

Abstract
Adult-onset Still’s disease (AoSD) is a rare but clinically well-known, polygenic, systemic autoinflammatory disease. Owing to its sporadic appearance in all adult age groups with potentially severe inflammatory onset accompanied by a broad spectrum of disease manifestation and complications, AoSD is an unsolved challenge for clinicians with limited therapeutic options. This Review provides a comprehensive insight into the complex and heterogeneous nature of AoSD, describing biomarkers of the disease and its progression and the cytokine signalling pathways that contribute to disease. The efficacy and safety of biologic therapeutic options are also discussed, and guidance for treatment decisions is provided. Improving the approach to AoSD in the future will require much closer cooperation between paediatric and adult rheumatologists to establish common diagnostic strategies, treatment targets and goals.
Subject terms: Rheumatic diseases, Inflammatory diseases, Diagnosis, Therapeutics
Adult-onset Still’s disease (AoSD) is not easily diagnosed, and treatment options are limited. This Review provides an overview of the disease and its pathogenesis, clinical trial results, therapeutic options and a plan to diagnose and clinically manage these patients.
Key points
Similar to systemic-onset juvenile idiopathic arthritis, adult-onset Still’s disease (AoSD) is a rare systemic autoinflammatory disease with potentially severe inflammatory onset accompanied by a broad spectrum of disease manifestation and complications.
AoSD should be considered in patients with persistent fever, and the diagnosis is based on the combination of clinical and laboratory findings as well as the exclusion of other inflammatory conditions.
Central to the pathogenesis of AoSD is the intense activation of innate immune cells and overproduction of several pro-inflammatory cytokines including IL-1, IL-6 and IL-18.
Two IL-1 antagonists have been approved for treatment of AoSD, and growing evidence suggests that other biologic agents are therapeutic options, such as anti-IL-6 and anti-IL-18 therapeutics.
As a reliable prediction of response and outcome is not possible, therapeutic decisions have to be made on the basis of clinical, biological or imaging characteristics of disease.
A close cooperation between paediatric and adult rheumatologists is required to establish common diagnostic strategies, treatment targets and goals.
Introduction
Adult-onset Still’s disease (AoSD) was first described in the early 1970s, by Eric Bywaters1, as an inflammatory condition in young adults. The disease was similar to childhood-onset Still’s disease (today called systemic-onset juvenile idiopathic arthritis (SoJIA)), which was described a century ago by Sir John Still2. Although the exact pathogenic mechanisms of the disease are unknown, substantial advances have been made to confirm the homology between AoSD and SoJIA; and AoSD has become the archetype of non-familial, or sporadic, systemic autoinflammatory disorders3–5.
This article addresses the immune background of AoSD including new biomarkers as well as treatment options. Furthermore, in accordance with the respective clinical manifestations, we give guidance for appropriate treatment decisions.
Autoimmunity versus autoinflammation
In the mid-2000s the hypotheses of two main pathogenic mechanisms underlying immune-mediated inflammation against the self were formulated, and a new classification for immunological diseases was proposed that distinguished autoimmunity from autoinflammation3,6. The term autoimmunity was used to refer to adaptive immunity and was defined as aberrant dendritic cell, B cell and T cell responses in primary and secondary lymphoid organs leading to a break in tolerance and development of immune reactivity towards native antigens (with autoantibodies in most cases). The term autoinflammation was used to refer to innate immunity and was defined as dysregulated activation of macrophages and neutrophils in response to a danger signal leading to tissue damage. These categories represent a continuum, which enabled a new classification of immune-mediated inflammatory disorders to be refined in subsequent years3,5.
The diagnosis of autoimmune diseases is often supported by the presence of autoantibodies or autoantigen-specific T cells and B cells. By contrast, no specific biomarker exists for systemic autoinflammatory disorders. The definition mainly relies on similarities with monogenic, hereditary periodic fever syndromes, which were at the origin of the concept. Autoinflammatory diseases have several key features, including intense inflammation with periodic fever, tissue inflammation depending on the disease, increased leukocyte and neutrophil counts, elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level, a pathogenic function of the inflammasome and a therapeutic response to IL-1 blockade7–9. Aside from monogenic familial syndromes, Crohn’s disease was the first classified non-familial polygenic autoinflammatory disorder10,11. A few years later, Still’s disease (SoJIA and AoSD) was described as another non-familial autoinflammatory disorder, becoming one of the most characteristic polygenic systemic autoinflammatory disorders4,12.
Pathogenesis
Our understanding of the mechanisms underlying AoSD pathogenesis is mostly hypothetical, but studies of patients with SoJIA and a generally growing understanding of systemic autoinflammatory disorders suggest the involvement of a pro-inflammatory cascade4,8,13,14 (Fig. 1).
Fig. 1. Pathogenic pathways in AoSD.

Danger signals (pathogen-associated molecular patterns (PAMPs) and damage-associated molecular patterns (DAMPs), such as infections or environmental chemical factors) are transmitted to macrophages and neutrophils through Toll-like receptors (TLRs), which excessively activate the NACHT, LRR and PYD domains-containing protein 3 (NLRP3) inflammasome in patients with a predisposing genetic background. This excessive activation of NLRP3 seems to be central and leads to intense production of IL-1β and IL-18. These cytokines intensely stimulate innate immune cell activation, as well as adaptive immune cells, leading to overproduction of several pro-inflammatory cytokines including IL-6, IL-8, IL-17 and TNF, as well as further production of IL-1β and IL-18. Several factors actively contribute to this amplified inflammatory response, which is often referred to as the cytokine ‘burst’ or ‘storm’. In addition to IL-1β itself conferring retrograde activation of macrophages and neutrophils, alarmins such as the S100 proteins and advanced glycation end products (AGEs) are involved. Aside from the amplification mechanisms, deficiency or failure in regulatory or anti-inflammatory mechanisms might be involved in the pathogenesis of autoinflammatory diseases, including deficiency in regulatory T (Treg) cells or natural killer (NK) cells, insufficient IL-10 production and deficiency in production of resolving lipid mediators, soluble receptors of AGEs (sRAGEs) or other resolution-associated molecular patterns (RAMPs). Hence, adult-onset Still’s disease (AoSD) pathogenesis is related to an imbalance between inflammation and resolution. DC, dendritic cell; ER, endoplasmic reticulum; PMN, polymorphonuclear neutrophil; ROS, reactive oxygen species; TGFβ, transforming growth factor-β; TH1, T helper 1; TH17, T helper 17.
A cytokine storm
The starting point of the pro-inflammatory cascade is probably specific danger signals such as pathogen-associated molecular patterns (PAMPs) or damage-associated molecular patterns (DAMPs). These danger signals are transmitted to macrophages and neutrophils via specific Toll-like receptors (TLRs) that activate specific inflammasomes, probably NACHT, LRR and PYD domains-containing protein 3 (NLRP3), leading to caspase activation and overproduction of active IL-1β9,14–16. This step seems to be central to the pathogenesis of AoSD and leads to intense innate immune cell activation and overproduction of several pro-inflammatory cytokines including IL-6, IL-8, IL-17, IL-18 and TNF9,14–16 (Fig. 1). Several factors actively contribute to an amplified inflammatory response, which is often referred to as the cytokine ‘burst’ or ‘storm’ (refs4,16). In addition to IL-1 itself conferring retrograde activation of macrophages and neutrophils, different alarmins such as the S100 proteins (with S100A12 seeming to be more specific to SoJIA) and advanced glycation end products (AGEs) are involved in these processes14,16–20. Aside from amplification mechanisms, deficiency or failure in regulatory or anti-inflammatory mechanisms might be involved in the pathogenesis of autoinflammatory diseases, including deficiency in regulatory T cells or natural killer cells, insufficient IL-10 production and deficiency in clearance of lipid mediators or production of soluble receptors of AGEs (sRAGEs) or other resolution-associated molecular patterns (RAMPs)21–24.
Infectious triggers
Bacteria or viruses are the usual suspects for the generation of danger signals. Many case reports describe the occurrence of AoSD after viral infection (with rubella virus, measles morbillivirus, mumps virus, Epstein–Barr virus, hepatitis A virus, hepatitis B virus, hepatitis C virus, HIV, cytomegalovirus, parvovirus B19, adenovirus, echovirus, human herpesvirus 6, influenza virus, parainfluenza viruses or coxsackie virus) or bacterial infection (with Yersinia enterocolitica, Campylobacter jejuni, Chlamydia trachomatis, Chlamydia pneumoniae, Mycoplasma pneumoniae or Borrelia burgdorferi)4,13,14. In addition, patients often experience odynophagia (sore throat) or pharyngitis just before the start of the disease or before a relapse25,26, which could correspond to the infectious danger signal that triggers TLRs and inflammation.
A role for genetics
In contrast to monogenic, hereditary, periodic fever syndromes, the underlying genetic background of AoSD is mostly unknown. The disease is present in different geographical regions and different ethnic groups4,5,13,14,27. Association studies have suggested a predisposing genetic background; however, no functional analysis has confirmed this hypothesis4,14,28. Two major findings have been reported in patients with SoJIA. First, a homoallelic missense mutation in LACC1 (which encodes the enzyme laccase domain-containing protein 1, a multicopper oxidoreductase) has been identified in 13 patients with SoJIA from 5 consanguineous families in Saudi Arabia29. This oxidoreductase promotes fatty-acid oxidation, with concomitant inflammasome activation, mitochondrial and NADPH-oxidase-dependent production of reactive oxygen species and bactericidal activity of macrophages30. Second, a large association study of 982 children with SoJIA and 8,010 healthy individuals identified a strong association between SoJIA and different HLA-DRB1*11 haplotypes, which all encode glutamate 58 (ref.31). This finding is unexpected, as it would implicate the involvement of adaptive immunity in the pathogenesis of Still’s disease. However, it is unclear whether the same risk alleles are also associated with AoSD32. Finally, the substantial advances made in exploring the human genome will facilitate the identification of potential mutations in genes involved in autoinflammatory pathways, including de novo germinal mutations or somatic mutations occurring during fetus development or after birth33,34.
Diagnostic and clinical manifestations
Prevalence and incidence
AoSD satisfies the definition of an orphan disease because its prevalence has been estimated at between 1 affected person per million in Europe35 and 10 affected people per million in Japan36. In the Japanese study, the incidence was estimated at ~1 affected person per million in the mid-1990s. Initially, the disease was characterized as affecting only young adults (that is, 16–35 years of age1); however, other series have identified cases in adults >35 years old and even in people >60 years old37–41. The sex ratio is almost balanced, with only a slight female predominance37,39–43. However, because of the substantial advances in AoSD diagnosis as well as differential diagnoses during the past two decades, these older prevalence and incidence estimates might be outdated, and new studies are needed to update these figures.
Common manifestations of AoSD
AoSD is traditionally characterized by four cardinal symptoms, with many other manifestations that can be associated4,13 (Fig. 2).
Fig. 2. Signs of AoSD.
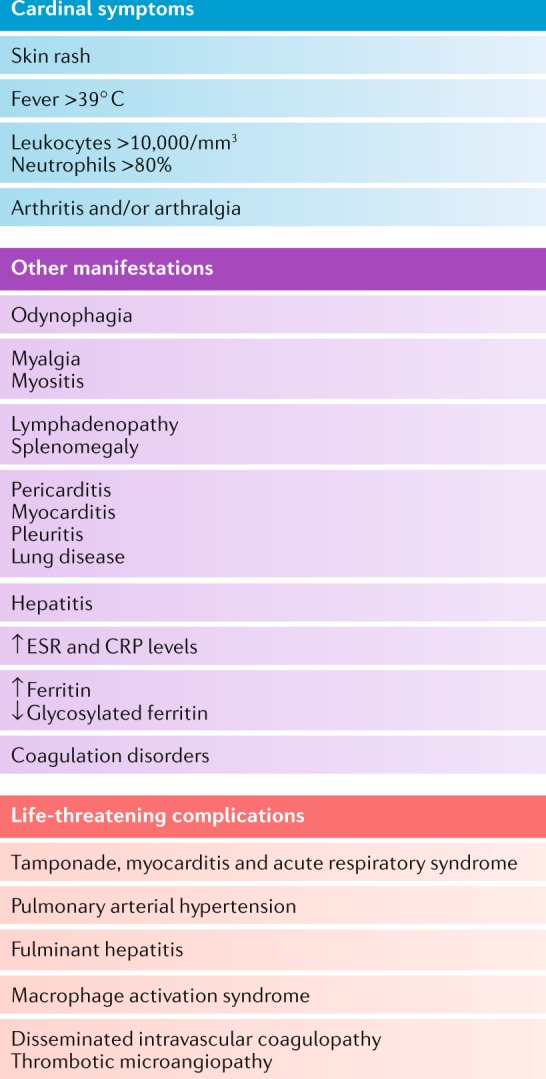
The schematic shows the major clinical symptoms for diagnosis of adult-onset Still’s disease (AoSD), as well as other manifestations and life-threatening complications. CRP; C-reactive protein; DIC, disseminated intravascular coagulation; ESR, erythrocyte sedimentation rate; GF, glycosylated ferritin; TMA, thrombotic microangiopathy.
Cardinal symptom 1: fever
Fever is constant when the disease is active, except in patients with established disease, in whom residual inflammation might remain without fever. Typically, fever starts suddenly, and temperature rapidly reaches 39 °C or more, with associated shivers4,13. The fever evolves with daily evening spikes for more than a week. Patients usually experience rapid deterioration of their general health as well as considerable weight loss. Importantly, fever may be the only clinical symptom of AoSD, and therefore, AoSD should be considered as a potential diagnosis in patients with fever of unknown origin44.
Cardinal symptom 2: arthralgia or arthritis
Joint pain or arthritis, with synovitis, is the second most common symptom and occurs in more than two-thirds of patients, usually with concomitant fever spikes4,13. All joints can be involved, including sacroiliac and distal interphalangeal joints. In some patients, the presentation is that of a bilateral symmetrical rheumatoid arthritis (RA)-like polyarthritis4,13. Synovial fluid analysis detects high cellularity (>2,000 cells/mm3), which confirms joint inflammation26. When performed, synovium biopsy can only be done to detect nonspecific synovitis. As disease progresses, arthritis can become erosive in one-third of patients; in these patients, isolated bilateral carpal ankylosis (that is, without structural damage of metacarpophalangeal or proximal interphalangeal joints, in contrast to RA) is highly suggestive of AoSD1,4,13 (Fig. 2).
Cardinal symptom 3: skin rashes
The skin rash in AoSD is typically coloured salmon pink and macular or maculopapular (Fig. 2). The rash is transient and is mainly visible during fever spikes on the proximal limbs or trunk and rarely involves the face, palms or soles of the feet4,13,45. No specific histological features have been described. Misdiagnosis with drug allergy is frequent and usually attributed to NSAIDs prescribed for joint symptoms or fever. Complete regression without scars is expected.
Urticaria and pruritis with dermographism have also been reported but are rather atypical4,13,45. Presence of purpuric lesions should lead to an urgent coagulation work-up because these lesions are suggestive of the AoSD haematological complications of haemophagocytic syndrome or reactive haemophagocytic lymphohistiocytosis (RHL), disseminated intravascular coagulation (DIC) or thrombotic microangiopathy (TMA), which is also called thrombotic thrombocytopenic purpura or Moschcowitz syndrome4,13.
Cardinal symptom 4: increased leukocyte and neutrophil counts
A major increase in leukocyte counts (>10,000/mm3) and neutrophil percentage (>80%) is detected4,13. Greatly increased leukocyte counts of >50,000/mm3 are typically associated with leukaemia. Leukopenia has also been described, in isolation or with anaemia and/or thrombocytopenia, and often indicates the presence of RHL or TMA4,13.
Other clinical symptoms
Odynophagia and sometimes pharyngitis are classical symptoms and are concomitant with fever (not present several days or weeks previously, as in post-streptococcal arthritis)3. All microbiological test results are negative. The presence of this symptom in such a systemic context seems to exclude lymphoma or another neoplastic disease46.
Diffuse and symmetrical lymphadenopathy is possible and can be associated with splenomegaly or even hepatomegaly. However, large and non-symmetrical lymphadenopathy should lead to the exclusion of malignant lymphoma by biopsy. Reactive polyclonal lymphoid hyperplasia is the usual pattern in AoSD4,13. Kikuchi necrotizing lymphadenitis has been described in a few patients47. Myalgia is frequent, but myositis or polymyositis are exceptional4,13,48,49. Finally, other systemic organ manifestations have been reported, including abdominal pain related to deep lymphadenitis, aseptic peritonitis or rarely acute pancreatitis, pleural effusion or pericarditis, or interstitial lung infiltrates4,13.
Other biological abnormalities
Aside from increased leukocyte and neutrophil counts, a substantial increase in acute-phase reactants (ESR, CRP, fibrinogen and serum immunoglobulins) is always present during AoSD flares4,13. Increased serum levels of liver enzymes are common, but fulminant hepatitis is rare and is related to systemic inflammation or the use of drugs such as antibiotics or NSAIDs as symptomatic treatment before diagnosis. Results of immunological work-ups to exclude other connective tissue diseases or inflammatory joint diseases must be negative.
AoSD biomarkers
Serum ferritin and glycosylated ferritin
High serum levels of ferritin, an indicator of macrophage activation, are common in AoSD37,38,50–53 (Table 1). Although hyperferritinaemia was first considered suggestive of AoSD, several studies have shown that hyperferritinaemia, whatever the threshold used, has a poor positive predictive value in isolation without a suggestive context54,55. Furthermore, some researchers have suggested that conditions such as AoSD, RHL, catastrophic anti-phospholipid syndrome and septic shock should be included under a common syndrome entity termed ‘hyperferritinaemic syndrome’ to underline the pro-inflammatory function of ferritin56. Indeed, ferritin has been hypothesized to have a pathogenic function: high serum levels of this protein, as detected in these four clinical conditions, might contribute to the development of a cytokine storm57,58. Indeed, in hepatic stellate cells, exogenous ferritin has been shown to activate the nuclear factor-κB (NF-κB) signalling pathway, leading to pro-inflammatory (including IL-1β) cytokine production58. High ferritin levels have also been shown to contribute to the development of a cytokine storm through a loop mechanism in which the inflammatory properties of ferritin are exacerbated14. The high levels of ferritin observed during inflammation result from increased production by histiocytes and macrophages and increased release from damaged hepatocytes. Many cytokines regulate the ferritin synthesis, including IL-1β, IL-18, TNF, IFNγ and IL-6. Interestingly, all these cytokines are involved in AoSD pathogenesis; levels of these cytokines in patients with AoSD positively correlate with disease activity, as do ferritin levels14. Hence, ferritin could be a mechanistic biomarker (that is, directly involved in the pathogenic mechanism) and not just a descriptive biomarker16.
Table 1.
Serum biomarkers in AoSD
| Biomarker | Diagnostic ability | Disease activity monitoring | Prognosis: severity (that is, predictive of life-threatening complications) | Prognosis: evolution (that is, predictive of evolution pattern) | Refs |
|---|---|---|---|---|---|
| Routine biomarkers | |||||
| CRP |
• High sensitivity • No specificity |
+ | _ | _ | 16 |
| Ferritin >ULN |
• High sensitivity • No specificity |
+ | + | +/− | 25, 38, 39, 54, 55, 156 |
| Ferritin ≥5 × ULN (≥1,000 μg/l) |
• Sensitivity 40.8% • Specificity 80.0% |
+ | + | High levels associated with systemic patterna | |
| GF ≤20% |
• Sensitivity 79.5% • Specificity 66.4% |
_ | + | NA | 59, 60 |
| Ferritin >ULN and GF ≤20% |
• Sensitivity 70.5% • Specificity 83.2% |
_ | _ | _ | 59, 60 |
| Ferritin >5 × ULN and GF ≤20% |
• Sensitivity 70.5% • Specificity 92.9% |
_ | _ | _ | 59, 60 |
| Calprotectin (S100A8–S100A9 proteins) | +/−b | + | NA | NA | 65, 66 |
| Procalcitonin | Weak (rule out sepsis) | NA | NA | NA | 64 |
| SAA | NA | NA |
+ (predictive of amyloid A amyloidosis) |
NA | 16 |
| Non-routine biomarkers | |||||
| IL-18 >150 ng/l |
• Sensitivity 88% • Specificity 78% |
+ |
+ (high levels are associated with RHLc, hepatitis and steroid dependence) |
+ (high levels potentially associated with systemic pattern) |
64, 156– 167 |
| IL-18 >366 ng/l |
• Sensitivity 91.7% • Specificity 99.1% |
||||
| IL-1βd | _e | + | +/− |
+/− (high levels potentially associated with systemic pattern) |
114, 158, 159 |
| IL-6d | _e | + |
+/− (high levels potentially associated with RHL) |
+/− (high levels potentially associated with arthritis pattern) |
158, 159 |
| TNFd | –e | – | – | – | 158, 159 |
| S100A12d | +/−f | + | NA | NA | 17, 19, 168 |
| AGEs and sRAGEsd | +/− | + | NA |
+ (higher AGE levels in serum with polycyclic or chronic articular patterns than monocyclic pattern) |
24 |
| CXCL10d | + | + | NA | NA | 70 |
| CXCL13d | + | + | NA | NA | 70 |
| sCD163d | +/− | NA | NA | NA | 68, 69 |
| MIFd | + | + | NA | NA | 169 |
| ICAM1d | +/− | + | NA | NA | 170 |
+, yes; –, no; +/–, tested but contradictory results. AGE, advanced glycation end product; AoSD, adult-onset Still’s disease; CRP, C-reactive protein; CXCL, CXC-chemokine ligand; GF, glycosylated ferritin; ICAM1, intracellular adhesion molecule 1; MIF, macrophage migration inhibitory factor; NA, not available; RHL, reactive haemophagocytic lymphohistiocytosis; SAA, serum amyloid A; sCD163, soluble CD163; sRAGE, soluble receptor for AGEs; ULN, upper limit of normal. aSerum ferritin levels are higher in the systemic subtype156, but high ferritin levels after adequate treatment might predict chronic articular course25. bCalprotectin levels help rule out rheumatoid arthritis, but further studies are needed to validate calprotectin as a diagnostic biomarker because of the lack of statistical difference between patients with AoSD and patients with sepsis, although the study populations were small16. cRegardless of whether the cause of RHL is AoSD-related, infectious, neoplastic or inflammatory. dReference range according to manufacturer. eHigh plasma levels of IL-1β, IL-6 and TNF have been detected in patients with AoSD, but the cytokine profile is not specific and cannot differentiate patients with AoSD from those with sepsis. fS100A12 is an efficient diagnostic and monitoring biomarker in systemic juvenile arthritis, but further studies are needed for validation in AoSD.
Aside from total ferritin levels, the diagnostic performance of measuring the glycosylated ferritin (GF) level has been investigated59. The GF level normally is more than half of the total ferritin level. In inflammatory conditions, the concentration of GF decreases and usually ranges from 20−50%; this finding is explained by the fact that glycosylation mechanisms cannot follow the increase in ferritin production54,59. However, in AoSD, the GF level is markedly decreased (<20%), which suggests the involvement of other mechanisms. Extensive data indicate 78% sensitivity and 64% specificity of a GF level ≤20% for AoSD diagnosis54. The combination of hyperferritinaemia and a GF level ≤20% yields 67% sensitivity and 84% specificity54. Of note, although serum ferritin levels fluctuate according to systemic inflammation, GF levels remain low for several weeks to months after disease remission60. However, as mentioned, low GF level is not completely specific to AoSD and also occurs in other inflammatory processes such as severe systemic infections48. Moreover, the GF level is usually low (≤20%) in haemophagocytic syndromes regardless of the cause (infection, neoplasm or inflammation)61–63.
Other potential biomarkers for routine settings
Procalcitonin, a marker of severe systemic infection, can be increased in patients with active AoSD and thus cannot be used to distinguish acute infection from an AoSD flare16,64. Serum level of calprotectin (which is a heterodimer of the S100A8 and S100A9 proteins) could be an additional disease activity biomarker because alarmins seem to have an important function in AoSD pathogenesis. However, this protein is not specific to AoSD and might be increased in many other inflammatory conditions16,18,65,66. Finally, an increase in the serum amyloid A (SAA) level, as an inflammatory biomarker, is predictive of the development of amyloidosis16.
Other potential biomarkers for research
Several other biomarkers (such as serum cytokine levels) have been proposed but have not been implemented in routine practice owing to technical or economic reasons. High serum levels of IL-1, IL-6 and IL-18 are detected in systemic forms of AoSD and might be used as activity biomarkers8,14,16. However, the additional value on top of CRP level and other inflammatory biomarkers is unclear, and these cytokines are clearly not specific to AoSD. Thus, these cytokines are not recommended biomarkers for routine investigation. Of importance, IL-18 seems to have an important function in RHL.
The serum concentration of AGEs and sRAGEs, which are involved in AoSD pathogenesis, might also be increased in other inflammatory disorders. In comparison with patients with AoSD and a monocyclic pattern, substantially higher AGE serum levels are detected in patients with AoSD and polycyclic or chronic articular patterns16,24. Serum level of soluble CD163, a macrophage activation biomarker, is elevated in AoSD but is not specific to the disease14–16,67–69. Finally, several chemokines, including CXC-chemokine ligand 10 (CXCL10), CXCL13 and macrophage migration inhibitory factor (MIF)), have potential as new diagnostic biomarkers for AoSD16. CXCL10 is produced in response to IFNγ. CXCL13 is constitutively expressed in secondary lymphoid tissues, and the expression is induced by TNF via T cell stimulation. Levels of both CXCL10 and CXCL13 have been shown to be higher in patients with AoSD than in patients with RA or healthy volunteers, and these levels correlate with disease activity, ferritin and systemic scores70. However, these findings need to be confirmed with larger patient groups.
Differential diagnoses
The list of differential diagnoses is long owing to the systemic nature of the disease and the diversity of symptoms (Table 2). After comprehensive investigations, no clinical sign or biological abnormality is specific enough to AoSD to ascertain diagnosis. Thus, the classification criteria may be helpful, but these criteria were developed more for clinical research than for diagnosis. Two sets of criteria have been validated. The Yamaguchi criteria, published in 1992, are the most widely used71 (Table 3); however, these criteria include exclusion criteria such as infections, malignancies and other rheumatic diseases. Thus, they should be used only after a broad diagnostic work-up, which is problematic in clinical practice. The Fautrel criteria have the advantage of including ferritin and GF levels as diagnostic biomarkers and do not require exclusion criteria40 (Table 3). In a 2018 validation study, both sets showed high sensitivity and specificity41.
Table 2.
Differential diagnosis of AoSD
| Diseases | Relevant work-ups | ||
|---|---|---|---|
| Infectious diseases | Bacteria | Pyogenic bacterial septicaemia, infectious endocarditis, biliary, colic or urinary occult infections, tuberculosis, brucellosis and yersiniosis | Blood cultures, procalcitonin, echocardiogram, CT scan, IGRAs, biopsy for bacteriology and histology, serology and PCR |
| Viruses | HIV infection, viral hepatitis, parvovirus B19 infection, herpesvirus infections, measles and rubella | Serology and PCR | |
| Parasites | Toxoplasmosis and abscessed parasitosis | Serology and PCR | |
| Malignant diseases | Haematological disease | Hodgkin disease or non-Hodgkin lymphoma, angioimmunoblastic lymphadenopathy, Castelman disease and myeloproliferative disorders | Biopsy of a large and asymmetrical lymphadenopathy, bone marrow smear or biopsy, CT scan and PET–CT scan |
| Solid cancers | Kidney, colon or lung cancer and paraneoplastic syndromes | CT scan and PET–CT scan | |
| Systemic diseases | Autoimmune diseases | Systemic lupus erythematosus, polymyositis, dermatomyositis, RA, polyarteritis nodosa or other vasculitis | Antinuclear autoantibodies, creatine phosphokinase, specific autoantibody, biopsy, RF, ACPA, joint ultrasonography, ANCAs and arteriography |
| Autoinflammatory disorders |
• Hereditary autoinflammatory syndromes: familial Mediterranean fever, mevalonate kinase deficiency, TNF receptor-associated periodic syndrome and cryopyrin-associated periodic syndromes • Neutrophilic dermatosis and Sweet syndrome |
• Familial history plus MEFV gene sequencing, urinary mevalonic acid, MVK sequencing, TNFRSF1A sequencing and NLRP3 sequencing • Skin biopsy |
|
| Other | Post-streptococcal arthritis, reactive arthritis, sarcoidosis, Schnitzler syndrome, Kikuchi-Fujimoto disease and drug-related hypersensitivity | ASLO, erythema nodosum, monoclonal gammopathy, biopsy of a large and asymmetrical lymphadenopathy, eosinophilia and drug investigation | |
ACPA, anti-citrullinated protein antibodies; ANCAs, anti-neutrophil cytoplasmic antibodies; AoSD, adult-onset Still’s disease; ASLO, anti-streptolysin O antibody; IGRA, IFNγ release assay; RA, rheumatoid arthritis; RF, rheumatoid factor.
Table 3.
Classification criteria for AoSD
| Criteria | Yamaguchi et al.71 | Fautrel et al.40 |
|---|---|---|
| Major criteria |
• Fever ≥39 °C lasting 1 week or more • Arthralgia lasting 2 weeks or more • Typical skin rash: maculopapular, nonpruritic, salmon-pink rash with concomitant fever spikes • Leukocytosis ≥10,000/mm3 with neutrophil polymorphonuclear proportion ≥80% |
• Spiking fever ≥39 °C • Arthralgia • Transient erythema • Pharyngitis • Neutrophil polymorphonuclear proportion ≥80% • GF proportion ≤20% |
| Minor criteria |
• Pharyngitis or sore throat • Lymphadenopathy and/or splenomegaly • Liver enzyme abnormalities (aminotransferases) • Negative for RF or antinuclear antibodies |
• Typical rash • Leukocytosis ≥10,000/mm3 |
| Exclusion criteria |
• Absence of infection, especially sepsis and Epstein–Barr viral infection • Absence of malignant diseases, especially lymphomas • Absence of inflammatory disease, especially polyarteritis nodosa |
None |
| Criteria requirement | At least five criteria, including two major criteria and no exclusion criteria | Four major criteria or three major criteria and two minor criteria |
| Classification criteria performance |
• Sensitivity 96.3%, specificity 98.2%, PPV 94.6% and NPV 99.3% • Modified Yamaguchi criteria, i.e., Yamaguchi criteria and ferritin >ULN: sensitivity 100%, specificity 97.1%, PPV 87.1% and NPV 100% • Alternative modified Yamaguchi criteria, i.e., Yamaguchi criteria and GF ≤20%: sensitivity 98.2%, specificity 98.6%, PPV 93.0% and NPV 99.6%41 |
Sensitivity 87.0%, Specificity 97.8%, PPV 88.7% and NPV 97.5%41 |
AoSD, adult-onset Still’s disease; GF, glycosylated ferritin; NPV, negative predictive value; PPV, positive predictive value; RF, rheumatoid factor; ULN, upper limit of normal.
Course of disease and prognosis
The course of AoSD can be diverse and is currently impossible to predict. Several patterns have been described; however, these patterns are mainly based on case series and not on robust epidemiological studies35,39,72–74. A monocyclic course is either self-limited or includes drug-free remission that is reached over time. The initial flare with systemic manifestations and (potentially) joint involvement develops over a few weeks. Remission can be achieved with NSAIDs, steroids or other immunomodulatory agents after a few days or weeks. These treatments can be progressively tapered then stopped without relapse after a few months. This pattern seems to account for 19–44% of affected patients72,74.
A recurrent or polycyclic course is characterized by AoSD relapses after a few months or years under immunomodulatory treatment or after its discontinuation. In this pattern, one classical presentation is a first flare during SoJIA diagnosed in childhood, followed by sustained drug-free remission for several years and then a relapse in adulthood. In most of these cases, recurrences combine systemic and joint involvement. This pattern represents 10–41% of affected patients72,74.
A chronic and progressive course involves continuous inflammation that is responsible for chronic and frequently erosive joint involvement with regular systemic flares. This pattern is the most frequent, estimated at 35–67% of affected patients, in old series from the pre-biologic era1,72,75. Although no new estimates are available, this pattern should be less likely now that targeted therapies are available.
Targeted therapies for AoSD
In the pre-biologic era, treatment options for AoSD were limited to non-selective anti-inflammatory approaches using NSAIDs, glucocorticoids or conventional synthetic DMARDs. Despite the well-known unfavourable safety profile of NSAIDs and glucocorticoids (such as hypertension and arteriosclerosis), efficacy of these therapeutics was not satisfactory, especially in severe manifestations. In fact, for at least 30–40% of patients, disease cannot be controlled by these traditional approaches, indicating a substantial medical requirement for a targeted therapy76,77. Successful developments in the treatment of other chronic rheumatic diseases triggered the use of different biologic agents in refractory AoSD. Evidence indicates that cytokine inhibitors targeting IL-1, IL-6, TNF and potentially IL-18 could interfere with the inflammatory response in AoSD77.
TNF inhibition
Stimulated by encouraging results from the treatment of other chronic inflammatory joint diseases (especially RA), TNF inhibitors were the first biologic agents used for AoSD78–83. However, driven by the deceptive impression that AoSD with a predominant arthritic phenotype is a subgroup of seronegative RA, the results from uncontrolled trials — usually involving small cohorts of patients — were inconsistent (Table 4). As favourable outcomes occur in only a few patients, without any specific characteristics, TNF inhibitors can be considered as only third-line drugs, preferentially for patients with chronic arthritis.
Table 4.
AoSD treatments
| Targeted therapy | International nonproprietary name and usual dose | Reported number of patients | Preferential AoSD pattern | Follow-up duration (months) | Complete remission (%) | Steroid dose reduction | Refs |
|---|---|---|---|---|---|---|---|
| IL-1 receptor antagonists | Anakinra (100 mg, sometimes 200 mg, daily subcutaneously) | >250 | Systemic and articular | >12 | 80 | Yes | 20, 85– 91, 94 |
| Anti-IL-1ß | Canakinumab (4 mg/kg up to max. 300 mg per month subcutaneously) | 10 | Systemic and articular | >12 | 100 | Yes | 98– 108 |
| IL-1 trap | Rilonacept (loading dose 100–320 mg and then 100–320 mg per week) | 11 | Systemic and articular | >12 | 100 | Yes | 84, 96 |
| TNF blockers |
• Infliximab (3.0–7.5 mg/kg weeks 0, 2 and 6 and then every 6–8 weeks intravenously) • Etanercept (50 mg per week subcutaneously) |
<100 | Articular | >12 | 0–100 | NA | 78– 83 |
| IL-6 receptor antagonists | Tocilizumab (8 mg/kg per month intravenously or 162 mg per week subcutaneously) | <150 | Systemic and articular | >12 | 60–85 | Yes | 104– 107, 109– 112 |
| Anti-IL-18 | Tadekinig alpha (80 mg per week subcutaneously or 160 mg per week subcutaneously) | <25 | NA | 4 | NA | NA | 113 |
| B cell-directed | Rituximab (1 g intravenous at day 1 and day 15, next cycle after 6 months) | 1 | NA | 12 | NA | NA | 171 |
| T cell-directed | Abatacept (500–1,000 mg per month intravenouslya or 125 mg per week subcutaneously) | 2 | NA | >12 | NA | NA | 172, 173 |
AoSD, adult-onset Still’s disease; NA, not available. aAbatacept dose depends on patient weight: <60 kg = 500 mg, 60–100 kg = 750 mg and ≥100 kg = 1,000 mg.
IL-1 inhibition
The successful use of IL-1 inhibitors for AoSD has contributed to the revival of this option in the treatment of rheumatic diseases and is now the primary choice for treating autoinflammatory diseases in general. However, clinical development took a surprisingly long time to move from cohort studies to randomized placebo-controlled trials. Currently, two inhibitors of IL-1 signalling (anakinra and canakinumab) are in phase II and phase III trials.
Anakinra, a recombinant IL-1 receptor antagonist, was the first biologic agent to show beneficial effects in treating the systemic and articular features of AoSD in many case series, uncontrolled trials and different national surveys84. Although the evidence for efficacy of anakinra is unproven in classical, double-blinded controlled trials, the overall number of (>250) published cases provides convincing results. In fact, a clear and sustained improvement has been described for systemic and arthritic symptoms in most treated patients85–90. Systemic features seem to show a more rapid response, whereas prolonged exposure of several weeks usually seems to be required for improvement of arthritis. Of major importance for long-term safety were consistent reports of a reduction or even discontinuation of glucocorticoids as well as NSAIDs. In this context, meta-analyses from eight case series and three national surveys (meeting predefined quality standards and including >100 patients with AoSD treated with anakinra) showed a remission rate of ~80% and a reduced use of steroids in ~35% of patients91. A large observational retrospective multicentre study from Italy added further evidence for a strong effect on disease activity using the Pouchot score as well as clinical and serological features, regardless of sex, age, disease pattern or co-medication as outcome measures20. In February 2018, the Committee for Medicinal Products for Human Use (CHMP) recommended a change to the terms of the marketing authorization for anakinra; notably, the indication is now broad, including both AoSD and SoJIA, with active systemic features of moderate to high disease activity, or patients with continued disease activity after treatment with NSAIDs or glucocorticoids92.
Since September 2017, a randomized, double-blind, placebo-controlled, multicentre, phase III study in the USA has recruited patients to evaluate the safety and efficacy of two different doses of anakinra (2 mg/kg daily, max 100 mg daily; or 4 mg/kg daily, max 200 mg daily) in patients newly diagnosed with SoJIA or AoSD. The primary end point (ACR30 response) has already been evaluated at week 2. Notably, the overall treatment period is short, with only 12 weeks of exposure followed by a 4-week safety follow-up93.
Of note, anakinra is the only IL-1 signalling inhibitor for which substantial long-term results exist in terms of efficacy and safety in AoSD94. In contrast to monogenetic autoinflammatory diseases, in AoSD, remission can continue in some cases even after treatment is stopped. However, a somewhat high withdrawal rate of 40% has been reported85 owing to loss of response over time and also to frequent injection site reactions to the required daily administrations.
Limited data are available for rilonacept, an IL-1 trap molecule, in terms of efficacy and safety in AoSD. Although different dosing regimens have been used, a published small case series of 11 patients confirmed an improvement in signs and symptoms under this approach95–97. Of note, one patient with AoSD that was refractory to anakinra responded to rilonacept. However, rilonacept is still not approved for therapeutic use in Europe.
The first approved biologic agent for AoSD is canakinumab, a fully human antibody against IL-1β. Canakinumab is also approved for treating other autoinflammatory diseases, including cryopyrin-associated periodic syndromes, familial Mediterranean fever, TNF receptor-associated periodic syndrome and hyper immunoglobulin D (IgD) syndrome, as well as SoJIA. Although the overall application of canakinumab for AoSD is still limited, the reported response of systemic features and arthritis is rapid and sustained over many months to years in most patients, frequently allowing for tapering of steroids98–100. Of note, canakinumab is highly effective for patients with difficult to treat AoSD, including those for whom treatment with NSAIDs, glucocorticoids and other IL-1 inhibitors has failed.
On the back of these promising results, a placebo-controlled, randomized, multicentre, phase II study of canakinumab in AoSD was performed101. The dosage of canakinumab in this study, with monthly injections of up to 4 mg/kg body weight, is according to the pharmacokinetic profile in adolescent patients with SoJIA. The primary aim is to investigate the efficacy of canakinumab in patients with AoSD and active joint involvement in terms of the proportion of patients with a clinically significant reduction in disease activity (disease activity score in 28 joints (DAS28) >1.2) following a treatment period of 12 weeks. The overall placebo-controlled period is 24 weeks, but non-responders can be unblinded and provided with treatment rescue at week 12. The core study is followed by an optional long-term extension over 2 years to provide additional safety results in the adult population.
Relevant safety considerations for all IL-1 antagonists include infections and the risk of macrophage activation syndrome. Whether macrophage activation syndrome should be considered a characteristic systemic manifestation of SoJIA and AoSD, or whether in some instances it is at least an adverse paradoxical effect of IL-1 inhibition, is unknown102. In summary, the published data for anti-IL-1 therapeutics in refractory AoSD clearly show a consistently high rate of full or partial remission with the additional achievement of lowering or stopping glucocorticoid medication84. Although published results from controlled clinical trials are still lacking, post hoc analysis from adolescent patients with SoJIA and biomarker analysis have already led to conditional approval of canakinumab for AoSD in Europe103. Furthermore, anakinra was approved for the treatment of Still’s disease (AoSD and SoJIA) by the European Medicines Agency in 2018 (ref.92).
IL-6 inhibition
Inhibition of IL-6 signalling is possible by two different approaches: direct neutralization of the cytokine or blockade of the respective receptor. Neither of these mechanisms has been investigated in AoSD in a controlled clinical trial. For the two different IL-6 receptor antagonists (tocilizumab and sarilumab) currently available in daily practice for treating rheumatic diseases, only case series for tocilizumab in AoSD have been published and reported at conferences104–108. To summarize, the observed anti-inflammatory effects were strong, rapid and sustained for most of these patients. Usually, the systemic features disappeared entirely, but arthritic manifestations also improved, and serologic activity decreased109,110. Also for tocilizumab, it was reported that joint manifestations seem to be more refractory to treatment than systemic manifestations108. However, because of limited data, the likelihood of response cannot be estimated as clearly as for IL-1 signalling inhibitors and seems to be 60–80% for full remission13. A meta-analysis of 10 original studies (147 individuals) on the efficacy of tocilizumab and AoSD showed overall high partial and complete remission rates of 85% and 77%, respectively. Tocilizumab prevented new flares, was well tolerated and could substantially reduce the need for corticosteroids111,112.
Whether other IL-6 inhibitors have similar effects is unknown; as shown for RA treatment, with AoSD, differences could exist with respect to safety, especially in comparison with the direct cytokine inhibitors. The advantages or disadvantages that distinguish IL-6 and IL-1 inhibition are unclear. Although IL-6 and IL-1 inhibitors have high response rates and are alternative approaches to treating AoSD, we have no way to predict the individual effects and define the ideal treatment algorithm.
IL-18 inhibition
Tadekinig alfa is a recombinant human IL-18-binding protein113. This drug was tested in healthy volunteers and patients with psoriasis or RA in phase I studies and demonstrated a good safety and tolerability profile with only mild adverse events at the injection site113. Because of the postulated role of IL-18 in the pathogenesis of AoSD, it was a logical step to investigate the effects of tadekinig alfa in this condition. A first open-label, dose-finding phase II study involving multiple centres in Europe was designed to capture safety information as the primary outcome113. Two doses (80 and 160 mg) were administered over 12 weeks, and patients were followed up for 4 more weeks. As a secondary outcome measurement, the efficacious dose at 3 weeks was defined as one leading to normalization of body temperature and a decrease of CRP level by 50% or more of baseline values.
Although limited by a low patient number (n = 23) and short observation period in the study, the safety profile of tadekinig alfa was acceptable overall, with injection site reactions and infections being the most frequent adverse events. In terms of efficacy, a reduced level of CRP as well as other inflammatory markers (including IL-18 and ferritin) was detected in some patients. Furthermore, an improvement in skin rash and a slight but statistically significant reduction in prednisolone doses was reported (median prednisone dosage was decreased from 12.5 mg/day at baseline to 10 mg/day at 12 weeks; P = 0.01)113. In summary, inhibition of IL-18 by tadekinig alfa could be a promising new approach to treat AoSD that needs to be investigated in a more controlled setting.
Treatment strategies and future trials
The treatment strategy for patients with AoSD is summarized in Fig. 3. No biomarker enables a reliable prediction of the response and outcome after any treatment at the individual level. Thus, it is not possible to make the choice of a specific targeted therapy on the unique basis of clinical, biological or imaging characteristics of the disease. In individual cases, articular manifestations can have a better response to IL-6 receptor blockers, whereas systemic features might improve with IL-1 blockers more than with IL-6 blockers. Such statements must be handled with care, however, as patients with arthritis-predominant AoSD usually respond well to IL-1 blockers and patients with systemic-predominant AoSD are also likely to respond to IL-6 receptor blockers.
Fig. 3. Managing patients with AoSD.

The schematic shows a therapeutic strategy to manage patients with adult-onset Still’s disease (AoSD), providing instruction on how to proceed in case of failing any given therapy. CR, complete response; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; F, failure; MDR, multidisciplinary round; PR, partial response.
Tapering and discontinuation of treatment is a frequent scenario in AoSD as well as SoJIA, which is justified by the high frequency of a monocyclic appearance and the likelihood of long-term remission. Of course, remission of disease should be a prerequisite for treatment — which is usually described as absence of systemic as well as organ-specific symptoms and normalization of biomarkers. However, no consensus exists, and no standardized protocol describes how and when tapering and discontinuation are appropriate.
Limited experience with controlled clinical trials in this indication and the lack of evaluated outcome measurements hamper the development of new compounds for treating AoSD. One way to overcome these issues would be to extrapolate from established approaches in SoJIA. However, whether the same trial designs and scores are applicable to the adult cohort is an unresolved issue. Furthermore, the different manifestations, with predominant systemic or articular features, must be considered.
From medical and ethical points of view, a classical placebo-controlled design is not feasible for severe systemic forms of AoSD. A flare design might be preferable, as used for other autoinflammatory diseases, by stopping the investigational drug after achieving low disease activity or remission. This study design could compare a standard treatment, for example, high-dose glucocorticoids, with the investigational product. However, such a scenario would require a high probability of response to the investigational product and could be feasible with IL-1 or IL-6 inhibitors, for example. It would be much more problematic and even unethical to use a comparator with limited experience, keeping in mind the risk of aggravating the systemic inflammatory response and initiating macrophage activation syndrome. Strict and comprehensive withdrawal criteria must be predefined.
For patients with predominantly articular involvement and low systemic activity, a period of placebo-controlled treatment could be acceptable. The design of clinical trials similar to those established in RA could include rescue scenarios in case of non-response. However, defining the optimal trial duration and time points for outcome measurements remains difficult.
In terms of outcome measurements, evaluated scores for systemic or articular disease manifestation are not available in AoSD. In addition, whether these features should be captured in a single or in separated scores needs discussion. Although the Anti-Inflammatory Disease Activity Index was developed and is used for different autoinflammatory diseases, it is not ideal for AoSD when considering the specific clinical symptoms of this disease. By contrast, the Pouchot score (with a range of 0–12, which considers 12 disease-related manifestations: fever, evanescent rash, pleuritis, pneumonia, pericarditis, hepatomegaly, serum ferritin levels >3,000 mg/l, lymphadenopathy, white blood cell count >15,000/mm3, sore throat, myalgia and arthritis) could be a good starting point to develop a specific tool for assessing disease activity in AoSD114. However, this score does not provide weighting for the different organ manifestations and has not been an accepted tool in controlled settings. At least for the articular signs and symptoms, established disease activity scores in RA such as DAS28 or ACR20, ACR50 and ACR70 responses could be useful. However, a separate evaluation should also be performed in AoSD cohorts.
In summary, international efforts are needed to establish and evaluate reliable and acceptable outcome measurements in AoSD. With already existing networks and growing cohorts of patients with AoSD, it should be possible to establish working groups in the near future.
Life-threatening complications
Several severe manifestations have been described in AoSD, which explains the potentially unfavourable prognosis of the disease4,115. Table 5 lists these complications, and the most frequent and relevant complications are discussed in more detail here.
Table 5.
Main life-threatening complications of AoSD
| Complications | Signs and symptoms | Diagnostic procedures | Treatment | Refs |
|---|---|---|---|---|
| RHL |
• High (>38.5 °C), persistent fevera • Peripheral lymphadenopathy, hepatomegaly and splenomegaly • Polymorphous skin rashesb: rashes, oedema, petechiae, urticaria or purpura • Multiple organ involvement: pulmonary, neurological, gastrointestinal or renal involvement and bleeding • Rapid change on haemography: resolution of high leukocyte and neutrophil counts and occurrence of anaemia and thrombocytopenia |
• Cytopeniac: anaemia, thrombocytopenia and/or leukopenia • Decreased ESRd • Increased liver function test results: transaminases and alkaline phosphatases • High LDH level • Hypertriglyceridaemia • Hyperferritinaemiae • High soluble CD25 or CD163 level • Haemophagocytosis in bone marrow smear (or reticuloendothelial organs) • Increased CD163 staining in bone marrow • H-scoref |
• Supportive care in ICU • Exclusion of an additional trigger: mainly infectionsg • Immunomodulatory agents: high-dose corticosteroids ± IL-1 or IL-6 inhibitors after a few days; if refractory, etoposide or ciclosporin A |
4, 62, 115 |
| DIC |
• Haematoma and bleeding • Thrombotic event • Multi-organ involvement or failure: ARDS, pleural effusion, myocarditis, pulmonary embolism, gastrointestinal bleeding and CNS involvement |
• Thrombocytopenia • Prolongation of prothrombin time and activated thromboplastin time • Decreased fibrinogen levels • Increased levels of fibrin degradation products |
• Supportive measures in ICU • Immunomodulatory agents: high-dose corticosteroids ± IL-1 or IL-6 inhibitors; if refractory, cyclosporin A |
28, 86, 91, 115, 118– 129 |
| TMA or Moschcowitz syndrome |
• Acute vision impairment (early sign) • Weakness • Confusion, seizures or coma • Abdominal pain, nausea, vomiting and diarrhoea • Cutaneous gangrene • Arrhythmias caused by myocardial damage • Multi-organ failure |
• Mechanical haemolytic anaemia (schistocytes on the peripheral blood smear with a negative Coombs test) • Thrombocytopenia • Multiple organ failure of varying severity (mainly the kidneys and the CNS) |
• Supportive measures in ICU • Specific treatment: high-dose corticosteroids and plasma exchange ± haemodialysis; if insufficient, multidisciplinary round ± IL-1 or IL-6 inhibitors or ciclosporin or intravenous immunoglobulin |
119, 130, 131, 135 |
| Fulminant hepatitis |
• Physical status deterioration: appetite loss and fatigue • Jaundice • Hepatomegaly • Right abdominal pain • Rarely, bleeding |
• Abnormal and rapidly increasing liver function test findings • High activity on multi-biomarker FibroTest • Liver biopsy (if performed): nonspecific portal infiltrates of lymphocytes, plasma cells and neutrophils, hepatocytic lesions or massive necrosis |
• Supportive measures in ICU • Discontinuation of all potentially hepatotoxic drugsh: mainly acetaminophen, aspirin, NSAIDs or methotrexate • Rule out RHL, DIC and/or TMA • Rule out viral reactivation • Specific treatment: high-dose corticosteroids ± IL-1 or IL-6 inhibitorsi or ciclosporin • Liver transplantation in extreme cases |
16, 119 |
| Cardiac complications |
• Pericarditis, sometimes recurrent • Tamponade • Myocarditis • Endocarditis (exceptional cases) |
• Electrocardiography • Echocardiography • Troponin and creatinine kinase levels increase if myocarditis |
• Supportive measures in ICU • Specific treatment: usually high-dose corticosteroids ± IL-1 or IL-6 inhibitors |
16, 119 |
| PAH |
• Dyspnoea (key symptom) • Fatigue and dizziness • Syncope • ARDS |
• Electrocardiography: right atrium hypertrophy • Echocardiography: systolic PAP >35 mmHg • Right heart catheterization (gold standard): mean PAP ≥25 mmHg at rest; end-expiratory PAWP ≤15 mmHg; pulmonary vascular resistance >3 Wood units |
• Close monitoring and referral to a pulmonary hypertension reference centre (multidisciplinary rounds) • Vasodilatation therapy: calcium channel blockers, endothelin receptor antagonists, phosphodiesterase 5 inhibitors and/or prostacyclin analogues • Immunosuppressive therapy: high-dose steroids ± IL-1 or IL-6 inhibitors or ciclosporin |
136– 147 |
| Pulmonary complications |
• Pleuritis • Interstitial lung disease with or without ARDS • Aseptic empyema • Diffuse alveolar haemorrhage |
• High-resolution CT • BAL (for differential diagnosis: in AoSD, nonspecific neutrophilic profile) • Pulmonary function tests |
• Supportive measures in ICU if ARDS • Rule out differential diagnoses: infections, cardiogenic causes (brain natriuretic peptide dosage, echocardiography), drug-related or iatrogenic causes and cancer • Specific treatment: usually high-dose corticosteroids ± IL-1 or IL-6 inhibitors |
16, 119 |
| Amyloid A amyloidosis |
• Exceptional these days • Renal failure, proteinuria, oedema and hydrops • Digestive involvement • Orthostatic hypotension and other neuropathies |
Biopsy of minor salivary gland, or abdominal fat pad, or kidney | Inflammation control with IL-1 or IL-6 inhibitors | 151– 155 |
AoSD, adult-onset Still’s disease; ARDS, acute respiratory distress syndrome; BAL, bronchoalveolar lavage; CNS, central nervous system; DIC, disseminated intravascular coagulation; ESR, erythrocyte sedimentation rate; ICU, intensive care unit; LDH, lactate dehydrogenase; PAH, pulmonary arterial hypertension; PAP, pulmonary arterial pressure; PAWP, pulmonary artery wedge pressure; RHL, reactive haemophagocytic lymphohistiocytosis; TMA, thrombotic microangiopathy. aIn AoSD fever is often remitting, with spikes. bIn AoSD, skin rash is classically maculopapular and evanescent. cIn non-complicated AoSD, white blood count is often ≥10,000/mm3, mainly neutrophils, and thrombocytosis is frequent. dIn non-complicated AoSD, ESR is high. eHyperferritinaemia is also seen in AoSD, but in case of very high ferritin levels or sudden increase, RHL or another systemic complication should be suspected. fThis scoring system is a set of nine weighted criteria (known underlying immunosuppression, temperature, organomegaly, number of cytopenia, ferritin, triglyceride, fibrinogen, serum glutamic oxaloacetic transaminase, hemophagocytosis features on bone marrow aspirate) that have been validated for the diagnosis of RHL in adults174. It is freely available online. gIn particular viral reactivation (Epstein-Barr virus, cytomegalovirus), which may trigger AoSD or be reactivated by immunosuppressive treatments. hDrug reaction with eosinophilia and systemic symptoms (DRESS) syndrome, potentially induced by IL-1 or IL-6 or another immunosuppressive agent, is a differential diagnosis that should always be ruled out because it can be responsible for a fulminant hepatitis and mimic AoSD systemic manifestations. iKeeping in mind that tocilizumab-induced hepatic injury has also been reported175.
RHL
RHL is a common complication of AoSD that can occur at the time of diagnosis, straight after treatment introduction or during the course of the disease. This serious complication should be suspected in a patient with persisting fever (in contrast to fever spiking in the evening) and a decrease in initially increased leukocyte and neutrophil counts4,62,115. The key issue with RHL is to identify whether its occurrence is related to AoSD intense inflammation or to concomitant infection (which could potentially occur owing to the use of immunomodulators introduced because of AoSD). The list of possible infections is long, with viral reactivation being the most common.
The development of RHL (which is also called macrophage activation syndrome) is associated with a cytokine storm, with the involvement of many pro-inflammatory cytokines. Management should include the following: first, treatment of symptoms in a medicine department or intensive care unit (ICU); second, active and rapid search for an infection; and third, introduction of high-dose steroids. Given that RHL has been described in patients undergoing IL-1 therapy84, it seems prudent to introduce this treatment only after control of RHL by steroids. However, owing to the life-threatening situation, cytokine-targeted approaches (anti-IL1 and anti-IL-6) should be considered early. Notably, the level of evidence is particularly low for intravenous immunoglobulins with controversial results, and most clinicians no longer recommend them for this indication116,117.
Coagulation disorders
Two serious coagulation disorders might complicate AoSD, mainly at the acute phase of the disease. The first disorder, DIC, occurs at a frequency of 1−5%28,115,118–125. This diagnosis should be suspected in a patient with a combination of thrombotic events and cutaneous or mucosal bleeding and perhaps specific organ involvement such as fulminant hepatitis, cardiac or respiratory failure or stroke. Haemostasis work-ups reveal platelet and coagulation factor consumption, increased thromboplastin time and high D-dimer levels. DIC is a medical emergency requiring the following care: supportive measures, which could include platelet transfusion, coagulation factors (or fresh frozen plasma) and fibrinogen (in cryoprecipitate) infusion to control severe bleeding or sometimes heparin if no active bleeding is present126; and specific anti-inflammatory agents (often decided in multidisciplinary rounds), including mainly high-dose corticosteroids, either intravenous (methylprednisolone 15 mg/kg daily) or oral (prednisone 1 mg/kg daily)115. To limit steroid exposure, the addition of other immunomodulatory agents such as IL-1 or IL-6 blockers or ciclosporin is recommended84,90,127–129.
The other rare, but quite severe, coagulation disorder is TMA. This disorder should be suspected in a patient with unexplained multi-organ failure or stroke. Organ damage in TMA is caused by multiple small thrombi leading to tissue ischaemia and mechanical haemolytic anemia119,130,131. Acute vision impairment, such as blurred vision related to Purtscher-like retinopathy, is often the first symptom130. Haemography is the key diagnostic test, displaying thrombocytopenia by platelet consumption, anaemia and schistocytes (fragmented red blood cells), which are specific to this diagnosis. Organ imaging may reveal multiple infarctions. In addition, a disintegrin and metalloproteinase with thrombospondin motifs 13 (ADAMTS13) enzymatic activity needs to be tested because acquired deficiency has been found to predispose to TMA115,132–134. TMA has been mainly described during AoSD flares related to intense inflammation or to concomitant infection with Shiga toxin-producing microorganisms130.
TMA treatment is complex and mandatorily includes the following119: supportive care in an ICU with plasma exchange being central133 and high-dose steroids intravenously and then orally. Other immunomodulatory agents proposed for refractory TMA cases include anakinra130, tocilizumab135, intravenous immunoglobulins, cyclophosphamide, azathioprine, ciclosporin A and rituximab119,130. Despite this treatment, mortality associated with TMA remains high (up to 20%)119.
Cardiac and pulmonary involvements
Although pleural effusion or pericarditis is frequent in AoSD, other serious cardiac or pulmonary manifestations have been described (Table 2). Their treatment combines supportive care, high-dose steroids and often IL-1 or IL-6 inhibitors.
Specific attention should be dedicated to the rare and very severe AoSD manifestation of pulmonary arterial hypertension (PAH), with several cases reported in the past 10 years136–147. PAH, either idiopathic or occurring with AoSD or other connective tissue diseases, is thought to be related at least in part to immune-related alteration of the endothelium with overproduction of IL-1, IL-6, IL-18 and TNF138,139,142,143,148. PAH may occur at AoSD onset or later and seems to mainly affect women140. The diagnosis should be suspected with unexplained and often rapidly progressing dyspnea115,138,140,149,150. Electrocardiography is rarely contributive, although it eventually discloses signs of right atrial hypertrophy. Echocardiography is more useful for screening of PAH by measuring systolic pulmonary artery pressure (>35 mmHg) and the exclusion of left ventricle dysfunction. The formal procedure for PAH diagnosis remains a right heart catheterization149,150.
Early diagnosis is central for the prognosis of this complication, with mortality as high as 40%119. Treatment for PAH includes the following139,141,142,144,145,149,150: hospitalization in an ICU and rapid referral to a specific reference centre for multidisciplinary round discussions; vasodilating therapies frequently combining endothelin receptor antagonists (bosentan and ambrisentan), phosphodiesterase 5 inhibitors and other guanylate cyclase stimulators (for example, sildenafil), and prostacyclin analogues; high-dose steroids, initially intravenously and then orally; and rapid introduction of biologic immunomodulatory agents targeting IL-1 or IL-6 or other immunosuppressive agents such as methotrexate, azathioprine, cyclophosphamide, ciclosporin or rituximab. However, these treatments must be carefully monitored because of potential adverse effects and the risk of PAH worsening despite their introduction138.
PAH needs to be well known by physicians caring for patients with AoSD; it was not described in most of the initial AoSD case series for several reasons. The main reason for a higher identification rate of PAH could be an improvement in available diagnostic tools. Furthermore, it is possible that cytokine inhibition alone influences only part of the pathogenic pathway in AoSD, which may favour the development of other complications, for example, of PAH.
Amyloidosis
In contrast to PAH, amyloid A amyloidosis is becoming extremely rare owing to the improved ability of AoSD treatments to control inflammation150–155. Amyloidosis might occur in patients with refractory disease or in patients who do not have access to adequate treatments for long periods of time. Multiple organs can be involved. Even administered late, AoSD therapy such as steroids and especially IL-1 and IL-6 blockers might (at least in part) improve the clinical and biological symptoms.
Conclusions
In the past 15 years, substantial progress has been made in the diagnosis and prognosis of AoSD. New insights have been obtained into the complex and heterogeneous nature of AoSD with data on genetic association, involvement of the innate immune system and the cytokine profile. Consequently, several established and new promising targeted therapies are in development for AoSD. However, no reliable prediction of the response and outcome is possible yet, and therapeutic decisions have to be made on the basis of clinical, biological or imaging characteristics. The coming years will probably contribute to a better understanding of the disease and its complications, notably a better understanding of disease pathogenesis and identification of diagnostic and prognostic biomarkers and of new targets for preventing both life-threatening manifestations and chronicity. Owing to obvious similarities between SoJIA and AoSD, these diseases may represent a disease continuum, and thus a close cooperation between paediatric and adult rheumatologists is desirable to establish common diagnostic and therapeutic strategies and approaches.
Acknowledgments
Reviewer information
Nature Reviews Rheumatology thanks M. McDermott, M. Gonzalez-Gay and Y. Shoenfeld for their contribution to the peer review of this work.
Author contributions
All authors contributed to researching data for the article, discussion of content and writing and reviewing and/or editing the manuscript before submission.
Competing interests
E.F. has received consultant fees from AbbVie, Biogen, BMS, Celgene, Janssen, Lilly, Medac, MSD, Nordic Pharma, Novartis, Pfizer, Roche, Sanofi-Aventis, Swedish Orphan Biovitrum and UCB, as well as research grants from BMS, Lilly, Novartis, Pfizer and Roche. S.M. has received consultant fees from BMS and Pfizer. B.F. has received consultant fees from AbbVie, Biogen, BMS, Celgene, Janssen, Lilly, Medac, MSD, Nordic Pharma, Novartis, Pfizer, Roche, Sanofi-Aventis, Swedish Orphan Biovitrum and UCB, as well as research grants from AbbVie, MSD and Pfizer.
Footnotes
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Related links
Saint-Antoine: http://saintantoine.aphp.fr/score/
Contributor Information
Eugen Feist, Email: eugen.feist@charite.de.
Stéphane Mitrovic, Email: stephane.mitrovic@yahoo.fr.
References
- 1.Bywaters EG. Still’s disease in the adult. Ann. Rheum. Dis. 1971;30:121–133. doi: 10.1136/ard.30.2.121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Still GF. On a form of chronic joint disease in children. Med. Chir. Trans.. 1897;80:47–60. [PMC free article] [PubMed] [Google Scholar]
- 3.McGonagle D, McDermott MF. A proposed classification of the immunological diseases. PLOS Med. 2006;3:e297. doi: 10.1371/journal.pmed.0030297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Fautrel B. Adult-onset Still disease. Best Pract. Res. Clin. Rheumatol. 2008;22:773–792. doi: 10.1016/j.berh.2008.08.006. [DOI] [PubMed] [Google Scholar]
- 5.Peckham D, Scambler T, Savic S, McDermott MF. The burgeoning field of innate immune-mediated disease and autoinflammation. J. Pathol. 2017;241:123–139. doi: 10.1002/path.4812. [DOI] [PubMed] [Google Scholar]
- 6.McGonagle D, Savic S, McDermott MF. The NLR network and the immunological disease continuum of adaptive and innate immune-mediated inflammation against self. Semin. Immunopathol. 2007;29:303–313. doi: 10.1007/s00281-007-0084-1. [DOI] [PubMed] [Google Scholar]
- 7.McDermott MF, et al. Germline mutations in the extracellular domains of the 55 kDa TNF receptor, TNFR1, define a family of dominantly inherited autoinflammatory syndromes. Cell. 1999;97:133–144. doi: 10.1016/s0092-8674(00)80721-7. [DOI] [PubMed] [Google Scholar]
- 8.Maria ATJ, et al. Adult onset Still’s disease (AOSD) in the era of biologic therapies: dichotomous view for cytokine and clinical expressions. Autoimmun. Rev. 2014;13:1149–1159. doi: 10.1016/j.autrev.2014.08.032. [DOI] [PubMed] [Google Scholar]
- 9.Church LD, Cook GP, McDermott MF. Primer: inflammasomes and interleukin 1beta in inflammatory disorders. Nat. Clin. Pract. Rheumatol. 2008;4:34–42. doi: 10.1038/ncprheum0681. [DOI] [PubMed] [Google Scholar]
- 10.Hugot JP, et al. Association of NOD2 leucine-rich repeat variants with susceptibility to Crohn’s disease. Nature. 2001;411:599–603. doi: 10.1038/35079107. [DOI] [PubMed] [Google Scholar]
- 11.Ogura Y, et al. A frameshift mutation in NOD2 associated with susceptibility to Crohn’s disease. Nature. 2001;411:603–606. doi: 10.1038/35079114. [DOI] [PubMed] [Google Scholar]
- 12.Vastert SJ, Kuis W, Grom AA. Systemic JIA: new developments in the understanding of the pathophysiology and therapy. Best Pract. Res. Clin. Rheumatol. 2009;23:655–664. doi: 10.1016/j.berh.2009.08.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gerfaud-Valentin M, Jamilloux Y, Iwaz J, Sève P. Adult-onset Still’s disease. Autoimmun. Rev. 2014;13:708–722. doi: 10.1016/j.autrev.2014.01.058. [DOI] [PubMed] [Google Scholar]
- 14.Jamilloux Y, et al. Pathogenesis of adult-onset Still’s disease: new insights from the juvenile counterpart. Immunol. Res. 2015;61:53–62. doi: 10.1007/s12026-014-8561-9. [DOI] [PubMed] [Google Scholar]
- 15.Mellins ED, Macaubas C, Grom AA. Pathogenesis of systemic juvenile idiopathic arthritis: some answers, more questions. Nat. Rev. Rheumatol. 2011;7:416–426. doi: 10.1038/nrrheum.2011.68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mitrovic S, Fautrel B. New markers for adult-onset Still’s disease. Joint Bone Spine. 2018;85:285–293. doi: 10.1016/j.jbspin.2017.05.011. [DOI] [PubMed] [Google Scholar]
- 17.Wittkowski H, et al. S100A12 is a novel molecular marker differentiating systemic-onset juvenile idiopathic arthritis from other causes of fever of unknown origin. Arthritis Rheum. 2008;58:3924–3931. doi: 10.1002/art.24137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Foell D, Roth J. Proinflammatory S100 proteins in arthritis and autoimmune disease. Arthritis Rheum. 2004;50:3762–3771. doi: 10.1002/art.20631. [DOI] [PubMed] [Google Scholar]
- 19.Foell D, et al. Monitoring neutrophil activation in juvenile rheumatoid arthritis by S100A12 serum concentrations. Arthritis Rheum. 2004;50:1286–1295. doi: 10.1002/art.20125. [DOI] [PubMed] [Google Scholar]
- 20.Colafrancesco S, et al. Response to interleukin-1 inhibitors in 140 Italian patients with adult-onset Still’s disease: a multicentre retrospective observational study. Front. Pharmacol. 2017;8:369. doi: 10.3389/fphar.2017.00369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Shields AM, Thompson SJ, Panayi GS, Corrigall VM. Pro-resolution immunological networks: binding immunoglobulin protein and other resolution-associated molecular patterns. Rheumatology. 2012;51:780–788. doi: 10.1093/rheumatology/ker412. [DOI] [PubMed] [Google Scholar]
- 22.Serhan CN. Pro-resolving lipid mediators are leads for resolution physiology. Nature. 2014;510:92–101. doi: 10.1038/nature13479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hofmann SR, et al. Altered expression of IL-10 family cytokines in monocytes from CRMO patients result in enhanced IL-1β expression and release. Clin. Immunol. 2015;161:300–307. doi: 10.1016/j.clim.2015.09.013. [DOI] [PubMed] [Google Scholar]
- 24.Chen D-Y, et al. The potential role of advanced glycation end products (AGEs) and soluble receptors for AGEs (sRAGE) in the pathogenesis of adult-onset still’s disease. BMC Musculoskelet. Disord. 2015;16:111. doi: 10.1186/s12891-015-0569-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Colina M, et al. The evolution of adult-onset Still disease: an observational and comparative study in a cohort of 76 Italian patients. Semin. Arthritis Rheum. 2011;41:279–285. doi: 10.1016/j.semarthrit.2010.12.006. [DOI] [PubMed] [Google Scholar]
- 26.Harth M, Thompson JM, Ralph ED. Adult-onset Still’s disease. Can. Med. Assoc. J. 1979;12:1507–1510. [PMC free article] [PubMed] [Google Scholar]
- 27.Grateau G, et al. How should we approach classification of autoinflammatory diseases? Nat. Rev. Rheumatol. 2013;9:624–629. doi: 10.1038/nrrheum.2013.101. [DOI] [PubMed] [Google Scholar]
- 28.Wouters JM, van de Putte LB. Adult-onset Still’s disease, clinical & laboratory features, treatment & progress of 45 cases. Q. J. Med. 1986;61:1055–1065. [PubMed] [Google Scholar]
- 29.Wakil SM, et al. Association of a mutation in L ACC1 with a monogenic form of systemic juvenile idiopathic arthritis. Arthritis Rheumatol. 2015;67:288–295. doi: 10.1002/art.38877. [DOI] [PubMed] [Google Scholar]
- 30.Cader MZ, et al. C13orf31 (FAMIN) is a central regulator of immunometabolic function. Nat. Immunol. 2016;9:1046–1056. doi: 10.1038/ni.3532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ombrello MJ, et al. HL A-DRB1*11 and variants of the MHC class II locus are strong risk factors for systemic juvenile idiopathic arthritis. Proc. Natl Acad. Sci. USA. 2015;112:15970–15975. doi: 10.1073/pnas.1520779112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Aksentijevich I, McDermott MF. Lessons from characterization and treatment of the autoinflammatory syndromes. Curr. Opin. Rheumatol. 2017;29:187–194. doi: 10.1097/BOR.0000000000000362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Touitou I. Inheritance of autoinflammatory diseases: shifting paradigms & nomenclature. J. Med. Genet. 2013;50:349–359. doi: 10.1136/jmedgenet-2013-101577. [DOI] [PubMed] [Google Scholar]
- 34.Sarrabay G, Touitou I. Autoinflammation. Management of hereditary recurrent fevers—SHARE experience. Nat. Rev. Rheumatol. 2015;11:567–569. doi: 10.1038/nrrheum.2015.114. [DOI] [PubMed] [Google Scholar]
- 35.Magadur-Joly G, et al. Epidemiology of adult Still’s disease: estimate of the incidence by a retrospective study in west France. Ann. Rheum. Dis. 1995;54:587–590. doi: 10.1136/ard.54.7.587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Wakai K, et al. Estimated prevalence and incidence of adult Still’s disease: findings by a nationwide epidemiological survey in Japan. J. Epidemiol. 1997;7:221–225. doi: 10.2188/jea.7.221. [DOI] [PubMed] [Google Scholar]
- 37.van de Putte LB, Wouters JM. Adult-onset Still’s disease. Baillieres Clin. Rheumatol. 1991;5:263–275. doi: 10.1016/s0950-3579(05)80283-3. [DOI] [PubMed] [Google Scholar]
- 38.Ota T, Higashi S, Suzuki H, Eto S. Increased serum ferritin levels in adult Still’s disease. Lancet. 1987;1:562–563. doi: 10.1016/s0140-6736(87)90204-2. [DOI] [PubMed] [Google Scholar]
- 39.Ohta A, et al. Adult Still’s disease: a multicenter survey of Japanese patients. J. Rheumatol. 1990;17:1058–1063. [PubMed] [Google Scholar]
- 40.Fautrel B, et al. Proposal for a new set of classification criteria for adult-onset Still disease. Medicine. 2002;81:194–200. doi: 10.1097/00005792-200205000-00003. [DOI] [PubMed] [Google Scholar]
- 41.Lebrun D, et al. Validation of the Fautrel classification criteria for adult-onset Still’s disease. Semin. Arthritis Rheum. 2018;47:578–585. doi: 10.1016/j.semarthrit.2017.07.005. [DOI] [PubMed] [Google Scholar]
- 42.Ohta A, Yamaguchi M, Kaneoka H, Nagayoshi T, Hiida M. Adult Still’s disease: review of 228 cases from the literature. J. Rheumatol. 1987;14:1139–1146. [PubMed] [Google Scholar]
- 43.Masson C, et al. Adult Still’s disease: part I. Manifestations and complications in sixty-five cases in France. Rev. Rhum. Engl. Ed. 1995;62:748–757. [PubMed] [Google Scholar]
- 44.Crispín JC, Martínez-Baños D, Alcocer-Varela J. Adult-onset Still disease as the cause of fever of unknown origin. Medicine. 2005;84:331–337. doi: 10.1097/01.md.0000188009.47085.76. [DOI] [PubMed] [Google Scholar]
- 45.Zuelgaray E, et al. Increased severity and epidermal alterations in persistent versus evanescent skin lesions in adult onset Still’s disease. J. Am. Acad. Dermatol. 2018 doi: 10.1016/j.jaad.2018.05.020. [DOI] [PubMed] [Google Scholar]
- 46.Nguyen KH, Weisman MH. Severe sore throat as a presenting symptom of adult onset Still’s disease: a case series & review of the literature. J. Rheumatol. 1997;24:592–597. [PubMed] [Google Scholar]
- 47.Lyberatos C. Two more cases of Still’s disease and Kikuchi’s. J. Rheumatol. 1990;17:568–569. [PubMed] [Google Scholar]
- 48.Samuels AJ, Berney SN, Tourtellotte CD, Artymyshyn R. Coexistence of adult onset Still’s disease & polymyositis with rhabdomyolysis successfully treated with methotrexate & corticosteroids. J. Rheumatol. 1989;16:685–687. [PubMed] [Google Scholar]
- 49.Moreno-Alvarez MJ, Citera G, Maldonado-Cocco JA, Taratuto AL. Adult Still’s disease and inflammatory myositis. Clin. Exp. Rheumatol. 1993;11:659–661. [PubMed] [Google Scholar]
- 50.Gonzalez-Hernandez T, Martin-Mola E, Fernandez-Zamorano A, Balsa-Criado A, de Miguel-Mendieta E. Serum ferritin can be useful for diagnosis in adult onset Still’s disease. J. Rheumatol. 1989;16:412–413. [PubMed] [Google Scholar]
- 51.Akritidis N, Giannakakis I, Giouglis T. Ferritin levels & response to treatment in patients with Adult Still’s disease. J. Rheumatol. 1996;23:201–202. [PubMed] [Google Scholar]
- 52.Schiller D, Mittermayer H. Hyperferritinemia as a marker of Still’s disease. Clin. Infect. Dis. 1998;26:534–535. doi: 10.1086/517085. [DOI] [PubMed] [Google Scholar]
- 53.Zandman-Goddard G, Shoenfeld Y. Ferritin in autoimmune diseases. Autoimmun. Rev. 2007;6:457–463. doi: 10.1016/j.autrev.2007.01.016. [DOI] [PubMed] [Google Scholar]
- 54.Fautrel B, et al. Diagnostic value of ferritin and glycosylated ferritin in adult onset Still’s disease. J. Rheumatol. 2001;28:322–329. [PubMed] [Google Scholar]
- 55.Lee MH, Means RT. Extremely elevated serum ferritin levels in a university hospital: associated diseases and clinical significance. Am. J. Med. 1995;98:566–571. doi: 10.1016/s0002-9343(99)80015-1. [DOI] [PubMed] [Google Scholar]
- 56.Rosário C, Zandman-Goddard G, Meyron-Holtz EG, D’Cruz DP, Shoenfeld Y. The hyperferritinemic syndrome: macrophage activation syndrome, Still’s disease, septic shock and catastrophic antiphospholipid syndrome. BMC Med. 2013;11:185. doi: 10.1186/1741-7015-11-185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Mehta B, Efthimiou P. Ferritin in adult-onset still’s disease: just a useful innocent bystander? Int. J. Inflam. 2012;2012:298405. doi: 10.1155/2012/298405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Ruddell RG, et al. Ferritin functions as a proinflammatory cytokine via iron-independent protein kinase C zeta/nuclear factor kappaB-regulated signaling in rat hepatic stellate cells. Hepatology. 2009;49:887–900. doi: 10.1002/hep.22716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Van Reeth C, et al. Serum ferritin and isoferritins are tools for diagnosis of active adult Still’s disease. J. Rheumatol. 1994;21:890–895. [PubMed] [Google Scholar]
- 60.Vignes S, et al. Percentage of glycosylated serum ferritin remains low throughout the course of adult onset Still’s disease. Ann. Rheum. Dis. 2000;59:347–350. doi: 10.1136/ard.59.5.347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Lambotte O, Costedoat-Chalumeau N, Amoura Z, Piette JC, Cacoub P. Drug-induced hemophagocytosis. Am. J. Med. 2002;112:592–593. doi: 10.1016/s0002-9343(02)01035-5. [DOI] [PubMed] [Google Scholar]
- 62.Lambotte O, et al. High ferritin and low glycosylated ferritin may also be a marker of excessive macrophage activation. J. Rheumatol. 2003;30:1027–1028. [PubMed] [Google Scholar]
- 63.Fardet L, et al. Low glycosylated ferritin, a good marker for the diagnosis of hemophagocytic syndrome. Arthritis Rheum. 2008;58:1521–1527. doi: 10.1002/art.23415. [DOI] [PubMed] [Google Scholar]
- 64.Scirè CA, et al. Diagnostic value of procalcitonin measurement in febrile patients with systemic autoimmune diseases. Clin. Exp. Rheumatol. 2006;24:123–128. [PubMed] [Google Scholar]
- 65.Kim H-A, An J-M, Nam J-Y, Jeon J-Y, Suh C-H. Serum S100A8/A9, but not follistatin-like protein 1 and interleukin 18, may be a useful biomarker of disease activity in adult-onset Still’s disease. J. Rheumatol. 2012;39:1399–1406. doi: 10.3899/jrheum.120079. [DOI] [PubMed] [Google Scholar]
- 66.Kim H-A, et al. TLR4 endogenous ligand S100A8/A9 levels in adult-onset Still’s disease and their association with disease activity and clinical manifestations. Int. J. Mol. Sci. 2016;17:1342. doi: 10.3390/ijms17081342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Møller HJ. Soluble CD163. Scand. J. Clin. Lab. Invest. 2012;72:1–13. doi: 10.3109/00365513.2011.626868. [DOI] [PubMed] [Google Scholar]
- 68.Bleesing J, et al. The diagnostic significance of soluble CD163 and soluble interleukin-2 receptor alpha-chain in macrophage activation syndrome and untreated new-onset juvenile idiopathic arthritis. Arthritis Rheum. 2007;56:965–971. doi: 10.1002/art.22416. [DOI] [PubMed] [Google Scholar]
- 69.Colafrancesco S, et al. sCD163 in AOSD: a biomarker for macrophage activation related to hyperferritinemia. Immunol. Res. 2014;60:177–183. doi: 10.1007/s12026-014-8563-7. [DOI] [PubMed] [Google Scholar]
- 70.Han JH, et al. Association of CXCL10 and CXCL13 levels with disease activity and cutaneous manifestation in active adult-onset Still’s disease. Arthritis Res. Ther. 2015;17:260. doi: 10.1186/s13075-015-0773-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Yamaguchi M, et al. Preliminary criteria for classification of adult Still’s disease. J. Rheumatol. 1992;19:424–430. [PubMed] [Google Scholar]
- 72.Pouchot J, et al. Adult Still’s disease: manifestations, disease course, and outcome in 62 patients. Medicine. 1991;70:118–136. [PubMed] [Google Scholar]
- 73.Efthimiou P, Kontzias A, Ward CM, Ogden NS. Adult-onset Still’s disease: can recent advances in our understanding of its pathogenesis lead to targeted therapy? Nat. Clin. Pract. Rheumatol. 2007;3:328–335. doi: 10.1038/ncprheum0510. [DOI] [PubMed] [Google Scholar]
- 74.Masson C, et al. Adult Still’s disease. Part II. Management, outcome, and prognostic factors. Rev. Rhum. Engl. Ed. 1995;62:758–765. [PubMed] [Google Scholar]
- 75.Medsger TA, Christy WC. Carpal arthritis with ankylosis in late onset Still’s disease. Arthritis Rheum. 1976;19:232–242. doi: 10.1002/art.1780190216. [DOI] [PubMed] [Google Scholar]
- 76.Franchini S, et al. Efficacy of traditional and biologic agents in different clinical phenotypes of adult-onset Still’s disease. Arthritis Rheum. 2010;62:2530–2535. doi: 10.1002/art.27532. [DOI] [PubMed] [Google Scholar]
- 77.Castañeda S, Blanco R, González-Gay MA. Adult-onset Still’s disease: advances in the treatment. Best Pract. Res. Clin. Rheumatol. 2016;30:222–238. doi: 10.1016/j.berh.2016.08.003. [DOI] [PubMed] [Google Scholar]
- 78.Husni ME, et al. Etanercept in the treatment of adult patients with Still’s disease. Arthritis Rheum. 2002;46:1171–1176. doi: 10.1002/art.10231. [DOI] [PubMed] [Google Scholar]
- 79.Kiyonaga Y, et al. Steroid-sparing effects of etanercept in a patient with steroid-dependent adult-onset Still’s disease. Intern. Med. 2014;53:1209–1213. doi: 10.2169/internalmedicine.53.1488. [DOI] [PubMed] [Google Scholar]
- 80.Kaneko K, et al. Exacerbation of adult-onset Still’s disease, possibly related to elevation of serum tumor necrosis factor-alpha after etanercept administration. Int. J. Rheum. Dis. 2010;13:e67–e69. doi: 10.1111/j.1756-185X.2010.01544.x. [DOI] [PubMed] [Google Scholar]
- 81.Kraetsch HG, Antoni C, Kalden JR, Manger B. Successful treatment of a small cohort of patients with adult onset of Still’s disease with infliximab: first experiences. Ann. Rheum. Dis. 2001;60(Suppl. 3):iii55–iii57. doi: 10.1136/ard.60.90003.iii55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Cavagna L, Caporali R, Epis O, Bobbio-Pallavicini F, Montecucco C. Infliximab in the treatment of adult Still’s disease refractory to conventional therapy. Clin. Exp. Rheumatol. 2001;19:329–332. [PubMed] [Google Scholar]
- 83.Fautrel B, Sibilia J, Mariette X, Combe B, Club Rhumatismes et Inflammation Tumour necrosis factor alpha blocking agents in refractory adult Still’s disease: an observational study of 20 cases. Ann. Rheum. Dis. 2005;64:262–266. doi: 10.1136/ard.2004.024026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Junge G, Mason J, Feist E. Adult onset Still’s disease — the evidence that anti-interleukin-1 treatment is effective and well-tolerated (a comprehensive literature review) Semin. Arthritis Rheum. 2017;47:295–302. doi: 10.1016/j.semarthrit.2017.06.006. [DOI] [PubMed] [Google Scholar]
- 85.Kötter I, et al. Anakinra in patients with treatment-resistant adult-onset Still’s disease: four case reports with serial cytokine measurements and a review of the literature. Semin. Arthritis Rheum. 2007;37:189–197. doi: 10.1016/j.semarthrit.2007.04.002. [DOI] [PubMed] [Google Scholar]
- 86.Fitzgerald AA, LeClercq SA, Yan A, Homik JE, Dinarello CA. Rapid responses to anakinra in patients with refractory adult-onset Still’s disease. Arthritis Rheum. 2005;52:1794–1803. doi: 10.1002/art.21061. [DOI] [PubMed] [Google Scholar]
- 87.Naumann L, et al. IL1-receptor antagonist anakinra provides long-lasting efficacy in the treatment of refractory adult-onset Still’s disease. Ann. Rheum. Dis. 2010;69:466–467. doi: 10.1136/ard.2009.108068. [DOI] [PubMed] [Google Scholar]
- 88.Kalliolias GD, Georgiou PE, Antonopoulos IA, Andonopoulos AP, Liossis S-NC. Anakinra treatment in patients with adult-onset Still’s disease is fast, effective, safe and steroid sparing: experience from an uncontrolled trial. Ann. Rheum. Dis. 2007;66:842–843. doi: 10.1136/ard.2006.066381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Lequerre T, et al. Interleukin-1 receptor antagonist (anakinra) treatment in patients with systemic-onset juvenile idiopathic arthritis or adult onset Still disease: preliminary experience in France. Ann. Rheum. Dis. 2007;67:302–308. doi: 10.1136/ard.2007.076034. [DOI] [PubMed] [Google Scholar]
- 90.Giampietro C, et al. Anakinra in adult-onset Still’s disease: long-term treatment in patients resistant to conventional therapy. Arthritis Care Res. 2013;65:822–826. doi: 10.1002/acr.21901. [DOI] [PubMed] [Google Scholar]
- 91.Hong D, et al. Interleukin 1 inhibition with anakinra in adult-onset Still disease: a meta-analysis of its efficacy and safety. Drug Des. Devel. Ther. 2014;8:2345–2357. doi: 10.2147/DDDT.S73428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.European Medicines Agency. Kineret. European Medicines Agencyhttp://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/000363/human_med_000874.jsp&mid=WC0b01ac058001d124 (2018).
- 93.US National Library of Medicine. ClinicalTrials.govhttps://clinicaltrials.gov/ct2/show/study/NCT03265132 (2018).
- 94.Ortiz-Sanjuán F, et al. Efficacy of anakinra in refractory adult-onset Still’s disease: multicenter study of 41 patients and literature review. Medicine. 2015;94:e1554. doi: 10.1097/MD.0000000000001554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Goldbach-Mansky R, et al. Differential response to the long acting IL-1 inhibitor IL-1 trap in 2 patients with adult onset Still’s disease (AOSD) Ann. Rheum. Dis. 2006;65:262–262. [Google Scholar]
- 96.Petryna O, Cush JJ, Efthimiou P. IL-1 trap rilonacept in refractory adult onset Still’s disease. Ann. Rheum. Dis. 2012;71:2056–2057. doi: 10.1136/annrheumdis-2012-201409. [DOI] [PubMed] [Google Scholar]
- 97.Henderson C, et al. Safety and efficacy of IL-1 trap in resistant adult onset Still’s disease: 24 month follow-up of open label treatment and biomarkers of response. Arthritis Rheum. 2010;62(Suppl. 10):S765. [Google Scholar]
- 98.Kontzias A, Efthimiou P. The use of canakinumab, a novel IL-1β long-acting inhibitor, in refractory adult-onset Still’s disease. Semin. Arthritis Rheum. 2012;42:201–205. doi: 10.1016/j.semarthrit.2012.03.004. [DOI] [PubMed] [Google Scholar]
- 99.Lo Gullo A, et al. Canakinumab in a case of Adult onset Still’s disease: efficacy only on systemic manifestations. Joint Bone Spine. 2014;81:376–377. doi: 10.1016/j.jbspin.2013.12.011. [DOI] [PubMed] [Google Scholar]
- 100.Barsotti S, et al. Successful treatment of refractory adult-onset Still disease with canakinumab: a case report. J. Clin. Rheumatol. 2014;20:121. doi: 10.1097/RHU.0000000000000082. [DOI] [PubMed] [Google Scholar]
- 101.US National Library of Medicine. ClinicalTrials.gov, https://clinicaltrials.gov/ct2/show/NCT02204293 (2018).
- 102.Banse C, et al. Reactive macrophage activation syndrome possibly triggered by canakinumab in a patient with adult-onset Still’s disease. Joint Bone Spine. 2013;80:653–655. doi: 10.1016/j.jbspin.2013.04.011. [DOI] [PubMed] [Google Scholar]
- 103.Nirmala N, et al. Gene-expression analysis of adult-onset Still’s disease and systemic juvenile idiopathic arthritis is consistent with a continuum of a single disease entity. Pediatr. Rheumatol. 2015;13:50. doi: 10.1186/s12969-015-0047-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Puéchal X, et al. Tocilizumab in refractory adult Still’s disease. Arthritis Care Res. 2011;63:155–159. doi: 10.1002/acr.20319. [DOI] [PubMed] [Google Scholar]
- 105.Elkayam O, et al. Tocilizumab in adult-onset Still’s disease: the Israeli experience. J. Rheumatol. 2014;41:244–247. doi: 10.3899/jrheum.130881. [DOI] [PubMed] [Google Scholar]
- 106.Cipriani P, et al. Tocilizumab for the treatment of adult-onset Still’s disease: results from a case series. Clin. Rheumatol. 2014;33:49–55. doi: 10.1007/s10067-013-2381-5. [DOI] [PubMed] [Google Scholar]
- 107.Thonhofer R, et al. Treatment of refractory adult-onset still’s disease with tocilizumab: report of two cases and review of the literature. Rheumatol. Int. 2011;31:1653–1656. doi: 10.1007/s00296-010-1631-y. [DOI] [PubMed] [Google Scholar]
- 108.Ortiz-Sanjuán F, et al. Efficacy of tocilizumab in conventional treatment-refractory adult-onset Still’s disease: multicenter retrospective open-label study of thirty-four patients: tocilizumab in AOSD refractory to standard treatment. Arthritis Rheumatol. 2014;66:1659–1665. doi: 10.1002/art.38398. [DOI] [PubMed] [Google Scholar]
- 109.Li T, et al. A pilot study on tocilizumab for treating refractory adult-onset Still’s disease. Sci. Rep. 2017;7:13477. doi: 10.1038/s41598-017-13639-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Song ST, et al. Efficacy of tocilizumab therapy in Korean patients with adult-onset Still’s disease: a multicentre retrospective study of 22 cases. Clin. Exp. Rheumatol. 2016;34:S64–S71. [PubMed] [Google Scholar]
- 111.Ma Y, et al. Efficacy and safety of tocilizumab with inhibition of interleukin-6 in adult-onset Still’s disease: a meta-analysis. Mod. Rheumatol. 2017 doi: 10.1080/14397595.2017.1416924. [DOI] [PubMed] [Google Scholar]
- 112.Nishina N, Kaneko Y, Kameda H, Takeuchi T. The effect of tocilizumab on preventing relapses in adult-onset Still’s disease: a retrospective, single-center study. Mod. Rheumatol. 2015;25:401–404. doi: 10.3109/14397595.2014.973659. [DOI] [PubMed] [Google Scholar]
- 113.Gabay C, et al. Open-label, multicentre, dose-escalating phase II clinical trial on the safety and efficacy of tadekinig alfa (IL-18BP) in adult-onset Still’s disease. Ann. Rheum. Dis. 2018;77:840–847. doi: 10.1136/annrheumdis-2017-212608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Rau M, et al. Clinical manifestations but not cytokine profiles differentiate adult-onset Still’s disease and sepsis. J. Rheumatol. 2010;37:2369–2376. doi: 10.3899/jrheum.100247. [DOI] [PubMed] [Google Scholar]
- 115.Mitrovic S, Fautrel B. Complications of adult-onset Still’s disease and their management. Exp. Rev. Clin. Immunol. 2018;14:351–365. doi: 10.1080/1744666X.2018.1465821. [DOI] [PubMed] [Google Scholar]
- 116.Néel A, et al. Diagnostic and management of life-threatening adult-onset Still disease: a French nationwide multicenter study and systematic literature review. Crit. Care. 2018;22:88. doi: 10.1186/s13054-018-2012-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Kumakura S, Murakawa Y. Clinical characteristics and treatment outcomes of autoimmune-associated hemophagocytic syndrome in adults: autoimmune-associated hemophagocytic syndrome. Arthritis Rheumatol. 2014;66:2297–2307. doi: 10.1002/art.38672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Gerfaud-Valentin M, et al. Adult-onset still disease: manifestations, treatment, outcome, and prognostic factors in 57 patients. Medicine. 2014;93:91–99. doi: 10.1097/MD.0000000000000021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Efthimiou P, Kadavath S, Mehta B. Life-threatening complications of adult-onset Still’s disease. Clin. Rheumatol. 2014;33:305–314. doi: 10.1007/s10067-014-2487-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Mimura T, Shimodaira M, Kibata M, Tsukadaira A, Shirahata K. Adult-onset Still’s disease with disseminated intravascular coagulation and hemophagocytic syndrome: a case report. BMC Res. Notes. 2014;7:940. doi: 10.1186/1756-0500-7-940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Shinohara T, Hidaka T, Matsuki Y, Suzuki K, Ohsuzu F. Calcinosis cutis and intestinal pseudoobstruction in a patient with adult onset Still’s disease associated with recurrent relapses of disordered coagulopathy. Intern. Med. 1999;38:516–520. doi: 10.2169/internalmedicine.38.516. [DOI] [PubMed] [Google Scholar]
- 122.Yokoyama M, et al. A case of adult onset Still’s disease complicated with adult respiratory distress syndrome and disseminated intravascular coagulation [Japanese] Nihon Rinsho Meneki Gakkai Kaishi. 1995;18:207–214. doi: 10.2177/jsci.18.207. [DOI] [PubMed] [Google Scholar]
- 123.Yamashita S, et al. Extremely high serum ferritin: an instrumental marker of masquerading adult-onset Still’s disease with hemophagocytic syndrome. Am. J. Case Rep. 2017;18:1296–1301. doi: 10.12659/AJCR.905684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Colina M, Govoni M, Trotta F. Fatal myocarditis in adult-onset Still disease with diffuse intravascular coagulation. Rheumatol. Int. 2009;29:1355–1357. doi: 10.1007/s00296-008-0813-3. [DOI] [PubMed] [Google Scholar]
- 125.Namas R, et al. An unusual case of adult-onset Still’s disease with hemophagocytic syndrome, necrotic leukoencephalopathy and disseminated intravascular coagulation. Case Rep. Rheumatol. 2014;2014:128623. doi: 10.1155/2014/128623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Sakata N, Shimizu S, Hirano F, Fushimi K. Epidemiological study of adult-onset Still’s disease using a Japanese administrative database. Rheumatol. Int. 2016;36:1399–1405. doi: 10.1007/s00296-016-3546-8. [DOI] [PubMed] [Google Scholar]
- 127.Matsumoto K, et al. Glucocorticoid and cyclosporine refractory adult onset Still’s disease successfully treated with tocilizumab. Clin. Rheumatol. 2009;28:485–487. doi: 10.1007/s10067-009-1097-z. [DOI] [PubMed] [Google Scholar]
- 128.Park J-H, et al. Adult-onset Still’s disease with disseminated intravascular coagulation and multiple organ dysfunctions dramatically treated with cyclosporine A. J. Korean Med. Sci. 2004;19:137–141. doi: 10.3346/jkms.2004.19.1.137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Kumar A, Kato H. Macrophage activation syndrome associated with adult-onset Still’s disease successfully treated with anakinra. Case Rep. Rheumatol. 2016;2016:3717392. doi: 10.1155/2016/3717392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.El Karoui K, et al. Thrombotic microangiopathy and purtscher-like retinopathy associated with adult-onset Still’s disease: a role for glomerular vascular endothelial growth factor? Arthritis Rheum. 2009;61:1609–1613. doi: 10.1002/art.24826. [DOI] [PubMed] [Google Scholar]
- 131.Zheng XL, Kaufman RM, Goodnough LT, Sadler JE. Effect of plasma exchange on plasma ADAMTS13 metalloprotease activity , inhibitor level, and clinical outcome in patients with idiopathic and nonidiopathic thrombotic thrombocytopenic purpura. Blood. 2004;103:4043–4049. doi: 10.1182/blood-2003-11-4035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Bianchi V, Robles R, Alberio L, Furlan M, Lämmle B. Von Willebrand factor-cleaving protease (ADAMTS13) in thrombocytopenic disorders: a severely deficient activity is specific for thrombotic thrombocytopenic purpura. Blood. 2002;100:710–713. doi: 10.1182/blood-2002-02-0344. [DOI] [PubMed] [Google Scholar]
- 133.Hirata S, et al. Deficient activity of von Willebrand factor-cleaving protease in thrombotic thrombocytopenic purpura in the setting of adult-onset Still’s disease. Rheumatology. 2006;45:1046–1047. doi: 10.1093/rheumatology/kel176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Gopal M, Cohn CD, McEntire MR, Alperin JB. Thrombotic thrombocytopenic purpura and adult onset Still’s disease. Am. J. Med. Sci. 2009;337:373–376. doi: 10.1097/MAJ.0b013e318191436e. [DOI] [PubMed] [Google Scholar]
- 135.Masuyama A, et al. A case of adult-onset Still’s disease complicated by thrombotic thrombocytopenic purpura with retinal microangiopathy and rapidly fatal cerebral edema. Mod. Rheumatol. 2013;23:379–385. doi: 10.1007/s10165-012-0650-9. [DOI] [PubMed] [Google Scholar]
- 136.Chen C-H, et al. Pulmonary arterial hypertension in autoimmune diseases: an analysis of 19 cases from a medical center in northern Taiwan. J. Microbiol. Immunol. Infect. 2006;39:162–168. [PubMed] [Google Scholar]
- 137.Menezes de Siqueira ME, Rodrigues RP, Kormann APM. Adult-onset Still’s disease and pulmonary arterial hypertension. Respir. Med. CME. 2009;2:70–72. [Google Scholar]
- 138.Guilleminault L, Laurent S, Foucher A, Poubeau P, Paganin F. Pulmonary arterial hypertension in adult onset Still’s disease: a case report of a severe complication. BMC Pulm. Med. 2016;16:72. doi: 10.1186/s12890-016-0237-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Kadavath S, Zapantis E, Zolty R, Efthimiou P. A novel therapeutic approach in pulmonary arterial hypertension as a complication of adult-onset Still’s disease: targeting IL-6. Int. J. Rheum. Dis. 2014;17:336–340. doi: 10.1111/1756-185X.12324. [DOI] [PubMed] [Google Scholar]
- 140.Lowther GH, Chertoff J, Cope J, Alnuaimat H, Ataya A. Pulmonary arterial hypertension and acute respiratory distress syndrome in a patient with adult-onset stills disease. Pulm. Circ. 2017;7:797–802. doi: 10.1177/2045893217712710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Mehta MV, Manson DK, Horn EM, Haythe J. An atypical presentation of adult-onset Still’s disease complicated by pulmonary hypertension and macrophage activation syndrome treated with immunosuppression: a case-based review of the literature. Pulm. Circ. 2016;6:136–142. doi: 10.1086/685112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Mubashir E, Ahmed MM, Hayat S, Heldmann M, Berney SM. Pulmonary hypertension in a patient with adult-onset Stills disease. Clin. Rheumatol. 2007;26:1359–1361. doi: 10.1007/s10067-006-0382-3. [DOI] [PubMed] [Google Scholar]
- 143.Padilla-Ibarra J, Sanchez-Ortiz A, Sandoval-Castro C, Ramos-Remus C. Rituximab treatment for pulmonary arterial hypertension in adult-onset Still’s disease. Clin. Exp. Rheumatol. 2013;31:657–658. [PubMed] [Google Scholar]
- 144.Thakare M, Habibi S, Agrawal S, Narsimulu G. Pulmonary arterial hypertension complicating adult-onset Still’s disease. Clin. Rheumatol. 2013;32(Suppl. 1):S1–S2. doi: 10.1007/s10067-009-1230-z. [DOI] [PubMed] [Google Scholar]
- 145.Weatherald J, Lategan J, Helmersen D. Pulmonary arterial hypertension secondary to adult-onset Still’s disease: response to cyclosporine and sildenafil over 15 years of follow-up. Respir. Med. Case Rep. 2016;19:27–30. doi: 10.1016/j.rmcr.2016.06.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Zen A, et al. A case of adult Still’s disease with pulmonary hypertension [Japanese] Ryumachi. 1990;30:45–52. [PubMed] [Google Scholar]
- 147.Campos M, Schiopu E. Pulmonary arterial hypertension in adult-onset Still’s disease: rapid response to anakinra. Case Rep. Rheumatol. 2012;2012:537613. doi: 10.1155/2012/537613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148.Huertas A, et al. Immune dysregulation and endothelial dysfunction in pulmonary arterial hypertension: a complex interplay. Circulation. 2014;129:1332–1340. doi: 10.1161/CIRCULATIONAHA.113.004555. [DOI] [PubMed] [Google Scholar]
- 149.McLaughlin VV, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension: a report of the American College of Cardiology Foundation Task Force on expert consensus documents and the American Heart Association: developed in collaboration with the American College of Chest Physicians, American Thoracic Society , Inc., and the Pulmonary Hypertension Association. Circulation. 2009;119:2250–2294. doi: 10.1161/CIRCULATIONAHA.109.192230. [DOI] [PubMed] [Google Scholar]
- 150.Galiè N, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Respir. J. 2015;46:903–975. doi: 10.1183/13993003.01032-2015. [DOI] [PubMed] [Google Scholar]
- 151.Uppal SS, Al-Mutairi M, Hayat S, Abraham M, Malaviya A. Ten years of clinical experience with adult onset Still’s disease: is the outcome improving? Clin. Rheumatol. 2007;26:1055–1060. doi: 10.1007/s10067-006-0440-x. [DOI] [PubMed] [Google Scholar]
- 152.Ben Ghorbel I, Khanfir M, Houman MH. Amyloidosis in adult onset Still’s disease [French] Rev. Med. Interne. 2004;25:675–677. doi: 10.1016/j.revmed.2004.04.025. [DOI] [PubMed] [Google Scholar]
- 153.Ishii T, et al. Systemic amyloidosis in a patient with adult onset Still’s disease. Intern. Med. 1993;32:50–52. doi: 10.2169/internalmedicine.32.50. [DOI] [PubMed] [Google Scholar]
- 154.Oh YB, et al. Secondary renal amyloidosis in adult onset Still’s disease: case report and review of the literature. Korean J. Intern. Med. 2000;15:131–134. doi: 10.3904/kjim.2000.15.2.131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 155.Rivera F, et al. Vascular renal AA amyloidosis in adult Still’s disease. Nephrol. Dial. Transplant. 1997;12:1714–1716. doi: 10.1093/ndt/12.8.1714. [DOI] [PubMed] [Google Scholar]
- 156.Ichida H, et al. Clinical manifestations of adult-onset Still’s disease presenting with erosive arthritis: association with low levels of ferritin and interleukin-18. Arthritis Care Res. 2014;66:642–646. doi: 10.1002/acr.22194. [DOI] [PubMed] [Google Scholar]
- 157.Kawashima M, et al. Levels of interleukin-18 and its binding inhibitors in the blood circulation of patients with adult-onset Still’s disease. Arthritis Rheum. 2001;44:550–560. doi: 10.1002/1529-0131(200103)44:3<550::AID-ANR103>3.0.CO;2-5. [DOI] [PubMed] [Google Scholar]
- 158.Chen D-Y, Lan J-L, Lin F-J, Hsieh T-Y. Proinflammatory cytokine profiles in sera and pathological tissues of patients with active untreated adult onset Still’s disease. J. Rheumatol. 2004;31:2189–2198. [PubMed] [Google Scholar]
- 159.Choi J-H, et al. Serum cytokine profiles in patients with adult onset Still’s disease. J. Rheumatol. 2003;30:2422–2427. [PubMed] [Google Scholar]
- 160.Priori R, et al. Interleukin 18: a biomarker for differential diagnosis between adult-onset Still’s disease and sepsis. J. Rheumatol. 2014;41:1118–1123. doi: 10.3899/jrheum.130575. [DOI] [PubMed] [Google Scholar]
- 161.Rooney T, et al. Synovial tissue interleukin-18 expression and the response to treatment in patients with inflammatory arthritis. Ann. Rheum. Dis. 2004;63:1393–1398. doi: 10.1136/ard.2003.016428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 162.Conigliaro P, et al. Lymph node IL-18 expression in adult-onset Still’s disease. Ann. Rheum. Dis. 2009;68:442–443. doi: 10.1136/ard.2008.093781. [DOI] [PubMed] [Google Scholar]
- 163.Priori R, et al. Markedly increased IL-18 liver expression in adult-onset Still’s disease-related hepatitis. Rheumatology. 2011;50:776–780. doi: 10.1093/rheumatology/keq397. [DOI] [PubMed] [Google Scholar]
- 164.Kawaguchi Y, Terajima H, Harigai M, Hara M, Kamatani N. Interleukin-18 as a novel diagnostic marker and indicator of disease severity in adult-onset Still’s disease. Arthritis Rheum. 2001;44:1716–1717. doi: 10.1002/1529-0131(200107)44:7<1716::AID-ART298>3.0.CO;2-I. [DOI] [PubMed] [Google Scholar]
- 165.Jung K-H, et al. Interleukin-18 as an efficient marker for remission and follow-up in patients with inactive adult-onset Still’s disease. Scand. J. Rheumatol. 2014;43:162–169. doi: 10.3109/03009742.2013.824023. [DOI] [PubMed] [Google Scholar]
- 166.Sugiura T, et al. Association between adult-onset Still’s disease and interleukin-18 gene polymorphisms. Genes Immun. 2002;3:394–399. doi: 10.1038/sj.gene.6363922. [DOI] [PubMed] [Google Scholar]
- 167.Maruyama J, Inokuma S. Cytokine profiles of macrophage activation syndrome associated with rheumatic diseases. J. Rheumatol. 2010;37:967–973. doi: 10.3899/jrheum.090662. [DOI] [PubMed] [Google Scholar]
- 168.Bae C-B, et al. Serum S100A12 may be a useful biomarker of disease activity in adult-onset Still’s disease. J. Rheumatol. 2014;41:2403–2408. doi: 10.3899/jrheum.140651. [DOI] [PubMed] [Google Scholar]
- 169.Zou Y-Q, et al. The levels of macrophage migration inhibitory factor as an indicator of disease activity and severity in adult-onset Still’s disease. Clin. Biochem. 2008;41:519–524. doi: 10.1016/j.clinbiochem.2008.01.008. [DOI] [PubMed] [Google Scholar]
- 170.Chen D-Y, Lan J-L, Lin F-J, Hsieh T-Y. Association of intercellular adhesion molecule-1 with clinical manifestations and interleukin-18 in patients with active, untreated adult-onset Still’s disease. Arthritis Rheum. 2005;53:320–327. doi: 10.1002/art.21164. [DOI] [PubMed] [Google Scholar]
- 171.Belfeki N, et al. Successful treatment of refractory adult onset Still’s disease with rituximab. Reumatismo. 2016;68:159–162. doi: 10.4081/reumatismo.2016.888. [DOI] [PubMed] [Google Scholar]
- 172.Ostrowski RA, Tehrani R, Kadanoff R. Refractory adult-onset still disease successfully treated with abatacept. J. Clin. Rheumatol. 2011;17:315–317. doi: 10.1097/RHU.0b013e31822c53ad. [DOI] [PubMed] [Google Scholar]
- 173.Quartuccio L, Maset M, De Vita S. Efficacy of abatacept in a refractory case of adult-onset Still’s disease. Clin. Exp. Rheumatol. 2010;28:265–267. [PubMed] [Google Scholar]
- 174.Fardet L, et al. Development and validation of the HScore, a score for the diagnosis of reactive hemophagocytic syndrome. Arthritis Rheumatol. 2014;66:2613–2620. doi: 10.1002/art.38690. [DOI] [PubMed] [Google Scholar]
- 175.Drepper M, Rubbia-Brandt L, Spahr L. Tocilizumab-induced acute liver injury in adult onset Still’s disease. Case Rep. Hepatol. 2013;2013:964828. doi: 10.1155/2013/964828. [DOI] [PMC free article] [PubMed] [Google Scholar]