverse event” and “erlotinib, gefitinib, afatinib, cetuximab, panitumumab, osimertinib, rociletinib, trastuzumab, pertuzumab, TDM-1, lapatinib, neratinib, bevacizumab, sunitinib, sorafenib, pazopanib, axitinib, lenvatinib, regorafenib, aflibercept, ramucirumab, cabozantinib, olaparib, niraparib, rucaparib, talazoparib, palbociclib, ribociclib, abemaciclib, crizotinib, ceritinib, alectinib, lorlatinib, brigatinib, vemurafenib, dabrafenib, trametinib, cobimetinib, ipilimumab, nivolumab, pembrolizumab, atezolizumab, durvalumab, avelumab, everolimus, temsirolimus, vismodegib, vandetanib, nintedanib”. We added a manual bibliography search of selected articles.
All case reports and case series of drug-related AEs resulting in an ICU admission in patients with solid cancer following treatment with an US Food and Drug Administration (FDA)-approved molecular targeted therapy (Table 1S) published up to March 2019 were included, with no language restrictions. Patients admitted to a high-dependency unit (HDU) or coronary care unit (CCU) were included. We excluded pediatric cases, cases in pregnancy and those referring to non-oncological indications of molecular therapies. All above-mentioned targeted therapies were considered, whether the patient received the treatment in a clinical trial, off label or as usual care. We excluded case reports on non-FDA-approved combinations of targeted agents or hormonal therapies. For each type of targeted therapy, we also collected grade III–IV sides effects described in the randomized controlled trial (Table 1).
Table 1.
Incidence of grade III or IV toxicities in phase III pivotal clinical trials by molecular targeted therapy
| % | Bevacizumaba [1, 18–26] | Sunitinib [49] | Sorafenib [50] | Gefitinib [51–53] | Erlotinib [54, 55] | Cetuximab [56–60] | Trastuzumabb [61–64] | Everolimus [65–67] | Vemurafenib [68, 69] | Ipilimumab [29–32] | Nivolumab [30, 31, 33–35] | Ipilimumab + nivolumab [30, 31] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Colitis/ileitis | NR | NR | NR | NR | NR | NR | NR | NR | NR | 5–14 | < 1 | 8–18 |
| Digestive perforation or fistula | < 1–6 | NR | NR | NR | NR | NR | NR | NR | NR | < 1 | NR | NR |
| Haemorrhagic events | 0–9.7 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Pneumonitis/ILD** | NR | NR | NR | 1–5.3 | < 1 | NR | NR | 2–3 | NR | 0–2 | < 1 | 1–2 |
| PRES | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Neurological events | NR | NR | NR | < 1 | NR | NR | NR | NR | NR | 1 | < 1 | NR |
| Heart failure | < 1 | NR | NR | NR | NR | NR | <1–4.1 | NR | 1 | NR | NR | NR |
| Ischemic events | < 1–3 | NR | 3 | < 1 | NR | NR | NR | NR | NR | NR | NR | NR |
| Thromboembolic events | 0–12.6 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Pericarditis | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | < 1 | NR |
| Renal injury | NR | 1 | NR | NR | NR | NR | 1 | NR | NR | < 1 | < 1 | NR |
| Hypersensitivity | NR | NR | NR | NR | NR | 1.2–4.5 | 6 | NR | NR | NR | NR | NR |
| Hepatitis | NR | 1–2 | NR | 26.3 | NR | NR | NR | 3 | 8–11 | 0–2 | 0.5–3 | 6–8 |
| Drug-related death | 0.5–2.3 | NR | NR | 1–3.8 | < 1 | 1.4 | 2–3 | < 1 | 1–2 | 0–3 | < 1 | 0–3 |
Adverse events reported above were attributed by the investigators only to mentioned molecular targeted therapy in case of combination with other treatment(s)
**Interstitial lung disease
aBevacizumab-related adverse events reported here were collected from pivotal clinical trials assessing bevacizumab at doses of either 7.5 mg/kg or 15 mg/kg every 3 weeks, 10 mg/kg every 2 weeks or 10 mg/kg every 3 weeks
bWithout combined anthracycline treatment. NR not reported
We collected clinical features of reported patients (age, gender, cancer localization, prior or concomitant anticancer treatments by chemotherapy, radiotherapy or corticosteroids). Characteristics of drug-related AEs by molecular therapy family (clinical presentation at ICU admission, time since treatment initiation, and diagnosis of complication), management of toxicity in ICU (required organ support, surgery, anti-infectious or immunosuppressive treatment, corticosteroids use) and outcomes were also collected.
Results
All cases
As shown in Fig. 1, 7344 case reports and series were identified, including 253 cases that were included in the present study. We identified 96 (37.9%) women and 157 (62.1%) men. Median age was 62 (23–88) years. Targeted treatments of interest were predominantly antiangiogenic agents (n = 102, 40.3%), immune checkpoint inhibitors (n = 85, 33.6%), EGFR inhibitors (n = 33, 13%), or monoclonal anti-HER2 antibodies (n = 10, 4.0%) (Table 2). Reported patients presented with various types of cancer, mainly melanoma (n = 64, 25.3%), kidney (n = 46, 18.2%), lung (n = 44, 17.4%), colorectal (n = 40, 15.8%), and breast (n = 18, 7.1%) cancer. All but 17 patients presented with unresectable or metastatic tumors at ICU admission (n = 236, 93.3%), and 129 patients received targeted therapy of interest as first-line treatment (51.0%). One hundred and seventy-one (67.6%) patients received molecular therapy as monotherapy, whereas chemotherapy and radiotherapy were associated with targeted therapy in 65 (25.7%) and five (1.9%) patients, respectively. Combinations of targeted molecular agents were reported in 12 (4.7%) patients.
Fig. 1.

Flow chart of screened publications
Table 2.
Molecular targeted therapy-related toxicity that required ICU admission
| n (%) | n | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| All (n = 253) | Anti-angiogenic agents (n = 102) | Immune checkpoint inhibitors (n = 85) | EGFR inhibitors (n = 33) | Anti-HER2 (n = 10) | mTOR inhibitor (n = 8) | BRAF inhibitors (n = 7) | ALK inhibitor (n = 3) | Otherd (n = 5) | |
| Gastrointestinal | 69 (27.3) | 42 | 20 | 3 | 1 | 1 | 1 | 1 | |
| Colitis/ileitis | 3 | 26a | 3 | 2c | 1 | 1c | 1 | 1 | |
| Digestive perforation | 44 | 6 | 15 | 1 | |||||
| Digestive fistula | 6 | 3 | 2 | ||||||
| Digestive hemorrhagia | 6 | 7 | |||||||
| Hepatitis | 10 | ||||||||
| Cardiovascular | 58 (22.9) | 23 | 27 | 3 | 4 | 1 | |||
| Toxic cardiomyopathy | 15 | 7 | 2 | 2 | 3 | 1 | |||
| Takotsubo syndrome | 6 | 5 | 1 | 1 | 1 | ||||
| Coronary vasospasm | 3 | 2 | 1 | ||||||
| Myocardial infarction | 3 | 2 | 1 | ||||||
| Acute aortic dissection | 3 | 3 | 1 | ||||||
| Pericarditis | 1 | 1 | 8 | ||||||
| Tamponade | 9 | 1 | 13 | ||||||
| Myocarditis | 13 | 1 | |||||||
| Pulmonary embolism | 1 | 1 | |||||||
| Ischemic colitis | 1 | ||||||||
| Intracardiac thrombus | 1 | ||||||||
| Ischemic cerebral vasculopathy | 2 | ||||||||
| Respiratory | 29 (11.5) | 7 | 7 | 11 | 1 | 2 | 1 | ||
| Pneumonitis/ILD* | 13 | 2 | 3 | 6 | 1 | 2 | 1 | ||
| ARDS** | 11 | 1 | 4 | 4 | |||||
| Pneumothorax | 5 | 4b | 1c | ||||||
| Neurological | 39 (15.4) | 12 | 23 | 2 | 1 | 1 | |||
| PRES*** | 11 | 10 | 9 | 1 | 1 | 1 | |||
| Guillain–Barre syndrome | 9 | 1 | 2 | 1 | |||||
| Meningoradiculoneuritis | 2 | 1 | 2 | ||||||
| Meningoencephalitis | 2 | 9 | |||||||
| Myasthenia gravis | 9 | 1 | |||||||
| Bulbar myopathy | 1 | ||||||||
| Intracranial hemorrhagia | 2 | ||||||||
| Unexplained coma | 2 | ||||||||
| Unexplained seizure | 1 | ||||||||
| Infectious events | 13 (6.3) | 4 | 4 | 4 | 1 | ||||
| Necrotizing fasciitis | 6 | 4 | 2 | 2 | 1 | ||||
| Pneumocystis pneumonia | 2 | 2 | 1 | ||||||
| B hepatitis virus reactivation | 2 | 1 | |||||||
| Otherd | 3 | ||||||||
| Renal | 10 (4.8) | 6 | 2 | 2 | |||||
| Acute renal failure | 3 | 3 | 2 | 2 | |||||
| Acute interstitial nephritis | 2 | 3 | |||||||
| Thrombotic microangiopathy | 5 | ||||||||
| Hypersensitivity/infusion reaction | 9 (4.3) | 7 | 1 | 1 | |||||
| Dermatologic | 4 (1.9) | 1 | 3 | ||||||
| Toxic epidermal necrolysis | 4 | 1 | 3 | ||||||
| Tumor lysis syndrome | 4 (1.9) | 1 | 1 | 1 | 1 | ||||
| Muscular | 3 (1.4) | 3 | |||||||
| Polymyositis | 3 | 3 | |||||||
| Endocrinal | 3 (1.4) | 3 | |||||||
| Severe hypothyroidism | 3 | 3 | |||||||
| Other eventsd | 12 (4.7) | 4 | 3 | 1 | 2 | 1 | 1 | ||
*Interstitial lung disease
**Acute respiratory distress syndrome
***Posterior reversible encephalopathy syndrome
aThree out of 26 cases were related to metastatic lesions necrosis
bTwo out of four events were related to tumor necrosis
cOne of these events was related to tumor necrosis
dDetails of other events and drugs are available in supplementary data
Median time from treatment initiation to ICU admission was 1.4 (0.03–54) months. We collected cases of 50 (19.8%) digestive perforations or fistulas, three (1.2%) non-perforated colitis and/or ileitis, 58 (22.9%) cardiovascular events, 29 (11.5%) pulmonary events, 39 (15.4%) neurological events, 13 (5.1%) infectious complications, 10 (4.0%) hepatic failures, 10 (4.0%) acute renal failures, 9 (3.6%) hypersensitivity or infusion-related reactions, 4 (1.6%) dermatological events, 3 (1.2%) muscular events, 3 (1.2%) severe hypothyroidism events, and 12 (4.7%) other complications (Table 2). ICU mortality was 31.6% (80 deaths). Time since treatment onset, ICU admission, and number of cases are detailed in Fig. 2.
Fig. 2.

Systematic review of molecular targeted therapy adverse events leading to ICU in oncology
Antiangiogenic agent: bevacizumab, sunitinib, sorafenib (Table 2S)
In the 102 patients who had received an antiangiogenic agent, gastrointestinal AEs were reported in 42.2% of the cases, mainly as digestive perforations (25.5%), which represent almost one-third of life-threatening bevacizumab-related events admitted into an ICU. Eight patients (30.8%) suffering from digestive perforations died in the ICU, mostly from post-operative septic shock. Additionally, 22.5% patients experienced a cardiovascular complication, mainly toxic cardiomyopathy, including 51.7% (4/7) who died during ICU stay. Moreover, ten (9.8%) cases of posterior reversible encephalopathy syndrome (PRES) were reported, eight cases of which occurred after bevacizumab treatment and led to three ICU deaths (30.0%). Other less frequent but relevant AEs included three (2.9%) cases of sunitinib-related severe hypothyroidism and three (2.9%) cases of sunitinib-related thrombotic microangiopathy syndrome. Median time from antiangiogenic agent initiation to ICU admission was 1.8 (0.03–54) months with a median number of received courses of three (1–34).
Mechanical ventilation and vasopressors were required in 55 (53.9%) and 23 (22.5%) patients, respectively. Death in the ICU was reported as a result of AEs in 30 (29.4%) patients, from which 12, 7, and 8 patients were treated with bevacizumab, sunitinib, and sorafenib, respectively. Of note, one case of sorafenib-related fulminant hepatitis was successfully treated with emergency hepatic transplantation [9].
Immune checkpoint inhibitors: nivolumab, pembrolizumab, ipilimumab (Table 3S)
Eighty-five cases of irAEs requiring admission into an ICU were collected. The most common reported irAEs were perforated colitis or enterocolitis (n = 15, 17.6%), fulminant myocarditis (n = 13, 15.3%), polyradiculoneuritis (n = 11, 12.9%), pericarditis (n = 9, 10.6%), and myasthenia gravis (n = 9, 10.6%). Most of reported cases concerned the anti-CTLA4 antibody ipilimumab in monotherapy (n = 34, 40.0%). Median time from immune checkpoint inhibitor initiation to ICU admission was 1.4 (0.2–16) months with a median number of received courses of two (1–32).
Mechanical ventilation, vasopressors, and plasmapheresis were required in 49 (57.6%), 23 (27.1%), and 22 (25.9%) patients, respectively. Sixty-nine (81.2%) patients received high-dose steroids, 23 (27.1%) intravenous immunoglobulins, 11 (12.9%) infliximab, and eight (9.4%) another immunosuppressive drug. ICU mortality rate after irAEs was 28.2% (n = 24). Immune-related adverse events associated with highest rate mortality the in ICU were fulminant myocarditis (7 deaths out of 13 cases, 53.8%) and neurologic events (9/23, 39.1%). Three patients presenting with ipilimumab-related perforated enterocolitis died during ICU stay from postoperative multiple-organ dysfunction syndrome [10–12]. One patient died from nivolumab-related acute respiratory distress syndrome, despite aggressive treatment including infliximab use [13]. Four out of ten (40.0%) patients who had received a combination of ipilimumab and nivolumab died in the ICU: two patients died from fulminant myocarditis [14], of which one was infliximab-refractory, one patient from immune-related myasthenia gravis with no response to intravenous immunoglobulins [15], and one from septic shock secondary to immunosuppression induced with high-dose steroids and mycophenolate mofetil, initiated as immune-related nephritis treatment [16].
EGFR inhibitors: erlotinib, gefitinib, cetuximab (Table 4S)
Thirty-three cases of anti-EGFR-related AEs requiring an ICU management were identified, of which ten (30.3%) cases were diagnosed as interstitial lung disease and seven (21.2%) as cetuximab-related hypersensitivity. ICU admission occurred after anti-EGFR initiation with a median time of 1.0 (0.2–4.5) month, except for cetuximab, for which related infusion reactions were observed during the first injection. Three (9.1%) cases of tumor necrosis-related events were reported, in addition to one case of cetuximab-related tumor lysis syndrome. Conceivably, all three cases occurred in patients with non-small cell lung cancer harboring an epidermal growth factor receptor (EGFR) mutation.
Most patients required mechanical ventilation (78.8%) and seven (21.2%) needed vasopressor. High-dose steroids were administered in 13 (39.4%) patients. Thirteen patients (39.4%) out of 33 died during ICU hospitalization. Acute respiratory distress syndrome occurred in four patients admitted with interstitial lung disease (40.0%), and all four died in the ICU. Two patients (28.6%) died on the day of ICU admission from cetuximab-related hypersensitivity.
Other molecular targeted therapies (Table 5S)
Ten patients were treated with trastuzumab, resulting in three (30.0%) cases of toxic cardiomyopathy with a median time from anti-HER2 initiation of 4.0 (2.3–6.0) months, corresponding to nine (3–12) received injections. There was no evidence of previous cardiac history or cardiotoxic medications. One of the three patients died in the ICU. Everolimus was administered to eight patients.
Two patients (25.0%) were admitted to the ICU for life-threatening interstitial lung disease, of which one was fatal. Strikingly, two patients developed Pneumocystis pneumonia after a median treatment time of 1.5 (1.0–2.0) months, with a favorable outcome [17]. Life-threatening AEs related to BRAF inhibitors, crizotinib, imatinib, and vandetanib are shown in Table 5S (supplementary data).
Discussion
Molecular targeted therapies, mainly immune checkpoint inhibitors, have drastically modified the therapeutic paradigm in solid oncology. In the years to come, an increasing number of patients with solid tumors will be treated with new drugs. While many AEs have been well-described in clinical trials, others remain unknown, due either to their sporadicity or their late onset during follow-up. Therefore, it is of clinical importance to collect data about drug-related AEs, including life-threatening complications during patient follow-up.
Our search yielded 253 cases of life-threatening drug-related AEs requiring an admission into an ICU in patients presenting with solid tumors. Almost half of these cases were related to use of antiangiogenic agents, involved in 26 (25.5%) reported cases of digestive perforation with a 30.8% mortality rate in the ICU. Of these, three cases (11.5%) were attributed to necrosis of metastatic digestive lesions. As reported in Table 1, digestive perforations were already described in 1–6% of patients in clinical trials assessing bevacizumab in several types of cancer [18–26]. In addition, we collected 23 (22.5%) cases of antiangiogenic-related cardiovascular issues, of which seven (30.4%) were lethal. Although the molecular mechanisms through which VEGF inhibitor use leads to cardiotoxicity remain unclear, it is suggested that patients with proteinuria and hypertension immediately after beginning antiangiogenic therapy are at increased risk for later cardiac AEs [27]. These findings pinpoint the importance of cardiovascular assessment before and during treatment with angiogenesis inhibitors, particularly for multi-targeted small molecules such as sunitinib and sorafenib [28].
The most significant reported immunotherapy-related serious toxicity was colitis or ileitis (n = 18, 21.2%), which is consistent with immunotherapy clinical trial results [29–37]. Surprisingly, only one case of life-threatening perforated enterocolitis due to ipilimumab and nivolumab combination was reported in literature [38], although the latter further increased the risk of autoimmune-like issues in clinical trials [30, 31]. Conceivably, the novelty of immunotherapies explains the small number and the heterogeneity of published cases we report. As recently reported by Wang et al., irAEs associated with the highest rate of mortality in the ICU in our cohort were fulminant myocarditis and neurologic events. However, analysis of the pharmacovigilance database indicates that fatal irAEs remain uncommon, occurring at a rate of 0.3–1.3% [39].
ICU mortality in our review was 31.6%. Although the paucity and variability regarding case reporting do not allow us to generalize this result, this figure is consistent with some previous studies focusing on survival of solid cancer patients admitted to the ICU [40]. Taken together, all these data emphasize the need for a careful selection of patients who are candidates for a targeted molecular therapy. An exhaustive and personalized evaluation of toxicity risk before treatment initiation is warranted. In particular, an autoimmune work-up aiming to rule out a subclinical systemic disease should be consistently undertaken. As recently shown by Johnson et al., patients with underlying pre-existing autoimmunity disease should not be de facto ineligible for immunotherapy, but would imperatively require thorough monitoring during and after treatment [41]. Critical care specialists and oncologists should be aware of warning symptoms for a prompt diagnosis of drug-related AEs, which might be resolved early with a dose reduction or transient discontinuation of treatment. Furthermore, although management of steroid-refractory irAEs with immunomodulatory medications such as infliximab, mycophenolate mofetil, or tacrolimus may be efficient in some cases [42–45], prospective trials assessing different treatment modalities are needed. Here, we report a published case of ipilimumab-related hepatitis refractory to mycophenolate mofetil but which resolved with use of T cell depleting antibody anti-thymocyte globulin [46]. Ultimately, more data are needed regarding optimal dose and administration schedule of ipilimumab to curtail the risk of autoimmune-like or immune-related toxicity [8], given the possible dose-toxicity relationship [37, 47].
There are several limitations inherent to this review. First of all, the small number of reported cases and their retrospective nature hamper assessment of molecular treatment imputability, particularly in the case of therapeutic combinations including chemotherapy and other drugs. Moreover, administered doses of targeted molecules are not always mentioned. Secondly, patients with life-threatening anticancer drug-related AEs may have declined, or were denied for ICU referral and were not included in this review. Furthermore, we could not differentiate ICU patients from HDU patients in some reported cases. Last, another important bias of this review lies in the reporting of only published cases (Fig. 1S). However, hierarchy in terms of proportions is maintained between AEs with respect to those described in pivotal clinical trials for each drug (Table 1), suggesting that our review may be representative of real-world patients, although widely underestimating the absolute number of serious drug-related AEs.
We believe that this review provides substantial information on the management and outcomes of patients presenting with life-threatening anticancer drug-related AEs. Our findings advocate for a thoughtful selection of patients likely to benefit from molecular targeted therapy and improved clinical and biological monitoring during and after treatment initiation. Further studies should identify optimal therapeutic doses and schedules to adopt and determine predictive biomarkers for adverse events, primarily those related to immune checkpoint inhibitors [48], in order to enhance the risk/benefit profile for each individual.
Electronic supplementary material
Below is the link to the electronic supplementary material.
{kind=link}
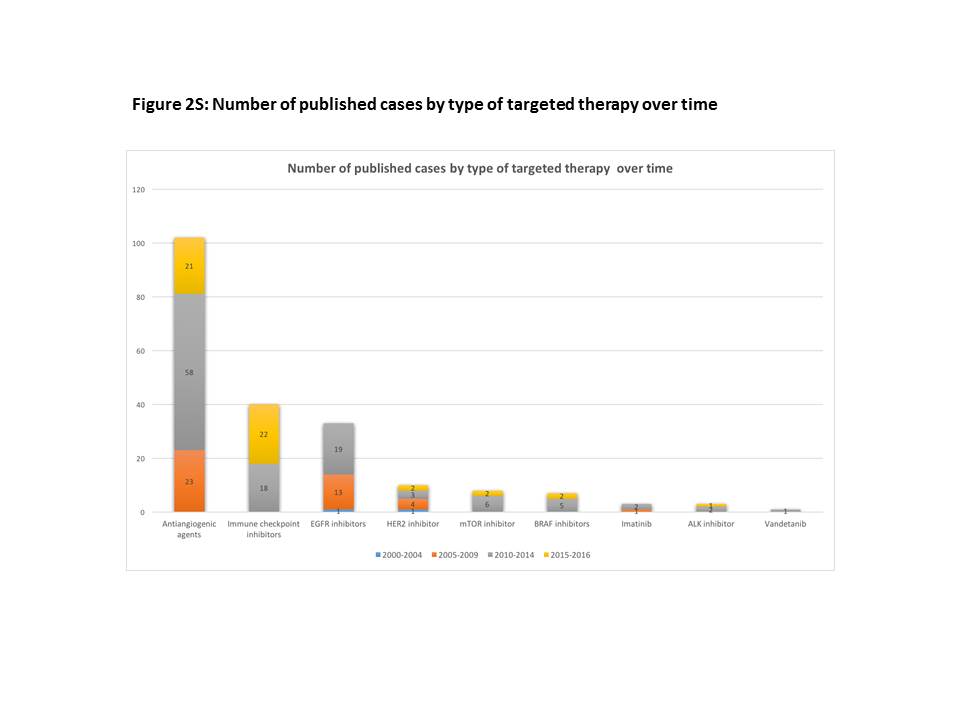
Fig. 1S: Number of published cases by type of targeted therapy over time (JPEG 30 kb)
Table 1S: Oncological licensed indications of reported molecular therapies in adult patients throughout United States and Europe in 2018 (DOCX 132 kb)
Table 2S: Adverse events related to antiangiogenic agents use (DOCX 21 kb)
Table 3S: Immune-related adverse events (DOCX 22 kb)
Table 4S: Anti-EGFR-related adverse events (DOCX 14 kb)
Table 5S: Adverse events related to other molecular targeted therapies (DOCX 15 kb)
Abbreviations
- ICU
Intensive care unit
- AEs
Adverse events
- irAEs
Immunotherapy-related adverse events
- HDU
High-dependency unit
- CCU
Coronary care unit
- EGFR
Epidermal growth factor receptor
Compliance with ethical standards
Conflicts of interest
Authors declare no conflict of interest in relation with this publication.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Allemani C, Matsuda T, Di Carlo V, et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet Lond Engl. 2018;391:1023–1075. doi: 10.1016/S0140-6736(17)33326-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Li F, Zhao C, Wang L. Molecular-targeted agents combination therapy for cancer: developments and potentials. Int J Cancer. 2014;134:1257–1269. doi: 10.1002/ijc.28261. [DOI] [PubMed] [Google Scholar]
- 3.Ott PA, Hodi FS, Kaufman HL, et al. Combination immunotherapy: a road map. J Immunother Cancer. 2017;5:16. doi: 10.1186/s40425-017-0218-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Widakowich C, de Castro G, de Azambuja E, et al. Review: side effects of approved molecular targeted therapies in solid cancers. Oncologist. 2007;12:1443–1455. doi: 10.1634/theoncologist.12-12-1443. [DOI] [PubMed] [Google Scholar]
- 5.Abdel-Wahab N, Shah M, Suarez-Almazor ME. Adverse events associated with immune checkpoint blockade in patients with cancer: a systematic review of case reports. PLoS One. 2016;11:e0160221. doi: 10.1371/journal.pone.0160221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bertrand A, Kostine M, Barnetche T, et al. Immune related adverse events associated with anti-CTLA-4 antibodies: systematic review and meta-analysis. BMC Med. 2015;13:211. doi: 10.1186/s12916-015-0455-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chen TW, Razak AR, Bedard PL, et al. A systematic review of immune-related adverse event reporting in clinical trials of immune checkpoint inhibitors. Ann Oncol Off J Eur Soc Med Oncol. 2015;26:1824–1829. doi: 10.1093/annonc/mdv182. [DOI] [PubMed] [Google Scholar]
- 8.Voskens CJ, Goldinger SM, Loquai C, et al. The price of tumor control: an analysis of rare side effects of anti-CTLA-4 therapy in metastatic melanoma from the ipilimumab network. PLoS One. 2013;8:e53745. doi: 10.1371/journal.pone.0053745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rao J, Feng M, Qian X, et al. Liver transplantation treating the patient with hepatic failure associated with sorafenib treatment: report of a case. Hepatogastroenterology. 2013;60:1317–1319. doi: 10.5754/hge13185. [DOI] [PubMed] [Google Scholar]
- 10.Dilling P, Walczak J, Pikiel P, Kruszewski WJ. Multiple colon perforation as a fatal complication during treatment of metastatic melanoma with ipilimumab—case report. Pol Przegl Chir. 2014;86:94–96. doi: 10.2478/pjs-2014-0017. [DOI] [PubMed] [Google Scholar]
- 11.Mitchell KA, Kluger H, Sznol M, Hartman DJ. Ipilimumab-induced perforating colitis. J Clin Gastroenterol. 2013;47:781–785. doi: 10.1097/MCG.0b013e31828f1d51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Shah R, Witt D, Asif T, Mir FF. Ipilimumab as a cause of severe pan-colitis and colonic perforation. Cureus. 2017;9:e1182. doi: 10.7759/cureus.1182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Nishino M, Sholl LM, Hodi FS, et al. Anti-PD-1-related pneumonitis during cancer immunotherapy. N Engl J Med. 2015;373:288–290. doi: 10.1056/NEJMc1505197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Johnson DB, Balko JM, Compton ML, et al. Fulminant myocarditis with combination immune checkpoint blockade. N Engl J Med. 2016;375:1749–1755. doi: 10.1056/NEJMoa1609214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Loochtan AI, Nickolich MS, Hobson-Webb LD. Myasthenia gravis associated with ipilimumab and nivolumab in the treatment of small cell lung cancer. Muscle Nerve. 2015;52:307–308. doi: 10.1002/mus.24648. [DOI] [PubMed] [Google Scholar]
- 16.Murakami N, Borges TJ, Yamashita M, Riella LV. Erratum: severe acute interstitial nephritis after combination immune-checkpoint inhibitor therapy for metastatic melanoma. Clin Kidney J. 2016;9:649. doi: 10.1093/ckj/sfw058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Loron M-C, Grange S, Guerrot D, et al. Pneumocystis jirovecii pneumonia in everolimus-treated renal cell carcinoma. J Clin Oncol Off J Am Soc Clin Oncol. 2015;33:e45–47. doi: 10.1200/JCO.2013.49.9277. [DOI] [PubMed] [Google Scholar]
- 18.Sandler A, Gray R, Perry MC, et al. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. N Engl J Med. 2006;355:2542–2550. doi: 10.1056/NEJMoa061884. [DOI] [PubMed] [Google Scholar]
- 19.Reck M, von Pawel J, Zatloukal P, et al. Phase III trial of cisplatin plus gemcitabine with either placebo or bevacizumab as first-line therapy for nonsquamous non-small-cell lung cancer: AVAil. J Clin Oncol Off J Am Soc Clin Oncol. 2009;27:1227–1234. doi: 10.1200/JCO.2007.14.5466. [DOI] [PubMed] [Google Scholar]
- 20.Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350:2335–2342. doi: 10.1056/NEJMoa032691. [DOI] [PubMed] [Google Scholar]
- 21.Giantonio BJ, Catalano PJ, Meropol NJ, et al. Bevacizumab in combination with oxaliplatin, fluorouracil, and leucovorin (FOLFOX4) for previously treated metastatic colorectal cancer: results from the Eastern Cooperative Oncology Group Study E3200. J Clin Oncol Off J Am Soc Clin Oncol. 2007;25:1539–1544. doi: 10.1200/JCO.2006.09.6305. [DOI] [PubMed] [Google Scholar]
- 22.Loupakis F, Cremolini C, Masi G, et al. Initial therapy with FOLFOXIRI and bevacizumab for metastatic colorectal cancer. N Engl J Med. 2014;371:1609–1618. doi: 10.1056/NEJMoa1403108. [DOI] [PubMed] [Google Scholar]
- 23.Miller K, Wang M, Gralow J, et al. Paclitaxel plus bevacizumab versus paclitaxel alone for metastatic breast cancer. N Engl J Med. 2007;357:2666–2676. doi: 10.1056/NEJMoa072113. [DOI] [PubMed] [Google Scholar]
- 24.Perren TJ, Swart AM, Pfisterer J, et al. A phase 3 trial of bevacizumab in ovarian cancer. N Engl J Med. 2011;365:2484–2496. doi: 10.1056/NEJMoa1103799. [DOI] [PubMed] [Google Scholar]
- 25.Tewari KS, Sill MW, Long HJ, et al. Improved survival with bevacizumab in advanced cervical cancer. N Engl J Med. 2014;370:734–743. doi: 10.1056/NEJMoa1309748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Chinot OL, Wick W, Mason W, et al. Bevacizumab plus radiotherapy-temozolomide for newly diagnosed glioblastoma. N Engl J Med. 2014;370:709–722. doi: 10.1056/NEJMoa1308345. [DOI] [PubMed] [Google Scholar]
- 27.Moslehi JJ. Cardiovascular toxic effects of targeted cancer therapies. N Engl J Med. 2016;375:1457–1467. doi: 10.1056/NEJMra1100265. [DOI] [PubMed] [Google Scholar]
- 28.Schmidinger M, Zielinski CC, Vogl UM, et al. Cardiac toxicity of sunitinib and sorafenib in patients with metastatic renal cell carcinoma. J Clin Oncol Off J Am Soc Clin Oncol. 2008;26:5204–5212. doi: 10.1200/JCO.2007.15.6331. [DOI] [PubMed] [Google Scholar]
- 29.Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363:711–723. doi: 10.1056/NEJMoa1003466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Larkin J, Chiarion-Sileni V, Gonzalez R, et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N Engl J Med. 2015;373:23–34. doi: 10.1056/NEJMoa1504030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Postow MA, Chesney J, Pavlick AC, et al. Nivolumab and ipilimumab versus ipilimumab in untreated melanoma. N Engl J Med. 2015;372:2006–2017. doi: 10.1056/NEJMoa1414428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Robert C, Schachter J, Long GV, et al. Pembrolizumab versus Ipilimumab in Advanced Melanoma. N Engl J Med. 2015;372:2521–2532. doi: 10.1056/NEJMoa1503093. [DOI] [PubMed] [Google Scholar]
- 33.Robert C, Long GV, Brady B, et al. Nivolumab in previously untreated melanoma without BRAF mutation. N Engl J Med. 2015;372:320–330. doi: 10.1056/NEJMoa1412082. [DOI] [PubMed] [Google Scholar]
- 34.Brahmer J, Reckamp KL, Baas P, et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N Engl J Med. 2015;373:123–135. doi: 10.1056/NEJMoa1504627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Borghaei H, Paz-Ares L, Horn L, et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N Engl J Med. 2015;373:1627–1639. doi: 10.1056/NEJMoa1507643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.De Velasco G, Je Y, Bossé D, et al. Comprehensive meta-analysis of key immune-related adverse events from CTLA-4 and PD-1/PD-L1 inhibitors in cancer patients. Cancer Immunol Res. 2017;5(4):312–318. doi: 10.1158/2326-6066.CIR-16-0237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Eggermont AMM, Chiarion-Sileni V, Grob J-J, et al. Prolonged survival in stage III melanoma with ipilimumab adjuvant therapy. N Engl J Med. 2016;375:1845–1855. doi: 10.1056/NEJMoa1611299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Mohamed AA, Richards CJ, Boyle K, Faust G (2018) Severe inflammatory ileitis resulting in ileal perforation in association with combination immune checkpoint blockade for metastatic malignant melanoma. BMJ Case Rep bcr-2018-224913 [DOI] [PMC free article] [PubMed]
- 39.Wang DY, Salem J-E, Cohen JV, et al. fatal toxic effects associated with immune checkpoint inhibitors: a systematic review and meta-analysis. JAMA Oncol. 2018;4:1721–1728. doi: 10.1001/jamaoncol.2018.3923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Puxty K, McLoone P, Quasim T, et al. Survival in solid cancer patients following intensive care unit admission. Intensive Care Med. 2014;40:1409–1428. doi: 10.1007/s00134-014-3471-9. [DOI] [PubMed] [Google Scholar]
- 41.Johnson DB, Sullivan RJ, Menzies AM. Immune checkpoint inhibitors in challenging populations. Cancer. 2017;123(11):1904–1911. doi: 10.1002/cncr.30642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Spain L, Diem S, Larkin J. Management of toxicities of immune checkpoint inhibitors. Cancer Treat Rev. 2016;44:51–60. doi: 10.1016/j.ctrv.2016.02.001. [DOI] [PubMed] [Google Scholar]
- 43.Weber JS, Kähler KC, Hauschild A. Management of immune-related adverse events and kinetics of response with ipilimumab. J Clin Oncol Off J Am Soc Clin Oncol. 2012;30:2691–2697. doi: 10.1200/JCO.2012.41.6750. [DOI] [PubMed] [Google Scholar]
- 44.Dadu R, Zobniw C, Diab A. Managing adverse events with immune checkpoint agents. Cancer J Sudbury Mass. 2016;22:121–129. doi: 10.1097/PPO.0000000000000186. [DOI] [PubMed] [Google Scholar]
- 45.Haanen JBAG, Carbonnel F, Robert C, et al. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol Off J Eur Soc Med Oncol. 2018;29:iv264–iv266. doi: 10.1093/annonc/mdy162. [DOI] [PubMed] [Google Scholar]
- 46.Chmiel KD, Suan D, Liddle C, et al. Resolution of severe ipilimumab-induced hepatitis after antithymocyte globulin therapy. J Clin Oncol Off J Am Soc Clin Oncol. 2011;29:e237–240. doi: 10.1200/JCO.2010.32.2206. [DOI] [PubMed] [Google Scholar]
- 47.Wolchok JD, Neyns B, Linette G, et al. Ipilimumab monotherapy in patients with pretreated advanced melanoma: a randomised, double-blind, multicentre, phase 2, dose-ranging study. Lancet Oncol. 2010;11:155–164. doi: 10.1016/S1470-2045(09)70334-1. [DOI] [PubMed] [Google Scholar]
- 48.Bakacs T, Mehrishi JN, Szabó M, Moss RW. Interesting possibilities to improve the safety and efficacy of ipilimumab (Yervoy) Pharmacol Res. 2012;66:192–197. doi: 10.1016/j.phrs.2012.03.015. [DOI] [PubMed] [Google Scholar]
- 49.Motzer RJ, Hutson TE, Tomczak P, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. 2007;356:115–124. doi: 10.1056/NEJMoa065044. [DOI] [PubMed] [Google Scholar]
- 50.Escudier B, Eisen T, Stadler WM, et al. Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med. 2007;356:125–134. doi: 10.1056/NEJMoa060655. [DOI] [PubMed] [Google Scholar]
- 51.Kim ES, Hirsh V, Mok T, et al. Gefitinib versus docetaxel in previously treated non-small-cell lung cancer (INTEREST): a randomised phase III trial. Lancet Lond. Engl. 2008;372:1809–1818. doi: 10.1016/S0140-6736(08)61758-4. [DOI] [PubMed] [Google Scholar]
- 52.Mok T, Wu YL, Thongprasert S, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361:947–957. doi: 10.1056/NEJMoa0810699. [DOI] [PubMed] [Google Scholar]
- 53.Maemondo M, Inoue A, Kobayashi K, et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010;362:2380–2388. doi: 10.1056/NEJMoa0909530. [DOI] [PubMed] [Google Scholar]
- 54.Shepherd FA, Rodrigues Pereira J, Ciuleanu T, et al. Erlotinib in previously treated non-small-cell lung cancer. N Engl J Med. 2005;353:123–132. doi: 10.1056/NEJMoa050753. [DOI] [PubMed] [Google Scholar]
- 55.Seto T, Kato T, Nishio M, et al. Erlotinib alone or with bevacizumab as first-line therapy in patients with advanced non-squamous non-small-cell lung cancer harbouring EGFR mutations (JO25567): an open-label, randomised, multicentre, phase 2 study. Lancet Oncol. 2014;15:1236–1244. doi: 10.1016/S1470-2045(14)70381-X. [DOI] [PubMed] [Google Scholar]
- 56.Cunningham D, Humblet Y, Siena S, et al. Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med. 2004;351:337–345. doi: 10.1056/NEJMoa033025. [DOI] [PubMed] [Google Scholar]
- 57.Jonker DJ, O’Callaghan CJ, Karapetis CS, et al. Cetuximab for the treatment of colorectal cancer. N Engl J Med. 2007;357:2040–2048. doi: 10.1056/NEJMoa071834. [DOI] [PubMed] [Google Scholar]
- 58.Van Cutsem E, Köhne CH, Hitre E, et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med. 2009;360:1408–1417. doi: 10.1056/NEJMoa0805019. [DOI] [PubMed] [Google Scholar]
- 59.Vermorken JB, Mesia R, Rivera F, et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N Engl J Med. 2008;359:1116–1127. doi: 10.1056/NEJMoa0802656. [DOI] [PubMed] [Google Scholar]
- 60.Bonner JA, Harari PM, Giralt J, et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N Engl J Med. 2006;354:567–578. doi: 10.1056/NEJMoa053422. [DOI] [PubMed] [Google Scholar]
- 61.Slamon DJ, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. 2001;344:783–792. doi: 10.1056/NEJM200103153441101. [DOI] [PubMed] [Google Scholar]
- 62.Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005;353:1659–1672. doi: 10.1056/NEJMoa052306. [DOI] [PubMed] [Google Scholar]
- 63.Baselga J, Cortés J, Kim SB, et al. Pertuzumab plus trastuzumab plus docetaxel for metastatic breast cancer. N Engl J Med. 2012;366:109–119. doi: 10.1056/NEJMoa1113216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Bang YJ, Van Cutsem E, Feyereislova A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet Lond Engl. 2010;376:687–697. doi: 10.1016/S0140-6736(10)61121-X. [DOI] [PubMed] [Google Scholar]
- 65.Motzer RJ, Escudier B, Oudard S, et al. Efficacy of everolimus in advanced renal cell carcinoma: a double-blind, randomised, placebo-controlled phase III trial. Lancet Lond Engl. 2008;372:449–456. doi: 10.1016/S0140-6736(08)61039-9. [DOI] [PubMed] [Google Scholar]
- 66.Yao JC, Shah MH, Ito T, et al. Everolimus for advanced pancreatic neuroendocrine tumors. N Engl J Med. 2011;364:514–523. doi: 10.1056/NEJMoa1009290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Baselga J, Campone M, Piccart M, et al. Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. N Engl J Med. 2012;366:520–529. doi: 10.1056/NEJMoa1109653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Chapman PB, Hauschild A, Robert C, et al. Improved survival with vemurafenib in melanoma with BRAF V600E mutation. N Engl J Med. 2011;364:2507–2516. doi: 10.1056/NEJMoa1103782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Larkin J, Ascierto PA, Dréno B, et al. Combined vemurafenib and cobimetinib in BRAF-mutated melanoma. N Engl J Med. 2014;371:1867–1876. doi: 10.1056/NEJMoa1408868. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Fig. 1S: Number of published cases by type of targeted therapy over time (JPEG 30 kb)
Table 1S: Oncological licensed indications of reported molecular therapies in adult patients throughout United States and Europe in 2018 (DOCX 132 kb)
Table 2S: Adverse events related to antiangiogenic agents use (DOCX 21 kb)
Table 3S: Immune-related adverse events (DOCX 22 kb)
Table 4S: Anti-EGFR-related adverse events (DOCX 14 kb)
Table 5S: Adverse events related to other molecular targeted therapies (DOCX 15 kb)