

Abstract
Aims
In male athletes, caffeine is considered an ergogenic aid to increase anaerobic performance during the Wingate anaerobic test (WANT). However, information about the effect of caffeine on WANT performance in female athletes is contradictory. Furthermore, it is unknown whether the ergogenicity of caffeine is present during all the phases of the menstrual cycle. The aim of this study was to investigate the effects of caffeine intake on WANT performance during 3 phases of the menstrual cycle.
Methods
Thirteen well‐trained eumenorrhoeic triathletes participated in a double‐blind, placebo‐controlled, cross‐over experimental trial. On 2 different days in each phase, and in randomized order, participants ingested caffeine (3 mg kg−1) or a placebo (cellulose). The menstrual cycle phases were individually characterized as follows: (i) early follicular; (ii) preovulatory; and (iii) midluteal. In each trial, participants performed a 15‐s adapted version of the WANT.
Results
In comparison to the placebo, caffeine increased peak power during the WANT in the early follicular (8.6 ± 0.8 vs 8.9 ± 0.9 W/kg, P = .04; effect size [d] = 0.45), preovulatory (8.6 ± 0.9 vs 8.9 ± 0.9 W/kg, P = .04; d = 0.23) and mid‐luteal phases (8.6 ± 0.8 vs 8.9 ± 0.9 W/kg, P < .01; d = 0.52).
Conclusion
The ergogenic effect of caffeine on WANT peak cycling power was of a similar magnitude in the follicular, preovulatory, and mid‐luteal phases. These results suggest that caffeine increases performance in the 15‐s Wingate test in women athletes and it might be considered an ergogenic aid to increase anaerobic performance in eumenorrhoeic women during their menstrual cycle.
Keywords: ergogenicity, exercise, menstrual cycle, physical activity, sex, stimulant, women
What is known about this subject
Previous research has led to the current notion that the acute ingestion of a moderate dose of caffeine can produce an increase in Wingate performance.
However, the current evidence has been obtained with study samples of only male participants or in investigations in which women represented a low proportion of the study subjects.
Thus, the inference of an enhancement in Wingate performance after caffeine intake obtained in prior investigations with male samples might not be useful for female athletes seeking the ergogenicity of caffeine.
What this study adds
The ingestion of 3 mg/kg of caffeine increased peak and mean cycling power during a 15‐s Wingate test in the follicular, preovulatory, and mid‐luteal menstrual phases of trained female triathletes.
Caffeine's ergogenic effect was of similar magnitude in the 3 phases of the menstrual cycle, suggesting that caffeine increases Wingate performance in women during the whole menstrual cycle.
In trained and eumenorrhoeic women who have not undergone oral contraceptive treatments, caffeine is effective to increase anaerobic performance, irrespective of the menstrual cycle phase.
1. INTRODUCTION
Despite the initial controversy on this topic,1, 2 the effectiveness of acute caffeine ingestion to improve peak and mean cycling power in the Wingate anaerobic performance test has been well established by recent investigations3, 4 and meta‐analytic data.5 However, evidence also suggests that doses <3 mg of caffeine/kg of body mass6 or the use of coffee as the form caffeine administration7 might be less effective than the use of 3–9 mg/kg via pure anhydrous caffeine or caffeinated energy drinks.3, 5, 8 Caffeine ergogenicity for the Wingate test might persist with daily ingestion of 3 mg/kg of caffeine for 15–18 days; however, the magnitude of its ergogenic effect is higher the first day of ingestion, suggesting tolerance to this substance.9 Lastly, caffeine might be used to improve both upper and lower body Wingate performance,4, 10 which suggests that the effect of caffeine to enhance anaerobic performance is independent of the muscle mass involved in the exercise. All this previous information has led to the current notion that the acute ingestion of a moderate dose of caffeine can produce an increase in Wingate performance and this outcome has been used to establish the ergogenicity of caffeine for anaerobic exercise routines.
The above‐mentioned investigations have been carried out using samples of only male participants2, 4, 8 or women represented a low proportion of the study subjects, impeding a subanalysis of caffeine effects on female participants.1, 3, 9 The meta‐analysis of the caffeine ergogenic effect on Wingate performance carried out by Grgic5 included 16 studies with 246 male participants and only 47 female participants. Interestingly, the only investigation of caffeine effects on Wingate performance using a sample of female participants concluded that 5 mg/kg of caffeine was not effective to increase any performance variable measured during the Wingate test.11 Thus, the inference of an enhancement in Wingate performance after caffeine intake obtained in prior investigations with male samples might not be useful for female athletes seeking the ergogenicity of caffeine.
In addition, the effect of caffeine on increasing blood pressure and enhancing mood can be modulated by variations in female sex hormones.12, 13 The use of oral contraceptives interferes with caffeine metabolism and excretion as the intake of ethinyloestradiol inhibits the activity of CYP1A2,14 an enzyme responsible for the metabolism of caffeine into dimethylxanthines.15 Thus, it is possible that the magnitude of the ergogenic effect of caffeine might be different during the different phases of the menstrual cycle which might explain the lack of caffeine ergogenicity on Wingate performance in women.11 A recent investigation has determined that acute caffeine ingestion (3 mg/kg) has the capacity of increasing peak aerobic cycling power to a similar extent in 3 different phases of the menstrual cycle (early follicular, preovulatory and midluteal phases16). However, the paucity of data on the effect of caffeine supplementation on Wingate performance in women impedes ascertaining whether caffeine is ergogenic in female athletes seeking enhanced anaerobic performance and whether caffeine ergogenicity is of similar magnitude during the different phases of the menstrual cycle. Thus, the main objective of this investigation was to determine the effect of caffeine on Wingate performance during 3 phases of the menstrual cycle in eumenorrhoeic females.
2. METHODS
2.1. Participants
Thirteen women triathletes volunteered to participate in this investigation (age = 31 ± 6 years; body mass = 58.6 ± 7.8 kg; body height = 1.66 ± 0.06 m, body fat = 14.5 ± 6.5%; maximal oxygen uptake = 48.1 ± 7.3 mL kg−1 min−1). The inclusion criteria were as follows: (i) age between 18 and 40 years; (ii) being involved in triathlon competitions and with an endurance training of ~2 h day−1, at least 5 days week−1 for the previous 2 months; (iii) having a daily caffeine consumption lower than 50 mg day−1 in the previous 3 months (measured with a food frequency questionnaire17; (iv) having a regular duration of their menstrual cycle, defined as a variation lower than 3 days in the range of their menstrual cycles' length for the previous 4 months.18 The exclusion criteria were: (i) having a menstrual disorder; (ii) positive smoking status; (iii) a previous history of cardiopulmonary diseases; (iv) any injury in the previous 6 months; (v) taking oral contraceptives or medications in the previous month; (vi) allergy to caffeine. Before the beginning of the experimental protocol, participants were fully informed of the experimental procedures and signed an informed written consent to participate in the investigation. The study was approved by the Camilo José Cela University Research Ethics Committee (CAFTRI‐2017). All the research protocols were in accordance with the latest version of the Declaration of Helsinki.
2.2. Experimental design
After enrolment, participants completed 2 trials in each of the following 3 phases of their individually‐characterized menstrual cycle: (i) early follicular (EF); (ii) preovulatory (PO); and (iii) mid‐luteal (ML). These 3 phases were chosen because they represent menses, peak serum oestrogen concentration and peak serum progesterone concentration, respectively.19 Each participant's regularity and length of the menstrual cycle (27 ± 2 days, interindividual range from 24 to 31 days) were monitored for 4 months prior to the investigation using a mobile application (Mycalendar, Period‐tracker, USA). The onset of each menstrual cycle phase was individually verified using characteristic events associated with the menstrual cycle stages,20 as follow: the first trial in EF was performed the day after the first signs of menstrual bleeding and the second trial was performed 48 h later; the first trial in PO was performed the day after an increase in the urine concentration of the luteinizing hormone (LH) measured with reactive test strips (One Step Ovulation LH Test Strip; CVS Corporation, US) and confirmed by an increase in basal tympanic temperature (model HDT8208C, Nursal Ear Thermometer, China); the second trial in PO was performed 48 h later; the first trial of ML was performed on the day equivalent to 70% of the individual menstrual cycle length (i.e. 20th day from the first day of the menstrual cycle for a 28‐day cycle length); the second trial in ML was performed 48 h later.
In each menstrual cycle phase, women ingested an opaque and unidentifiable capsule containing either caffeine (3 mg kg−1; Bulk Powders, UK) or a placebo (cellulose, Guinama, Spain). The order of the substances within each phase of the menstrual cycle was randomized. The first phase of the investigated menstrual cycle was randomly assigned, and a similar number of participants started in EF (5 participants), PO (4 participants) and ML (4 participants). An alphanumeric code was assigned to each trial by a person independent of the study to blind the participants and researchers to the substances analysed and this same person assigned the order of the trials. All these settings were arranged to produce a double‐blind, placebo‐controlled cross‐over experiment. The drug/molecular target nomenclature used in this investigation conforms to the Guide to pharmacology nomenclature classification of the International Union of Basic and Clinical Pharmacology (IUPHAR) and the British Pharmacological Society (BPS15).
2.3. Experimental protocol
Participants were encouraged to avoid nutritional supplements and sympathetic stimulants in their diets and to maintain their training routines during the whole duration of the experiment. Two weeks before beginning the experimental trials, participants performed 2 days of familiarization with the testing. The day before each trial, participants performed light and standardized training, consisting of 60 min of cycling at 60% of their peak heart rate. Fluid and diet guidelines21, 22 were given to assure carbohydrate bioavailability and euhydration in all experimental trials. A self‐selected precompetitive diet/fluid routine that fulfilled these guidelines was chosen by each participant before the first trial, and it was replicated before all the remaining trials. The day of each trial, participants arrived at the laboratory in a fed state (~3 h after their last meal) and 2 h after ingesting 7 mL/kg of water. All the trials were performed in the morning (from 10 AM to 12 PM) to avoid the effect of circadian variations in the results of the study. Ambient temperature and humidity were kept constant at 21.0 ± 0.8 C and 42 ± 5%, respectively. Upon arrival, participants were weighed (B‐418, Tanita, Japan) and the capsule was provided to be ingested with 150 mL of water. Sixty minutes after the capsule ingestion, participants performed a 15‐min warm‐up and a maximal ramp test to assess maximal oxygen uptake. The results of this protocol of increasing intensity have been discussed elsewhere.16
After 10 min of recovery, which consisted of pedalling at 50 W, participants performed an adapted version of the Wingate anaerobic test. The test was performed on a cycle ergometer (SNT Medical, Cardgirus, Spain), set to produce a resistance to pedalling that represented 7.5% of the participant's body mass. For this test, participants started from a stationary position with their dominant leg ready to pedal and were told that “they had to pedal as fast as they could from the beginning and for the whole duration of the test”. After the “start” command, the resistance load was progressively applied within 1 s to produce an acceleration phase. During the Wingate test, standardized encouragement and feedback were given to the participants in all trials by the same researcher who was blinded to the treatments. This researcher also verified that participants remained seated during the whole test. During the Wingate test, cycling power was obtained with a frequency of 1 Hz and the peak and mean cycling power (in W/kg) obtained during the test were recorded as previously described.9 In addition, peak and minimum cycling power were used to calculate the Wingate fatigue index (%) as previously suggested.4 One minute after the end of the test, a blood sample was obtained from a fingertip to analyse blood lactate concentration (Lactate Pro 2, Arkay, Japan, in mmol/L). Finally, participants were asked about their self‐perceived muscle power during the test (1–10 point scale) and exertion (2–20 point, Borg scale).
2.4. Statistical analysis
Data were collected as previously indicated and the results of each test were blindly introduced into the statistical package SPSS v 20.0 for later analysis. Normality was tested and confirmed for each variable with the Shapiro–Wilk test (P > .05). As the objective of this investigation was to identify the ergogenic effect of caffeine within each phase of the menstrual cycle, differences between the caffeine vs placebo protocols were determined by 2‐way analysis of variance (substance × menstrual cycle) with repeated measures and LSD posthoc analysis. As the objective of this investigation was to identify the ergogenic effect of caffeine in each phase of the menstrual cycle, only placebo‐caffeine comparisons within the same phase were identified. Cohen's effect size (d) was calculated in all statistically significant pairwise comparisons.23 The criteria to interpret the magnitude of effect size were: ≤0.2 trivial, >0.2–0.6 small, >0.6–1.2 moderate, >1.2–2.0 large, >2.0 very large.24 The results are presented as group average ± standard deviation. The significance level was set at P < .05.
3. RESULTS
There was a main effect of caffeine on Wingate peak power (P < .01) with no main effect on menstrual cycle nor interaction (Table 1). In comparison to the placebo, caffeine intake increased 15‐s Wingate peak power in EF (+1.8 ± 2.8%, d = 0.45; P = .04), in PO (+1.9 ± 3.4%, d = 0.23; P = .04) and in ML (+3.6 ± 2.9%, d = 0.52; P < .01, Figure 1). The number of participants who did not increase their Wingate peak power in response to caffeine was 2 in EF, 4 in PO, and 1 in ML. Figure 2 depicts the individual caffeine‐induced changes in Wingate peak cycling power in the 3 different phases of the menstrual cycle. Except for participants 3, 9 and 13, all the triathletes increased their Wingate peak power in response to caffeine in at least 2 phases of their menstrual cycle. All participants presented an increase in Wingate peak cycling power with caffeine in at least 1 of the menstrual cycle phases.
Table 1.
Mean power, fatigue index, blood lactate concentration and self‐reported fatigue and muscle strength during a 15‐s Wingate test with the administration of 3 mg kg−1 of caffeine or a placebo in 3 different phases of the menstrual cycle
| Variable (units) | Early follicular | Preovulatory | Mid‐luteal | Main effect | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Placebo | Caffeine | d | Placebo | Caffeine | d | Placebo | Caffeine | d | Substance | Cycle | Interaction | |
| Peak power (W/kg) | 8.6 ± 0.8 | 8.9 ± 0.9* | 0.45 | 8.6 ± 0.9 | 8.9 ± 0.9* | 0.23 | 8.6 ± 0.8 | 8.9 ± 0.8* | 0.52 | <0.01 | 0.69 | 0.37 |
| Mean power (W/kg) | 7.8 ± 0.8 | 7.9 ± 0.7* | 0.20 | 7.8 ± 0.9 | 8.0 ± 0.8* | 0.25 | 8.0 ± 0.7 | 8.2 ± 0.7* | 0.37 | <0.01 | 0.14 | 0.05 |
| Fatigue index (%) | 25.8 ± 6.6 | 27.5 ± 10.4 | 0.27 | 26.0 ± 10.0 | 26.3 ± 7.5 | 0.04 | 25.4 ± 10.7 | 25.6 ± 7.1 | 0.02 | 0.15 | 0.23 | 0.31 |
| Blood lactate concentration (mmol/L) | 10.0 ± 2.6 | 11.7 ± 4.1* | 0.68 | 10.9 ± 3.6 | 11.9 ± 2.6 | 0.47 | 10.8 ± 3.4 | 11.9 ± 4.5 | 0.41 | 0.04 | 0.58 | 0.80 |
| Borg scale (a.u) | 19 ± 1 | 19 ± 1 | 0.24 | 19 ± 1 | 19 ± 1 | −0.37 | 19 ± 1 | 19 ± 1 | −0.14 | 0.58 | 0.45 | 0.12 |
| Perceived muscle power (a.u) | 8.3 ± 1.0 | 8.9 ± 1.1 | 0.79 | 8.9 ± 1.0 | 8.8 ± 0.8 | −0.24 | 8.7 ± 1.3 | 8.6 ± 1.0 | −0.15 | 0.77 | 0.59 | 0.25 |
(*) Caffeine different from placebo within the same menstrual cycle phase at P < .05. a.u. = arbitrary units.
Figure 1.
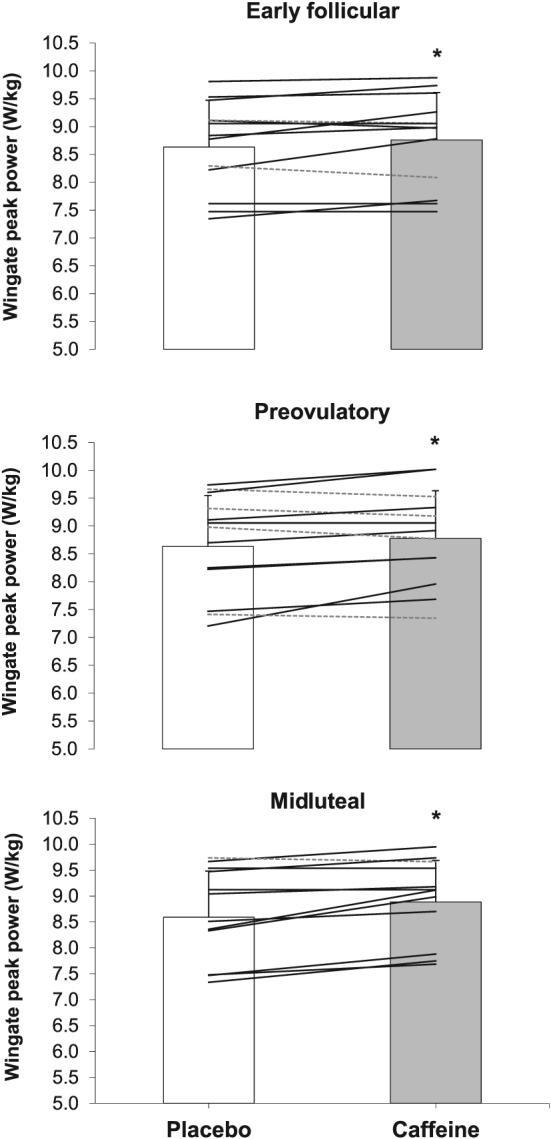
Peak cycling power (W/kg) during a 15‐s Wingate test with the administration of 3 mg kg−1 of caffeine or a placebo in the early follicular, preovulatory, and midluteal phases of the menstrual cycle.The columns represent the group's average and the whiskers represent 1 standard deviation. The solid lines represent individual responses for participants with increased Wingate peak power in the caffeine vs placebo comparison. The dotted lines represent individual responses in subjects that decreased Wmax as a result of caffeine ingestion. (*) Caffeine different from placebo within the same menstrual cycle phase at P < .05
Figure 2.
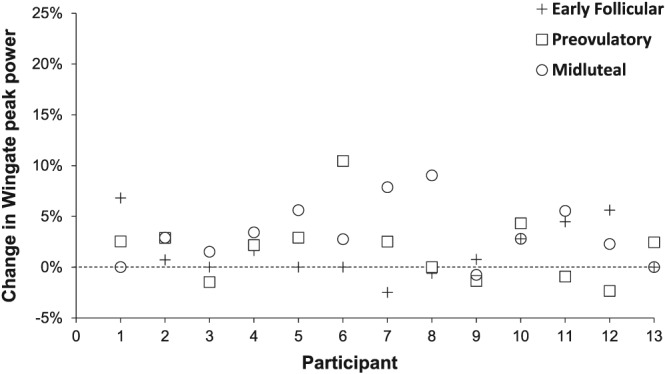
Individual responses for the percentage change with the administration of 3 mg kg−1 of caffeine relative to a placebo in Wingate peak power (W/kg) in the different phases of the menstrual cycle
Table 1 presents information about the effect of caffeine on 15‐s Wingate mean power, fatigue index, blood lactate concentration and self‐perceived fatigue and muscle power during the menstrual cycle. Briefly, there was a main effect of caffeine on Wingate mean power (P < .01) with no main effect on menstrual cycle and a tendency for interaction (P = .05). In the pairwise comparison, caffeine was effective to increase mean cycling power in EF (+1.0 ± 1.8%, d = 0.20; P = .03), PO (+2.1 ± 3.0%, d = 0.25; P = .02) and ML (+2.4 ± 2.1%, d = 0.37; P = .02). However, caffeine did not affect the Wingate fatigue index in any of the phases of the menstrual cycle (Table 1). There was a main effect of caffeine on blood lactate concentration (P = .04), although the ingestion of caffeine increased blood lactate concentration at the end of the Wingate test only in EF (+16.6 ± 28.1%, d = 0.68; P = .03) while this effect was not present in PO or ML phases (Table 1). Caffeine did not affect the rating of exertion measured with the Borg scale or the self‐reported rating of muscle power (Table 1).
4. DISCUSSION
The main objective of this study was to investigate the effect of the intake of a moderate dose of caffeine on Wingate performance during 3 phases of the menstrual cycle. The key outcomes of this investigation indicate that, in well‐trained women triathletes, 3 mg of caffeine per kg of body mass, ingested 60 min before exercise, can be effective to increase peak and mean cycling power during an adapted version of the Wingate test. In addition, the magnitude of the caffeine‐induced performance enhancement was similar in the early follicular, preovulatory and mid‐luteal phases of the participants' menstrual cycles (Figure 1). Although the ergogenic effect was significant in statistical terms, caffeine ergogenicity was catalogued as small in terms of size for both peak and mean cycling power (Table 1) without a clear effect of the menstrual cycle phase under investigation on caffeine's effectiveness to increase Wingate performance. All these outcomes indicate that caffeine might be effective to increase performance in the 15‐s adapted version of the Wingate anaerobic test during the menstrual cycle. Measuring individual responses to caffeine should be conducted before caffeine is recommended as a substance to increase anaerobic performance in women, as it has been reported that some individuals do not positively respond to caffeine.3, 25
As previously suggested,26, 27 peak and mean cycling power during the Wingate test are unaffected by the menstrual cycle in both women with normal menstrual cycles and those using oral contraceptives. These outcomes have been corroborated by the current analysis because no main effect of the menstrual cycle was found for any variable (Table 1). However, the fluctuations in main female sex hormones during the menstrual cycle might interfere with the metabolism of caffeine and thus change the effectiveness of this stimulant as an ergogenic aid.14 Specifically, the activity of the human cytochrome P450 CYP1A2 might be affected by oestradiol28 producing slower caffeine metabolism in the follicular phase of the menstrual cycle than in the luteal phase. Ultimately, the slower conversion of caffeine into paraxanthine might increase the effects of caffeine on the human body in the follicular phase, a speculation that has some empirical support because the effects of caffeine on increasing blood pressure are higher in the follicular vs the luteal phase of adolescent women after the ingestion of 2 mg/kg of caffeine.12 Nevertheless, it has been found that pharmacokinetics of caffeine might be unaffected by the menstrual cycle29 while the ergogenic effect of caffeine on aerobic performance is of similar magnitude in the early follicular, preovulatory and mid‐luteal phases of the menstrual cycle.16
A number of recent investigations have concluded that caffeine enhances exercise performance in populations of female athletes.30, 31, 32, 33 In addition, a recent investigation indicates that caffeine might have a similar ergogenic effect in men and women, at least during an endurance performance trial in cycling.34 However, these findings contrast with the lack of effect of caffeine to increase peak and mean cycling performance on the Wingate test in women,11 while it seems that caffeine effectiveness to increase anaerobic performance might be lower in women than in men despite the use of the same dose of caffeine.35 The inconsistency among these results regarding caffeine ergogenicity in women's exercise performance might be related to the moment at which it is tested: in most of the previously mentioned investigations, caffeine was compared to a placebo during only 1 specific phase of the menstrual cycle—often, the follicular phase of the menstrual cycle minimizing the impacts of oestradiol and progesterone on the study outcomes.36 However, there is no evidence to ascertain whether caffeine ergogenicity on anaerobic performance fluctuates during the menstrual cycle.
The present investigation is novel because it investigates the effect of caffeine on Wingate performance at 3 different moments during the menstrual cycle, helping to provide a complete understanding of caffeine ergogenicity in women. Interestingly, 3 mg/kg of caffeine increased both mean and peak cycling power in the early follicular, preovulatory and mid‐luteal phases of the menstrual cycle. In addition, the magnitude of the effect on peak (~2.3%) and mean (~1.8%) cycling power was similar across menstrual cycle phases and was very comparable to meta‐analytic data obtained with investigations using mainly male study samples (4 and 3% for peak and mean cycling power in the Wingate test5). These results coincide with the effect of caffeine to increase peak wattage obtained during a ramp exercise test in all these 3 phases of the menstrual cycle (2.7–3.6%16;). Together, this information suggests that caffeine might be effective to increase performance by 2–3% in aerobic‐ and anaerobic‐based exercises in women while this ergogenic effect is similar across the menstrual cycle, at least in eumenorrhoeic women. Nevertheless, Figure 2 depicts that this ergogenic effect of caffeine might have different magnitude depending on the individual and thus, caffeine should be recommended to increase performance on an individualized basis.
Previous investigations have repeatedly reported that acute caffeine intake increases both performance and postexercise blood lactate concentration after anaerobic tests.37, 38 In the current investigation, the ergogenic effect after caffeine intake was accompanied by an increased blood lactate concentration in the early follicular phase. Although it did not reach statistical significance, caffeine produced an effect of small magnitude to increase blood lactate concentration in the preovulatory and mid‐luteal phases (Table 1). These concomitant increases in the 15‐s Wingate performance and in the blood lactate concentration after caffeine intake make difficult to determine the cause of the effect. To the authors' opinion, the effect of caffeine on postexercise blood lactate concentration is the result of increased performance with caffeine (indirect effect) rather than effect of caffeine on metabolic pathways during exercise (direct effect). Nevertheless, postexercise blood concentration was similar in all phases of the menstrual cycle confirming the lack of influence of the menstrual cycle on blood lactate concentration during exercise.39 Taken together, these outcomes indicate that caffeine's ergogenicity during maximal exercise tests might be accompanied by increased blood lactate concentrations as the result of increased physical performance while the menstrual cycle has little effect on the association caffeine ergogenicity–blood lactate concentration, as previously found for peak aerobic performance.16
The present investigation does have some limitations and their explanation might be useful to interpret the study outcomes. First, the adapted version of the Wingate test performed in this investigation was carried out 10 min after the end of an incremental maximal cycle ergometer test, which results have been recently published.16 Although preliminary data showed no influence of the incremental test on the results of the Wingate test, it remains possible that a certain fatigue was present at the onset of the Wingate test in our results. Second, there was no assessment of serum concentration of oestrogens or progesterone during the duration of the study. Although the onset of each menstrual cycle phases was based on several physiological measurements (previous cycle length, menstrual bleeding, urine LH upsurge and the change in tympanic temperature) that validate the study,20 the measurement of serum concentrations of the main female sex hormones would have helped to confirm each stage of the cycle. Third, although the experiment was controlled by a placebo, double‐blinded, and the order of trials and the menstrual cycle phases was randomized, participants were aware that their menstrual cycle was under investigation. This could have biased some of the investigation results. Finally, the study sample was limited to eumenorrhoeic women with minor symptoms associated with pre‐menstrual syndrome. Thus, the outcomes of this investigation are only applicable to women that share these characteristics and further investigations are required to ascertain caffeine ergogenicity in women taking oral contraceptives.
In summary, the ingestion of 3 mg/kg of caffeine increased peak and mean cycling power during a 15‐s Wingate test in the follicular, preovulatory, and mid‐luteal menstrual phases of trained women triathletes. In addition, the caffeine‐placebo ergogenic effect in the 3 phases of the menstrual cycle was of similar magnitude, suggesting that caffeine increases Wingate performance in women during the whole menstrual cycle. These outcomes might indicate that, in trained and eumenorrhoeic women who have not undergone oral contraceptive treatments, caffeine is effective to increase some aspects of anaerobic performance, irrespective of the menstrual cycle phase.
COMPETING INTERESTS
There are no competing interests to declare.
CONTRIBUTORS
B.L., B.R.M. and J.D.C. formulated the research question, B.L., B.R.M. and J.D.C. designed the study, B.L., J.G.H. and C.R.M. carried it out, B.L., J.G.H. and J.D.C. analysed the data, B.L. and J.D.C. wrote the article, J.G.H., C.R. and B.R.M. revised the article.
ACKNOWLEDGEMENTS
The authors would like to thank the participants for their invaluable contribution to this research effort to investigate the effects of caffeine on women athletes. The authors are also very grateful to the Spanish Triathlon Federation for its support and help in the recruitment process.
The study was part of the CAFTRI project supported by a grant from the Spanish Higher Council for Sport conceded to the Spanish Triathlon Federation, which financed the expenses necessary to carry out this project.
Lara B, Gutiérrez Hellín J, Ruíz‐Moreno C, Romero‐Moraleda B, Del Coso J. Acute caffeine intake increases performance in the 15‐s Wingate test during the menstrual cycle. Br J Clin Pharmacol. 2020;86:745–752. 10.1111/bcp.14175
Juan Del Coso is the PI for this research.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- 1. Collomp K, Ahmaidi S, Audran M, Chanal JL, Préfaut C. Effects of caffeine ingestion on performance and anaerobic metabolism during the Wingate test. Int J Sports Med. 1991;12(05):439‐443. 10.1055/s-2007-1024710 [DOI] [PubMed] [Google Scholar]
- 2. Greer F, McLean C, Graham TE. Caffeine, performance, and metabolism during repeated Wingate exercise tests. J Appl Physiol. 1998;85(4):1502‐1508. 10.1152/jappl.1998.85.4.1502 [DOI] [PubMed] [Google Scholar]
- 3. Salinero JJ, Lara B, Ruiz‐Vicente D, et al. CYP1A2 genotype variations do not modify the benefits and drawbacks of caffeine during exercise: a pilot study. Nutrients. 2017;9(3):e269 10.3390/nu9030269 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Duncan MJ, Eyre E, Grgic J, Tallis J. The effect of acute caffeine ingestion on upper and lower body anaerobic exercise performance. Eur J Sport Sci. 2019;19(10):1‐8. 10.1080/17461391.2019.1601261 [DOI] [PubMed] [Google Scholar]
- 5. Grgic J. Caffeine ingestion enhances Wingate performance: a meta‐analysis. Eur J Sport Sci. 2018;18(2):219‐225. 10.1080/17461391.2017.1394371 [DOI] [PubMed] [Google Scholar]
- 6. Turley KR, Eusse PA, Thomas MM, Townsend JR, Morton AB. Effects of different doses of caffeine on anaerobic exercise in boys. Pediatr Exerc Sci. 2015;27(1):50‐56. 10.1123/pes.2014-0032 [DOI] [PubMed] [Google Scholar]
- 7. Anderson DE, LeGrand SE, McCart RD. Effect of caffeine on Sprint cycling in experienced cyclists. J Strength Cond Res. 2018;32(8):2221‐2226. 10.1519/JSC.0000000000002685 [DOI] [PubMed] [Google Scholar]
- 8. Chtourou H, Trabelsi K, Ammar A, Shephard RJ, Bragazzi NL. Acute effects of an “energy drink” on short‐term maximal performance, reaction times, psychological and physiological parameters: insights from a randomized double‐blind, placebo‐controlled, counterbalanced crossover trial. Nutrients. 2019;11(5):e992 10.3390/nu11050992 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Lara B, Ruiz‐Moreno C, Salinero JJ, Del Coso J. Time course of tolerance to the performance benefits of caffeine. PLoS One. 2019;14(1):e0210275 10.1371/journal.pone.0210275 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Duncan MJ, Dobell AP, Caygill CL, Eyre E, Tallis J. The effect of acute caffeine ingestion on upper body anaerobic exercise and cognitive performance. Eur J Sport Sci. 2019;19(1):103‐111. 10.1080/17461391.2018.1508505 [DOI] [PubMed] [Google Scholar]
- 11. Mahdavi R, Daneghian S, Jafari A, Homayouni A. Effect of acute caffeine supplementation on anaerobic power and blood lactate levels in female athletes. J Caffeine Res. 2015;5(2):83‐87. 10.1089/jcr.2014.0034 [DOI] [Google Scholar]
- 12. Temple JL, Ziegler AM. Gender differences in subjective and physiological responses to caffeine and the role of steroid hormones. J Caffeine Res. 2011;1(1):41‐48. 10.1089/jcr.2011.0005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Temple JL, Ziegler AM, Graczyk A, Bendlin A, Sion T, Vattana K. Cardiovascular responses to caffeine by gender and pubertal stage. Pediatrics. 2014;134(1):e112‐e119. 10.1542/peds.2013-3962 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Arnaud MJ. Pharmacokinetics and metabolism of natural Methylxanthines in animal and man. Methylxanthines. 2011;33‐91. [DOI] [PubMed] [Google Scholar]
- 15. International Union of Basic and Clinical Pharmacology (IUPHAR) and the British Pharmacological Society (BPS) . caffeine|Ligand page|IUPHAR/BPS Guide to PHARMACOLOGY. https://www.guidetopharmacology.org/GRAC/LigandDisplayForward?ligandId=407. Accessed 3 Oct 2019
- 16. Lara B, Gutiérrez‐Hellín J, García‐Bataller A, et al. Ergogenic effects of caffeine intake on peak aerobic cycling power during the menstrual cycle. Eur J Nutr. In press 2019;1‐10. [DOI] [PubMed] [Google Scholar]
- 17. Gonçalves LS, Painelli VS, Yamaguchi G, et al. Dispelling the myth that habitual caffeine consumption influences the performance response to acute caffeine supplementation. J Appl Physiol. 2017;123(1):213‐220. 10.1152/japplphysiol.00260.2017 [DOI] [PubMed] [Google Scholar]
- 18. Creinin MD, Keverline S, Meyn LA. How regular is regular? An analysis of menstrual cycle regularity. Contraception. 2004;70(4):289‐292. 10.1016/j.contraception.2004.04.012 [DOI] [PubMed] [Google Scholar]
- 19. Shechter A, Boivin DB. Sleep, hormones, and circadian rhythms throughout the menstrual cycle in healthy women and women with premenstrual dysphoric disorder. Int J Endocrinol. 2010:259345 10.1155/2010/259345 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Janse de Jonge XAK. Effects of the menstrual cycle on exercise performance. Sport Med. 2003;33(11):833‐851. 10.2165/00007256-200333110-00004 [DOI] [PubMed] [Google Scholar]
- 21. Burke LM, Hawley JA, Wong SHS, Jeukendrup AE. Carbohydrates for training and competition. J Sports Sci. 2011;29(sup1):S17‐S27. 10.1080/02640414.2011.585473 [DOI] [PubMed] [Google Scholar]
- 22. McDermott BP, Anderson SA, Armstrong LE, et al. National Athletic Trainers' association position statement: fluid replacement for the physically active. J Athl Train. 2017;52(9):877‐895. 10.4085/1062-6050-52.9.02 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Cohen J. Statistical power analysis for the behavioral sciences, Second Edition. Hillsdale, New Jersey: Lawrence Erlbaum Associates Inc; 1988. [Google Scholar]
- 24. Batterham AM, Hopkins WG. Making meaningful inferences about magnitudes. Int J Sports Physiol Perform. 2006;1(1):50‐57. [PubMed] [Google Scholar]
- 25. Lara B, Ruiz‐Vicente D, Areces F, et al. Acute consumption of a caffeinated energy drink enhances aspects of performance in sprint swimmers. Br J Nutr. 2015;114(6):908‐914. 10.1017/S0007114515002573 [DOI] [PubMed] [Google Scholar]
- 26. Bushman B, Masterson G, Nelsen J. Anaerobic power performance and the menstrual cycle: eumenorrheic and oral contraceptive users. J Sports Med Phys Fitness. 2006;46(1):132‐137. [PubMed] [Google Scholar]
- 27. Okudan N, Gökbel H, Uçok K, Baltaci A. Serum leptin concentration and anaerobic performance do not change during the menstrual cycle of young females. Neuro Endocrinol Lett. 2005;26(4):297‐300. [PubMed] [Google Scholar]
- 28. Granfors MT, Backman JT, Laitila J, Neuvonen PJ. Oral contraceptives containing ethinyl estradiol and gestodene markedly increase plasma concentrations and effects of tizanidine by inhibiting cytochrome P450 1A2. Clin Pharmacol Ther. 2005;78(4):400‐411. 10.1016/j.clpt.2005.06.009 [DOI] [PubMed] [Google Scholar]
- 29. McLean C, Graham TE. Effects of exercise and thermal stress on caffeine pharmacokinetics in men and eumenorrheic women. J Appl Physiol. 2002;93(4):1471‐1478. 10.1152/japplphysiol.00762.2000 [DOI] [PubMed] [Google Scholar]
- 30. Fett CA, Aquino NM, Schantz Junior J, Brandão CF, de Araújo Cavalcanti JD, Fett WC. Performance of muscle strength and fatigue tolerance in young trained women supplemented with caffeine. J Sports Med Phys Fitness. 2018;58(3):249‐255. 10.23736/S0022-4707.17.06615-4 [DOI] [PubMed] [Google Scholar]
- 31. Lara B, Gonzalez‐Millán C, Salinero JJ, et al. Caffeine‐containing energy drink improves physical performance in female soccer players. Amino Acids. 2014;46(5):1385‐1392. 10.1007/s00726-014-1709-z [DOI] [PubMed] [Google Scholar]
- 32. Pérez‐López A, Salinero JJ, Abian‐Vicen J, et al. Caffeinated energy drinks improve volleyball performance in elite female players. Med Sci Sports Exerc. 2015;47(4):850‐856. 10.1249/MSS.0000000000000455 [DOI] [PubMed] [Google Scholar]
- 33. Portillo J, Del Coso J, Abián‐Vicén J. Effects of caffeine ingestion on skill performance during an international female Rugby sevens competition. J Strength Cond Res. 2017;31(12):3351‐3357. 10.1519/JSC.0000000000001763 [DOI] [PubMed] [Google Scholar]
- 34. Skinner TL, Desbrow B, Arapova J, et al. Women experience the same ergogenic response to caffeine as men. Med Sci Sports Exerc. 2019;51(6):1195‐1202. 10.1249/MSS.0000000000001885 [DOI] [PubMed] [Google Scholar]
- 35. Mielgo‐Ayuso J, Marques‐Jiménez D, Refoyo I, del Coso J, León‐Guereño P, Calleja‐González J. Effect of caffeine supplementation on sports performance based on differences between sexes: a systematic review. Nutrients. 2019;11(10):e2313 10.3390/NU11102313 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Bruinvels G, Burden RJ, McGregor AJ, et al. Sport, exercise and the menstrual cycle: where is the research? Br J Sports Med. 2017;51(6):487‐488. 10.1136/bjsports-2016-096279 [DOI] [PubMed] [Google Scholar]
- 37. Glaister M, Muniz‐Pumares D, Patterson SD, Foley P, McInnes G. Caffeine supplementation and peak anaerobic power output. Eur J Sport Sci. 2015;15(5):400‐406. 10.1080/17461391.2014.962619 [DOI] [PubMed] [Google Scholar]
- 38. Davis JK, Green JM. Caffeine and anaerobic performance: ergogenic value and mechanisms of action. Sports Med. 2009;39(10):813‐832. 10.2165/11317770-000000000-00000 [DOI] [PubMed] [Google Scholar]
- 39. Lamont LS. Lack of influence of the menstrual cycle on blood lactate. Phys Sportsmed. 1986;14(11):159‐163. 10.1080/00913847.1986.11709230 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.