

Abstract
Background:
Jowl fat overhang can reduce jawline definition. The most common treatment to reduce jowl fat is liposuction. ATX-101 (deoxycholic acid injection), a minimally invasive treatment approved for submental fat reduction, may also be an effective treatment for jowl fat. The current study evaluated the efficacy and safety of ATX-101 treatment for reducing jowl fat.
Methods:
In this prospective single-site study, 66 adults were treated for excess jowl fat with ATX-101 (area-adjusted dose: 2 mg/cm2). Eligible patients had pinchable fat on the jawline and relatively minimal skin laxity in the jowl. Depending on the size of the treatment area, ATX-101 injections of 0.2 ml spaced 1.0 cm apart or 0.1 ml spaced 0.50 to 0.75 cm apart were administered. Improvement in jowl appearance was assessed 6 months or more after the last treatment in person by the clinician. Improvement was also assessed by the patient and two independent plastic surgeons using blinded before/after treatment photographs. Safety was evaluated via adverse events.
Results:
The mean number of ATX-101 treatments received was 1.8, with a mean injection volume of 0.8 ml per treatment per jowl. The majority of patients (98 percent) experienced an improvement in jowl appearance. Common adverse events were injection-site edema, numbness, tenderness, and bruising. Injection-site marginal mandibular nerve paresis and alopecia were experienced by three patients each; all events resolved without sequelae.
Conclusions:
ATX-101 effectively reduced jowl fat and was well tolerated in this small cohort. Care should be taken when injecting ATX-101 into jowl fat to avoid underlying anatomic structures such as the marginal mandibular nerve.
CLINICAL QUESTION/LEVEL OF EVIDENCE:
Therapeutic, IV.
The chin and jawline are common areas of aesthetic concern1,2 and loss of chin definition occurs as part of the natural aging process.3 A youthful neck has a distinct inferior mandibular border with no jowl overhang.4 Excess jowl fat influences perceptions of age and attractiveness,5 and its positioning is an important component of facial rejuvenation.6
Jowl fat consists of the superior and inferior fat pads, with the mandibular septum acting like a sling beneath both jowl fat pads and fusing with the platysma muscle.7 Changes over time to subcutaneous fat compartments around the mandibular septum can lead to jowling and facial aging. Jowling may be caused by atrophy of subcutaneous tissue, ptosis resulting from compartment displacement, and/or mandibular septum dehiscence, allowing fat to flow into the neck.8 Facial aging is on a continuum of several anatomic changes, including fat accumulation in some fat pads and atrophy in others. There is laxity of retaining ligaments and dermal thinning/compromise of collagen and elasticity. Skeletal resorption leads to less support for the soft-tissue structures. Finally, muscle laxity and loss of mechanical advantage occur. Accurate analysis of the jowling mechanism for each patient is necessary to determine the appropriate course of treatment. Patients must be carefully selected because sagging skin in the jowl should not be treated with fat-reducing procedures.8,9
Jowl fat is currently treated through traditional aesthetic surgical procedures performed under general anesthesia, targeted liposuction, ultrasound and radiofrequency procedures, and unlicensed lipolytic drugs. Physician survey data from 2012 found that liposuction was used in 81 percent of jowl fat reduction procedures; however, more than half of physicians agreed that they would likely try a noninvasive treatment for this area.10
Injection adipocytolysis may be an appropriate treatment for some patients presenting with jowl fat. Injection of jowl fat with phosphatidylcholine and other compounded formulas results in fat reduction and skin retraction according to 21 percent (16/75) of physicians responding to a 2006 survey.11 Phosphatidylcholine/sodium deoxycholate injection can reduce sagging jowls9 and eliminate normal jowl fat that contributes to rounding of the jawline.12,13 Phosphatidylcholine, phosphatidylcholine/sodium deoxycholate, and other compounded formulas are not approved by regulatory agencies. ATX-101 (deoxycholic acid injection; Kybella in the United States; Belkyra in Canada, Australia, Europe, and South Korea; Kythera Biopharmaceuticals, Inc, an affiliate of Allergan, Westlake Village, Calif., an affiliate of Allergan)14,15 is an approved adipocytolytic treatment for reduction of submental fat that may also be useful in treating jowling caused by excess fat. When injected into subcutaneous fat, the active ingredient of ATX-101 (deoxycholic acid) disrupts adipocyte cell membranes, and a subsequent inflammatory response clears the injection site of cellular debris and liberated lipids.16–21 Treatment of jowl fat has been safely accomplished with ATX-101.22,23 The current study was conducted to evaluate the efficacy and safety of ATX-101 for reduction of jowl fat. To the author’s knowledge, this is the first prospective, interventional study for the treatment of jowl fat with ATX-101.
PATIENTS AND METHODS
Study Design and Patient Selection
This prospective, interventional study was conducted at a single site (Luxurgery, New York, N.Y.) in accordance with the Declaration of Helsinki and the International Conference on Harmonisation Tripartite Guidelines for Good Clinical Practice. The study period was 1 year (January 1 to December 31, 2016). Written and verbal informed consent was obtained from each patient.
All patients were adults with pinchable fat on the jawline. The presence of moderate to severe skin laxity of the jowl is a relative contraindication for ATX-101 treatment. Patients with extreme skin laxity of the jowl were excluded.
Treatment Procedure
Patients were eligible to receive ATX-101 treatment for reduction of both jowl fat and submental fat. Most jowl fat treatments were administered in the same session as submental fat treatments, although some patients continued jowl treatments after completion of the submental fat treatment course. The 1.0-cm injection grid with 0.2 ml per injection (area-adjusted dose: 2 mg/cm2) recommended for ATX-101 treatment of submental fat was used on the jowl unless the surface area was relatively small. In instances in which surface area was limited, 0.1-ml injections were administered at 0.50- to 0.75-cm intervals. The depth of each injection was 6 to 10 mm using a 0.5-inch, 32-gauge needle. Injections were administered in the anatomic area superior to the inferior mandibular border, anterior to the antegonial notch, posterior to the caudal continuation of the oral commissure into the prejowl sulcus, and inferior to the line created by extending the midline labiomental sulcus to the ear lobule (Fig. 1).24 [See Video (online), which provides a demonstration of the marking for injection of ATX-101 into the fat pad of the jowl of a patient.] During injection, fat and skin were pinched and pulled away from the underlying musculature and neurovascular structures. This technique allows for perpendicular injection into the jowl fat by presenting the target area and optimizing the angle of injection. The terminal arborization of the marginal mandibular nerve typically occurs in the jowl but is deep to the subcutaneous fat. Pinching and retracting the skin and fat decreases the likelihood of temporary marginal mandibular nerve paresis. Comfort measures used to reduce adverse events included local anesthesia (lidocaine plus epinephrine 10 minutes before treatment), postinjection ice (for 48 hours after treatment), and postinjection oral analgesia (acetaminophen).
Fig. 1.
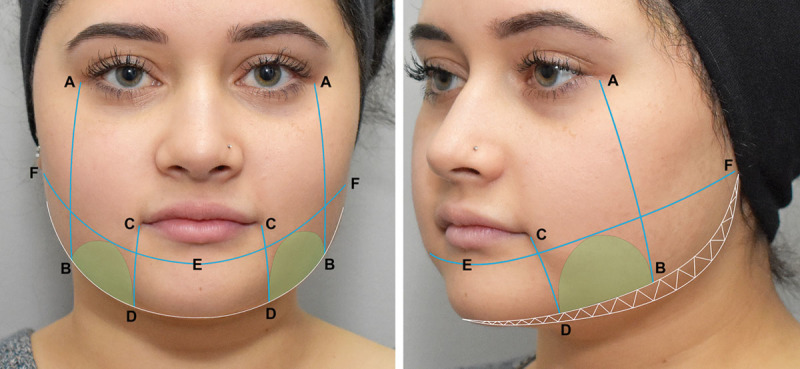
Diagram of facial markings used to isolate the jowl treatment area. A, Lateral canthus; B, antegonial notch; C, oral commissure; D, prejowl sulcus; E, midline labiomental sulcus; F, ear lobule. White hatched area is the zone of marginal mandibular nerve innervation at the inferior border of the mandible. Green shaded area is the inferior jowl fat pad.
Data Collected
The total volume of ATX-101 injected into each jowl during each treatment and the ATX-101 volume per injection were recorded. Standardized photographs were acquired at baseline (pretreatment) and at the final follow-up assessment (≥6 months after final treatment). Improvement in jowl appearance (as a function of improved jawline definition) was evaluated at the final follow-up assessment. This timing allowed for resolution of most adverse events and for treatment effects to be fully realized. Efficacy was evaluated in person by the clinician (author) through visual appraisal and physical palpation of the treatment area. In addition to assessment by the clinician, blinded before/after treatment photographs were classified by the patient and two independent plastic surgeons as before or after. The clinician, patient, and at least one of the two blinded plastic surgeons had to agree that improvement in jowl appearance was achieved for a patient to be classified as “improved.” The incidence and duration of adverse events were monitored throughout the study.
RESULTS
In this study, 66 patients were treated with ATX-101 to reduce their jowl fat (Table 1). The mean age was 46.4 years (range, 23 to 68), and 58 percent were women. Half of all patients had undergone previous cosmetic procedures.
Table 1.
Demographic and Baseline Characteristics
| Patients (N = 66) | |
|---|---|
| Age, mean (SD), year | 46.4 (11.6) |
| Sex, no. (%) female | 38 (58) |
| BMI, mean (SD), kg/m2 | 26.2 (3.3) |
| Previous cosmetic procedures, no. (%) | 33 (50) |
BMI, body mass index.
The mean number of ATX-101 treatments for reduction of jowl fat was 1.8 per patient (Table 2). Mean ATX-101 injection volume was 0.8 ml per treatment per jowl, and mean interval between ATX-101 jowl treatments was 8.6 weeks. Fifteen patients received 0.1-ml injections, whereas the remaining 51 patients received 0.2-ml injections in the jowl. All patients received both jowl and submental fat treatments concurrently or in separate sessions.
Table 2.
Jowl Treatment Parameters
| Patients (N = 66) | |
|---|---|
| No. of ATX-101 treatments, mean (SD) | 1.8 (0.8) |
| Interval between ATX-101 treatments, mean (SD), wk | 8.6 (4.8) |
| Total volume of ATX-101 injected per treatment, mean (SD), ml | 0.8 (0.3) |
| Total volume of ATX-101 per injection, mean (SD), ml | 0.2 (0.0) |
Improvement in jowl appearance was achieved by 98 percent (65/66) of patients. One patient did not see sufficient improvement in jowl appearance after one ATX-101 treatment and was considering a neck lift for further treatment. Representative before/after treatment photographs are shown in Figures 2 through 4.
Fig. 2.

A 59-year-old female patient received two ATX-101 treatments for reduction of jowl fat (1.0 ml per jowl per treatment; total volume: 4 ml) and submental fat (8 and 6 ml; total volume: 14 ml). She is seen here before the first treatment (above) and 6 months after her final treatment (below).
Fig. 4.

A 62-year-old male patient received two ATX-101 treatments over a 3-month period for reduction of jowl fat. The jowls were treated equally and bilaterally with 1.2 ml and 0.8 ml, respectively. He is seen here before the first treatment (above) and 9 months after his second and final treatment (below).
Fig. 3.

A 47-year-old female patient received three ATX-101 treatments (5 ml, 5 ml, 2 ml, respectively) over a 9-month period for reduction of submental fullness and jowl fat. The jowls were treated equally and bilaterally with 1.2 ml, 0.8 ml, and 0.6 ml, respectively. She is seen here before the first treatment (above) and 6 months after her third and final treatment (below).
Video. This video provides a demonstration of the marking for injection of ATX-101 into the fat pad of the jowl of a patient.
Common injection-site adverse events included edema, numbness, tenderness, and bruising, which resolved with a mean duration of 4 to 29 days (Table 3). Three patients experienced injection-site marginal mandibular nerve paresis, which resolved within a mean period of 26 days (range, 14 to 40 days). Three patients experienced injection-site alopecia, which resolved within a mean period of 95 days (range, 64 to 126 days).
Table 3.
Incidence and Duration of Injection-Site Adverse Events
| Adverse Event | N = 66 | |
|---|---|---|
| Incidence, No. (%) | Duration, Mean (SD), days | |
| Edema | 66 (100) | 6.8 (3.5)* |
| Numbness | 66 (100) | 28.6 (11.3)† |
| Tenderness | 60 (91) | 4.4 (3.5)‡ |
| Bruising | 11 (17) | NA |
| Marginal mandibular nerve paresis | 3 (5) | 26.0 (13.1) |
| Alopecia | 3 (5) | 95.0 (31.0)§ |
NA, not available.
*Duration of edema for three events was not available.
†Duration of numbness for nine events was not available.
‡Duration of tenderness for two events was not available.
§Duration of alopecia for one event was not available.
DISCUSSION
The loss of jawline definition is a hallmark of the aging face, even in individuals with a well-contoured neck. Jowl fat is frequently contiguous with submental fat, and it is rare for patients to have focal descending jowl fat with no submental fullness in the maturing face. On the other hand, younger patients often present with submental fat but no signs of jowling, and only treatment of the submentum is required. Evaluation of both the jowl and submental area is essential for global lower face rejuvenation.
Jowl fat and submental fat can be treated at the same time or separately. Patients often request these treatments simultaneously, because they can appreciate the neck and jawline as a single aesthetic unit. Careful assessment of the jowling mechanism and contributors to submental fullness is critical before treatment. Only jowling caused by fat flow over the mandible without evidence of major superior compartment ptosis should be considered for treatment with ATX-101. If treating submental fat as well, one must ensure that an obtuse cervicomental angle is the result of excess preplatysmal submental fat for ATX-101 to be effective. Patients can have submental fullness with causes other than excess preplatysmal submental fat, such as skin laxity and platysma diastasis, which contraindicate use of ATX-101. Prominent submandibular glands, postplatysmal fat, or digastric muscle hypertrophy can also contribute to submental fullness and would not be improved with ATX-101 treatment. ATX-101, however, could be used as adjunctive treatment to reduce residual fat along the jawline and jowls after surgical rejuvenation of the aging face.
The methods described here provide insights into treating jowl fat with ATX-101. The author recommends that injection volume and spacing be reduced for treatment of small jowl surface areas. The marginal mandibular nerve is superficial to the facial artery and vein,25 and care must be taken to avoid injury to this nerve when treating jowl fat and submental fat. It has been proposed that an asymmetric smile may be more likely from damage to the cervical nerve branches when ATX-101 is injected too deeply, hitting the platysmal surface, causing muscular injury and dysfunction. The authors recommended ensuring that injections of ATX-101 are within the midsubcutaneous space.26 The injection technique requires adequate pinching and pulling of fat and skin away from underlying structures. Jowl fat should be assessed by the physician and patient at least 30 days after each treatment to determine if additional treatments are appropriate and/or desired.
Men may be particularly interested in jowl fat treatment compared with typical cosmetic procedures. Loss of jawline definition occurs as men age and is an area of aesthetic concern.1,27 Survey data among men and women from 2015 show that 74 percent (80/108) of respondents found a male jaw angle concealed by fat, sagging skin, and/or a beard aesthetically unpleasing.28 The availability of ATX-101 as a minimally invasive treatment for improving the contour of the chin and jaw attracts aesthetically naive men to the clinic.29 Furthermore, in the author’s experience, the high satisfaction rate with ATX-101 treatment brings both established and procedure-naive patients (men and women) back for other procedures. A number of patients in this study had previous chin and neck treatments but wanted further improvement in their jaw, chin, and neck contour using less invasive treatments such as ATX-101.
Limitations of this study include the relatively small number of patients; the lack of a randomized, placebo-controlled design; a limited follow-up period; and the lack of a validated assessment tool for jowl fat reduction.
In this first prospective, interventional study, ATX-101 was effective in improving jowl appearance and was well tolerated in this patient population, providing a minimally invasive treatment option for jowling caused by excess fat. Further investigations are warranted to develop an assessment tool for jowl fat reduction and establish standards of practice for maximal safety and efficacy when treating excess jowl fat with ATX-101.
PATIENT CONSENT
Patients provided written consent for the use of their images.
ACKNOWLEDGMENTS
Medical writing and editorial assistance were provided by Laura Breshears, Ph.D., of Evidence Scientific Solutions, and funded via an independent grant by Allergan plc, Dublin, Ireland. No payments were made for authorship, and Allergan was not involved in data generation and analysis or in the development of the manuscript.
Footnotes
Disclosure: Dr. Shridharani receives writing assistance from and is an advisory board member for Allergan. He is an advisory board member for Galderma, Merz, and Sientra.
A “Hot Topic Video” by Editor-in-Chief Rod J. Rohrich, M.D., accompanies this article. Go to PRSJournal.com and click on “Plastic Surgery Hot Topics” in the “Digital Media” tab to watch.
Related digital media are available in the full-text version of the article on www.PRSJournal.com.
REFERENCES
- 1.Jagdeo J, Keaney T, Narurkar V, Kolodziejczyk J, Gallagher CJ. Facial treatment preferences among aesthetically oriented men. Dermatol Surg. 2016;42:1155–1163. [DOI] [PubMed] [Google Scholar]
- 2.Narurkar V, Shamban A, Sissins P, Stonehouse A, Gallagher C. Facial treatment preferences in aesthetically aware women. Dermatol Surg. 2015;41(suppl 1):S153–S160. [DOI] [PubMed] [Google Scholar]
- 3.Honigman R, Castle DJ. Aging and cosmetic enhancement. Clin Interv Aging. 2006;1:115–119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ellenbogen R, Karlin JV. Visual criteria for success in restoring the youthful neck. Plast Reconstr Surg. 1980;66:826–837. [DOI] [PubMed] [Google Scholar]
- 5.Forte AJ, Andrew TW, Colasante C, Persing JA. Perception of age, attractiveness, and tiredness after isolated and combined facial subunit aging. Aesthetic Plast Surg. 2015;39:856–869. [DOI] [PubMed] [Google Scholar]
- 6.Rohrich RJ, Pessa JE. The fat compartments of the face: Anatomy and clinical implications for cosmetic surgery. Plast Reconstr Surg. 2007;119:2219–2227; discussion 2228–2231. [DOI] [PubMed] [Google Scholar]
- 7.Reece EM, Pessa JE, Rohrich RJ. The mandibular septum: Anatomical observations of the jowls in aging-implications for facial rejuvenation. Plast Reconstr Surg. 2008;121:1414–1420. [DOI] [PubMed] [Google Scholar]
- 8.Reece EM, Rohrich RJ. The aesthetic jaw line: Management of the aging jowl. Aesthet Surg J. 2008;28:668–674. [DOI] [PubMed] [Google Scholar]
- 9.Duncan DI, Palmer M. Fat reduction using phosphatidylcholine/sodium deoxycholate injections: Standard of practice. Aesthetic Plast Surg. 2008;32:858–872. [DOI] [PubMed] [Google Scholar]
- 10.Schlessinger J, Weiss SR, Jewell M, et al. Perceptions and practices in submental fat treatment: A survey of physicians and patients. Skinmed 2013;11:27–31. [PubMed] [Google Scholar]
- 11.Duncan DI, Chubaty R. Clinical safety data and standards of practice for injection lipolysis: A retrospective study. Aesthet Surg J. 2006;26:575–585. [DOI] [PubMed] [Google Scholar]
- 12.Kim IS, Hyun MY, Park KY, Kim CW, Kim BJ, Kim MN. Phosphatidylcholine and bipolar radiofrequency for treatment of localized fat deposits. J Dermatolog Treat. 2014;25:308–309. [DOI] [PubMed] [Google Scholar]
- 13.Wong GR, Chen WP. Phosphatidylcholine/deoxycholate lipolysis and hyaluronic acid augmentation to enhance nonsurgical lower facial contouring using botulinum toxin type A. J Cosmet Dermatol. 2011;10:159–162. [DOI] [PubMed] [Google Scholar]
- 14.Kybella (deoxycholic acid) injection [prescribing information]. 2015. Available at: https://www.allergan.com/assets/pdf/kybella_pi. Accessed July 10, 2018.
- 15.Belkyra (deoxycholic acid injection) [product monograph]. 2016. Available at: http://allergan-web-cdn-prod.azureedge.net/allergancanadaspecialty/allergancanadaspecialty/media/actavis-canada-specialty/en/products/pms/belkyra-pm-2016-03-28_e.pdf. Accessed July 10, 2018.
- 16.Duncan D, Rubin JP, Golitz L, et al. Refinement of technique in injection lipolysis based on scientific studies and clinical evaluation. Clin Plast Surg. 2009;36:195–209. [DOI] [PubMed] [Google Scholar]
- 17.Rotunda AM. Injectable treatments for adipose tissue: Terminology, mechanism, and tissue interaction. Lasers Surg Med. 2009;41:714–720. [DOI] [PubMed] [Google Scholar]
- 18.Rotunda AM, Suzuki H, Moy RL, Kolodney MS. Detergent effects of sodium deoxycholate are a major feature of an injectable phosphatidylcholine formulation used for localized fat dissolution. Dermatol Surg. 2004;30:1001–1008. [DOI] [PubMed] [Google Scholar]
- 19.Thuangtong R, Bentow JJ, Knopp K, Mahmood NA, David NE, Kolodney MS. Tissue-selective effects of injected deoxycholate. Dermatol Surg. 2010;36:899–908. [DOI] [PubMed] [Google Scholar]
- 20.Walker PS, Lee DR, Toth BA, Bowen B. Histological analysis of the effect of ATX-101 (deoxycholic acid injection) on subcutaneous fat: Results from a phase 1 open-label study. Dermatol Surg. 2020;46:70–77. [DOI] [PubMed] [Google Scholar]
- 21.Yagima Odo ME, Cucé LC, Odo LM, Natrielli A. Action of sodium deoxycholate on subcutaneous human tissue: Local and systemic effects. Dermatol Surg. 2007;33:178–188; discussion 188–191. [DOI] [PubMed] [Google Scholar]
- 22.Mess SA. Lower face rejuvenation with injections: Botox, Juvederm, and Kybella for marionette lines and jowls. Plast Reconstr Surg Glob Open 2017;5:e1551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Carruthers J, Humphrey S. Sodium deoxycholate for contouring of the jowl: Our preliminary experience. Dermatol Surg. 2019;45:165–167. [DOI] [PubMed] [Google Scholar]
- 24.Shridharani SM. Novel surface anatomic landmarks of the jowl to guide treatment with ATX-101. Plast Reconstr Surg Glob Open 2019;7:e2459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Batra AP, Mahajan A, Gupta K. Marginal mandibular branch of the facial nerve: An anatomical study. Indian J Plast Surg. 2010;43:60–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sorenson E, Chesnut C. Marginal mandibular versus pseudo-marginal mandibular nerve injury with submandibular deoxycholic acid injection. Dermatol Surg. 2018;44:733–735. [DOI] [PubMed] [Google Scholar]
- 27.de Maio M. Ethnic and gender considerations in the use of facial injectables: Male patients. Plast Reconstr Surg. 2015;136(5 suppl):40S–43S. [DOI] [PubMed] [Google Scholar]
- 28.Mommaerts MY. The ideal male jaw angle: An Internet survey. J Craniomaxillofac Surg. 2016;44:381–391. [DOI] [PubMed] [Google Scholar]
- 29.Shridharani SM, Behr KL. ATX-101 (deoxycholic acid injection) treatment in men: Insights from our clinical experience. Dermatol Surg. 2017;43(suppl 2):S225–S230. [DOI] [PubMed] [Google Scholar]