

Abstract
Background
Fecal polymerase chain reaction (PCR) testing for Tritrichomonas foetus is considered the most sensitive means for diagnosis of infection but results could be influenced by fecal collection technique and prior use of antimicrobial drugs.
Objectives
To establish any association between fecal collection technique or treatment history and results of fecal PCR testing for T. foetus.
Animals
Fecal samples from 1717 cats submitted by veterinarians between January 2012 and December 2017.
Methods
This study used a retrospective analysis. T. foetus PCR test results from 1808 fecal samples submitted for diagnostic testing were examined for their association with method of fecal collection and prior antimicrobial treatments. Data were collected from sample submission form.
Results
Positive T. foetus PCR test results were obtained for 274 (16%) cats. Fecal samples collected via fecal loop had increased probability of positive PCR test results (odds ratio [OR] 2.04, 95% confidence interval [CI] 1.31‐3.17, P = .002) compared to samples collected by colonic flush. There was no association between PCR test results and treatment history, treatment type, or prior treatment with ronidazole. After an initial positive PCR test, 4/19 (21%; 95% CI 2.7%‐39.4%) cats treated with ronidazole had a second positive test result.
Conclusions and Clinical Importance
Results of this study support that fecal samples collected by loop might be better for PCR diagnosis of T. foetus infection. Lack of association of ronidazole with PCR test results and a 21% all‐potential‐causes failure rate of ronidazole in cats with preconfirmed infection are important limitations to use of this drug.
Keywords: diarrhea, retrospective, risk factors, ronidazole
1. INTRODUCTION
Tritrichomonas foetus is a common cause of chronic large‐bowel diarrhea in cats.1, 2 Over the past 15 years, numerous risk factors for infection have been identified, but definitive diagnosis and treatment of the infection remain challenging.2, 3, 4 Polymerase chain reaction (PCR) testing for the presence of T. foetus rDNA in feces is considered to be the most sensitive means for diagnosis of T. foetus infection in cats.2, 5 Nevertheless, PCR test results are suspected to be influenced by fecal collection technique and recent administration of antimicrobial medications.6, 7 Current recommendations, based on anecdote,7 state that the colonic flush technique is the optimal fecal sample collection method and yields diagnostically superior results compared to voided or loop‐collected fecal samples. Likewise, recent administration of antimicrobial drugs is suspected to decrease the sensitivity of PCR either indirectly or directly by reducing the number of T. foetus organisms.8, 9, 10, 11, 12, 13, 14 The influence of treatment history and specific type of treatment on T. foetus PCR test results has yet to be examined. Based on studies conducted in experimentally infected cats, ronidazole is the only medication effective in eliminating T. foetus infection,15 but clinical outcome is unclear in cats with naturally occurring T. foetus infection.16, 17, 18, 19 Treatment failure with ronidazole is suspected to be common but the incidence of this is largely unknown.20
Without determination of the impact of fecal collection conditions on PCR test results for T. foetus or knowledge of the effectiveness of ronidazole, it remains difficult to optimize diagnosis and expectations of treatment outcome of T. foetus infection. The objective of this study was to explore any relationship between reported fecal collection technique or treatment history and results of fecal PCR testing for T. foetus. This information was gathered by retrospective review of the submission forms accompanying samples submitted for feline T. foetus PCR testing to the North Carolina State University Intestinal Pathogens Research Laboratory. A secondary objective was to evaluate this data set for the presence of risk factors significantly associated with a positive T. foetus PCR test result.
2. MATERIALS AND METHODS
2.1. Sample collection
This was a retrospective study evaluating T. foetus diagnostic PCR test results and submission form data collected by the North Carolina State University Intestinal Pathogens Research Laboratory (NCSU IPRL) from January 2012 to December 2017. Fecal samples were collected from individual cats and submitted by veterinarians to the NCSU IPRL for T. foetus PCR testing. Fecal samples were collected either after voiding, by using a fecal loop inserted through the anus into the colon, or by using a colonic flush technique. The colonic flush technique is performed by inserting an 8‐12 French red rubber catheter through the anus and instilling approximately 10 mL of saline into the proximal colon. The resulting fecal slurry is aspirated back into the syringe and allowed to sediment or is centrifuged, before discarding the saline supernatant.7 Samples were requested to be at least lima bean‐sized, free of litter or other debris, and shipped in isopropyl alcohol at room temperature.
2.2. Data gathering
Each fecal sample was accompanied by a submission form. When reported on the submission form, information gathered included the cat's age, breed, sex, and neuter status, whether the cat was from a single‐ or multiple‐cat household, method of fecal sample collection (voided, fecal loop, or colon flush), and prior treatments administered. The submission form did not request specific information regarding prior treatments such as recency of administration, dose, frequency, or duration. Age was categorized on the basis of life stage21 as kitten (0‐6 months), junior (7‐35 months), prime (36‐83 months), mature (84‐131 months), senior (132‐179 months), and geriatric (180+ months). Domestic longhair, domestic medium hair, and domestic shorthair cats were classified together as “domestic” cats. A geographic map identifying the location of individual veterinary clinics in the United States from which samples were received was created by R (version 3.6.1; Foundation for Statistical Computing, Vienna, Austria).
2.3. DNA extraction and PCR amplification
Upon arrival to the NCSU IPRL, fecal samples were stored for less than 1 week at 4°C before DNA extraction. DNA was extracted from 100 mg of feces by using a previously validated commercial kit (ZR Fecal DNA Kit, Zymo Research, Orange, California).22 All DNA extracts underwent single‐tube nested PCR amplification of 347 and 208 base pair (bp) fragments of the internal transcribed spacer (ITS) region 1, 5.8S, and ITS 2 ribosomal RNA gene by using T. foetus‐specific primers as previously described.5, 22 Reactions generating amplicons that only appeared to be 208 bp in size after gel electrophoresis were digested with the ApoI restriction enzyme (New England Biolabs, Beverly, Massachusetts) at 50°C for 90 minutes. Gel electrophoresis was performed with 10 μL of each digest loaded into a 3.5% agarose gel containing ethidium bromide; confirmatory bands at 89 and 119 bp indicated a positive result. Positive and negative controls were included in each run and consisted of T. foetus‐spiked feline feces and sterile water (extraction controls) and purified T. foetus genomic DNA and sterile water (reaction controls), respectively. Results were collated along with the aforementioned submission form data until analysis.
2.4. Data analysis
Data were examined by using standard descriptive statistics and reported as mean, median, and range where applicable. Age, sex (including neuter status), breed, method of fecal sample collection (void, loop, or saline flush), housing density (single cat versus multiple cats), and type of treatment administered (none, anthelmintic, probiotic, steroid, systemic antibiotic, tylosin, albon or ponazuril, metronidazole, or ronidazole) were considered as variables. A logistic regression model was fit to determine the effect of the various risk factors on incidence of positive T. foetus PCR test results by using backward selection with the Akaike information criteria to reduce the model from an initial containing age, breed, sex, housing density, and the collection method for the sample. Breeds with fewer than 30 cats were combined to an “other” category which was used as the baseline for breed. Domestic breeds were combined into a single “domestic” category. In order to examine the effectiveness of the treatments administered, a logistic regression model was fit with indicator variables for each type of treatment administered with lack of treatment serving as the baseline and intercept for the model. Confidence intervals (CIs) were constructed for 95% confidence. These analyses were performed by R (version 3.6.1; Foundation for Statistical Computing).
3. RESULTS
3.1. Geographic location and housing density
From January 2012 to December 2017, 1808 fecal samples from 1717 individual cats were submitted for T. foetus PCR testing. Repeat testing was performed on 87 cats, with 83 cats having 2 PCR tests performed, and 4 cats having 3 PCR tests performed. Among the 1717 individual cats, 274 (16%) tested positive on initial screening for T. foetus. Fecal samples were submitted from 559 veterinary clinics and 2 commercial laboratories; samples originated from the United States (546), Canada (12), Mexico (1), England (1), and Taiwan (1) (Figure 1).
Figure 1.
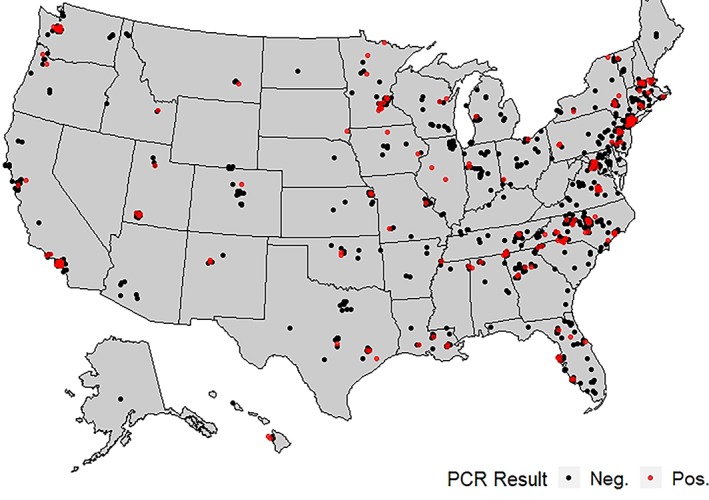
Geographical distribution of veterinary clinics from which fecal samples were submitted for Tritrichomonas foetus polymerase chain reaction testing
Information on housing density was available for 1006 (59%) of the 1717 individual cats. No significant association was observed between PCR result and whether cats were reported to be from a single‐cat household (n = 205 cats; 18% PCR positive) or multi‐cat household (n = 801; 15.6% PCR positive) household.
3.2. Signalment
Age was reported for 1555 (91%) of the 1717 individual cats in this population. The mean and median ages of cats were 3.2 years and 1 year, respectively (range: 9 months to 24 years). Sex and neuter status were reported for 1641 (95%) of the 1717 individual cats (Table 1). Based on the developed logistic regression model, neither life stage nor sex was identified as significantly associated with positive PCR test results for T. foetus infection. However, a small but significant association between decreasing age (when considered as a continuous variable) and probability of PCR positivity was identified (odds ratio [OR] 0.99; 95% CI 0.99‐1.00; P = .04).
Table 1.
Signalment of the 1717 cats included in the study population
| Signalment | Number (%) of cats | Number (%) of cats with positive polymerase chain reaction test result |
|---|---|---|
| Life stage (age in months) | ||
| Kitten (0‐6) | 407 (26) | 73 (18) |
| Junior (7‐35) | 590 (38) | 118 (20) |
| Prime (36‐83) | 267 (17) | 34 (13) |
| Mature (84‐131) | 166 (11) | 18 (11) |
| Senior (132‐179) | 103 (7) | 7 (7) |
| Geriatric (180+) | 22 (1) | 3 (14) |
| Sex and neuter status | ||
| Male, intact | 260 (16) | 69 (27) |
| Male, castrated | 611 (37) | 86 (14) |
| Female, intact | 302 (18) | 50 (17) |
| Female, spayed | 468 (29) | 62 (13) |
Breed was reported for 1570 (91%) of the 1717 individual cats. Forty‐one different breeds were represented. The most common breed was the domestic cat. Based on the results of the logistic regression analysis, when compared to this referent “other” group that comprises all breeds with less than 30 samples submitted, domestic cats were approximately 4 times less likely than other cats to have a positive PCR test result. The only breed with significantly increased odds for positive PCR test results compared to other cats was the Abyssinian (Table 2).
Table 2.
Results of the logistic regression model examining association between breed and positive results of Tritrichomonas foetus polymerase chain reaction (PCR) testing
| Breed | Number (%) of cats | Number (%) of cats with positive PCR test result | OR | 95% CI | P value |
|---|---|---|---|---|---|
| Domestic | 866 (55) | 76 (9) | 0.24 | 0.14‐0.42 | <.001*** |
| Bengal | 205 (13) | 48 (23) | 0.94 | 0.52‐1.68 | .83 |
| Abyssinian | 81 (5) | 31 (38) | 2.11 | 1.09‐4.08 | .03* |
| Siamese | 65 (4) | 16 (25) | 1.03 | 0.39‐2.47 | .95 |
| Ragdoll | 61 (4) | 14 (23) | 1.42 | 0.58‐3.29 | .43 |
| Persian | 38 (2) | 11 (29) | 1.47 | 0.51‐3.94 | .46 |
| Maine Coon | 38 (2) | 8 (21) | 0.62 | 0.17‐1.82 | .42 |
| Sphinx | 31 (2) | 7 (23) | 0.54 | 0.08‐2.14 | .44 |
| Devon Rexa | 15 (1) | 2 (13) | ‐ | ‐ | ‐ |
| Highlandera | 13 (1) | 4 (31) | ‐ | ‐ | ‐ |
| Burmesea | 12 (1) | 3 (25) | ‐ | ‐ | ‐ |
| Siberiana | 12 (1) | 0 (0) | ‐ | ‐ | ‐ |
| Savannaha | 11 (1) | 5 (46) | ‐ | ‐ | ‐ |
| Cornish Rexa | 10 (1) | 5 (50) | ‐ | ‐ | ‐ |
| British Shorthaira | 10 (1) | 1 (10) | ‐ | ‐ | ‐ |
| Himalayana | 10 (1) | 1 (10) | ‐ | ‐ | ‐ |
Note: Odds ratio (OR), 95% confidence interval (CI), and P value for significant association with positive results of PCR testing for T. foetus are shown for each variable. Breeds represented by fewer than 10 cats (number of cats): Norwegian Forest cat (8), Balinese (7), Exotic shorthair (7), Tonkinese (7), Birman (6), Egyptian Mau (6), Russian Blue (6), Scottish Fold (6), Ocicat (5), Oriental shorthair (5), Manx (4), Somali (4), Japanese Bobtail (3), Pixie‐bob (3), Bombay (2), Cheetoh (2), Havanese (2), Singapura (2), Australian Mist cat (1), Chartreux (1), Ragamuffin (1), Serval (1), Snowshoe (1), Thai (1), Turkish Angora (1).
Breeds represented by fewer than 30 cats were combined and used as the baseline category for the logistic regression model.
3.3. Reason for sample submission
A reason for sample submission was provided for 792 (46%) of the 1717 individual cats. The most common reason for sample submission was a history of diarrhea (n = 648 cats; 15% PCR positive), followed by exposure to other cats that had tested positive (n = 39 cats, 31% PCR positive), general screening of cats with no clinical signs due to at‐risk breed, age, or breeder's request (n = 26 cats; 23% PCR positive), and retesting after a previously positive test (n = 25 cats; 48% PCR positive). Multiple reasons were provided for 54 (7%) cats, including having diarrhea as well as exposure to positive cats (n = 28 cats; 21% PCR positive), and having diarrhea as well as a previously positive test (n = 26 cats; 19% PCR positive).
3.4. Fecal sample collection method
The method of fecal sample collection was reported for 1016 (59%) of the 1717 individual cats. Samples were collected after voiding from 314 (31%) cats, with use of a fecal loop from 237 (23%) cats, or by using the colonic flush technique from 465 (46%) cats. Based on the results of the logistic regression analysis, fecal samples that were collected by using a fecal loop were 2.04 times more likely to be associated with a positive PCR test result compared to fecal samples collected by using the colonic flush technique (Table 3).
Table 3.
Distribution of 1016 fecal samples by method of collection and results of logistic regression examining an association with positive polymerase chain reaction (PCR) test results for Tritrichomonas foetus
| Fecal collection method | Number (%) of cats | Number (%) of cats with positive PCR test result | OR | 95% CI | P value |
|---|---|---|---|---|---|
| Voided | 314 (31) | 46 (15) | 1.09 | 0.68‐1.72 | .72 |
| Looped | 237 (23) | 54 (23) | 2.04 | 1.31‐3.17 | .002** |
| Flusheda | 465 (46) | 64 (14) | ‐ | ‐ | ‐ |
Note: Odds ratio (OR), 95% confidence interval (CI), and P value for significant association with positive results of PCR testing for T. foetus are shown for each variable.
This group composed the baseline category for the logistic regression model.
3.5. Impact of reported prior treatment
A treatment history was provided for 571 (33%) of the 1717 individual cats in the study. Treatments were divided into the following categories: metronidazole, anthelmintics, ronidazole, probiotics, albon or ponazuril, steroids, systemic antibiotics, tylosin, and no treatment. There was no significant association between PCR test results for T. foetus and prior administration of any treatment, any individual treatment category, or lack of prior treatment (Table 4).
Table 4.
Treatments administered to 571 cats before initial sample submission and their association with positive polymerase chain reaction (PCR) test results for Tritrichomonas foetus based on results of logistic regression
| Prior treatment administered | Number (%) of catsa | Number (%) of cats with positive PCR test result | Compared to no treatment | ||
|---|---|---|---|---|---|
| OR | 95% CI | P value | |||
| Metronidazole | 322 (56) | 39 (12) | 0.68 | 0.40‐1.14 | 0.14 |
| Anthelmintics | 172 (30) | 23 (13) | 1.09 | 0.61‐1.93 | 0.78 |
| Ronidazole | 103 (18) | 19 (18) | 1.00 | 0.51‐1.89 | 0.99 |
| Probiotics | 96 (17) | 12 (13) | 0.91 | 0.44‐1.76 | 0.79 |
| Albon or ponazuril | 87 (15) | 9 (10) | 0.72 | 0.31‐1.53 | 0.41 |
| Steroids | 70 (12) | 9 (13) | 1.01 | 0.44‐2.08 | 0.98 |
| Systemic antibiotics | 51 (9) | 9 (18) | 0.36 | 0.09‐1.03 | 0.10 |
| Tylosin | 32 (6) | 3 (9) | 0.40 | 0.06‐1.40 | 0.23 |
| No treatment | 62 (11) | 2 (3) | ‐ | ‐ | ‐ |
Note: Odds ratio (OR), 95% confidence interval (CI), and P value for significant association with positive results of PCR testing for T. foetus are shown for each variable as compared to no treatment.
Individual cats may have received >1 treatment and therefore may appear in >1 group.
3.6. Repeat testing
Of the 87 cats that had repeat PCR testing performed, 54 cats (62%) had a negative result for all tests, 3 cats (3%) were negative initially and positive on subsequent testing, 8 cats (9%) were positive on all tests, 21 cats (24%) tested positive initially with a negative subsequent test, and 1 cat (1%) tested positive initially followed by a negative and then positive subsequent tests.
Ronidazole was reported to have been administered to 42 cats before repeat testing, with 23 (55%) of these cats having had a negative result both before and after treatment. Nineteen cats were positive on initial testing before receiving ronidazole. After treatment, 15 (79%) of these cats tested negative for T. foetus, whereas 4 (21%) remained positive. The mean intertest interval for these cats was 2.5 months (range 0.5‐6.5 months). All 4 cats that remained positive, as well as 14 of the 15 of the cats with negative subsequent test results, were from multi‐cat households.
4. DISCUSSION
The overall prevalence of positive results of samples submitted for T. foetus PCR testing in this study was 16%. Most of the samples were collected from cats residing in the United States. Reasons for sample submission included testing cats that were having diarrhea, exposure to other cats that previously tested positive, general screening for cats without clinical signs, and cats undergoing repeat testing following a previously positive test. The majority of samples were from cats less than 3 years of age. A metadata analysis of multiple prior studies has identified that cats less than or equal to 1 year of age were 2.1 times more likely to be infected with T. foetus.23 In the present study, we divided this sample population into ages based on life stage, which might be more physiologically and socially pertinent. Following multiple logistic regression analysis, we did not observe a significant association between life stage and probability of a positive PCR test result for T. foetus infection. However, when age was evaluated as a continuous variable, a significant negative association was found between age and PCR positivity. This supports the general clinical impression that younger cats are more likely to be diagnosed with T. foetus infection, whereas older cats may be at less risk of infection.
Male cats are reported to be more likely to have positive PCR test results for T. foetus.23, 24, 25, 26 By dividing these groupings further into sex and neuter status, and in consideration of other factors including age and breed, we did not observe a significant association between sex and probability of a positive PCR test result for T. foetus infection. Odds ratios for diagnosis of T. foetus infection in purebred cats range from 26.325 to >999.9.27 Siamese and Bengal breeds appear to be at a greater risk in the United Kingdom,27 Norwegian Forest cats in Germany,28 and Abyssinian, Bengal, and Siamese cats in the United States.3 Based on the results of a multiple regression analysis, only the Abyssinian breed was identified as having increased probability of a positive PCR test result for T. foetus infection in this study population. Breeds that were represented by fewer than 30 cats were not included in the analysis and therefore were not tested for an association. It is likely that differences in breed prevalence from country to country accounts for some variation in breeds observed to be at significantly increased odds of infection. In contrast to purebred cats, domestic cats were significantly less likely than other breeds to have a positive PCR test result. Contrary to several prior studies,2, 25, 29 we did not identify a significant difference in odds of positive T. foetus PCR test results between cats living in a single‐ or multiple‐cat household. The number of other cats in the household was not quantified and could therefore be a limiting factor in this analysis. One study has previously shown that cats sharing a house with more than 5 cats are 4.6 times more likely to be infected with T. foetus.25
Results of this study identify that fecal samples collected by using a fecal loop were 2.04 times more likely to be associated with positive PCR test results for T. foetus compared to samples collected by using the colon flush technique. This finding challenges the assumption that colon flush is the best fecal collection technique,7 and merits consideration for a specific prospective study to determine the impact of sample collection technique on fecal PCR test results for T. foetus. Results of the present study cannot be interpreted as proving a causal association. However, it is compelling to speculate that the fecal loop could promote collection of samples from the surface of the colonic mucosa where the trichomonads are found to adhere to the mucus and epithelial lining.30, 31
A variety of treatments were reportedly administered to cats before PCR testing for T. foetus. Many of these medications have already been shown to be ineffective for treatment of feline T. foetus 1, 6, 15, 32 and none were associated with decreased odds for positive PCR test results. Cats reported to have received no prior treatment were also no more likely to test positive for T. foetus by PCR, suggesting that these medications also did not interfere with PCR testing. The authors have previously suggested that concurrent administration of antimicrobials should be avoided when testing cats for T. foetus infection because of concerns that doing so may decrease PCR sensitivity.7 These findings do not necessarily negate this concern because information on the timing of treatment relative to fecal collection was not requested on the sample submission forms.
Before initial testing, 18% of cats were reported to have been treated with ronidazole. Cats with this history did not have decreased odds of testing positive for T. foetus by PCR. Among a small group of 19 cats with an original positive PCR test result for T. foetus, 21% remained PCR positive when subsequently retested after reported treatment with ronidazole. These results, coupled with failure of ronidazole to decrease odds of positive PCR results compared to cats receiving no treatment or any other treatment, suggest that ronidazole could be less effective than previously thought. Ronidazole resistance, reinfection, PCR amplification of DNA from dead T. foetus, or failure to administer the recommended dose or duration of ronidazole might all contribute to these findings. Although the 4 cats that remained PCR positive on subsequent testing were all reported as living in multiple cat households, it is of interest to note that 14 of the 15 cats that had a negative repeat test were also reported as living in multiple cat households. Accordingly, any clinical suspicion that treatment failures are more common in households with multiple cats was not supported by the results of this study. Ultimately, an unambiguous determination of treatment efficacy in naturally infected cats would require a prospective, randomized study comparing ronidazole treatment and no treatment arms. There are few studies reporting follow‐up test results of cats after treatment of naturally occurring T. foetus infection with ronidazole, with failure rates ranging from 5 to 25%. Twenty‐four cats with T. foetus infection treated with ronidazole at 30 mg/kg PO q12h were subsequently negative for T. foetus by culture of a rectal swab but positive results were observed in the only cat tested by means of PCR.19 After treatment of 12 cats with ronidazole at 30 mg/kg PO q12h, 9 cats tested negative for T. foetus by means of PCR (7 cats) or fecal wet mount (2 cats).17 Treatment of 25 T. foetus infected cats with guar gum‐coated ronidazole at 30 mg/kg q24h for 14 days resulted in 21 cats (84%) testing negative for T. foetus by means of PCR performed on a fecal swab.18 Collectively, these studies are apt to underestimate the prevalence of ronidazole treatment failure because of small fecal sample sizes (eg, swab) and use of tests with lower sensitivity than PCR (wet mount or culture).
This study was necessarily limited in scope to information that could be obtained from data reported on a submission form created 8 years before conception of the study. Not all veterinarians answered each question and these findings are reliant on the completeness and accuracy of the information that was provided. Accordingly, data analysis was limited to only questions for which answers were recorded. It is also important to note that the questionnaire submitted with each fecal sample did not request specific information regarding previous treatments, such as recency of administration, dose, frequency, and duration. This reported failure rate of ronidazole could therefore be skewed because of many undetermined factors including unknown dose, duration, formulation, and owner compliance. Although PCR is considered the most sensitive test for detection of feline T. foetus, there exists no gold standard for diagnosis of the infection. Test results are likely influenced by sample collection method (as demonstrated in this study), handling, shipment, or other undetermined factors. Every cat did not undergo each sample collection technique, thus making it impossible to establish a causal relationship between sample collection technique and results of T. foetus PCR testing. Nonetheless, while considering multiple risk factors in this large and diverse sample population, collection technique remained as a significant factor associated with results of T. foetus PCR testing.
Identification of risk factors, optimal sample collection techniques, and expectations of treatment efficacy are integral in providing a timely and accurate diagnosis and treatment for T. foetus infection. Risk factors for PCR diagnosis of T. foetus infection identified in this study include decreasing age of the cat and Abyssinian breed. Polymerase chain reaction identification of T. foetus was more common in samples collected with a fecal loop. Test results were not influenced by medications that the cats had received before testing, though the timing of medication administration relative to sample collection was unknown. In cats that underwent repeated PCR testing, ronidazole was found to have a 21% failure rate in eliminating T. foetus infection. The aforementioned findings provide compelling support for additional prospective studies examining the influence of fecal collection technique and efficacy of ronidazole on results of T. foetus PCR testing in cats.
CONFLICT OF INTEREST DECLARATION
The corresponding author's laboratory offers commercial PCR testing for feline T. foetus infection. The data described in the manuscript were obtained from these accessions. Results of this study do not promote the use of PCR or the choice of where clinicians submit their samples for PCR testing.
OFF‐LABEL ANTIMICROBIAL DECLARATION
Authors declare no off‐label use of antimicrobials.
INSTITUTIONAL ANIMAL CARE AND USE COMMITTEE (IACUC) OR OTHER APPROVAL DECLARATION
Authors declare no IACUC or other approval was needed.
HUMAN ETHICS APPROVAL DECLARATION
Authors declare human ethics approval was not needed for this study.
Abbreviations
- bp
base pair
- ITS
internal transcribed spacer
- NCSU IPRL
North Carolina State University Intestinal Pathogens Research Laboratory
- PCR
polymerase chain reaction
ACKNOWLEDGMENTS
The authors thank Laura Whisenant, Katherine Hanrahan, Brittany Bellis, Sophia Amirsultan, and Morgan Fitch for their assistance with this project.
Hedgespeth BA, Stauffer SH, Robertson JB, Gookin JL. Association of fecal sample collection technique and treatment history with Tritrichomonas foetus polymerase chain reaction test results in 1717 cats. J Vet Intern Med. 2020;34:734–741. 10.1111/jvim.15727
Funding information North Carolina Veterinary Medical Foundation STRIVE FUND (Support for T. foetus Research Innovation and Veterinary Education)
REFERENCES
- 1. Gookin JL, Breitschwerdt EB, Levy MG, et al. Diarrhea associated with trichomonosis in cats. J Am Vet Med Assoc. 1999;215:1450‐1454. [PubMed] [Google Scholar]
- 2. Gookin JL, Stebbins ME, Hunt E, et al. Prevalence of and risk factors for feline Tritrichomonas foetus and Giardia infection. J Clin Microbiol. 2004;42:2707‐2710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Queen EV, Marks SL, Farver TB. Prevalence of selected bacterial and parasitic agents in feces from diarrheic and healthy control cats from Northern California. J Vet Intern Med. 2012;26:54‐60. [DOI] [PubMed] [Google Scholar]
- 4. Galián M, Heusinger A, Gentil M, et al. Tritrichomonas fetus in cats. Argos Informativo Veterinario. 2011;134:44‐45. [Google Scholar]
- 5. Gookin JL, Birkenheuer AJ, Breitschwerdt EB, Levy MG. Single‐tube nested PCR for detection of Tritrichomonas foetus in feline feces. J Clin Microbiol. 2002;40:4126‐4130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Foster DM, Gookin JL, Poore MF, Stebbins ME, Levy MG. Outcome of cats with diarrhea and Tritrichomonas foetus infection. J Am Vet Med Assoc. 2004;225:888‐892. [DOI] [PubMed] [Google Scholar]
- 7. Gookin JL, Hanrahan K, Levy MG. The conundrum of feline Trichomonosis. J Feline Med Surg. 2017;19:261‐274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Tolbert MK, Gookin JL. Mechanisms of Tritrichomonas foetus pathogenicity in cats with insights from venereal trichomonosis. J Vet Intern Med. 2016;30:516‐526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Figueroa‐Angulo EE, Rendon‐Gandarilla FJ, Puente‐Rivera J, et al. The effects of environmental factors on the virulence of Trichomonas vaginalis . Microbes Infect. 2012;14:1411‐1427. [DOI] [PubMed] [Google Scholar]
- 10. Midlej V, Benchimol M. Trichomonas vaginalis kills and eats—evidence for phagocytic activity as a cytopathic effect. Parasitology. 2010;137:65‐76. [DOI] [PubMed] [Google Scholar]
- 11. Pereira‐Neves A, Benchimol M. Phagocytosis by Trichomonas vaginalis: new insights. Biol Cell. 2007;99:87‐101. [DOI] [PubMed] [Google Scholar]
- 12. Rendon‐Maldonado JG, Espinosa‐Cantellano M, Gonzalez‐Robles A, et al. Trichomonas vaginalis: in vitro phagocytosis of lactobacilli, vaginal epithelial cells, leukocytes, and erythrocytes. Exp Parasitol. 1998;89:241‐250. [DOI] [PubMed] [Google Scholar]
- 13. Francioli P, Shio H, Roberts RB, Muller M. Phagocytosis and killing of Neisseria gonorrhoeae by Trichomonas vaginalis . J Infect Dis. 1983;147:87‐94. [DOI] [PubMed] [Google Scholar]
- 14. Demirezen S. Phagocytosis of rod‐shaped bacteria and cocci by Trichomonas vaginalis: light microscopic observations. Acta Cytol. 2001;45:1088‐1089. [PubMed] [Google Scholar]
- 15. Gookin JL, Copple CN, Papich MG, et al. Efficacy of ronidazole for treatment of feline Tritrichomonas foetus infection. J Vet Intern Med. 2006;20:536‐543. [DOI] [PubMed] [Google Scholar]
- 16. Xenoulis PG, Lopinski DJ, Read SA, Suchodolski JS, Steiner JM. Intestinal Tritrichomonas foetus infection in cats: a retrospective study of 104 cases. J Feline Med Surg. 2013;15:1098‐1103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Bell ET, Gowan RA, Lingard AE, McCoy RJ, Šlapeta J, Malik R. Naturally occurring Tritrichomonas foetus infections in Australian cats: 38 cases. J Feline Med Surg. 2010;12:889‐898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Grellet A, Makhlouf SE, Desquilbet L, et al. Efficacy of guar gum‐based ronidazole capsules as a treatment for Tritrichomonas foetus infection in cats. J Feline Med Surg. 2017;19:177‐184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Holliday M, Deni D, Gunn‐Moore DA. Tritrichomonas foetus infection in cats with diarrhoea in a rescue colony in Italy. J Feline Med Surg. 2009;11:131‐134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Gookin JL, Stauffer SH, Dybas D, Cannon DH. Documentation of in vivo and in vitro aerobic resistance of feline T. foetus isolates to ronidazole. J Vet Intern Med. 2010;24:1003‐1007. [DOI] [PubMed] [Google Scholar]
- 21. Vogt AH, Rodan I, Brown M, et al. AAFP–AAHA feline life stage guidelines. J Am Anim Hosp Assoc. 2010;46:70‐85. [DOI] [PubMed] [Google Scholar]
- 22. Stauffer SH, Birkenheuer AJ, Levy MG, Marr H, Gookin JL. Evaluation of four DNA extraction methods for the detection of Tritrichomonas foetus in feline stool specimens by polymerase chain reaction. J Vet Diagn Invest. 2008;20:639‐641. [DOI] [PubMed] [Google Scholar]
- 23. Yao C, Koster LS. Tritrichomonas foetus infection, a cause of chronic diarrhea in the domestic cat. Vet Res. 2015;46:35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Gray SG, Hunter SA, Stone MR, Gookin JL. Assessment of reproductive tract disease in cats at risk for Tritrichomonas foetus . Am J Vet Res. 2010;71:76‐81. [DOI] [PubMed] [Google Scholar]
- 25. Hosein A, Kruth SA, Pearl DL, et al. Isolation of Tritrichomonas foetus from cats sampled at a cat clinic, cat shows and a humane society in southern Ontario. J Feline Med Surg. 2013;15:706‐711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Koster LS, Chow C, Yao C. Trichomonosis in cats with diarrhoea in Hong Kong, China, between 2009 and 2014. JFMS Open Reports. 2015;1:2055116915623561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Gunn‐Moore DA, McCann TM, Reed N, et al. Prevalence of Tritrichomonas foetus infection in cats with diarrhoea in the UK. J Feline Med Surg. 2007;9:214‐218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Kuehner KA, Marks SL, Kass PH, et al. Tritrichomonas foetus infection in purebred cats in Germany: prevalence of clinical signs and the role of co‐infection with other enteroparasites. J Feline Med Surg. 2011;13:251‐258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Arranz‐Solis D, Pedraza‐Diaz S, Miro G, et al. Tritrichomonas foetus infection in cats with diarrhea from densely housed origins. Vet Parasitol. 2016;221:118‐122. [DOI] [PubMed] [Google Scholar]
- 30. Tolbert MK, Stauffer SH, Brand MD, Gookin JL. Cysteine protease activity of feline Tritrichomonas foetus promotes adhesion‐dependent cytotoxicity to intestinal epithelial cells. Infect Immun. 2014;82:2851‐2859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Tolbert MK, Stauffer SH, Gookin JL. Feline Tritrichomonas foetus adhere to intestinal epithelium by receptor‐ligand‐dependent mechanisms. Vet Parasitol. 2013;192:75‐82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Gookin JL, Levy MG, Law MJ, et al. Experimental infection of cats with Tritrichomonas foetus . Am J Vet Res. 2001;62:1690‐1697. [DOI] [PubMed] [Google Scholar]